
Music Tempo: A Tool for Regulating Walking Cadence and Physical Activity Intensity in Overweight Adults?

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Characteristics and Randomisation
2.2. Development of Walking Programmes and Playlists
2.3. Laboratory Procedures
2.4. Statistical Analysis
3. Results
3.1. Descriptive Data
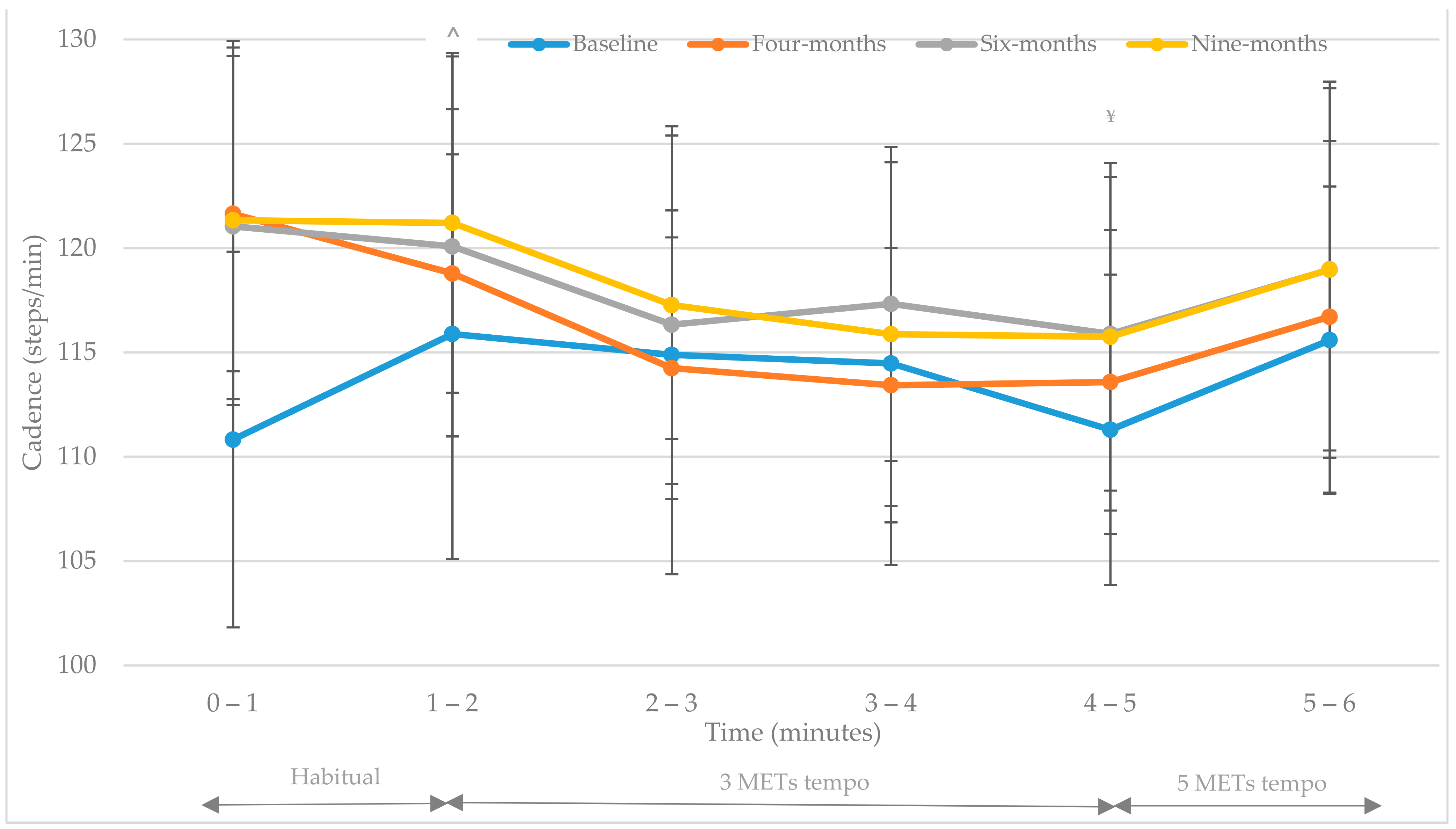
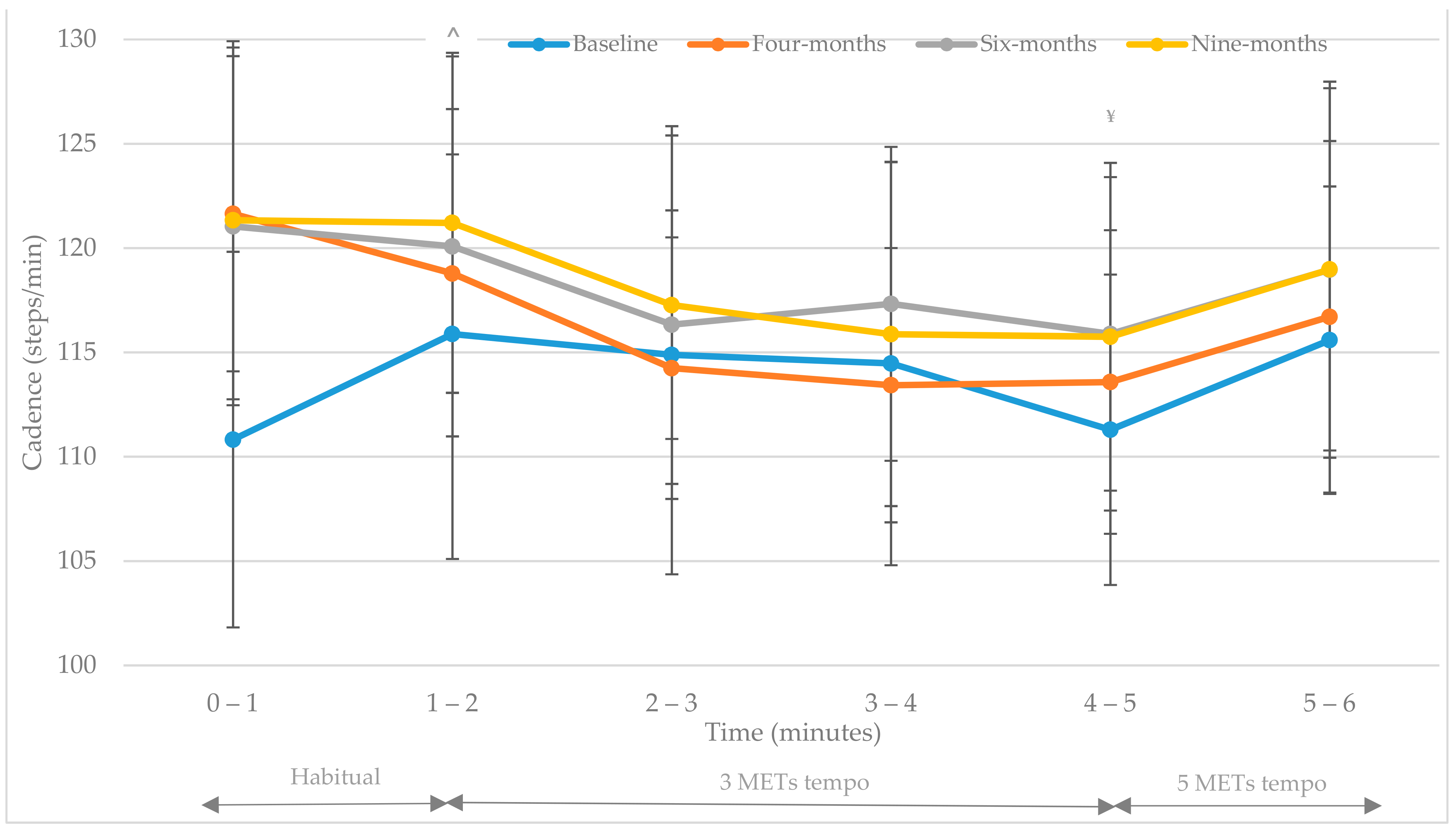
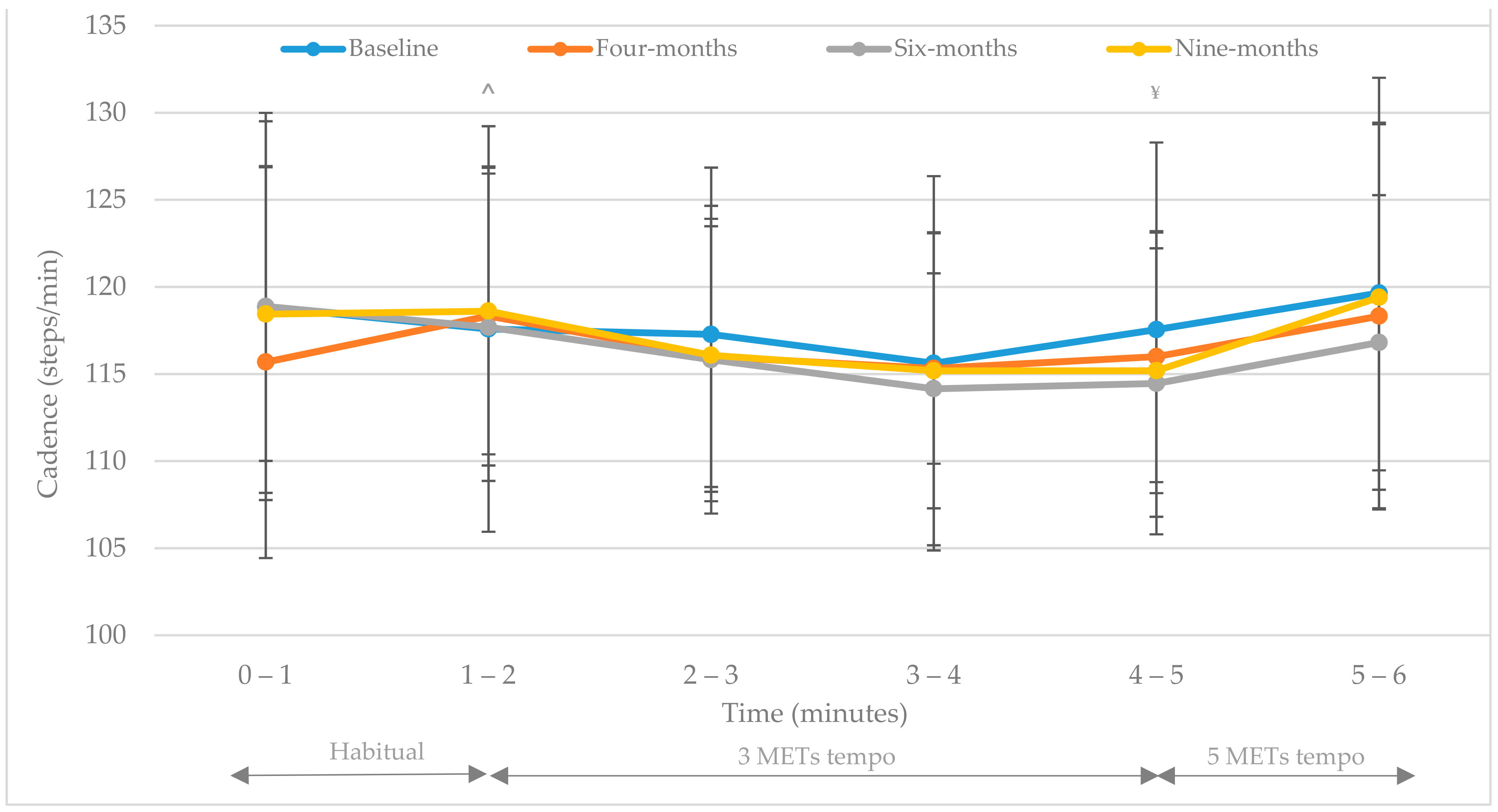
3.2. Cadence (Steps/Min)
3.3. Heart Rate (bpm)
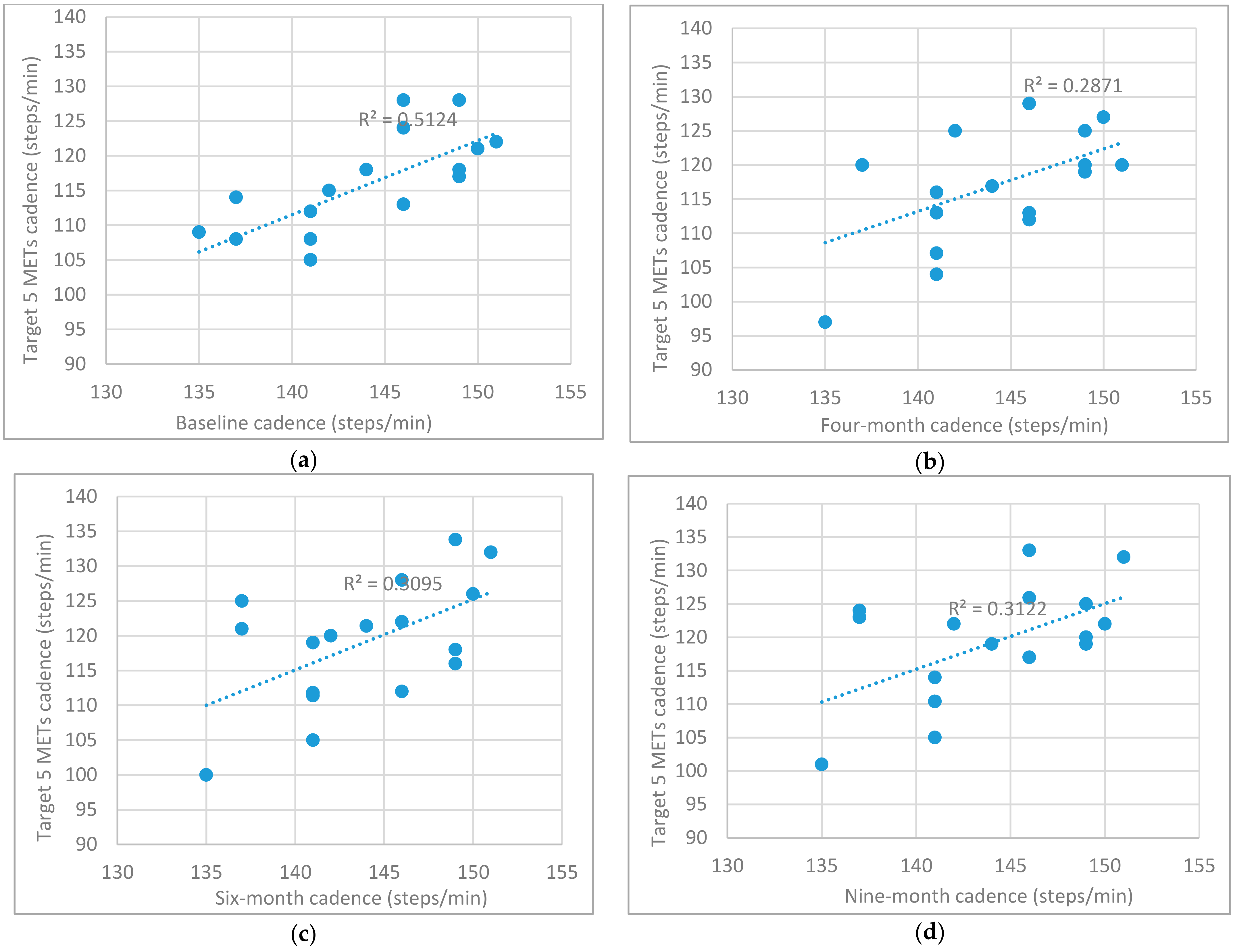
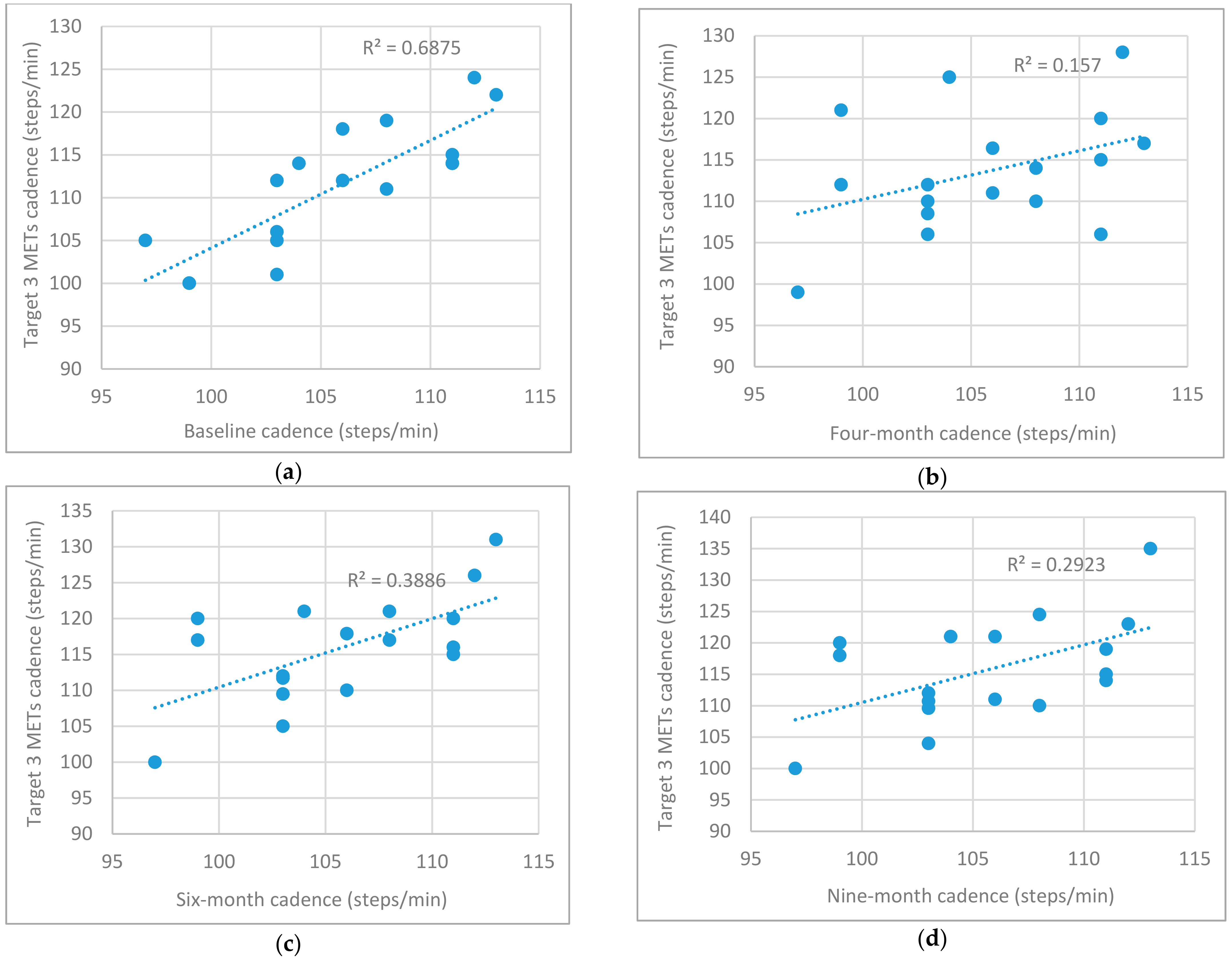
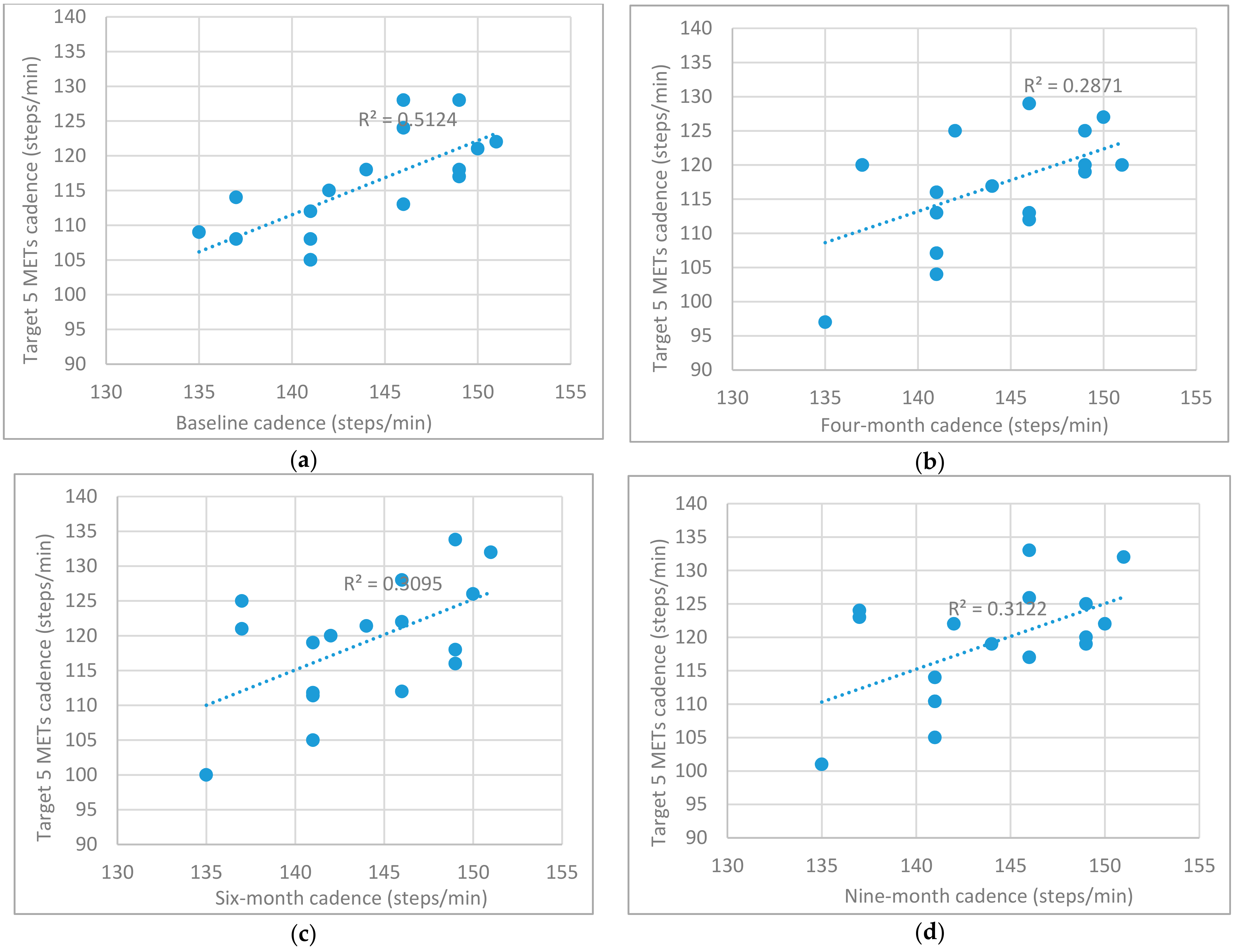
3.4. Cadence (Steps/Min) vs. Predetermined Height Related Stride Rate Cut-Points (3 METs and 5 METs Target)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 21 April 2021).
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 21 April 2021).
- World Health Organization Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. Global Action Plan on Physical Activity 2018-2030: More Active People for a Healthier World: At-a-Glance 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/272721/WHO-NMH-PND-18.5-eng.pdf (accessed on 26 May 2021).
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Department of Health and Social Care UK Chief Medical Officers’ Physical Activity Guidelines 2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/832868/uk-chief-medical-officers-physical-activity-guidelines.pdf (accessed on 21 April 2021).
- Parise, C.; Sternfeld, B.; Samuels, S.; Tager, I.B. Brisk Walking Speed in Older Adults Who Walk for Exercise. J. Am. Geriatr. Soc. 2004, 52, 411–416. [Google Scholar] [CrossRef]
- Rowe, D.A.; Kang, M.; Sutherland, R.; Holbrook, E.A.; Barreira, T.V. Evaluation of inactive adults’ ability to maintain a moderate-intensity walking pace. J. Sci. Med. Sport 2013, 16, 217–221. [Google Scholar] [CrossRef]
- Centre for Disease Control and Prevention Walking Campaign Tools. Available online: http://www.cdc.gov/nationalhealthyworksite/join/walkingtools.html (accessed on 26 May 2021).
- Walking for Health Walking for Health. Available online: https://www.walkingforhealth.org.uk/ (accessed on 26 May 2021).
- Tudor-Locke, C.; Ducharme, S.W.; Aguiar, E.J.; Schuna, J.M.; Barreira, T.V.; Moore, C.C.; Chase, C.J.; Gould, Z.R.; Amalbert-Birriel, M.A.; Mora-Gonzalez, J. Walking cadence (steps/min) and intensity in 41 to 60-year-old adults: The CA-DENCE-adults study. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.W.; Kivell, M.J.; Wojcik, W.R.; d’Entremont, G.; Kimmerly, D.S.; Fowles, J.R. Step rate thresholds associated with moderate and vigorous physical activity in adults. Int. J. Environ. Res. Public Health 2018, 15, 2454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tudor-Locke, C.; Schuna, J. Steps to Preventing Type 2 Diabetes: Exercise, Walk More, or Sit Less? Front. Endocrinol. 2012, 3. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W.; Andrews, A.W. Normal walking speed: A descriptive meta-analysis. Physiotherapy 2011, 97, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Glass, S.; Dwyer, G.B.; American College of Sports Medicine (Eds.) ACSM’s Metabolic Calculations Handbook; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- American College of Sports Medicine (Ed.) ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Tudor-Locke, C.; Rowe, D.A. Using cadence to study free-living ambulatory behaviour. Sports Med. 2012, 42, 381–398. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Brashear, M.M.; Kotzmarzyk, P.T.; Johnson, W.D. Peak stepping cadence in free-living adults: 2005–2006 NHANES. J. Phys. Act. Health 2012, 9, 1125. [Google Scholar] [CrossRef]
- Rowe, D.A.; Welk, G.J.; Heil, D.P.; Mahar, M.T.; Kemble, C.D.; Calabró, M.A.; Camenisch, K. Stride rate recommendations for moderate-intensity walking. Med. Sci. Sports Exerc. 2011, 43, 312. [Google Scholar] [CrossRef] [PubMed]
- Styns, F.; van Noorden, L.; Moelants, D.; Leman, M. Walking on music. Hum. Mov. Sci. 2007, 26, 769–785. [Google Scholar] [CrossRef]
- Faulkner, M.; Murphy, M.; Davison, G.; Rowe, D.; Hewitt, A.; Nevill, A.; Duly, E.; Trinick, T.; McNeilly, A.M. The physiological effects of a walking to music intervention in adults with intermediate hyperglycemia. Open J. Endocr. Metab. Dis. 2021, 11, 43–51. [Google Scholar] [CrossRef]
- Faulkner, M.; McNeilly, A.; Davison, G.; Rowe, D.; Hewitt, A.; Nevill, A.; Duly, E.; Trinick, T.; Murphy, M. Recruitment, retention and compliance of overweight inactive adults with intermediate hyperglycaemia to a novel walking intervention. Obesities 2021, 1, 88–100. [Google Scholar] [CrossRef]
- Perry, D.C.; Moore, C.C.; Sands, C.J.; Aguiar, E.J.; Gould, Z.R.; Tudor-Locke, C.; Ducharme, S.W. Using music-based cadence entrainment to manipulate walking intensity. J. Phys. Act. Health 2019, 16, 1039–1046. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Craig, C.; Brown, W.; Clemes, S.; De Cocker, K.; Giles-Corti, B.; Hatano, Y.; Inoue, S.; Matsudo, S.; Mutrie, N.; et al. How Many Steps/Day are Enough? For Adults. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 79. Available online: http://www.ijbnpa.org/content/8/1/79 (accessed on 6 May 2021). [CrossRef] [Green Version]
- Fegan, D. Cross-Validation of the American College of Sports Medicine’s Metabolic Prediction Equation for Walking in Older Females. Ph.D. Thesis, San Jose State University, San Jose, CA, USA, 1992. [Google Scholar]
- Cunha, F.A.; Catalao, R.P.; Midgley, A.W.; Gurgel, J.; Porto, F.; Farinatti, P.T. Do the speeds defined by the American College of Sports Medicine metabolic equation for running produce target energy expenditures during isocaloric exercise bouts? Eur. J. Appl. Physiol. 2012, 112, 3019–3026. [Google Scholar] [CrossRef]
- Saitoh, M.; Matsunaga, A.; Kamiya, K.; Ogura, M.N.; Sakamoto, J.; Yonezawa, R.; Kasahara, Y.; Watanabe, H.; Masuda, T. Comparison of cardiovascular responses between upright and recumbent cycle ergometers in healthy young volunteers performing low-intensity exercise: Assessment of reliability of the oxygen uptake calculated by using the ACSM metabolic equation. Arch. Phys. Med. Rehabil. 2005, 86, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- Murtagh, E.M.; Mair, J.L.; Aguiar, E.; Tudor-Locke, C.; Murphy, M.H. Outdoor walking speeds of apparently healthy adults: A systematic review and meta-analysis. Sports Med. 2021, 51, 1–17. [Google Scholar] [CrossRef]
- Hills, A.P.; Byrne, N.M.; Wearing, S.; Armstrong, T. Validation of the intensity of walking for pleasure in obese adults. Prev. Med. 2006, 42, 47–50. [Google Scholar] [CrossRef]
- Karageorghis, C.I.; Terry, P.C.; Lane, A.M.; Bishop, D.T.; Priest, D. The BASES expert statement on the use of music in exercise. Sport Exerc. Sci. 2011, 28, 18–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karageorghis, C.I.; Priest, D.L. Music in the exercise domain: A review and synthesis (Part I). Int. Rev. Sport Exerc. Psychol. 2012, 5, 44–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karageorghis, C.I.; Priest, D.L. Music in the exercise domain: A review and synthesis (Part II). Int. Rev. Sport Exerc. Psychol. 2012, 5, 67–84. Available online: https://www.tandfonline.com/doi/full/10.1080/1750984X.2011.631027 (accessed on 1 May 2021). [CrossRef]
- Almeida, F.A.M.; Nunes, R.F.H.; dos Santos Ferreira, S.; Krinski, K.; Elsangedy, H.M.; Buzzachera, C.F.; Alves, R.C.; da Silva, S.G. Effects of musical tempo on physiological, affective, and perceptual variables and performance of self-selected walking pace. J. Phys. Ther. Sci. 2015, 27, 1709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terry, P.C.; Karageorghis, C.I.; Saha, A.M.; D’Auria, S. Effects of synchronous music on treadmill running among elite triathletes. J. Sci. Med. Sport 2012, 15, 52–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karageorghis, C.I.; Mouzourides, D.A.; Priest, D.; Sasso, T.A.; Morrish, D.J.; Walley, C.L. Psychophysical and ergogenic effects of synchronous music during treadmill walking. J. Sport Exerc. Psychol. 2009, 31, 18–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation Physical Inactivity: A Global Public Health Problem. Available online: https://www.who.int/ncds/prevention/physical-activity/inactivity-global-health-problem/en/#:~:text=Regular%20physical%20activity%20is%20a,and%20breast%20and%20colon%20cancer (accessed on 26 May 2021).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Height (Inches) | Height (cm) | Stride Rate (3 METs) | Stride Rate (4 METs) | Stride Rate (5 METs) |
|---|---|---|---|---|
| Generic a | 103 | 122 | 141 | |
| 60 | 152.4 | 113 | 132 | 151 |
| 61 | 154.9 | 112 | 131 | 150 |
| 62 | 157.5 | 111 | 130 | 149 |
| 63 | 160.0 | 109 | 128 | 147 |
| 64 | 162.6 | 108 | 127 | 146 |
| 65 | 165.1 | 107 | 126 | 145 |
| 66 | 167.6 | 106 | 125 | 144 |
| 67 | 170.2 | 104 | 123 | 142 |
| 68 | 172.7 | 103 | 122 | 141 |
| 69 | 175.3 | 102 | 121 | 140 |
| 70 | 177.8 | 100 | 119 | 138 |
| 71 | 180.3 | 99 | 118 | 137 |
| 72 | 182.9 | 98 | 117 | 136 |
| 73 | 185.4 | 97 | 116 | 135 |
| 74 | 188.0 | 95 | 114 | 133 |
| 75 | 190.5 | 94 | 113 | 132 |
| 76 | 193.0 | 93 | 112 | 131 |
| 77 | 195.6 | 91 | 110 | 129 |
| 78 | 198.1 | 90 | 109 | 128 |
| Variable | Group | (n) | Mean | SD |
|---|---|---|---|---|
| Age (years) | IG | 17 | 48.53 | 9.87 |
| UC | 20 | 50.75 | 13.81 | |
| Height (cm) | IG | 17 | 168.18 | 10.10 |
| UC | 20 | 168.53 | 9.20 | |
| Body mass (kg) | IG | 17 | 96.24 | 15.66 |
| UC | 20 | 93.48 | 18.45 |
| Group (n) | Music Tempo (Beats Per Minute) 3 METs | Music Tempo (Beats Per Minute) 5 METs | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Range (Min) | Range (Max) | Mean | SD | Range (Min) | Range (Max) | |
| IG (n = 17) | 105.7 | 4.9 | 97 | 113 | 143.8 | 4.9 | 135 | 151 |
| UC (n = 20) | 105.9 | 4.6 | 99 | 112 | 143.9 | 4.6 | 137 | 150 |
| Overall (n = 37) | 105.8 | 4.7 | 97 | 113 | 143.8 | 4.7 | 135 | 151 |
| Assessment Time-Point | Cadence Target | Time (Mins) | Cadence (Steps/Min) | Heart Rate Response (bpm) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IG (n = 17) | UC (n = 20) | Overall (n = 37) | IG (n = 17) | UC (n = 20) | Overall (n = 37) $ | |||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Baseline | Habitual | 0–1 | 110.82 † | 9.00 | 118.85 † | 10.67 | 115.16 | 10.61 ^ | 106 | 13 | 108 | 13 | 107 | 13 |
| 1–2 | 115.88 | 10.78 | 117.70 | 11.64 | 116.87 | 11.14 ^ | 112 | 15 | 112 | 15 | 112 | 15 | ||
| 3 METs | 2–3 | 114.88 | 10.52 | 117.26 | 9.58 | 116.17 | 9.95 ^,¥ | 116 | 18 | 114 | 14 | 115 | 15 | |
| 3–4 | 114.47 | 9.67 | 115.73 | 10.74 | 115.15 | 10.14 ^,¥ | 118 | 17 | 116 | 14 | 117 | 15 | ||
| 4–5 | 111.29 | 7.44 | 117.67 | 10.74 | 114.74 | 9.79 ^,¥ | 120 | 18 | 117 | 14 | 119 | 16 | ||
| 5 METs | 5–6 | 115.59 | 7.37 | 119.81 | 12.36 | 117.87 | 10.45 ¥ | 122 | 17 | 119 | 17 | 121 | 17 | |
| Four-months | Habitual | 0–1 | 121.64 ǐ | 7.56 | 115.95 | 11.25 | 118.57 | 10.02 ^ | 107 | 10 | 112 | 7 | 110 | 9 |
| 1–2 | 118.78 | 5.71 | 118.56 | 8.58 | 118.66 | 7.31 ^ | 111 | 11 | 116 | 9 | 114 | 10 | ||
| 3 METs | 2–3 | 114.25 | 6.27 | 116.26 | 7.48 | 115.34 | 6.93 ^,¥ | 111 | 13 | 118 | 10 | 115 | 12 | |
| 3–4 | 113.43 | 6.58 | 115.70 | 5.47 | 114.66 | 6.03 ^,¥ | 112 | 14 | 120 | 10 | 116 | 12 | ||
| 4–5 | 113.58 | 7.28 | 116.34 | 7.21 | 115.08 | 7.27 ^,¥ | 114 | 15 | 120 | 10 | 117 | 12 | ||
| 5 METs | 5–6 | 116.71 | 8.43 | 118.71 | 11.10 | 117.79 | 9.88 ¥ | 116 | 16 | 122 | 11 | 119 | 14 | |
| Six-months | Habitual | 0–1 | 121.04 ǐ | 8.57 | 119.33 | 11.12 | 120.12 | 9.93 ^ | 108 | 15 | 109 | 11 | 109 | 13 |
| 1–2 | 120.08 | 9.11 | 118.25 | 8.83 | 119.09 | 8.88 ^ | 114 | 16 | 114 | 14 | 114 | 15 | ||
| 3 METs | 2–3 | 116.33 | 5.47 | 116.08 | 8.83 | 116.20 | 7.38 ^,¥ | 117 | 20 | 118 | 12 | 118 | 16 | |
| 3–4 | 117.33 | 7.52 | 114.44 | 8.98 | 115.77 | 8.36 ^,¥ | 118 | 21 | 120 | 15 | 119 | 18 | ||
| 4–5 | 115.88 | 7.52 | 114.84 | 8.66 | 115.32 | 8.06 ^,¥ | 118 | 20 | 121 | 14 | 119 | 17 | ||
| 5 METs | 5–6 | 118.96 | 9.01 | 117.27 | 8.46 | 118.05 | 8.64 ¥ | 121 | 22 | 123 | 15 | 122 | 18 | |
| Nine-months | Habitual | 0–1 | 121.33 ǐ | 8.59 | 118.82 | 8.43 | 119.98 | 8.48 ^ | 108 | 12 | 108 | 10 | 108 | 11 |
| 1–2 | 121.21 | 8.15 | 118.98 | 8.23 | 120.01 | 8.16 ^ | 112 | 14 | 112 | 11 | 112 | 12 | ||
| 3 METs | 2–3 | 117.27 | 8.58 | 116.37 | 7.84 | 116.78 | 8.08 ^,¥ | 115 | 17 | 114 | 12 | 114 | 14 | |
| 3–4 | 115.88 | 8.24 | 115.53 | 7.90 | 115.69 | 7.95 ^,¥ | 116 | 16 | 115 | 12 | 115 | 14 | ||
| 4–5 | 115.75 | 8.33 | 115.53 | 7.03 | 115.63 | 7.54 ^,¥ | 117 | 15 | 116 | 12 | 117 | 13 | ||
| 5 METs | 5–6 | 118.98 | 8.68 | 119.64 | 9.93 | 119.34 | 9.26 ¥ | 119 | 18 | 120 | 15 | 119 | 16 | |
| Assessment Time-Points (Actual Cadence, Steps/Min) | IG (n = 17) | UC (n = 20) | IG (n = 17) | UC (n = 20) |
|---|---|---|---|---|
| 3 METs Target Cadence (Steps/Min) | 3 METs Target Cadence (Steps/Min) | 5 METs Target Cadence (Steps/Min) | 5 METs Target Cadence (Steps/Min) | |
| Baseline (steps/min) | 0.86 ** | 0.03 | 0.75 ** | 0.12 |
| Four months (steps/min) | 0.40 | 0.03 | 0.50 * | 0.19 |
| Six months (steps/min) | 0.59 * | 0.11 | 0.53 * | 0.30 |
| Nine months (steps/min) | 0.54 * | −0.09 | 0.50 * | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faulkner, M.; McNeilly, A.; Davison, G.; Rowe, D.; Hewitt, A.; Nevill, A.; Duly, E.; Trinick, T.; Murphy, M. Music Tempo: A Tool for Regulating Walking Cadence and Physical Activity Intensity in Overweight Adults? Int. J. Environ. Res. Public Health 2021, 18, 7855. https://doi.org/10.3390/ijerph18157855
Faulkner M, McNeilly A, Davison G, Rowe D, Hewitt A, Nevill A, Duly E, Trinick T, Murphy M. Music Tempo: A Tool for Regulating Walking Cadence and Physical Activity Intensity in Overweight Adults? International Journal of Environmental Research and Public Health. 2021; 18(15):7855. https://doi.org/10.3390/ijerph18157855
Chicago/Turabian StyleFaulkner, Maria, Andrea McNeilly, Gareth Davison, David Rowe, Allan Hewitt, Alan Nevill, Ellie Duly, Tom Trinick, and Marie Murphy. 2021. "Music Tempo: A Tool for Regulating Walking Cadence and Physical Activity Intensity in Overweight Adults?" International Journal of Environmental Research and Public Health 18, no. 15: 7855. https://doi.org/10.3390/ijerph18157855