In this section, we present and then analyze a stylized game-theoretic model of a market with heterogeneous healthcare providers that allowed us to examine the optimal PGHD- and platform-adoption strategies in a competitive equilibrium. As is customary in game-theoretic analyses, each player maximized either a utility function (in the case of consumers) or a profit function (in the case of providers), while taking into account the best response of other players to the decisions that they make. An outcome that arises from a specific set of decisions made by the participating players is said to be an “equilibrium” when no player has an incentive to deviate from their decision. As we analyzed the potential equilibria, we also checked the impact of PGHD adoption on social welfare, which was the total aggregate surplus (utility and profit) in the market.
For comparison purposes, we first started with the case with no PGHD.
3.1. Benchmark Case: No PGHD
The market is composed of three types of players: providers, consumers, and a monopolist platform. There are two profit-maximizing providers (denoted with and ) who are differentiated with respect to their effectiveness in delivering healthcare. Factors such as past experience and available technology and resources may allow a provider to outperform others. Consequently, consumers derive different gross utilities when they receive care from the providers. We denote the gross utilities of receiving care from and by and , respectively, where without loss of generality.
In addition to effectiveness, the providers are also distinguished by the number of consumers for whom they have medical and health records on file. In what follows, we refer to the totality of medical and health records about a consumer as “digital records.” Each consumer starts the game as having been assigned to one of the providers. Hence, each consumer’s complete digital history is held by one of the two providers. We denote the proportion of digital consumer health records that has on file by .
Furthermore, the start of the game is characterized by a random “disturbance” to the consumers’ provider preferences. Such disturbances can arise because of changes in preferences, attitudes, situational conditions, etc. Healthcare is a service that can be considered as an experience good, and experiences affect and refine preferences. There can be a host of reasons as to why a consumer may want to end an established medical relationship with a provider. For example, preferences may change when a consumer relocates to a new area. The possibility of switching providers arising from the exogenous change in preferences at the outset of the game reflects the common phenomenon of patients who, for various reasons, consider obtaining healthcare from a different provider.
To characterize the change in consumer preferences at the beginning of the game, we assumed a randomly assigned and uniformly distributed disutility associated with each consumer. In other words, each consumer is randomly placed on a Hotelling-style linear city [0,1], regardless of their previously established provider relationship, while the providers were located at the two ends of the city (it is conceivable that in reality, a provider will have fewer patients who do not particularly favor them than those who do. The conceptualization could be generalized by assuming that the density of patients whose records reside with uniformly drop from at point 0 to at point 1, where . Although such a conceptualization is arguably closer to reality, it significantly complicates the analysis without adding any new insights). Accordingly, when a consumer receives care from a provider, they incur a utility loss equivalent to the distance on the linear city between her location and that of the provider due to this change in consumer preferences. We further assumed for simplicity and ease of exposition that the two segments of consumers (those who have their records with and ) are also uniformly distributed in the linear city. In doing so, we took the view that the disturbance to the consumer utility is independent of the likelihood of having digital records with a certain healthcare provider.
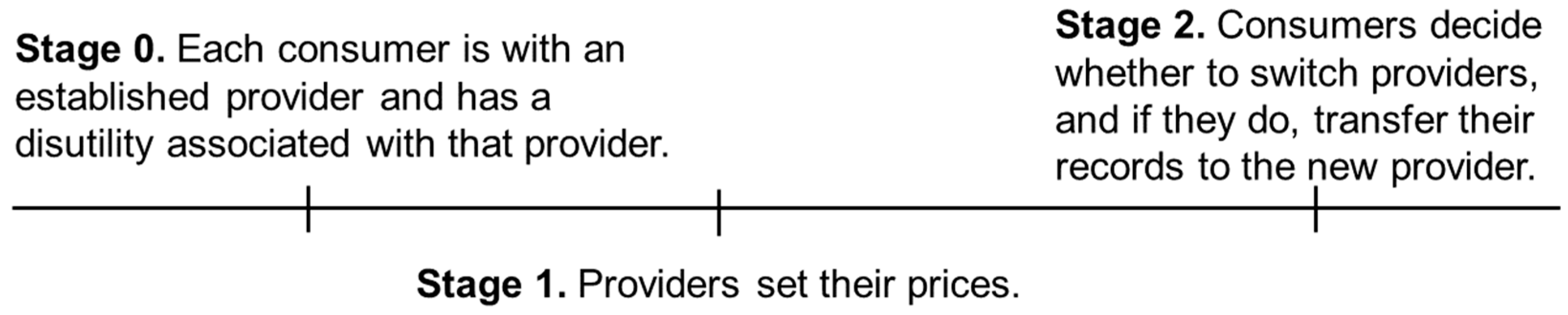
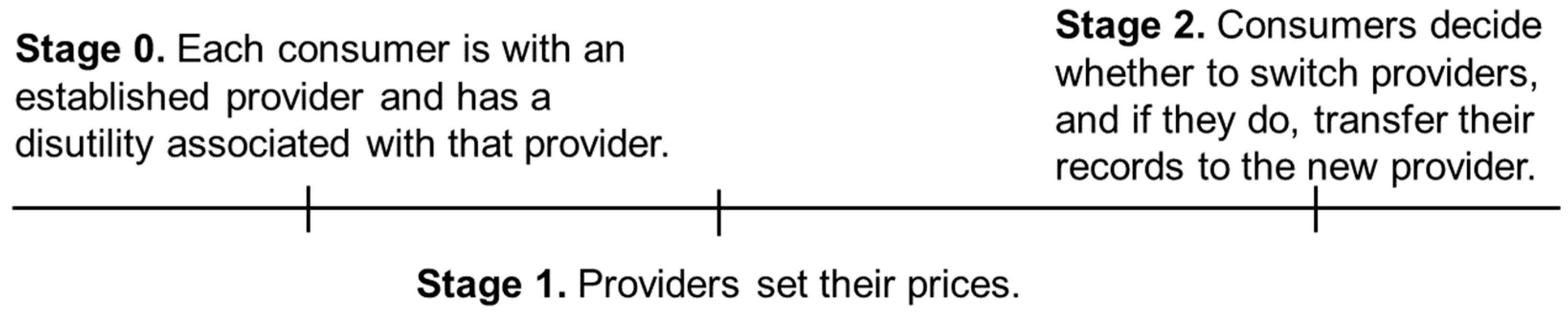
The process of seeking care from a new provider entails providing authorizations; establishing a medical and health history through transferring records from the previous provider to the new provider; filling out online forms at the new provider’s website; and repeating certain tests in case the previous test results are missing, incomplete, or simply deemed uninformative or unacceptable by the new provider. These tasks involve both pecuniary and non-pecuniary costs to the consumer. Especially in the case of emergencies during travel, these tasks may not be easily performed, in which case the patient may incur certain utility losses due to not getting the best treatment in the absence of pertinent information. We denote the expected cost of these tasks and situations to the consumer by
and henceforth call it the “switching cost.” As we will see later, the switching cost can drop when providers can electronically share documents. In the analyses that follow, the consumers who consider receiving care from a new provider weigh the utility gain from switching to the new provider on the one hand and the associated cost of the process on the other. The sequence of events is illustrated in
Figure 1.
It is worth noting that taking as exogenous (1) the pre-existing provider–patient relationships and (2) the subsequent changes in consumer preferences allow for the characterization of a market with consumer switching behavior in equilibrium in a static model. An alternative approach would have been to set up a dynamic model where each period would be characterized by a new disturbance to consumer preferences. The static model presented here captures the essence of all the strategic elements that are needed to answer the research questions presented in
Section 1 while maintaining simplicity and analytical tractability. When we introduce the availability of PGHD in
Section 3, we compare the consumers’ switching behavior in that case versus the benchmark case presented here. That comparison is based solely on the impact of the adoption of PGHD on the equilibrium outcomes.
Solution and analysis: In order to find the market shares of each provider, we needed to determine the precise utility change (i.e., locations) of consumers who are indifferent between working with their established provider and switching to a new one.
For consumers whose health records are initially maintained by
, the utility of obtaining care from the same provider is
, where
is the patient’s distance from the provider. Alternatively, these consumers can incur the cost
to switch to
and obtain the utility
. Taking into account the prices charged by these providers, the location of the indifferent consumer who has an established relationship with
satisfies
Similarly, for consumers whose records are initially maintained by
, the location of the indifferent consumer (denoted with
) satisfies
Recall that the size of the first segment of consumers is
. In the first segment,
proportion of consumers continue to work with
, while the rest switch to
. In the second segment,
proportion of consumers switch to
, while the rest continue to work with
. We assumed that there exists at least one consumer who switches from
to
and from
to
in equilibrium:
. Thus, the providers’ profits are given as
Solving for
and
and the profit-maximizing prices, we found the optimal profits to be the following, where the superscript
represents the benchmark case. Here, as well as later, all second-order conditions hold.
Note that the switching cost has opposite effects on the profits of the two providers. The provider that maintains fewer medical records at the beginning of the game benefits from a drop in the switching cost, while the other provider is harmed by it. This is because
and
for
, and vice versa, assuming a positive market share for both providers in equilibrium. We also found that the number of patients that switch to
and
are
and
, respectively. The rate of switching increases with the difference in utility that one provider offers with respect to the other and decreases with the cost of switching. The consumer surplus is calculated as follows:
3.2. The Availability and Providers’ Adoption of Patient-Generated Health Data
Much like the emergence of the genome, the proteome, and the microbiome, telemedicine and electronic health records are leading the emergence of the digitome—how patients’ digital records are used for diagnostic predictions and how patients respond to their therapies [
37]. In our context, the providers have the option to integrate and aggregate their patients’ PGHD on their EHR systems and monitor them at a cost denoted with
. We call this option the “adoption of PGHD on-premise.” This service benefits the patients of the adopting provider and increases their gross utility of receiving care there. The service is costly to the provider because, in addition to any necessary investment needed for the existing EHR infrastructure to handle the new data, there is also a need to develop stringent quality, supervision, and training programs to manage patient- and provider-specific risks associated with the storage and usage of PGHD. In particular, patients may pose a barrier to healthcare providers’ participation in PGHD due to various concerns, including issues related to trust, privacy, security, and identity (we thank an anonymous referee for this insightful comment) [
38].
The increase in utility depends on the nature of the provider–patient relationship. The utility increases more if the service is obtained from the established provider than when it is obtained from a new provider , where , unless the patient transfers any existing PGHD from the previous provider to the new provider. If both providers offer the PGHD service and the patient switches providers, then they may transfer any existing PGHD from the previous provider to the new provider at a cost denoted with (this is in addition to the cost associated with switching providers). In other words, the adoption of PGHD increases the switching cost for patients since additional data need to be transferred to the EHR system of the new provider for the patient to receive a similar service there. Subject to such a transfer, which we assumed to increase the utility , the patient obtains the full utility increase with the new provider’s PGHD service.
Solution and analysis: Each provider decides whether to adopt PGHD, resulting in a total of four potential outcome combinations. Thus, there are three
new scenarios to consider. The solution methodologies for these scenarios are similar to the one provided above. For example, when only
adopts PGHD, equations (1) and (2) above become
In Equation (7), the left-hand side of the equation has the additional utility because the established patients of benefit more from PGHD adoption compared with the patients who recently switched from and get the additional utility shown on the left-hand side of Equation (8).
The case where only
adopts PGHD is symmetric to the above, and in the case where both providers adopt PGHD, these equations become
The optimal outcomes for the providers in all these cases are presented in
Table 1, where
.
denotes the advantage
has over
due to offering a more valuable service and having a larger established clientele by
. The upper and lower expressions in each cell are the profits of
and
, respectively. As can be seen, the adopting provider potentially increases its profit subject to the implementation cost
being low enough.
We now investigate the providers’ incentives to aggregate their patients’ PGHD, which, as we will see, may indeed occur in equilibrium. However, we would like to first introduce a lemma that suggests that a provider’s decision to adopt PGHD may be negatively impacted by its competitor’s adoption. In other words, if a provider has the incentive to adopt PGHD when its competitor also adopts them, the provider will continue to have the incentive to adopt PGHD when its competitor does not adopt them.
Lemma 1. The incentive to aggregate and monitor PGHD is smaller when the competing provider adopts PGHD than when it does not.
Lemma 2 outlines which of the two providers is likely to have a larger incentive to adopt PGHD. The larger the market share, the easier it is for a provider to recoup the cost of aggregating and monitoring their patients’ PGHD. Since the provider that offers more utility to its patients is guaranteed to command a larger share of the market if it starts the game with a larger base of patients, it will also have a larger incentive to adopt PGHD than its competitor.
Lemma 2. The better/larger provider has a larger incentive to aggregate and monitor PGHD.
For ease of exposition, we henceforth consider the more realistic case where (since the services of a better provider will be utilized more). Let , which is always positive. is a measure of the advantage has over due to offering a more valuable service and having a larger established clientele . Also, let , where and . is a measure of the weighted average utility gain for ’s patients when it adopts PGHD. The larger the established clientele for , the larger the weighted average utility gain.
Proposition 1. If , then neither provider adopts PGHD. If , then only adopts PGHD. If , then both providers adopt PGHD.
As expected, the adoption of PGHD is more likely with a small implementation cost and a large incremental surplus for consumers due to adoption. We also observed that adoption by both providers is facilitated by a lower cost of transferring PGHD and a lower level of differentiation between providers in terms of taste, quality, and market share.
Note also that the providers make the same profit when they both adopt PGHD and when neither adopts them, but in the former case, providers incur the additional implementation cost. In other words, the adoption of PGHD puts the providers in a worse situation than the benchmark case. Using economic terminology, this represents a Prisoner’s dilemma for the providers—either would be better off not adopting PGHD, but competitive pressures force them to do so regardless. The benefits of PGHD adoption are completely absorbed by the consumers.
Proposition 2. The adoption of PGHD always raises the consumer surplus. However, when the PGHD adoption cost is high, the utility of the new service to the patients is low, and when the cost to transfer PGHD between providers is low, social welfare may drop with the adoption of PGHD.
The consumer surplus increases with the utility coming from the improved service
, while provider surplus decreases with the cost of PGHD implementation
. Comparing the benchmark case and the case where both providers adopt PGHD, all consumers get the additional
utility after adoption.
’s patients pay
extra, while
’s patients pay
less in equilibrium with PGHD compared with the benchmark case. Also, consumers who switch providers incur the extra switching cost
. Given that
, the net benefit to consumers (
less a fraction of
) is positive. The optimal prices are provided in
Appendix A in Equations (A5) through (A10).
We also found that the provider surplus increases with the cost of transferring PGHD
. This is because
’s profit decreases with
, while
’s profit increases with it. Comparing the profits in
Table 1 when neither provider adopts PGHD and when they both adopt,
’s profit increases more than that of
with respect to their profits in the benchmark case. The difference in differences of profits compared with the case with no PGHD adoption
equals
, suggesting that higher values of
benefits
more than it sets
back from a competitive perspective.
Social welfare is the sum of consumer surplus and provider profits, and it may drop for high values of and low values of and . We calculated the consumer surplus using Equation (6) for the benchmark case and similarly for other cases.
3.3. The PGHD Platform
We introduce the emergence of a platform in this section while keeping the possibility of providers integrating PGHD into their EHR systems themselves. Similar to Amazon Halo, a PGHD platform (henceforth referred to as “the platform”) offers an online data aggregation service to patients and providers. The data is encrypted and stored in the cloud in a format that readily integrates with the providers’ EHR systems. The main benefit of this service is that it provides patients with up-to-date online and secure access to their complete PGHD collected from various devices, wearable or otherwise. However, the online storage of health records, especially by a platform, may exacerbate consumers’ privacy concerns [
39], and we denote the associated cost with
. Granted, consumers may also experience a privacy loss when they share their PGHD with only their provider. However, because a platform can easily develop and offer value-added services using consumer health data, with or without the use of third parties, the privacy loss is typically greater than that in the case of sharing PGHD with a healthcare provider. When it comes to consumer psychology, it does not always matter what the platform can or cannot do legally; what really matters is what the platform can do with consumer health data in the presence of perceived ineffective or incomplete governmental regulation and/or potential noncompliance. Accordingly, we assumed that the utility loss in the latter case is zero.
To offer patients this value-added service, each provider should first sign up with the platform by paying the fee . A fixed fee implies that the platform does not price discriminate between providers. We later relaxed this assumption and allowed for price discrimination, which is equivalent to charging a price as a function of provider characteristics, including the number of patients being cared for.
After paying the platform fee, consumers can then establish an account with the platform and start aggregating their data in the cloud, knowing that their provider will have access to their data. Because this is a value-added service, we assumed that individuals derive a net utility benefit from the PGHD adoption and, therefore, always accept the service whenever their provider makes it available, despite the privacy loss (i.e., is sufficiently small). By strategically positioning itself between patients and providers, the platform can act as the intermediary as far as PGHD are concerned.
The platform takes on the responsibility of developing the technological infrastructure that enables the automatic transfer of patients’ PGHD from the cloud to the providers’ EHR systems. Having a platform account eliminates the cost a patient incurs when transferring their PGHD to a new provider () when both providers are on the platform. All the patient needs to do in this case is to grant appropriate access rights to the new provider. If the new provider has not joined the platform, they can download the records and email them to the provider or bring physical copies in person. We assume that the cost of transferring records in this fashion is still .
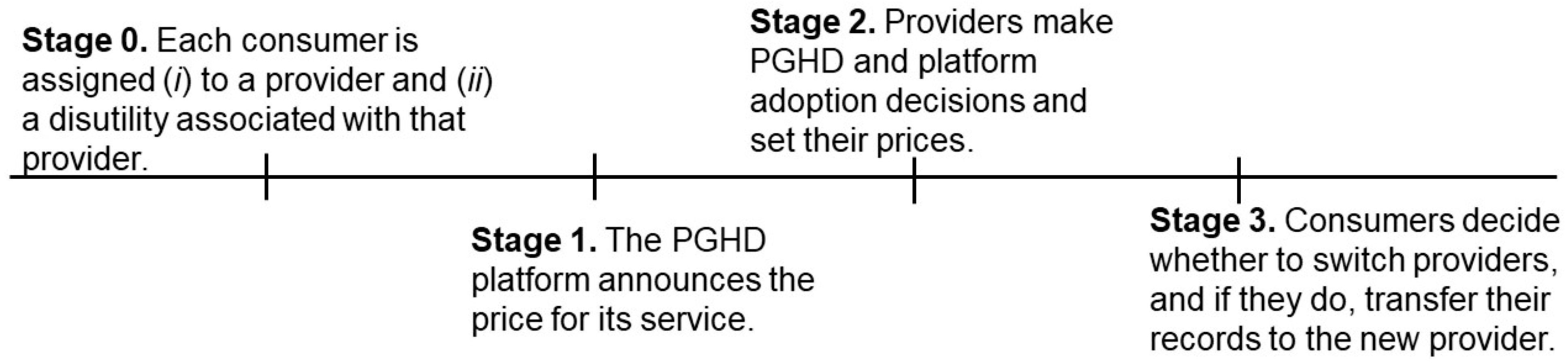
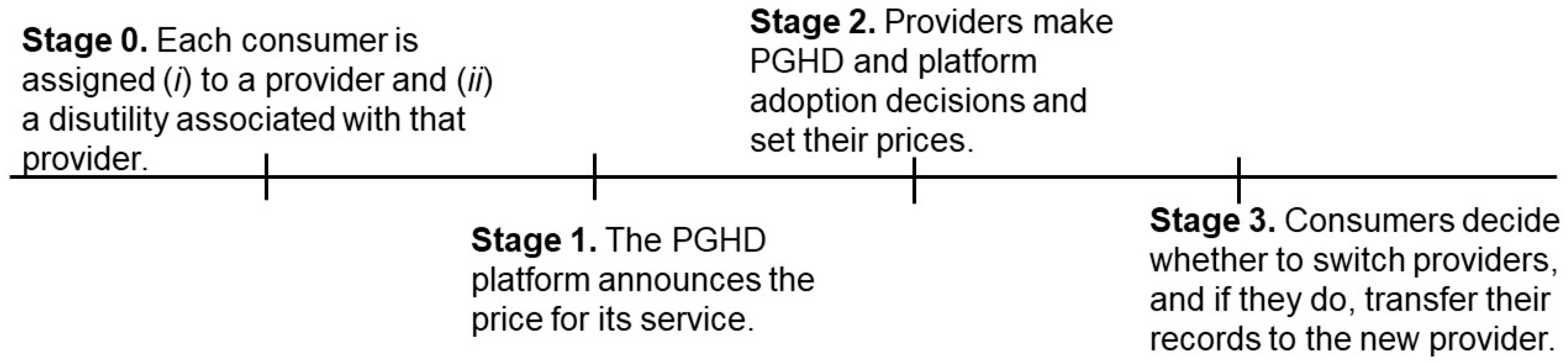
Assuming that the providers handle PGHD integrations themselves in the absence of a platform, the sequence of events is as follows. In the first stage, consumers are assigned to their providers with an associated disutility. In the second stage, the platform announces the price that it charges to providers for its service (
). In the third stage, providers simultaneously decide whether to aggregate their patients’ PGHD themselves or whether to join the platform. They then announce their prices (
and
) for delivering healthcare. Finally, given the switching costs and PGHD strategies of the providers, consumers decide which provider to work with and transfer their records if necessary. These stages are illustrated in
Figure 2.
Solution and analysis: A provider would either join the platform or handle the integration itself; it would not do both. The benchmark case in this section is the one where both providers handle PGHD integrations themselves, for which we have established provider profits (see
Table 1):
where the arguments of the profit expressions indicate the platform adoption decisions of providers (
J for “join” and
NJ for “do not join”; the first argument is for
and the second one is for
). Since both providers adopt and monitor PGHD, all consumers receive the full associated utility increase
. As we have seen in Proposition 1, the providers find themselves in this equilibrium when
is sufficiently small. Even if PGHD integration costs are not sufficiently small to lead to such an equilibrium today, we expect that Moore’s law will all but guarantee it in the not-too-distant future. We later compare the platform’s impact with the case when the providers’ benchmark decision is not to adopt PGHD at all.
The platform knows that it should structure its service in an attractive way to the providers. When a provider joins the platform, it gains access to the PGHD of its patients stored in the cloud and can then monitor patients remotely, thereby improving clinical outcomes and the value of its service as perceived by the patients. When both providers join the platform, then the sharing of PGHD between providers becomes seamless (). Since providers will join the platform as long as doing so will improve their bottom line, and because they still have the option to integrate PGHD into their EHR systems, the platform has to make sure that providers are better off with the platform than without it in pricing its service. The platform charges to providers and offers its service to consumers free of charge. This is in line with the freely available services, such as Apple’s Health app. The alternative would require the platform to charge both the providers and consumers, which would limit the providers’ ability to raise their prices in return for their platform adoption.
There are three possibilities regarding who joins the platform: (i) only , (ii) only , and (iii) both and . Recall that has more incentive to monitor PGHD than according to Lemma 2. The ability to offer the value-added service of monitoring PGHD to a larger group of patients means a larger economic incentive to make such an investment. We have seen that this is due to offering a more valuable service to a larger patient segment. It may be tempting to think that should have more incentive to join the platform than as well since the same incentive structure should be in play regardless of whether PGHD integration is executed on-premise or acquired through a platform. This was also our initial expectation. However, we will see that this is not necessarily true.
Suppose that only
and its patients join the platform. Recall that these patients incur the privacy cost
. Among the consumers whose records are initially maintained by
, the location of the one (denoted with
) who is indifferent between continuing with
and switching to
satisfies
For consumers whose records are initially maintained by
, the location of the consumer (denoted with
) who is indifferent between continuing with
and switching to
satisfies
The profit expressions are the same as in Equations (3) and (4). Solving for
and
and the profit-maximizing prices, we found the optimal profits to be the following:
where
is the price the platform charges for its service.
The case when only
and its patients join the platform is symmetric and leads to the following profit expressions:
The platform’s optimal prices in these outcomes
is derived in the proof of Lemma 3 in
Appendix A.
Suppose now that both providers and all patients join the platform. This time, patients who switch their providers no longer incur the cost
in transferring their PGHD. They simply log in to their PGHD account and give the new provider access to their data. This allows any switching patient to obtain the full additional utility of
with the new provider. Among the consumers whose records are initially maintained by
, the location of the one (denoted by
) who is indifferent between continuing with
and switching to
satisfies
The location of the indifferent consumer (denoted by
) among those whose records are initially maintained by
satisfies
Once again, the profit expressions are the same as in Equations (3) and (4). Solving for
and
and the profit-maximizing prices, we found the optimal profits to be the following:
The platform’s optimal price in this outcome
is derived in the proof of Lemma 3, which is available in
Appendix A.
Lemma 3. Given the option to integrate PGHD into EHR systems when not joining the platform, the smaller provider has a larger incentive to join the platform than the larger provider
The intuition is that since the platform does not accrue any additional benefit to the consumers because their PGHD will be monitored anyway, the provider with the larger patient base stands to lose more from the privacy concerns originating from the aggregation of PGHD by the platform. While both providers benefit from any cost advantages of joining the platform versus implementing the PGHD themselves, such benefits are mitigated by privacy costs, which are cumulatively higher for the larger provider.
Note that this result is predicated on our choice of benchmark. The larger provider would have a higher incentive to join the platform if we were to take the “No PGHD” as our comparison benchmark (see the top-left cell in
Table 1) due to the cost of PGHD integration
being too high or this option being unavailable altogether. The larger provider would then have a larger incentive to join the platform because it would benefit more from an increase in its service value due to having a larger customer base. Note that since the platform does not raise switching costs for patients, the larger provider does not benefit from a higher switching cost regime, unlike the case when both providers integrate PGHD into their EHR systems (which is our benchmark in this section). Accordingly, while the larger provider would have a larger incentive to join the platform in the absence of the in-house PGHD integration option, such an incentive would not be as strong as what we characterized in Lemma 2.
Now that we have established that would be the first to join the platform in the absence of price discrimination, we can state the possible equilibrium outcomes.
Proposition 3. In the absence of price discrimination, the following occurs:
If , the platform charges and works with and its patients only.
Otherwise, the platform charges and works with both providers and all patients.
The platform’s price is set in reference to the providers’ cost savings
, as well as their incentives associated with improving their service with respect to their competition. Since
has a larger incentive to join the platform (see Lemma 3), the platform can charge a relatively high price to enroll
only. Alternatively, it can lower its price and work with both providers. Since higher cost savings
mean a higher revenue from each provider, the platform is more likely to work with both providers when the cost of adopting PGHD is high. A lower privacy cost
and a lower switching cost (
) allows the platform to charge a higher price and increases the likelihood of working with both providers and all patients (see the proof of Lemma 3 and Proposition 3 in
Appendix A). Accordingly, publicly emphasizing and promoting strong data and privacy protection policies is essential for today’s platforms. Early indications suggest that this is indeed taking place. For example, Amazon’s Halo service encrypts any health data it collects in transit and in the cloud. It deletes body scan images and voice snippets automatically after processing. Consumers are able to delete all other data. Amazon also pledged to never sell consumers’ PGHD to any third party or to correlate them with any other data for product recommendation purposes or otherwise [
15].
Another implication of Proposition 3 is that a low PGHD transfer cost makes more likely to join the platform. Since is the second to join and has inherent incentives to keep switching costs high due to its larger established clientele, a drop in transfer costs makes more likely to join the platform. Accordingly, platforms have the economic incentive to invest in the interoperability of PGHD across various EHR systems. The ability to seamlessly transfer PGHD from the platform to the EHR system of a new provider who is not yet on the platform would increase that provider’s incentive to also join.
Proposition 4. The larger provider is always better off with the emergence of the platform. The smaller provider is indifferent when it is the only provider on the platform and better off when the competing provider also joins. Accordingly, the platform raises provider surplus. Consumers are worse off when only the smaller provider joins the platform; they may or may not be better off when both providers join. These comparisons are all with respect to the benchmark case where both providers integrate PGHD into their EHR systems when they do not join the platform.
Comparing in Equation (15) with the one in the benchmark case , we found that the larger provider benefits from the partnership between the platform and its competitor, mainly due to the elevated privacy concerns of ’s patients. In the equilibrium when only joins the platform, all of ’s patients incur the privacy cost . ’s patients pay less than the amount they pay in the benchmark case, and thus, ’s patients are cumulatively worse off by 2 with the platform. ’s patients pay more in this equilibrium than the amount they pay in the benchmark case, and thus, ’s patients are also worse off with the emergence of the platform.
In the equilibrium when both providers join the platform, all patients incur the privacy cost . ’s patients pay more than the amount they pay in the benchmark case, while ’s patients pay less. Also, patients who switch providers no longer incur . Therefore, the overall impact of both providers’ joining the platform on consumer surplus is not clear cut.
We found that the larger provider benefits from its competitor having more interest in joining the platform. The platform gives an advantage when it enrolls only since ’s patients now incur the privacy cost. The optimal price that is attractive enough for to join the platform makes both providers better off. As a result, benefits from ’s muted interest when the platform’s optimal strategy is to enroll both of them. Interestingly, every consumer is worse off when only joins the platform. ’s patients are worse off because they incur the privacy cost, and the improvement in the provider’s price does not make up for the privacy loss. ’s patients are worse off as well, as this provider finds it optimal to raise its price given the privacy loss of the competing provider’s patients, although the negative impact of ’s higher price for them is less than the privacy-related utility loss that ’s patients experience.
So far, we have assumed that the providers would integrate PGHD into their EHR systems when they do not join the platform and referred to this outcome as the “benchmark case” of this section. We previously established that this outcome represented a Prisoner’s dilemma for the providers since their profits drop after adopting PGHD (see Proposition 1), and we took this outcome as given when analyzing the optimal strategies in the presence of the platform. It is in the context of this “new” benchmark case that producer surplus rises with the emergence of the platform. Since the platform does not face the PGHD implementation cost structure that providers do, it can reduce its price as necessary in order to make its service attractive to the providers. Similar to Lemma 2 and contrary to Lemma 3, when the on-premise implementation of PGHD is not a viable option for the providers for whatever reason, has a larger incentive to join the platform than , and the platform would price its service accordingly. Since providers are more likely to join the platform than to implement PGHD themselves due to the platform’s cost advantage, a Prisoner’s dilemma (i.e., a drop in equilibrium profits) is now more likely. However, given what we found in Proposition 4 regarding the provider surplus, such a dilemma is less unfavorable for the providers than the one in which they implement PGHD themselves.
Propositions 3 and 4 assume that the platform charges the same price to both providers. We noted earlier that we would relax this assumption and allow for price discrimination. Charging a price as a function of provider characteristics, including the number of patients being cared for, can be possible. Our last proposition outlines the impact of the platform’s ability to price discriminate on providers’ profits. Please note that when we allow for price discrimination, the platform charges a separate price to each provider by taking into account each provider’s characteristics, such as perceived quality and the number of patients.
Proposition 5. The larger provider is indifferent to price discrimination. The smaller provider benefits from price discrimination when the platform’s optimal strategy is to work with the smaller provider only in the absence of price discrimination, and it is worse off otherwise.
The platform is strictly better off as it either enrolls the larger provider that it would not otherwise or by charging a higher price to the smaller provider (when working with both providers). Due to having a smaller incentive to join the platform than , is always indifferent to joining the platform—with or without price discrimination. The potentially interesting finding is that can be better off with price discrimination when the platform’s optimal strategy is to work with only in the absence of price discrimination, in which case is indifferent to joining the platform (it makes the same profit as in the benchmark case). This is because the platform works with both providers when it can price discriminate, and the highest price it can charge is what makes indifferent to joining when is on the platform. Since makes more profit when only joins (in which case ’s patients incur the privacy cost while ’s patients do not) compared with its profit in the benchmark case where neither provider joins the platform, is better off with price discrimination under these conditions.
We established earlier that a low PGHD implementation cost , a high privacy cost , and a high PGHD transfer cost are associated with the optimal platform strategy of working with the smaller provider only in the absence of price discrimination. Therefore, these are also the same conditions that render the platform’s price discrimination a Pareto-optimal scenario for the market participants.




{kind=link}
{kind=link}