



Quantitative Insight into PCA Formation following Different Chlorhexidine Activation Methods in Endodontic Treatment


Abstract
:1. Introduction
2. Results
2.1. CHX Activation and Temperature Effect
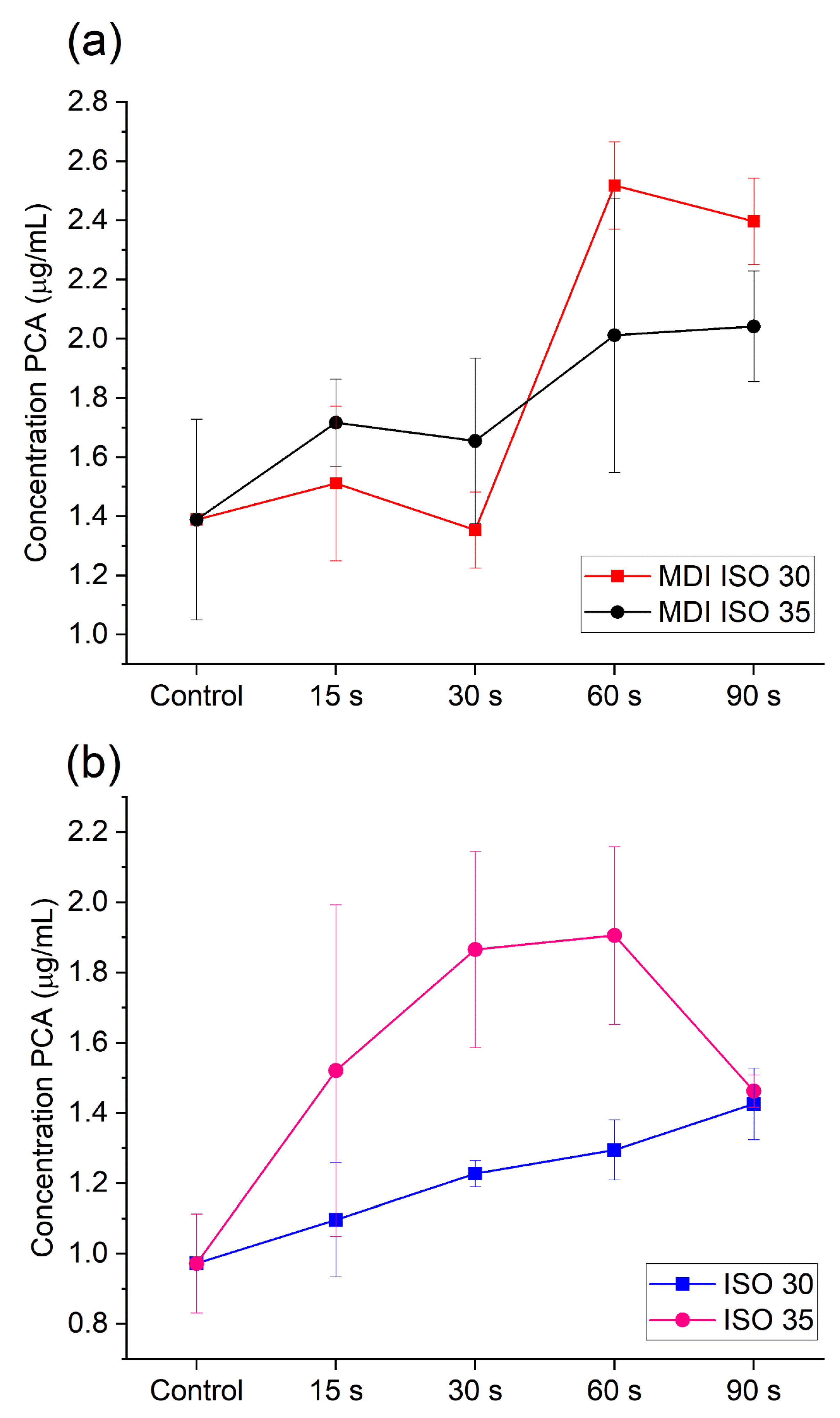
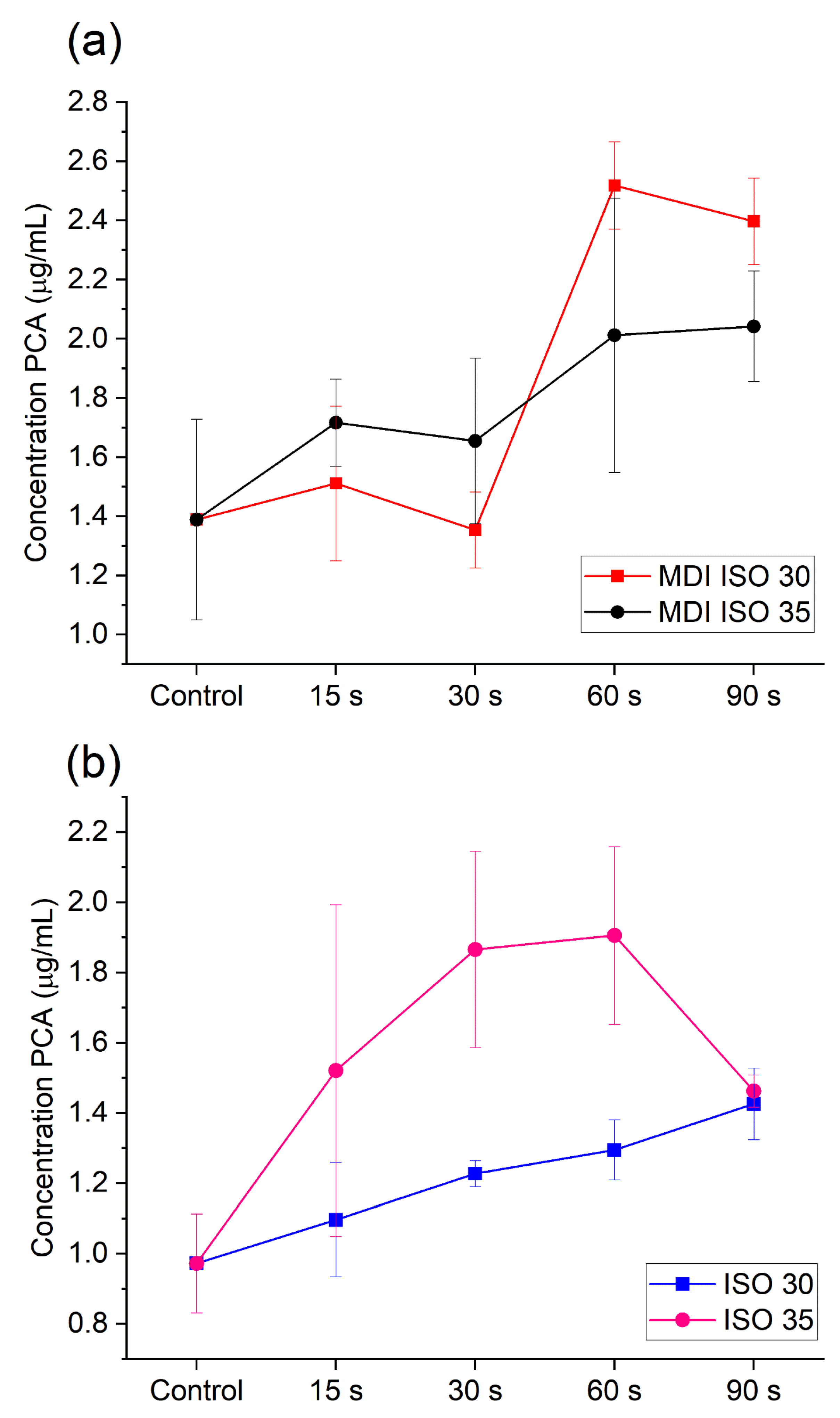
2.2. PCA Release during US and MDI Activation of 2% CHX
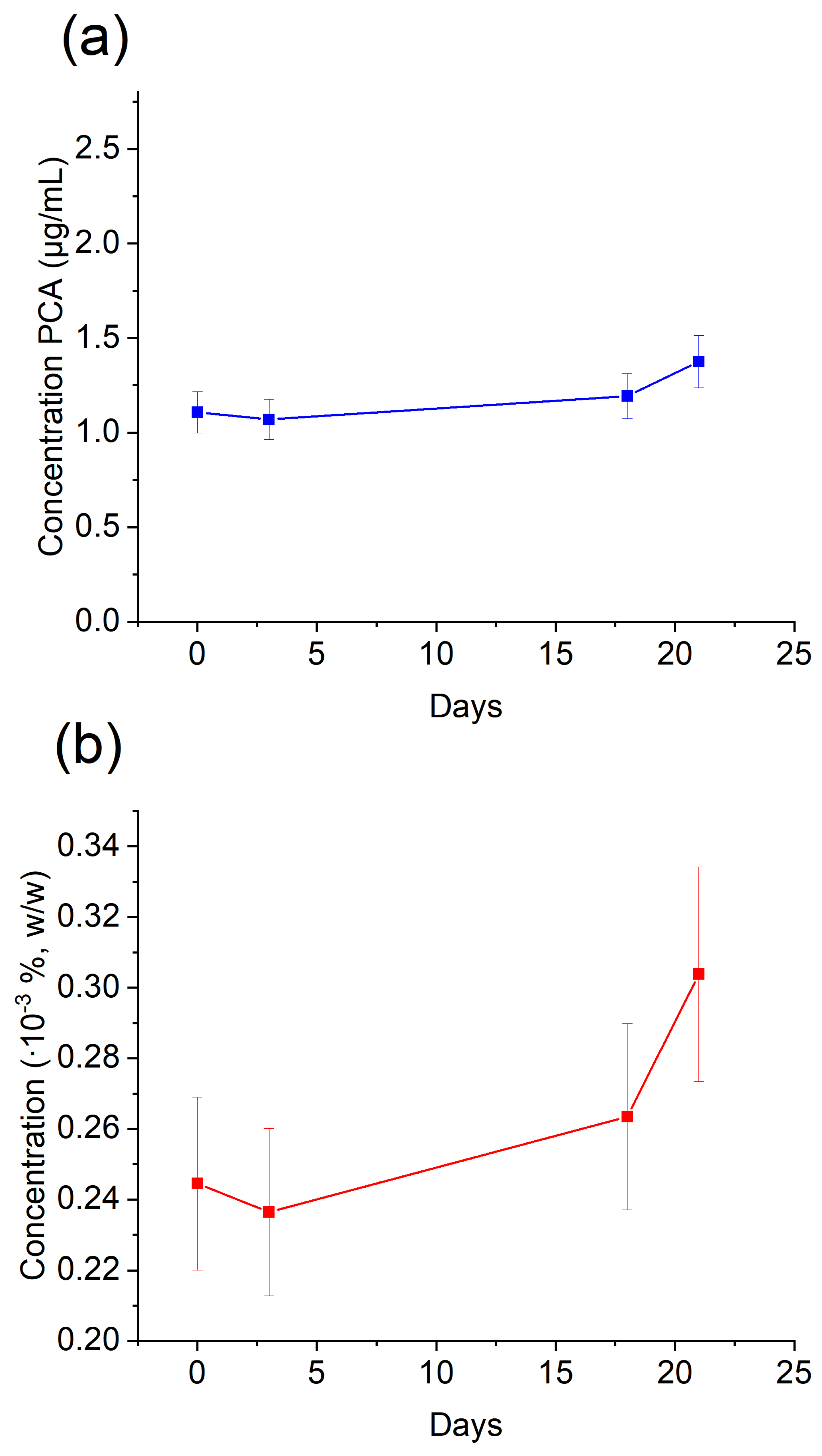
2.3. PCA Release from Shelf-Stored 2% CHX
3. Discussion
4. Materials and Methods
4.1. Instrumentation
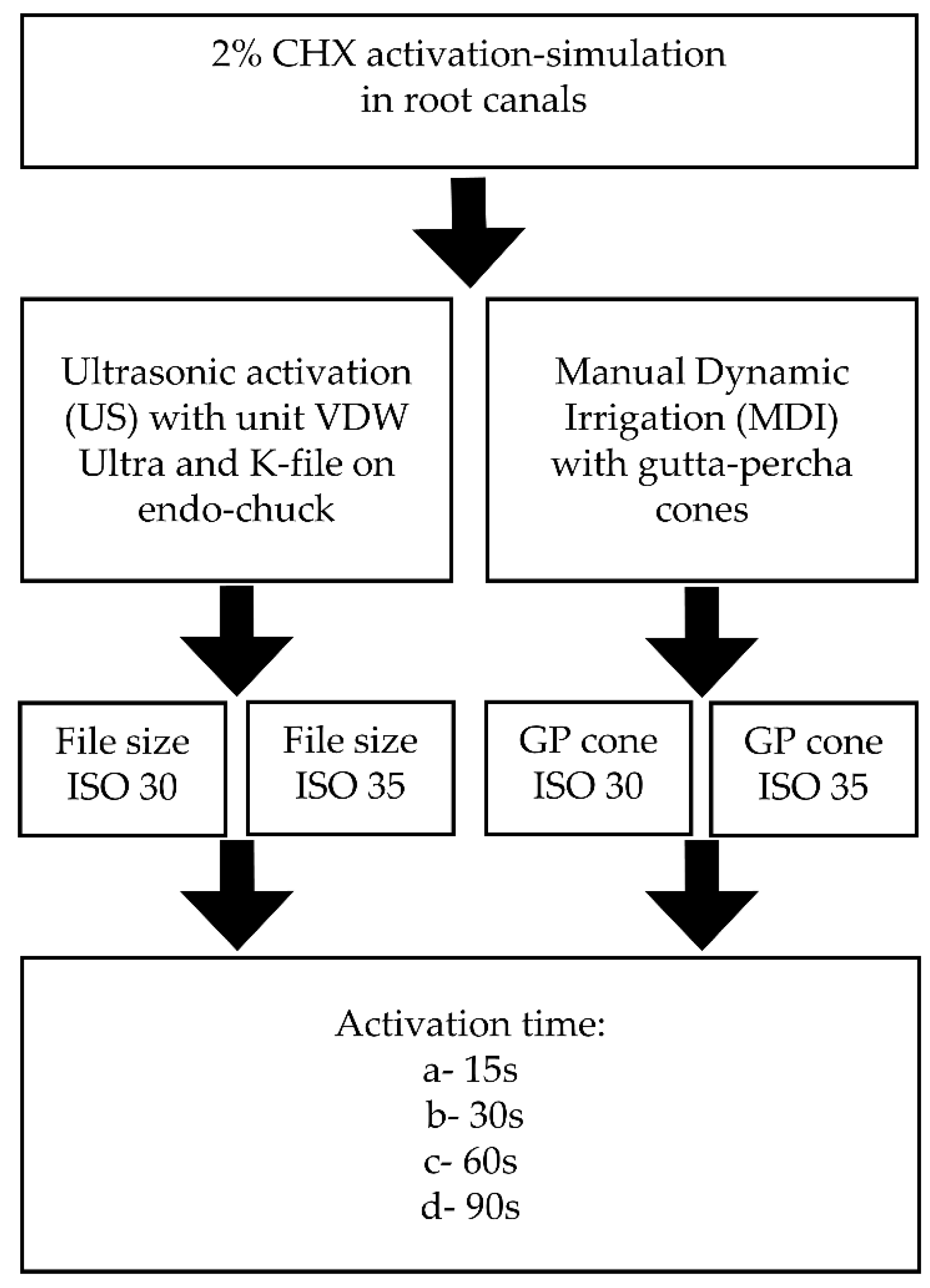
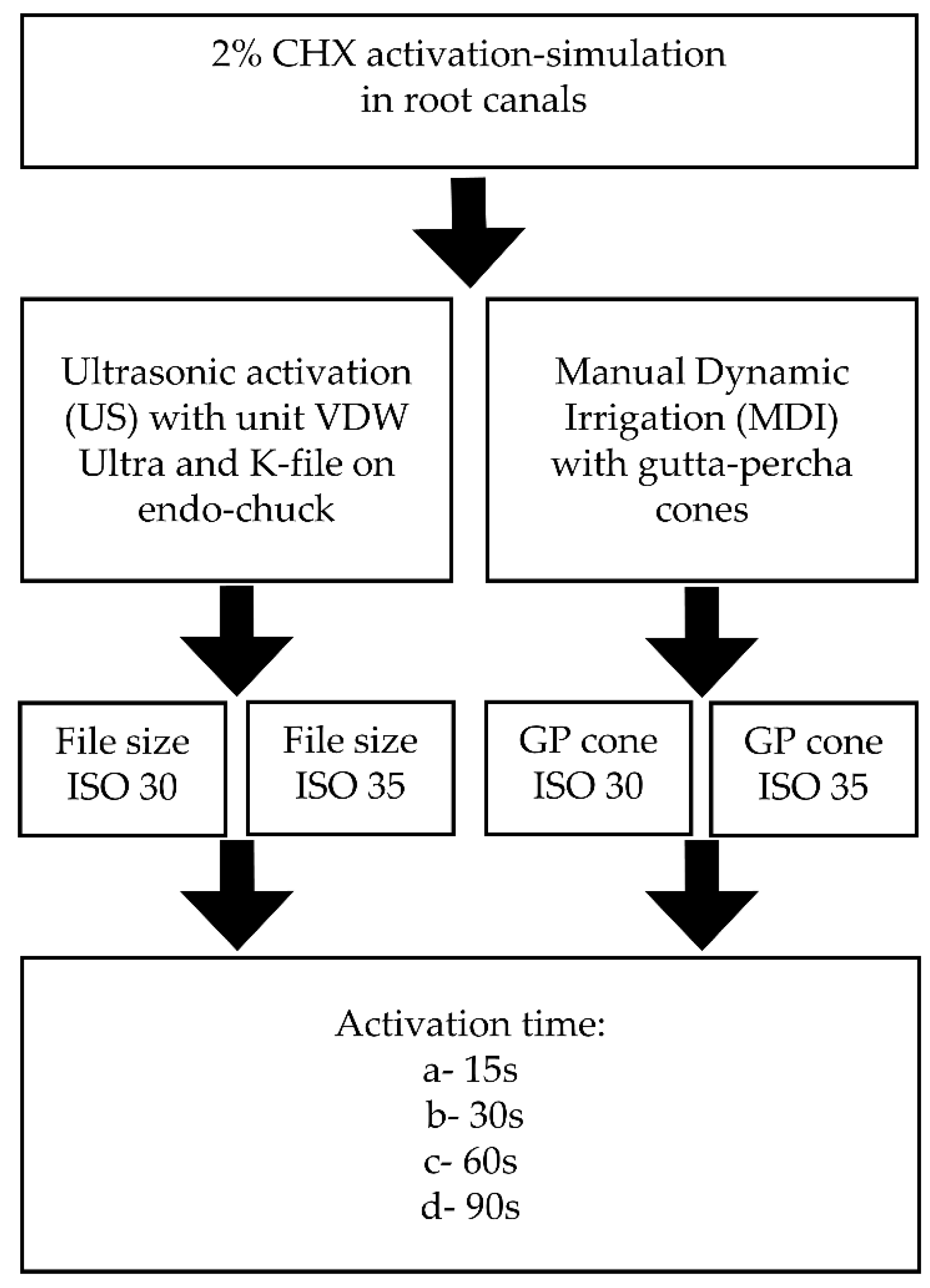
4.2. Design of Experiment: Experimental Groups and CHX Agitation Procedure with Dental Equipment
4.3. Preparation of Samples for HPLC Analysis
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Liang, A.; Huang, L.; Li, B.; Huang, Y.; Zhou, X.; Zhang, X.; Gong, Q. Micro-CT Evaluation of Different Root Canal Irrigation Protocols on the Removal of Accumulated Hard Tissue Debris: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 6053. [Google Scholar] [CrossRef]
- Vashisht, R.; Kumar, U.; Jhamb, S.; Singla, R. Comparative evaluation of cleaning efficiency of single file NiTi rotary system during root canal treatment procedure—A scanning electron microscope study. J. Conserv. Dent. 2023, 26, 316–320. [Google Scholar] [CrossRef]
- Haapasalo, M.; Shen, Y.; Wang, Z.; Gao, Y. Irrigation in endodontics. Br. Dent. J. 2014, 216, 299–303. [Google Scholar] [CrossRef]
- Cai, C.; Chen, X.; Li, Y.; Jiang, Q. Advances in the Role of Sodium Hypochlorite Irrigant in Chemical Preparation of Root Canal Treatment. BioMed Res. Int. 2023, 13, 8858283. [Google Scholar] [CrossRef] [PubMed]
- Chalub, L.O.; Nunes, G.P.; Strazzi-Sahyon, H.B.; Ferrisse, T.M.; dos Santos, P.H.; Gomes-Filho, J.E.; Cintra, L.T.A.; Sivieri-Araujo, G. Antimicrobial effectiveness of ultrasonic irrigation in root canal treatment: A systematic review of randomized clinical trials and meta-analysis. Clin. Oral Investig. 2023, 27, 1343–1361. [Google Scholar] [CrossRef]
- Hülsmann, M.; Heckendorff, M.; Lennon, Á. Chelating agents in root canal treatment: Mode of action and indications for their use. Int. Endod. J. 2003, 36, 810–830. [Google Scholar] [CrossRef]
- Machado, R.; Garcia, L.D.F.R.; da Silva Neto, U.X.; Cruz Filho, A.M.D.; Silva, R.G.; Vansan, L.P. Evaluation of 17% EDTA and 10% citric acid in smear layer removal and tubular dentin sealer penetration. Microsc. Res. Tech. 2018, 81, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Delgado, M.; Camps-Font, O.; Luz, L.; Sanz, D.; Mercade, M. Update on citric acid use in endodontic treatment: A systematic review. Odontology 2023, 111, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Souza, M.; Cecchin, D.; Farina, A.P.; Leite, C.E.; Cruz, F.F.; Pereira, C.d.C.; Ferraz, C.C.R.; Figueiredo, J.A.P. Evaluation of Chlorhexidine Substantivity on Human Dentin: A Chemical Analysis. J. Endod. 2012, 38, 1249–1252. [Google Scholar] [CrossRef]
- Siqueira, F.S., Jr.; Rôças, I.D.N.; Marceliano-Alves, M.F.; Pérez, A.R.; Ricucci, D. Unprepared root canal surface areas: Causes, clinical implications, and therapeutic strategies. Braz. Oral Res. 2018, 32 (Suppl. S1), e65. [Google Scholar] [CrossRef]
- Natanasabapathy, V.; Durvasulu, A.; Krithikadatta, J.; Namasivayam, A.; Deivanayagam, K.; Manali, S.; Sureshbabu, N.M. Current Trends in the Use of Irrigant Activation Techniques Among Endodontists & Post-Graduate Dental Students in India—A Knowledge, Attitude and Practice Based Survey. Eur. Endod. J. 2020, 5, 73–80. [Google Scholar] [CrossRef]
- Adcock, J.M.; Sidow, S.J.; Looney, S.W.; Liu, Y.; McNally, K.; Lindsey, K.; Tay, F.R. Histologic Evaluation of Canal and Isthmus Debridement Efficacies of Two Different Irrigant Delivery Techniques in a Closed System. J. Endod. 2011, 37, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.-M.; Verhaagen, B.; Versluis, M.; Langedijk, J.; Wesselink, P.; van der Sluis, L.W. The Influence of the Ultrasonic Intensity on the Cleaning Efficacy of Passive Ultrasonic Irrigation. J. Endod. 2011, 37, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.-M.; Lak, B.; Eijsvogels, L.M.; Wesselink, P.; van der Sluis, L.W. Comparison of the Cleaning Efficacy of Different Final Irrigation Techniques. J. Endod. 2012, 38, 838–841. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Patni, P.M.; Jain, P.; Raghuwanshi, S.; Pandey, S.H.; Tripathi, S.; Soni, A. Comparison of Dentinal Tubular Penetration of Intracanal Heated and Preheated Sodium Hypochlorite Through Different Agitation Techniques. J. Endod. 2023, 49, 686–691. [Google Scholar] [CrossRef]
- Rico-Romano, C.; Zubizarreta-Macho, Á.; Baquero-Artigao, M.-R.; Mena-Alvarez, J. An analysis in vivo of intracanal bacterial load before and after chemo-mechanical preparation: A comparative analysis of two irrigants and two activation techniques. J. Clin. Exp. Dent. 2016, 8, e9–e13. [Google Scholar] [CrossRef]
- Salas, H.; Castrejon, A.; Fuentes, D.; Luque, A.; Luque, E. Evaluation of the penetration of CHX 2% on dentinal tubules using Conventional Irrigation, Sonic Irrigation (EDDY) and Passive Ultrasonic Irrigation (PUI) techniques: An in vitro study. J. Clin. Exp. Dent. 2021, 13, e37–e42. [Google Scholar] [CrossRef]
- Machtou, P. Manual Dynamic Activation (MDA) Technique. In Endodontic Irrigation, 1st ed.; Basrani, B., Ed.; Springer: Cham, Switzerland, 2015; Volume 1, pp. 149–155. [Google Scholar]
- Gonzalez, C.; Forner, L.; Llena, C.; Lozano, A. Temperature changes in 2% chlorhexidine gluconate using two activation methods with different intensity levels. J. Clin. Exp. Dent. 2018, 10, e458–e461. [Google Scholar] [CrossRef]
- Zeltner, M.; Peters, O.A.; Paqué, F. Temperature Changes During Ultrasonic Irrigation with Different Inserts and Modes of Activation. J. Endod. 2009, 35, 573–577. [Google Scholar] [CrossRef]
- Basrani, B.R.; Manek, S.; Fillery, E. Using Diazotization to Characterize the Effect of Heat or Sodium Hypochlorite on 2.0% Chlorhexidine. J. Endod. 2009, 35, 1296–1299. [Google Scholar] [CrossRef]
- Jeong, J.W.; Sarmast, N.D.; Terlier, T.; van der Hoeven, R.; Holland, J.N.; Parikh, N. Assessment of the cytotoxic effects and chemical composition of the insoluble precipitate formed from sodium hypochlorite and chlorhexidine gluconate. Int. Endod. J. 2021, 54, 1892–1901. [Google Scholar] [CrossRef] [PubMed]
- Chhabra, R.; Huff, J.; Haseman, J.; Elwell, M.; Peters, A. Carcinogenicity of p-chloroaniline in rats and mice. Food Chem. Toxicol. 1991, 29, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Bui, T.B.; Baumgartner, J.C.; Mitchell, J.C. Evaluation of the Interaction between Sodium Hypochlorite and Chlorhexidine Gluconate and its Effect on Root Dentin. J. Endod. 2008, 34, 181–185. [Google Scholar] [CrossRef]
- Burkhardt-Holm, P.; Oulmi, Y.; Schroeder, A.; Storch, V.; Braunbeck, T. Toxicity of 4-Chloroaniline in Early Life Stages of Zebrafish (Danio rerio): II. Cytopathology and Regeneration of Liver and Gills After Prolonged Exposure to Waterborne 4-Chloroaniline. Arch. Environ. Contam. Toxicol. 1999, 37, 85–102. [Google Scholar] [CrossRef]
- Hazardous Substances Data Bank (HSDB): A Database of the National Library of Medicines. Compound Summary: 4-Chloroaniline. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/7812 (accessed on 12 April 2023).
- van der Vorst, M.M.J.; Tamminga, P.; Wijburg, F.A.; Schutgens, R.B.H. Severe methaemoglobinaemia due to para-chloraniline intoxication in premature neonates. Eur. J. Pediatr. 1990, 150, 73. [Google Scholar] [CrossRef] [PubMed]
- Basrani, B.R.; Manek, S.; Sodhi, R.N.; Fillery, E.; Manzur, A. Interaction between Sodium Hypochlorite and Chlorhexidine Gluconate. J. Endod. 2007, 33, 966–969. [Google Scholar] [CrossRef] [PubMed]
- Barbin, L.E.; Saquy, P.C.; Guedes, D.F.C.; Sousa-Neto, M.D.; Estrela, C.; Pécora, J.D. Determination of para-Chloroaniline and Reactive Oxygen Species in Chlorhexidine and Chlorhexidine Associated with Calcium Hydroxide. J. Endod. 2008, 34, 1508–1514. [Google Scholar] [CrossRef]
- Macedo, R.G.; Verhaagen, B.; Wesselink, P.R.; Versluis, M.; van der Sluis, L.W.M. Influence of refreshment/activation cycles and temperature rise on the reaction rate of sodium hypochlorite with bovine dentine during ultrasonic activated irrigation. Int. Endod. J. 2014, 47, 147–154. [Google Scholar] [CrossRef]
- De Bem, S.H.C.; Estrela, C.; Guedes, D.F.C.; Sousa-Neto, M.D.; Pécora, J.D. Determination of chemical components derived from 2% chlorhexidine gel degradation using gas chromatography-mass spectrometry. Acta Odontol. Scand. 2014, 72, 630–638. [Google Scholar] [CrossRef]
- Özdemir, O.; Kopac, T. Cytotoxicity and biocompatibility of root canal sealers: A review on recent studies. J. Appl. Biomater. Funct. Mater. 2022, 20, 22808000221076325. [Google Scholar] [CrossRef]
- Tartari, T.; Wichnieski, C.; Silva, R.M.; Letra, A.; Duarte, M.A.H.; Bramante, C.M. Final irrigation protocols can be used to promote stable long-term bond strength of AH Plus to dentin. J. Appl. Oral Sci. 2023, 31, e20230005. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Available online: https://cfpub.epa.gov/ncea/pprtv/documents/Chloroanilinep.pdf (accessed on 12 April 2023).


{kind=link}
{kind=link}
{kind=link}
| Activation Type | Activation Time [s] | Temperature Change ΔT, [°C] | |
|---|---|---|---|
| ISO 30 | ISO 35 | ||
| US | 15 | +3 | +4 |
| 30 | +3 | +3 | |
| 60 | +3 | +3 | |
| 90 | +4 | +4 | |
| ISO 30 | ISO 35 | ||
| MDI | 15 | 0 | 0 |
| 30 | 0 | 0 | |
| 60 | 0 | 0 | |
| 90 | 0 | 0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czopik, B.; Woźniakiewicz, A.; Świętoniowska, N.; Zarzecka, J.; Woźniakiewicz, M. Quantitative Insight into PCA Formation following Different Chlorhexidine Activation Methods in Endodontic Treatment. Molecules 2023, 28, 6159. https://doi.org/10.3390/molecules28166159
Czopik B, Woźniakiewicz A, Świętoniowska N, Zarzecka J, Woźniakiewicz M. Quantitative Insight into PCA Formation following Different Chlorhexidine Activation Methods in Endodontic Treatment. Molecules. 2023; 28(16):6159. https://doi.org/10.3390/molecules28166159
Chicago/Turabian StyleCzopik, Barbara, Aneta Woźniakiewicz, Natalia Świętoniowska, Joanna Zarzecka, and Michał Woźniakiewicz. 2023. "Quantitative Insight into PCA Formation following Different Chlorhexidine Activation Methods in Endodontic Treatment" Molecules 28, no. 16: 6159. https://doi.org/10.3390/molecules28166159
APA StyleCzopik, B., Woźniakiewicz, A., Świętoniowska, N., Zarzecka, J., & Woźniakiewicz, M. (2023). Quantitative Insight into PCA Formation following Different Chlorhexidine Activation Methods in Endodontic Treatment. Molecules, 28(16), 6159. https://doi.org/10.3390/molecules28166159