
Polymyxin B Combined with Minocycline: A Potentially Effective Combination against blaOXA-23-harboring CRAB in In Vitro PK/PD Model


Abstract
1. Introduction
2. Results
2.1. Genetic Information, MICs, and Checkboard Assays
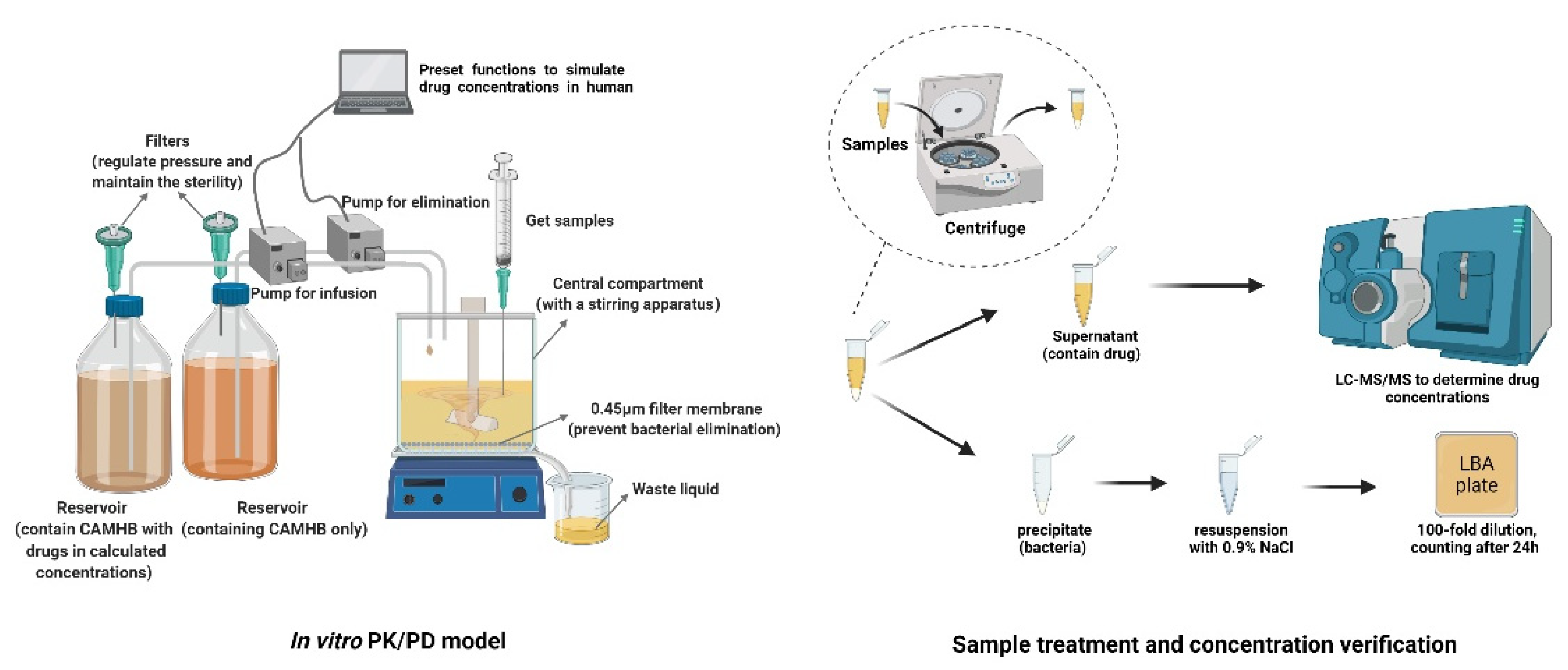
2.2. Dynamic PK/PD Model
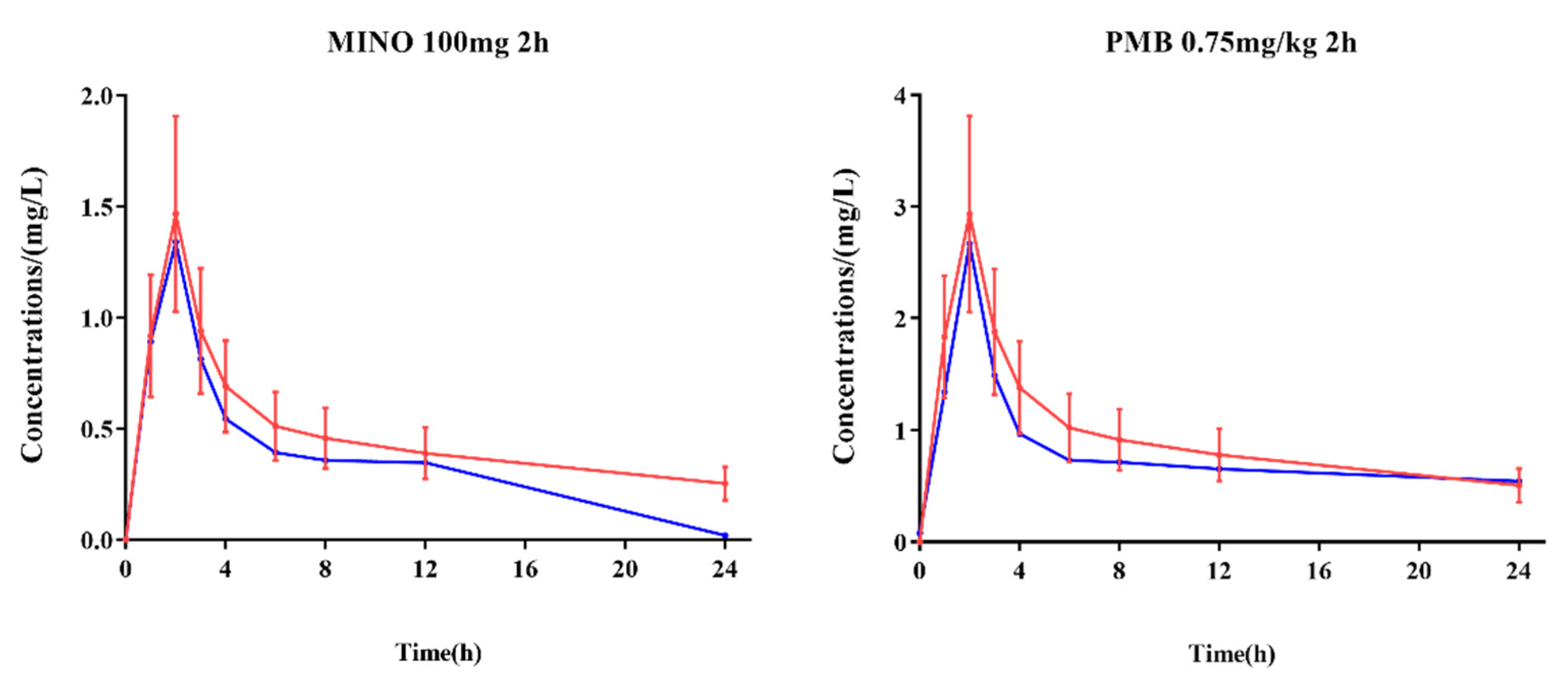
2.2.1. Concentration Verification
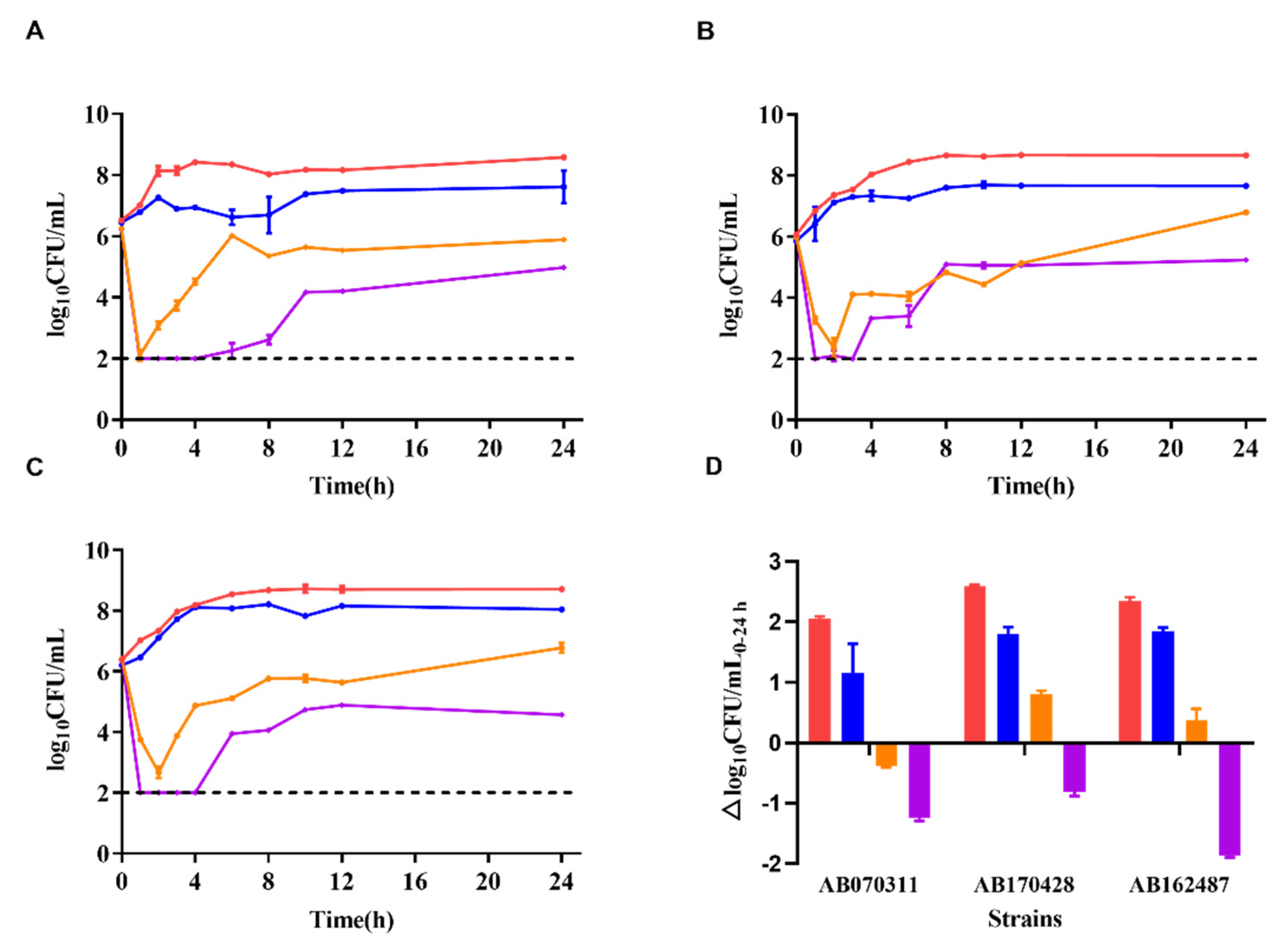
2.2.2. Time-Kill Curves
2.2.3. PK/PD Calculation
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savoldi, A.; Carrara, E.; Piddock, L.J.V.; Franceschi, F.; Ellis, S.; Chiamenti, M.; Bragantini, D.; Righi, E.; Tacconelli, E. The role of combination therapy in the treatment of severe infections caused by carbapenem resistant gram-negatives: A systematic review of clinical studies. BMC Infect. Dis. 2021, 21, 545. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Zhao, C.; Li, H.; Wang, R.; Wang, Q.; Wang, H. Clinical profile, prognostic factors, and outcome prediction in hospitalized patients with bloodstream infection: Results from a 10-year prospective multicenter study. Front. Med. 2021, 8, 629671. [Google Scholar] [CrossRef] [PubMed]
- Peleg, A.Y.; Hooper, D.C. Hospital-acquired infections due to gram-negative bacteria. N. Engl. J. Med. 2010, 362, 1804–1813. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Kasiakou, S.K. Toxicity of polymyxins: A systematic review of the evidence from old and recent studies. Crit. Care 2006, 10, R27. [Google Scholar] [CrossRef] [PubMed]
- Velkov, T.; Dai, C.; Ciccotosto, G.D.; Cappai, R.; Hoyer, D.; Li, J. Polymyxins for CNS infections: Pharmacology and neurotoxicity. Pharmacol. Ther. 2018, 181, 85–90. [Google Scholar] [CrossRef]
- Tam, V.H.; Schilling, A.N.; Vo, G.; Kabbara, S.; Kwa, A.L.; Wiederhold, N.P.; Lewis, R.E. Pharmacodynamics of polymyxin B against Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2005, 49, 3624–3630. [Google Scholar] [CrossRef] [PubMed]
- Cheah, S.E.; Wang, J.; Nguyen, V.T.; Turnidge, J.D.; Li, J.; Nation, R.L. New pharmacokinetic/pharmacodynamic studies of systemically administered colistin against Pseudomonas aeruginosa and Acinetobacter baumannii in mouse thigh and lung infection models: Smaller response in lung infection. J. Antimicrob. Chemother. 2015, 70, 3291–3297. [Google Scholar]
- Nang, S.C.; Azad, M.A.K.; Velkov, T.; Zhou, Q.T.; Li, J. Rescuing the last-line polymyxins: Achievements and challenges. Pharmacol. Rev. 2021, 73, 679–728. [Google Scholar] [CrossRef]
- Ma, X.; He, Y.; Yu, X.; Cai, Y.; Zeng, J.; Cai, R.; Lu, Y.; Chen, L.; Chen, C.; Huang, B. Ceftazidime/avibactam improves the antibacterial efficacy of polymyxin B against polymyxin b heteroresistant KPC-2-producing Klebsiella pneumoniae and hinders emergence of resistant subpopulation in vitro. Front. Microbiol. 2019, 10, 2029. [Google Scholar] [CrossRef]
- Charretier, Y.; Diene, S.M.; Baud, D.; Chatellier, S.; Santiago-Allexant, E.; van Belkum, A.; Guigon, G.; Schrenzel, J. Colistin heteroresistance and involvement of the PmrAB regulatory system in Acinetobacter baumannii. Antimicrob. Agents Chemother. 2018, 62, e00788-18. [Google Scholar] [CrossRef]
- Lashinsky, J.N.; Henig, O.; Pogue, J.M.; Kaye, K.S. Minocycline for the treatment of multidrug and extensively drug-resistant A. baumannii: A review. Infect. Dis. Ther. 2017, 6, 199–211. [Google Scholar] [CrossRef]
- Bishburg, E.; Bishburg, K. Minocycline—An old drug for a new century: Emphasis on methicillin-resistant Staphylococcus aureus (MRSA) and Acinetobacter baumannii. Int. J. Antimicrob. Agents 2009, 34, 395–401. [Google Scholar] [CrossRef]
- Greig, S.L.; Scott, L.J. Intravenous minocycline: A review in Acinetobacter infections. Drugs 2016, 76, 1467–1476. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Mesa, N.; Zarzuelo, A.; Gálvez, J. Minocycline: Far beyond an antibiotic. Br. J. Pharmacol. 2013, 169, 337–352. [Google Scholar] [CrossRef] [PubMed]
- Alfouzan, W.A.; Noel, A.R.; Bowker, K.E.; Attwood, M.L.G.; Tomaselli, S.G.; MacGowan, A.P. Pharmacodynamics of minocycline against Acinetobacter baumannii studied in a pharmacokinetic model of infection. Int. J. Antimicrob. Agents 2017, 50, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.A.; Bauer, K.A.; Mangino, J.E. Bad bugs need old drugs: A stewardship program’s evaluation of minocycline for multidrug-resistant Acinetobacter baumannii infections. Clin. Infect. Dis. 2014, 59 (Suppl. S6), S381–S387. [Google Scholar] [CrossRef] [PubMed]
- He, S.; He, H.; Chen, Y.; Chen, Y.; Wang, W.; Yu, D. In vitro and in vivo analysis of antimicrobial agents alone and in combination against multi-drug resistant Acinetobacter baumannii. Front. Microbiol. 2015, 6, 507. [Google Scholar] [CrossRef] [PubMed]
- Bowers, D.R.; Cao, H.; Zhou, J.; Ledesma, K.R.; Sun, D.; Lomovskaya, O.; Tam, V.H. Assessment of minocycline and polymyxin B combination against Acinetobacter baumannii. Antimicrob. Agents Chemother. 2015, 59, 2720–2725. [Google Scholar] [CrossRef]
- Aranzana-Climent, V.; Buyck, J.M.; Smani, Y.; Pachón-Diaz, J.; Marchand, S.; Couet, W.; Grégoire, N. Semi-mechanistic PK/PD modelling of combined polymyxin B and minocycline against a polymyxin-resistant strain of Acinetobacter baumannii. Clin. Microbiol. Infect. 2020, 26, 1254.e9–1254.e15. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, F.; Sun, E.; Ma, R.; Qu, C.; Ma, L. In vitro antibacterial activity of combinations of fosfomycin, minocycline and polymyxin B on pan-drug-resistant Acinetobacter baumannii. Exp. Ther. Med. 2013, 5, 1737–1739. [Google Scholar] [CrossRef]
- Bian, X.; Liu, X.; Zhang, X.; Li, X.; Zhang, J.; Zheng, H.; Song, S.; Li, X.; Feng, M. Epidemiological and genomic characteristics of Acinetobacter baumannii from different infection sites using comparative genomics. BMC Genom. 2021, 22, 530. [Google Scholar] [CrossRef]
- LaPlante, K.L.; Rybak, M.J.; Leuthner, K.D.; Chin, J.N. Impact of Enterococcus faecalis on the bactericidal activities of arbekacin, daptomycin, linezolid, and tigecycline against methicillin-resistant Staphylococcus aureus in a mixed-pathogen pharmacodynamic model. Antimicrob. Agents Chemother. 2006, 50, 1298–1303. [Google Scholar] [CrossRef]
- Lyu, C.; Zhang, Y.; Liu, X.; Wu, J.; Zhang, J. Clinical efficacy and safety of polymyxins based versus non-polymyxins based therapies in the infections caused by carbapenem-resistant Acinetobacter baumannii: A systematic review and meta-analysis. BMC Infect. Dis. 2020, 20, 296. [Google Scholar] [CrossRef]
- Beganovic, M.; Daffinee, K.E.; Luther, M.K.; LaPlante, K.L. Minocycline alone and in combination with polymyxin b, meropenem, and sulbactam against carbapenem-susceptible and -resistant Acinetobacter baumannii in an in vitro pharmacodynamic model. Antimicrob. Agents Chemother. 2021, 65, e01680-20. [Google Scholar] [CrossRef] [PubMed]
- Bian, X.; Liu, X.; Hu, F.; Feng, M.; Chen, Y.; Bergen, P.J.; Li, J.; Li, X.; Guo, Y.; Zhang, J. Pharmacokinetic/pharmacodynamic based breakpoints of polymyxin B for bloodstream infections caused by multidrug-resistant gram-negative pathogens. Front. Pharmacol. 2022, 12, 785893. [Google Scholar] [CrossRef] [PubMed]
- Duan, N.; Sun, L.; Huang, C.; Li, H.; Cheng, B. Microbial distribution and antibiotic susceptibility of bloodstream infections in different intensive care units. Front. Microbiol. 2021, 12, 792282. [Google Scholar] [CrossRef]
- Bian, X.; Liu, X.; Feng, M.; Bergen, P.J.; Li, J.; Chen, Y.; Zheng, H.; Song, S.; Zhang, J. Enhanced bacterial killing with colistin/sulbactam combination against carbapenem-resistant Acinetobacter baumannii. Int. J. Antimicrob. Agents 2021, 57, 106271. [Google Scholar] [CrossRef] [PubMed]
- Bian, X.; Liu, X.; Chen, Y.; Chen, D.; Li, J.; Zhang, J. Dose optimization of colistin combinations against carbapenem-resistant Acinetobacter baumannii from patients with hospital-acquired pneumonia in China by using an in vitro pharmacokinetic/pharmacodynamic model. Antimicrob. Agents Chemother. 2019, 63, e01989-18. [Google Scholar] [CrossRef]
- He, J.; Liu, S.; Xia, P.; Chen, Y.; Tang, M.; Dai, Q.; Xiong, L. Pharmacokinetics of single and multiple intravenous doses of minocycline hydrochloride. Chin. J. New Drugs 2006, 15, 824–827. [Google Scholar]
- Welling, P.G.; Shaw, W.R.; Uman, S.J.; Tse, F.L.; Craig, W.A. Pharmacokinetics of minocycline in renal failure. Antimicrob. Agents Chemother. 1975, 8, 532–537. [Google Scholar] [CrossRef]
- Macdonald, H.; Kelly, R.G.; Allen, E.S.; Noble, J.F.; Kanegis, L.A. Pharmacokinetic studies on minocycline in man. Clin. Pharmacol. Ther. 1973, 14, 852–861. [Google Scholar] [CrossRef] [PubMed]
- MINOCIN® Minocycline for Injection 100 mg/vial. Available online: https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=e415c323-8219-464b-9e3e-72c5a796cdaa (accessed on 1 January 2022).
- Kubin, C.J.; Nelson, B.C.; Miglis, C.; Scheetz, M.H.; Rhodes, N.J.; Avedissian, S.N.; Cremers, S.; Yin, M.T. Population pharmacokinetics of intravenous polymyxin B from clinical samples. Antimicrob. Agents Chemother. 2018, 62, e01493-17. [Google Scholar] [CrossRef] [PubMed]
- Trimble, M.J.; Mlynárčik, P.; Kolář, M.; Hancock, R.E. Polymyxin: Alternative mechanisms of action and resistance. Cold Spring Harb. Perspect. Med. 2016, 6, a025288. [Google Scholar] [CrossRef] [PubMed]
- Asadi, A.; Abdi, M.; Kouhsari, E.; Panahi, P.; Sholeh, M.; Sadeghifard, N.; Amiriani, T.; Ahmadi, A.; Maleki, A.; Gholami, M. Minocycline, focus on mechanisms of resistance, antibacterial activity, and clinical effectiveness: Back to the future. J. Glob. Antimicrob. Resist. 2020, 22, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Morozumi, M.; Okada, T.; Tajima, T.; Ubukata, K.; Iwata, S. Killing kinetics of minocycline, doxycycline and tosufloxacin against macrolide-resistant Mycoplasma pneumoniae. Int. J. Antimicrob. Agents 2017, 50, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Athamna, A.; Athamna, M.; Medlej, B.; Bast, D.J.; Rubinstein, E. In vitro post-antibiotic effect of fluoroquinolones, macrolides, beta-lactams, tetracyclines, vancomycin, clindamycin, linezolid, chloramphenicol, quinupristin/dalfopristin and rifampicin on Bacillus anthracis. J. Antimicrob. Chemother. 2004, 53, 609–615. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Homenuik, K.; Nichol, K.; Noreddin, A.; Vercaigne, L.; Embil, J.; Gin, A.; Karlowsky, J.A.; Hoban, D.J. The glycylcyclines: A comparative review with the tetracyclines. Drugs 2004, 64, 63–88. [Google Scholar] [CrossRef] [PubMed]
- Zavascki, A.P.; Nation, R.L. Nephrotoxicity of polymyxins: Is there any difference between colistimethate and polymyxin B? Antimicrob. Agents Chemother. 2017, 61, e02319-16. [Google Scholar] [CrossRef]
- Liu, X.; Chen, Y.; Yang, H.; Li, J.; Yu, J.; Yu, Z.; Cao, G.; Wu, X.; Wang, Y.; Wu, H.; et al. Acute toxicity is a dose-limiting factor for intravenous polymyxin B: A safety and pharmacokinetic study in healthy Chinese subjects. J. Infect. 2021, 82, 207–215. [Google Scholar] [CrossRef]
- Hu, J.; Kholmukhamedov, A.; Lindsey, C.C.; Beeson, C.C.; Jaeschke, H.; Lemasters, J.J. Translocation of iron from lysosomes to mitochondria during acetaminophen-induced hepatocellular injury: Protection by starch-desferal and minocycline. Free Radic. Biol. Med. 2016, 97, 418–426. [Google Scholar] [CrossRef]
- Dai, C.; Ciccotosto, G.D.; Cappai, R.; Wang, Y.; Tang, S.; Xiao, X.; Velkov, T. Minocycline attenuates colistin-induced neurotoxicity via suppression of apoptosis, mitochondrial dysfunction and oxidative stress. J. Antimicrob. Chemother. 2017, 72, 1635–1645. [Google Scholar] [CrossRef]
- Fragkou, P.C.; Poulakou, G.; Blizou, A.; Blizou, M.; Rapti, V.; Karageorgopoulos, D.E.; Koulenti, D.; Papadopoulos, A.; Matthaiou, D.K.; Tsiodras, S. The Role of minocycline in the treatment of nosocomial infections caused by multidrug, extensively drug and pandrug resistant Acinetobacter baumannii: A systematic review of clinical evidence. Microorganisms 2019, 7, 159. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.; Xiao, X.; Li, J.; Ciccotosto, G.D.; Cappai, R.; Tang, S.; Schneider-Futschik, E.K.; Hoyer, D.; Velkov, T.; Shen, J. Molecular mechanisms of neurotoxicity induced by polymyxins and chemoprevention. ACS Chem. Neurosci. 2019, 10, 120–131. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, B.T.; Pogue, J.M.; Zavascki, A.P.; Paul, M.; Daikos, G.L.; Forrest, A.; Giacobbe, D.R.; Viscoli, C.; Giamarellou, H.; Karaiskos, I.; et al. International consensus guidelines for the optimal use of the polymyxins: Endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy 2019, 39, 10–39. [Google Scholar] [PubMed]
- Neu, H.C. Mecillinam-an amidino penicillin which acts synergistically with other beta-lactam compounds. J. Antimicrob. Chemother. 1977, 3 (Suppl. SB), 43–52. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, S.; Sun, Z.; Han, B.; Kong, Y.; Zhou, L.; Zhu, Z.; Luo, Y.; Zhang, X. Population pharmacokinetics of polymyxin B in patients with sepsis. Chin. Pharm. J. 2021, 56, 744–748. [Google Scholar]
- Liu, X.; Yu, Z.; Wang, Y.; Wu, H.; Bian, X.; Li, X.; Fan, Y.; Guo, B.; Zhang, J. Therapeutic drug monitoring of polymyxin B by LC-MS/MS in plasma and urine. Bioanalysis 2020, 12, 845–855. [Google Scholar] [CrossRef]
- Patel, D.S.; Sharma, N.; Patel, M.C.; Patel, B.N.; Shrivastav, P.S.; Sanyal, M. Analysis of a second-generation tetracycline antibiotic minocycline in human plasma by LC-MS/MS. Bioanalysis 2011, 3, 2177–2194. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ARO Name | AB070311 | AB170428 | AB162487 | Antimicrobial Agents’ Classes |
|---|---|---|---|---|
| lpxC | √ | √ | √ | peptide antibiotic |
| lpxA | √ | √ | √ | |
| tetA | √ | √ | √ | glycylcycline; tetracycline antibiotic |
| tetR | √ | √ | √ | |
| adeA | √ | √ | √ | |
| adeB | √ | √ | √ | |
| adeC | √ | √ | √ | |
| adeR | √ | √ | √ | |
| adeS | √ | √ | √ | |
| adeF | √ | √ | √ | tetracycline antibiotic; fluoroquinolone antibiotic |
| adeG | √ | √ | √ | |
| adeH | √ | √ | √ | |
| adeL | √ | √ | √ | |
| adeN | √ | tetracycline antibiotic; fluoroquinolone antibiotic; cephalosporin; macrolide antibiotic; carbapenem; rifamycin antibiotic; lincosamide antibiotic; diaminopyrimidine antibiotic; phenicol antibiotic; penem | ||
| adeI | √ | √ | √ | |
| adeJ | √ | √ | √ | |
| adeK | √ | √ | √ | |
| MexK | √ | √ | √ | tetracycline antibiotic; triclosan; macrolide antibiotic |
| rpsJ | √ | √ | √ | tetracycline antibiotic |
| OXA-66 | √ | √ | √ | cephalosporin; penam |
| OXA-366 | √ | |||
| OXA-23 | √ | √ | √ | |
| TEM-1 | √ | √ | cephalosporin; penam; penem; monobactam | |
| Acinetobacter baumannii OprD conferring resistance to imipenem | √ | √ | √ | cephalosporin; penam; penem; monobactam; carbapenem; cephamycin |
| carO | √ | √ | √ | carbapenem |
| ADC-61 | √ | √ | cephalosporin | |
| ADC-78 | √ | |||
| MLST | ST195 | ST208 | ST191 |
| Antimicrobial Agents | AB070311 | AB170428 | AB162487 |
|---|---|---|---|
| polymyxin B | 0.5 (I) | 0.5 (I) | 0.25 (I) |
| minocycline | 4 (S) | 4 (S) | 8 (I) |
| doxycycline | 64 (R) | 64 (R) | 64 (R) |
| meropenem | 64 (R) | 16 (R) | 16 (R) |
| doripenem | 64 (R) | 32 (R) | 16 (R) |
| aztreonam * | 64 | 64 | 64 |
| cefoperazone * | >256 | >256 | >256 |
| sulbactam * | 16 | 16 | 16 |
| FICI(PMB/MINO) | 0.56 | 0.56 | 0.375 |
| AB070311 | AB170428 | AB163560 | ||||
|---|---|---|---|---|---|---|
| MIC | AUC/MIC | MIC | AUC/MIC | MIC | AUC/MIC | |
| PMB Alone | 0.50 | 38.14 | 0.50 | 38.14 | 0.25 | 76.28 |
| PMB Combined with MINO | 0.25 | 76.28 | 0.25 | 76.28 | 0.06 | 305.12 |
| MINO Alone | 4.00 | 2.15 | 4.00 | 2.15 | 8.00 | 1.08 |
| MINO Combined with PMB | 0.25 | 34.42 | 0.25 | 34.42 | 1.00 | 8.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qu, X.; Bian, X.; Chen, Y.; Hu, J.; Huang, X.; Wang, Y.; Fan, Y.; Wu, H.; Li, X.; Li, Y.; et al. Polymyxin B Combined with Minocycline: A Potentially Effective Combination against blaOXA-23-harboring CRAB in In Vitro PK/PD Model. Molecules 2022, 27, 1085. https://doi.org/10.3390/molecules27031085
Qu X, Bian X, Chen Y, Hu J, Huang X, Wang Y, Fan Y, Wu H, Li X, Li Y, et al. Polymyxin B Combined with Minocycline: A Potentially Effective Combination against blaOXA-23-harboring CRAB in In Vitro PK/PD Model. Molecules. 2022; 27(3):1085. https://doi.org/10.3390/molecules27031085
Chicago/Turabian StyleQu, Xingyi, Xingchen Bian, Yuancheng Chen, Jiali Hu, Xiaolan Huang, Yu Wang, Yaxin Fan, Hailan Wu, Xin Li, Yi Li, and et al. 2022. "Polymyxin B Combined with Minocycline: A Potentially Effective Combination against blaOXA-23-harboring CRAB in In Vitro PK/PD Model" Molecules 27, no. 3: 1085. https://doi.org/10.3390/molecules27031085
APA StyleQu, X., Bian, X., Chen, Y., Hu, J., Huang, X., Wang, Y., Fan, Y., Wu, H., Li, X., Li, Y., Guo, B., Liu, X., & Zhang, J. (2022). Polymyxin B Combined with Minocycline: A Potentially Effective Combination against blaOXA-23-harboring CRAB in In Vitro PK/PD Model. Molecules, 27(3), 1085. https://doi.org/10.3390/molecules27031085