
Lumbar Roll Usage While Sitting Reduces the Forward Head Posture in Healthy Individuals: A Systematic Review with Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Identification and Selection of Studies
2.2. Assessment of the Studies’ Characteristics
2.3. Data Analysis
3. Results
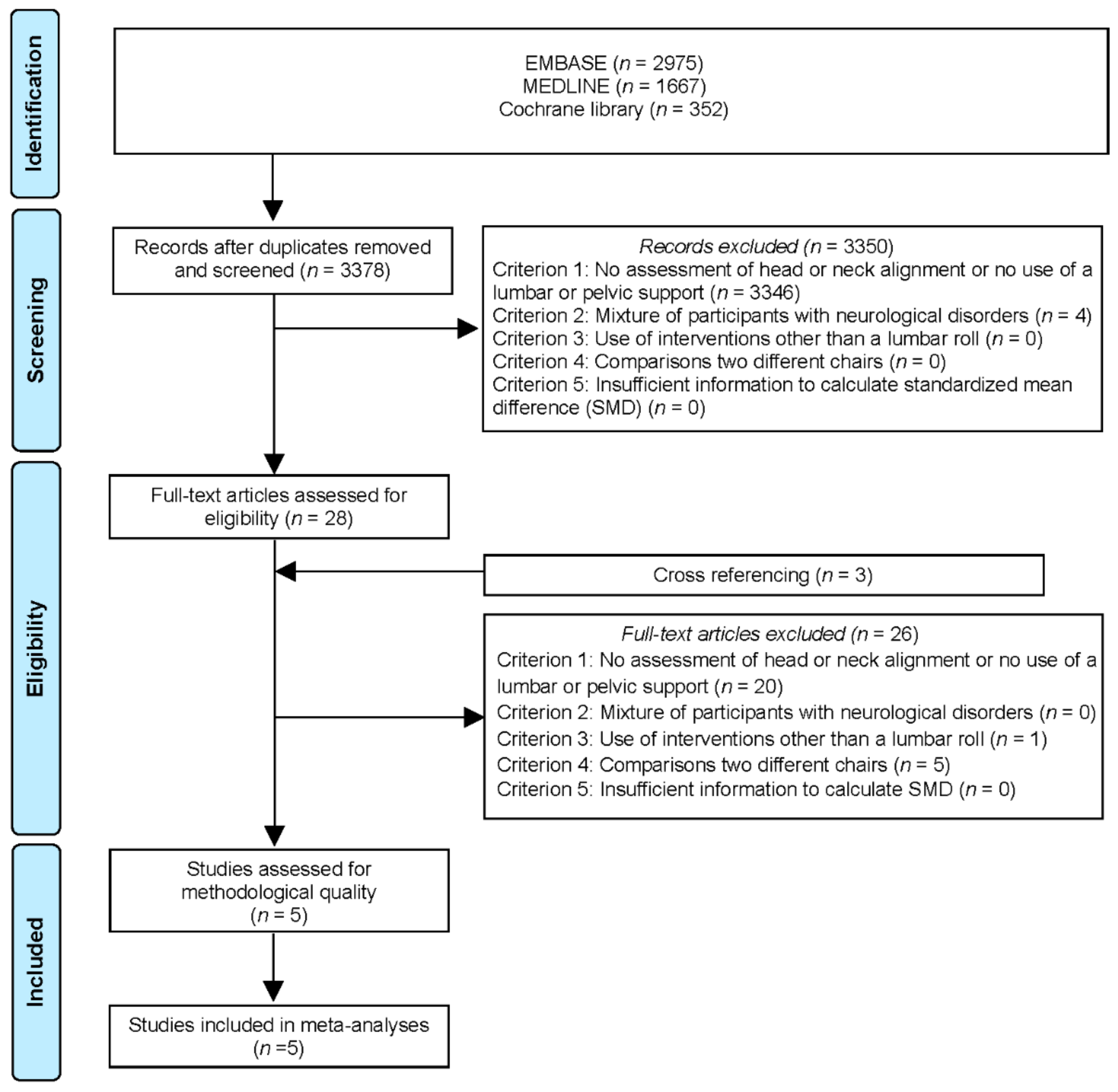
3.1. Flow of Study Selection
3.2. Characteristics of Studies
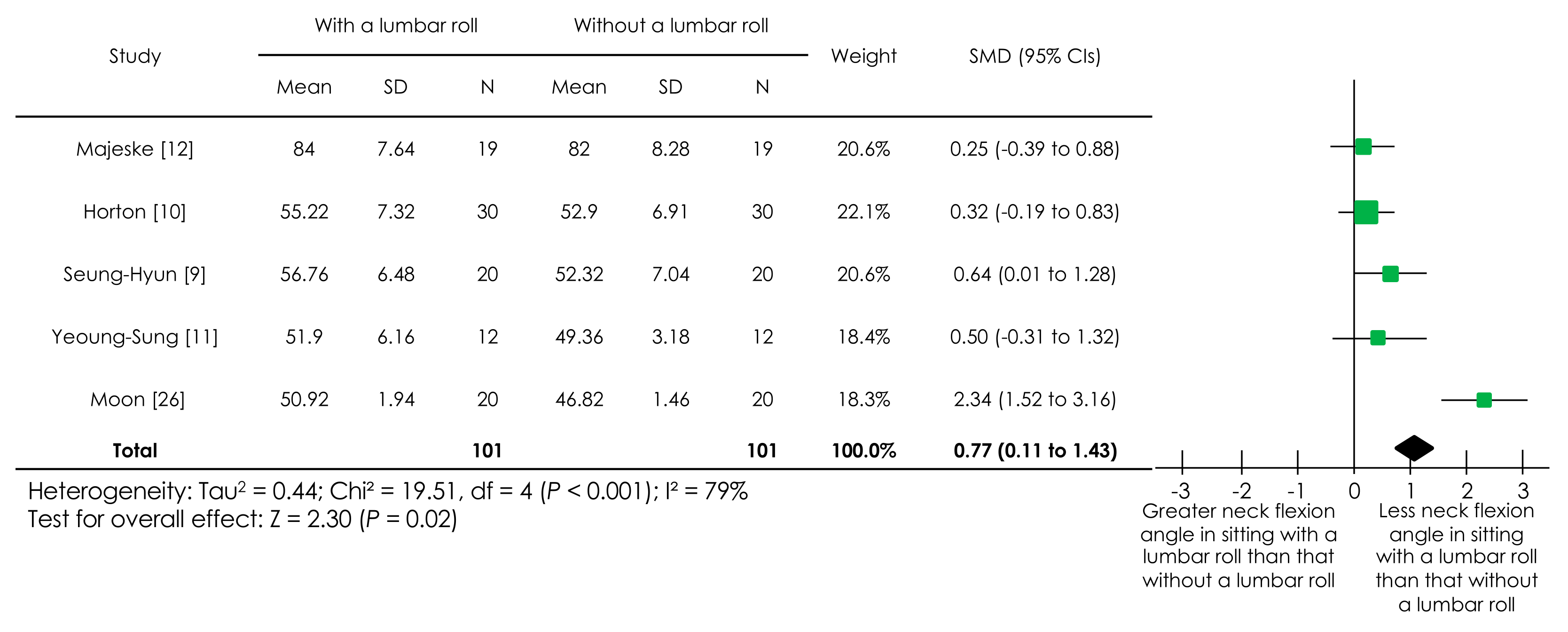
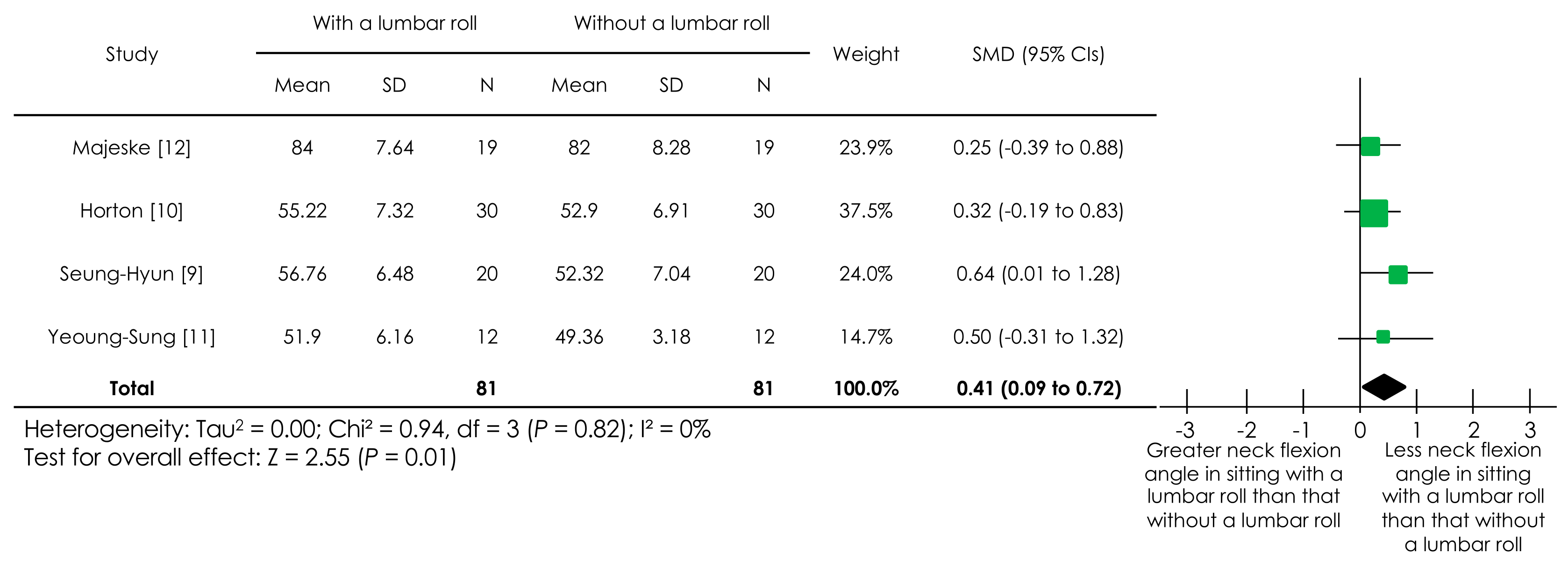
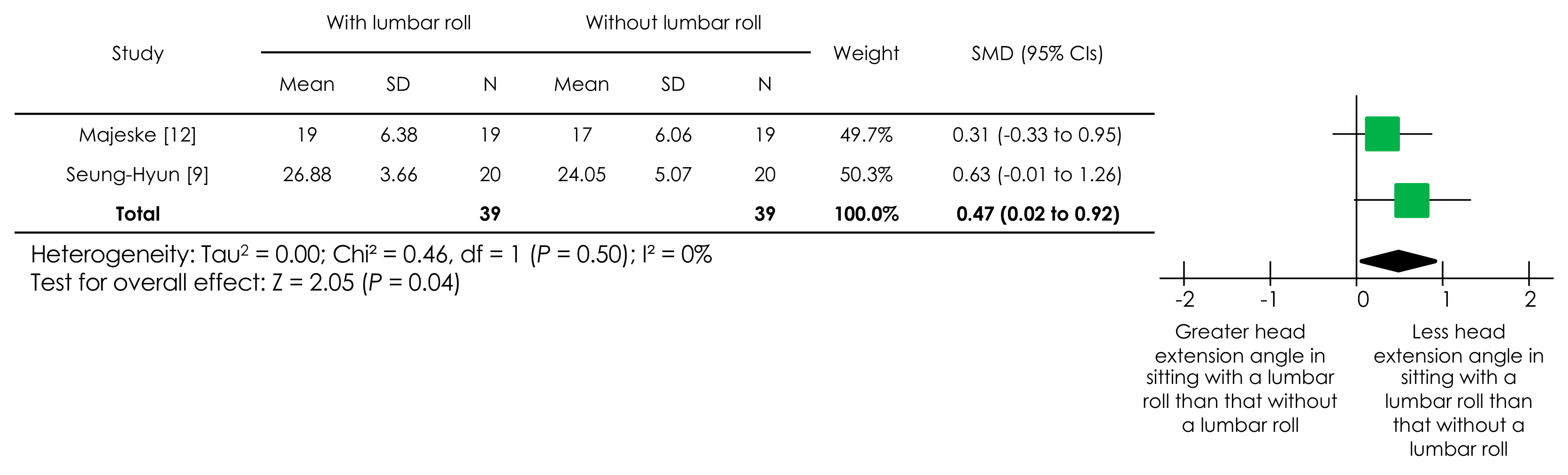
Effect of Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Visscher, C.M.; de Boer, W.; Naeije, M. The relationship between posture and curvature of the cervical spine. J. Manip. Physiol. Ther. 1998, 21, 388–391. [Google Scholar]
- Mayer, J.; Kraus, T.; Ochsmann, E. Longitudinal evidence for the association between work-related physical exposures and neck and/or shoulder complaints: A systematic review. Int. Arch. Occup. Environ. Health 2012, 85, 587–603. [Google Scholar] [CrossRef] [PubMed]
- Charles, L.E.; Ma, C.C.; Burchfiel, C.M.; Dong, R.G. Vibration and ergonomic exposures associated with musculoskeletal disorders of the shoulder and neck. Saf. Health Work 2018, 9, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-de-las-Penas, C.; Alonso-Blanco, C.; Cuadrado, M.L.; Gerwin, R.D.; Pareja, J.A. Trigger points in the suboccipital muscles and forward head posture in tension-type headache. Headache 2006, 46, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-de-las-Penas, C.; Alonso-Blanco, C.; Cuadrado, M.L.; Pareja, J.A. Forward head posture and neck mobility in chronic tension-type headache: A blinded, controlled study. Cephalalgia 2006, 26, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Mingels, S.; Dankaerts, W.; van Etten, L.; Thijs, H.; Granitzer, M. Comparative analysis of head-tilt and forward head position during laptop use between females with postural induced headache and healthy controls. J. Bodyw. Mov. Ther. 2016, 20, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Shaghayegh Fard, B.; Ahmadi, A.; Maroufi, N.; Sarrafzadeh, J. Evaluation of forward head posture in sitting and standing positions. Eur. Spine J. 2016, 25, 3577–3582. [Google Scholar] [CrossRef] [PubMed]
- Caneiro, J.P.; O’Sullivan, P.; Burnett, A.; Barach, A.; O’Neil, D.; Tveit, O.; Olafsdottir, K. The influence of different sitting postures on head/neck posture and muscle activity. Man. Ther. 2010, 15, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Seung-Hyun, K.; Yu-Shin, K. Influence of the lumbar spine adjustment using the lumbar roll support on head and neck posture in older adults. J. Korea Contents Assoc. 2011, 9, 800–806. [Google Scholar]
- Horton, S.J.; Johnson, G.M.; Skinner, M.A. Changes in head and neck posture using an office chair with and without lumbar roll support. Spine (Phila PA 1976) 2010, 35, E542–E548. [Google Scholar] [CrossRef]
- Yeoung-Sung, K.; Han-Kyu, P.; Min-Chull, P. Research the effects of thoracic and lumbar support fixtures on forward head posture during visual display terminal work. J. Korean Soc. Phys. Med. 2016, 11, 41–47. [Google Scholar]
- Majeske, C.; Buchanan, C. Quantitative description of two sitting postures: With and without a lumbar support pillow. Phys. Ther. 1984, 64, 1531–1535. [Google Scholar] [CrossRef]
- Ghogomu, E.A.; Maxwell, L.J.; Buchbinder, R. Updated method guidelines for cochrane musculoskeletal group systematic reviews and metaanalyses. J. Rheumatol. 2014, 41, 194–205. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research; Chapman & Hall: London, UK, 1991. [Google Scholar]
- Takasaki, H.; Miki, T. The impact of continuous use of lumbosacral orthoses on trunk motor performance: A systematic review with meta-analysis. Spine J. 2017, 17, 889–900. [Google Scholar] [CrossRef]
- Wells, C.; Kolt, G.S.; Marshall, P.; Hill, B.; Bialocerkowski, A. The effectiveness of pilates exercise in people with chronic low back pain: A systematic review. PLoS ONE 2014, 9, e100402. [Google Scholar] [CrossRef]
- Hori, M.; Hasegawa, H.; Takasaki, H. Comparisons of hamstring flexibility between individuals with and without low back pain: Systematic review without low back pain: Systematic review with meta-analysis. Physiother. Theory Pract. 2019, 18, 1–24. [Google Scholar]
- Daly, A.E.; Bialocerkowski, A.E. Does evidence support physiotherapy management of adult Complex Regional Pain Syndrome Type One? A systematic review. Eur. J. Pain 2009, 13, 339–353. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Sultan, S.; Glasziou, P.; Akl, E.A.; Alonso-Coello, P.; Atkins, D.; Kunz, R.; Brozek, J.; Montori, V.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Sultan, S.; Glasziou, P.; Akl, E.A.; Alonso-Coello, P.; Atkins, D.; Kunz, R.; Brozek, J.; Montori, V.; et al. GRADE guidelines: 9. Rating up the quality of evidence. J. Clin. Epidemiol. 2011, 64, 1311–1316. [Google Scholar] [CrossRef]
- Pollock, A.; Farmer, S.E.; Brady, M.C.; Langhorne, P.; Mead, G.E.; Mehrholz, J.; van Wijck, F.; Wiffen, P.J. An algorithm was developed to assign GRADE levels of evidence to comparisons within systematic reviews. J. Clin. Epidemiol. 2016, 70, 106–110. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE guidelines: 8. Rating the quality of evidence—Indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. GRADE guidelines: 5. Rating the quality of evidence—Publication bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Moon, J.H.; Jung, J.H.; Hahm, S.C.; Oh, H.K.; Jung, K.S.; Cho, H.Y. Effects of lumbar lordosis assistive support on craniovertebral angle and mechanical properties of the upper trapezius muscle in subjects with forward head posture. J. Phys. Ther. Sci. 2018, 30, 457–460. [Google Scholar] [CrossRef]
- Mahmoud, N.F.; Hassan, K.A.; Abdelmajeed, S.F.; Moustafa, I.M.; Silva, A.G. The relationship between forward head posture and neck pain: A systematic review and meta-analysis. Curr. Rev. Musculoskelet. Med. 2019, 12, 562–577. [Google Scholar] [CrossRef]
- Korakakis, V.; O’Sullivan, K.; O’Sullivan, P.B.; Evagelinou, V.; Sotiralis, Y.; Sideris, A.; Sakellariou, K.; Karanasios, S.; Giakas, G. Physiotherapist perceptions of optimal sitting and standing posture. Musculoskelet. Sci. Pract. 2019, 39, 24–31. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Corresponding Author Responded or Not or Not Contacted, and the Source of Funding | Design | Participants (N, Important Eligibility Criteria, Age, Gender) | Interventions (Lumbar Roll, Backrest Angle) | Comparisons (Measurement Time Points) | Outcomes (Measures, Measurement Tools, Other Outcome Measures Not Included in the Current Review) |
|---|---|---|---|---|---|
| Yeoung-Sung [11] Not responded Not described | Randomized controlled design | Total: N = 36 Healthy male students Control group (n = 12) Thoracic support group (n = 12) Lumbar support group (n = 12) Age: 26.2 ± 2.7 years Gender: 36 men | Air-mesh and high elastic urethane materials (39 cm wide, 32 cm long, and 8 cm thick) Backrest angles of 90–100° | Immediately after using the lumbar roll while visual display terminal work 20 min after using the lumbar roll while visual display terminal work | Neck: Cranio-vertebral angle 1 Measurement tool: Digital image analysis Other objective measures that were not included in this review: Angle between a line from the spinous process of C7 through the tragus of the ear and a line from the tragus of the ear through the eye |
| Moon [26] Not contacted Not described | Randomized controlled design (cross-over) | Total: N = 20 Individuals with the cranio-vertebral angle < 51° Age: 26.6 ± 3.8 years Gender: 10 women and 10 men | Lumbar lordosis assistive support (Chiropractic cushion, Balancecord Inc., Republic of Korea) at L2–4 level Backrest angles of 90° | Immediately after using the lumbar roll while relaxed sitting | Neck: Cranio-vertebral angle 1 Measurement tool: Digital image analysis Other objective measures that were not included in this review: Muscle tone, stiffness, and viscoelasticity of the upper trapezius muscle in a sitting position |
| Horton [10] Not contacted No funding | Before–after design (Quasi-randomized controlled design) | Total: N = 30 Healthy males Age: 21.7 ± 3.3 years Gender: 30 men | McKenzie lumbar roll (length (28 cm), diameter (13 cm), and foam density (28 kg/m3)) Backrest angles of 90°, 100°, and 110° | Immediately after using the lumbar roll while relaxed sitting | Neck: Cranio-vertebral angle 1 Measurement tool: Image analysis Other objective measures that were not included in this review: None |
| Seung-Hyun [9] Not contacted Not described | Before–after design (Quasi-randomized controlled design) | Total: N = 20 Healthy individuals Age: 71 ± 3.6 yearsGender: 1 man, 19 women | McKenzie lumbar roll (length: 28 cm, diameter: 11 cm) Backrest angles of 90° | One minute after using the lumbar roll while watching a TV program on a visual display | Head: The angle between a horizontal line through the tragus of the ear and a line from the tragus of the ear through the eye Neck: Cranio-vertebral angle 1 Measurement tool: Image analysis Other objective measures that were not included in this review: None |
| Majeske [12] Not contacted Not described | Before–after design (Quasi-randomized controlled design) | Total: N = 19 Healthy individuals Age: 27.7 ± 5.8 years Gender: 10 women and 9 men | Body Therapeutics at L3 level Backrest angles of 105° | Immediately after using the lumbar roll while relaxed sitting | Head: The angle between a horizontal line through the tragus of the ear and a line from the tragus of the ear through the eye Neck: The angle between a horizontal line through the acromion and a line from the acromion through the tragus of the ear Measurement tool: Analog image analysis Other objective measures that were not included in this review: Angles of trunk, pelvis, upper arm and forearm, and sitting height |
| Studies | Criterion No. | Total | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | ||
| Yeoung-Sung [11] | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 13 |
| Moon [26] | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 13 |
| Horton [10] | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 12 |
| Seung-Hyun [9] | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 |
| Majeske [12] | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 11 |
| Quality Assessment | Summary of Findings | |||||||
|---|---|---|---|---|---|---|---|---|
| No. of Studies | Risk of Bias | Imprecision | Inconsistency | Indirectness | Publication Bias | No. of Participants (with a Lumbar Roll/without a Lumbar Roll) | Pooled Standardized Mean Difference (95% Confidence Intervals) | Quality of Evidence |
| Neck angle | ||||||||
| 5 | No serious limitation due to only studies with acceptable methodological quality, do not downgrade (low quality) | Very serious imprecision due to very limited sample sizes, rate down one level (i.e., from low to very low quality) | Serious inconsistency due to statistically significant evidence of heterogeneity (p < 0.001), rate down one level (i.e., from low to very low quality) | Serious indirectness due to inclusion of not completely the same measurements, rate down one level (i.e., from low to very low quality) | Likely due to available evidence from several small studies, rate down one level (i.e., from low to very low quality) | 101/101 | 0.77(0.11 to 1.43) | ⊕〇〇〇 Very Low |
| Head angle | ||||||||
| 2 | No serious limitation due to only studies with acceptable methodological quality, do not downgrade (low quality) | Very serious imprecision due to very limited sample sizes, rate down two levels (i.e., from low to very low quality) | No serious inconsistency, do not downgrade (low quality) | Serious indirectness due to inclusion of clinically different populations, rate down one level (i.e., from low to very low quality) | Likely due to available evidence from several small studies, rate down one level (i.e., from low to very low quality) | 39/39 | 0.47(0.02 to 0.92) | ⊕〇〇〇 Very Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Handa, Y.; Okada, K.; Takasaki, H. Lumbar Roll Usage While Sitting Reduces the Forward Head Posture in Healthy Individuals: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 5171. https://doi.org/10.3390/ijerph18105171
Handa Y, Okada K, Takasaki H. Lumbar Roll Usage While Sitting Reduces the Forward Head Posture in Healthy Individuals: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(10):5171. https://doi.org/10.3390/ijerph18105171
Chicago/Turabian StyleHanda, Yusuke, Kenya Okada, and Hiroshi Takasaki. 2021. "Lumbar Roll Usage While Sitting Reduces the Forward Head Posture in Healthy Individuals: A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 10: 5171. https://doi.org/10.3390/ijerph18105171
APA StyleHanda, Y., Okada, K., & Takasaki, H. (2021). Lumbar Roll Usage While Sitting Reduces the Forward Head Posture in Healthy Individuals: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health, 18(10), 5171. https://doi.org/10.3390/ijerph18105171