
Effect of Food and Dosing Regimen on Safety and Efficacy of Proton Pump Inhibitors Therapy—A Literature Review



Abstract
1. Introduction
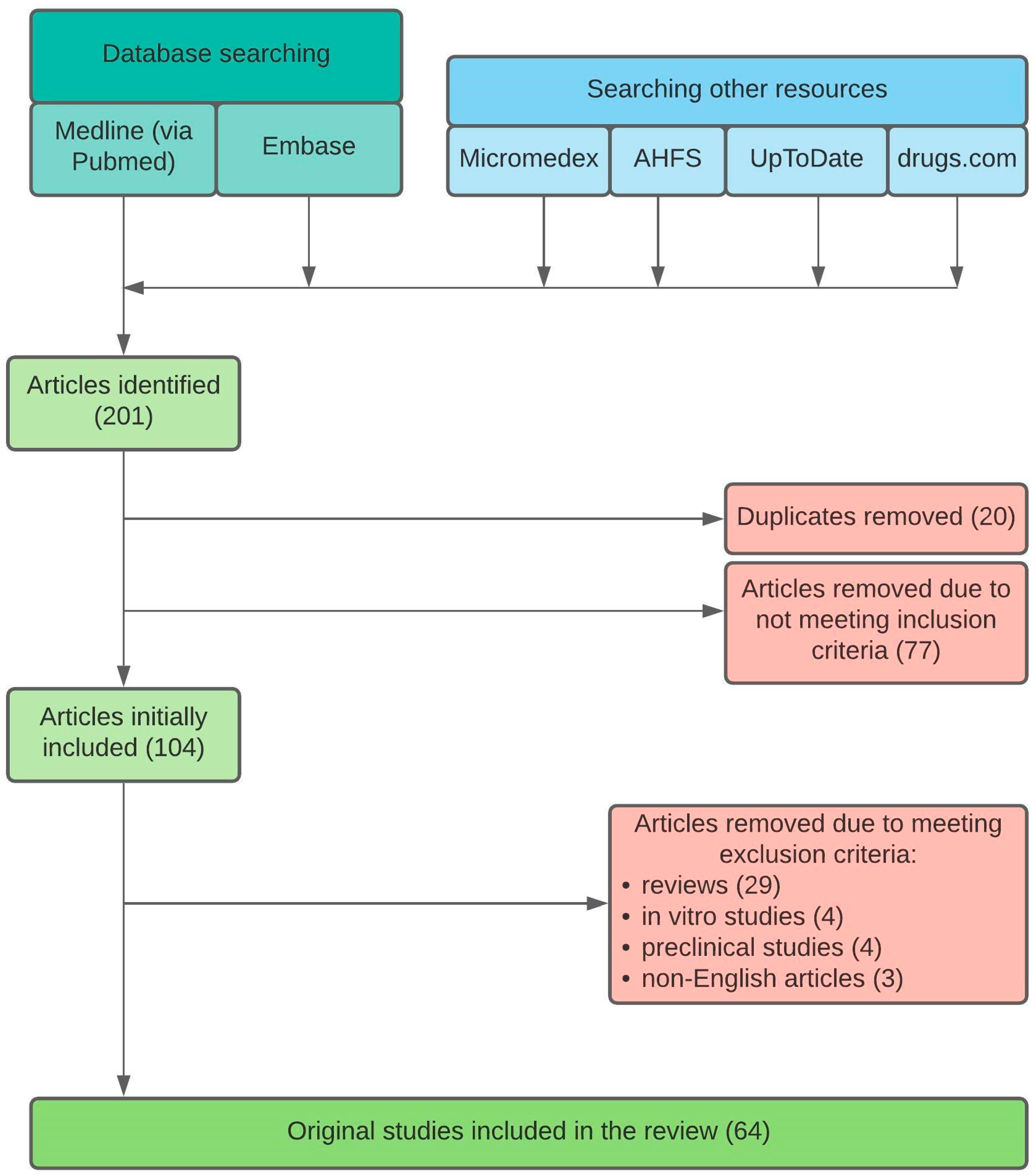
2. Materials and Methods
3. Results and Discussion
3.1. Aspects of PPI Pharmacokinetics
3.2. Esomeprazole
3.2.1. Food Effect
3.2.2. Dosing Regimen
3.2.3. Administration Modes
3.3. Omeprazole
3.3.1. Food Effect
3.3.2. Omeprazole and Grapefruit Juice (GFJ) Consumption
3.3.3. Interaction with Cranberry Juice
3.3.4. Omeprazole and Alcohol Consumption
3.3.5. Dosing Regimen
3.3.6. Administration Modes
3.4. Pantoprazole
3.4.1. Food Effect
3.4.2. Dosing Regimen
3.4.3. Administration Modes
3.5. Rabeprazole
3.5.1. Food Effect
3.5.2. Dosing Regimen
3.5.3. Administration Modes
3.6. Lansoprazole
3.6.1. Food Effect
3.6.2. Lansoprazole and Grapefruit Juice Consumption
3.6.3. Lansoprazole and Alcohol Consumption
3.6.4. Dosing Regimen
3.6.5. Administration Modes
3.7. Dexlansoprazole
3.7.1. Food Effect
3.7.2. Dosing Regimen
3.7.3. Administration Modes
3.8. Limitations of Studies
- presence of the older studies—from the 1980s and 1990s,
- unavailable data—in some studies, PPI formulation was not mentioned, as well as the quantitative and/or qualitative meal composition, not every drug formulation was tested in the presence of food,
- the attendance of healthy volunteers in many of studies—such studies cannot be fully translated to the clinical practice,
- scarce data of PPI clinical effectiveness in the presence of food—the vast majority of studies focused on changes in pharmacokinetic parameters (e.g., AUC, Cmax, tmax) instead of more clinically relevant endpoints, such as response to treatment, symptoms alleviation or the lesion healing, limited data of PPI clinical effectiveness in different dosing regimens—only single studies evaluated the effect of PPI dosing regimen on nighttime syndromes, whereas the majority examined the changes in pharmacodynamic parameters (e.g., 24 h intragastric pH) that cannot fully reflect the clinical practice.
4. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ridder, M. Top OTC Product Categories in the US 2020, Based on Sales. Available online: https://www.statista.com/statistics/807186/leading-us-over-the-counter-product-categories/ (accessed on 9 February 2021).
- Fass, R. Approach to refractory Gastroesophageal Reflux Disease in Adults. Available online: http://www-uptodate-com.offcampus.lib.washington.edu/contents/approach-to-refractory-gastroesophageal-reflux-disease-in-adults?topicKey=GAST/2239&elapsedTimeMs=6&source=search_result&searchTerm=gerd&selectedTitle=1~150&view=print&displayedView=full# (accessed on 9 February 2021).
- Fass, R.; Shapiro, M.; Dekel, R.; Sewell, J. Systematic review: Proton-pump inhibitor failure in gastro-oesophageal reflux disease—where next? Aliment. Pharmacol. Ther. 2005, 22, 79–94. [Google Scholar] [CrossRef]
- Hussain, Z.H.; Henderson, E.E.; Maradey-Romerao, C.; George, N.; Fass, R.; Lacy, B.E. The proton pump inhibitor non-responder: A clinical conundrum. Clin. Transl. Gastroenterol. 2015, 6, e106-11. [Google Scholar] [CrossRef]
- Patel, D.; Fass, R.; Vaezi, M. Untangling Non-erosive Reflux Disease From Functional Heartburn. Clin. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef]
- Domingues, G.; Moraes-Filho, J.P.P. Noncompliance is an impact factor in the treatment of gastroesophageal reflux disease. Expert Rev. Gastroenterol. Hepatol. 2014, 8, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Waghray, A.; Waghray, N.; Perzynski, A.T.; Votruba, M.; Wolfe, M.M. Optimal omeprazole dosing and symptom control: A randomized controlled trial (OSCAR Trial). Dig. Dis. Sci. 2019, 64, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Solem, C.; Mody, R.; Stephens, J.; Macahilig, C.; Gao, X. Mealtime-related dosing directions for proton-pump inhibitors in gastroesophageal reflux disease: Physician knowledge, patient adherence. J. Am. Pharm. Assoc. 2014, 54, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Alam, G. Proton pump inhibitors: Present and future a review. Int. J. Pharm. Res. Dev. 2012, 4, 119–131. [Google Scholar]
- Okamoto, C.T.; Forte, J.G. Vesicular trafficking machinery, the actin cytoskeleton, and H+-K+-ATPase recycling in the gastric parietal cell. J. Physiol. 2001, 532, 287–296. [Google Scholar] [CrossRef]
- Strand, D.S.; Kim, D.; Peura, D.A. 25 years of proton pump inhibitors: A comprehensive review. Gut Liver 2017, 11, 27–37. [Google Scholar] [CrossRef]
- Shin, J.M.; Kim, N. Pharmacokinetics and pharmacodynamics of the proton pump inhibitors. J. Neurogastroenterol. Motil. 2013, 19, 25–35. [Google Scholar] [CrossRef]
- Liu, T.J.; Jackevicius, C.A. Drug interaction between clopidogrel and proton pump inhibitors. Pharmacotherapy 2010, 30, 275–289. [Google Scholar] [CrossRef] [PubMed]
- Bouziana, S.D. Clinical relevance of clopidogrel-proton pump inhibitors interaction. World J. Gastrointest. Pharmacol. Ther. 2015, 6, 17. [Google Scholar] [CrossRef] [PubMed]
- Dickson, E.J.; Stuart, R.C. Genetics of Response to Proton Pump Inhibitor Therapy. Am. J. Pharm. 2003, 3, 303–315. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.; Tybring, G.; Dahl, M.L.; Gotharson, E.; Sagar, M.; Seensalu, R.; Bertilsson, L. Interphenotype differences in disposition and effect on gastrin levels of omeprazole—suitability of omeprazole as a probe for CYP2C19. Br. J. Clin. Pharmacol. 1995, 39, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Nexium (AstraZeneca Pharmaceuticals LP). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/022101s014021957s017021153s050lbl.pdf (accessed on 10 February 2021).
- Vegesna, V.; Li, J.; Pollack, C.; Moreira, S. Assessing the bioequivalence of over-the-counter esomeprazole banded capsules and multiple-unit pellet system tablets. Int. J. Clin. Pharmacol. Ther. 2018, 56, 90–92. [Google Scholar] [CrossRef]
- Esomeprazole Strontium (ParaPRO LLC). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/202342s005lbl.pdf (accessed on 10 February 2021).
- Vimovo (Astra Zeneca). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/022511s017lbl.pdf (accessed on 10 February 2021).
- Liu, Z.-Z.; Ren, Q.; Zhou, Y.-N.; Yang, H.-M. Bioequivalence of two esomeprazole magnesium enteric-coated formulations in healthy Chinese subjects. World J. Clin. Cases 2020, 8, 5518–5528. [Google Scholar] [CrossRef]
- Sostek, M.B.; Chen, Y.; Andersson, T. Effect of timing of dosing in relation to food intake on the pharmacokinetics of esomeprazole. Br. J. Clin. Pharmacol. 2007, 64, 386–390. [Google Scholar] [CrossRef]
- Furuta, K.; Kohata, Y.; Fujiwara, Y.; Sugimoto, M.; Uotani, T.; Yamade, M.; Sahara, S.; Ichikawa, H.; Furuta, T.; Nio, K.; et al. Intra-gastric pH following single oral administrations of rabeprazole and esomeprazole: Double-blind cross-over comparison. J. Clin. Biochem. Nutr. 2014, 55, 178–183. [Google Scholar] [CrossRef][Green Version]
- Furuta, K.; Adachi, K.; Aimi, M.; Shimura, S.; Mikami, H.; Nishimura, N.; Ishimura, N.; Ishihara, S.; Naora, K.; Kinoshita, Y. Effect of timing of proton pump inhibitor administration on acid suppression. Digestion 2016, 93, 111–120. [Google Scholar] [CrossRef]
- Nexium (AstraZeneca Canada, Inc.). Product Monograph. Available online: https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/nexium-product-monogarph-en.pdf (accessed on 11 February 2021).
- Boltin, D.; Zvidi, I.; Raskin, M.; Kayless, H.; Schmilovitz-Weiss, H.; Gingold-Belfer, R.; Niv, Y.; Dickman, R. Effect of postprandial administration of esomeprazole on reflux symptoms in gastroesophageal reflux disease: A randomized, controlled trial. Dig. Dis. 2018, 36, 257–263. [Google Scholar] [CrossRef]
- Wilder-Smith, C.; Röhss, K.; Bokelund Singh, S.; Sagar, M.; Nagy, P. The effects of dose and timing of esomeprazole administration on 24-h, daytime and night-time acid inhibition in healthy volunteers. Aliment. Pharmacol. Ther. 2010, 32, 1249–1256. [Google Scholar] [CrossRef]
- Maejima, R.; Koike, T.; Nakagawa, K.; Iijima, K.; Shimosegawa, T. Effects of dose and timing of esomeprazole administration on inhibition of gastric acid secretion in healthy Japanese volunteers. Gastroenterology 2014, 146, S-760. [Google Scholar] [CrossRef]
- Nexium Control (GlaxoSmithKline). Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/nexium-control-epar-product-information_en.pdf (accessed on 11 February 2021).
- Bladh, N.; Blychert, E.; Johansson, K.; Backlund, A.; Lundin, C.; Niazi, M.; Pettersson, G.; Fjellman, M. A new esomeprazole packet (sachet) formulation for suspension: In vitro characteristics and comparative pharmacokinetics versus intact capsules/tablets in healthy volunteers. Clin. Ther. 2007, 29, 640–649. [Google Scholar] [CrossRef]
- Andersson, T.; Magner, D.; Patel, J.; Rogers, P.; Levine, J.G. Esomeprazole 40mg capsules are bioequivalent when administered intact or as the contents mixed with applesauce. Clin. Drug Investig. 2001, 21, 67–71. [Google Scholar] [CrossRef]
- Zegerid (Salix Pharmaceuticals, Inc.). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/021849s010021636s016lbl.pdf (accessed on 11 February 2021).
- Prilosec (Astra Zeneca). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/019810s096lbl.pdf (accessed on 11 February 2021).
- Liu, Z.; Ding, L.; Zhong, S.; Cao, X.; Jiang, L.; Duan, H. Pharmacokinetics of a new immediate-release compound omeprazole capsule and its comparison with the enteric-coated formulation under fasting and fed conditions. Drug Res. (Stuttg). 2013, 63, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, D.; Román, M.; Cabaleiro, T.; Saiz-Rodríguez, M.; Mejía, G.; Abad-Santos, F. Effect of food on the pharmacokinetics of omeprazole, pantoprazole and rabeprazole. BMC Pharmacol. Toxicol. 2020, 21, 1–9. [Google Scholar] [CrossRef]
- Pillai, G.K.; Hassan, M.M.; Salem, M.S.; Najib, N.M. Effect of food on the bioavailability of omeprazole. Int. J. Pharm. Med. 1998, 12, 199–202. [Google Scholar]
- Andersson, T.; Andrén, K.; Cederberg, C.; Heggelund, A.; Lundborg, P.; Röhss, K. Bioavailability of omeprazole as enteric-coated (EC) granules in conjunction with food on the first and seventh days of treatment. Drug Investig. 1990, 2, 184–188. [Google Scholar] [CrossRef]
- Rhoss, K.; Andren, K.; Heggelund, A. Bioavailability of omeprazole given in conjunction with food. II World Congr for Clin Pharmacol Ther, Stockholm July-Aug 1986. Acta Pharmacol. Toxicol. 1986, 85, 207. [Google Scholar]
- Vaz-da-Silva, M.; Loureiro, A.I.; Nunes, T.; Maia, J.; Tavares, S.; Falcão, A.; Silveira, P.; Almeida, L.; Soares-da-Silva, P. Bioavailability and bioequivalence of two enteric-coated formulations of omeprazole in fasting and fed conditions. Clin. Drug Investig. 2005, 25, 391–399. [Google Scholar] [CrossRef]
- Raffaelli, R. Omeprazole Delayed Release Orally Disintegrating Tablet, 20 mg—Clinical Review. 2017. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/209400Orig1s000MedR.pdf (accessed on 12 February 2021).
- Thomson, A.B.R.; Sinclair, P.; Matisko, A.; Rosen, E.; Andersson, T.; Olofsson, B. Influence of food on the bioavailability of an enteric-coated tablet formulation of omeprazole 20 mg under repeated dose conditions. Can. J. Gastroenterol. 1997, 11, 663–667. [Google Scholar] [CrossRef]
- Shinkai, H.; Koike, T.; Shimada, M.; Nakagawa, K.; Iijima, K.; Matsumoto, Y.; Maekawa, M.; Mano, N.; Shimosegawa, T. Influence of the meal and genotype of CYP2C19 on the pharmacokinetics of proton pump inhibitors in healthy Japanese subjects. Pharmacol. Pharm. 2013, 04, 502–509. [Google Scholar] [CrossRef][Green Version]
- Hatlebakk, J.G.; Katz, P.O.; Camacho-Lobato, L.; Castell, D.O. Proton pump inhibitors: Better acid suppression when taken before a meal than without a meal. Aliment. Pharmacol. Ther. 2000, 14, 1267–1272. [Google Scholar] [CrossRef]
- Tassaneeyakul, W.; Tassaneeyakul, W.; Vannaprasaht, S.; Yamazoe, Y. Formation of omeprazole sulphone but not 5-hydroxyomeprazole is inhibited by grapefruit juice. Br. J. Clin. Pharmacol. 2000, 49, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Mouly, S.; Paine, M.F. Effect of grapefruit juice on the disposition of omeprazole. Br. J. Clin. Pharmacol. 2001, 52, 216–217. [Google Scholar] [CrossRef] [PubMed]
- Shmuely, H.; Yahav, J.; Samra, Z.; Chodick, G.; Koren, R.; Niv, Y.; Ofek, I. Effect of cranberry juice on eradication of Helicobacter pylori in patients treated with antibiotics and a proton pump inhibitor. Mol. Nutr. Food Res. 2007, 51, 746–751. [Google Scholar] [CrossRef]
- Saltzman, J.R.; Kemp, J.A.; Golner, B.B.; Pedrosa, M.C.; Dallal, G.E.; Russell, R.M. Effect of hypochlorhydria due to omeprazole treatment or atrophic gastritis on protein-bound vitamin bi2 absorption. J. Am. Coll. Nutr. 1994, 13, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.S.J.M.; James, O.F.W. Omeprazole, ranitidine and cimetidine have no effect on peak blood ethanol concentrations, first pass metabolism or area under the time-ethanol curve under “real-life” drinking conditions. Aliment. Pharmacol. Ther. 1998, 12, 141–145. [Google Scholar] [CrossRef]
- Roine, R.; Hernández-Muñoz, R.; Baraona, E.; Greenstein, R.; Lieber, C.S. Effect of omeprazole on gastric first-pass metabolism of ethanol. Dig. Dis. Sci. 1992, 37, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Minocha, A.; Rahal, P.S.; Brier, M.E.; Levinson, S.S. Omeprazole therapy does not affect pharmacokinetics of orally administered ethanol in healthy male subjects. J. Clin. Gastroenterol. 1995, 21, 107–109. [Google Scholar] [CrossRef]
- Chiverton, S.G.; Howden, C.W.; Burget, D.W.; Hunt, R.H. Omeprazole (20 mg) daily given in the morning or evening: A comparison of effects on gastric acidity, and plasma gastrin and omeprazole concentration. Aliment. Pharmacol. Ther. 1992, 6, 103–111. [Google Scholar] [CrossRef]
- Prichard, P.J.; Yeomans, N.D.; Mihaly, G.W.; Jones, D.B.; Buckle, P.J.; Smallwood, R.A.; Louis, W.J. Omeprazole: A study of its inhibition of gastric pH and oral pharmacokinetics after morning or evening dosage. Gastroenterology 1985, 88, 64–69. [Google Scholar] [CrossRef]
- Hendel, J.; Hendel, L.; Aggestrup, S. Morning or evening dose of omeprazole for gastro-esophageal reflux? Aliment. Pharmacol. Ther. 1995, 9, 693–697. [Google Scholar] [CrossRef] [PubMed]
- Hatlebakk, J.G.; Katz, P.O.; Kuo, B.; Castell, D.O. Nocturnal gastric acidity and acid breakthrough on different regimens of omeprazole 40 mg daily. Aliment. Pharmacol. Ther. 1998, 12, 1235–1240. [Google Scholar] [CrossRef] [PubMed]
- Howden, C.W. Review article: Immediate-release proton-pump inhibitor therapy—Potential advantages. Aliment. Pharmacol. Ther. 2005, 22 (Suppl. 3), 25–30. [Google Scholar] [CrossRef]
- Protonix (Pfizer). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020987s045lbl.pdf (accessed on 12 February 2021).
- De Campos, D.R.; Vieira, N.R.; Bernasconi, G.; Barros, F.A.P.; Meurer, E.C.; Marchioretto, M.A.; Coelho, E.C.; Calafatti, S.A.; Sommer, C.; Couto, J.M.; et al. Bioequivalence of two enteric coated formulations of pantoprazole in healthy volunteers under fasting and fed conditions. Arzneim. Forsch. Drug Res. 2007, 57, 309–314. [Google Scholar] [CrossRef]
- Mendes, F.D.; Patni, A.K.; Reyer, S.; Monif, T.; Moreira, L.D.; Ilha, J.O.; Mendes, G.D.; De Nucci, G. Comparative bioavailability study with two pantoprazole delayed-released tablet formulations administered with and without food in healthy subjects. Arzneimittelforschung 2008, 58, 141–148. [Google Scholar] [CrossRef]
- PANTO-BYK (Takeda Canada, Inc.). Product Monograph. Available online: https://pdf.hres.ca/dpd_pm/00019369.PDF (accessed on 13 February 2021).
- IPP (Sandoz GmbH). Product Characteristics. Available online: http://leki.urpl.gov.pl/files/25_IPP20_tabl_dojelit_20.pdf (accessed on 13 February 2021).
- Müssig, S.; Witzel, L.; Lühmann, R.; Schneider, A. Morning and evening administration of pantoprazole: A study to compare the effect on 24-hour intragastric pH. Eur. J. Gastroenterol. Hepatol. 1997, 9, 599–602. [Google Scholar] [CrossRef]
- Tammara, B.; Weisel, K.; Katz, A.; Meng, X. Bioequivalence among three methods of administering pantoprazole granules in healthy subjects. Am. J. Heal. Pharm. 2009, 66, 1923–1928. [Google Scholar] [CrossRef] [PubMed]
- Aciphex (FSC Laboratories, Inc.). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/020973s035204736s005lbl.pdf (accessed on 13 February 2021).
- Yasuda, S.; Ohnishi, A.; Ogawa, T.; Tomono, Y.; Hasegawa, J.; Nakai, H.; Shimamura, Y.; Morishita, N. Pharmacokinetic properties of E3810, a new proton pump inhibitor, in healthy male volunteers. Int. J. Clin. Pharmacol. Ther. 1994, 32, 466–473. [Google Scholar]
- Thyssen, A.; Solanki, B.; Gonzalez, M.; Leitz, G.; Treem, W.; Mannaert, E. Pharmacokinetics of rabeprazole granules versus tablets, and the effect of food on the pharmacokinetics of rabeprazole granules in healthy adults-cross-study comparison. Clin. Pharmacol. Drug Dev. 2014, 3, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Pehlivanov, N.D.; Olyaee, M.; Sarosiek, I.; McCallum, R.W. Comparison of morning and evening administration of rabeprazole for gastro-oesophageal reflux and nocturnal gastric acid breakthrough in patients with reflux disease: A double-blind, cross-over study. Aliment. Pharmacol. Ther. 2003, 18, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Miki, M.; Adachi, K.; Azumi, T.; Koshino, K.; Furuta, K.; Kinoshita, Y. A comparative study of intragastric acidity during post-breakfast and pre-dinner administration of low-dose proton pump inhibitors: A randomized three-way crossover study. Aliment. Pharmacol. Ther. 2006, 24, 1445–1451. [Google Scholar] [CrossRef]
- Thyssen, A.; Solanki, B.; Treem, W. Randomized, open-label, single-dose, crossover, relative bioavailability study in healthy adults, comparing the pharmacokinetics of rabeprazole granules administered using soft food or infant formula as dosing vehicle versus suspension. Clin. Ther. 2012, 34, 1636–1645. [Google Scholar] [CrossRef] [PubMed]
- Bergstrand, R.; Grind, M.; Nyberg, G.; Olofsson, B. Decreased oral bioavailability of lansoprazole in healthy volunteers when given with a standardised breakfast. Clin. Drug Investig. 1995, 9, 67–71. [Google Scholar] [CrossRef]
- Delhotal-Landes, B.; Cournot, A.; Vermerie, N.; Dellatolas, F.; Benoit, M.; Flouvat, B. The effect of food and antacids on lansoprazole absorption and disposition. Eur. J. Drug Metab. Pharmacokinet. 1991, 3, 315–320. [Google Scholar]
- Prevacid (Takeda Pharmaceuticals America, Inc.). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020406s078-021428s025lbl.pdf (accessed on 14 February 2021).
- Fujiwara, Y.; Okazaki, H.; Higashimori, A.; Sugita, N.; Tanaka, M.; Sakai, T.; Kobayashi, M.; Shindo, M.; Machida, H.; Tanigawa, T.; et al. The effect of food intake on pharmacokinetics of lansoprazole OD tablet. Jpn. Pharmacol. Ther. 2011, 39, 961–966. [Google Scholar]
- Moules, I.; Garrett, A.; Brocklebank, D.; Oliver, S. Gastric acid inhibition by the proton pump inhibitor lansoprazole is unaffected by food. Br. J. Clin. Res. 1993, 4, 153–161. [Google Scholar]
- Brummer, R.J.M.; Geerling, B.J.; Stockbrügger, R.W. Initial and chronic gastric acid inhibition by lansoprazole and omeprazole in relation to meal administration. Dig. Dis. Sci. 1997, 42, 2132–2137. [Google Scholar] [CrossRef]
- Miura, M.; Kagaya, H.; Tada, H.; Uno, T.; Yasui-Furukori, N.; Tateishi, T.; Suzuki, T. Intestinal CYP3A4 is not involved in the enantioselective disposition of lansoprazole. Xenobiotica 2006, 36, 95–102. [Google Scholar] [CrossRef]
- Uno, T.; Yasui-Furukori, N.; Takahata, T.; Sugawara, K.; Tateishi, T. Lack of significant effect of grapefruit juice on the pharmacokinetics of lansoprazole and its metabolites in subjects with different CYP2C19 genotypes. J. Clin. Pharmacol. 2005, 45, 690–694. [Google Scholar] [CrossRef]
- Battiston, L.; Tulissi, P.; Moretti, M.; Pozzato, G. Lansoprazole and ethanol metabolism: Comparison with omeprazole and cimetidine. Pharmacol. Toxicol. 1997, 81, 247–252. [Google Scholar]
- Fraser, A.G.; Sawyerr, A.M.; Hudson, M.; Smith, M.S.H.; Pounder, R.E. Morning versus evening dosing of lansoprazole 30 mg daily on twenty-four-hour intragastric acidity in healthy subjects. Aliment. Pharmacol. Ther. 1996, 10, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.W.; Tolman, K.G.; Greski, P.A.; Jennings, D.E.; Hoyos, P.A.; Page, J.G. The effects of lansoprazole, a new H+,K+-ATPase inhibitor, on gastric pH and serum gastrin. Aliment. Pharmacol. Ther. 1992, 6, 359–372. [Google Scholar] [CrossRef] [PubMed]
- Hongo, M.; Ohara, S.; Hirasawa, Y.; Abe, S.; Asaki, S.; Toyota, T. Effect of lansoprazole on intragastric pH—Comparison between morning and evening dosing. Dig. Dis. Sci. 1992, 37, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Chun, A.H.C.; Erdman, K.; Zhang, Y.; Achari, R.; Cavanaugh, J.H. Effect on bioavailability of admixing the contents of lansoprazole capsules with selected soft foods. Clin. Ther. 2000, 22, 231–236. [Google Scholar] [CrossRef]
- Chun, A.H.C.; Erdman, K.; Chiu, Y.L.; Pilmer, B.L.; Achari, R.; Cavanaugh, J.H. Bioavailability of lansoprazole granules administered in juice or soft food compared with the intact capsule formulation. Clin. Ther. 2002, 24, 1322–1331. [Google Scholar] [CrossRef]
- Iwasaki, K.; Ito, Y.; Shibata, N.; Takada, K.; Sakurai, Y.; Takagi, N.; Irie, S.; Nakamura, K. Effect of water intake on pharmacokinetics of lansoprazole from fast disintegrating tablet in human subjects. Drug Metab. Pharmacokinet. 2004, 19, 390–395. [Google Scholar] [CrossRef]
- Skrzydło-Radomańska, B.; Radwan, P. Dexlansoprazole—A new-generation proton pump inhibitor. Prz. Gastroenterol. 2015, 10, 191–196. [Google Scholar] [CrossRef]
- Fass, R.; Frazier, R. The role of dexlansoprazole modified release in the management of gastroesophageal reflux disease. Ther. Adv. Gastroenterol. 2017, 10, 243–251. [Google Scholar] [CrossRef]
- Sharma, P.; Shaheen, N.J.; Perez, M.C.; Pilmer, B.L.; Lee, M.; Atkinson, S.N.; Peura, D. Healing of erosive oesophagitis with dexlansoprazole MR, a proton pump inhibitor with a novel dual delayed-release formulation—Results from two randomized controlled studies. Aliment. Pharmacol. Ther. 2009, 29, 731–741. [Google Scholar] [CrossRef]
- Lee, R.D.; Vakily, M.; Mulford, D.; Wu, J.; Atkinson, S.N. Clinical trial: The effect and timing of food on the pharmacokinetics and pharmacodynamics of dexlansoprazole MR, a novel Dual Delayed Release formulation of a proton pump inhibitor—Evidence for dosing flexibility. Aliment. Pharmacol. Ther. 2009, 29, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Dexilant (Takeda Canada, Inc.). Product Monograph. Available online: https://www.takeda.com/48f445/siteassets/en-ca/home/what-we-do/our-medicines/product-monographs/dexilant/dexilant-pm-en.pdf (accessed on 14 February 2021).
- Kukulka, M.; Nudurupati, S.; Perez, M.C. Bioavailability of a dexlansoprazole Delayed-Release orally disintegrating tablet: Effects of food and mode of administration. Clin. Exp. Gastroenterol. 2017, 10, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.D.; Mulford, D.; Wu, J.; Atkinson, S.N. The effect of time-of-day dosing on the pharmacokinetics and pharmacodynamics of dexlansoprazole MR: Evidence for dosing flexibility with a Dual Delayed Release proton pump inhibitor. Aliment. Pharmacol. Ther. 2010, 31, 1001–1011. [Google Scholar] [CrossRef]
- Dexilant SoluTab (Takeda Pharmaceuticals America, Inc.). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/208056lbl.pdf (accessed on 14 February 2021).
- Wiesner, A.; Gajewska, D.; Paśko, P. Levothyroxine Interactions with Food and Dietary Supplements–A Systematic Review. Pharmaceuticals. 2021, 14, 206. [Google Scholar] [CrossRef]
- Palimonka, K.; Paśko, P.; Szuta, M.; Sowizdraniuk, J. Antazoline renaissance in the treatment of cardiac arrhythmia: A review. Acta Pol. Pharm. 2020, 77, 209–219. [Google Scholar] [CrossRef]
- Heuberger, R. Polypharmacy and food–drug interactions among older persons: A review. J. Nutr. Gerontol. Geriatr. 2012, 31, 325–403. [Google Scholar] [CrossRef] [PubMed]
- Paśko, P.; Rodacki, T.; Domagała-Rodacka, R.; Owczarek, D. A short review of drug–food interactions of medicines treating overactive bladder syndrome. Int. J. Clin. Pharm. 2016, 38, 1350–1356. [Google Scholar] [CrossRef]
- Hunt, R.H.; Scarpignato, C. Potent Acid Suppression with PPIs and P-CABs: What’s New? Curr. Treat. Options Gastroenterol. 2018, 16, 570–590. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Drug | Formulation | Food Effect | Recommended Intake Regarding Food | Recommended Dosing Regimen |
|---|---|---|---|---|
| Esomeprazole | DR capsules | after single dose: ↓ AUC (by 43–53%), ↓ Cmax (74–78%) [17,19,20,21], ↑ tmax (by 2.4–3 h) [16] after repeated doses: ↓ AUC (by 25%), ↓ Cmax (by 23%) [17] |
| |
| DR granules for oral suspension | no studies found | |||
| DR tablets | no studies found | |||
| Omeprazole | IR capsules | ↓ AUC (by 24 and 28%, depending on the study), ↓ Cmax (by 47 and 63%, depending on the study) [32,34,35], ↑ tmax (by 0.6 h) [34,35] |
| |
| IR powder for oral suspension | ↓ AUC (by 24%), ↓ Cmax (by 63%) [32] | |||
| DR orally disintegrating tablets | ↓ AUC (by 19%), ↓ Cmax (by 56%), ↑ tmax (by 2 h) [40] | |||
| DR capsules | ↓ AUC (by 35–38%) [34], ↓ Cmax (by 24–40% and 58–63%, depending on the study) [36,38], ↑ tmax (by 2 h) [36] | |||
| DR granules for oral suspension | no studies found | |||
| DR tablets | no significant changes in AUC and Cmax, ↑ tmax (by 1.3 h) [41] | |||
| Pantoprazole | DR tablets | slightly ↓ AUC (by 17–25%), no significant changes in Cmax, ↑ tmax (by 4–5 h) [57] |
|
|
| DR granules for oral suspension | ↓ AUC (by 29%), ↓ Cmax (by 51%), ↑ tmax (by 2 h) [56] | |||
| Rabeprazole | DR capsules | ↓ AUC (by 27%), ↓ Cmax (by 55%), ↑ tmax (by 2 h) [65] |
| |
| DR tablets | no significant changes in AUC and Cmax, ↑ tmax (by 2.5 h) [42] no significant changes in median intragastric pH [23,24] | |||
| Lansoprazole | DR capsules | ↓ AUC and ↓ Cmax (both by 50%), ↑ tmax (by 1.5 h) [69] median intragastric pH not altered [73,74] |
|
|
| DR orally disintegrating tablets | ↓ AUC (by 32%), ↓ Cmax (by 50%), ↑ tmax (by 1.3 h) [72] |
| ||
| Dexlansoprazole | DDR capsules | not significant [87] |
|
|
| DR orally disintegrating tablets | no significant changes in AUC, ↓ Cmax (by 38%), ↑ tmax (by 2 h) [89] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiesner, A.; Zwolińska-Wcisło, M.; Paśko, P. Effect of Food and Dosing Regimen on Safety and Efficacy of Proton Pump Inhibitors Therapy—A Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 3527. https://doi.org/10.3390/ijerph18073527
Wiesner A, Zwolińska-Wcisło M, Paśko P. Effect of Food and Dosing Regimen on Safety and Efficacy of Proton Pump Inhibitors Therapy—A Literature Review. International Journal of Environmental Research and Public Health. 2021; 18(7):3527. https://doi.org/10.3390/ijerph18073527
Chicago/Turabian StyleWiesner, Agnieszka, Małgorzata Zwolińska-Wcisło, and Paweł Paśko. 2021. "Effect of Food and Dosing Regimen on Safety and Efficacy of Proton Pump Inhibitors Therapy—A Literature Review" International Journal of Environmental Research and Public Health 18, no. 7: 3527. https://doi.org/10.3390/ijerph18073527
APA StyleWiesner, A., Zwolińska-Wcisło, M., & Paśko, P. (2021). Effect of Food and Dosing Regimen on Safety and Efficacy of Proton Pump Inhibitors Therapy—A Literature Review. International Journal of Environmental Research and Public Health, 18(7), 3527. https://doi.org/10.3390/ijerph18073527