
First Responder Resiliency ECHO: Innovative Telementoring during the COVID-19 Pandemic

Abstract
:1. Introduction
Brief History of Project ECHO
2. Materials and Methods
2.1. Program, Hub Team, and Demographics
2.2. Curriculum
2.3. Participant Survey
2.4. Focus Groups
- How has participation in the First Responder Resiliency ECHO program impacted you?
- After open discussion, the focus group facilitator probed for impact on:
- Self-care or coping skills;
- Dealing with anxiety and stress;
- Listening to family members, colleagues, or patients;
- Quality of relationships.
- How has participation in this ECHO impacted the way you respond to or work in stressful environments?
- What challenges or barriers have you experienced to using the materials and skills from this ECHO?
- Do you have any suggestions on how to improve this ECHO or its content?
3. Results
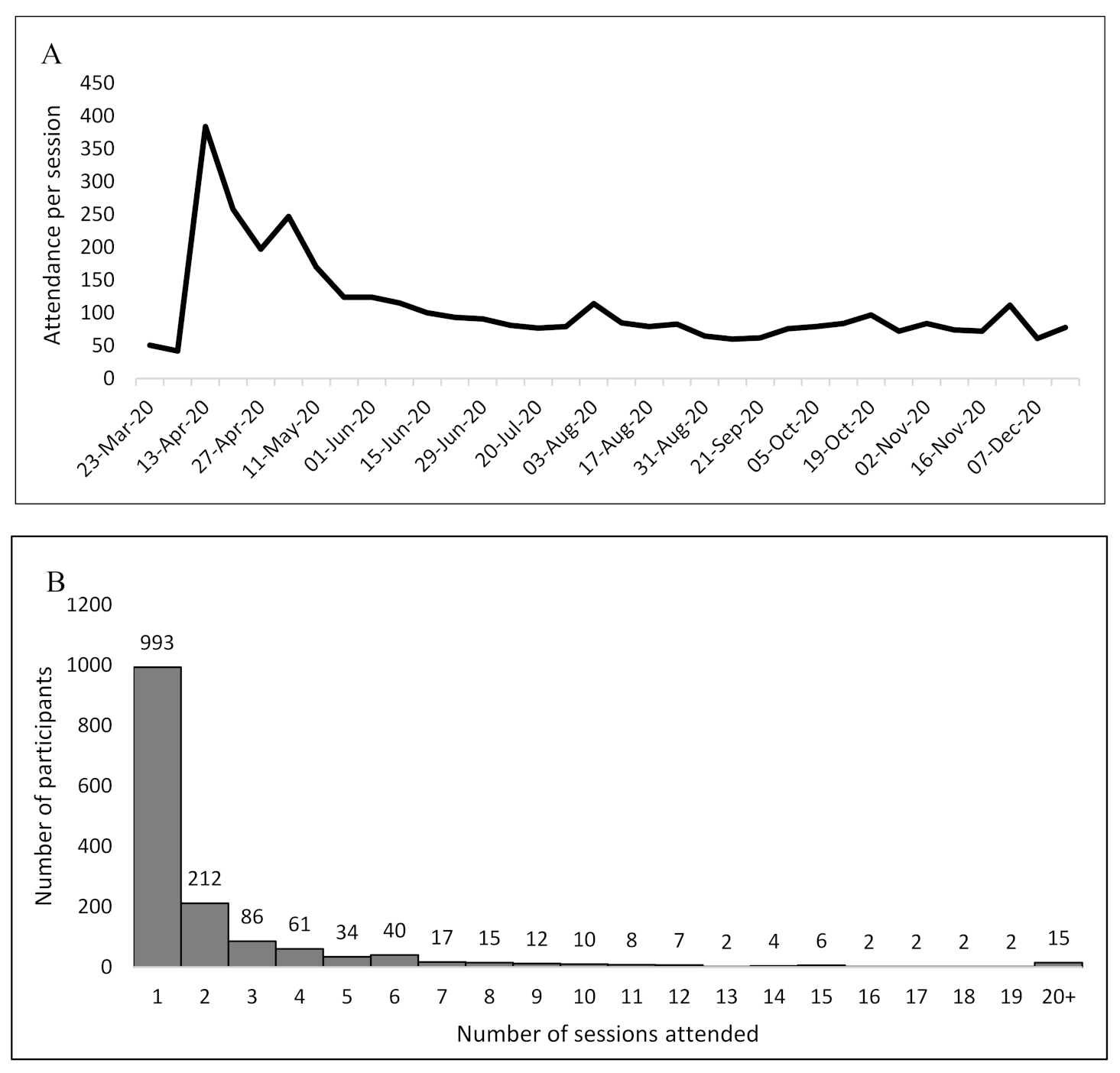
3.1. Attendance
3.2. Participant Survey
3.3. Focus Groups
4. Discussion
4.1. Weekly FRR ECHO Sessions
4.2. Facilitated Listening Sessions
4.3. Community of Practice
4.4. Participant Survey
4.5. Focus Group
4.6. Predominance of Female Participants
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jones, S. Describing the Mental Health Profile of First Responders: A Systematic Review. J. Am. Psychiatr. Nurses Assoc. 2017, 23, 200–214. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Nagel, C.; McSweeney, J.; Curran, G. Prevalence and correlates of psychiatric symptoms among first responders in a Southern State. Arch. Psychiatr. Nurs. 2018, 32, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Stanley, I.H.; Hom, M.A.; Joiner, T.E. A systematic review of suicidal thoughts and behaviors among police officers, firefighters, EMTs, and paramedics. Clin. Psychol. Rev. 2016, 44, 25–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malcolm, A.S.; Seaton, J.; Perera, A.; Sheehan, D.C.; Van Hasselt, V.B. Critical incident stress debriefing and law enforcement: An evaluative review. Brief Treat. Crisis Interv. 2005, 5, 261–278. [Google Scholar] [CrossRef] [Green Version]
- Bauwens, J.; Tosone, C. Professional posttraumatic growth after a shared traumatic experience: Manhattan clinicians’ perspectives on post-9/11 practice. J. Loss Trauma 2010, 15, 498–517. [Google Scholar] [CrossRef]
- Planning Committee on Workforce Resiliency Programs; Board on Health Sciences Policy; Institute of Medicine. Building a Resilient Workforce, Opportunities for the Department of Homeland Security: Workshop Summary; National Academies Press (US): Washington, DC, USA, 2012; ISBN1 13: 978-0-309-25511-0. ISBN2 10: 0-309-25511-2. [Google Scholar]
- Thornton, A.R.; Blumberg, D.M.; Papazoglou, K.; Giromini, L. The HEROES Project: Building Mental Resilience in First Responders. In Mental Health Intervention and Treatment of First Responders and Emergency Workers; IGI Global: Hershey, PA, USA, 2020; 15p. [Google Scholar] [CrossRef]
- Thompson, J. Enhancing resilience during the COVID-19 pandemic: A thematic analysis and evaluation of the warr; or 21 program. J. Community Saf. Well-Being 2020, 5, 51–56. [Google Scholar] [CrossRef]
- Ussery, W.J.; Waters, J.A. COP-2-COP hotlines: Programs to address the needs of first responders and their families. Brief Treat. Crisis Interv. 2006, 6, 66. [Google Scholar] [CrossRef]
- Szeto, A.; Dobson, K.S.; Knaak, S. The Road to Mental Readiness for First Responders: A Meta-Analysis of Program Outcomes. Can. J. Psychiatry 2019, 64, 18S–29S. [Google Scholar] [CrossRef]
- Gunderson, J.; Grill, M.; Callahan, P.; Marks, M. Responder resilience. JEMS 2014, 39, 57–61. [Google Scholar]
- Knight, C. Indirect trauma: Implications for self-care, supervision, the organization, and the academic institution. Clin. Superv. 2013, 32, 224–243. [Google Scholar] [CrossRef]
- Kreitzer, M.J.; Klatt, M. Educational innovations to foster resilience in the health professions. Med. Teach. 2017, 39, 153–159. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Maunder, R.G.; Lancee, W.J.; Balderson, K.E.; Bennett, J.P.; Borgundvaag, B.; Evans, S.; Fernandes, C.M.B.; Goldbloom, D.S.; Gupta, M.; Hunter, J.J.; et al. Long-term Psychological and Occupational Effects of Providing Hospital Healthcare during SARS Outbreak. Emerg. Infect. Dis. 2006, 12, 1924–1932. [Google Scholar] [CrossRef]
- Wu, P.; Liu, X.; Fang, Y.; Fan, B.; Fuller, C.J.; Guan, Z.; Yao, Z.; Kong, J.; Lu, J.; Litvak, I.J. Alcohol Abuse/Dependence Symptoms Among Hospital Employees Exposed to a SARS Outbreak. Alcohol Alcohol. 2008, 43, 706–712. [Google Scholar] [CrossRef]
- McAlonan, G.M.; Lee, A.M.; Cheung, V.; Cheung, C.; Tsang, K.W.; Sham, P.C.; Chua, S.E.; Wong, J.G. Immediate and Sustained Psychological Impact of an Emerging Infectious Disease Outbreak on Health Care Workers. Can. J. Psychiatry 2007, 52, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Bzdok, D.; Dunbar, R.I.M. The Neurobiology of Social Distance. Trends Cogn. Sci. 2020, 24, 717–733. [Google Scholar] [CrossRef]
- Katzman, N.; Medrano, J.; Swift, R.; Menking, P. First Responder ECHO: Developing an Innovative Telementoring Program. Creat. Educ. 2019, 10, 1982–1987. [Google Scholar] [CrossRef] [Green Version]
- Heath, C.; Sommerfield, A.; von Ungern-Sternberg, B.S. Resilience strategies to manage psychological distress among healthcare workers during the COVID-19 pandemic: A narrative review. Anaesthesia 2020, 75, 1364–1371. [Google Scholar] [CrossRef]
- Arora, S.; Kalishman, S.; Dion, D. Partnering urban academic medical centers and rural primary care clinicians to provide complex chronic disease care. Health Aff. 2011, 30, 1176–1184. [Google Scholar] [CrossRef]
- Katzman, J.G. ECHO Telementoring for pain, palliative care, and opioid management: Progress, challenges, and future goals. Pain Med. 2020, 21, 220–225. [Google Scholar] [CrossRef] [Green Version]
- Project ECHO website. First Responder Resiliency TeleECHO Program. Available online: https://hsc.unm.edu/echo/institute-programs/covid-19-response/nm-covid19/first-responder/ (accessed on 12 April 2021).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A meta-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Assessment Instruments for First Responders and Public Health Emergency Workers. Center for the Study of Traumatic Stress, Uniformed Services University. Available online: https://www.cstsonline.org/resources/resource-master-list/assessment-instruments-for-first-responders-and-public-health-emergency-workers (accessed on 12 April 2021).
- Dedoose Version 7.0.23, Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data; SocioCultural Research Consultants, LLC: Los Angeles, CA, USA, 2016.
- Rutkow, L.; Gable, L.; Links, J.M. Protecting the mental health of first responders: Legal and ethical considerations. J. Law Med. Ethics 2011, 39, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Katzman, J.G.; Tomedi, L.E.; Thornton, K. Innovative COVID-19 programs to rapidly serve New Mexico: Project ECHO. Public Health Rep. 2021, 136, 39–46. [Google Scholar] [CrossRef]
- Lalloo, C.; Osei-Twum, J.A.; Rapoport, A. Pediatric Project ECHO®: A virtual community of practice to improve palliative care knowledge and self-efficacy among interprofessional health care providers. J. Palliat. Med. 2020, in press. [Google Scholar] [CrossRef]
- Arora, S.; Thornton, K.; Komaromy, M.; Kalishman, S.; Katzman, J.; Duhigg, D. Demonopolizing medical knowledge. Acad. Med. 2014, 89, 30–32. [Google Scholar] [CrossRef]
- Papazoglou, K.; Blumberg, D.M.; Chiongbian, V.B.; Tuttle, B.M.; Kamkar, K.; Chopko, B.; Milliard, B.; Aukhojee, P.; Koskelainen, M. The role of moral injury in PTSD among law enforcement officers: A brief report. Front. Psychol. 2020, 11, 310. [Google Scholar] [CrossRef]
- Clay, J.M.; Parker, M.O. Alcohol use and misuse during the COVID-19 pandemic: A potential public health crisis? Lancet Public Health 2020, 5, e259. [Google Scholar] [CrossRef]
- McKnight-Eily, L.R.; Okoro, C.A.; Strine, T.W.; Verlenden, J.; Hollis, N.D.; Njai, R.; Mitchell, E.W.; Board, A.; Puddy, R.; Thomas, C. Racial and ethnic disparities in the prevalence of stress and worry, mental health conditions, and increased substance use among adults during the COVID-19 pandemic—United States, April and May 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 162–166. [Google Scholar] [CrossRef]
- Schafer, K.; Sutter, R.; Gibbons, S. Characteristics of Individuals and Employment among First Responders; U.S. Department of Labor: Washington, DC, USA, 2015. [Google Scholar] [CrossRef]
- Hodges, E.A.; Rowsey, P.J.; Gray, T.F.; Kneipp, S.M.; Giscombe, C.W.; Foster, B.B.; Alexander, G.R.; Kowlowitz, V. Bridging the gender divide: Facilitating the educational path for men in nursing. J. Nurs. Educ. 2017, 56, 295–299. [Google Scholar] [CrossRef]

{kind=link}
| Attendance (N = 919) | Survey (N = 45) | Focus Groups (N = 18) | ||||
|---|---|---|---|---|---|---|
| Characteristic | n | % | n | % | n | % |
| Gender | ||||||
| Female | - | - | 30 | 66.7% | 14 | 77.8% |
| Male | - | - | 15 | 33.3% | 4 | 22.2% |
| Job Category | ||||||
| First Responders (law, fire, EMT) | 216 | 23.5% | 16 | 35.6% | 7 | 38.9% |
| Medical Professionals (MD, RN, PA) | 393 | 42.8% | 16 | 35.6% | 3 | 16.7% |
| Mental Health (SW, PsyD, LMFT) | 206 | 22.4% | 7 | 15.6% | 6 | 33.3% |
| Other Degrees (BS, BA, MPA, PhD) | 104 | 11.3% | 6 | 13.3% | 2 | 11.1% |
| Confidence in Using Skills | Mean Score (Before) | Mean Score (Sfter) | p-Value |
|---|---|---|---|
| Using the elements of psychological first aid | 2.64 | 3.17 | <0.01 |
| Practicing self-care | 2.93 | 3.26 | <0.01 |
| Responding to and caring for patients who may be positive for or are suffering from SARS-CoV-2 (COVID-19) 3 | 2.37 | 2.93 | <0.01 |
| Recognizing and managing emergencies related to severe mental illness (e.g., psychosis, depression, etc.) as a first responder | 2.64 | 3.02 | <0.01 |
| Incorporating trauma-informed care into your response to emergencies as a first responder | 2.40 | 2.86 | <0.01 |
| Recognizing and responding to a coworker struggling with mental health issues | 2.77 | 3.14 | <0.01 |
| Recognizing and responding to a coworker struggling with substance use issues | 2.56 | 2.98 | <0.01 |
| Recognizing and accessing rural-specific resources to address mental health and substance use in the community | 2.57 | 3.02 | <0.01 |
| Agreement with statements about work stress | |||
| I often felt tired/fatigued rather than energetic, even when I had enough sleep | 3.07 | 3.02 | 0.79 |
| I felt overwhelmed by my work | 3.12 | 2.86 | 0.15 |
| I was absent and sick more often than I’d liked to have been | 1.91 | 1.91 | N/A |
| The public’s lack of respect for my profession was problematic | 2.61 | 2.64 | 0.89 |
| I often felt in danger while working | 2.61 | 2.66 | 0.75 |
| Agreement with statements about coping mechanisms | |||
| … Spending time with people helped counteract my work stress | 3.67 | 3.84 | 0.11 |
| … I spent time with various colleagues from work to counteract my work stress | 3.43 | 3.36 | 0.63 |
| … When I experienced professional stress, I was able to manage it proactively | 3.66 | 3.88 | 0.15 |
| … When I became stressed due to work, I tended to “shut down” and not talk to others about what is on my mind | 2.98 | 2.65 | 0.04 |
| ... I noticed that my coworkers increased their substance use to deal with job stress | 2.93 | 2.76 | 0.13 |
| ... I sometimes drank more alcohol than I planned to in order to deal with job stress | 2.36 | 3.68 | <0.01 |
| Total | Rural | Urban | NTFR | TFR | |||||
|---|---|---|---|---|---|---|---|---|---|
| External Factors Caused Stress | N 1 | n | % | n | % | n | % | n | % |
| Experienced world stress | 16 | 4 | 8.2% | 12 | 9.6% | 12 | 24.0% | 4 | 19.0% |
| Political and global turmoil | 8 | 2 | 4.1% | 6 | 4.8% | 8 | 16.0% | 0 | 0.0% |
| Did not want to be seen as weak | 6 | 2 | 4.1% | 4 | 3.2% | 5 | 10.0% | 1 | 4.8% |
| COVID is like a battle | 4 | 3 | 6.1% | 1 | 0.8% | 3 | 6.0% | 4 | 19.0% |
| External barriers make skills hard to use | 4 | 1 | 2.0% | 3 | 2.4% | 2 | 4.0% | 2 | 9.5% |
| Feeling overwhelmed prevents using skills | 1 | 1 | 2.0% | 0 | 0.0% | 1 | 2.0% | 0 | 0.0% |
| ECHO 2 Provides Community | |||||||||
| Provided sense of community | 28 | 9 | 18.4% | 19 | 15.2% | 16 | 32.0% | 12 | 57.1% |
| Reflected/normalized | 9 | 4 | 8.2% | 5 | 4.0% | 6 | 12.0% | 3 | 14.3% |
| Encouraged empathy for others | 8 | 3 | 6.1% | 5 | 4.0% | 3 | 6.0% | 5 | 23.8% |
| Was a safe space | 8 | 3 | 6.1% | 5 | 4.0% | 3 | 6.0% | 5 | 23.8% |
| Found people they can trust | 6 | 0 | 0.0% | 6 | 4.8% | 4 | 8.0% | 2 | 9.5% |
| Provided “me” time | 3 | 0 | 0.0% | 3 | 2.4% | 2 | 4.0% | 1 | 4.8% |
| Networking opportunities | 2 | 0 | 0.0% | 2 | 1.6% | 0 | 0.0% | 2 | 9.5% |
| Quality of Program | |||||||||
| Content was applicable | 19 | 5 | 10.2% | 14 | 11.2% | 15 | 30.0% | 4 | 19.0% |
| Shared skills with colleagues | 13 | 6 | 12.2% | 7 | 5.6% | 8 | 16.0% | 5 | 23.8% |
| Content was a good reminder | 7 | 1 | 2.0% | 6 | 4.8% | 5 | 10.0% | 2 | 9.5% |
| Used skills from ECHO | 6 | 1 | 2.0% | 5 | 4.0% | 4 | 8.0% | 2 | 9.5% |
| Need more time to learn applications | 5 | 0 | 0.0% | 5 | 4.0% | 5 | 10.0% | 0 | 0.0% |
| Not enough time | 5 | 0 | 0.0% | 5 | 4.0% | 4 | 8.0% | 1 | 4.8% |
| Zoom format works well | 3 | 0 | 0.0% | 3 | 2.4% | 1 | 2.0% | 2 | 9.5% |
| Wanted to be in a breakout with similar people | 3 | 2 | 4.1% | 1 | 0.8% | 3 | 6.0% | 0 | 0.0% |
| Liked interdisciplinary teaching | 2 | 1 | 2.0% | 1 | 0.8% | 1 | 2.0% | 1 | 4.8% |
| Met participants’ needs | 2 | 1 | 2.0% | 1 | 0.8% | 1 | 2.0% | 1 | 4.8% |
| Enjoyed breakout sessions | 2 | 0 | 0.0% | 2 | 1.6% | 2 | 4.0% | 0 | 0.0% |
| Content moved too quickly | 1 | 0 | 0.0% | 1 | 0.8% | 1 | 2.0% | 0 | 0.0% |
| Participants not wanting to share was a barrier | 1 | 0 | 0.0% | 1 | 0.8% | 0 | 0.0% | 1 | 4.8% |
| There were technical problems | 1 | 0 | 0.0% | 1 | 0.8% | 0 | 0.0% | 1 | 4.8% |
| Discussion was honest | 1 | 0 | 0.0% | 1 | 0.8% | 0 | 0.0% | 1 | 4.8% |
| 174 | 49 | 100.0% | 125 | 100.0% | 50 | 100.0% | 21 | 100.0% | |
| Quote | Codes |
|---|---|
| “[It has been helpful] to process different problems that arise whether it’s a tough call or dealing with your coworkers and trying to come in with a clean slate and trying not to come in with that baggage that you have always. That interfere[s] with working with other people and working with patients.” | Content was applicable |
| “…as a healthcare worker … you don’t want to be the one seen as weak, so you have to have a safe space to go to where you can … process everything that you’re going through.” | Did not want to be seen as weak, Was a safe space |
| “…just sharing feelings with other people from different states. They’re going through the same thing, so I’m not alone.” | Provided sense of community |
| “in law enforcement, sometimes we have just one-way vision, and I think that with everything that’s going on now for law enforcement and the climate right now, I think it’s been really important for all of us [to have] compassion towards each other and those stressors and with how we approach our jobs.” | Encouraged empathy for others |
| “I thought that the material that we got was really helpful, and I think that the listening groups offered a little bit of time to talk about some of those a little bit and kind of apply them.” | Content was applicable, Enjoyed breakout sessions |
| “One of the things that … I really like about this program is often times when I am working with other individuals after we’ve had a call or whatever is going on is that it just gives me more things to be able to turn to and set up for them.” | Shared skills with colleagues |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katzman, J.G.; Tomedi, L.E.; Everly, G.; Greenwood-Ericksen, M.; Romero, E.; Rosenbaum, N.; Medrano, J.; Menking, P.; Archer, G.R.D.; Martin, C.; et al. First Responder Resiliency ECHO: Innovative Telementoring during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4900. https://doi.org/10.3390/ijerph18094900
Katzman JG, Tomedi LE, Everly G, Greenwood-Ericksen M, Romero E, Rosenbaum N, Medrano J, Menking P, Archer GRD, Martin C, et al. First Responder Resiliency ECHO: Innovative Telementoring during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(9):4900. https://doi.org/10.3390/ijerph18094900
Chicago/Turabian StyleKatzman, Joanna G., Laura E. Tomedi, George Everly, Margaret Greenwood-Ericksen, Elizabeth Romero, Nils Rosenbaum, Jessica Medrano, Paige Menking, Gaelyn R.D. Archer, Chamron Martin, and et al. 2021. "First Responder Resiliency ECHO: Innovative Telementoring during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 9: 4900. https://doi.org/10.3390/ijerph18094900
APA StyleKatzman, J. G., Tomedi, L. E., Everly, G., Greenwood-Ericksen, M., Romero, E., Rosenbaum, N., Medrano, J., Menking, P., Archer, G. R. D., Martin, C., Dow, K. A., McCoy-Hayes, S., & Katzman, J. W. (2021). First Responder Resiliency ECHO: Innovative Telementoring during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(9), 4900. https://doi.org/10.3390/ijerph18094900