
Antibacterial Properties of Tebipenem Pivoxil Tablet, a New Oral Carbapenem Preparation against a Variety of Pathogenic Bacteria in Vitro and in Vivo

Abstract
:1. Introduction
2. Results
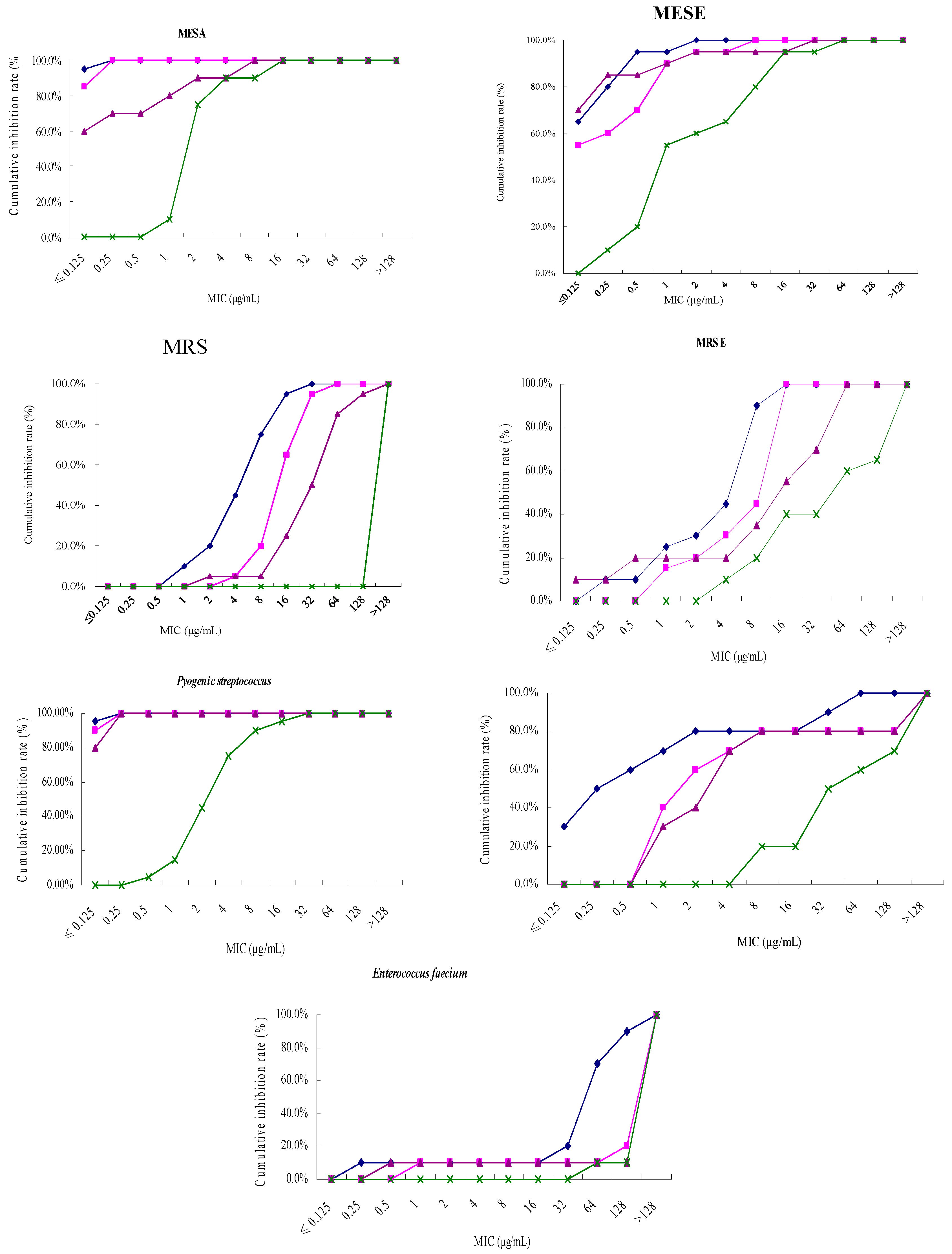
2.1. Tebipenem Pivoxil Displays Excellent Antibacterial Activity against a Variety of Pathogenic Bacteria in Vitro


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strain | MIC50/MIC90 (μg/mL) | |||
|---|---|---|---|---|
| Tebipenem Pivoxil | Meropenem | Imipenem and Cilastatin | Ceftriaxone | |
| MSSA | ≤0.125/0.125 | ≤0.125/0.25 | ≤0.125/2 | 2/4 |
| MRSA | 8/16 | 16/32 | 32/128 | >128/>128 |
| MSSE | ≤0.125/0.5 | ≤0.125/1 | ≤0.125/1 | 1/16 |
| MRSE | 8/8 | 16/16 | 16/64 | 64/>128 |
| Enterococcus faecalis | 0.25/32 | 2/>128 | 4/>128 | 32/>128 |
| Enterococcus faecium | 64/128 | >128/>128 | >128/>128 | >128/>128 |
| Pyogenic streptococcus | ≤0.125/≤0.125 | ≤0.125/≤0.125 | ≤0.125/0.25 | 4/8 |
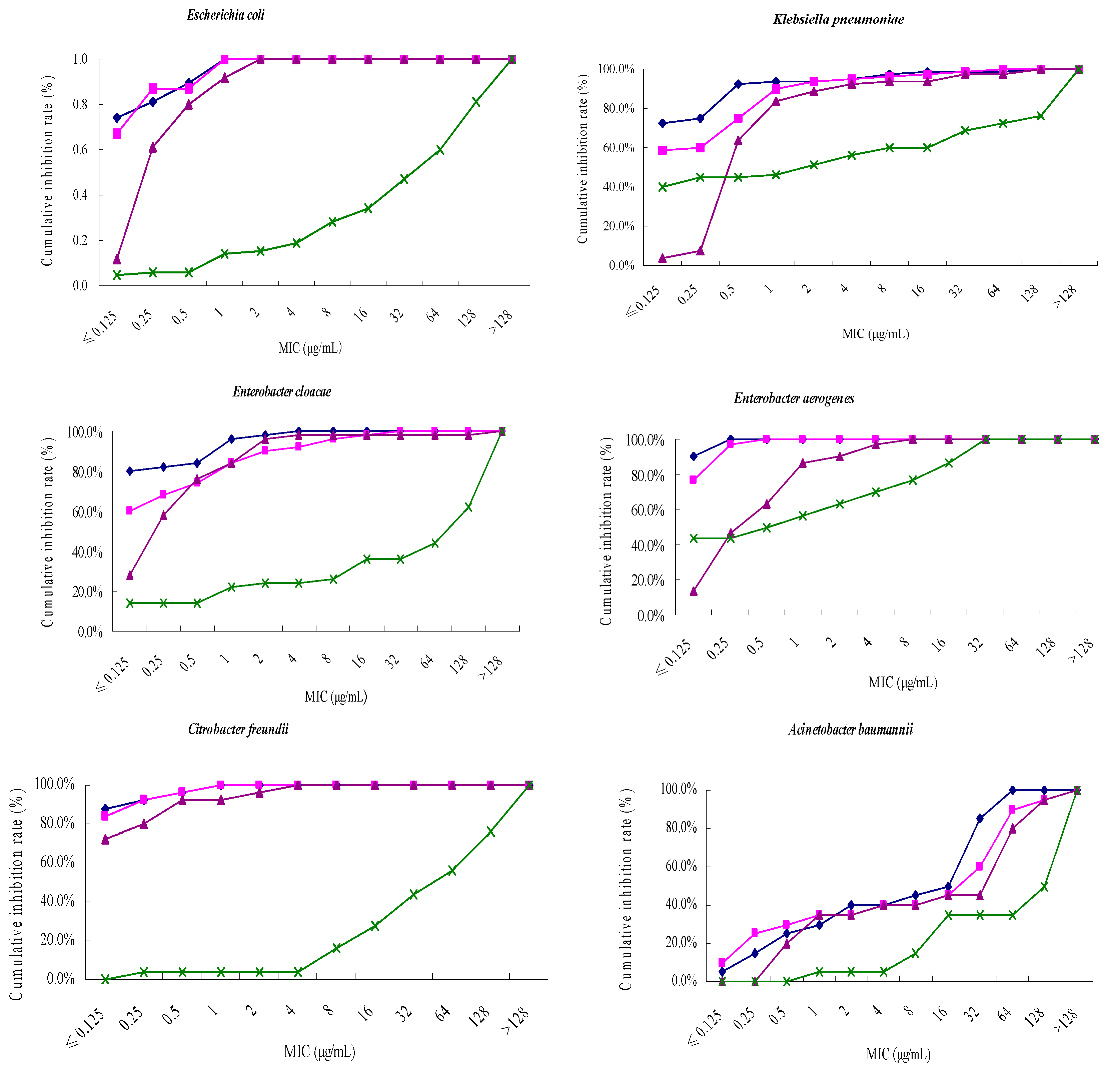
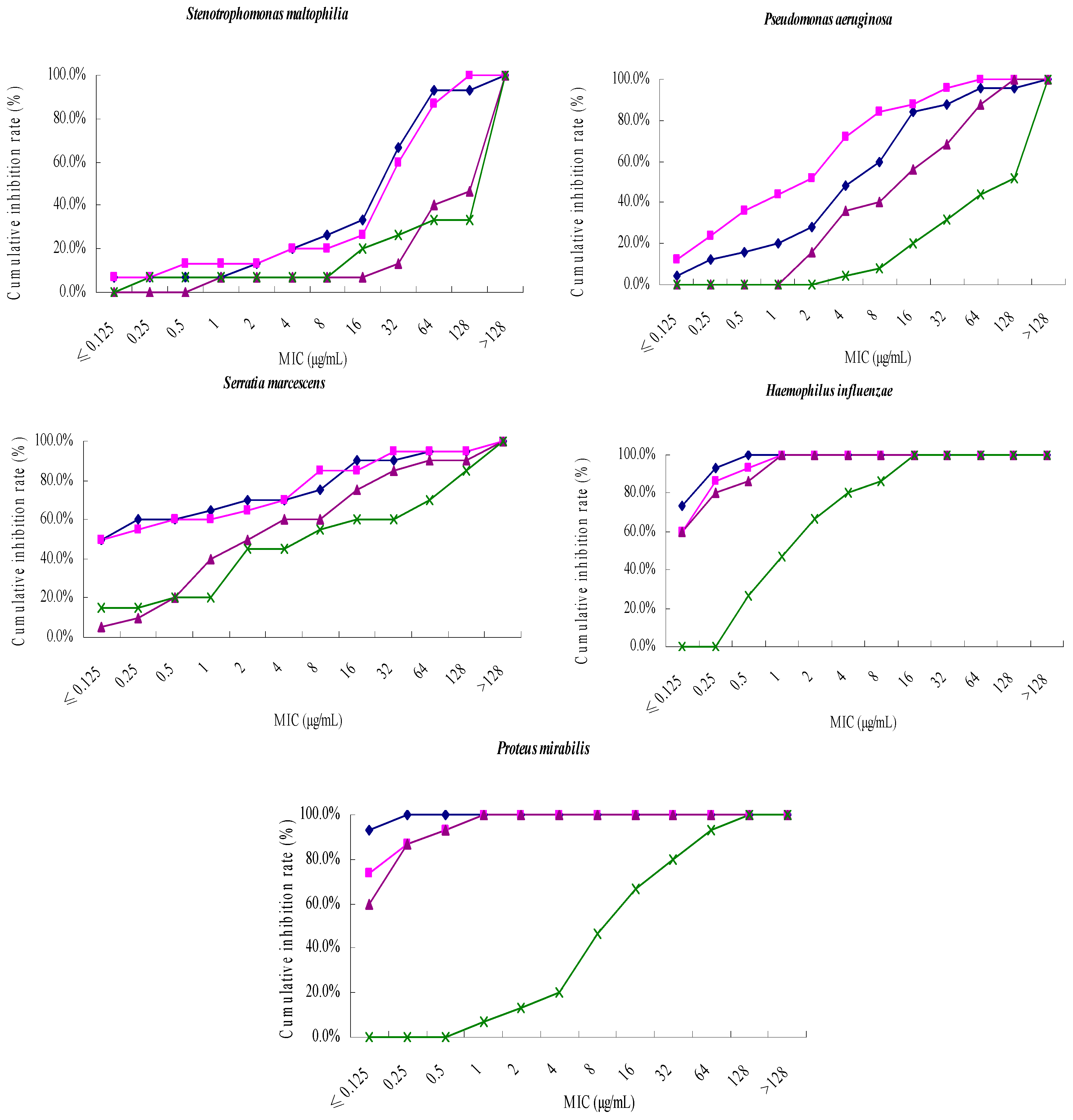
| Strain | MIC50/MIC90 (μg/mL) | |||
|---|---|---|---|---|
| Tebipenem Pivoxil | Meropenem | Imipenem and Cilastatin | Ceftriaxone | |
| Escherichia coli | ≤0.125/1 | ≤0.125/1 | 0. 25/1 | 64/>128 |
| Klebsiella pneumoniae | ≤0.125/0.5 | ≤0.125/1 | 0.5/4 | 2/>128 |
| Enterobacter cloacae | ≤0.125/1 | ≤0.125/2 | 0.25/2 | 128/>128 |
| Enterobacter aerogenes | ≤0.125/≤0.125 | ≤0.125/0.25 | 0.5/2 | 0.5/32 |
| Citrobacter freundii | ≤0.125/0.25 | ≤0.125/0.25 | ≤0.125/0.5 | 64/>128 |
| Acinetobacter baumannii | 16/64 | 32/64 | 64/128 | 128/>128 |
| Stenotrophomonas maltophilia | 32/64 | 32/128 | >128/>128 | >128/>128 |
| Pseudomonas aeruginosa | 8/64 | 2/32 | 16/128 | 128/>128 |
| Serratia marcescens | ≤0.125/16 | ≤0.125/32 | 2/64 | 8/>128 |
| Haemophilus influenzae | ≤0.125/0.25 | ≤0.125/0.5 | ≤0.125/1 | 2/16 |
| Proteus mirabilis | ≤0.125/≤0.125 | ≤0.125/0.5 | ≤0.125/0.5 | 16/64 |
| Strain | MBC/MIC (μg/mL) |
|---|---|
| Escherichia coli | |
| ATCC25922 | 0.031/0.016 |
| Clinical strain 03 | 0.125/0.016 |
| Clinical strain 10 | 1/0.25 |
| Clinical strain 14 | 2/1 |
| Clinical strain 17 | 0.25/0.031 |
| Clinical strain 49 | 0.125/0.125 |
| Clinical strain 63 | 1/0.5 |
| Clinical strain 75 | 0.25/0.063 |
| Clinical strain 79 | 0.016/0.016 |
| Clinical strain 80 | 0.031/0.031 |
| Staphylococcus aureus | |
| ATCC25923 | 0.125/0.031 |
| Clinical strain 02 | 0.063/0.016 |
| Clinical strain 14 | 2/0.25 |
| Clinical strain 19 | 0.125/0.063 |
| Clinical strain 21 | 32/4 |
| Clinical strain 24 | 4/2 |
| Clinical strain 27 | 2/1 |
| Clinical strain 31 | 8/4 |
| Clinical strain 33 | 4/1 |
| Clinical strain 34 | 4/2 |
| Klebsiella pneumoniae | |
| ATCC10031 | 1/0.5 |
| Clinical strain 07 | 0.063/0.031 |
| Clinical strain 18 | 1/0.25 |
| Clinical strain 20 | 32/8 |
| Clinical strain 28 | 0.125/0.016 |
| Clinical strain 39 | 0.031/0.016 |
| Clinical strain47 | 0.5/0.063 |
| Clinical strain 64 | 1/0.125 |
| Clinical strain 70 | 2/0.5 |
| Clinical strain 73 | 0.063/0.016 |
2.2. Acute Toxicity Measurement of Tebipenem Pivoxil Tablet in Mice
| Group | Dosage (g/kg) | Body Weight (g) | |||
|---|---|---|---|---|---|
| Time after Administration (Day) | |||||
| 0 | 3 | 7 | 14 | ||
| Vehicle | - | 19.5 ± 1.6 | 23.4 ± 1.5 | 25.2 ± 2.9 | 26.9 ± 4.0 |
| Tebipenem pivoxil | 4.00 | 18.7 ± 0.7 | 22.3 ± 1.4 | 25.4 ± 1.8 | 27.6 ± 3.2 |
| 3.40 | 19.5 ± 1.5 | 23.9 ± 2.6 | 25.3 ± 3.1 | 26.3 ± 3.5 | |
| 2.89 | 19.2 ± 1.1 | 23.2 ± 2.0 | 25.3 ± 2.7 | 26.6 ± 2.7 | |
| Reagent | Dosage (g/kg) | Liver Toxicity | Kidney Toxicity | ||
|---|---|---|---|---|---|
| Present | Absent | Present | Absent | ||
| Tebipenem pivoxil | 4.00 | 6 | 13 | 5 | 14 |
| 3.20 | 4 | 16 | 4 | 16 | |
| 2.89 | 3 | 17 | 2 | 18 | |
| Vehicle | - | 0 | 0 | 0 | 0 |
2.3. Tebipenem Pivoxil Tablet Protects Sepsis Mice from Lethal Challenges with Pathogenic Bacteria
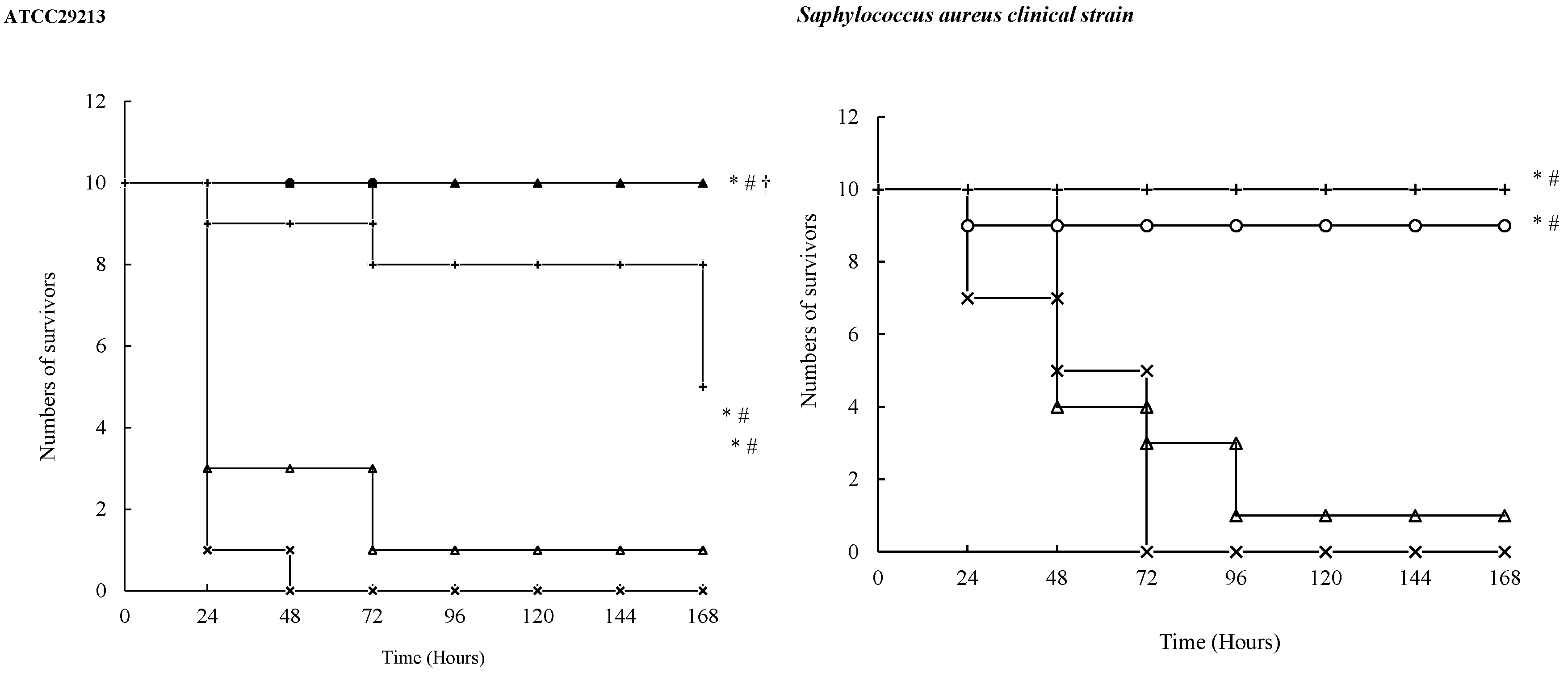

2.4. Measurements of ED50s of Tebipenem Pivoxil Tablet in Sepsis Mouse Models
| Strain | Dose (mg/kg) | Survival Number | ED50 (mg/kg) | 95% CI (mg/kg) |
|---|---|---|---|---|
| ATCC29213 | 50.0 | 10 | 7.0281 | 4.8242~10.2389 |
| 25.0 | 9 | |||
| 12.5 | 7 | |||
| 6.25 | 7 | |||
| 3.13 | 1 | |||
| Staphylococcus aureus clinical strain | 100.0 | 10 | 18.6414 | 12.1759~28.5401 |
| 50.0 | 7 | |||
| 25.0 | 6 | |||
| 12.5 | 4 | |||
| 6.25 | 2 | |||
| 3.13 | 0 | |||
| ATCC10031 | 25 | 10 | 5.3265 | 3.6176~7.8426 |
| 12.5 | 8 | |||
| 6.25 | 4 | |||
| 3.125 | 3 | |||
| 1.56 | 1 | |||
| 0.78 | 0 | |||
| Klebsiella pneumoniae clinical strain | 25 | 10 | 2.3205 | 1.6219~3.3201 |
| 12.5 | 9 | |||
| 6.25 | 9 | |||
| 3.125 | 7 | |||
| 1.56 | 7 | |||
| 0.78 | 0 | |||
| ATCC29522 | 6.25 | 10 | 1.5529 | 1.0720~2.2496 |
| 3.125 | 8 | |||
| 1.56 | 5 | |||
| 0.78 | 2 | |||
| 0.39 | 0 | |||
| Escherichia coli clinical strain | 12.5 | 10 | 3.0932 | 2.1156~4.5224 |
| 6.25 | 8 | |||
| 3.125 | 4 | |||
| 1.56 | 3 | |||
| 0.78 | 0 | |||
| ATCC27853 | 100 | 10 | 20.8060 | 14.7041~29.4400 |
| 50 | 9 | |||
| 25 | 7 | |||
| 12.5 | 3 | |||
| 6.25 | 0 | |||
| Pseudomonas aeruginosa clinical strain | 100 | 10 | 20.6961 | 14.3390~29.8717 |
| 50 | 9 | |||
| 25 | 6 | |||
| 12.5 | 4 | |||
| 6.25 | 0 |
3. Discussion
4. Materials and Methods
4.1. Bacterial Strains
4.2. Experimental Animals
4.3. Main Reagents
4.4. Drug Susceptibility Assay
4.5. Acute Toxicity Measurement of Tebipenem Pivoxil Tablet in Mice
4.6. Establishment of Sepsis Mouse Models Challenged with Pathogenic Bacteria and Treatments
4.7. Measurements of 50% Effective Dosages (ED50) of Tebipenem Pivoxil Tablet in Bacterial Sepsis Mouse Models
4.8. Statistics and Presentation of Data
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bassetti, M.; Nicolini, L.; Esposito, S.; Righi, E.; Viscoli, C. Current status of newer carbapenems. Curr. Med. Chem. 2009, 16, 564–575. [Google Scholar] [CrossRef] [PubMed]
- El-Gamal, M.I.; Oh, C.H. Current status of carbapenem antibiotics. Curr. Top. Med. Chem. 2010, 10, 1882–1897. [Google Scholar] [CrossRef] [PubMed]
- Sugita, R. Good transfer of tebipenem into middle ear effusion conduces to the favorable clinical outcomes of tebipenem pivoxil in pediatric patients with acute otitis media. J. Infect. Chemother. 2013, 19, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Kijima, K.; Sato, N.; Koresawa, T.; Morita, J.; Hayashi, H.; Shibasaki, S.; Kurosawa, T.; Totsuka, K. Pharmacokinetics analysis of tebipenem pivoxil in a phase II clinical trial in otolaryngological infections. Jpn. J. Antibiot. 2009, 62, 143–154. [Google Scholar] [PubMed]
- Ouchi, K.; Sunakawa, K. Effect of new oral antimicrobial agents in outpatient treatment of pneumonia in children. Jpn. J. Antibiot. 2014, 67, 157–166. [Google Scholar] [PubMed]
- Cone, L.A.; Stone, R.A.; Jesser, K.; Nelson, R. Clinical experience with drotrecogin alfa in treating gram-positive and -negative pathogens in patients with severe sepsis. J. Investig. Med. 2004, 52, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Sakata, H. Clinical efficacy of tebipenem pivoxil treatment in children with pneumonia, who had no relief despite having administered oral beta-lactam antibiotics. Jpn. J. Antibiot. 2011, 64, 171–177. [Google Scholar] [PubMed]
- Kuroki, H.; Tateno, N.; Ikeda, H.; Saito, N. Investigation of pneumonia-causing pathogenic organisms in children and the usefulness of tebipenem pivoxil for their treatment. J. Infect. Chemother. 2010, 16, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Sato, N.; Kijima, K.; Koresawa, T.; Mitomi, N.; Morita, J.; Suzuki, H.; Hayashi, H.; Shibasaki, S.; Kurosawa, T.; Totsuka, K. Population pharmacokinetics of tebipenem pivoxil (ME1211), a novel oral carbapenem antibiotic, in pediatric patients with otolaryngological infection or pneumonia. Drug Metab. Pharmacokinet. 2008, 23, 434–446. [Google Scholar] [CrossRef] [PubMed]
- Baba, S.; Yamanaka, N.; Suzuki, K.; Furukawa, M.; Furuya, N.; Ubukata, K.; Totsuka, K. Clinical efficacy, safety and PK-PD analysis of tebipenem pivoxil in a phase II clinical trial in otolaryngological infections. Jpn. J. Antibiot. 2009, 62, 155–177. [Google Scholar] [PubMed]
- Moellering, R.C., Jr. MRSA: The first half century. J. Antimicrob. Chemother. 2012, 67, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Cimolai, N. Methicillin-resistant Staphylococcus aureus in Canada: A historical perspective and lessons learned. Can. J. Microbiol. 2010, 56, 89–120. [Google Scholar] [CrossRef] [PubMed]
- Tambyah, P.A.; Kumarasinghe, G. Methicillin-resistant Staphylococcus aureus control at the National University Hospital, Singapore: A historical perspective. Ann. Acad. Med. Singap. 2008, 37, 855–860. [Google Scholar] [PubMed]
- Friães, A.; Resina, C.; Manuel, V.; Lito, L.; Ramirez, M.; Melo-Cristino, J. Epidemiological survey of the first case of vancomycin-resistant Staphylococcus aureus infection in Europe. Epidemiol. Infect. 2015, 143, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Limbago, B.M.; Kallen, A.J.; Zhu, W.; Eggers, P.; McDougal, L.K.; Albrecht, V.S. Report of the 13th vancomycin-resistant Staphylococcus aureus isolate from the United States. J. Clin. Microbiol. 2014, 52, 998–1002. [Google Scholar] [CrossRef] [PubMed]
- Gardete, S.; Tomasz, A. Mechanisms of vancomycin resistance in Staphylococcus aureus. J. Clin. Investig. 2014, 124, 2836–2840. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, Y.; Li, B.; Mao, Y.; Wu, X.; Zou, X.; Gao, P.; Yan, H.; Yang, D.; Ling, Y.; et al. Three supplementary methods for analyzing cytotoxicity of Escherichia coli O157:H7. J. Microbiol. Methods 2016, 120, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Koga, V.L.; Scandorieiro, S.; Vespero, E.C.; Oba, A.; de Brito, B.G.; de Brito, K.C.T.; Nakazato, G.; Kobayashi, R.K.T. Comparison of Antibiotic Resistance and Virulence Factors among Escherichia coli Isolated from Conventional and Free-Range Poultry. Biomed. Res. Int. 2015, 2015, 618752. [Google Scholar] [CrossRef] [PubMed]
- Thamlikitkul, V.; Lorchirachoonkul, N.; Tiengrim, S. In vitro and in vivo activity of tebipenem against ESBL-producing E. coli. J. Med. Assoc. Thail. 2014, 97, 1259–1268. [Google Scholar]
- Muratani, T.; Doi, K.; Kobayashi, T.; Nakamura, T.; Matsumoto, T. Antimicrobial activity of tebipenem against various clinical isolates from various specimen, mainly urinary tract. Jpn. J. Antibiot. 2009, 62, 116–126. [Google Scholar] [PubMed]
- Tamayo, E.; Almansa, R.; Carrasco, E.; Ávila-Alonso, A.; Rodríguez-Fernández, A.; Wain, J.; Heredia, M.; Gomez-Sanchez, E.; Soria, S.; Rico, L.; et al. Quantification of IgM molecular response by droplet digital PCR as a potential tool for the early diagnosis of sepsis. Crit. Care 2014, 18, 433. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhou, H.; Zheng, J.; Cheng, J.; Liu, W.; Ding, G.; Wang, L.; Luo, P.; Lu, Y.; Cao, H.; et al. The antimalarial artemisinin synergizes with antibiotics to protect against lethal live Escherichia coli challenge by decreasing proinflammatory cytokine release. Antimicrob. Agents Chemother. 2006, 50, 2420–2427. [Google Scholar] [CrossRef] [PubMed]
- Morrison, D.C.; Bucklin, S.E. Evidence for antibiotic-mediated endotoxin release as a contributing factor to lethality in experimental gram-negative sepsis. Scand. J. Infect. Dis. Suppl. 1996, 101, 3–8. [Google Scholar] [PubMed]
- Hong, Z.; Jiang, Z.; Liangxi, W.; Guofu, D.; Ping, L.; Yongling, L.; Wendong, P.; Minghai, W. Chloroquine protects mice from challenge with CpG ODN and LPS by decreasing proinflammatory cytokine release. Int. Immunopharmacol. 2004, 4, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Ahmad-Nejad, P.; Häcker, H.; Rutz, M.; Bauer, S.; Vabulas, R.M.; Wagner, H. Bacterial CpG-DNA and lipopolysaccharides activate Toll-like receptors at distinct cellular compartments. Eur. J. Immunol. 2002, 32, 1958–1968. [Google Scholar] [CrossRef]
- Kaisho, T.; Akira, S. Toll-like receptors as adjuvant receptors. Biochim. Biophys. Acta 2002, 1589, 1–13. [Google Scholar] [CrossRef]
- Byerley, L.O.; Alcock, N.W.; Starnes, H.F., Jr. Sepsis-induced cascade of cytokine mRNA expression: Correlation with metabolic changes. Am. J. Physiol. 1992, 262, E728–E735. [Google Scholar] [PubMed]
- Kijima, K.; Morita, J.; Suzuki, K.; Aoki, M.; Kato, K.; Hayashi, H.; Shibasaki, S.; Kurosawa, T. Pharmacokinetics of tebipenem pivoxil, a novel oral carbapenem antibiotic, in experimental animals. Jpn. J. Antibiot. 2009, 62, 214–240. [Google Scholar] [PubMed]
- Baba, S.; Kasahara, H.; Morita, J.; Aizawa, K.; Sunakawa, K. Tissue and aural discharge distribution of tebipenem pivoxil. Jpn. J. Antibiot. 2009, 62, 127–135. [Google Scholar] [PubMed]
- Sample Availability: Samples of the compounds are available from the authors.
© 2016 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yao, Q.; Wang, J.; Cui, T.; Yang, Z.; Su, M.; Zhao, P.; Yan, H.; Zhan, Y.; Yang, H. Antibacterial Properties of Tebipenem Pivoxil Tablet, a New Oral Carbapenem Preparation against a Variety of Pathogenic Bacteria in Vitro and in Vivo. Molecules 2016, 21, 62. https://doi.org/10.3390/molecules21010062
Yao Q, Wang J, Cui T, Yang Z, Su M, Zhao P, Yan H, Zhan Y, Yang H. Antibacterial Properties of Tebipenem Pivoxil Tablet, a New Oral Carbapenem Preparation against a Variety of Pathogenic Bacteria in Vitro and in Vivo. Molecules. 2016; 21(1):62. https://doi.org/10.3390/molecules21010062
Chicago/Turabian StyleYao, Qi, Jingkun Wang, Tao Cui, Zhi Yang, Mei Su, Peiyue Zhao, Hong Yan, Yi Zhan, and Hongbo Yang. 2016. "Antibacterial Properties of Tebipenem Pivoxil Tablet, a New Oral Carbapenem Preparation against a Variety of Pathogenic Bacteria in Vitro and in Vivo" Molecules 21, no. 1: 62. https://doi.org/10.3390/molecules21010062
APA StyleYao, Q., Wang, J., Cui, T., Yang, Z., Su, M., Zhao, P., Yan, H., Zhan, Y., & Yang, H. (2016). Antibacterial Properties of Tebipenem Pivoxil Tablet, a New Oral Carbapenem Preparation against a Variety of Pathogenic Bacteria in Vitro and in Vivo. Molecules, 21(1), 62. https://doi.org/10.3390/molecules21010062