Application of a Modified Entropy Computational Method in Assessing the Complexity of Pulse Wave Velocity Signals in Healthy and Diabetic Subjects


 ,
, 

Abstract
:
1. Introduction
2. Methods
2.1. Subject Population and Grouping
2.2. Measurement Protocol
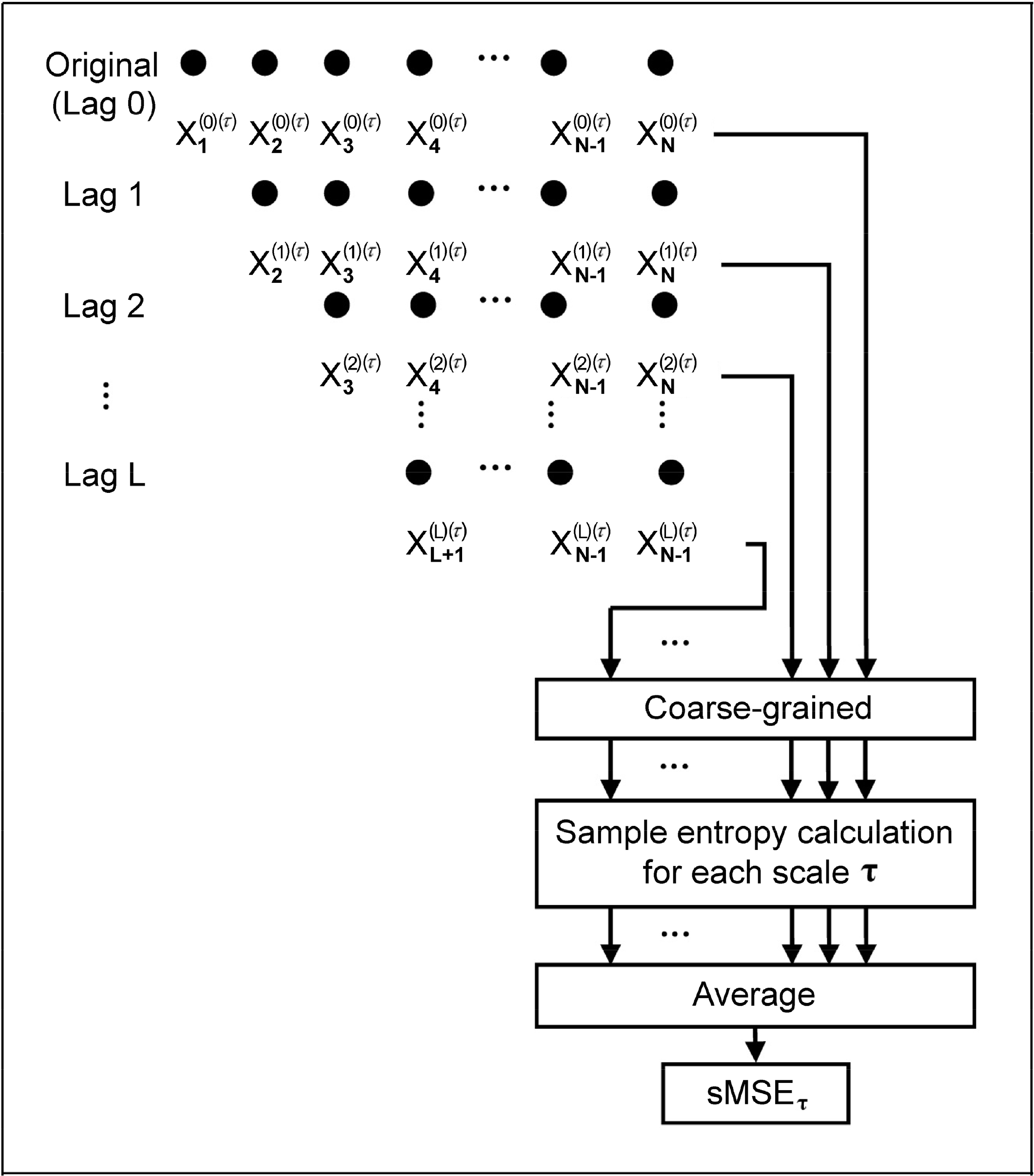
2.3. Short Time Multiscale Entropy (sMSE)
2.4. Short Time Multi-scale Entropy Index (sMEI) Using PWV Series
2.5. Study Design
2.6. Statistical Analysis
3. Results
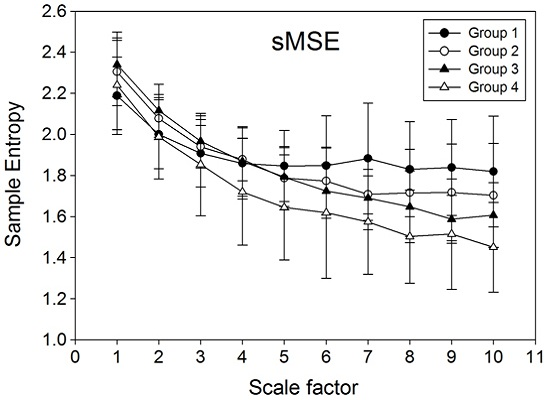
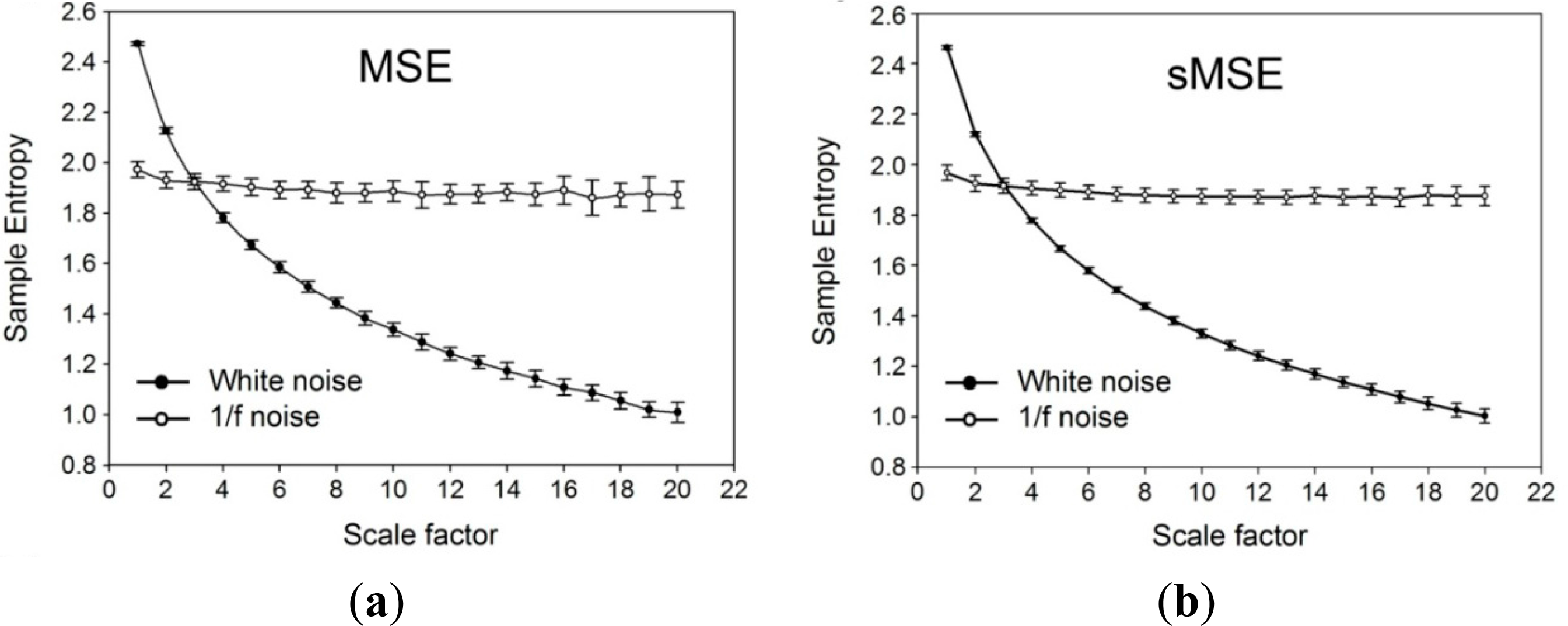
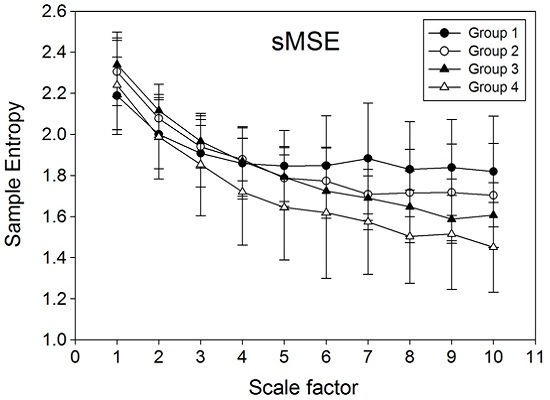
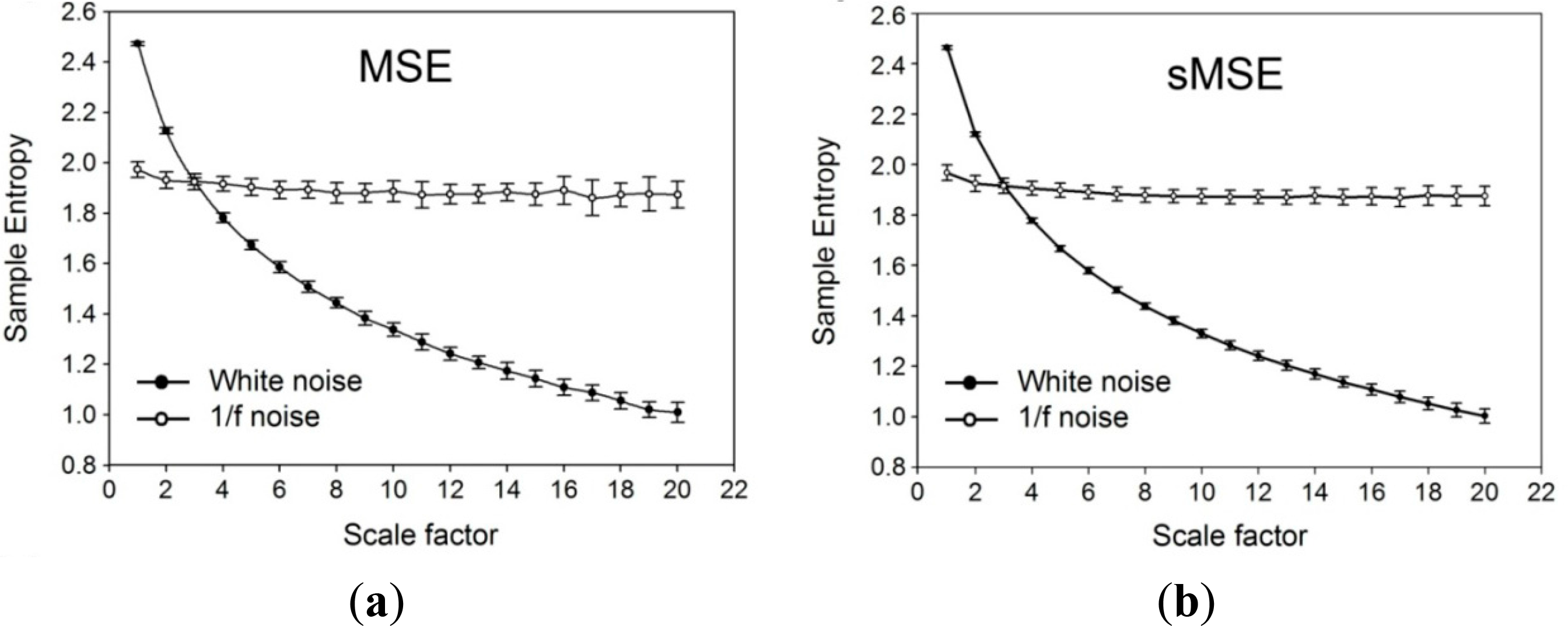
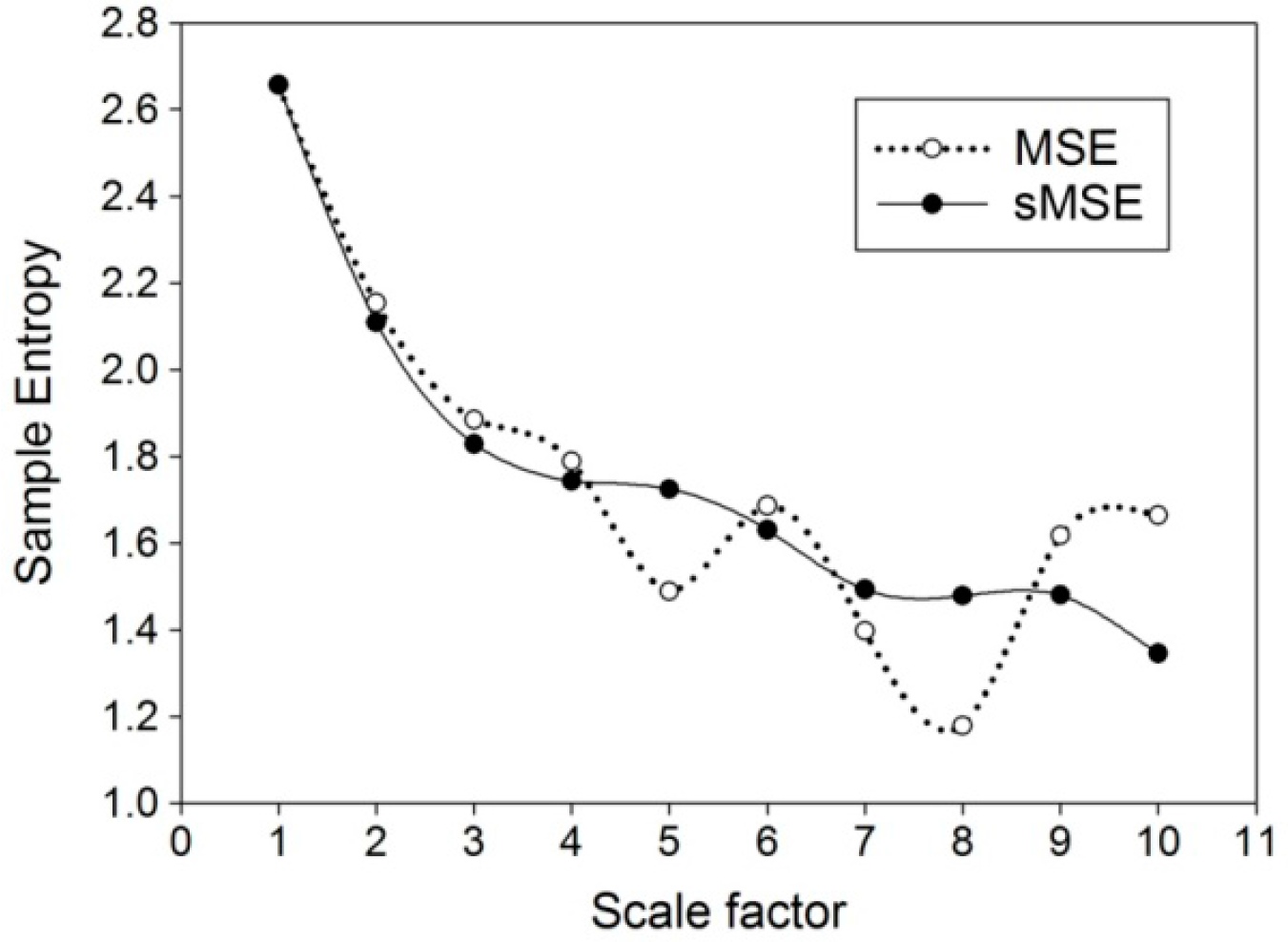
3.1. Computation of Sample Entropy Using Multi-Scale Entropy (MSE) and Short Time Multi-Scale Entropy (sMSE) Methods on Simulation Signals
3.2. Demographic and Biochemical Parameters
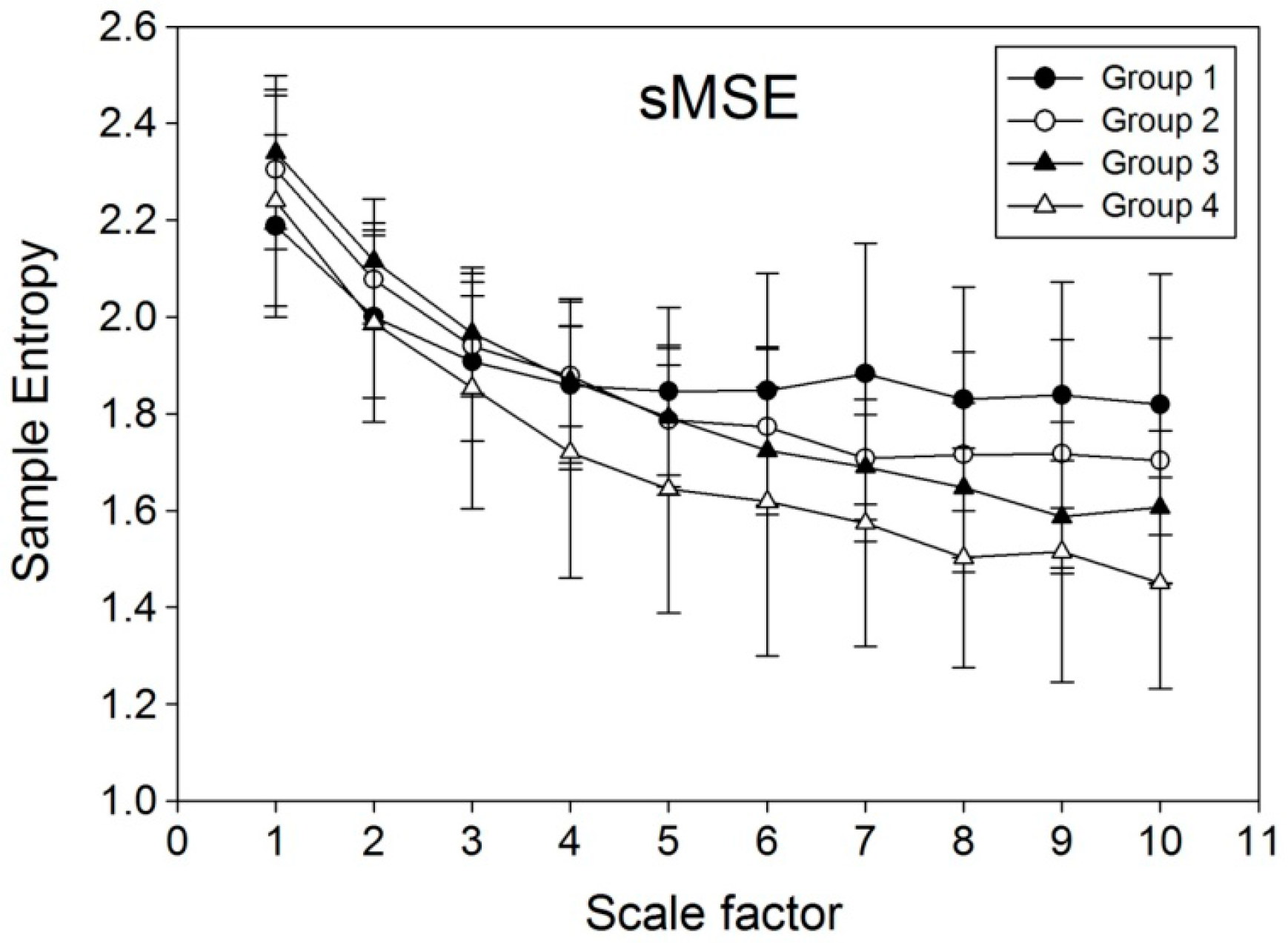
3.3. Comparisons among PWV1000, MEISS (PWV1000), MEILS (PWV1000), MEISS (PWV600), MEILS (PWV600), sMEISS (PWV600) and sMEILS (PWV600)
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Blacher, J.; Asmar, R.; Djane, S.; London, G.M.; Safar, M.E. Aortic pulse wave velocity as a marker of cardiovascular risk in hypertensive patients. Hypertension 1999, 33, 1111–1117. [Google Scholar]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 2001, 37, 1236–1241. [Google Scholar]
- Yamashina, A.; Tomiyama, H.; Takeda, K.; Tsuda, H.; Arai, T.; Hirose, K.; Koji, Y.; Hori, S.; Yamamoto, Y. Validity, reproducibility, and clinical significance of noninvasive brachial-ankle pulse wave velocity measurement. Hypertens. Res 2002, 25, 359–364. [Google Scholar]
- Mitchell, G.F.; Parise, H.; Benjamin, E.J.; Larson, M.G.; Keyes, M.J.; Vita, J.A.; Vasan, R.S.; Levy, D. Changes in arterial stiffness and wave reflection with advancing age in healthy men and women the Framingham Heart Study. Hypertension 2004, 43, 1239–1245. [Google Scholar]
- Tsai, W.C.; Chen, J.Y.; Wang, M.C.; Wu, H.T.; Chi, C.K.; Chen, Y.K.; Chen, J.H.; Lin, L.J. Association of Risk Factors With Increased Pulse Wave Velocity Detected by a Novel Method Using Dual-Channel Photoplethysmography*. Am. J. Hypertens 2005, 18, 1118–1122. [Google Scholar]
- Wu, H.T.; Hsu, P.C.; Liu, A.B.; Chen, Z.L.; Huang, R.M.; Chen, C.P.; Tang, C.J.; Sun, C.K. Six-channel ECG-based pulse wave velocity for assessing whole-body arterial stiffness. Blood Press 2012, 21, 167–176. [Google Scholar]
- Costa, M.; Goldberger, A.; Peng, C.K. Multiscale entropy to distinguish physiologic and synthetic RR time series. Proceedings of the IEEE Computers in Cardiology, Memphis, TN, USA, 22–25 September 2002; pp. 137–140.
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett 2002, 89. [Google Scholar] [CrossRef]
- Costa, M.; Healey, J. Multiscale entropy analysis of complex heart rate dynamics: discrimination of age and heart failure effects. Proceedings of the IEEE Computers in Cardiology, Thessaloniki Chalkidiki, Greece, 21–24 September 2003; pp. 705–708.
- Costa, M.; Peng, C.K.; Goldberger, A.L. Hausdorff JM Multiscale entropy analysis of human gait dynamics. Physica A 2003, 330, 53–60. [Google Scholar]
- Wu, H.T.; Hsu, P.C.; Lin, C.F.; Wang, H.J.; Sun, C.K.; Liu, A.B.; Lo, M.T.; Tang, C.J. Multiscale entropy analysis of pulse wave velocity for assessing atherosclerosis in the aged and diabetic. IEEE Trans. Biomed. Eng 2011, 58, 2978–2981. [Google Scholar]
- Ho, Y.L.; Lin, C.; Lin, Y.H.; Lo, M.T. The Prognostic Value of Non-Linear Analysis of Heart Rate Variability in Patients with Congestive Heart Failure—A Pilot Study of Multiscale Entropy. PLOS ONE 2011, 6. [Google Scholar] [CrossRef]
- Yuan, H.K.; Lin, C.; Tsai, P.H.; Chang, F.C.; Lin, K.P.; Hu, H.H.; Su, M.C.; Lo, M.T. Acute increase of complexity in the neurocardiovascular dynamics following carotid stenting. Acta Neurol. Scand 2011, 123, 187–192. [Google Scholar]
- Escudero, J.; Abásolo, D.; Hornero, R.; Espino, P.; López, M. Analysis of electroencephalograms in Alzheimer’s disease patients with multiscale entropy. Physiol. Meas 2006, 27, 1091–1106. [Google Scholar]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol.Heart Circ. Physiol 2000, 278, 2039–2049. [Google Scholar]
- Cecelja, M.; Chowienczyk, P. Dissociation of aortic pulse wave velocity with risk factors for cardiovascular disease other than hypertension a systematic review. Hypertension 2009, 54, 1328–1336. [Google Scholar]
- Chang, K.M.; Liu, S.H. Gaussian noise filtering from ECG by Wiener filter and ensemble empirical mode decomposition. J. Signal Process. Syst 2011, 64, 249–264. [Google Scholar]
- Wu, Z.; Huang, N.E. Ensemble empirical mode decomposition: a noise-assisted data analysis method. Adv. Adapt. Data Anal 2009, 1, 1–41. [Google Scholar]
- Lei, W.K.; Li, B.N.; Dong, M.C.; Vai, M.I. AFC-ECG: An adaptive fuzzy ECG classifier. In Soft Computing in Industrial Applications, Proceedings of The 12th Online World Conference on Soft Computing in Industrial Applications (WSC12), 16–26 October 2007; Springer: Berlin, Germany, 2007; pp. 189–199. [Google Scholar]
- Yang, A.C.C.; Hseu, S.S.; Yien, H.W.; Goldberger, A.L.; Peng, C.K. Linguistic analysis of the human heartbeat using frequency and rank order statistics. Phys. Rev. Lett 2003, 90. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Hausdorff, J.M.; Ivanov, P.C.; Peng, C.K.; Stanley, H.E. Fractal dynamics in physiology: Alterations with disease and aging. Proc. Natl. Acad. Sci. USA 2002, 99, 2466–2472. [Google Scholar]
- Tapanainen, J.M.; Thomsen, P.E.B.; Køber, L.; Torp-Pedersen, C.; Mäkikallio, T.H.; Still, A.M.; Lindgren, K.S.; Huikuri, H.V. Fractal analysis of heart rate variability and mortality after an acute myocardial infarction. Am.J. Cardiol 2002, 90, 347–352. [Google Scholar]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of biological signals. Phys.Rev. E 2005, 71. [Google Scholar] [CrossRef]
- Cheng, D.; Tsai, S.J.; Hong, C.J.; Yang, A.C. Reduced physiological complexity in robust elderly adults with the APOE ε4 allele. PLOS ONE 2009, 4. [Google Scholar] [CrossRef]
- Costa, M.D.; Peng, C.K.; Goldberger, A.L. Multiscale analysis of heart rate dynamics: Entropy and time irreversibility measures. Cardiovasc. Eng 2008, 8, 88–93. [Google Scholar]
- Manor, B.; Costa, M.D.; Hu, K.; Newton, E.; Starobinets, O.; Kang, H.G.; Peng, C.; Novak, V.; Lipsitz, L.A. Physiological complexity and system adaptability: evidence from postural control dynamics of older adults. J. Appl. Physiol 2010, 109, 1786–1791. [Google Scholar]
- Javorka, M.; Trunkvalterova, Z.; Tonhajzerova, I.; Javorkova, J.; Javorka, K.; Baumert, M. Short-term heart rate complexity is reduced in patients with type 1 diabetes mellitus. Clin. Neurophysiol 2008, 119, 1071–1081. [Google Scholar]
- Skinner, J.E.; Weiss, D.N.; Anchin, J.M.; Turianikova, Z.; Tonhajzerova, I.; Javorkova, J.; Javorka, K.; Baumert, M.; Javorka, M. Nonlinear PD2i heart rate complexity algorithm detects autonomic neuropathy in patients with type 1 diabetes mellitus. Clin. Neurophysiol 2011, 122, 1457–1462. [Google Scholar]
- Tarvainen, M.P.; Cornforth, D.J.; Kuoppa, P.; Lipponen, J.A.; Jelinek, H.F. Complexity of heart rate variability in type 2 diabetes-effect of hyperglycemia. In Engineering in Medicine and Biology Society (EMBC), Proceedings of 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC’13), Osaka, Japan, 3–7 July 2013; pp. 5558–5561.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group 1 | Group 2 | Group 3 | Group 4 |
|---|---|---|---|---|
| Number | 24 | 30 | 18 | 22 |
| Ages (years) | 25.8 ± 5.6 | 52.6 ± 6.6 ** | 56.5 ± 9.3 | 57.9 ± 9.5 |
| Duration of Diabetes (years) | 0 | 0 | 6.8 ± 3.8 | 11.7 ± 6.8 ++ |
| Circumference (cm) | 79.9 ± 10.8 | 84.3 ± 10.1 | 92.2 ± 10.1 ε | 96.7 ± 12.8 |
| BMI (kg/m2) | 22.6 ± 3.5 | 24.2 ± 3.9 | 26.9 ± 3.7 | 28.4 ± 5.2 |
| SBP (mmHg) | 115.5 ± 9.8 | 115.5 ± 14.4 | 129.8 ± 22.0 ε | 125.7 ± 19.4 |
| DBP (mmHg) | 70.1 ± 6.6 | 73.9 ± 10.0 | 78.5 ± 13.6 | 75.5 ± 10.8 |
| PP (mmHg) | 44.5 ± 6.6 | 41.1 ± 9.4 | 51.2 ± 12.3 ε | 45.1 ± 6.7 |
| HbA1c (%) | 5.5 ± 0.2 | 5.8 ± 0.4 * | 6.8 ± 0.7 εε | 9.53 ± 1.9 ++ |
| HDL (mg/dL) | 41.7 ± 11.5 | 49.4 ± 14.1 | 39.9 ± 11.4 | 43.2 ± 14.9 |
| Triglyceride (mg/dL) | 100.6 ± 74.0 | 106.0 ± 54.9 | 107.0 ± 51.7 | 156.9 ± 74.3 + |
| Fasting Blood Sugar (mg/dL) | 92.4 ± 8.4 | 96.1 ± 9.9 | 128.5 ± 28.1 εε | 182.8 ± 61.9 + |
| Parameter | Group 1 | Group 2 | Group 3 | Group 4 |
|---|---|---|---|---|
| PWV1000(m/s) | 4.4 ± 0.3 | 4.7 ± 0.4 * | 5.0 ± 0.3 ε | 5.1 ± 0.6 |
| MEISS (PWV1000) | 96.5 ± 4.4 | 97.4 ± 4.3 | 98.4 ± 6.7 | 91.5 ± 12.5+ |
| MEILS (PWV1000) | 89.4 ± 7.3 | 84.3 ± 6.3 * | 79.6 ± 9.2 ε | 71.9 ± 12.6+ |
| MEISS (PWV600) | 97.0 ± 7.6 | 99.1 ± 4.3 | 100.9 ± 8.3 | 93.3 ± 12.4+ |
| MEILS (PWV600) | 88.3 ± 10.8 | 86.1 ± 12.8 | 85.2 ± 11.0 | 82.9 ± 11.6 |
| sMEISS (PWV600) | 95.9 ± 10.0 | 96.8 ± 7.1 | 96.9 ± 11.3 | 89.2 ± 12.1+ |
| sMEILS (PWV600) | 92.2 ± 8.9 | 86.8 ± 11.3 * | 80.5 ± 6.2 ε | 73.7 ± 11.4+ |
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Chang, Y.-C.; Wu, H.-T.; Chen, H.-R.; Liu, A.-B.; Yeh, J.-J.; Lo, M.-T.; Tsao, J.-H.; Tang, C.-J.; Tsai, I.-T.; Sun, C.-K. Application of a Modified Entropy Computational Method in Assessing the Complexity of Pulse Wave Velocity Signals in Healthy and Diabetic Subjects. Entropy 2014, 16, 4032-4043. https://doi.org/10.3390/e16074032
Chang Y-C, Wu H-T, Chen H-R, Liu A-B, Yeh J-J, Lo M-T, Tsao J-H, Tang C-J, Tsai I-T, Sun C-K. Application of a Modified Entropy Computational Method in Assessing the Complexity of Pulse Wave Velocity Signals in Healthy and Diabetic Subjects. Entropy. 2014; 16(7):4032-4043. https://doi.org/10.3390/e16074032
Chicago/Turabian StyleChang, Yi-Chung, Hsien-Tsai Wu, Hong-Ruei Chen, An-Bang Liu, Jung-Jen Yeh, Men-Tzung Lo, Jen-Ho Tsao, Chieh-Ju Tang, I-Ting Tsai, and Cheuk-Kwan Sun. 2014. "Application of a Modified Entropy Computational Method in Assessing the Complexity of Pulse Wave Velocity Signals in Healthy and Diabetic Subjects" Entropy 16, no. 7: 4032-4043. https://doi.org/10.3390/e16074032
APA StyleChang, Y.-C., Wu, H.-T., Chen, H.-R., Liu, A.-B., Yeh, J.-J., Lo, M.-T., Tsao, J.-H., Tang, C.-J., Tsai, I.-T., & Sun, C.-K. (2014). Application of a Modified Entropy Computational Method in Assessing the Complexity of Pulse Wave Velocity Signals in Healthy and Diabetic Subjects. Entropy, 16(7), 4032-4043. https://doi.org/10.3390/e16074032