
A Herbal Formula, Atofreellage, Ameliorates Atopic Dermatitis-Like Skin Lesions in an NC/Nga Mouse Model



Abstract
:1. Introduction
2. Results
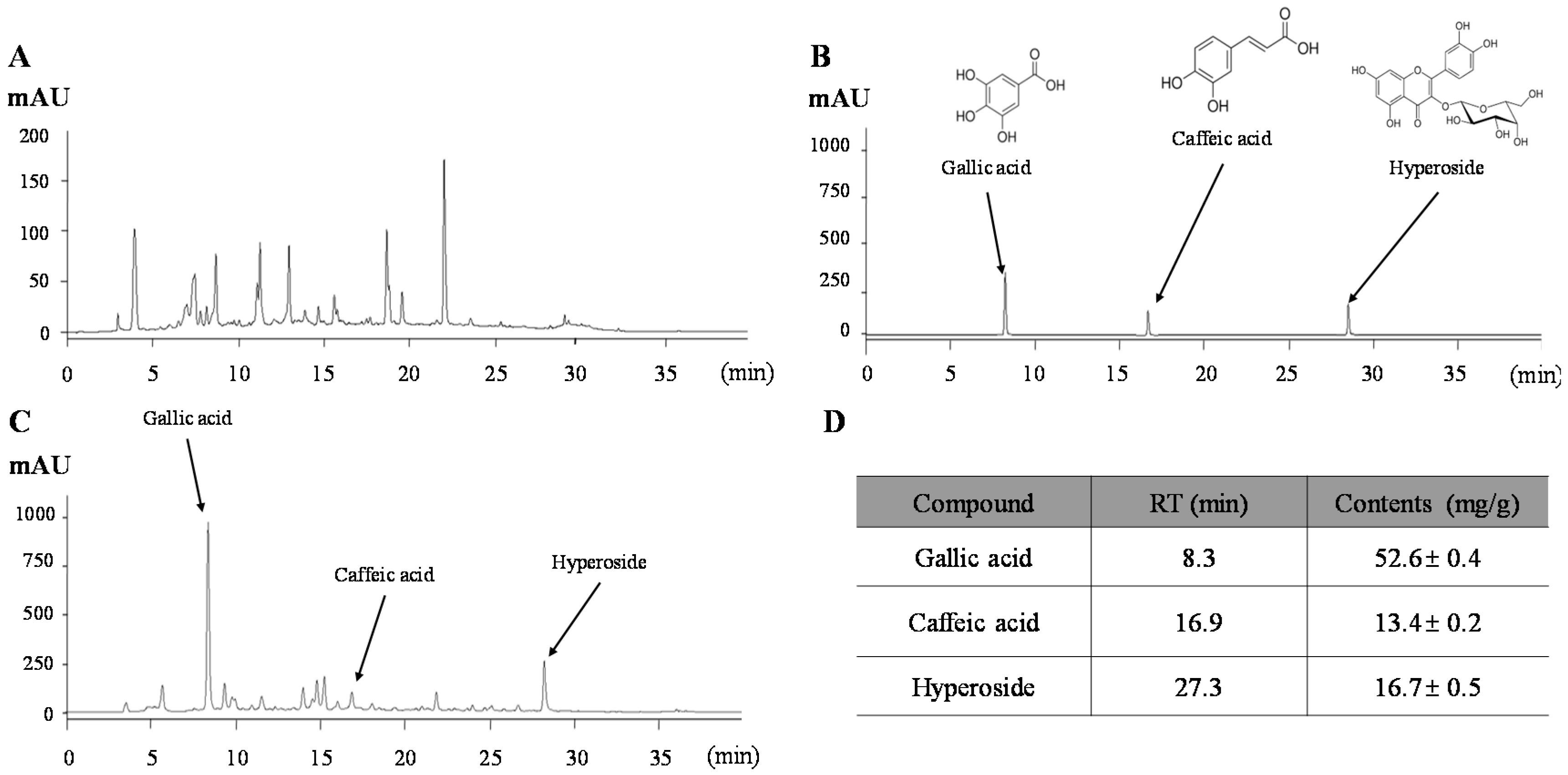
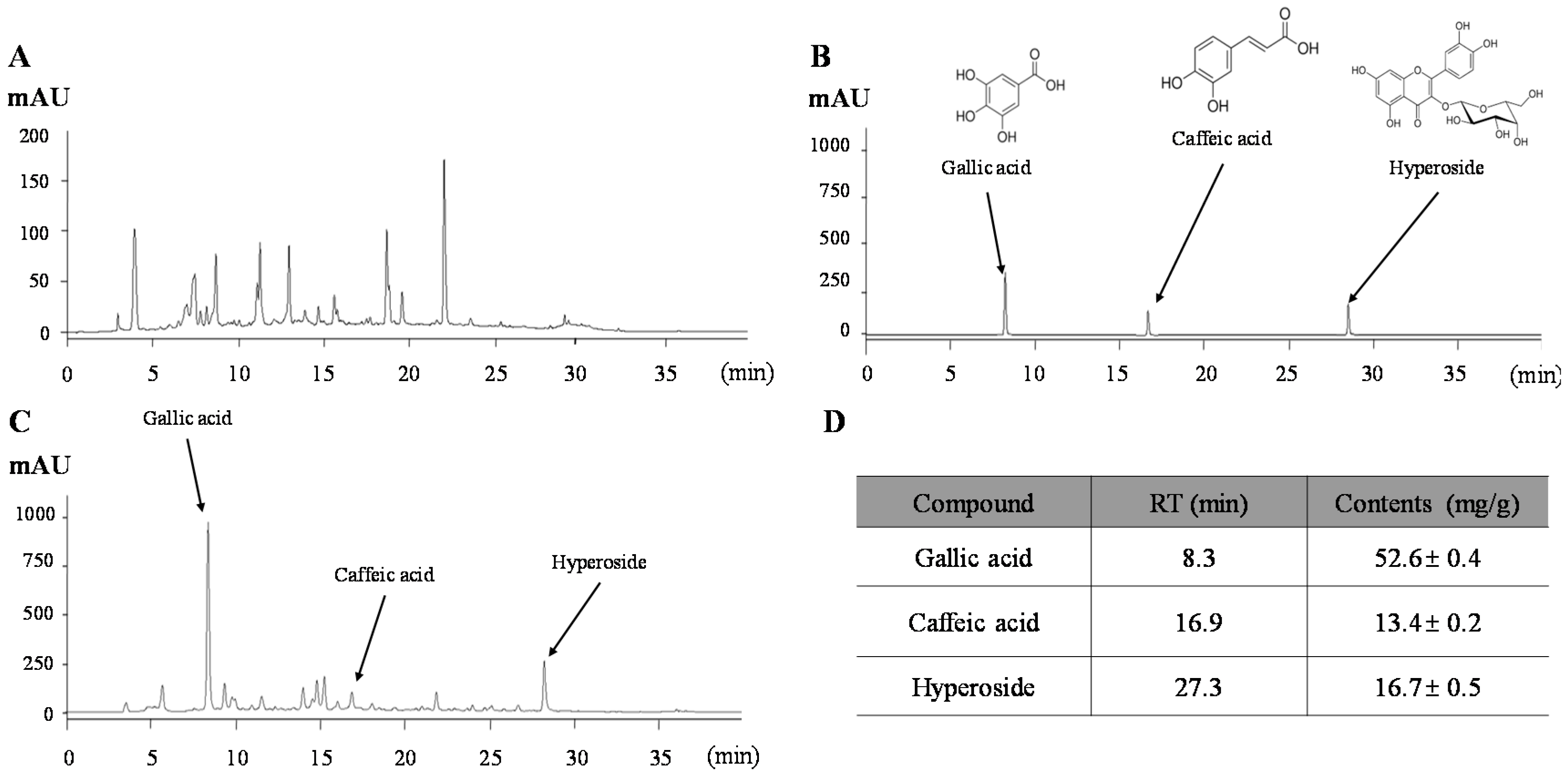
2.1. Chemical Constitution Analysis of Atofreellage
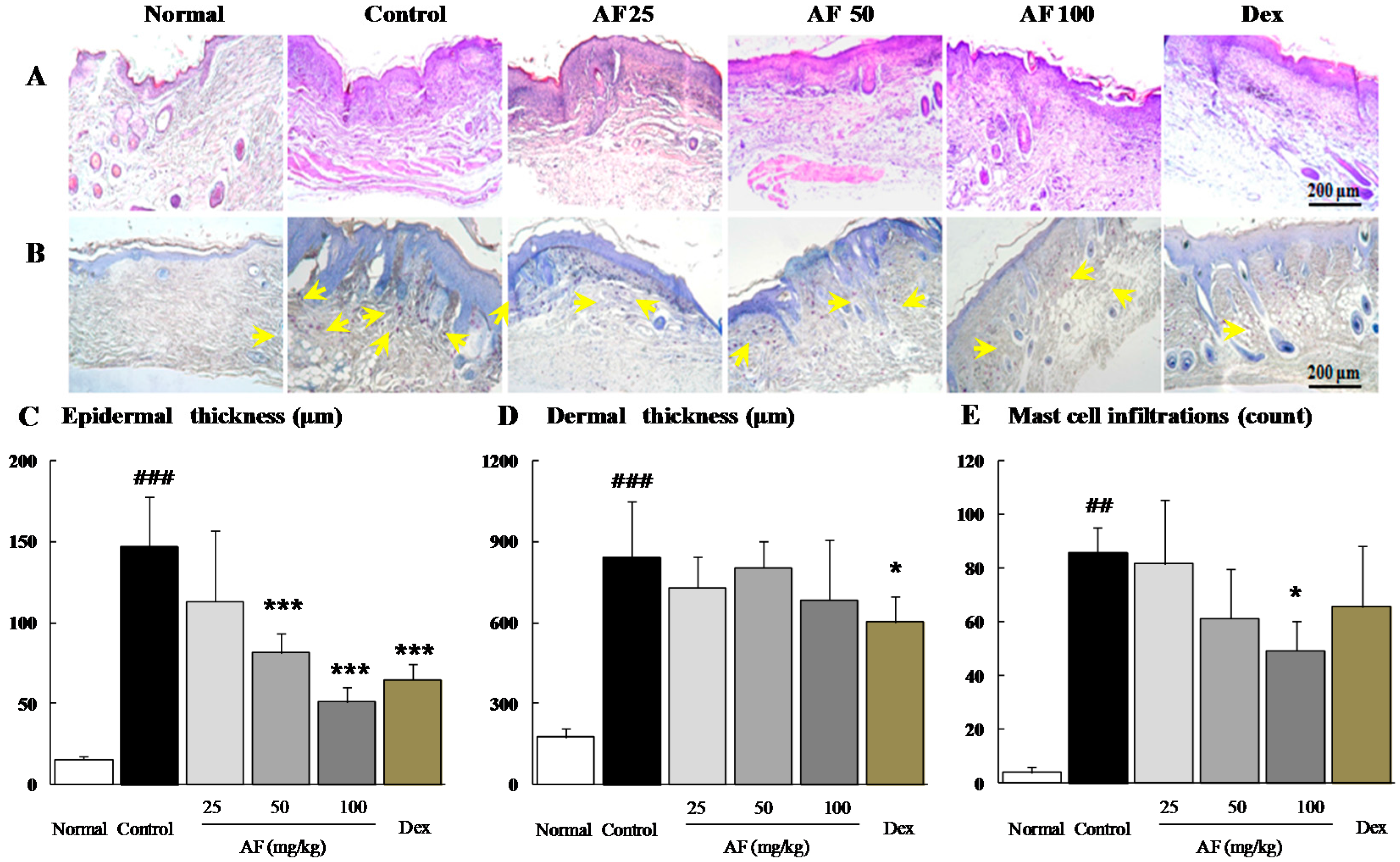
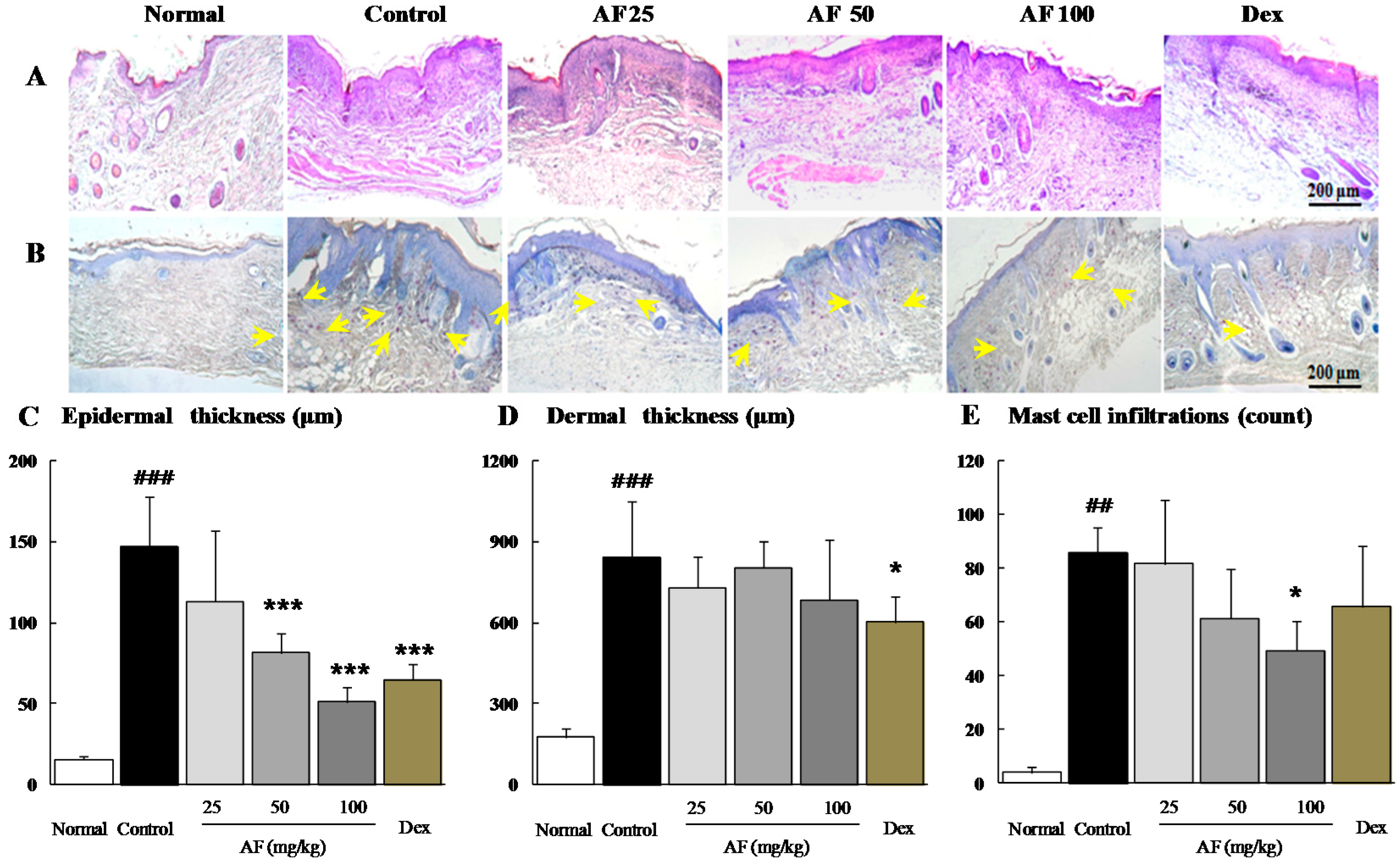
2.2. Effects on the Histopathological Analysis
2.3. Effects on the Peripheral Blood Cell Populations

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categories | Normal | Control | Atofreellage (200 μL/Head) | Dexamethasone 3 mg/kg | ||
|---|---|---|---|---|---|---|
| 25 mg/mL | 50 mg/mL | 100 mg/mL | ||||
| WBC (k/μL) | 2.34 ± 0.65 | 3.51 ± 0.75 # | 3.58 ± 1.04 | 2.75 ± 0.62 | 2.94 ± 0.61 | 2.80 ± 0.16 |
| Lymphocyte (k/μL) | 1.68 ± 0.31 | 1.97 ± 0.57 | 2.19 ± 0.44 | 1.83 ± 0.35 | 2.21 ± 0.42 | 2.1 ± 0.22 |
| Monocyte (k/μL) | 0.06 ± 0.01 | 0.07 ± 0.02 | 0.07 ± 0.02 | 0.07 ± 0.01 | 0.06 ± 0.02 | 0.07 ± 0.01 |
| Neutrophil (k/μL) | 0.59 ± 0.11 | 1.33 ± 0.20 ## | 1.18 ± 0.15 | 0.78 ± 0.24 | 0.59 ± 0.16 * | 0.56 ± 0.13 * |
| Eosinophil (k/μL) | 0.01 ± 0.01 | 0.12 ± 0.03 ### | 0.08 ± 0.06 | 0.08 ± 0.06 | 0.08 ± 0.03 * | 0.04 ± 0.04 ** |
| Basophil (k/μL) | 0.01 ± 0.00 | 0.05 ± 0.01 ## | 0.03 ± 0.02 * | 0.03 ± 0.02 ** | 0.02 ± 0.02 ** | 0.02 ± 0.02 ** |
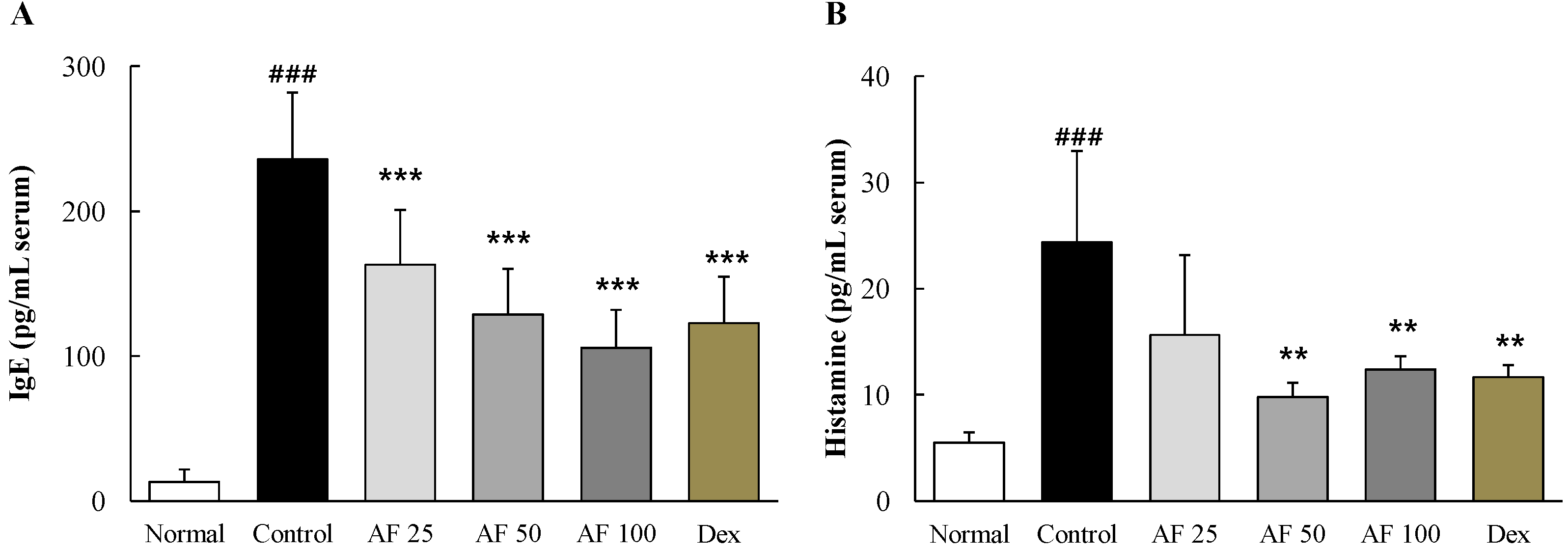
2.4. Effects on Serum IgE and Histamine
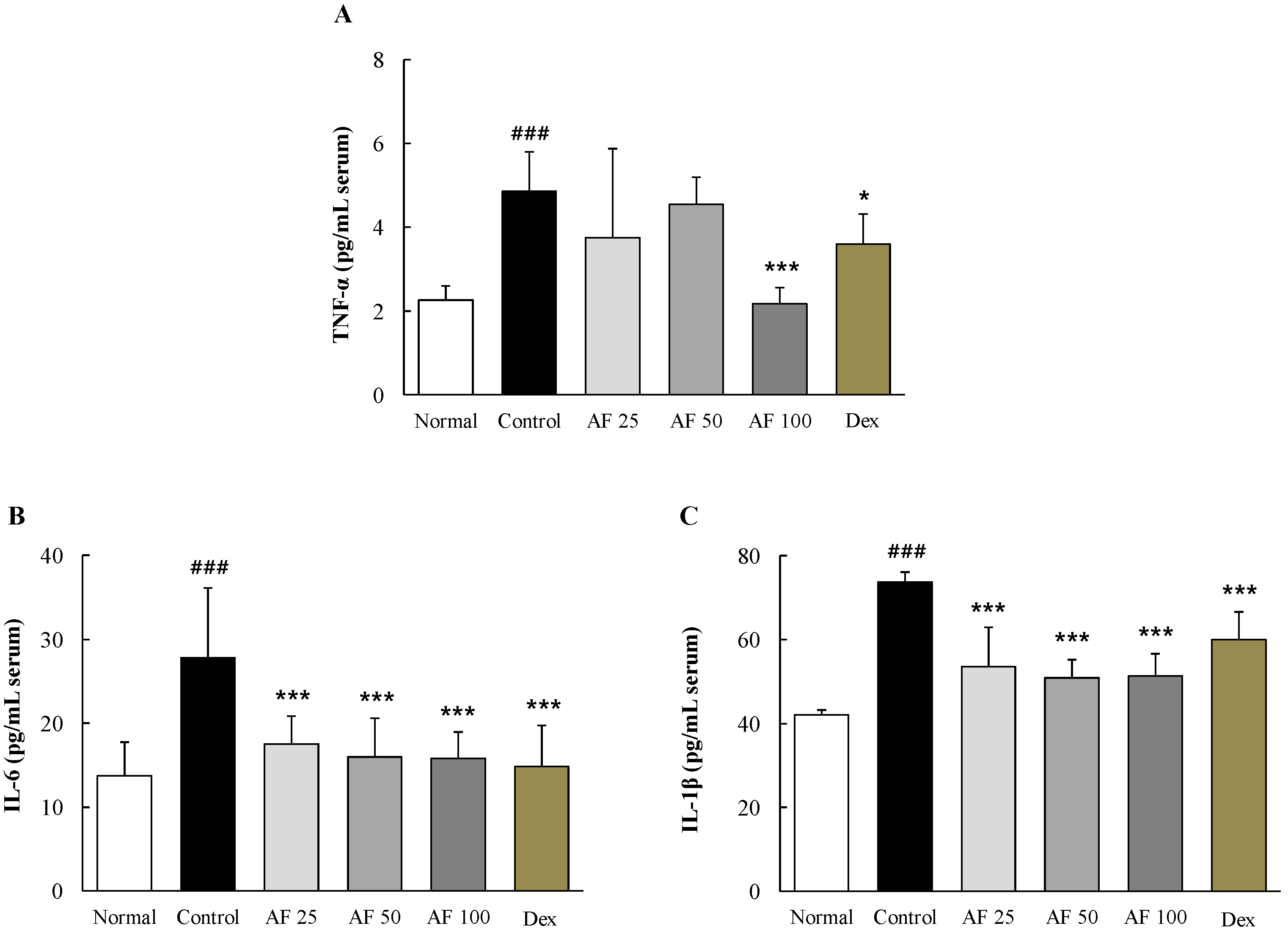
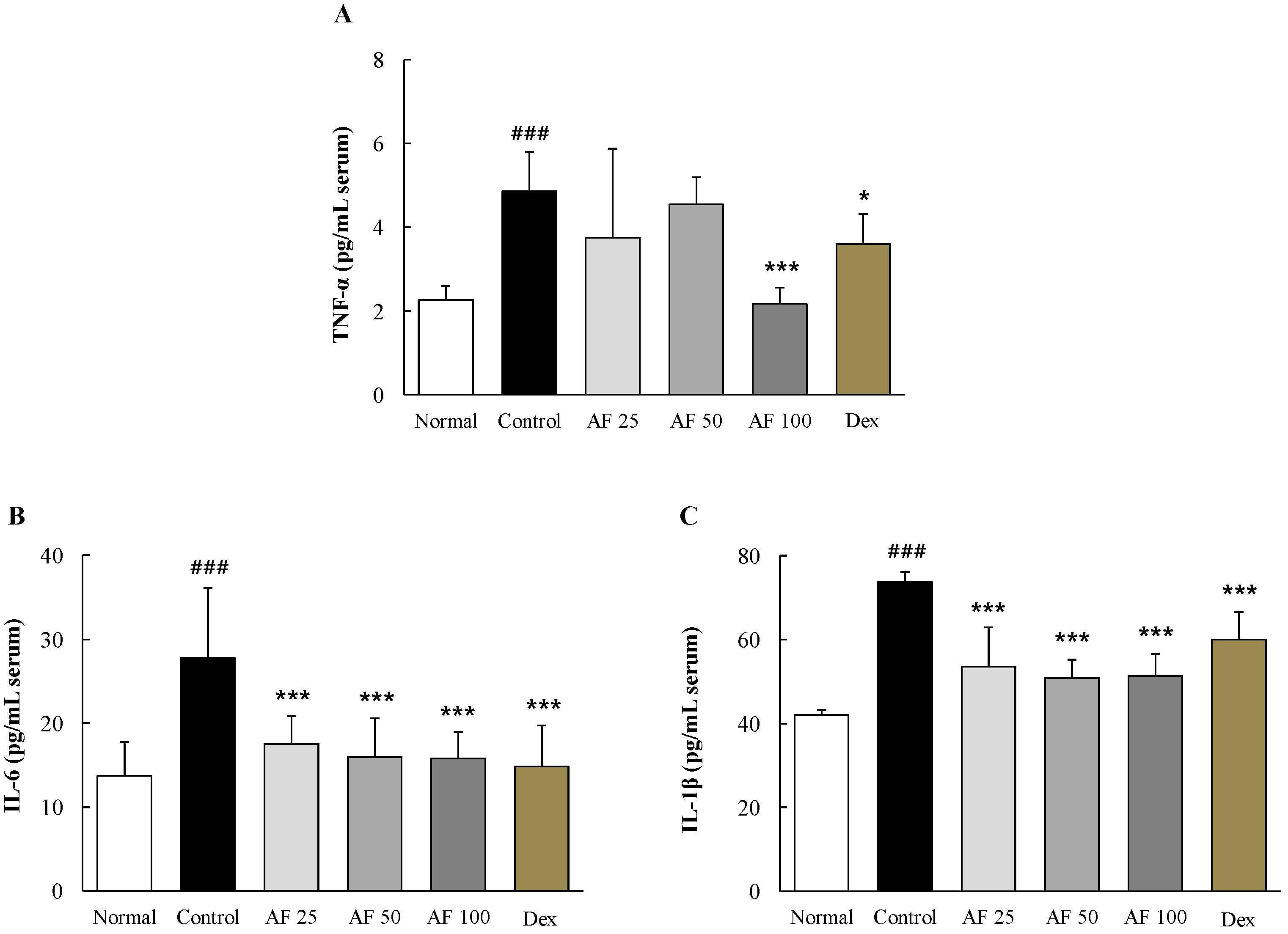
2.5. Effects on Serum Pro-Inflammatory Cytokines
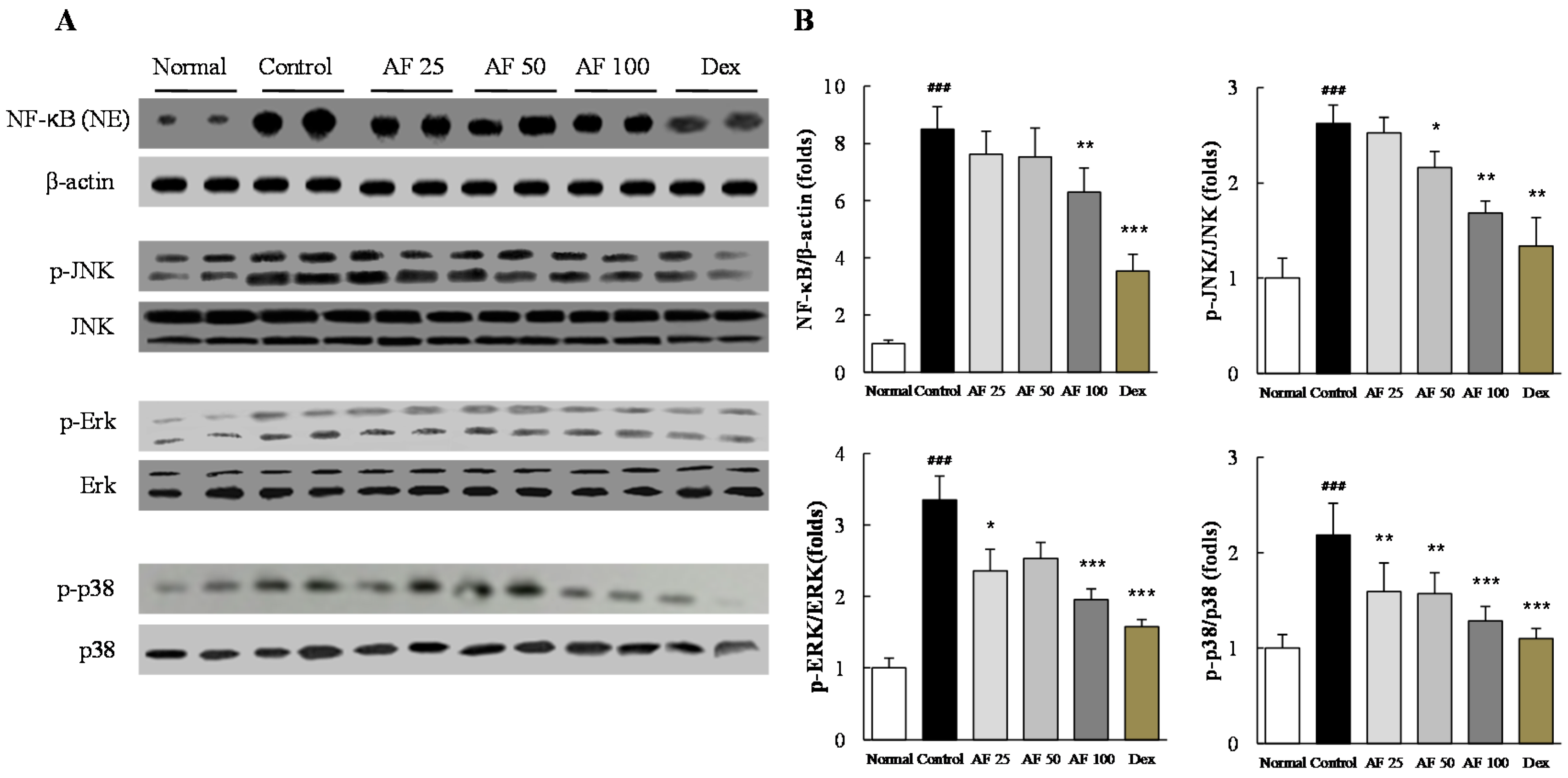
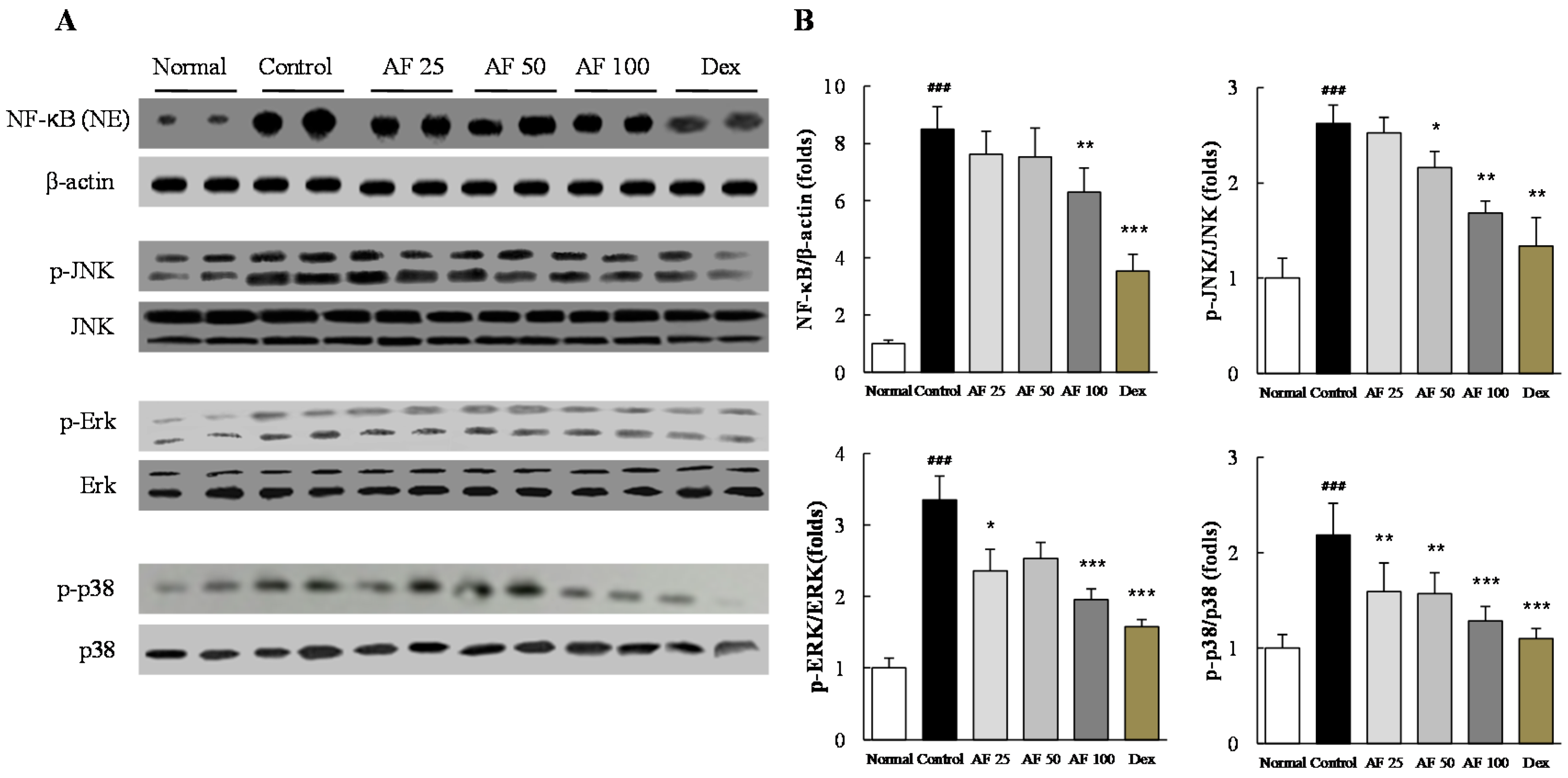
2.6. Effects on Inflammatory Signaling Pathways
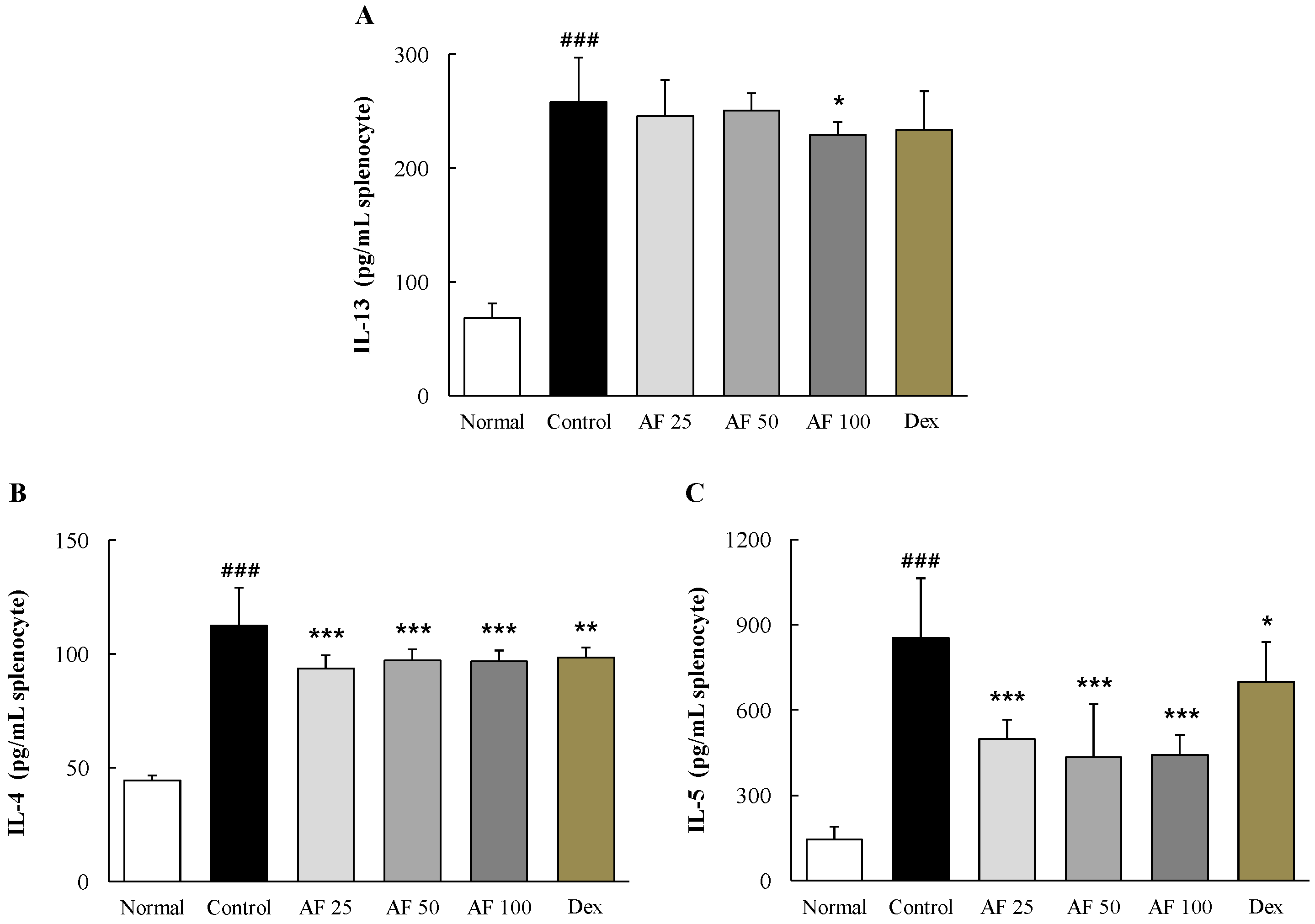
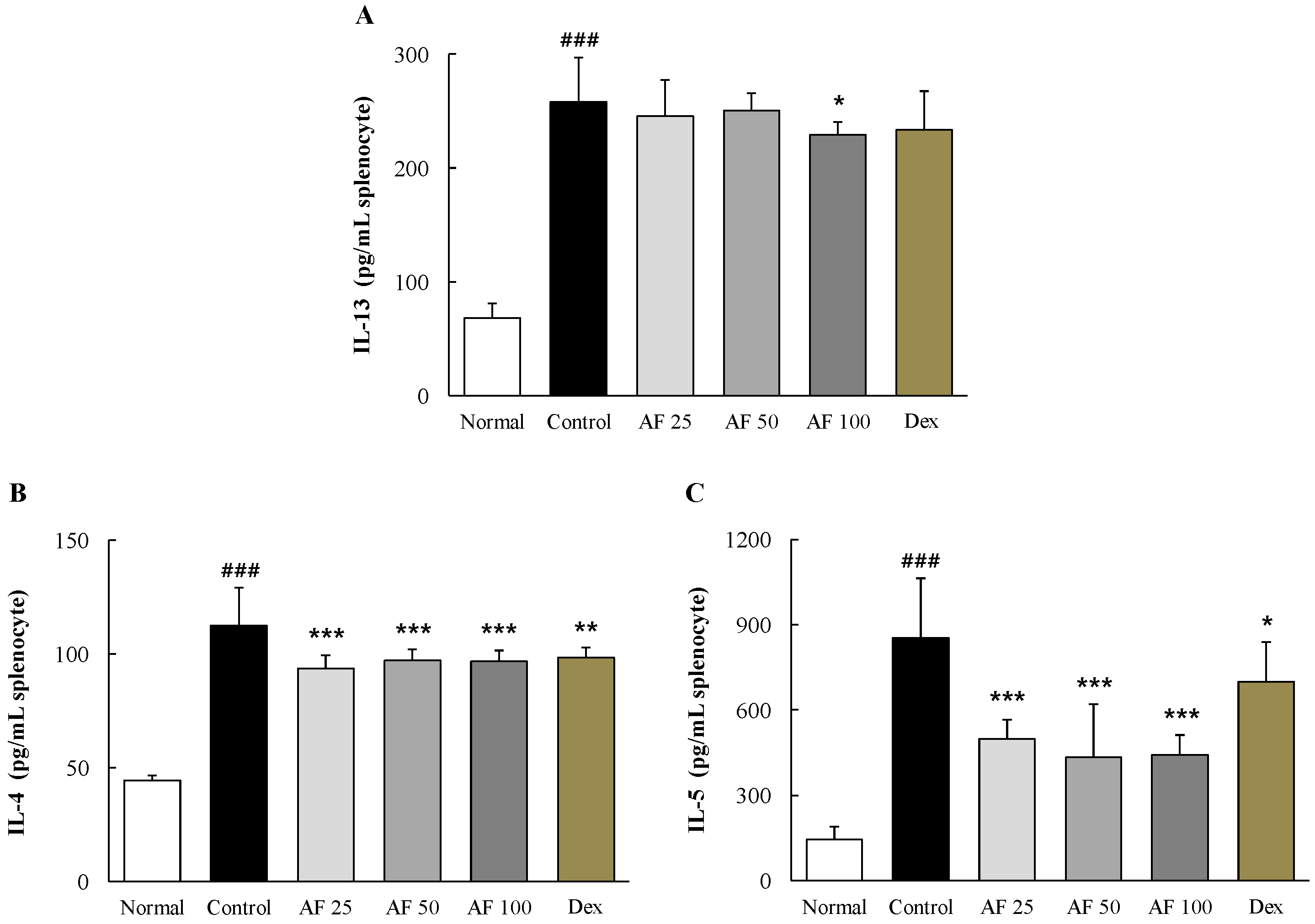
2.7. Effects on Th2 Cell-Related Cytokines in Primary Cultures of Splenocytes
3. Discussion
4. Experimental Section
4.1. Chemicals
4.2. Preparations of Atofreellage and Chemical Component Analysis
4.3. Obtaining the Fingerprint of Atofreellage
4.4. Animal and Experiment Schedule
4.5. Histopathological Examination of AD-Like Skin Lesions
4.6. Analysis of Leukocytes in Peripheral Blood
4.7. Measurement of total IgE and Histamine Concentrations in Serum
4.8. Measurement of Pro-Inflammatory Cytokine Concentrations in Serum
4.9. Western Blot Analysis
4.10. Ex Vivo Experiment for the Determination of Th2 Cell-Related Cytokines
4.11. Statistical Analysis
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- DaVeiga, S.P. Epidemiology of atopic dermatitis: A review. Allergy Asthma Proc. 2012, 33, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Berke, R.; Singh, A.; Guralnick, M. Atopic dermatitis: An overview. Am. Fam. Phys. 2012, 86, 35–42. [Google Scholar]
- Levy, R.M.; Gelfand, J.M.; Yan, A.C. The epidemiology of atopic dermatitis. Clin. Dermatol. 2003, 21, 109–115. [Google Scholar] [CrossRef]
- Navi, D.; Saegusa, J.; Liu, F.T. Mast cells and immunological skin diseases. Clin. Rev. Allergy Immunol. 2007, 33, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.; Bieber, T. Atopic dermatitis. Lancet 2003, 361, 151–160. [Google Scholar] [CrossRef]
- Bantz, S.K.; Zhu, Z.; Zheng, T. The atopic March: Progression from atopic dermatitis to allergic rhinitis and asthma. J. Clin. Cell. Immunol. 2014, 5, 202. [Google Scholar] [PubMed]
- Braun-Fahrlander, C. Environmental exposure to endotoxin and other microbial products and the decreased risk of childhood atopy: Evaluating developments since April 2002. Curr. Opin. Allergy Clin. Immunol. 2003, 3, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Simpson, E.L. Atopic dermatitis: A review of topical treatment options. Curr. Med. Res. Opin. 2010, 26, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Lee, Y.B.; Lee, J.H.; Kim, H.S.; Lee, K.H.; Park, Y.M.; Cho, S.H.; Lee, J.Y. Disease awareness and management behavior of patients with atopic dermatitis: A questionnaire survey of 313 patients. Ann. Dermatol. 2015, 27, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Madan, V.; Griffiths, C.E. Systemic ciclosporin and tacrolimus in dermatology. Dermatol. Ther. 2007, 20, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Slater, N.A.; Morrell, D.S. Systemic therapy of childhood atopic dermatitis. Clin. Dermatol. 2015, 33, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Williams, H. New treatments for atopic dermatitis. BMJ 2002, 324, 1533–1534. [Google Scholar] [CrossRef] [PubMed]
- Sung, Y.Y.; Yang, W.K.; Lee, A.Y.; Kim, D.S.; Nho, K.J.; Kim, Y.S.; Kim, H.K. Topical application of an ethanol extract prepared from Illicium verum suppresses atopic dermatitis in NC/Nga mice. J. Ethnopharmacol. 2012, 144, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Choi, C.H.; Lee, K.; Lee, M.; Ham, I.; Choi, H.Y. Effects of Catalpa ovata stem bark on atopic dermatitis-like skin lesions in NC/Nga mice. J. Ethnopharmacol. 2013, 145, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Spergel, J.M.; Paller, A.S. Atopic dermatitis and the atopic march. J. Allergy Clin. Immunol. 2003, 112, S118–S127. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y. Atopic dermatitis: New insights and opportunities for therapeutic intervention. J. Allergy Clin. Immunol. 2000, 105, 860–876. [Google Scholar] [CrossRef] [PubMed]
- Akdis, C.A.; Akdis, M.; Bieber, T.; Bindslev-Jensen, C.; Boguniewicz, M.; Eigenmann, P.; Hamid, Q.; Kapp, A.; Leung, D.Y.; Lipozencic, J.; et al. Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergology and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL Consensus Report. Allergy 2006, 61, 969–987. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Lin, Y.H.; Wu, J.C.; Hu, S.; Yang, S.H.; Chen, J.L.; Chen, Y.C.; Lo, S.S. Use of traditional Chinese medicine reduces exposure to corticosteroid among atopic dermatitis children: A 1-year follow-up cohort study. J. Ethnopharmacol. 2015, 159, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Shiohara, T.; Hayakawa, J.; Mizukawa, Y. Animal models for atopic dermatitis: Are they relevant to human disease? J. Dermatol. Sci. 2004, 36, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Anton Martinez, M.C.; Leis-Dosil, V.; Alfageme-Roldan, F.; Paravisini, A.; Sanchez-Ramon, S.; Suarez Fernandez, R. Omalizumab for the treatment of atopic dermatitis. Actas DermoSifiliogr. 2012, 103, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Zhang, E.Y.; Chen, A.Y.; Zhu, B.T. Mechanism of dinitrochlorobenzene-induced dermatitis in mice: Role of specific antibodies in pathogenesis. PLoS ONE 2009, 4, e7703. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Wood, R.A.; American Academy of Pediatrics Section on Allergy and Immunology. Allergy testing in childhood: Using allergen-specific IgE tests. Pediatrics 2012, 129, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Theoharides, T.C.; Alysandratos, K.D.; Angelidou, A.; Delivanis, D.A.; Sismanopoulos, N.; Zhang, B.; Asadi, S.; Vasiadi, M.; Weng, Z.; Miniati, A.; et al. Mast cells and inflammation. Biochim. Biophys. Acta 2012, 1822, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.J.; Loehle, J.A.; Griffin, A.R.; Doll, M.A.; Kearns, G.L.; Sullivan, J.E.; Hein, D.W. Association of the histamine N-methyltransferase C314T (Thr105Ile) polymorphism with atopic dermatitis in Caucasian children. Pharmacotherapy 2008, 28, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- Stone, K.D.; Prussin, C.; Metcalfe, D.D. IgE, mast cells, basophils, and eosinophils. J. Allergy Clin. Immunol. 2010, 125 (Suppl. S2), S73–S80. [Google Scholar] [CrossRef] [PubMed]
- Hebert, A.A.; Koo, J.; Fowler, J.; Berman, B.; Rosenberg, C.; Levitt, J. Desoximetasone 0.25% and tacrolimus 0.1% ointments versus tacrolimus alone in the treatment of atopic dermatitis. Cutis 2006, 78, 357–363. [Google Scholar] [PubMed]
- Lewis, D.B. Allergy immunotherapy and inhibition of Th2 immune responses: A sufficient strategy? Curr. Opin. Immunol. 2002, 14, 644–651. [Google Scholar] [CrossRef]
- Nakamura, A.; Osonoi, T.; Terauchi, Y. Relationship between urinary sodium excretion and pioglitazone-induced edema. J. Diabetes Investig. 2010, 1, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Foroughi, S.; Foster, B.; Kim, N.; Bernardino, L.B.; Scott, L.M.; Hamilton, R.G.; Metcalfe, D.D.; Mannon, P.J.; Prussin, C. Anti-IgE treatment of eosinophil-associated gastrointestinal disorders. J. Allergy Clin. Immunol. 2007, 120, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Shirakawa, I.; Deichmann, K.A.; Izuhara, I.; Mao, I.; Adra, C.N.; Hopkin, J.M. Atopy and asthma: Genetic variants of IL-4 and IL-13 signalling. Immunol. Today 2000, 21, 60–64. [Google Scholar] [CrossRef]
- Wong, C.K.; Ho, C.Y.; Ko, F.W.; Chan, C.H.; Ho, A.S.; Hui, D.S.; Lam, C.W. Proinflammatory cytokines (IL-17, IL-6, IL-18 and IL-12) and Th cytokines (IFN-gamma, IL-4, IL-10 and IL-13) in patients with allergic asthma. Clin. Exp. Immunol. 2001, 125, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, H.; Tomohiro, N.; Ido, Y.; Kubo, M. Anti-allergic effects of cnidii monnieri fructus (dried fruits of Cnidium monnieri) and its major component, osthol. Biol. Pharm. Bull. 2002, 25, 809–812. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kim, I.S.; Kim, J.H.; Kim, J.S.; Kim, D.H.; Yun, C.Y. Suppressive effects of Houttuynia cordata Thunb (Saururaceae) extract on Th2 immune response. J. Ethnopharmacol. 2008, 117, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.K.; Fuseda, K.; Shibata, T.; Tanaka, H.; Inagaki, N.; Nagai, H. Kampo medicines for mite antigen-induced allergic dermatitis in NC/Nga mice. Evid. Based Complement. Altern. Med. 2005, 2, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.N.; Kim, M.Y.; Choi, C.H.; Kim, B.J.; Kim, K.Y.; Kim, G.Y.; Jeong, H.W.; Kim, H.W. Effect of lithospermi radix on contact dermatitis induced by dinitrofluorobenzene in mice. J. Pharmacopunct. 2012, 15, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.K.; Son, H.U.; Kim, J.M.; Heo, J.C.; Lee, S.H.; Kim, J.G. Cinnamomum cassia bark produced by solid-state fermentation with Phellinus baumii has the potential to alleviate atopic dermatitis-related symptoms. Int. J. Mol. Med. 2015, 35, 187–194. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zuckerman, G.B.; Bielory, L. Complementary and alternative medicine herbal therapies for atopic disorders. Am. J. Med. 2002, 113 (Suppl. S9A), S47–S51. [Google Scholar] [CrossRef]
- Kim, S.H.; Jun, C.D.; Suk, K.; Choi, B.J.; Lim, H.; Park, S.; Lee, S.H.; Shin, H.Y.; Kim, D.K.; Shin, T.Y. Gallic acid inhibits histamine release and pro-inflammatory cytokine production in mast cells. Toxicol. Sci. 2006, 91, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.Y.; Hu, S.; Chan, B.C.; Wat, E.C.; Lau, C.B.; Hon, K.L.; Fung, K.P.; Leung, P.C.; Hui, P.C.; Lam, C.W.; et al. Anti-inflammatory and anti-allergic activities of Pentaherb formula, Moutan Cortex (Danpi) and gallic acid. Molecules 2013, 18, 2483–2500. [Google Scholar] [CrossRef] [PubMed]
- Hossen, M.A.; Inoue, T.; Shinmei, Y.; Minami, K.; Fujii, Y.; Kamei, C. Caffeic acid inhibits compound 48/80-induced allergic symptoms in mice. Biol. Pharm. Bull. 2006, 29, 64–66. [Google Scholar] [CrossRef] [PubMed]
- Ha, H.; Lee, H.; Seo, C.S.; Lim, H.S.; Lee, J.K.; Lee, M.Y.; Shin, H. Artemisia capillaris inhibits atopic dermatitis-like skin lesions in Dermatophagoides farinae-sensitized Nc/Nga mice. BMC Complement. Altern. Med. 2014, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Programme on Traditional Medicine. In General Guidelines for Methodologies on Research and Evaluation of Traditional Medicine; World Health Organization: Geneva, Switzerland, 2000; p. 71. [Google Scholar]
- Kim, H.U.; Ryu, J.Y.; Lee, J.O.; Lee, S.Y. A systems approach to traditional oriental medicine. Nat. Biotechnol. 2015, 33, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Sample Availability: Samples of the compounds (gallic acid, caffeic acid, and hyperoside) are available from the authors.
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, W.-Y.; Kim, H.-G.; Lee, H.-W.; Lee, J.-S.; Im, H.-J.; Kim, H.-S.; Lee, S.-B.; Son, C.-G. A Herbal Formula, Atofreellage, Ameliorates Atopic Dermatitis-Like Skin Lesions in an NC/Nga Mouse Model. Molecules 2016, 21, 35. https://doi.org/10.3390/molecules21010035
Kim W-Y, Kim H-G, Lee H-W, Lee J-S, Im H-J, Kim H-S, Lee S-B, Son C-G. A Herbal Formula, Atofreellage, Ameliorates Atopic Dermatitis-Like Skin Lesions in an NC/Nga Mouse Model. Molecules. 2016; 21(1):35. https://doi.org/10.3390/molecules21010035
Chicago/Turabian StyleKim, Won-Yong, Hyeong-Geug Kim, Hye-Won Lee, Jin-Seok Lee, Hwi-Jin Im, Hyo-Seon Kim, Sung-Bae Lee, and Chang-Gue Son. 2016. "A Herbal Formula, Atofreellage, Ameliorates Atopic Dermatitis-Like Skin Lesions in an NC/Nga Mouse Model" Molecules 21, no. 1: 35. https://doi.org/10.3390/molecules21010035
APA StyleKim, W.-Y., Kim, H.-G., Lee, H.-W., Lee, J.-S., Im, H.-J., Kim, H.-S., Lee, S.-B., & Son, C.-G. (2016). A Herbal Formula, Atofreellage, Ameliorates Atopic Dermatitis-Like Skin Lesions in an NC/Nga Mouse Model. Molecules, 21(1), 35. https://doi.org/10.3390/molecules21010035