Selenium in Oncology: From Chemistry to Clinics †



{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Historical Perspective
3. Biochemistry and Pathobiochemistry of Selenium
3.1. In Vitro Cytoprotection by Selenium
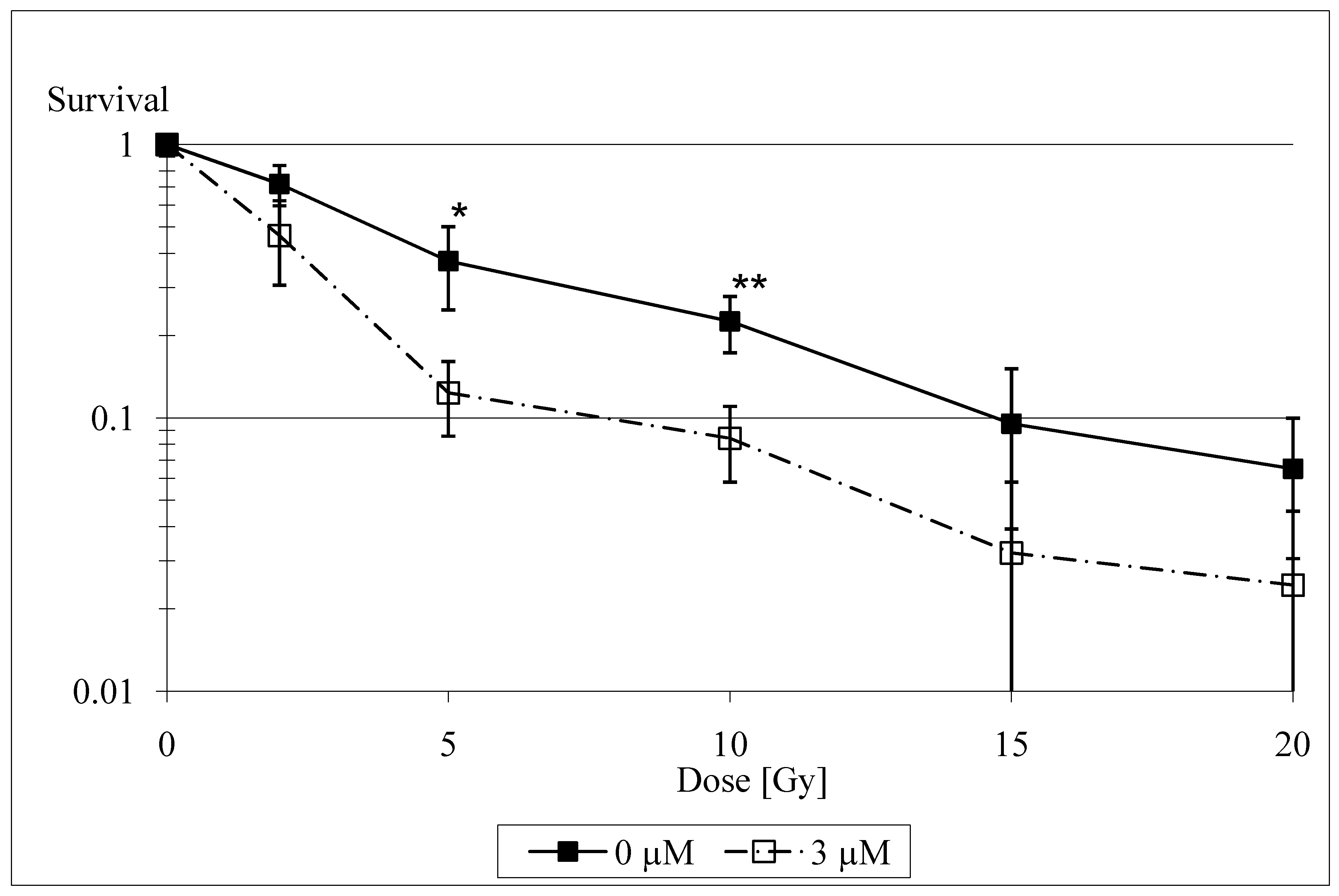
3.2. In Vitro Radiosensitization by Selenium
4. Clinical Studies on Selenium
4.1. Clinical Studies on Cytoprotection by Selenium
4.2. Antiedematous Effect of Selenium
4.3. Selenium in Cancer Prevention
5. Conclusions
References
- Büntzel, J.; Kisters, K.; Micke, O.; Mücke, R. (Eds.) Zytoprotektion, Spurenelemente und Elektrolyte in der Tumortherapie; Dustri-Verlag: München-Deisenhofen, Germany, 2004. [Google Scholar]
- Wassermann, A.V.; Keysser, F.; Wassermann, M. Beiträge zum Problem: Geschwülste von der Blutbahn aus therapeutisch zu beeinflussen. Dtsch. Med. Wschr. 1911, 37, 2389–2391. [Google Scholar] [CrossRef]
- Schrauzer, G.N. Selen: Neue Entwicklungen aus Biologie, Biochemie und Medizin, 3rd ed.; Barth: Heidelberg, Germany, 1998. [Google Scholar]
- Walker, C.H.; Klein, F. Selenium—Its therapeutic value, especially in cancer. Am. Med. J. 1915, 628–629. [Google Scholar]
- Watson-Williams, E. The treatment of inoperable cancer with selenium. Brit. J. Surg. 1920, 8, 50–58. [Google Scholar] [CrossRef]
- Weissberger, A.S.; Suhrland, L.G. Studies on analogues of L-cysteine and L-cystine. III. The effect of selenium cystine on leukemia. Blood 1956, 11, 19–30. [Google Scholar]
- Schomburg, L.; Koehrle, J. Selenium: Benefits and risks. MMW Fortschr. Med. 2007, 149, 34–36. [Google Scholar] [PubMed]
- Papp, L.V.; Lu, J.; Holmgren, A.; Khanna, K.K. From selenium to selenoproteins: Synthesis, identity, and their role in human health. Antioxid. Redox Signal. 2007, 9, 775–806. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Hill, K.E.; Byrne, D.W.; Xu, J.; Burk, R.F. Effectiveness of selenium supplements in a low-selenium area of China. Am. J. Clin. Nutr. 2005, 8, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Schomburg, L.; Schweizer, U. Hierarchical regulation of selenoprotein expression and sex-specific effects of selenium. Biochim. Biophys. Acta 2009. [Google Scholar] [CrossRef] [PubMed]
- Burk, R.F.; Hill, K.E.; Motley, A.K. Plasma selenium in specific and non-specific forms. Biofactors 2001, 14, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Combs, G.F., Jr. Selenium in global food systems. Br. J. Nutr. 2001, 85, 517–547. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. The importance of selenium to human health. Lancet 2000, 356, 233–241. [Google Scholar] [CrossRef]
- Weiss, J.F.; Landauer, M.R. History and development of radiation-protective agents. Int. J. Radiat. Biol. 2009, 85, 539–573. [Google Scholar] [CrossRef] [PubMed]
- Patchen, M.L.; MacVittie, T.J.; Weiss, J.F. Combined modality radioprotection: The use of glucan and selenium with WR-2721. Int. J. Radiat. Oncol. Biol. Phys. 1990, 18, 1069–1075. [Google Scholar] [CrossRef]
- Arthur, J.R. The glutathione peroxidases. Cell. Mol. Life Sci. 2000, 57, 1825–1835. [Google Scholar] [CrossRef] [PubMed]
- Epp, O.; Ladenstein, R.; Wendel, A. The refined structure of the selenoenzyme glutathione peroxidase at 0.2 nm resolution. Eur. J. Biochem. 1983, 133, 51–69. [Google Scholar] [CrossRef] [PubMed]
- Zhung, W.; Yan, T.; Lim, R.; Oberley, L.W. Expression of superoxide dismutases, catalase, and glutathione peroxidase in glioma cells. Free Radic. Biol. Med. 1999, 27, 1334–1345. [Google Scholar] [CrossRef]
- Mutlu-Türkoglu, Ü.; Erbil, Y; Öztezcan, S.; Olgac, V.; Toker, G.; Uysal, M. The effect of selenium and/or vitamin E treatments on radiation-induced intestinal injury in rats. Life Sciences 2000, 66, 1905–1913. [Google Scholar] [CrossRef]
- Hehr, T.; Bamberg, M.; Rodemann, H.P. Präklinische und klinische Relevanz der radiopro-tektiven Wirkung von Natriumselenit. InFoOnkologie 1999, 2 (Suppl. 2), 25–29. [Google Scholar]
- Schleicher, U.M.; Lopez Cotarelo, C.; Andreopoulos, D.; Handt, S.; Ammon, J. Radioprotection of human endothelial cells by sodium selenite. Med. Klin. (Munich) 1999, 94 (Suppl. 3), 35–38. [Google Scholar] [CrossRef]
- Gehrisch, A.; Dörr, W. Effects of systemic or topical administration of sodium selenite on early radiation effects in mouse oral mucosa. Strahlenther. Onkol. 2007, 183, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Margulies, B.S.; Damron, T.A.; Allen, M.J. The differential effects of the radioprotectant drugs amifostine and sodium selenite treatment in combination with radiation therapy on constituent bone cells, Ewing’s sarcoma of bone tumor cells, and rhabdomyosarcoma tumor cells in vitro. J. Orthop. Res. 2008, 26, 1512–1519. [Google Scholar] [CrossRef] [PubMed]
- Stewart, M.S.; Spallholz, J.E.; Neldner, K.H.; Pence, B.C. Selenium compounds have disparate abilities to impose oxidative stress and include apoptosis. Free Radic. Biol. Med. 1999, 26, 42–48. [Google Scholar] [CrossRef]
- Spallholz, J.E. On the nature of selenium toxicity and carcinostatic activity. Free Radic. Biol. Med. 1994, 17, 45–64. [Google Scholar] [CrossRef]
- Lanfear, J.; Fleming, J.; Wu, L.; Webster, G.; Harrisson, P.R. The selenium metabolite selenoglutathione induces p53 and apoptosis: Relevance to the chemoprotective effects of selenium? Carcinogenesis 1994, 15, 1387–1392. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.L.; Spallholz, J.E. Inhibition of selenite-catalyzed superoxide generation and formation of elemental selenium (Se0) by copper, zinc, and aurintricarboxylic acid (ATA). Biochem. Pharmacol. 1996, 51, 1015–1020. [Google Scholar] [CrossRef]
- Lu, J.X.; Kaeck, M.; Jiang, C.; Wilson, A.C.; Thompson, H.J. Selenite induction of DNA strand breaks and apoptosis in mouse leukemic L1210 cells. Biochem. Pharmacol. 1994, 47, 1531–1535. [Google Scholar] [CrossRef]
- Frisk, P.; Saetre, A.; Couze, B.; Stenerlöw, B.; Carlsson, J.; Lindh, U. Effects of Pb2+, Ni2+, Hg2+ and Se4+ on cultured cells. Analysis of uptake, toxicity and influence on radiosensitivity. BioMetals 1997, 10, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Schüller, P.; Püttmann, S.; Micke, O.; Senner, V.; Schäfer, U.; Willich, N. Selenium—A novel radiosensitizer? Trace Elem. Electrolytes 2005, 22, 201–206. [Google Scholar] [CrossRef]
- Rodemann, H.P.; Hehr, T.; Bamberg, M. Relevance of the radioprotective effect of sodium selenite. Med. Klin. (Munich) 1999, 94 (Suppl. 3), 39–41. [Google Scholar] [CrossRef]
- Schüller, P.; Püttmann, S.; Micke, O.; Senner, V.; Schäfer, U.; Willich, N. Selenium influences the radiation sensitivity of C6 rat glioma cells. Anticancer Res. 2004, 24, 2913–2917. [Google Scholar]
- Dörr, W. Effects of selenium on radiation responses of tumor cells and tissue. Strahlenther. Onkol. 2006, 182, 693–695. [Google Scholar] [CrossRef] [PubMed]
- Büntzel, J.; Glatzel, M.; Bruns, F.; Kisters, K.; Micke, O.; Mücke, R. Selenium supplementation in head and neck surgery. Trace Elem. Electrolytes 2008, 25, 221. [Google Scholar]
- Micke, O.; Büntzel, J.; Bruns, F.; Glatzel, M.; Hunger, R.; Kisters, K.; Mücke, R. Clinical elementology in oncology: Experiences and proposals from Germany. Trace Elem. Electrolytes 2008, 25, 221. [Google Scholar]
- Last, K.W.; Cornelius, V.; Delves, T.; Sieniawska, C.H.; Fitzgibbon, J.; Norton, A.; Amess, J.; Wilson, A.; Rohatiner, A.; Lister, A.T. Presentation serum selenium predicts for overall survival, dose delivery, and first treatment response in aggressive non-Hodgkin´s lymphoma. J. Clin. Oncol. 2003, 21, 2335–2341. [Google Scholar] [CrossRef] [PubMed]
- Last, K.; Maharaj, L.; Perry, J.; Strauss, S.; Fitzgibbon, J.; Lister, T.A.; Joel, S. The activity of methylated and non-methylated selenium species in lymphoma cell lines and primary tumours. Ann. Oncol. 2006, 17, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Fraunholz, I.; Eberlein, K.; Schopohl, B.; Böttcher, H.D.; Rödel, C. Selenium levels during the course of radiotherapy. No influence of irradiation on blood selenium concentration. Strahlenther. Onkol. 2008, 184, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Büntzel, J.; Mücke, R.; Micke, O. Mineral status and enzymatic antioxidative capacities during radiochemotherapy in patients with advanced head and neck cancer. Trace Elem. Electrolytes 2000, 18, 98. [Google Scholar]
- Micke, O.; Bruns, F.; Mücke, R.; Schäfer, U.; Glatzel, M.; DeVries, A.F.; Schönekaes, K.; Kisters, K.; Büntzel, J. Selenium in the treatment of radiation-associated secondary lymphedema. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 40–49. [Google Scholar] [CrossRef]
- Mücke, R.; Büntzel, J.; Glatzel, M.; Bruns, F.; Kisters, K.; Prott, F.J.; Schmidberger, H.; Micke, O. Postoperative serum and whole blood selenium levels in patients with squamous cell and adenocarcinomas of the uterus after curative surgical treatment. Trace Elem. Electrolytes 2009, 26, 78–82. [Google Scholar] [CrossRef]
- Mücke, R.; Glatzel, M.; Bernd-Skorka, R.; Baaske, D.; Reichl, B.; Büntzel, J.; Kundt, G.; Prott, F.J.; de Vries, A.; Micke, O. Multicenter, phase-III study comparing selenium supplementation with observation in gynecologic radiation oncology. J. Clin. Oncol. 2008, 26, Number15S, [Abstr. 9539]. [Google Scholar] [CrossRef]
- Bruns, F.; Büntzel, J.; Mücke, R.; Schönekaes, K.; Kisters, K.; Micke, O. Selenium in the treatment of head and neck lymphedema. Med. Princ. Pract. 2004, 13, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Kasseroller, R. Sodium selenite as prophylaxis against erysipelas in secondary lymphedema. Anticancer Res. 1998, 18, 2227–2230. [Google Scholar] [PubMed]
- Brenke, R.; Siems, W.; Grune, T. Measures for therapy optimization in chronic lymphedema. Z. Lymphol. 1997, 21, 1–29. [Google Scholar]
- Schrauzer, G.N. Selenium in the therapy of chronic lymphedema - mechanistic perspectives and practical applications. Z. Lymphol. 1997, 21, 16–19. [Google Scholar]
- Miller, S.; Walker, S.W.; Arthur, J.R.; Nicol, F.; Pickard, K.; Lewin, M.H.; Howie, A.F.; Beckett, G.J. Selenite protects human endothelial cells from oxidative damage and induces thioredoxin reductase. Clin. Sci. 2001, 100, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Shamberger, R.J.; Frost, D.V. Possible protective effect of selenium against human cancer. Can. Med. Assoc. J. 1969, 100, 682. [Google Scholar] [PubMed]
- Yu, S.Y.; Zhu, Y.J.; Li, W.G.; Huang, Q.S.; Huang, C.Z.; Zhang, Q.N.; Hou, C. A preliminary report on the intervention trials of primary liver cancer in high–risk populations with nutritional supplementation of selenium in China. Biol. Trace Elem. Res. 1991, 29, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.C.; Combs, G.F.; Turnbull, B.W.; Slate, E.H.; Chalker, D.K.; Chow, J.; Davis, L.S.; Glover, R.A.; Graham, G.F.; Gross, E.G.; Krongrad, A.; Lesher, J.L.; Park, H.K.; Sanders, B.B.; Smith, C.L.; Taylor, J.R. Effects of selenium supplementation for cancer prevention in patients with carcinoma of the skin. A randomized controlled trial. Nutritional Prevention of Cancer Study Group. JAMA 1996, 276, 1957–1963. [Google Scholar] [CrossRef] [PubMed]
- Bleys, J.; Navas-Acie, A.; Guallar, E. Serum selenium levels and all cause, cancer, and cardiovascular mortality among US adults. Arch. Intern. Med. 2008, 168, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Karita, K.; Hamada, G.S.; Tsugane, S. Comparison of selenium status between Japanese living in Tokyo and Japanese brazilians in São Paulo, Brazil. Asia Pac. J. Clin. Nutr. 2001, 10, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Rajpathak, S.; Rimm, E.; Morris, J.S.; Hu, F. Toenail selenium and cardiovascular disease in men with diabetes. J. Am. Coll. Nutr. 2005, 24, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Lippman, S.M.; Klein, E.A.; Goodman, P.J.; Lucia, M.S.; Thompson, I.M.; Ford, L.G.; Parnes, H.L.; Minasian, L.M.; Gaziano, J.M.; Hartline, J.A.; Parsons, J.K.; Bearden, J.D.; Crawford, E.D.; Goodman, G.E.; Claudio, J.; Winquist, E.; Cook, E.D.; Karp, D.D.; Walther, P.; Lieber, M.M.; Kristal, A.R.; Darke, A.K.; Arnold, K.B.; Ganz, P.A.; Santella, R.M.; Albanes, D.; Taylor, P.R.; Probstfield, J.L.; Jagpal, T.J.; Crowley, J.J.; Meyskens, F.L.; Baker, L.H.; Coltman, C.A. Effect of selenium and vitamin E on risk of prostate cancer and other cancers: The selenium and vitamin E cancer prevention trial (SELECT). JAMA 2009, 301, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Stranges, S.; Marshall, J.R.; Natarajan, R.; Donahue, R.P.; Trevisan, M.; Combs, G.F.; Cappuccio, F.P.; Ceriello, A.; Reid, M.E. Effects of long-term selenium supplementation on the incidence of type 2 diabetes: a randomized trial. Ann. Intern. Med. 2007, 147, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Gann, P.H. Randomized trials of antioxidant supplementation for cancer prevention: First bias, now chance - next, cause. JAMA 2009, 301, 102–103. [Google Scholar] [CrossRef] [PubMed]
- Moyad, M.A. Selenium and vitamin E supplements for prostate cancer: Evidence or embellishment? Urology 2002, 59, 9–19. [Google Scholar] [CrossRef]
- Drake, E.N. Cancer chemoprevention: Selenium as a prooxidant, not an antioxidant. Med. Hypotheses 2006, 67, 318–322. [Google Scholar] [CrossRef] [PubMed]
- El-Bayoumy, K. The negative results of the SELECT study do not necessarily discredit the selenium-cancer prevention hypothesis. Nutr. Cancer. 2009, 61, 285–286. [Google Scholar] [CrossRef] [PubMed]
- Schrauzer, G.N. Lessons from the selenium and vitamin E cancer prevention trial (SELECT). Crit. Rev. Biotechnol. 2009, 29, 81. [Google Scholar] [CrossRef] [PubMed]
- Hatfield, D.L.; Gladyshev, V.N. The outcome of selenium and vitamin E cancer prevention trial (SELECT) reveals the need for better understanding of selenium biology. Mol. Interv. 2009, 1, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Dennert, G.; Horneber, M. Selenium for alleviating the side effects of chemotherapy, radiotherapy and surgery in cancer patients. Cochrane Database Syst. Rev. 2006, 3, CD005037. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: Not available. |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Micke, O.; Schomburg, L.; Buentzel, J.; Kisters, K.; Muecke, R. Selenium in Oncology: From Chemistry to Clinics. Molecules 2009, 14, 3975-3988. https://doi.org/10.3390/molecules14103975
Micke O, Schomburg L, Buentzel J, Kisters K, Muecke R. Selenium in Oncology: From Chemistry to Clinics. Molecules. 2009; 14(10):3975-3988. https://doi.org/10.3390/molecules14103975
Chicago/Turabian StyleMicke, Oliver, Lutz Schomburg, Jens Buentzel, Klaus Kisters, and Ralph Muecke. 2009. "Selenium in Oncology: From Chemistry to Clinics" Molecules 14, no. 10: 3975-3988. https://doi.org/10.3390/molecules14103975
APA StyleMicke, O., Schomburg, L., Buentzel, J., Kisters, K., & Muecke, R. (2009). Selenium in Oncology: From Chemistry to Clinics. Molecules, 14(10), 3975-3988. https://doi.org/10.3390/molecules14103975