COVID-19 Vaccine Concerns about Safety, Effectiveness, and Policies in the United States, Canada, Sweden, and Italy among Unvaccinated Individuals

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Data Collection
2.2. Vaccine Hesitancy
2.3. COVID-19 Vaccine Concerns
2.4. Statistical Analysis
3. Results
3.1. Objective 1—Describe and Compare Vaccine Hesitancy Proportions by Country
3.2. Objective 2—Categorize Vaccine-Related Concerns
3.3. Objective 3—Rank Vaccine-Related Concerns
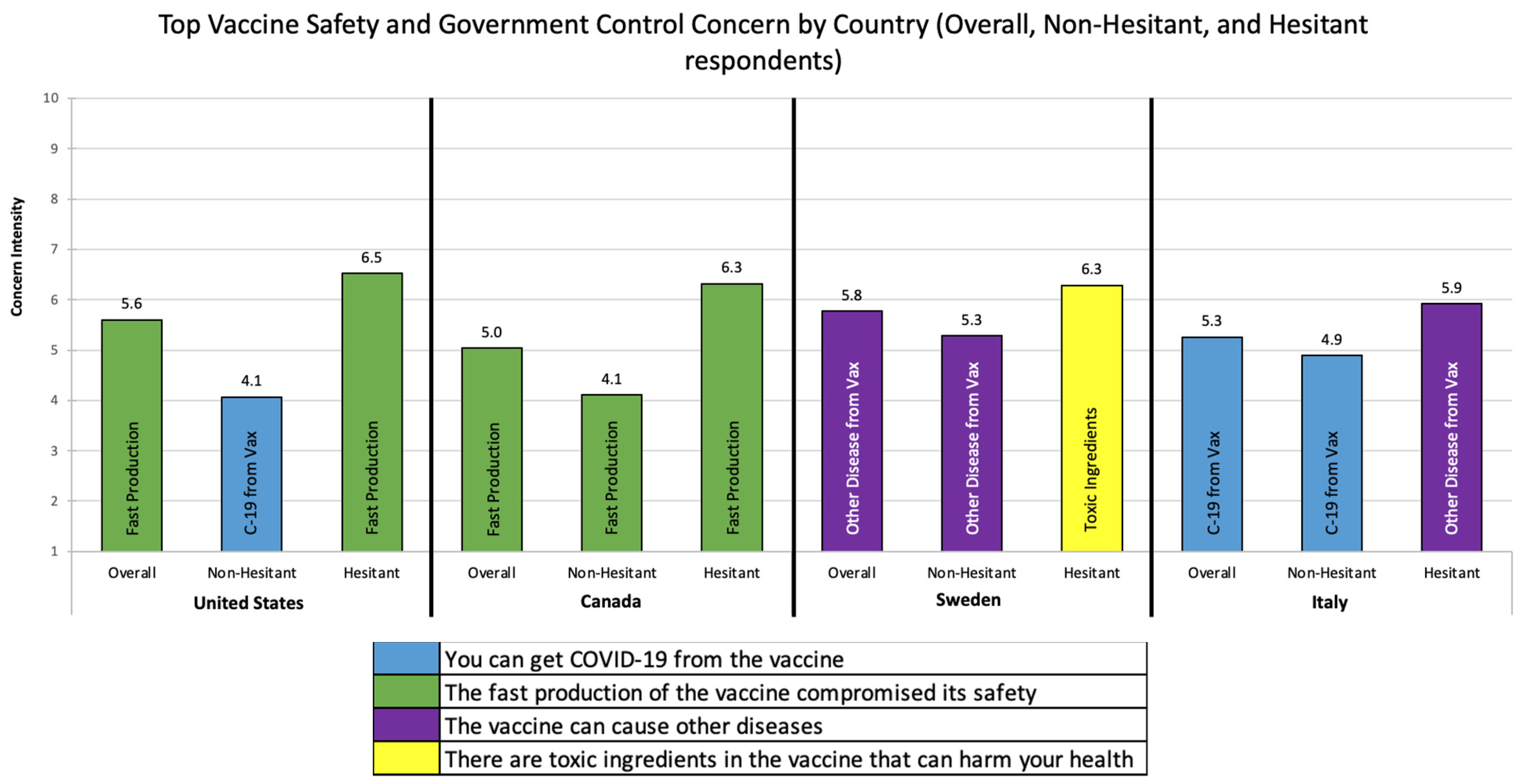
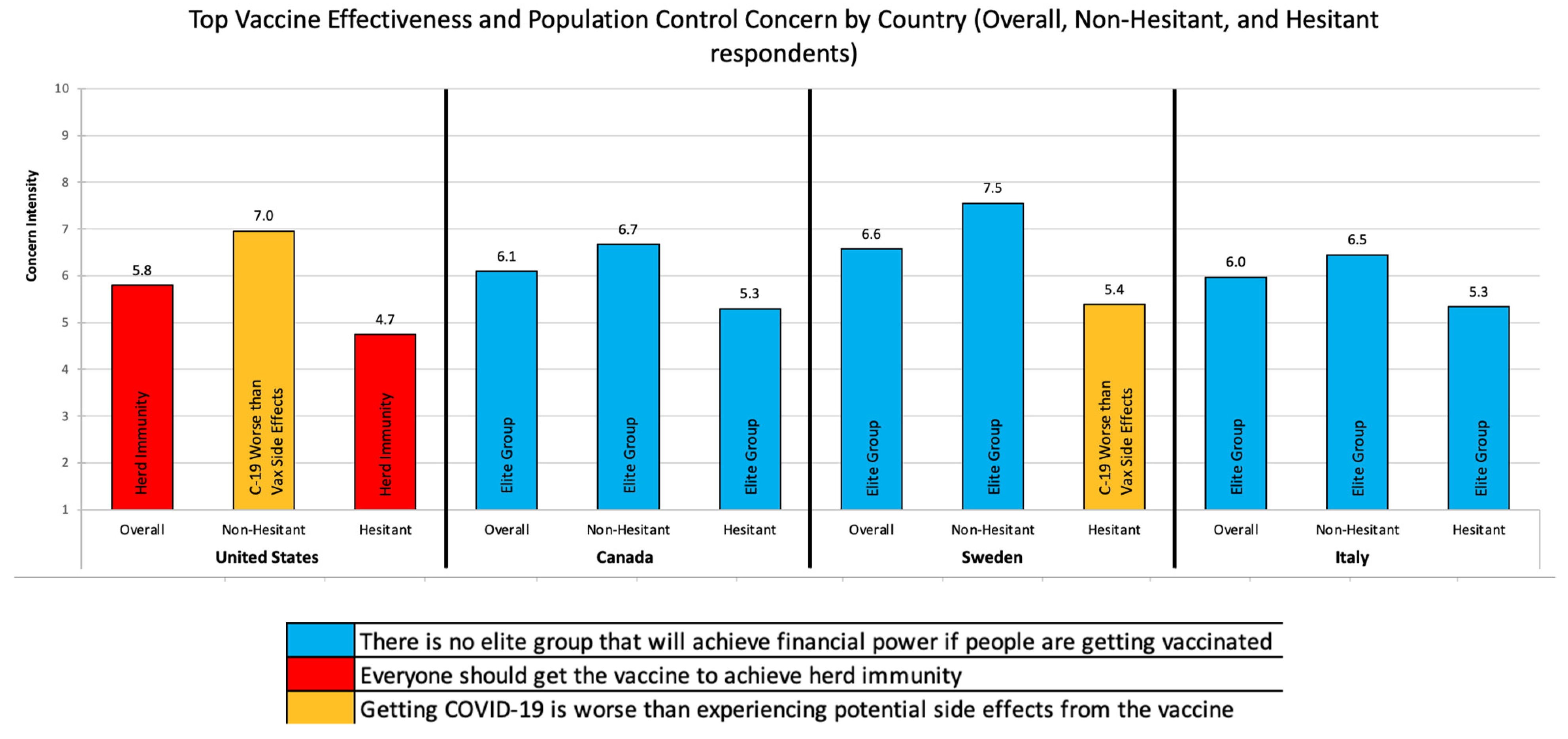
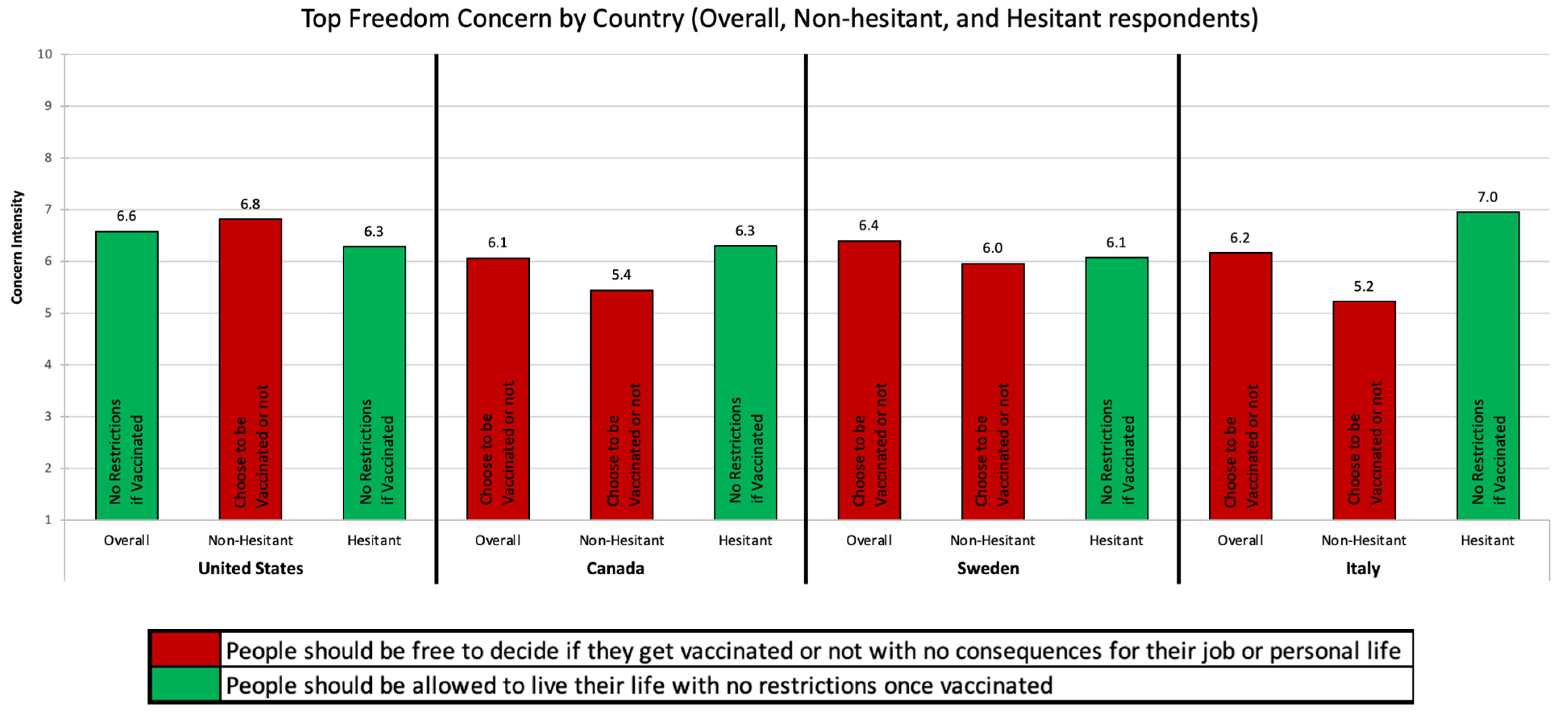
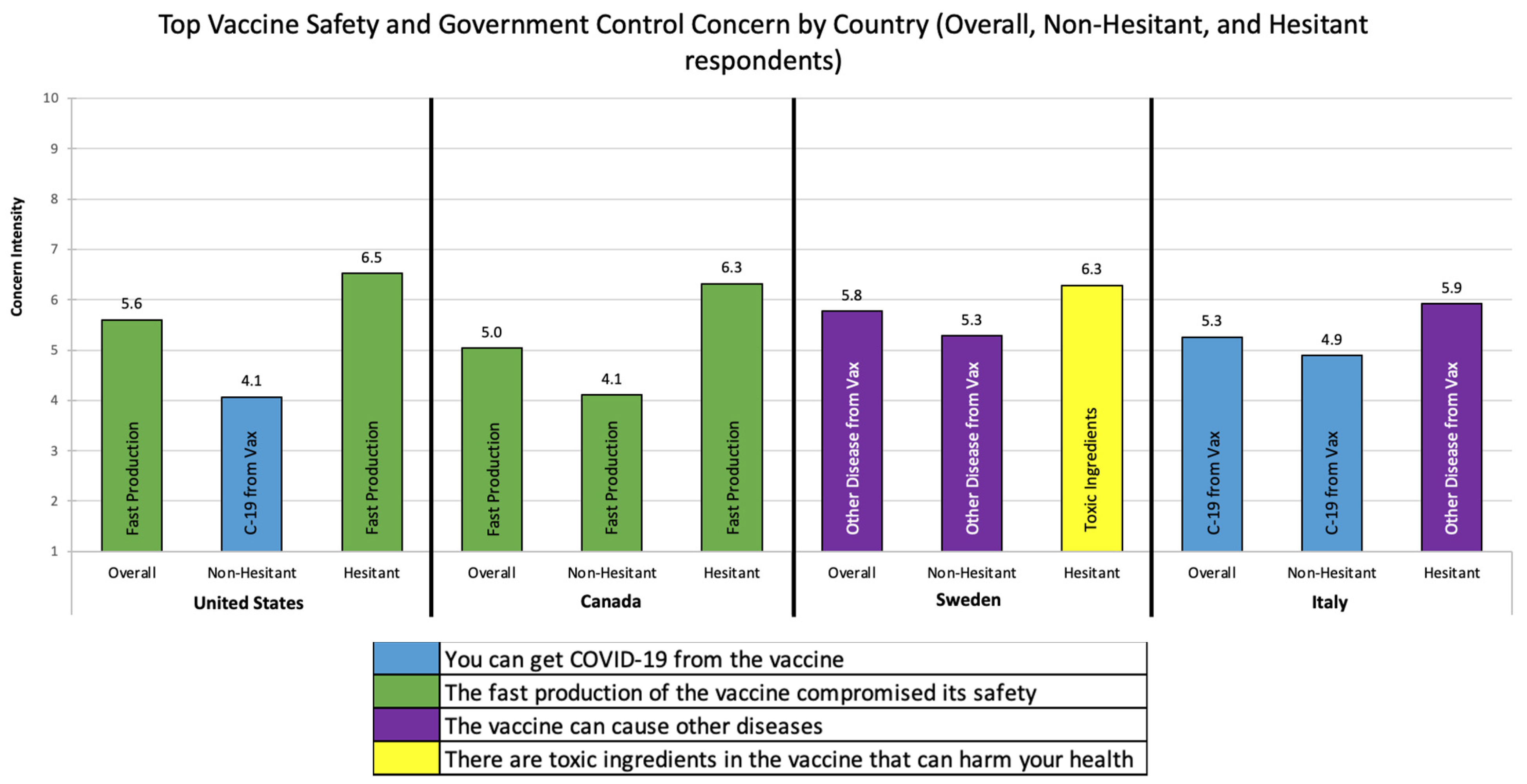
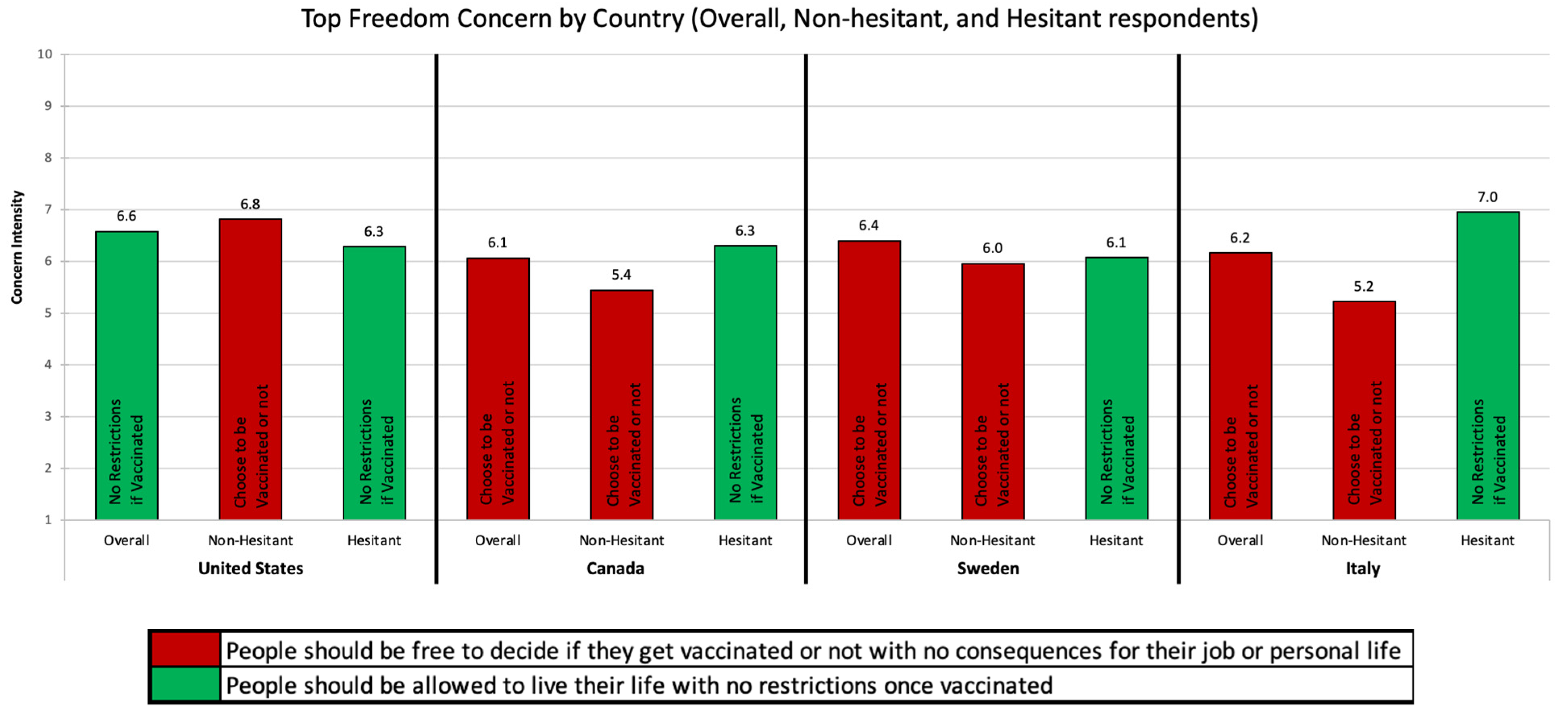
3.4. Objective 4—Vaccine Concerns by Country and Hesitancy Status
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Ten Threats to Global Health in 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Rozek, L.; Jones, P.; Menon, A.; Hicken, A.; Apsley, S.; King, E. Understanding Vaccine Hesitancy in the Context of COVID-19: The Role of Trust and Confidence in a Seventeen-Country Survey. Int. J. Public Health 2021, 66, 48. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; Rauh, L.; Rabin, K.; Ratzan, S.; Gostin, L.O.; Larson, H.J.; El-Mohandes, A. Hesitant or Not? The Association of Age, Gender, and Education with Potential Acceptance of a COVID-19 Vaccine: A Country-level Analysis. J. Health Commun. 2020, 25, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada. Coronavirus Disease (COVID-19). Available online: https://www.canada.ca/en/public-health/services/diseases/coronavirus-disease-covid-19.html (accessed on 16 August 2021).
- How CDC Is Making COVID-19 Vaccine Recommendations. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations-process.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fvaccines%2Frecommendations.html (accessed on 30 August 2021).
- Folkhalsomyndigheten-Public Health Agency of Sweden: Vaccination against COVID-19. Available online: https://www.folkhalsomyndigheten.se/the-public-health-agency-of-sweden/communicable-disease-control/covid-19/vaccination-against-covid-19/ (accessed on 16 August 2021).
- L’epidemiologia per la Sanità Pubblica-Istituto Superiore di Sanità-Piano Nazionale di Vaccinazione COVID-19. Available online: https://www.epicentro.iss.it/vaccini/covid-19-piano-vaccinazione (accessed on 10 August 2021).
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Romer, D.; Jamieson, K.H. Patterns of Media Use, Strength of Belief in COVID-19 Conspiracy Theories, and the Prevention of COVID-19 From March to July 2020 in the United States: Survey Study. J. Med. Internet Res. 2021, 23, e25215. [Google Scholar] [CrossRef] [PubMed]
- Griffith, J.; Marani, H.; Monkman, H. COVID-19 Vaccine Hesitancy in Canada: Content Analysis of Tweets Using the Theoretical Domains Framework. J. Med. Internet Res. 2021, 23, e26874. [Google Scholar] [CrossRef] [PubMed]
- Hamel, L.; Lopes, L.; Sparks, G.; Stokes, M.; Brodie, M. KFF COVID-19 Vaccine Monitor: April 2021; Kaiser Family Foundation: San Francisco, CA, USA, 2021. [Google Scholar]
- Giles-Vernick, T.; Vray, M.; Heyerdahl, L.o.; Lana, B.; Gobat, N.; Tonkin-Crine, S.; Anthierens, S. Public Views of COVID-19 Vaccination in Seven European Countries: Options for Response. RECOVER: Rapid European COVID-19 Emergency Research Response. 2021. Available online: https://www.recover-europe.eu/wp-content/uploads/2021/02/Social-science-policy-brief_Vaccination_v5.pdf (accessed on 8 September 2021).
- Pollfish. Available online: https://www.pollfish.com (accessed on 30 May 2021).
- Collis, H. Politics threaten to cloud EU countries’ pause of Oxford/AstraZeneca vaccine. POLITICO-Europe, 16 March 2021. [Google Scholar]
- Dettmer, J. EU Solidarity Breaks Down, States Complain of Unfair Vaccine Distribution. VOA—Voice of America, 22 March 2021. [Google Scholar]
- Horowitz, J.; Mueller, B. Europe’s Vaccine Suspension May Be Driven as Much by Politics as Science. The New York Times, 24 March 2021. [Google Scholar]
- McCulloch, C. Why Canada Leaped Ahead of US in COVID-19 Vaccinations. VOA—Voice of America, 31 July 2021. [Google Scholar]
- Kirzinger, A.; Sparks, G.; Hamel, L.; Lopes, L.; Kearney, A.; Stokes, M.; Brodie, M. KFF COVID-19 Vaccine Monitor: July 2021; Kaiser Family Foundation: San Francisco, CA, USA, 2021. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| US | Canada | Sweden | Italy | Total | ||||||
| N | % | N | % | N | % | N | % | N | % | |
| I would not take it at the moment but would consider it later on | 81 | 11% | 46 | 5% | 37 | 4% | 37 | 4% | 201 | 5% |
| Very unlikely | 133 | 18% | 83 | 8% | 62 | 6% | 37 | 4% | 315 | 9% |
| Somewhat unlikely | 41 | 6% | 31 | 3% | 44 | 5% | 30 | 3% | 146 | 4% |
| I am not sure | 86 | 12% | 113 | 11% | 152 | 16% | 100 | 10% | 451 | 12% |
| Somewhat likely | 118 | 16% | 140 | 14% | 176 | 18% | 222 | 23% | 656 | 18% |
| Very likely | 268 | 37% | 572 | 58% | 494 | 51% | 560 | 57% | 1894 | 52% |
| Total | 727 | 985 | 965 | 986 | 3663 | |||||
| Dichotomous Recoding | ||||||||||
| US | Canada | Sweden | Italy | Total | ||||||
| N | % | N | % | N | % | N | % | N | % | |
| Vaccine-Hesitant | 459 | 63% | 413 | 42% | 471 | 49% | 426 | 43% | 1769 | 48% |
| Non-Hesitant | 268 | 37% | 572 | 58% | 494 | 51% | 560 | 57% | 1894 | 52% |
| Reason | Mean (SD) | |
|---|---|---|
| Vaccine Safety and Government Control | The vaccine can cause other diseases | 5.3 (2.6) |
| Vaccine Effectiveness and Population Control | There is no elite group that will achieve financial power if people are getting vaccinated | 6.1 (2.7) |
| Freedom | People should be free to decide if they get vaccinated or not with no consequences for their job or personal life | 6.3 (2.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piltch-Loeb, R.; Harriman, N.W.; Healey, J.; Bonetti, M.; Toffolutti, V.; Testa, M.A.; Su, M.; Savoia, E. COVID-19 Vaccine Concerns about Safety, Effectiveness, and Policies in the United States, Canada, Sweden, and Italy among Unvaccinated Individuals. Vaccines 2021, 9, 1138. https://doi.org/10.3390/vaccines9101138
Piltch-Loeb R, Harriman NW, Healey J, Bonetti M, Toffolutti V, Testa MA, Su M, Savoia E. COVID-19 Vaccine Concerns about Safety, Effectiveness, and Policies in the United States, Canada, Sweden, and Italy among Unvaccinated Individuals. Vaccines. 2021; 9(10):1138. https://doi.org/10.3390/vaccines9101138
Chicago/Turabian StylePiltch-Loeb, Rachael, Nigel Walsh Harriman, Julia Healey, Marco Bonetti, Veronica Toffolutti, Marcia A. Testa, Max Su, and Elena Savoia. 2021. "COVID-19 Vaccine Concerns about Safety, Effectiveness, and Policies in the United States, Canada, Sweden, and Italy among Unvaccinated Individuals" Vaccines 9, no. 10: 1138. https://doi.org/10.3390/vaccines9101138
APA StylePiltch-Loeb, R., Harriman, N. W., Healey, J., Bonetti, M., Toffolutti, V., Testa, M. A., Su, M., & Savoia, E. (2021). COVID-19 Vaccine Concerns about Safety, Effectiveness, and Policies in the United States, Canada, Sweden, and Italy among Unvaccinated Individuals. Vaccines, 9(10), 1138. https://doi.org/10.3390/vaccines9101138