
Immediate Effects of Dry Needling on the Autonomic Nervous System and Mechanical Hyperalgesia: A Randomized Controlled Trial

 , ,
, ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
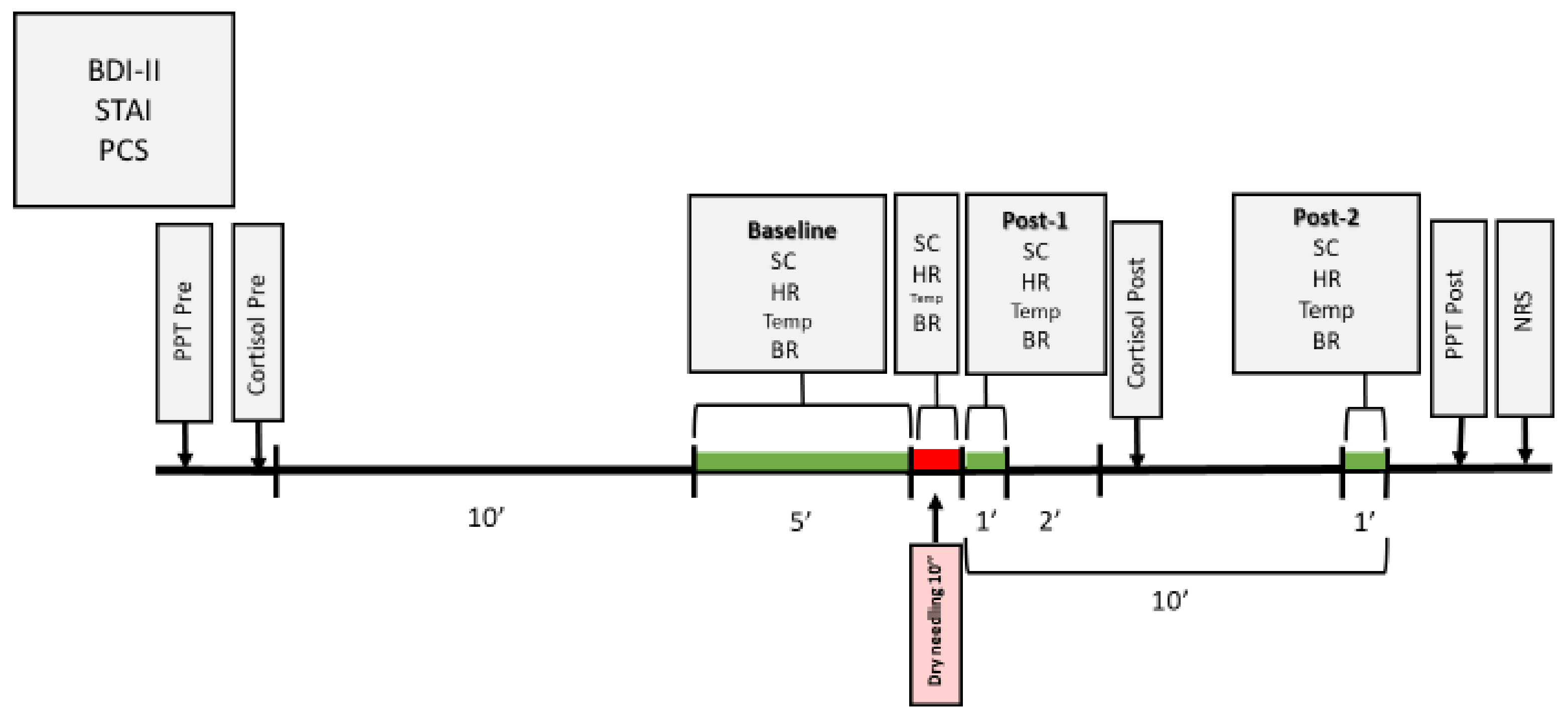
2.1. Study Design
2.2. Participants
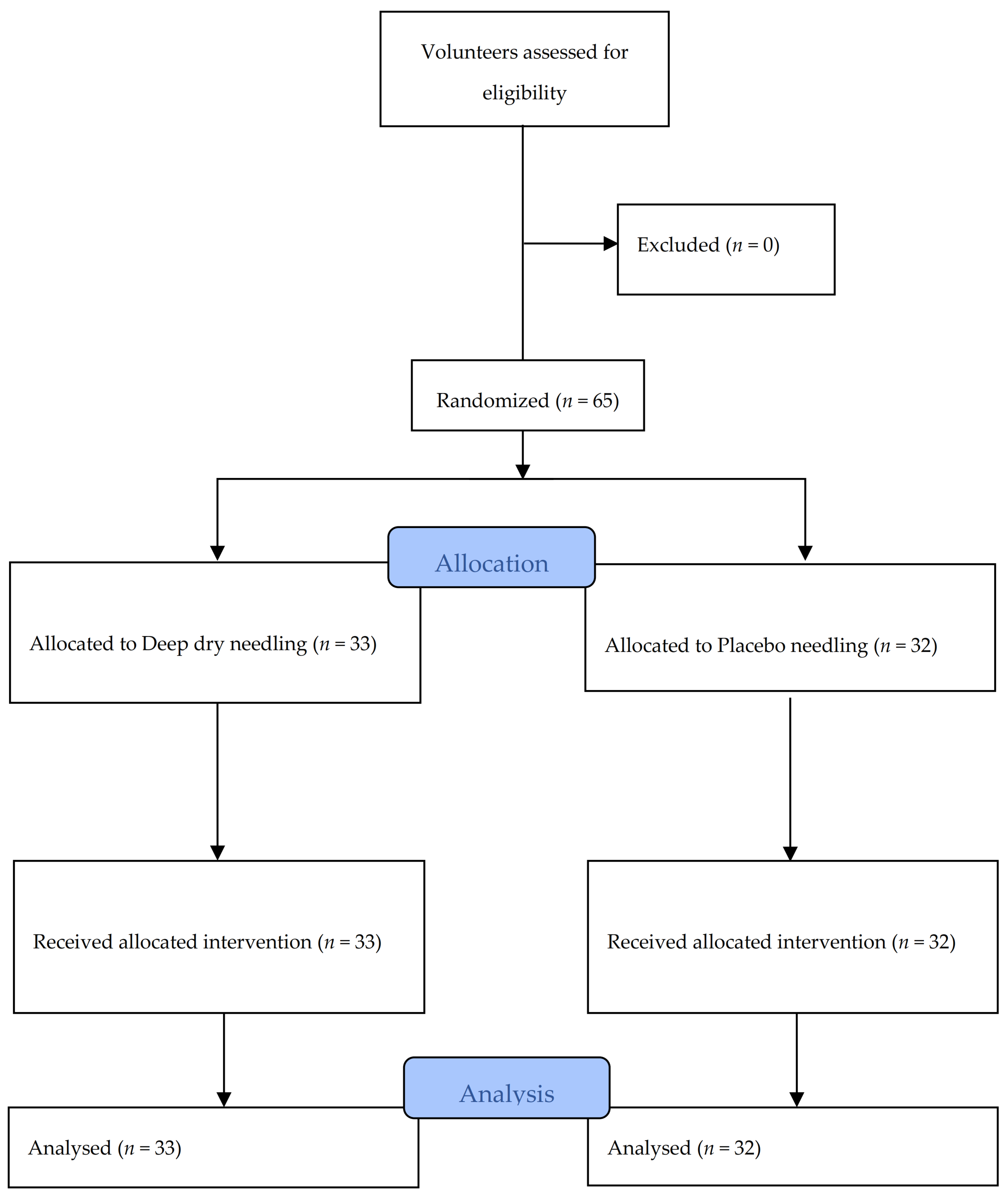
2.3. Randomization and Blinding
2.4. Procedure
2.4.1. Deep Dry Needling Group
2.4.2. Placebo Needling Group
2.5. Outcome Measures
2.5.1. Psychological Factors
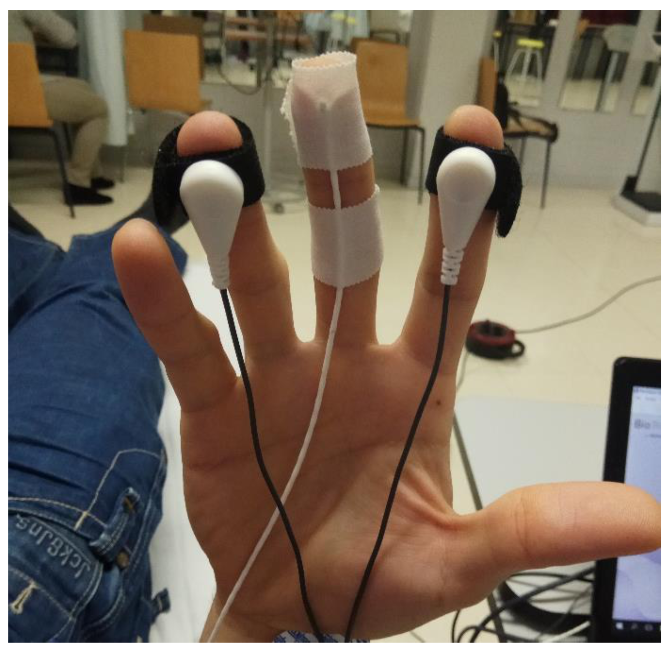
2.5.2. Autonomic Nervous System Assessments: Primary Outcomes
Physiological Variables
Cortisol
2.5.3. Pain Assessments: Secondary Outcomes
Pain Intensity
Pressure Pain Threshold (PPT)
2.6. Sample Size
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Autonomic Nervous System Assessments: Primary Outcomes
3.3. Pressure Pain Threshold
3.4. Correlations between Pain Intensity, Physiological Variables and Cortisol
4. Discussion
4.1. Clinical Implications
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gattie, E.; Cleland, J.A.; Snodgrass, S. The effectiveness of trigger point dry needling for musculoskeletal conditions by physical therapists: A systematic review and meta-analysis. J. Orthop. Sports Phys. Ther. 2017, 47, 133–149. [Google Scholar] [CrossRef] [PubMed]
- Dunning, J.; Butts, R.; Mourad, F.; Young, I.; Flannagan, S.; Perreault, T. Dry needling: A literature review with implications for clinical practice guidelines. Phys. Ther. Rev. 2014, 19, 252–265. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Huang, Q.M.; Liu, Q.G.; Thitham, N.; Li, L.H.; Ma, Y.T.; Zhao, J.M. Evidence for Dry Needling in the Management of Myofascial Trigger Points Associated With Low Back Pain: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 99, 144–152.e2. [Google Scholar] [CrossRef] [PubMed]
- Vier, C.; Almeida, M.B.; Neves, M.L.; Santos, A.R.S.; Bracht, M.A. The effectiveness of dry needling for patients with orofacial pain associated with temporomandibular dysfunction: A systematic review and meta-analysis. Braz. J. Phys. Ther. 2019, 23, 3–11. [Google Scholar] [CrossRef]
- Liu, L.; Huang, Q.; Liu, Q.; Ye, G.; Bo, C.; Chen, M.; Li, P. Effectiveness of dry needling for myofascial trigger points associated with neck and shoulder pain: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2015, 96, 944–955. [Google Scholar] [CrossRef]
- Donnelly, J.M.; Fernandez-de-Las-Peñas, C.; Finnegan, M.; Freeman, J.L. Travell, Simons & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual, 3rd ed.; Wolters Kluwer: Philadelphia, PA, USA, 2019. [Google Scholar]
- Shah, J.P.; Thaker, N.; Heimur, J.; Aredo, J.V.; Sikdar, S.; Gerber, L. Myofascial trigger points then and now: A historical and scientific perspective. PM R 2015, 7, 746–761. [Google Scholar] [CrossRef]
- Jafri, M.S. Mechanisms of Myofascial Pain. Int. Sch. Res. Not. 2014, 2014, 1–16. [Google Scholar] [CrossRef]
- Cagnie, B.; Dewitte, V.; Barbe, T.; Timmermans, F.; Delrue, N.; Meeus, M. Physiologic effects of dry needling. Curr. Pain Headache Rep. 2013, 17, 348. [Google Scholar] [CrossRef]
- Schlereth, T.; Birklein, F. The sympathetic nervous system and pain. NeuroMol. Med. 2008, 10, 141–147. [Google Scholar] [CrossRef]
- Yilmaz, P.; Diers, M.; Diener, S.; Rance, M.; Wessa, M.; Flor, H. Brain correlates of stress-induced analgesia. Pain 2010, 151, 522–529. [Google Scholar] [CrossRef]
- McEwen, B.S.; Kalia, M. The role of corticosteroids and stress in chronic pain conditions. Metabolism 2010, 59, S9–S15. [Google Scholar] [CrossRef]
- Rotenberg, S.; McGrath, J.J. Inter-Relation between autonomic and HPA axis activity in children and adolescents. Biol. Psychol. 2016, 117, 16–25. [Google Scholar] [CrossRef]
- Greaney, J.L.; Kenney, W.L. Measuring and quantifying skin sympathetic nervous system activity in humans. J. Neurophysiol. 2017, 118, 2181–2193. [Google Scholar] [CrossRef]
- De La Cruz Torres, B.; Cabello, M.A.; Bermejo, P.G.; Orellana, J.N. Autonomic responses to ultrasoundguided percutaneous needle electrolysis of the patellar tendon in healthy male footballers. Acupunct. Med. 2016, 34, 275–279. [Google Scholar] [CrossRef]
- La Touche, R.; Paris-Alemany, A.; Mannheimer, J.S.; Angulo-Diaz-Parreno, S.; Bishop, M.D.; Lopez-Valverde-Centeno, A.; von Piekartz, H.; Fernandez-Carnero, J. Does mobilization of the upper cervical spine affect pain sensitivity and autonomic nervous system function in patients with cervico-craniofacial pain?: A randomized-controlled trial. Clin. J. Pain 2013, 29, 205–215. [Google Scholar] [CrossRef]
- Hannibal, K.E.; Bishop, M.D. Chronic Stress, Cortisol Dysfunction, and Pain: A Psychoneuroendocrine Rationale for Stress Management in Pain Rehabilitation. Phys. Ther. 2014, 94, 1816–1825. [Google Scholar] [CrossRef]
- Gaab, J.; Jiménez, J.; Voneschen, L.; Oschwald, D.; Meyer, A.H.; Nater, U.M.; Krummenacher, P. Psychosocial Stress-Induced Analgesia: An Examination of Effects on Heat Pain Threshold and Tolerance and of Neuroendocrine Mediation. Neuropsychobiology 2017, 74, 87–95. [Google Scholar] [CrossRef]
- Butler, R.K.; Finn, D.P. Stress-induced analgesia. Prog. Neurobiol. 2009, 88, 184–202. [Google Scholar] [CrossRef]
- Brady, S.; McEvoy, J.; Dommerholt, J.; Doody, C. Adverse events following trigger point dry needling: A prospective survey of chartered physiotherapists. J. Man. Manip. Ther. 2014, 22, 134–140. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef]
- Cobos-Carbó, A.; Augustovski, F. Declaración CONSORT 2010: Actualización de la lista de comprobación para informar ensayos clínicos aleatorizados de grupos paralelos. Med. Clin. 2011, 137, 213–215. [Google Scholar] [CrossRef] [PubMed]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT statement. J. Evid. Based. Med. 2010, 3, 140–155. [Google Scholar] [CrossRef] [PubMed]
- Takai, N.; Yamaguchi, M.; Aragaki, T.; Eto, K.; Uchihashi, K.; Nishikawa, Y. Effect of psychological stress on the salivary cortisol and amylase levels in healthy young adults. Arch. Oral Biol. 2004, 49, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Myburgh, C.; Lauridsen, H.H.; Larsen, A.H.; Hartvigsen, J. Standardized manual palpation of myofascial trigger points in relation to neck/shoulder pain; the influence of clinical experience on inter-examiner reproducibility. Man. Ther. 2011, 16, 136–140. [Google Scholar] [CrossRef]
- Huang, W.; Taylor, A.; Howie, J.; Robinson, N. Is the Diurnal Profile of Salivary Cortisol Concentration a Useful Marker for Measuring Reported Stress in Acupuncture Research? A Randomized Controlled Pilot Study. J. Altern. Complement. Med. 2012, 18, 242–250. [Google Scholar] [CrossRef]
- Edwards, S.; Evans, P.; Hucklebridge, F.; Clow, A. Association between time of awakening and diurnal cortisol secretory activity. Psychoneuroendocrinology 2001, 26, 613–622. [Google Scholar] [CrossRef]
- Pecos-Martín, D.; Montañez-Aguilera, F.J.; Gallego-Izquierdo, T.; Urraca-Gesto, A.; Gómez-Conesa, A.; Romero-Franco, N.; Plaza-Manzano, G. Effectiveness of dry needling on the lower trapezius in patients with mechanical neck pain: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2015, 96, 775–781. [Google Scholar] [CrossRef]
- Llamas-Ramos, R.; Pecos-Martín, D.; Gallego-Izquierdo, T.; Llamas-Ramos, I.; Plaza-Manzano, G.; Ortega-Santiago, R.; Cleland, J.; Fernández-de-Las-Peñas, C. Comparison of the Short-Term Outcomes Between Trigger Point Dry Needling and Trigger Point Manual Therapy for the Management of Chronic Mechanical Neck Pain: A Randomized Clinical Trial. J Orthop Sport. Phys. Ther. 2015, 44, 852–861. [Google Scholar] [CrossRef]
- Hong, C.Z. Lidocaine injection versus dry needling to myofascial trigger point: The importance of the local twitch response. Am. J. Phys. Med. Rehabil. 1994, 73, 256–263. [Google Scholar] [CrossRef]
- Tough, E.A.; White, A.R.; Richards, S.H.; Campbell, J.L. Myofascial trigger point needling for whiplash associated pain-A feasibility study. Man. Ther. 2010, 15, 529–535. [Google Scholar] [CrossRef]
- Braithwaite, F.A.; Walters, J.L.; Li, L.S.K.; Moseley, G.L.; Williams, M.T.; McEvoy, M.P. Blinding Strategies in Dry Needling Trials: Systematic Review and Meta-Analysis. Phys. Ther. 2019, 99, 1461–1480. [Google Scholar] [CrossRef]
- Sanz, J.; Perdigón, A.L.; Vázquez, C. Adaptación española del Inventario para la Depresión de Beck-II (BDI-II): 2. Propiedades psicométricas en población general. Clin. Salud 2003, 14, 249–280. [Google Scholar]
- Guillén-Riquelme, A.; Buela-Casal, G. Metaanálisis de comparación de grupos y metaanálisis de generalización de la fiabilidad del Cuestionario State-Trait Anxiety Inventory (STAI). Rev. Esp. Salud. Pública 2014, 88, 101–112. [Google Scholar] [CrossRef]
- Seyler, A.; Hernández-Guzmán, L.; Freyre, M.; González-Montesinos, M.; Sullivan, M. Validez de la Escala de Catastrofización del Dolor. Rev. El Dolor 2014, 61, 18–24. [Google Scholar]
- De Kooning, M.; Tobbackx, Y.; Meeus, M.; Wauters, L.; Ickmans, K.; De Vilder, P.; Roose, J.; Verhaeghe, T.; Nijs, J. Acupuncture-analgesia following a single treatment session in chronic whiplash is unrelated to autonomic nervous system changes: A randomized cross-over trial. Pain Physician 2015, 18, 527–536. [Google Scholar]
- De Kooning, M.; Daenen, L.; Roussel, N.; Cras, P.; Buyl, R.; Ickmans, K.; Struyf, F.; Nijs, J. Endogenous pain inhibition is unrelated to autonomic responses in acute whiplash-associated disorders. J. Rehabil. Res. Dev. 2015, 52, 431–440. [Google Scholar] [CrossRef]
- Witt, C.M.; Meissner, K.; Pach, D.; Thiele, C.; Lüdtke, R.; Ghadiyali, Z.; Deter, H.C.; Zimmermann-Viehoff, F. Stimulation of gastric slow waves with manual acupuncture at acupuncture points ST36 and PC6-A randomized single blind controlled trial. Neurogastroenterol. Motil. 2012, 24, 438–445. [Google Scholar] [CrossRef]
- Westermann, J.; Demir, A.; Herbst, V. Determination of cortisol in saliva and serum by a luminescene-enhanced enzyme immunoassay. Clin. Lab. 2004, 50, 11–24. [Google Scholar]
- Wessa, M.; Rohleder, N.; Kirschbaum, C.; Flor, H. Altered cortisol awakening response in posttraumatic stress disorder. Psychoneuroendocrinology 2006, 31, 209–215. [Google Scholar] [CrossRef]
- Kirschbaum, C.; Hellhammer, D.H. Salivary cortisol in psychobiological research: An overview. Neuropsychobiology 1989, 22, 150–169. [Google Scholar] [CrossRef]
- Maidana, P.; Bruno, O.D.; Mesch, V. A critical analysis of cortisol measurements: An update. Medicina 2013, 73, 579–584. [Google Scholar] [PubMed]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63, 240–252. [Google Scholar]
- Díez-Burón, F.; Marcos-Vidal, J.; Baticón-Escudero, P.; Montes-Armenteros, A.; Bermejo-López, J.; Merino-García, M. Concordancia entre la escala verbal numérica y la escala visual analógica en el seguimiento del dolor agudo postoperatorio. Rev. Esp. Anestesiol. Reanim. 2011, 58, 279–282. [Google Scholar] [CrossRef]
- Waller, R.; Straker, L.; O’Sullivan, P.; Sterling, M.; Smith, A. Reliability of pressure pain threshold testing in healthy pain free young adults. Scand. J. Pain 2015, 9, 38–41. [Google Scholar]
- Chesterton, L.; Sim, J.; Wright, C.; Foster, N. Interrater Reliability of Algometry in Measuring Pressure Pain Thresholds in Healthy Humans, Using Multiple Raters. Clin. J. Pain 2007, 23, 760–766. [Google Scholar] [CrossRef]
- Perry, J.; Green, A. An investigation into the effects of a unilaterally applied lumbar mobilisation technique on peripheral sympathetic nervous system activity in the lower limbs. Man. Ther. 2008, 13, 492–499. [Google Scholar] [CrossRef]
- Berntson, G.G.; Bigger, J.T., Jr.; Eckberg, D.L.; Grossman, P.; Kaufmann, P.G.; Malik, M.; Nagaraja, H.N.; Porges, S.W.; Saul, J.P.; Stone, P.H.; et al. Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology 1997, 34, 623–648. [Google Scholar] [CrossRef]
- Sillevis, R.; Van Duijn, J.; Shamus, E.; Hard, M. Time effect for in-situ dry needling on the autonomic nervous system, a pilot study. Physiother. Theory Pract. 2019, 1–9. [Google Scholar] [CrossRef]
- Haker, E.; Egekvist, H.; Bjerring, P. Effect of sensory stimulation (acupuncture) on sympathetic and parasympathetic activities in healthy subjects. J. Auton. Nerv. Syst. 2000, 79, 52–59. [Google Scholar] [CrossRef]
- Sandberg, M.; Lindberg, L.G.; Gerdle, B. Peripheral effects of needle stimulation (acupuncture) on skin and muscle blood flow in fibromyalgia. Eur. J. Pain 2004, 8, 163–171. [Google Scholar] [CrossRef]
- Ozden, A.V.; Alptekin, H.K.; Esmaeilzadeh, S.; Cihan, C.; Aki, S.; Aksoy, C.; Oncu, J. Evaluation of the Sympathetic Skin Response to the Dry Needling Treatment in Female Myofascial Pain Syndrome Patients. J. Clin. Med. Res. 2016, 8, 513–518. [Google Scholar] [CrossRef]
- Kubo, K.; Iizuka, Y.; Yajima, H.; Takayama, M.; Takakura, N. Changes in Blood Circulation of the Tendons and Heart Rate Variability during and after Acupuncture. Med. Acupunct. 2020. [Google Scholar] [CrossRef]
- Kitagawa, Y.; Kimura, K.; Yoshida, S. Spectral analysis of heart rate variability during trigger point acupuncture. Acupunct. Med. 2014, 32, 273–278. [Google Scholar] [CrossRef]
- Núñez-Cortés, R.; Cruz-Montecinos, C.; Vásquez-Rosel, Á.; Paredes-Molina, O.; Cuesta-Vargas, A. Dry Needling Combined With Physical Therapy in Patients With Chronic Postsurgical Pain Following Total Knee Arthroplasty: A Case Series. J. Orthop. Sports Phys. Ther. 2017, 47, 209–216. [Google Scholar] [CrossRef]
- Hsieh, Y.; Kao, M.; Kuan, T.; Chen, S.; Chen, J.; Hong, C. Dry needling to a key myofascial trigger point may reduce the irritability of satellite MTrPs. Am. J. Phys. Med. Rehabil. 2007, 86, 397–403. [Google Scholar] [CrossRef]
- Martín-Pintado-Zugasti, A.; Rodríguez-Fernández, Á.L.; Fernandez-Carnero, J. Postneedling soreness after deep dry needling of a latent myofascial trigger point in the upper trapezius muscle: Characteristics, sex differences and associated factors. J. Back Musculoskelet. Rehabil. 2016, 29, 301–308. [Google Scholar] [CrossRef]
- Martín-Pintado Zugasti, A.; Rodríguez-Fernández, Á.L.; García-Muro, F.; López-López, A.; Mayoral, O.; Mesa-Jiménez, J.; Fernández-Carnero, J. Effects of spray and stretch on postneedling soreness and sensitivity after dry needling of a latent myofascial trigger point. Arch. Phys. Med. Rehabil. 2014, 95, 1925–1932.e1. [Google Scholar] [CrossRef]
- Martín-Pintado-Zugasti, A.; Pecos-Martin, D.; Rodríguez-Fernández, Á.L.; Alguacil-Diego, I.M.; Portillo-Aceituno, A.; Gallego-Izquierdo, T.; Fernandez-Carnero, J. Ischemic Compression After Dry Needling of a Latent Myofascial Trigger Point Reduces Postneedling Soreness Intensity and Duration. PM R 2015, 7, 1026–1034. [Google Scholar] [CrossRef]
- Mejuto-Vázquez, M.J.; Salom-Moreno, J.; Ortega-Santiago, R.; Truyols-Domínguez, S.; Fernández-de-Las-Peñas, C. Short-term changes in neck pain, widespread pressure pain sensitivity, and cervical range of motion after the application of trigger point dry needling in patients with acute mechanical neck pain: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2014, 44, 252–260. [Google Scholar] [CrossRef]
- Sterling, M.; Vicenzino, B.; Souvlis, T.; Connelly, L.B. Dry-needling and exercise for chronic whiplash-associated disorders: A randomized single-blind placebo-controlled trial. Pain 2015, 156, 635–643. [Google Scholar] [CrossRef]
- Ziaeifar, M.; Arab, A.M.; Karimi, N.; Nourbakhsh, M.R. The effect of dry needling on pain, pressure pain threshold and disability in patients with a myofascial trigger point in the upper trapezius muscle. J. Bodyw. Mov. Ther. 2014, 18, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.P.; Danoff, J.; Desai, M.J.; Parikh, S.; Nakamura, L.; Phillips, T.M.; Gerber, L.H. Biochemicals Associated With Pain and Inflammation are Elevated in Sites Near to and Remote From Active Myofascial Trigger Points. Arch. Phys. Med. Rehabil. 2008, 89, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.P.; Phillips, T.M.; Danoff, J.V.G.L. An in vivo microanalytical technique for measuring the local biochemical milieu of human skeletal muscle. J Appl. Physiol. 2005, 99, 1977–1984. [Google Scholar] [CrossRef] [PubMed]
- Chou, L.-W.; Kao, M.-J.; Lin, J.-G. Probable mechanisms of needling therapies for myofascial pain control. Evid. Based Complement Altern. Med. 2012, 1–11. [Google Scholar] [CrossRef]
- Knardahl, S.; Elam, M.; Olausson, B.; Wallin, B.G. Sympathetic nerve activity after acupuncture in humans. Pain 1998, 75, 19–25. [Google Scholar] [CrossRef]
- Muñoz Sastre, M.T.; Albaret, M.C.; Maria Raich Escursell, R.; Mullet, E. Fear of pain associated with medical procedures and illnesses. Eur. J. Pain 2006, 10, 57. [Google Scholar] [CrossRef]
- Loggia, M.L.; Juneau, M.; Bushnell, M.C. Autonomic responses to heat pain: Heart rate, skin conductance, and their relation to verbal ratings and stimulus intensity. Pain 2011, 152, 592–598. [Google Scholar] [CrossRef]
- Kang, O.S.; Chang, D.S.; Lee, M.H.; Lee, H.; Park, H.J.; Chae, Y. Autonomic and subjective responses to real and sham acupuncture stimulation. Auton. Neurosci. Basic Clin. 2011, 159, 127–130. [Google Scholar] [CrossRef]
- Lee, I.S.; Jo, H.J.; Lee, S.H.; Lee, H.; Lee, H.; Park, H.J.; Chae, Y. Fear of acupuncture enhances sympathetic activation to acupuncture stimulation. Acupunct. Med. 2013, 31, 276–281. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Dry Needling Group (n = 33) Mean ± SD (Range) | Placebo Group (n = 32) Mean ± SD (Range) | p-Value * | |
|---|---|---|---|---|
| Age (years) | 26.88 ± 8.05 (19–51) | 28.72 ± 8.79 (19–53) | 0.382 | |
| Gender † | Male | 16 (48.5) | 17 (53.1) | 0.708 ‡ |
| Female | 17 (51.5) | 15 (46.9) | ||
| Weight (kg) | 71.28 ± 12.02 (46.6–98.4) | 68.08 ± 16.00 (47.1–108.1) | 0.366 | |
| Height (m) | 1.71 ± 0.06 (1.58–1.82) | 1.69 ± 0.08 (1.54–1.83) | 0.262 | |
| BMI (kg/m2) | 24.29 ± 3.52 (18.67–32.16) | 23.66 ± 4.33 (17.78–33.36) | 0.522 | |
| Wake-up time | 7:28 ± 55.8 min (5:40–9:00) | 7:36 ± 52.4 min (4:30–9:00) | 0.565 | |
| BDI-II | 5.85 ± 4.75 (0–21) | 5.03 ± 4.04 (0–13) | 0.458 | |
| STAI | State Anxiety | 9.82 ± 7.48 (0–32) | 12.34 ± 6.79 (0–29) | 0.160 |
| Trait Anxiety | 12.27 ± 7.47 (0–25) | 13.31 ± 6.87 (0–25) | 0.561 | |
| PCS | Rumination | 2.97 ± 2.21 (0–8) | 2.09 ± 2.94 (0–9) | 0.179 |
| Helplessness | 2.61 ± 2.79 (0–10) | 1.66 ± 2.44 (0–9) | 0.150 | |
| Magnification | 1.94 ± 1.87 (0–6) | 1.31 ±1.65 (0–7) | 0.158 | |
| Total Score | 7.00 ± 6.17 (0–21) | 5.03 ± 5.69 (0–20) | 0.187 | |
| Variables | Measurement | Dry Needling Group (n = 33) | Placebo Group (n = 32) | p-Value * | Effect Size Cohen’s d | |
|---|---|---|---|---|---|---|
| SC (µs) | Baseline | 2.95 ± 1.57 | 2.33 ± 1.26 | 0.082 | 0.43 | |
| Needling | 8.42 ± 4.06 | 7.71 ± 3.22 | 0.437 | 0.19 | ||
| Post-1 | 7.43 ± 3.43 | 6.01 ± 2.54 | 0.063 | 0.47 | ||
| Post-2 | 4.76 ± 2.49 | 4.12 ± 2.32 | 0.288 | 0.27 | ||
| HR | Baseline | 65.76 ± 11.29 | 68.39 ± 10.30 | 0.329 | 0.24 | |
| Needling | 78.93 ± 14.61 | 72.40 ± 16.51 | 0.096 | 0.42 | ||
| Post-1 | 66.50 ± 11.46 | 65.69 ± 12.04 | 0.784 | 0.07 | ||
| Post-2 | 62.96 ± 10.93 | 65.42 ± 10.08 | 0.349 | 0.23 | ||
| Temperature (°C) | Baseline | 30.81 ± 4.12 | 31.78 ± 3.79 | 0.275 | 0.24 | |
| Needling | 31.21 ± 3.88 | 31.72 ± 3.28 | 0.328 | 0.14 | ||
| Post-1 | 31.13 ± 3.82 | 31.64 ± 3.29 | 0.572 | 0.14 | ||
| Post-2 | 31.51 ± 3.93 | 32.61 ± 3.17 | 0.567 | 0.31 | ||
| BR | Baseline | 15.61 ± 3.48 | 14.03 ± 4.10 | 0.099 | 0.42 | |
| Needling | 21.26 ± 4.18 | 19.44 ± 4.01 | 0.079 | 0.44 | ||
| Post-1 | 19.24 ± 3.61 | 18.27 ± 4.29 | 0.326 | 0.25 | ||
| Post-2 | 16.52 ± 3.33 | 15.76 ± 5.14 | 0.478 | 0.18 | ||
| Cortisol (µg/dL) | Baseline | 0.53 ± 0.29 | 0.55 ± 0.27 | 0.734 | 0.07 | |
| Post-test | 0.59 ± 0.33 | 0.57 ± 0.32 | 0.822 | 0.06 | ||
| PPT (Kg/cm2) | Thumb adductor | Baseline | 2.13 ± 0.35 | 2.18 ± 0.43 | 0.562 | 0.13 |
| Post-test | 2.72 ± 0.39 | 2.37 ± 0.43 | 0.001 | 0.85 | ||
| Anterior Tibialis | Baseline | 4.96 ± 0.59 | 5.04 ± 0.64 | 0.630 | 0.13 | |
| Post-test | 5.57 ± 0.56 | 5.23 ± 0.62 | 0.022 | 0.58 | ||
| NRS Pain | Post-test | 5.87 ± 2.01 | 1.09 ± 1.17 | 0.001 | 2.89 | |
| Variables | % Change between Measurements | Dry Needling Group (n = 33) | Placebo Group (n = 32) | p-Value * | Effect Size Cohen’s d |
|---|---|---|---|---|---|
| SC | Baseline to Needling | 248.89 ± 37.66 | 323.14 ± 47.48 | 0.224 | 0.30 |
| Baseline to Post-1 | 214.45 ± 40.51 | 225.74 ± 36.02 | 0.836 | 0.05 | |
| Baseline to Post-2 | 72.13 ± 10.54 | 90.91 ± 15.17 | 0.311 | 0.25 | |
| Needling to Post-1 | −10.36 ± 1.96 | −21.50 ± 1.99 | 0.001 | 0.98 | |
| Needling to Post-2 | −41.78 ± 3.79 | −45.39 ± 4.03 | 0.518 | 0.16 | |
| Post-1 to Post-2 | −35.16 ± 3.86 | −31.28 ± 4.51 | 0.516 | 0.16 | |
| HR | Baseline to Needling | 20.60 ± 2.88 | 5.33 ± 2.32 | 0.001 | 1.02 |
| Baseline to Post-1 | 1.40 ± 1.52 | −4.10 ± 1.17 | 0.006 | 0.71 | |
| Baseline to Post-2 | −4.07 ± 1.05 | −4.20 ± 0.90 | 0.927 | 0.02 | |
| Needling to Post-1 | −15.10 ± 1.47 | −8.00 ± 1.67 | 0.002 | 0.79 | |
| Needling to Post-2 | −19.15 ± 1.92 | −7.81 ± 1.98 | 0.001 | 1.02 | |
| Post-1 to Post-2 | −4.87 ± 8.39 | 0.16 ± 1.06 | 0.007 | 0.69 | |
| Temperature | Baseline to Needling | 1.51 ± 0.78 | 0.14 ± 0.98 | 0.275 | 0.27 |
| Baseline to Post-1 | 1.27 ± 0.78 | −0.11 ± 0.99 | 0.280 | 0.27 | |
| Baseline to Post-2 | 2.59 ± 1.25 | 3.09 ± 1.20 | 0.773 | 0.07 | |
| Needling to Post-1 | −0.23 ± 0.13 | −0.25 ± 0.16 | 0.961 | 0.02 | |
| Needling to Post-2 | 1.01 ± 0.72 | 2.96 ± 0.69 | 0.055 | 0.49 | |
| Post-1 to Post-2 | 1.25 ± 0.70 | 3.21 ± 0.65 | 0.045 | 0.51 | |
| BR | Baseline to Needling | 43.13 ± 8.04 | 47.05 ± 7.66 | 0.725 | 0.09 |
| Baseline to Post-1 | 29.32 ± 7.08 | 36.82 ± 7.08 | 0.457 | 0.19 | |
| Baseline to Post-2 | 9.24 ± 5.04 | 15.04 ± 5.46 | 0.438 | 0.19 | |
| Needling to Post-1 | −7.98 ± 2.77 | −4.70 ± 3.63 | 0.473 | 0.18 | |
| Needling to Post-2 | −20.56 ± 3.04 | −18.47 ± 3.87 | 0.671 | 0.11 | |
| Post-1 to Post-2 | −12.03 ± 3.47 | −12.61 ± 3.94 | 0.912 | 0.03 | |
| Cortisol | Baseline to Post-test | 11.27 ± 4.76 | 1.51 ± 3.08 | 0.920 | 0.42 |
| PPT | Thumb adductor | 28.57 ± 2.16 | 9.09 ± 1.40 | 0.001 † | 1.87 |
| Anterior Tibialis | 12.69 ± 1.19 | 3.94 ± 0.59 | 0.001 † | 1.61 |
| % Change between Measurements | NRS Dry Needling Group (n = 33) | NRS Placebo Group (n = 32) | ||
|---|---|---|---|---|
| Pearson’s Correlation Coefficient (r) | p-Value | Pearson’s Correlation Coefficient (r) | p-Value | |
| SC Baseline—Needling | 0.183 | 0.307 | 0.011 | 0.951 |
| HR Baseline—Needling | 0.049 | 0.786 | 0.039 | 0.833 |
| Temperature Baseline—Needling | −0.227 | 0.204 | 0.033 | 0.857 |
| BR Baseline—Needling | −0.015 | 0.933 | −0.127 | 0.488 |
| Cortisol Baseline—Post-test | 0.102 | 0.572 | 0.117 | 0.523 |
| Variables | % Change between Measurements | BDI-II | State Anxiety | Trait Anxiety | PCS Total |
|---|---|---|---|---|---|
| SC | Baseline to Needling | r = 0.024 | r = 0.037 | r = −0.016 | r = −0.129 |
| p = 0.895 | p = 0.840 | p = 0.929 | p = 0.473 | ||
| Needling to Post-1 | r = 0.096 | r = 0.093 | r = 0.291 | r = −0.122 | |
| p = 0.596 | p = 0.606 | p = 0.100 | p = 0.500 | ||
| Post-1 to Post-2 | r = −0.044 | r = 0.039 | r = 0.202 | r = 0.126 | |
| p = 0.806 | p = 0.828 | p = 0.259 | p = 0.484 | ||
| HR | Baseline to Needling | r = 0.016 | r = −0.070 | r = −0.142 | r = −0.079 |
| p = 0.929 | p = 0.700 | p = 0.429 | p = 0.662 | ||
| Needling to Post-1 | r = −0.219 | r = −0.006 | r = 0.052 | r = −0.047 | |
| p = 0.220 | p = 0.974 | p = 0.774 | p = 0.797 | ||
| Post-1 to Post-2 | r = 0.048 | r = 0.077 | r = 0.072 | r = 0.081 | |
| p = 0.790 | p = 0.670 | p = 0.689 | p = 0.654 | ||
| Temperature | Baseline to Needling | r = 0.007 | r = −0.060 | r = 0.041 | r = −0.134 |
| p = 0.970 | p = 0.738 | p = 0.822 | p = 0.458 | ||
| Needling to Post-1 | r = 0.091 | r = 0.350 | r = 0.290 | r = 0.202 | |
| p = 0.614 | p = 0.046 | p = 0.101 | p = 0.259 | ||
| Post-1 to Post-2 | r = 0.058 | r = −0.080 | r = 0.143 | r = −0.130 | |
| p = 0.748 | p = 0.659 | p = 0.427 | p = 0.471 | ||
| BR | Baseline to Needling | r = 0.002 | r = 0.023 | r = 0.014 | r = −0.291 |
| p = 0.990 | p = 0.899 | p = 0.940 | p = 0.101 | ||
| Needling to Post-1 | r = −0.006 | r = −0.203 | r = −0.003 | r = −0.126 | |
| p = 0.974 | p = 0.258 | p = 0.986 | p = 0.486 | ||
| Post-1 to Post-2 | r = −0.035 | r = 0.061 | r = −0.85 | r = 0.393 | |
| p = 0.845 | p = 0.735 | p = 0.637 | p = 0.024 | ||
| Cortisol | Baseline to Post-test | r = 0.043 | r = 0.211 | r = −0.067 | r = 0.042 |
| p = 0.813 | p = 0.239 | p = 0.713 | p = 0.815 |
| Variables | % Change between Measurements | BDI-II | State Anxiety | Trait Anxiety | PCS Total |
|---|---|---|---|---|---|
| SC | Baseline to Needling | r = 0.157 | r = 0.013 | r = −0.041 | r = 0.001 |
| p = 0.392 | p = 0.943 | p = 0.823 | p = 0.999 | ||
| Needling to Post-1 | r = −0.055 | r = 0.072 | r = 0.045 | r = 0.078 | |
| p = 0.767 | p = 0.695 | p = 0.807 | p = 0.673 | ||
| Post-1 to Post-2 | r = −0.153 | r = −0.196 | r = −0.093 | r = 0.179 | |
| p = 0.403 | p = 0.283 | p = 0.612 | p = 0.327 | ||
| HR | Baseline to Needling | r = 0.111 | r = −0.039 | r = 0.070 | r = 0.009 |
| p = 0.544 | p = 0.834 | p = 0.705 | p = 0.961 | ||
| Needling to Post-1 | r = −0.120 | r = 0.074 | r = 0.035 | r = 0.050 | |
| p = 0.514 | p = 0.689 | p = 0.851 | p = 0.786 | ||
| Post-1 to Post-2 | r = −0.086 | r = −0.254 | r = −0.196 | r = −0.36 | |
| p = 0.639 | p = 0.161 | p = 0.282 | p = 0.846 | ||
| Temperature | Baseline to Needling | r = −0.121 | r = 0.053 | r = 0.024 | r = 0.222 |
| p = 0.510 | p = 0.775 | p = 0.895 | p = 0.222 | ||
| Needling to Post-1 | r = 0.111 | r = 0.056 | r = 0.160 | r = −0.076 | |
| p = 0.544 | p = 0.761 | p = 0.381 | p = 0.678 | ||
| Post-1 to Post-2 | r = 0.061 | r = 0.016 | r = −0.119 | r = −0.025 | |
| p = 0.741 | p = 0.932 | p = 0.517 | p = 0.890 | ||
| BR | Baseline to Needling | r = 0.042 | r = 0.098 | r = 0.211 | r = −0.159 |
| p = 0.819 | p = 0.593 | p = 0.247 | p = 0.385 | ||
| Needling to Post-1 | r = −0.139 | r = 0.138 | r = 0.053 | r = 0.155 | |
| p = 0.447 | p = 0.453 | p = 0.773 | p = 0.398 | ||
| Post-1 to Post-2 | r = −0.018 | r = −0.354 | r = −0.325 | r = 0.002 | |
| p = 0.923 | p = 0.047 | p = 0.069 | p = 0.993 | ||
| Cortisol | Baseline to Post-test | r = −0.407 | r = −0.416 | r = −0.371 | r = 0.064 |
| p = 0.021 | p = 0.018 | p = 0.037 | p = 0.728 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lázaro-Navas, I.; Lorenzo-Sánchez-Aguilera, C.; Pecos-Martín, D.; Jiménez-Rejano, J.J.; Navarro-Santana, M.J.; Fernández-Carnero, J.; Gallego-Izquierdo, T. Immediate Effects of Dry Needling on the Autonomic Nervous System and Mechanical Hyperalgesia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 6018. https://doi.org/10.3390/ijerph18116018
Lázaro-Navas I, Lorenzo-Sánchez-Aguilera C, Pecos-Martín D, Jiménez-Rejano JJ, Navarro-Santana MJ, Fernández-Carnero J, Gallego-Izquierdo T. Immediate Effects of Dry Needling on the Autonomic Nervous System and Mechanical Hyperalgesia: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(11):6018. https://doi.org/10.3390/ijerph18116018
Chicago/Turabian StyleLázaro-Navas, Irene, Cristina Lorenzo-Sánchez-Aguilera, Daniel Pecos-Martín, Jose Jesús Jiménez-Rejano, Marcos Jose Navarro-Santana, Josué Fernández-Carnero, and Tomás Gallego-Izquierdo. 2021. "Immediate Effects of Dry Needling on the Autonomic Nervous System and Mechanical Hyperalgesia: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 11: 6018. https://doi.org/10.3390/ijerph18116018
APA StyleLázaro-Navas, I., Lorenzo-Sánchez-Aguilera, C., Pecos-Martín, D., Jiménez-Rejano, J. J., Navarro-Santana, M. J., Fernández-Carnero, J., & Gallego-Izquierdo, T. (2021). Immediate Effects of Dry Needling on the Autonomic Nervous System and Mechanical Hyperalgesia: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 18(11), 6018. https://doi.org/10.3390/ijerph18116018