
Application of Propolis in Protecting Skeletal and Periodontal Health—A Systematic Review



Abstract
1. Introduction
2. Results
2.1. Selection of Articles
2.2. Study Characteristics
3. Discussion
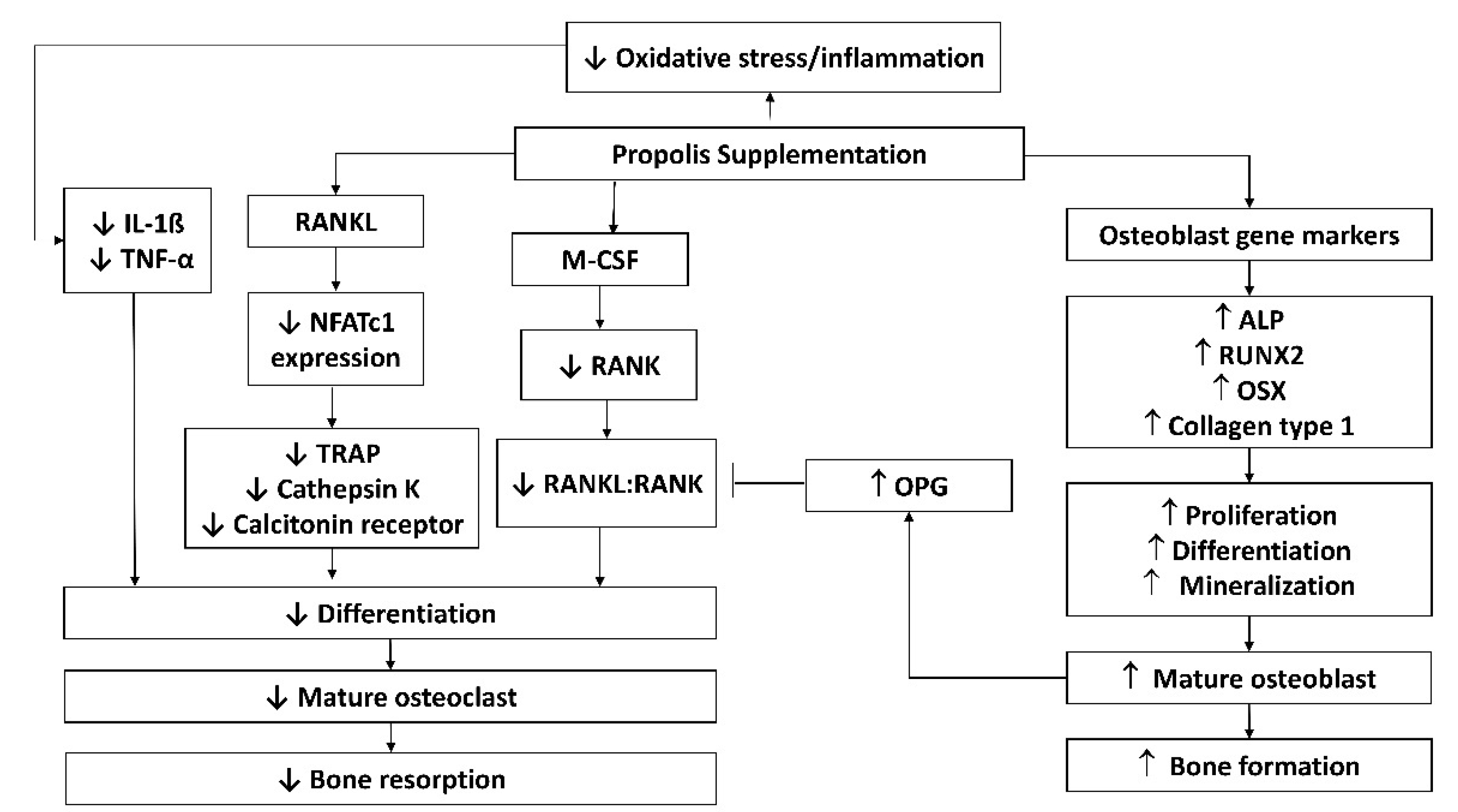
3.1. Possible Molecular Mechanisms of Propolis in Preserving Skeletal Health
3.2. Bioavailability and Safety Concerns of Propolis
4. Materials and Methods
4.1. Literature Review
4.2. Selection of Research Articles
4.3. Data Extraction
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clarke, B. Normal bone anatomy and physiology. Clin. J. Am. Soc. Nephrol. 2008, 3 (Suppl. 3), S131–S139. [Google Scholar] [CrossRef] [PubMed]
- Seeman, E.; Delmas, P.D. Bone quality—The material and structural basis of bone strength and fragility. N. Engl. J. Med. 2006, 354, 2250–2261. [Google Scholar] [CrossRef]
- Manolagas, S.C. Birth and death of bone cells: Basic regulatory mechanisms and implications for the pathogenesis and treatment of osteoporosis. Endocr. Rev. 2000, 21, 115–137. [Google Scholar] [CrossRef]
- Baron, R.; Hesse, E. Update on Bone Anabolics in Osteoporosis Treatment: Rationale, Current Status, and Perspectives. J. Clin. Endocrinol. Metab. 2012, 97, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Lean, J.M.; Jagger, C.J.; Kirstein, B.; Fuller, K.; Chambers, T.J. Hydrogen peroxide is essential for estrogen-deficiency bone loss and osteoclast formation. Endocrinology 2005, 146, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Manolagas, S.C. From Estrogen-Centric to Aging and Oxidative Stress: A Revised Perspective of the Pathogenesis of Osteoporosis. Endocr. Rev. 2010, 31, 266–300. [Google Scholar] [CrossRef]
- Banfi, G.; Iorio, E.L.; Corsi, M.M. Oxidative stress, free radicals and bone remodeling. Clin. Chem. Lab. Med. 2008, 46, 1550–1555. [Google Scholar] [CrossRef] [PubMed]
- Baek, K.H.; Oh, K.W.; Lee, W.Y.; Lee, S.S.; Kim, M.K.; Kwon, H.S.; Rhee, E.J.; Han, J.H.; Song, K.H.; Cha, B.Y.; et al. Association of oxidative stress with postmenopausal osteoporosis and the effects of hydrogen peroxide on osteoclast formation in human bone marrow cell cultures. Calcif. Tissue Int. 2010, 87, 226–235. [Google Scholar] [CrossRef]
- Mann, V.; Huber, C.; Kogianni, G.; Collins, F.; Noble, B. The antioxidant effect of estrogen and Selective Estrogen Receptor Modulators in the inhibition of osteocyte apoptosis in vitro. Bone 2007, 40, 674–684. [Google Scholar] [CrossRef] [PubMed]
- Fontani, F.; Marcucci, G.; Iantomasi, T.; Brandi, M.L.; Vincenzini, M.T. Glutathione, N-acetylcysteine and lipoic acid down-regulate starvation-induced apoptosis, RANKL/OPG ratio and sclerostin in osteocytes: Involvement of JNK and ERK1/2 signalling. Calcif. Tissue Int. 2015, 96, 335–346. [Google Scholar] [CrossRef]
- Marathe, N.; Rangaswami, H.; Zhuang, S.; Boss, G.R.; Pilz, R.B. Pro-survival effects of 17β-estradiol on osteocytes are mediated by nitric oxide/cGMP via differential actions of cGMP-dependent protein kinases I and II. J. Biol. Chem. 2012, 287, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, L.I.; Aguirre, J.I.; Kousteni, S.; Manolagas, S.C.; Bellido, T. Bisphosphonates and estrogens inhibit osteocyte apoptosis via distinct molecular mechanisms downstream of extracellular signal-regulated kinase activation. J. Biol. Chem. 2005, 280, 7317–7325. [Google Scholar] [CrossRef]
- Jun, J.H.; Lee, S.-H.; Kwak, H.B.; Lee, Z.H.; Seo, S.-B.; Woo, K.M.; Ryoo, H.-M.; Kim, G.-S.; Baek, J.-H. N-acetylcysteine stimulates osteoblastic differentiation of mouse calvarial cells. J. Cell. Biochem. 2008, 103, 1246–1255. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, C.; Marcucci, G.; Favilli, F.; Zonefrati, R.; Mavilia, C.; Galli, G.; Tanini, A.; Iantomasi, T.; Brandi, M.L.; Vincenzini, M.T. Role of GSH/GSSG redox couple in osteogenic activity and osteoclastogenic markers of human osteoblast-like SaOS-2 cells. FEBS J. 2013, 280, 867–879. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.Y.; Ima-Nirwana, S. Vitamin C and Bone Health: Evidence from Cell, Animal and Human Studies. Curr. Drug Targets 2018, 19, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.Y.; Ima-Nirwana, S. Olives and bone: A green osteoporosis prevention option. Int. J. Environ. Res. Public Health 2016, 13, 755. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.; Mohamad, N.-V.; Ibrahim, N.; Chin, K.-Y.; Shuid, A.; Ima-Nirwana, S. The Molecular Mechanism of Vitamin E as a Bone-Protecting Agent: A Review on Current Evidence. Int. J. Mol. Sci. 2019, 20, 1453. [Google Scholar] [CrossRef] [PubMed]
- Ekeuku, S.O.; Pang, K.L.; Chin, K.Y. Effects of Caffeic Acid and Its Derivatives on Bone: A Systematic Review. Drug Des. Devel. Ther. 2021, 15, 259–275. [Google Scholar] [CrossRef]
- Biswas, S.K. Does the Interdependence between Oxidative Stress and Inflammation Explain the Antioxidant Paradox? Oxid. Med. Cell. Longev. 2016, 2016, 5698931. [Google Scholar] [CrossRef]
- Lugrin, J.; Rosenblatt-Velin, N.; Parapanov, R.; Liaudet, L. The role of oxidative stress during inflammatory processes. Biol. Chem. 2014, 395, 203–230. [Google Scholar] [CrossRef]
- Mundy, G.R. Osteoporosis and inflammation. Nutr. Rev. 2007, 65, S147–S151. [Google Scholar] [CrossRef] [PubMed]
- Romas, E.; Gillespie, M.T. Inflammation-induced bone loss: Can it be prevented? Rheum. Dis. Clin. N. Am. 2006, 32, 759–773. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Han, C.; van der Heijde, D.M.F.M.; Emery, P.; Bathon, J.M.; Keystone, E.; Maini, R.N.; Kalden, J.R.; Aletaha, D.; Baker, D.; et al. Radiographic changes in rheumatoid arthritis patients attaining different disease activity states with methotrexate monotherapy and infliximab plus methotrexate: The impacts of remission and tumour necrosis factor blockade. Ann. Rheum. Dis. 2009, 68, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Bankova, V.S.; Castro, S.L.D.; Marcucci, M.C. Propolis: Recent advances in chemistry and plant origin. Apidologie 2000, 31, 3–15. [Google Scholar] [CrossRef]
- Burdock, G.A. Review of the biological properties and toxicity of bee propolis (propolis). Food Chem. Toxicol. 1998, 36, 347–363. [Google Scholar] [CrossRef]
- de Castro, P.A.; Savoldi, M.; Bonatto, D.; Barros, M.H.; Goldman, M.H.S.; Berretta, A.A.; Goldman, G.H. Molecular scharacterisation of propolis-induced cell death in Saccharomyces cerevisiae. Eukaryot. Cell 2011, 10, 398–411. [Google Scholar] [CrossRef]
- Khalil, M.L. Biological activity of bee propolis in health and disease. Asian Pac. J. Cancer Prev. 2006, 7, 22–31. [Google Scholar] [PubMed]
- Pahlavani, N.; Sedaghat, A.; Bagheri Moghaddam, A.; Mazloumi Kiapey, S.S.; Gholizadeh Navashenaq, J.; Jarahi, L.; Reazvani, R.; Norouzy, A.; Nematy, M.; Safarian, M.; et al. Effects of propolis and melatonin on oxidative stress, inflammation, and clinical status in patients with primary sepsis: Study protocol and review on previous studies. Clin. Nutr. ESPEN 2019, 33, 125–131. [Google Scholar] [CrossRef]
- Kolankaya, D.; Selmanoǧlu, G.; Sorkun, K.; Salih, B. Protective effects of Turkish propolis on alcohol-induced serum lipid changes and liver injury in male rats. Food Chem. 2002, 78, 213–217. [Google Scholar] [CrossRef]
- Tan-no, K.; Nakajima, T.; Shoji, T.; Nakagawasai, O.; Niijima, F.; Ishikawa, M.; Endo, Y.; Sato, T.; Satoh, S.; Tadano, T. Anti-inflammatory Effect of Propolis through Inhibition of Nitric Oxide Production on Carrageenin-Induced Mouse Paw Edema. Biol. Pharm. Bull. 2006, 29, 96–99. [Google Scholar] [CrossRef][Green Version]
- Krol, W.; Scheller, S.; Czuba, Z.; Matsuno, T.; Zydowicz, G.; Shani, J.; Mos, M. Inhibition of neutrophils’ chemiluminescence by ethanol extract of propolis (EEP) and its phenolic components. J. Ethnopharmacol. 1996, 55, 19–25. [Google Scholar] [CrossRef]
- Marcucci, M.C. Propolis: Chemical composition, biological properties and therapeutic activity. Apidologie 1995, 26, 83–99. [Google Scholar] [CrossRef]
- Aliyazicioglu, Y.; Demir, S.; Turan, I.; Cakiroglu, T.N.; Akalin, I.; Deger, O.; Bedir, A. Preventive and Protective Effects of Turkish Propolis on H2O2-induced DNA Damage in Foreskin Fibroblast Cell Lines. Acta Biol. Hung. 2011, 62, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Silva, V.; Genta, G.; Möller, M.N.; Masner, M.; Thomson, L.; Romero, N.; Radi, R.; Fernandes, D.C.; Laurindo, F.R.M.; Heinzen, H.; et al. Antioxidant Activity of Uruguayan Propolis. In Vitro and Cellular Assays. J. Agric. Food Chem. 2011, 59, 6430–6437. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.-Q.; Wen, Y.-F.; Bhadauria, M.; Nirala, S.K.; Sharma, A.; Shrivastava, S.; Shukla, S.; Agrawal, O.P.; Mathur, R. Protective effects of propolis on inorganic mercury induced oxidative stress in mice. Indian J. Exp. Biol. 2009, 47, 264–269. [Google Scholar] [PubMed]
- Jasprica, I.; Mornar, A.; Debeljak, Ž.; Smolčić-Bubalo, A.; Medić-Šarić, M.; Mayer, L.; Romić, Ž.; Bućan, K.; Balog, T.; Sobočanec, S.; et al. In vivo study of propolis supplementation effects on antioxidative status and red blood cells. J. Ethnopharmacol. 2007, 110, 548–554. [Google Scholar] [CrossRef]
- Kart, A.; Cigremis, Y.; Ozen, H.; Dogan, O. Caffeic acid phenethyl ester prevents ovary ischemia/reperfusion injury in rabbits. Food Chem. Toxicol. 2009, 47, 1980–1984. [Google Scholar] [CrossRef]
- Tekin, I.O.; Sipahi, E.Y.; Comert, M.; Acikgoz, S.; Yurdakan, G. Low-Density Lipoproteins Oxidized After Intestinal Ischemia/Reperfusion in Rats. J. Surg. Res. 2009, 157, e47–e54. [Google Scholar] [CrossRef]
- Pileggi, R.; Antony, K.; Johnson, K.; Zuo, J.; Shannon Holliday, L. Propolis inhibits osteoclast maturation. Dent. Traumatol. 2009, 25, 584–588. [Google Scholar] [CrossRef]
- Wimolsantirungsri, N.; Makeudom, A.; Louwakul, P.; Sastraruji, T.; Chailertvanitkul, P.; Supanchart, C.; Krisanaprakornkit, S. Inhibitory effect of Thai propolis on human osteoclastogenesis. Dent. Traumatol. 2018, 34, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Somsanith, N.; Kim, Y.-K.; Jang, Y.-S.; Lee, Y.-H.; Yi, H.-K.; Jang, J.-H.; Kim, K.-A.; Bae, T.-S.; Lee, M.-H. Enhancing of Osseointegration with Propolis-Loaded TiO2 Nanotubes in Rat Mandible for Dental Implants. Materials 2018, 11, 61. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.K.; Yoo, S.Y.; Jang, Y.Y.; Lee, B.C.; Lee, D.S.; Kook, J.-K. Anti-inflammatory and in vitro bone formation effects of Garcinia mangostana L. and propolis extracts. Food Sci. Biotechnol. 2020, 29, 539–548. [Google Scholar] [CrossRef]
- Al-Hariri, M. Glycemic control and anti-osteopathic effect of propolis in diabetic rats. Diabetes Metab. Syndr. Obes. 2011, 4, 377. [Google Scholar] [CrossRef] [PubMed]
- Meimandi-Parizi, A.; Oryan, A.; Sayahi, E.; Bigham-Sadegh, A. Propolis extract a new reinforcement material in improving bone healing: An in vivo study. Int. J. Surg. 2018, 56, 94–101. [Google Scholar] [CrossRef]
- Guney, A.; Karaman, I.; Oner, M.; Yerer, M.B. Effects of Propolis on Fracture Healing: An Experimental Study. Phytother. Res. 2011, 25, 1648–1652. [Google Scholar] [CrossRef] [PubMed]
- Bereket, C.; Özan, F.; Şener, İ.; Tek, M.; Altunkaynak, B.Z.; Semirgin, S.U.; Şenel, E.; Özdemir, M. Propolis accelerates the consolidation phase in distraction osteogenesis. J. Craniofac. Surg. 2014, 25, 1912–1916. [Google Scholar] [CrossRef]
- Nakajima, M.; Arimatsu, K.; Minagawa, T.; Matsuda, Y.; Sato, K.; Takahashi, N.; Nakajima, T.; Yamazaki, K. Brazilian propolis mitigates impaired glucose and lipid metabolism in experimental periodontitis in mice. BMC Complement. Altern. Med. 2016, 16, 329. [Google Scholar] [CrossRef]
- Toker, H.; Ozan, F.; Ozer, H.; Ozdemir, H.; Eren, K.; Yeler, H. A Morphometric and Histopathologic Evaluation of the Effects of Propolis on Alveolar Bone Loss in Experimental Periodontitis in Rats. J. Periodontol. 2008, 79, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Yuanita, T.; Zubaidah, N.; Kunarti, S. Expression of Osteoprotegrin and Osteoclast Level in Chronic Apical Periodontitis Induced with East Java Propolis Extract. Iran. Endod. J. 2018, 13, 42–46. [Google Scholar] [CrossRef]
- Kresnoadi, U.; Lunardhi, L.C.; Agustono, B. Propolis extract and bovine bone graft combination in the expression of VEGF and FGF2 on the preservation of post extraction socket. J. Indian Prosthodont. Soc. 2020, 20, 417–423. [Google Scholar] [CrossRef]
- Kresnoadi, U.; Rahayu, R.P.; Ariani, M.D.; Soesanto, S. The Potential of Natural Propolis Extract Combined with Bovine Bone Graft in Increasing Heat Shock Protein 70 and Osteocalcin on Socket Preservation. Eur. J. Dent. 2020, 14, 31–37. [Google Scholar] [CrossRef]
- Wiwekowati, W.; Ma’ruf, M.T.; Walianto, S.; Sabir, A.; Widyadharma, I.P.E. Indonesian Propolis Reduces Malondialdehyde Level and Increase Osteoblast Cell Number in Wistar Rats with Orthodontic Tooth Movement. Open Access Maced. J. Med. Sci. 2020, 8, 100–104. [Google Scholar] [CrossRef]
- Gulinelli, J.L.; Panzarini, S.R.; Fattah, C.M.R.D.S.; Poi, W.R.; Sonoda, C.K.; Negri, M.R.; Saito, C.T.M.H. Effect of root surface treatment with propolis and fluoride in delayed tooth replantation in rats. Dent. Traumatol. 2008, 24, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Altan, B.A.; Kara, I.M.; Nalcaci, R.; Ozan, F.; Erdogan, S.M.; Ozkut, M.M.; Inan, S. Systemic propolis stimulates new bone formation at the expanded suture. Angle Orthod. 2013, 83, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Zohery, A.A.; Meshri, S.M.; Madi, M.I.; Abd El Rehim, S.S.; Nour, Z.M. Egyptian propolis compared to nanohydroxyapatite graft in the treatment of Class II furcation defects in dogs. J. Periodontol. 2018, 89, 1340–1350. [Google Scholar] [CrossRef] [PubMed]
- Aral, C.A.; Kesim, S.; Greenwell, H.; Kara, M.; Çetin, A.; Yakan, B. Alveolar bone protective and hypoglycemic effects of systemic propolis treatment in experimental periodontitis and diabetes mellitus. J. Med. Food 2015, 18, 195–201. [Google Scholar] [CrossRef]
- Liu, L.; Webster, T.J. In Situ Sensor Advancements for Osteoporosis Prevention, Diagnosis, and Treatment. Curr. Osteoporos. Rep. 2016, 14, 386–395. [Google Scholar] [CrossRef]
- Russow, G.; Jahn, D.; Appelt, J.; Märdian, S.; Tsitsilonis, S.; Keller, J. Anabolic Therapies in Osteoporosis and Bone Regeneration. Int. J. Mol. Sci. 2019, 20, 83. [Google Scholar] [CrossRef]
- Valderrábano, R.J.; Linares, M.I. Diabetes mellitus and bone health: Epidemiology, etiology and implications for fracture risk stratification. Clin. Diabetes Endocrinol. 2018, 4, 1–8. [Google Scholar] [CrossRef]
- Lenzen, S. The mechanisms of alloxan- and streptozotocin-induced diabetes. Diabetologia 2008, 51, 216–226. [Google Scholar] [CrossRef]
- Duque, G.; Demontiero, O.; Troen, B.R. Prevention and treatment of senile osteoporosis and hip fractures. Minerva Med. 2009, 100, 79–94. [Google Scholar]
- Ekegren, C.; Edwards, E.; de Steiger, R.; Gabbe, B. Incidence, Costs and Predictors of Non-Union, Delayed Union and Mal-Union Following Long Bone Fracture. Int. J. Environ. Res. Public Health 2018, 15, 2845. [Google Scholar] [CrossRef]
- Bodic, F.; Hamel, L.; Lerouxel, E.; Baslé, M.F.; Chappard, D. Bone loss and teeth. Jt. Bone Spine 2005, 72, 215–221. [Google Scholar] [CrossRef]
- Hienz, S.A.; Paliwal, S.; Ivanovski, S. Mechanisms of Bone Resorption in Periodontitis. J. Immunol. Res. 2015, 2015, 615486. [Google Scholar] [CrossRef] [PubMed]
- Periodontology, A.A.O. Glossary of Periodontal Terms. Available online: https://members.perio.org/libraries/glossary?ssopc=1 (accessed on 26 April 2021).
- Li, Y.; Jacox, L.A.; Little, S.H.; Ko, C.-C. Orthodontic tooth movement: The biology and clinical implications. Kaohsiung J. Med. Sci. 2018, 34, 207–214. [Google Scholar] [CrossRef]
- Baysal, A.; Karadede, I.; Hekimoglu, S.; Ucar, F.; Ozer, T.; Veli, İ.; Uysal, T. Evaluation of root resorption following rapid maxillary expansion using cone-beam computed tomography. Angle Orthod. 2011, 82, 488–494. [Google Scholar] [CrossRef]
- Ettl, T.; Gerlach, T.; Schüsselbauer, T.; Gosau, M.; Reichert, T.E.; Driemel, O. Bone resorption and complications in alveolar distraction osteogenesis. Clin. Oral Investig. 2010, 14, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Engquist, B.; Astrand, P.; Anzén, B.; Dahlgren, S.; Engquist, E.; Feldmann, H.; Karlsson, U.; Nord, P.-G.; Sahlholm, S.; Svärdström, P. Simplified methods of implant treatment in the edentulous lower jaw: A 3-year follow-up report of a controlled prospective study of one-stage versus two-stage surgery and early loading. Clin. Implant Dent. Relat. Res. 2005, 7, 95–104. [Google Scholar] [CrossRef]
- Möhlhenrich, S.C.; Modabber, A.; Steiner, T.; Mitchell, D.A.; Hölzle, F. Heat generation and drill wear during dental implant site preparation: Systematic review. Br. J. Oral Maxillofac. Surg. 2015, 53, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Franco, R.; Schoneveld, O.J.; Pappa, A.; Panayiotidis, M.I. The central role of glutathione in the pathophysiology of human diseases. Arch. Physiol. Biochem. 2007, 113, 234–258. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.-S.; Park, D.-H.; Shin, E.-J.; Kwon, M.S.; Ko, K.H.; Kim, W.-K.; Jhoo, J.H.; Jhoo, W.-K.; Wie, M.-B.; Jung, B.D.; et al. Antioxidant propolis attenuates kainate-induced neurotoxicity via adenosine A1 receptor modulation in the rat. Neurosci. Lett. 2004, 355, 231–235. [Google Scholar] [CrossRef]
- Osés, S.M.; Pascual-Maté, A.; Fernández-Muiño, M.A.; López-Díaz, T.M.; Sancho, M.T. Bioactive properties of honey with propolis. Food Chem. 2016, 196, 1215–1223. [Google Scholar] [CrossRef]
- Cao, G.; Ying, P.; Yan, B.; Xue, W.; Li, K.; Shi, A.; Sun, T.; Yan, J.; Hu, X. Pharmacokinetics, safety, and tolerability of single and multiple-doses of pinocembrin injection administered intravenously in healthy subjects. J. Ethnopharmacol. 2015, 168, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Weaver, C.M.; Barnes, S.; Wyss, J.M.; Kim, H.; Morré, D.M.; Morré, D.J.; Simon, J.E.; Lila, M.A.; Janle, E.M.; Ferruzzi, M.G. Botanicals for age-related diseases: From field to practice. Am. J. Clin. Nutr. 2008, 87, 493S–497S. [Google Scholar] [CrossRef]
- Moreno, M.I.; Isla, M.I.; Sampietro, A.R.; Vattuone, M.A. Comparison of the free radical-scavenging activity of propolis from several regions of Argentina. J. Ethnopharmacol. 2000, 71, 109–114. [Google Scholar] [CrossRef]
- Russo, A.; Longo, R.; Vanella, A. Antioxidant activity of propolis: Role of caffeic acid phenethyl ester and galangin. Fitoterapia 2002, 73 (Suppl. 1), S21–S29. [Google Scholar] [CrossRef]
- Hamasaka, T.; Kumazawa, S.; Fujimoto, T.; Nakayama, T. Antioxidant Activity and Constituents of Propolis Collected in Various Areas of Japan. Food Sci. Technol. Res. 2004, 10, 86–92. [Google Scholar] [CrossRef]
- Dougall, W.C.; Glaccum, M.; Charrier, K.; Rohrbach, K.; Brasel, K.; De Smedt, T.; Daro, E.; Smith, J.; Tometsko, M.E.; Maliszewski, C.R.; et al. RANK is essential for osteoclast and lymph node development. Genes Dev. 1999, 13, 2412–2424. [Google Scholar] [CrossRef]
- Kong, Y.Y.; Yoshida, H.; Sarosi, I.; Tan, H.L.; Timms, E.; Capparelli, C.; Morony, S.; Oliveira-dos-Santos, A.J.; Van, G.; Itie, A.; et al. OPGL is a key regulator of osteoclastogenesis, lymphocyte development and lymph-node organogenesis. Nature 1999, 397, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Wiktor-Jedrzejczak, W.; Bartocci, A.; Ferrante, A.W., Jr.; Ahmed-Ansari, A.; Sell, K.W.; Pollard, J.W.; Stanley, E.R. Total absence of colony-stimulating factor 1 in the macrophage-deficient osteopetrotic (op/op) mouse. Proc. Natl. Acad. Sci. USA 1990, 87, 4828–4832. [Google Scholar] [CrossRef]
- Yoshida, H.; Hayashi, S.; Kunisada, T.; Ogawa, M.; Nishikawa, S.; Okamura, H.; Sudo, T.; Shultz, L.D.; Nishikawa, S. The murine mutation osteopetrosis is in the coding region of the macrophage colony stimulating factor gene. Nature 1990, 345, 442–444. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Sato, K.; Asagiri, M.; Morita, I.; Soma, K.; Takayanagi, H. Contribution of nuclear factor of activated T cells c1 to the transcriptional control of immunoreceptor osteoclast-associated receptor but not triggering receptor expressed by myeloid cells-2 during osteoclastogenesis. J. Biol. Chem. 2005, 280, 32905–32913. [Google Scholar] [CrossRef]
- Kim, K.; Kim, J.H.; Lee, J.; Jin, H.-M.; Lee, S.-H.; Fisher, D.E.; Kook, H.; Kim, K.K.; Choi, Y.; Kim, N. Nuclear factor of activated T cells c1 induces osteoclast-associated receptor gene expression during tumor necrosis factor-related activation-induced cytokine-mediated osteoclastogenesis. J. Biol. Chem. 2005, 280, 35209–35216. [Google Scholar] [CrossRef]
- Matsumoto, M.; Kogawa, M.; Wada, S.; Takayanagi, H.; Tsujimoto, M.; Katayama, S.; Hisatake, K.; Nogi, Y. Essential role of p38 mitogen-activated protein kinase in cathepsin K gene expression during osteoclastogenesis through association of NFATc1 and PU.1. J. Biol. Chem. 2004, 279, 45969–45979. [Google Scholar] [CrossRef] [PubMed]
- Takayanagi, H.; Kim, S.; Koga, T.; Nishina, H.; Isshiki, M.; Yoshida, H.; Saiura, A.; Isobe, M.; Yokochi, T.; Inoue, J.-I.; et al. Induction and activation of the transcription factor NFATc1 (NFAT2) integrate RANKL signaling in terminal differentiation of osteoclasts. Dev. Cell 2002, 3, 889–901. [Google Scholar] [CrossRef]
- Jimi, E.; Takakura, N.; Hiura, F.; Nakamura, I.; Hirata-Tsuchiya, S. The Role of NF-κB in Physiological Bone Development and Inflammatory Bone Diseases: Is NF-κB Inhibition “Killing Two Birds with One Stone”? Cells 2019, 8, 1636. [Google Scholar] [CrossRef]
- Yan, S.-D.; Huang, C.-C. The role of tumor necrosis factor-alpha in bone resorption of cholesteatoma. Am. J. Otolaryngol. 1991, 12, 83–89. [Google Scholar] [CrossRef]
- Yellon, R.F.; Leonard, G.; Marucha, P.T.; Craven, R.; Carpenter, R.J.; Lehmann, W.B.; Burleson, J.A.; Kreutzer, D.L. Characterization of cytokines present in middle ear effusions. Laryngoscope 1991, 101, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Wang, Y.; Shi, B.; Zhao, Y. Effect of propolis on preserving human periodontal ligament cells and regulating pro-inflammatory cytokines. Dent. Traumatol. 2018, 34, 245–253. [Google Scholar] [CrossRef]
- Neiva, K.G.; Catalfamo, D.L.; Holliday, S.; Wallet, S.M.; Pileggi, R. Propolis decreases lipopolysaccharide-induced inflammatory mediators in pulp cells and osteoclasts. Dent. Traumatol. 2014, 30, 362–367. [Google Scholar] [CrossRef]
- Fakhry, M.; Hamade, E.; Badran, B.; Buchet, R.; Magne, D. Molecular mechanisms of mesenchymal stem cell differentiation towards osteoblasts. World J. Stem Cells 2013, 5, 136–148. [Google Scholar] [CrossRef]
- Chen, D.; Zhao, M.; Mundy, G.R. Bone morphogenetic proteins. Growth Factors 2004, 22, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Kawai, M.; Bessho, K.; Maruyama, H.; Miyazaki, J.-I.; Yamamoto, T. Simultaneous gene transfer of bone morphogenetic protein (BMP)-2 and BMP-7 by in vivo electroporation induces rapid bone formation and BMP-4 expression. BMC Musculoskelet. Disord. 2006, 7, 62. [Google Scholar] [CrossRef]
- Lin, Y.; Murray, M.A.; Garrett, I.R.; Gutierrez, G.E.; Nyman, J.S.; Mundy, G.; Fast, D.; Gellenbeck, K.W.; Chandra, A.; Ramakrishnan, S. A targeted approach for evaluating preclinical activity of botanical extracts for support of bone health. J. Nutr. Sci. 2014, 3, e13. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lazarenko, O.P.; Wu, X.; Tong, Y.; Blackburn, M.L.; Gomez-Acevedo, H.; Shankar, K.; Badger, T.M.; Ronis, M.J.J.; Chen, J.-R. Differential effects of short term feeding of a soy protein isolate diet and estrogen treatment on bone in the pre-pubertal rat. PLOS ONE 2012, 7, e35736. [Google Scholar] [CrossRef] [PubMed]
- Pandareesh, M.D.; Mythri, R.B.; Srinivas Bharath, M.M. Bioavailability of dietary polyphenols: Factors contributing to their clinical application in CNS diseases. Neurochem. Int. 2015, 89, 198–208. [Google Scholar] [CrossRef]
- Alkhaldy, A.; Edwards, C.A.; Combet, E. The urinary phenolic acid profile varies between younger and older adults after a polyphenol-rich meal despite limited differences in in vitro colonic catabolism. Eur. J. Nutr. 2019, 58, 1095–1111. [Google Scholar] [CrossRef] [PubMed]
- Yesiltas, B.; Capanoglu, E.; Firatligil-Durmus, E.; Sunay, A.E.; Samanci, T.; Boyacioglu, D. Investigating the in-vitro bioaccessibility of propolis and pollen using a simulated gastrointestinal digestion System. J. Apic. Res. 2014, 53, 101–108. [Google Scholar] [CrossRef]
- Bazmandegan, G.; Boroushaki, M.T.; Shamsizadeh, A.; Ayoobi, F.; Hakimizadeh, E.; Allahtavakoli, M. Brown propolis attenuates cerebral ischemia-induced oxidative damage via affecting antioxidant enzyme system in mice. Biomed. Pharm. 2017, 85, 503–510. [Google Scholar] [CrossRef]
- Cornara, L.; Biagi, M.; Xiao, J.; Burlando, B. Therapeutic Properties of Bioactive Compounds from Different Honeybee Products. Front. Pharm. 2017, 8, 412. [Google Scholar] [CrossRef]
- Dobrowolski, J.W.; Vohora, S.B.; Sharma, K.; Shah, S.A.; Naqvi, S.A.; Dandiya, P.C. Antibacterial, antifungal, antiamoebic, antiinflammatory and antipyretic studies on propolis bee products. J. Ethnopharmacol. 1991, 35, 77–82. [Google Scholar] [CrossRef]
- Arvouet-Grand, A.; Lejeune, B.; Bastide, P.; Pourrat, A.; Privat, A.M.; Legret, P. Propolis extract. I. Acute toxicity and determination of acute primary cutaneous irritation index. J. Pharm. Belg. 1993, 48, 165–170. [Google Scholar] [PubMed]
- Hamza, R.; Elaziz, A.; Diab, A.; El-Aziz, E.-S.A.A. Hyperglycemic effect of Chlorpyrifos, Profenofos and possible ameliorative role of Propolis and ginseng. Scientia Adv. Agric. Biol. 2014, 1, 9–14. [Google Scholar]
- Hsu, C.-Y.; Chiang, W.-C.; Weng, T.-I.; Chen, W.-J.; Yuan, A. Laryngeal edema and anaphalactic shock after topical propolis use for acute pharyngitis. Am. J. Emerg. Med. 2004, 22, 432–433. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-J.; Lin, J.-L.; Yang, C.-W.; Yu, C.-C. Acute renal failure induced by a Brazilian variety of propolis. Am. J. Kidney Dis. 2005, 46, e125–e129. [Google Scholar] [CrossRef] [PubMed]
- Walgrave, S.E.; Warshaw, E.M.; Glesne, L.A. Allergic contact dermatitis from propolis. Dermatitis 2005, 16, 209–215. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Researcher | Study Design | Findings |
|---|---|---|
| Cell Culture Studies | ||
| Pileggi et al. [39] | Cell: RAW 264.7 and mouse marrow cells Induction: RANKL-induced osteoclastogenesis Treatment: 1 and 10 μL propolis for 7 days Control: Negative: no treatment Positive: no | ↑ mononuclear TRAP+ cells vs. negative control ↓ multinuclear and giant TRAP+ cells vs. negative control ↓ actin rings formation vs. negative control |
| Wimolsantirungsri et al. [40] | Cell: Human peripheral blood mononuclear cells Induction: RANKL and M-CSF-induced osteoclastogenesis Treatment: 0.025–10 mg/mL propolis for 24 h or 7 days Control: Negative: no treatment Positive: no | ↓ TRAP-positive cells with the range 0.1–10 mg/mL vs. negative control ↓ expression of osteoclast-specific genes (NFAT2, CTSK, RANK, CLCN7, and CTR) in dose dependent manner in 0.1 and 0.5 mg/mL vs. negative control |
| Somsanith et al. [41] | Cell: MC-3T3-E1 pre-osteoblasts Induction: Treatment: 60% crude propolis-loaded TNT-Ti (PL-TNT-Ti) plates for 1, 5 and 14 days Control: Negative: CP-Ti Positive: TNT-Ti | ↑ cell proliferation and ALP activity vs. negative control |
| Lim et al. [42] | Cell: Human osteoblast-like cell line MG-63 Induction: NA Treatment: 17 and 34 μg/mL propolis extract for 24 h Control: Negative: no treatment Positive: 10 ng/mL rhBMP2 | ↑ mineralisation and ALP activity in 34 µg/mL propolis-treated group vs. negative control ↑ RUNX2 expression on day 2 and 8 in 34 µg/mL propolis-treated group and day 8 in 17 µg/mL propolis group compared to negative control ↑ OSX expression on day 4 in 17 and 34 µg/mL propolis treated group vs. negative control; ↓ OSX expression on day 8 in 34 µg/mL propolis-treated group vs. negative control ↓ type 1 collagen alpha expression on day 2 in 34 µg/mL propolis-treated group, day 2 and 8 in 17 µg/mL propolis group and ↑ on day 1 in 17 µg/mL vs. negative control ↑ osteocalcin expression on day 2, 4 and 8 in 17 µg/mL propolis group vs. negative control |
| Animal Studies | ||
| Toker et al. [48] | Animals: Male Wistar rats (300–330 g) Disease Model: Ligature-induced periodontitis Treatment: 100 and 200 mg/kg of propolis (oral gavage) for 11 days Control: Negative: no treatment Positive: no | ↓ alveolar bone loss vs. negative control ↓ osteoclast number in alveolar bone vs. negative control |
| Gulinelli et al. [53] | Animals: Male Wistar rats (250–300 g) Disease Model: Delayed tooth replantation Treatment: Extracted teeth was immersed in 20 mL of 15% propolis in propylene glycol solution for 10 min before replantation Control: Negative: 20 mL physiologic saline Positive: 20 mL of 2% acidulated phosphate sodium fluoride | ⟷ inflammatory resorption in alveolar bone vs. positive and negative control ⟷ replacement resorption in alveolar bone vs. positive and negative control ⟷ extent of fusion between alveolar bone and cementum vs. positive and negative control |
| Al-Hariri et al. [43] | Animals: Adult male albino rats (150–300 g) Disease Model: STZ-induced diabetes Treatment: 300 and 600 mg/kg of propolis (oral gavage) for 6 weeks Control: Negative: no treatment Positive: Insulin injection (5 IU/kg/day) | ↓ calcitonin and PTH in plasma vs. negative control ⟷ ratio of femur ash to femur weight and magnesium in femur ash vs. negative control and positive control ↑ calcium and phosphorus in femur ash vs. negative and positive control ↑ femur weight to body weight ratio vs. negative control |
| Guney et al. [45] | Animals: Male Sprague Dawley rats (280–480 g) Disease Model: Femur fracture and retrograde fixation Treatment: 200 mg/kg/day of propolis (oral gavage) for 3 weeks and 6 weeks Control: Negative: no treatment Positive: no | ↑ bone mineral density vs. negative control ↑ radiological and histological scores in femur vs. negative control ↓ plasma SOD at week 3 vs. negative control ⟷ plasma SOD at week 6 vs. negative control ↓ SOD in bone tissue at weeks 3 and 6 vs. negative control ↓ total GSH and MPO levels in plasma and bone tissue at weeks 3 and 6 vs. negative control |
| Altan et al. [54] | Animals: Male Wistar albino rats 200 g (±10 g) 12 weeks old Model: RMET reatment: 100 mg/kg/day of propolis (oral gavage) for 12 days. Control: Negative: no treatment Positive: no | ↑ osteoclast, osteoblast and capillary numbers in maxillary bone vs. negative control ↑ new bone formation and inflammatory cell infiltration in maxillary bone vs. negative control |
| Bereket et al. [46] | Animals: Male New Zealand white rabbits (2.5–3.0 kg). Model: Distraction osteogenesis Treatment: 100 (P100) and 200 (P200) mg/kg/day of propolis (oral gavage) for 32 days. Control: Negative: no treatment Positive: no | ↓ new bone formation in distraction gap of mandible bone vs. control group. ↑ area of matured bone in distraction gap of mandible bone in P200 vs. P100 and control group. ⟷ volume of connective tissue (Vct), number of capillaries (Nc) in distraction gap of mandible bone vs. control group. ↓volume of new bone area (Vn) in distraction gap of mandible bone of P200 vs. P100 and control group ↑ BMC for P200 at week 1 and 4 vs. P100 and control group ↑ BMD for P200 at week 1 and 4 vs. P100 and control group |
| Aral et al. [56] | Animals: Male Wistar albino rats (300–350 g) Disease Model: Ligature-induced periodontitis/STZ-induced diabetes Treatment: 100 mg/kg/day of propolis (oral gavage) for 21 days. Control: Negative: no treatment Positive: no | ↓ alveolar bone loss vs. negative control ⟷ plasma IL-1β, TNF-α, and MMP-8 levels vs. negative control ↓ linear distance from cementoenamel junction to the alveolar bone crest vs. negative control. |
| Nakajima et al. [47] | Animals: Male C57BL/6 mice (8 weeks old) Disease Model: Porphyromonas gingivalis-induced periondotitis Treatment: 200 mg/kg propolis (oral gavage) for 5 weeks. Control: Negative: no treatment Positive: no | ⟷ alveolar bone loss vs. negative control |
| Somsanith et al. [41] | Animals: Male Sprague-Dawley rats Model: Dental implantation Treatment: Crude propolis extract (purity 60%)-loaded TNT-Ti implants (PL-TNT-Ti) for 1 and 4 weeks Control: Negative: TNT-Ti implants Positive: no | ↑ new bone formation around implants in mandibular bone vs. negative control at 4 weeks ↑ bone mineral density and the volume of newly formed bone around implants in mandibular bone vs. negative control at 1, 2, 3, and 4 weeks ↑ expression of well-formed collagenous bone trabeculae, muscle fibres and cytoplasm around implants in mandibular bone vs. negative control ↑ formation of new bone with concentration of macrophages and nuclei around implant surface in mandibular bone vs. negative control ↓ expression of inflammatory cytokines such as IL-1β, and TNF-α around the surface of the implant in mandibular bone vs. negative control. ↑ expression of bone formation molecules BMP-2 and 7 around the surface of the implant in mandibular bone vs. negative control |
| Yuanita et al. [49] | Animals: Male Wistar rats (130–150 g) Disease Model: Enterococcus faecalis-induced chronic apical periodontitis Treatment: 10 μL of 12% propolis aqua destilata (pure water) Control: Negative: no treatment Positive: no | ↓ osteoclast number and ↑ OPG expression in periapical of alveolar bone vs. negative control |
| Zohery et al. [55] | Animals: Male Mongrel dogs (18–24 months old, 18–24 kg) Disease Model: Surgically created grade II furcation defects Treatment: 400 mg propolis graft for 1 and 3 months Control: Negative: no Positive: nanohydroxyapatite graft | ⟷ newly formed bone in alveolar bone after 1 month vs. positive control ↑ trabecular bone in inter-radicular defect after 3 months vs. positive control ↑ bone height and surface area of inter-radicular bone vs. positive control |
| Meimandi-Parizi et al. [44] | Animals: Male Wistar rats (8 weeks old, 200–250 g) Disease Model: critical non-union bone defect Treatment: 0.1 mL of 250 mg/mL propolis extract (injected percutaneously into defect site) on day of operation and day 3 post operation (chitosan-propolis and DBM-propolis) Control: Negative: no treatment Positive: Chitosan and DBM scaffolds | ↑ formation of fresh bone tissue, woven bone and cartilage tissue in radius and ulna complexes of DBM-propolis group vs. negative control, positive control and chitosan-propolis group ↑ maximum load, maximum stress and yield load and ↓ ultimate strain and yield strain in radius and ulna complexes of DBM-propolis group vs. negative control, positive control and chitosan-propolis group |
| Wiwekowati et al. [52] | Animals: Male Wistar rats (200–250 g) Disease Model: Orthodontic tooth movement Treatment: 5% propolis in carboxymethyl cellulose/nipagin/glyceryl/triethanolamine gel mixture for 17 days Control: Negative: no treatmentPositive: no | ↑ osteoblast number in alveolar bone vs. negative control ↓ serum MDA level vs. negative control |
| Kresnoadi et al. [50] | Animals: Male guinea pigs (3–3.5 months, 300–350 g) Disease Model: Orthodontic tooth movement Treatment: 100 µL (0.1 cc) of propolis extract (filled into alveolar bone socket) for 3 and 7 days Control: Negative: polyethylene glycol Positive: bovine bone graft | ↑ osteoblast number in alveolar bone vs. negative control |
| Kresnoadi et al. [51] | Animals: Male guinea pigs (3–3.5 months, 300–350 g) Disease Model: Orthodontic tooth movement Treatment: 2% (0.5 g) propolis in polyethylene glycol (filled into alveolar bone socket) for 3 and 7 days Control: Negative: polyethylene glycol Positive: bovine bone graft | ↑ osteoblast number, osteocalcin expression and ↓ osteoclast number in alveolar bone vs. negative control |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekeuku, S.O.; Chin, K.-Y. Application of Propolis in Protecting Skeletal and Periodontal Health—A Systematic Review. Molecules 2021, 26, 3156. https://doi.org/10.3390/molecules26113156
Ekeuku SO, Chin K-Y. Application of Propolis in Protecting Skeletal and Periodontal Health—A Systematic Review. Molecules. 2021; 26(11):3156. https://doi.org/10.3390/molecules26113156
Chicago/Turabian StyleEkeuku, Sophia Ogechi, and Kok-Yong Chin. 2021. "Application of Propolis in Protecting Skeletal and Periodontal Health—A Systematic Review" Molecules 26, no. 11: 3156. https://doi.org/10.3390/molecules26113156
APA StyleEkeuku, S. O., & Chin, K.-Y. (2021). Application of Propolis in Protecting Skeletal and Periodontal Health—A Systematic Review. Molecules, 26(11), 3156. https://doi.org/10.3390/molecules26113156