
Circulating Levels of Dephosphorylated-Uncarboxylated Matrix Gla Protein in Patients with Acute Coronary Syndrome


 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design and Ethical Considerations
4.2. Subjects and Inclusion/Exclusion Criteria
4.3. Clinical and Laboratory Evaluations
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
References
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction. J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Gomar, F.; Perez-Quilis, C.; Leischik, R.; Lucia, A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann. Transl. Med. 2016, 4, 256. [Google Scholar] [CrossRef]
- Taylor, A.J.; Burke, A.P.; O’Malley, P.G.; Farb, A.; Malcom, G.T.; Smialek, J.; Virmani, R.A. comparison of the Framingham risk index, coronary artery calcification, and culprit plaque morphology in sudden cardiac death. Circulation 2000, 101, 1243–1248. [Google Scholar] [CrossRef]
- Kumrić, M.; Tičinović Kurir, T.; Borovac, J.A.; Božić, J. The Role of Natural Killer (NK) Cells in Acute Coronary Syndrome: A Comprehensive Review. Biomolecules 2020, 10, 1514. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, C.M.; Cary, N.R.; Salisbury, J.R.; Proudfoot, D.; Weissberg, P.L.; Edmonds, M.E. Medial localization of mineralization-regulating proteins in association with Monckeberg’s sclerosis: Evidence for smooth muscle cell-mediated vascular calcification. Circulation 1999, 100, 2168–2176. [Google Scholar] [CrossRef] [PubMed]
- Zettervall, S.L.; Marshall, A.P.; Fleser, P.; Guzman, R.J. Association of arterial calcification with chronic limb ischemia in patients with peripheral artery disease. J. Vasc. Surg. 2018, 67, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Moe, S.M.; O’Neill, K.D.; Duan, D.; Ahmed, S.; Chen, N.X.; Leapman, S.B.; Fineberg, N.; Kopecky, K. Medial artery calcification in ESRD patients is associated with deposition of bone matrix proteins. Kidney Int. 2002, 61, 638–647. [Google Scholar] [CrossRef] [PubMed]
- Tyson, K.L.; Reynolds, J.L.; McNair, R.; Zhang, Q.; Weissberg, P.L.; Shanahan, C.M. Osteochondrocytic transcription factors and their target genes exhibit distinct patterns of expression in human arterial calcification. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 489–494. [Google Scholar] [CrossRef]
- Bobryshev, Y.V. Transdifferentiation of smooth muscle cells into chondrocytes in atherosclerotic arteries in situ: Implications for diffuse intimal calcification. J. Pathol. 2005, 205, 641–650. [Google Scholar] [CrossRef]
- Yao, Y.; Jumabay, M.; Ly, A.; Radparvar, M.; Cubberly, M.R.; Boström, K.I. A role for the endothelium in vascular calcification. Circ. Res. 2013, 113, 495–504. [Google Scholar] [CrossRef]
- Price, P.A.; Otsuka, A.A.; Poser, J.W.; Kristaponis, J.; Raman, N. Characterization of a gamma-carboxyglutamic acid-containing protein from bone. Proc. Natl. Acad. Sci. USA 1976, 73, 1447–1451. [Google Scholar] [CrossRef] [PubMed]
- Speer, M.Y.; Yang, H.Y.; Brabb, T.; Leaf, E.; Look, A.; Lin, W.L.; Frutkin, A.; Dichek, D.; Giachelli, C.M. Smooth muscle cells give rise to osteochondrogenic precursors and chondrocytes in calcifying arteries. Circ. Res. 2009, 104, 733–741. [Google Scholar] [CrossRef]
- Barrett, H.; O’Keeffe, M.; Kavanagh, E.; Walsh, M.; O’Connor, E.M. Is Matrix Gla Protein Associated with Vascular Calcification? A Systematic Review. Nutrients 2018, 10, 415. [Google Scholar] [CrossRef]
- Schurgers, L.J.; Spronk, H.M.; Skepper, J.N.; Hackeng, T.M.; Shanahan, C.M.; Vermeer, C.; Weissberg, P.L.; Proudfoot, D.J. Post-translational modifications regulate matrix Gla protein function: Importance for inhibition of vascular smooth muscle cell calcification. Thromb. Haemost. 2007, 5, 2503–2511. [Google Scholar] [CrossRef] [PubMed]
- Dalmeijer, G.W.; van der Schouw, Y.T.; Magdeleyns, E.; Ahmed, N.; Vermeer, C.; Beulens, J.W. The effect of menaquinone-7 supplementation on circulating species of matrix Gla protein. Atherosclerosis 2012, 225, 397–402. [Google Scholar] [CrossRef]
- Luo, G.; Ducy, P.; McKee, M.D.; Pinero, G.J.; Loyer, E.; Behringer, R.R.; Karsenty, G. Spontaneous calcification of arteries and cartilage in mice lacking matrix GLA protein. Nature 1997, 386, 78–81. [Google Scholar] [CrossRef]
- Khavandgar, Z.; Roman, H.; Li, J.; Lee, S.; Vali, H.; Brinckmann, J.; Davis, E.C.; Murshed, M.J. Elastin haploinsufficiency impedes the progression of arterial calcification in MGP-deficient mice. Bone Miner. Res. 2014, 29, 327–337. [Google Scholar] [CrossRef]
- Shanahan, C.M.; Cary, N.R.; Metcalfe, J.C.; Weissberg, P.L. High expression of genes for calcification-regulating proteins in human atherosclerotic plaques. J. Clin. Investig. 1994, 93, 2393–2402. [Google Scholar] [CrossRef] [PubMed]
- Dhore, C.R.; Cleutjens, J.P.; Lutgens, E.; Cleutjens, K.B.; Geusens, P.P.; Kitslaar, P.J.; Tordoir, J.H.; Spronk, H.M.; Vermeer, C.; Daemen, M.J. Differential expression of bone matrix regulatory proteins in human atherosclerotic plaques. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 1998–2003. [Google Scholar] [CrossRef] [PubMed]
- Braam, L.A.; Dissel, P.; Gijsbers, B.L.; Spronk, H.M.; Hamulyák, K.; Soute, B.A.; Debie, W.; Vermeer, C. Assay for human matrix gla protein in serum: Potential applications in the cardiovascular field. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Schurgers, L.J.; Teunissen, K.J.; Knapen, M.H.; Kwaijtaal, M.; van Diest, R.; Appels, A.; Reutelingsperger, C.P.; Cleutjens, J.P.; Vermeer, C. Novel conformation-specific antibodies against matrix gamma-carboxyglutamic acid (Gla) protein: Undercarboxylated matrix Gla protein as marker for vascular calcification. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1629–1633. [Google Scholar] [CrossRef] [PubMed]
- Theuwissen, E.; Smit, E.; Vermeer, C. The role of vitamin K in soft-tissue calcification. Adv. Nutr. 2012, 3, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Mayer, O.; Seidlerová, J.; Wohlfahrt, P.; Filipovský, J.; Vaněk, J.; Cífková, R.; Windrichová, J.; Topolčan, O.; Knapen, M.H.; Drummen, N.E.; et al. Desphospho-uncarboxylated matrix Gla protein is associated with increased aortic stiffness in a general population. J. Hum. Hypertens. 2016, 30, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Vilovic, M.; Dogas, Z.; Ticinovic Kurir, T.; Borovac, J.A.; Supe-Domic, D.; Vilovic, T.; Ivkovic, N.; Rusic, D.; Novak, A.; Bozic, J. Bone metabolism parameters and inactive matrix Gla protein in patients with obstructive sleep apnea. Sleep 2020, 43, zsz243. [Google Scholar] [CrossRef]
- Dong, L.; Mintz, G.S.; Witzenbichler, B.; Metzger, D.C.; Rinaldi, M.J.; Duffy, P.L.; Weisz, G.; Stuckey, T.D.; Brodie, B.R.; Yun, K.H.; et al. Comparison of plaque characteristics in narrowings with ST-elevation myocardial infarction (STEMI), non-STEMI/unstable angina pectoris and stable coronary artery disease (from the ADAPT-DES IVUS Substudy). Am. J. Cardiol. 2015, 115, 860–866. [Google Scholar] [CrossRef]
- Lee, K.L.; Woodlief, L.H.; Topol, E.J.; Weaver, W.D.; Betriu, A.; Col, J.; Simoons, M.; Aylward, P.; Van de Werf, F.; Califf, R.M. Predictors of 30-day mortality in the era of reperfusion for acute myocardial infarction. Results from an international trial of 41,021 patients. GUSTO-I Investigators. Circulation 1995, 91, 1659–1668. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. ESC Scientific Document Group. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart. J. 2020, ehaa575. [Google Scholar] [CrossRef]
- Gale, C.P.; Manda, S.O.; Weston, C.F.; Birkhead, J.S.; Batin, P.D.; Hall, A.S. Evaluation of risk scores for risk stratification of acute coronary syndromes in the Myocardial Infarction National Audit Project (MINAP) database. Heart 2009, 95, 221–227. [Google Scholar] [CrossRef]
- Hong, Y.J.; Jeong, M.H.; Choi, Y.H.; Ma, E.H.; Ko, J.S.; Lee, M.G.; Park, K.H.; Sim, D.S.; Yoon, N.S.; Youn, H.J.; et al. Differences in intravascular ultrasound findings in culprit lesions in infarct-related arteries between ST segment elevation myocardial infarction and non-ST segment elevation myocardial infarction. J. Cardiol. 2010, 56, 15–22. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dalmeijer, G.W.; van der Schouw, Y.T.; Vermeer, C.; Magdeleyns, E.J.; Schurgers, L.J.; Beulens, J.W. Circulating matrix Gla protein is associated with coronary artery calcification and vitamin K status in healthy women. J. Nutr. Biochem. 2013, 24, 624–628. [Google Scholar] [CrossRef]
- Boxma, P.Y.; van den Berg, E.; Geleijnse, J.M.; Laverman, G.D.; Schurgers, L.J.; Vermeer, C.; Kema, I.P.; Muskiet, F.A.; Navis, G.; Bakker, S.J.; et al. Vitamin k intake and plasma desphospho-uncarboxylated matrix Gla-protein levels in kidney transplant recipients. PLoS ONE 2012, 7, e47991. [Google Scholar] [CrossRef]
- Bjørklund, G.; Svanberg, E.; Dadar, M.; Card, D.J.; Chirumbolo, S.; Harrington, D.J.; Aaseth, J. The Role of Matrix Gla Protein (MGP) in Vascular Calcification. Curr. Med. Chem. 2020, 27, 1647–1660. [Google Scholar] [CrossRef]
- Ueland, T.; Dahl, C.P.; Gullestad, L.; Aakhus, S.; Broch, K.; Skårdal, R.; Vermeer, C.; Aukrust, P.; Schurgers, L.J. Circulating levels of non-phosphorylated undercarboxylated matrix Gla protein are associated with disease severity in patients with chronic heart failure. Clin. Sci. 2011, 121, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Schurgers, L.J.; Cranenburg, E.C.; Vermeer, C. Matrix Gla-protein: The calcification inhibitor in need of vitamin K. Thromb. Haemost. 2008, 100, 593–603. [Google Scholar] [PubMed]
- Leopold, J.A. Vascular calcification: An age-old problem of old age. Circulation 2013, 127, 2380–2382. [Google Scholar] [CrossRef] [PubMed]
- Mayer, O., Jr.; Seidlerová, J.; Bruthans, J.; Filipovský, J.; Timoracká, K.; Vaněk, J.; Cerná, L.; Wohlfahrt, P.; Cífková, R.; Theuwissen, E.; et al. Desphospho-uncarboxylated matrix Gla-protein is associated with mortality risk in patients with chronic stable vascular disease. Atherosclerosis 2014, 235, 162–168. [Google Scholar] [CrossRef]
- Dalmeijer, G.W.; van der Schouw, Y.T.; Magdeleyns, E.J.; Vermeer, C.; Verschuren, W.M.; Boer, J.M.; Beulens, J.W. Matrix Gla protein species and risk of cardiovascular events in type 2 diabetic patients. Diabetes Care 2013, 36, 3766–3771. [Google Scholar] [CrossRef]
- van den Heuvel, E.G.; van Schoor, N.M.; Lips, P.; Magdeleyns, E.J.; Deeg, D.J.; Vermeer, C.; den Heijer, M. Circulating uncarboxylated matrix Gla protein, a marker of vitamin K status, as a risk factor of cardiovascular disease. Maturitas 2014, 77, 137–141. [Google Scholar] [CrossRef]
- Dalmeijer, G.W.; van der Schouw, Y.T.; Magdeleyns, E.J.; Vermeer, C.; Verschuren, W.M.; Boer, J.M.; Beulens, J.W. Circulating desphospho-uncarboxylated matrix γ-carboxyglutamate protein and the risk of coronary heart disease and stroke. J. Thromb. Haemost. 2014, 12, 1028–1034. [Google Scholar] [CrossRef]
- Liu, Y.P.; Gu, Y.M.; Thijs, L.; Knapen, M.H.; Salvi, E.; Citterio, L.; Petit, T.; Carpini, S.D.; Zhang, Z.; Jacobs, L.; et al. Inactive matrix Gla protein is causally related to adverse health outcomes: A Mendelian randomization study in a Flemish population. Hypertension 2015, 65, 463–470. [Google Scholar] [CrossRef]
- Wang, T.J. Assessing the role of circulating, genetic, and imaging biomarkers in cardiovascular risk prediction. Circulation 2011, 123, 551–565. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Iervasi, G. New insights for matrix Gla protein, vascular calcification and cardiovascular risk and outcome. Atherosclerosis 2014, 235, 236–238. [Google Scholar] [CrossRef]
- Fain, M.E.; Kapuku, G.K.; Paulson, W.D.; Williams, C.F.; Raed, A.; Dong, Y.; Knapen, M.H.J.; Vermeer, C.; Pollock, N.K. Inactive Matrix Gla Protein, Arterial Stiffness, and Endothelial Function in African American Hemodialysis Patients. Am. J. Hypertens. 2018, 31, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Schurgers, L.J.; Barreto, D.V.; Barreto, F.C.; Liabeuf, S.; Renard, C.; Magdeleyns, E.J.; Vermeer, C.; Choukroun, G.; Massy, Z.A. The circulating inactive form of matrix gla protein is a surrogate marker for vascular calcification in chronic kidney disease: A preliminary report. Clin. J. Am. Soc. Nephrol. 2010, 5, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.L.; McClelland, R.L.; Allison, M.A.; Cushman, M.; Garg, P.K.; Tsai, M.Y.; Rye, K.A.; Tabet, F. Lipoprotein (a) and coronary artery calcification: Prospective study assessing interactions with other risk factors. Metabolism 2021, 116, 154706. [Google Scholar] [CrossRef] [PubMed]
- Antonopoulos, S.; Mylonopoulou, M.; Angelidi, A.M.; Kousoulis, A.A.; Tentolouris, N. Association of matrix γ-carboxyglutamic acid protein levels with insulin resistance and Lp(a) in diabetes: A cross-sectional study. Diabetes Res. Clin. Pract. 2017, 130, 252–257. [Google Scholar] [CrossRef]
- Tintut, Y.; Hsu, J.J.; Demer, L.L. Lipoproteins in Cardiovascular Calcification: Potential Targets and Challenges. Front. Cardiovasc. Med. 2018, 5, 172. [Google Scholar] [CrossRef]
- Cesaro, A.; Schiavo, A.; Moscarella, E.; Coletta, S.; Conte, M.; Gragnano, F.; Fimiani, F.; Monda, E.; Caiazza, M.; Limongelli, G.; et al. Lipoprotein(a): A genetic marker for cardiovascular disease and target for emerging therapies. J. Cardiovasc. Med. 2021, 22, 151–161. [Google Scholar] [CrossRef]
- Schlieper, G.; Westenfeld, R.; Krüger, T.; Cranenburg, E.C.; Magdeleyns, E.J.; Brandenburg, V.M.; Djuric, Z.; Damjanovic, T.; Ketteler, M.; Vermeer, C.; et al. Circulating nonphosphorylated carboxylated matrix gla protein predicts survival in ESRD. J. Am. Soc. Nephrol. 2011, 22, 387–395. [Google Scholar] [CrossRef]
- Wernio, E.; Magorzewicz, S.; Jagielak, D. Comparison of calcification inhibitor-matrix gla protein level in elderly patients with severe aortic stenosis and healthy volunteers. Clin. Nutr. ESPEN 2020, 40, 538–539. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (n = 90) | STEMI (n = 46) | NSTEMI (n = 44) | p-Value |
|---|---|---|---|---|
| Age, years | 67.2 ± 9.1 | 66.2 ± 8.8 | 68.2 ± 9.4 | 0.308 1 |
| Male sex | 71 (78.9%) | 35 (76.1%) | 36 (81.8%) | 0.505 1 |
| Body mass index, kg/m2 | 27.08 ± 2.54 | 27.45 ± 2.71 | 26.70 ± 2.31 | 0.158 3 |
| Waist-to-hip ratio | 1.04 ± 0.68 | 1.04 ± 0.68 | 1.04 ± 0.69 | 0.630 3 |
| Systolic blood pressure, mmHg | 134.7 ± 21.0 | 134.3 ± 21.3 | 135.1 ± 20.9 | 0.845 3 |
| Diastolic blood pressure, mmHg | 79.7 ± 12.6 | 81.2 ± 12.3 | 78.1 ± 12.9 | 0.252 3 |
| Heart rate at admission, bpm | 75.0 ± 16.9 | 76.7 ± 18.6 | 73.3 ± 14.9 | 0.353 3 |
| Diabetes mellitus | 13 (14.4%) | 4 (8.7%) | 9 (20.5%) | 0.140 2 |
| Arterial hypertension | 51 (56.7%) | 27 (58.7%) | 24 (54.5%) | 0.832 1 |
| Smoking | 43 (47.8%) | 24 (52.2%) | 19 (43.2%) | 0.393 1 |
| Dyslipidemia | 14 (15.6%) | 6 (13.0%) | 8 (18.2%) | 0.501 1 |
| Atrial fibrillation | 12 (13.3%) | 8 (17.4%) | 4 (9.1%) | 0.355 2 |
| Family history of cardiovascular disease | 17 (18.9%) | 10 (21.7%) | 7 (15.9%) | 0.480 1 |
| History of PCI or CABG | 16 (17.8%) | 4 (8.7%) | 12 (27.3%) | 0.028 2 |
| History of CV-related hospitalizations | 24 (26.7%) | 5 (10.9%) | 19 (43.2%) | 0.001 2 |
| GRACE score, points | 121.4 ± 22.0 | 121.1 ± 23.1 | 121.7 ± 23.1 | 0.906 3 |
| Left ventricular ejection fraction, % | 50.7 ± 10.3 | 51.2 ± 9.7 | 50.1 ± 11.1 | 0.652 3 |
| Mean Killip class * | 1.0 (1.0-1.0) | 1.0 (1.0-1.0) | 1.1 (1.0-1.0) | 0.136 4 |
| ST segment deviation in first contact ECG | 82 (91.1%) | 46 (100%) | 36 (81.8%) | 0.002 1 |
| PCI performed while in-hospital | 74 (82.2%) | 44 (95.7%) | 30 (68.2%) | 0.001 1 |
| Multi-vessel disease | 10 (13.3%) | 2 (4.4%) | 8 (26.7%) | 0.012 2 |
| Beta-blocker use | 29 (32.2%) | 12 (26.1%) | 17 (38.6%) | 0.203 1 |
| ACE inhibitor or ARB use | 41 (45.6%) | 21 (45.7%) | 20 (45.5%) | 0.985 1 |
| Calcium channel blocker use | 14 (15.6%) | 8 (17.4%) | 6 (13.6%) | 0.623 1 |
| Statin use | 18 (20.0%) | 6 (13.0%) | 12 (27.3%) | 0.092 1 |
| Diuretic use | 20 (22.2%) | 8 (17.4%) | 12 (27.3%) | 0.260 1 |
| Acetylsalicylic acid use | 23 (25.6%) | 7 (15.2%) | 16 (36.4%) | 0.021 1 |
| P2Y12 inhibitor use | 4 (4.4%) | 1 (2.2%) | 3 (6.8%) | 0.355 2 |
| Anticoagulant use | 7 (7.8%) | 4 (8.7%) | 3 (6.8%) | 1.000 2 |
| Prothrombin time—INR | 1.09 ± 0.39 | 1.07 ± 0.25 | 1.11 ± 0.50 | 0.608 3 |
| Activated partial thromboplastin time, s | 24.13 ± 4.02 | 23.96 ± 4.21 | 24.32 ± 3.85 | 0.672 3 |
| C-reactive protein, mg/L | 6.4 ± 5.0 | 6.6 ± 5.2 | 6.2 ± 4.9 | 0.664 3 |
| High-sensitivity cardiac troponin I at admission, ng/L | 331.0 ± 293.8 | 335.2 ± 306.1 | 326.9 ± 284.8 | 0.894 3 |
| Potassium, mmol/L | 4.04 ± 0.40 | 3.98 ± 0.39 | 4.10 ± 0.41 | 0.176 3 |
| Urea, mmol/L | 7.6 ± 3.2 | 7.0 ± 2.2 | 8.2 ± 4.0 | 0.094 3 |
| Creatinine, μmol/L | 0.428 | 88.0 ± 21.6 | 102.9 ± 44.3 | 0.045 3 |
| Variable | r-Correlation Coefficient | p-Value 1 |
|---|---|---|
| Age, years | 0.259 | 0.014 |
| GRACE score, points | 0.247 | 0.019 |
| Prothrombin time—INR | 0.257 | 0.015 |
| Activated partial thromboplastin time, s | 0.251 | 0.017 |
| Second high-sensitivity cardiac troponin I, ng/L | 0.236 | 0.026 |
| Urea, mmol/L | 0.369 | <0.001 |
| Creatinine, μmol/L | 0.428 | <0.001 |
| Variable | Univariate Model | Multivariate Model | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value 1 | |
| Age | 1.06 | 1.01–1.12 | 0.034 | 1.04 | 0.98–1.11 | 0.220 |
| Sex | 1.62 | 0.57–4.59 | 0.364 | - | - | - |
| BMI | 1.09 | 0.91 –1.29 | 0.346 | - | - | - |
| Diabetes mellitus | 4.00 | 1.18–13.57 | 0.026 | 2.12 | 0.46–7.80 | 0.336 |
| Arterial hypertension | 1.87 | 0.75–4.66 | 0.178 | - | - | - |
| Dyslipidemia | 2.30 | 0.73–7.32 | 0.157 | - | - | - |
| Acute kidney injury | 4.75 | 1.10–20.57 | 0.037 | 2.60 | 0.45–10.16 | 0.289 |
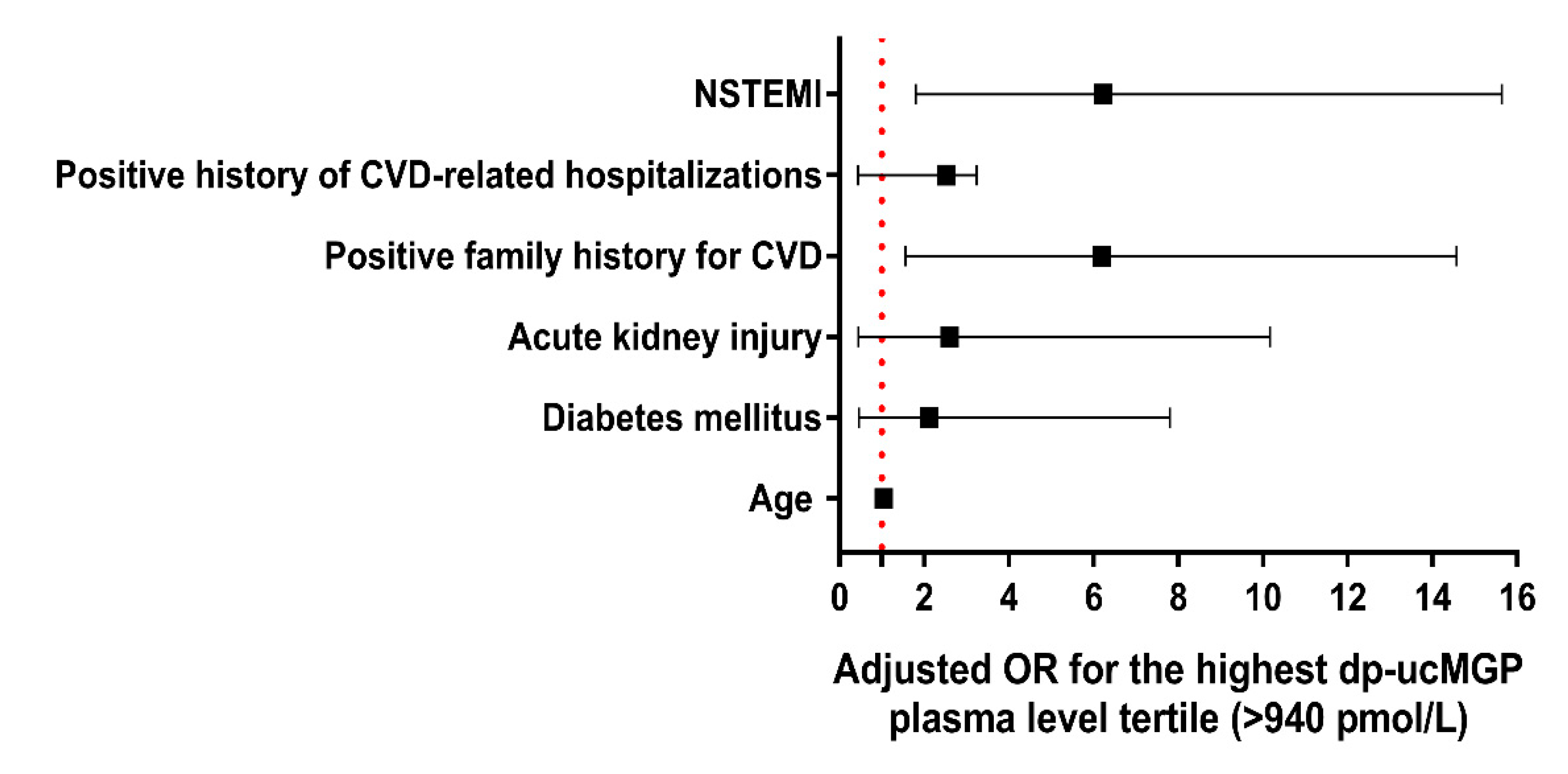
| Positive family history for CVD | 3.79 | 1.27–11.31 | 0.017 | 6.19 | 1.56–14.57 | 0.0101 |
| Positive history of CVD-related hospitalizations | 3.27 | 1.17–9.16 | 0.024 | 2.53 | 0.44–3.24 | 0.849 |
| NSTEMI | 4.75 | 1.81–12.46 | 0.002 | 6.23 | 1.80–15.64 | 0.004 1 |
| Multivessel disease | 3.06 | 0.78–11.96 | 0.107 | - | - | - |
| LVEF | 0.98 | 0.94–1.04 | 0.631 | - | - | - |
| High GRACE score (>140 points) | 1.36 | 0.47–3.95 | 0.577 | - | - | - |
| Variable | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| dp-ucMGP, pmol/L | 1.004 | 1.001–1.006 | 0.011 1 |
| Age, years | 1.018 | 0.948–1.092 | 0.629 |
| Sex | 0.626 | 0.147–2.654 | 0.525 |
| Body mass index, kg/m2 | 0.856 | 0.692–1.059 | 0.153 |
| Creatinine, μmol/L | 0.999 | 0.974–1.024 | 0.917 |
| C-reactive protein, mg/L | 0.996 | 0.980–1.011 | 0.580 |
| Left-ventricular ejection fraction, % | 0.993 | 0.938–1.050 | 0.795 |
| Systolic blood pressure, mmHg | 1.007 | 0.980–1.036 | 0.600 |
| Smoking | 0.987 | 0.294–3.315 | 0.983 |
| Diabetes mellitus type II | 0.970 | 0.161–5.852 | 0.973 |
| Arterial hypertension | 0.557 | 0.182–1.704 | 0.305 |
| Dyslipidemia | 2.439 | 0.486–12.227 | 0.278 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bilalic, A.; Ticinovic Kurir, T.; Kumric, M.; Borovac, J.A.; Matetic, A.; Supe-Domic, D.; Bozic, J. Circulating Levels of Dephosphorylated-Uncarboxylated Matrix Gla Protein in Patients with Acute Coronary Syndrome. Molecules 2021, 26, 1108. https://doi.org/10.3390/molecules26041108
Bilalic A, Ticinovic Kurir T, Kumric M, Borovac JA, Matetic A, Supe-Domic D, Bozic J. Circulating Levels of Dephosphorylated-Uncarboxylated Matrix Gla Protein in Patients with Acute Coronary Syndrome. Molecules. 2021; 26(4):1108. https://doi.org/10.3390/molecules26041108
Chicago/Turabian StyleBilalic, Admira, Tina Ticinovic Kurir, Marko Kumric, Josip A. Borovac, Andrija Matetic, Daniela Supe-Domic, and Josko Bozic. 2021. "Circulating Levels of Dephosphorylated-Uncarboxylated Matrix Gla Protein in Patients with Acute Coronary Syndrome" Molecules 26, no. 4: 1108. https://doi.org/10.3390/molecules26041108
APA StyleBilalic, A., Ticinovic Kurir, T., Kumric, M., Borovac, J. A., Matetic, A., Supe-Domic, D., & Bozic, J. (2021). Circulating Levels of Dephosphorylated-Uncarboxylated Matrix Gla Protein in Patients with Acute Coronary Syndrome. Molecules, 26(4), 1108. https://doi.org/10.3390/molecules26041108