
Data-Driven Decision Making and Proactive Citizen–Scientist Communication: A Cross-Sectional Study on COVID-19 Vaccination Adherence

 ,
,  ,
,
Abstract
:1. Introduction
- To provide an efficient technological solution (digital platform) for communication between scientists and the general population to discuss personalized risk factors for severe COVID-19 disease.
- To use this technological solution to investigate the association between vaccination readiness and the risk of COVID-19 infection or severe disease among the population of Latvia within an exploratory study.
2. Materials and Methods
2.1. Development of the Digital Platform
2.2. Exploratory Study
2.2.1. Study Design and Population
2.2.2. Statistical Analysis
Then, Severity Percentage = ((SEVERITY ∗ 0.95)/4.6) ∗ 100.
3. Results
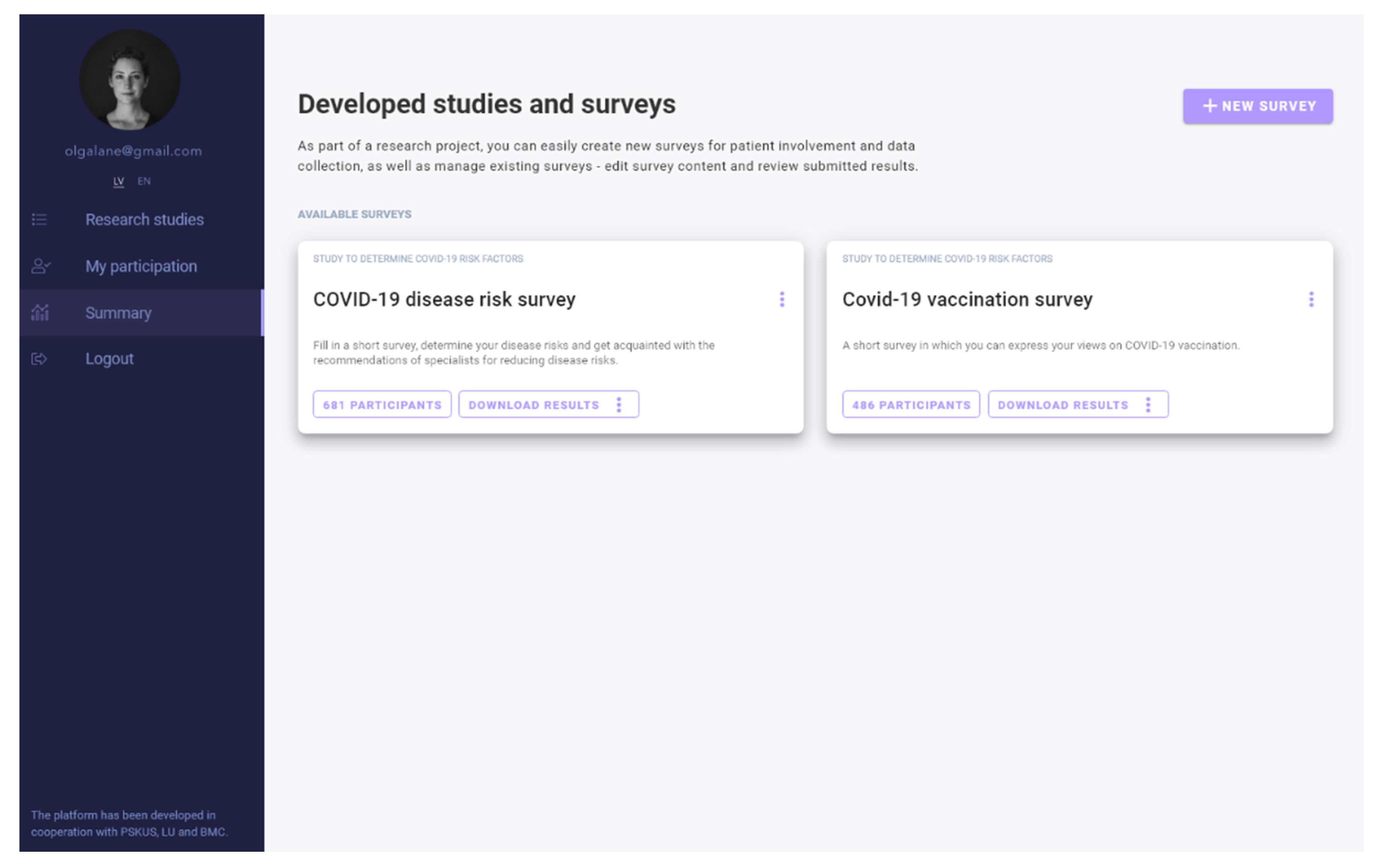
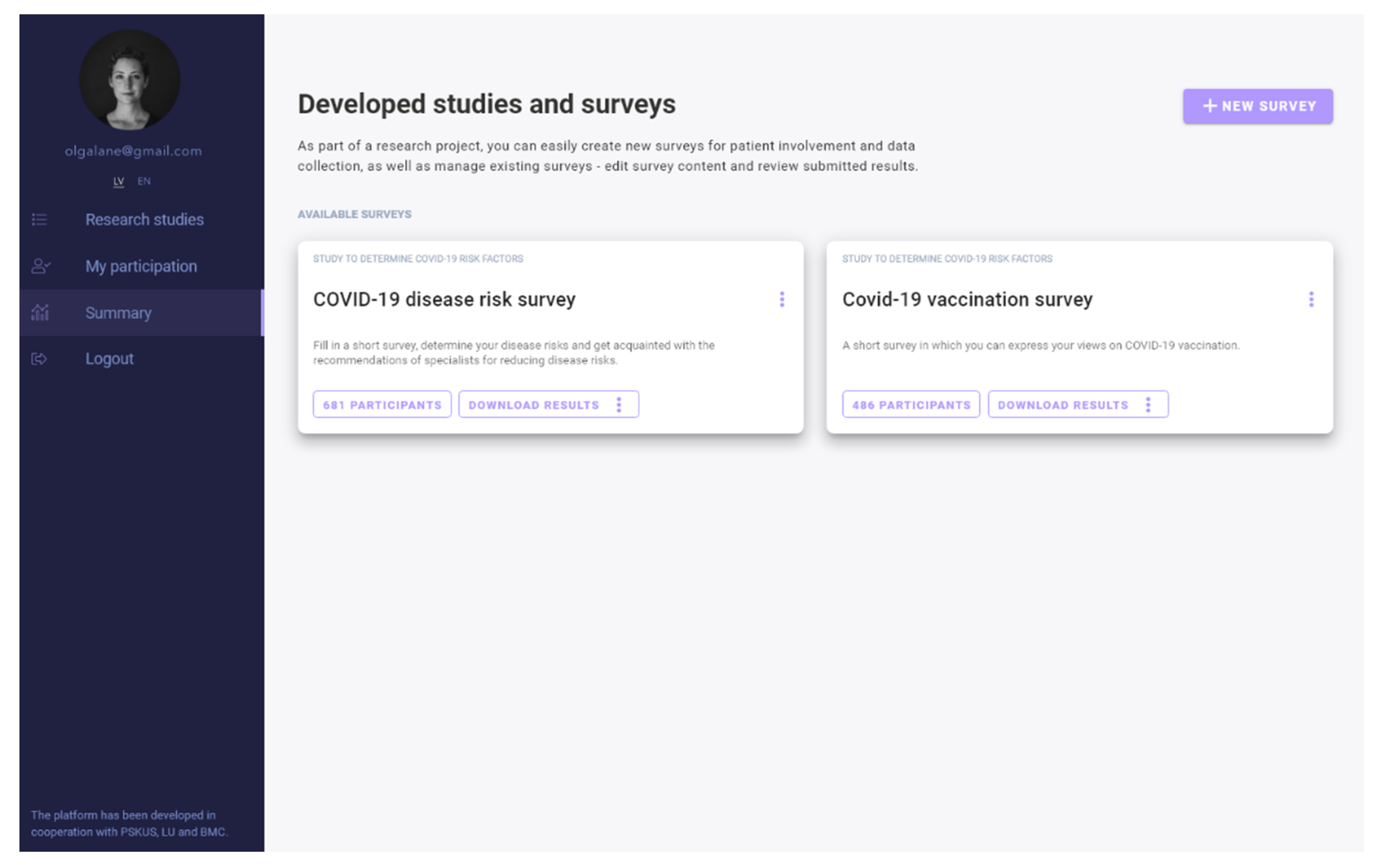
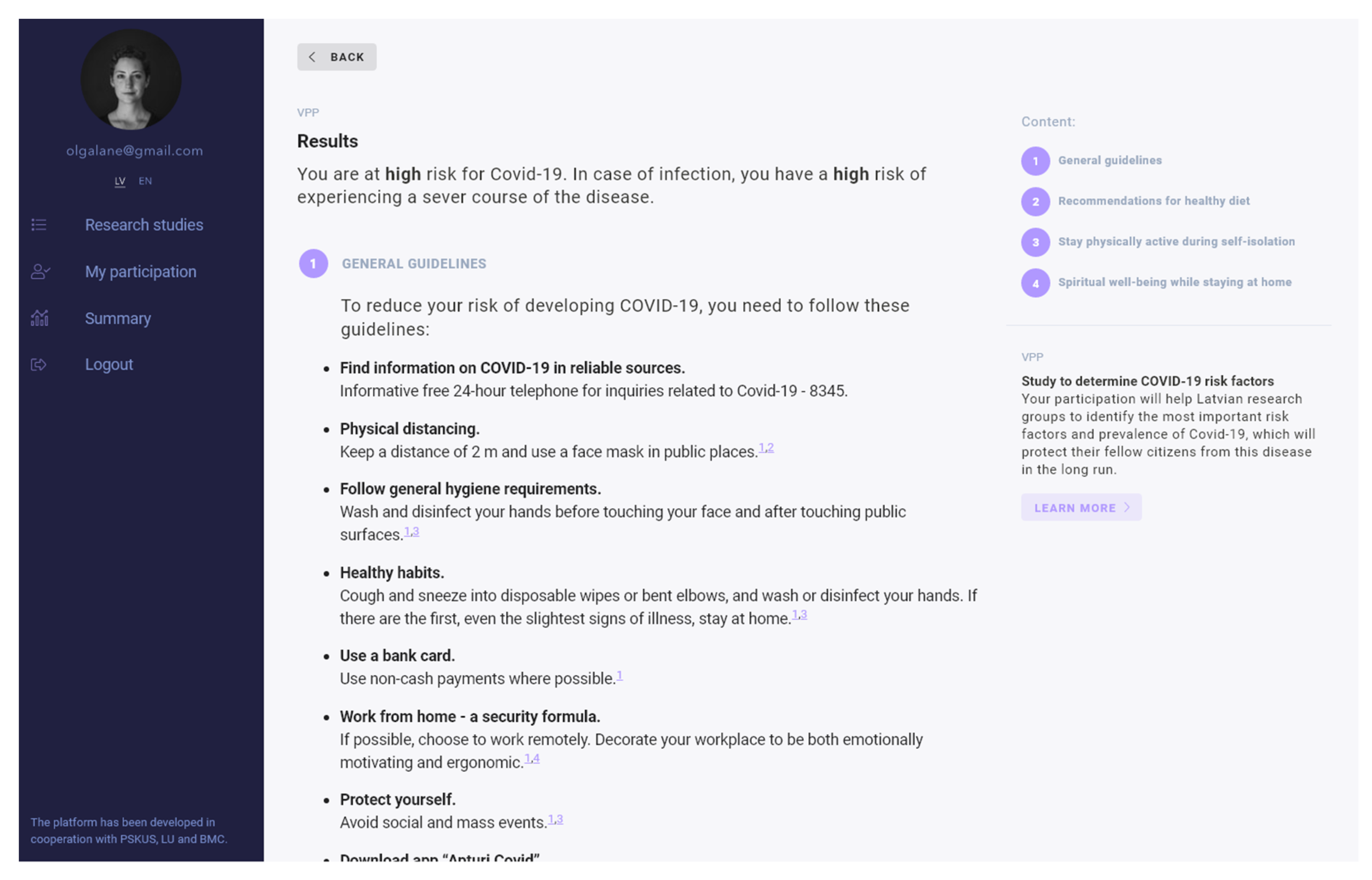
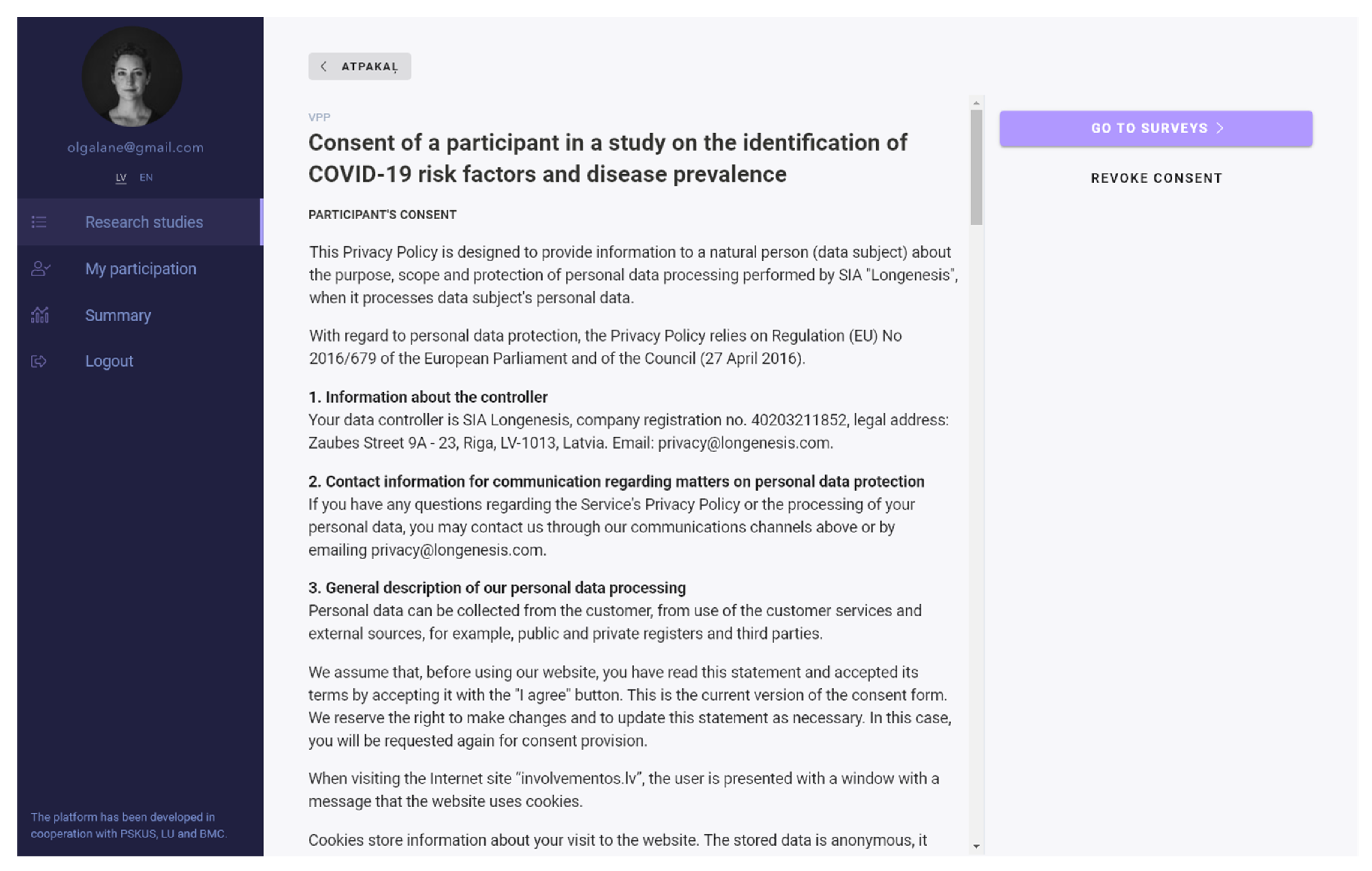
3.1. Structure of the Digital Platform
3.2. Results of the Exploratory Study
4. Discussion
Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
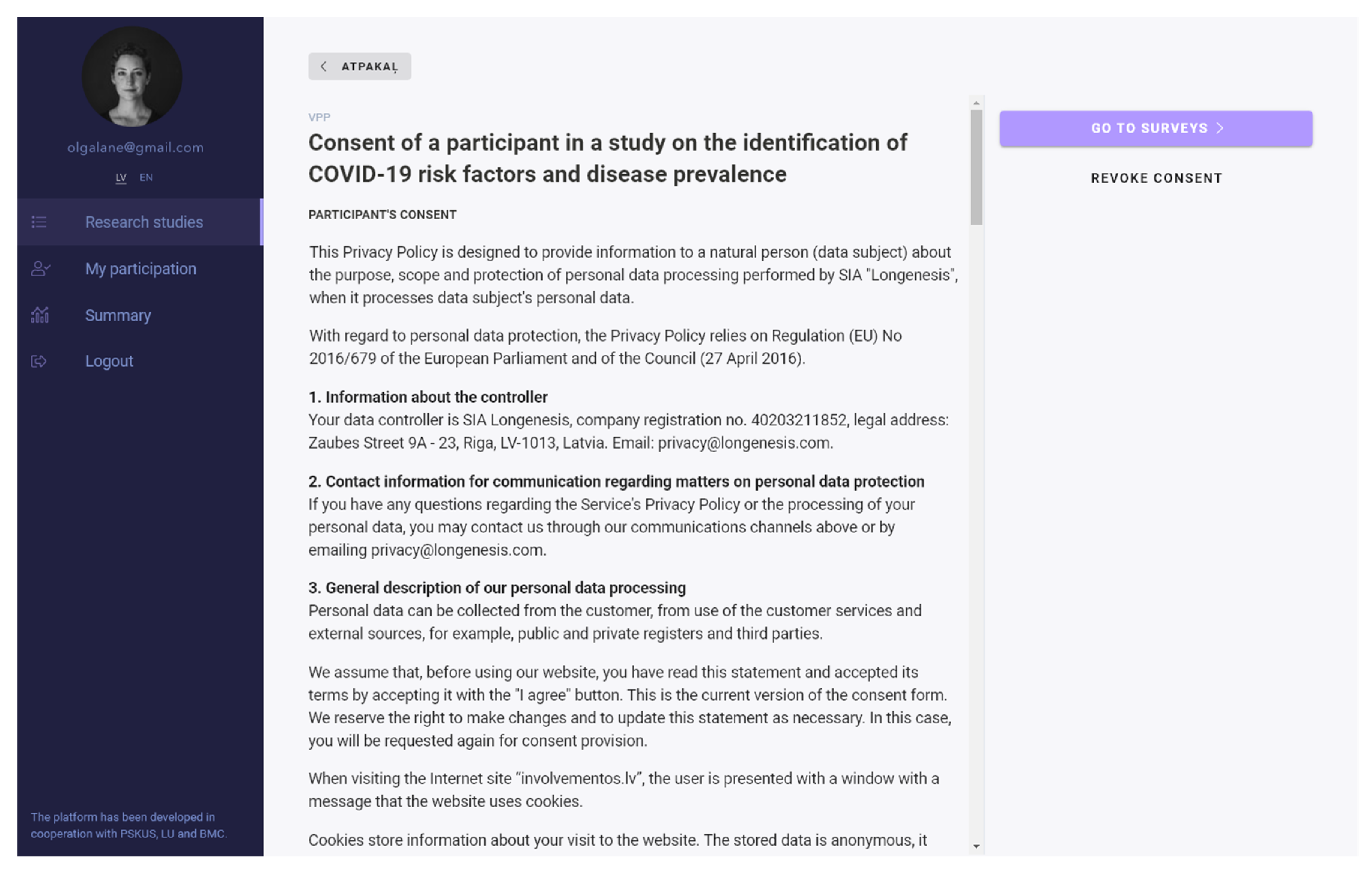
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
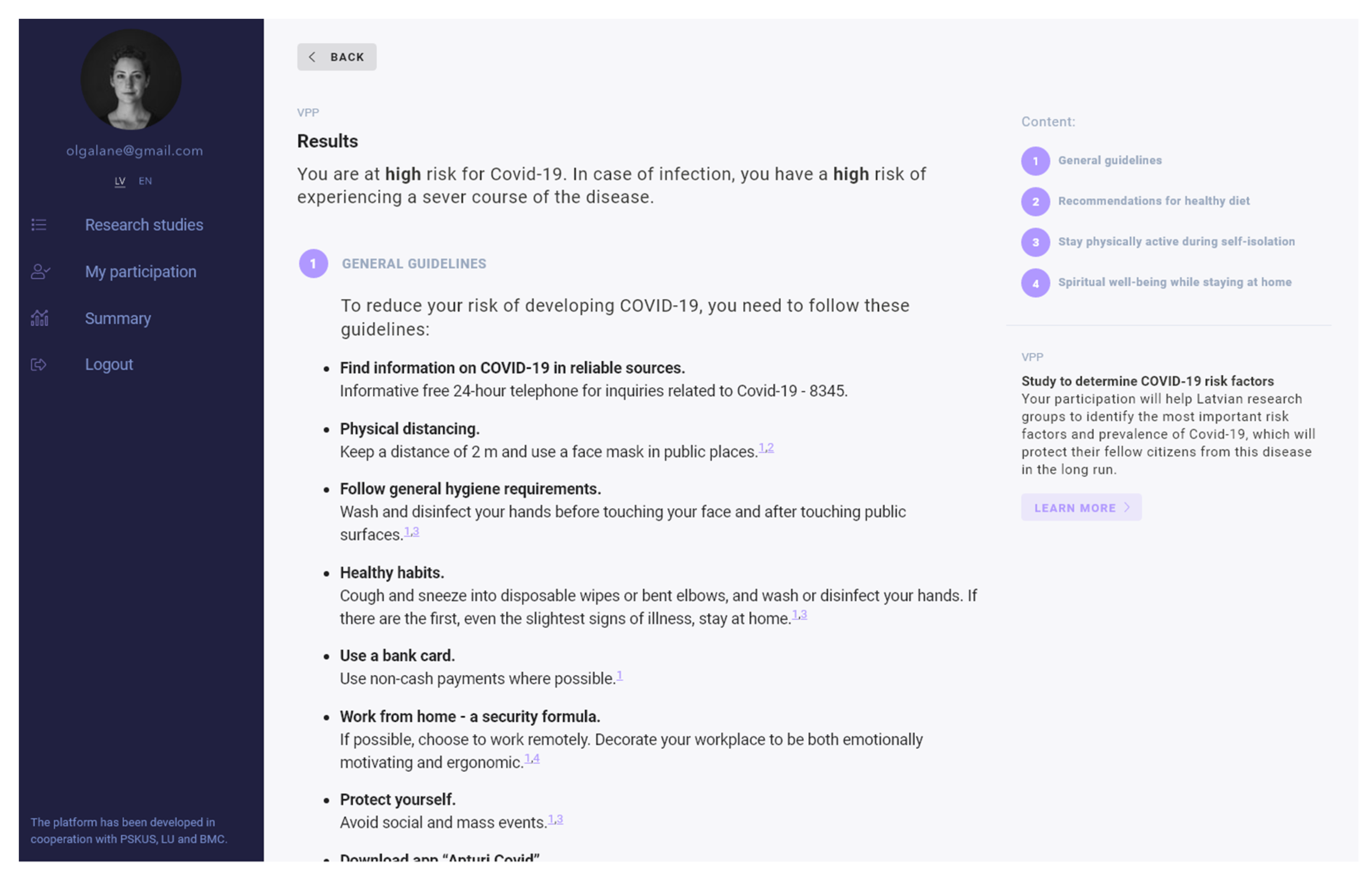
Appendix A. Standardized Recommendations for Study Participants
- 1.
- GENERAL GUIDELINE
- Seek information on COVID-19 in reliable sources. Informative free 24-h telephone for inquiries related to COVID-19: 8345.
- Physical distancing. Keep a distance of 2 m and use a face mask in public places.
- Follow general hygiene requirements. Wash and disinfect hands before touching the face and after touching public surfaces.
- Healthy habits. Cough and sneeze into disposable wipes or bent elbow, and wash or disinfect your hands. If there are the first, even the slightest, signs of illness, stay at home.
- Use a bank card. Use non-cash payments as much as possible.
- Working from home is a security formula. If possible, choose to work remotely. Arrange your workplace to be both emotionally motivating and ergonomic.
- Protect yourself. Avoid social and mass events.
- Download the Stop COVID app. The app is the fastest way to find out if you have been in contact with a COVID-19 carrier. Do not remain ignorant, and make informed decisions. Find out more at https://www.apturicovid.lv/#en (accessed on 18 November 2021).
- Avoid sick people.
- Shop when the store is not crowded or ask someone to do it for you.
- Avoid public transport during traffic congestion.
- Exercise outdoors.
- Get medical attention immediately if you notice any symptoms of COVID-19.
- 2.
- RECOMMENDATIONS FOR HEALTHY NUTRITION
- Cook at home, plan your purchases in time—create your menu!
- The right strategy for creating a menu—prioritize fresh produce.
- Be aware of the portion size of the food!
- Control your salt and sugar intake, and as much as possible avoid trans fats.
- 3.
- STAY PHYSICALLY ACTIVE DURING SELF-ISOLATION
- Take short active breaks during the day. Dancing, playing with children, and doing housework like cleaning and gardening are just some of the ways to stay active at home.
- Attend sports classes online. Take advantage of the available online gym classes. Many of them are free and can be found on YouTube. Before trying them, carefully evaluate your abilities!
- Take a walk. Even in small spaces, walking around or walking on the spot can help keep you active.
- Get up. Reduce sedentary time whenever you get up. Ideally, try to interrupt your sitting time every 30 min.
- 4.
- MENTAL WELL-BEING AT HOME
- Pause. Inhale. Reflect. Inhale slowly through your nose, then exhale slowly. Such breathing is one of the best ways to relieve stress, as it signals to your brain the need for rest.
- Connect with others. Contact people close to you regularly. Tell them how you feel and share your thoughts.
- Limit the time you spend reading the news. Better use this time to relax from your computer screen or take a walk in the fresh air.
- Schedule time for hobbies. If we feel anxious, lonely or low, we can stop doing things that we normally enjoy.
- 5.
- REFERENCES
- [1]
- https://likumi.lv/ta/id/314641-ieteikumi-covid-19-infekcijas-profilaksei (accessed on 18 November 2021).
- [2]
- https://www.spkc.gov.lv/lv/masku-lietosana (accessed on 18 November 2021).
- [3]
- https://www.ecdc.europa.eu/en/covid-19/prevention-and-control/protect-yourself (accessed on 18 November 2021).
- [4]
- https://www.spkc.gov.lv/lv/darba-devejiem (accessed on 18 November 2021).
Appendix B

{kind=link}
{kind=link}
{kind=link}
| Area of Investigation | Questions | Explanation of Measures |
|---|---|---|
| Demographic and anthropometric questions (9 items) | What is your age group (in years)? What is your gender? What is your marital status? How many children do you have? What is your education level? What is your district of residence? Are you currently pregnant? What is your weight? What is your height? | 7 groups with 10 years range 4 categories 5 categories Range 0–4 and more 4 categories (from less than high school to postgraduate) List of Latvia districts Pregnancy status (yes/no) Kg Cm |
| COVID-19-related behavioral factors that could increase the risk of infection (15 items) | What is your smoking status? Duration of cigarette smoking When did you quit smoking? Which way of transport do you use? What are your working conditions? Do you comply with social distancing? Do you use face mask? How often do you disinfect your hands? Do you disinfect your hands before touching your face? How much do you worry about COVID-19? What are your living conditions? What is your profession? What are your thoughts about the existing COVID-19 restrictions? Did you in last 14 days travel abroad or visit mass events? What is in your opinion of the percentage of people that follow the official state COVID-19 restrictions? | 4 categories Years Years 4 items 7 items Yes/no 3 categories 3 categories 3 categories 3 categories 4 categories of living density 4 categories, increased risk of infection in workplace 3 categories, attitude 4 answers 3 categories (from < 50% to > 80%) |
| Personal risk factors that could increase the risk of severe disease (10 items) | Do you have chronic diseases? | 10 items (yes/no) |
| Reasons for vaccination (10 items) | Please explain your motivation to vaccinate or not: • Fear of COVID-19 • To protect my family and our relatives • Confidence in our healthcare providers • Confidence in our pharmaceutical industry • The COVID-19 vaccines are revolutionary and use innovative technology • Employer recommends/demands • Confidence in governmental leadership’s guidance • It is my civic responsibility to take this vaccine • Myself or relatives got sick with COVID-19 • Free of charge | Scaled from 1 (completely disagree) to 5 (completely agree) |
References
- The Global Risks Report 2021. World Economic Forum. Available online: https://www.weforum.org/reports/the-global-risks-report-2021 (accessed on 26 March 2021).
- Status of COVID-19 Vaccines within WHO EUL/PQ Evaluation Process Name. Available online: https://extranet.who.int/pqweb/sites/default/files/documents/Status_COVID_VAX_16Feb2021.pdf (accessed on 26 March 2021).
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet. Lancet Publ. Group 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Latvia COVID: 133,098 Cases and 2370 Deaths—Worldometer. Available online: https://www.worldometers.info/coronavirus/country/latvia/ (accessed on 31 May 2021).
- COVID-19 Izmeklējumi, Apstiprinātie Gadījumi un Iznākumi—Datu Kopas—Latvijas Atvērto datu Portāls. Available online: https://data.gov.lv/dati/lv/dataset/covid-19 (accessed on 31 May 2021).
- Zaudējis Spēku—Par Ārkārtējās Situācijas Izsludināšanu. Available online: https://likumi.lv/ta/id/313191 (accessed on 31 May 2021).
- Aktualitātes par COVID-19 Slimību Profilakses un Kontroles Centrs. Available online: https://www.spkc.gov.lv/lv/aktualitates-par-covid-19 (accessed on 31 May 2021).
- Coronavirus (COVID-19) Vaccinations—Statistics and Research—Our World in Data. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 26 March 2021).
- Latvia Demographics Profile. Available online: https://www.indexmundi.com/latvia/demographics_profile.html (accessed on 31 May 2021).
- Wymant, C.; Ferretti, L.; Tsallis, D.; Charalambides, M.; Abeler-Dörner, L.; Bonsall, D.; Hinch, R.; Kendall, M.; Milsom, L.; Ayres, M.; et al. The epidemiological impact of the NHS COVID-19 App. Nature 2021, 594, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.spkc.gov.lv/lv/jaunums/lietotne-apturi-covid-lejupieladeta-300-000-reizu (accessed on 18 November 2021).
- Shen, S.; Dubey, V. Addressing vaccine hesitancy. Clinical guidance for primary care physicians working with parents. Can. Fam. Physician 2019, 65, 175–181. [Google Scholar] [PubMed]
- Butler, R.; McDonald, N.E. Diagnosing the determinants of vaccine hesitancy in specific subgroups: The Guide to Tailoring Immunization Programmes (TIP). Vaccine 2015, 33, 4176–4179. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, F.A.; Ahmad, B.; Khalid, M.D.; Fazal, A.; Javaid, M.M.; Butt, D.Q. Factors influencing COVID-19 vaccine hesitancy and acceptance among the Pakistani population. Hum. Vaccines Immunother. 2021, 17, 3365–3370. [Google Scholar] [CrossRef]
- Cerda, A.A.; Garcia, L.Y. Hesitation and refusal factors in individuals’ decision-making process regarding a Coronavirus Disease 2019 vaccination. Front. Public Health 2021, 9, 626852. [Google Scholar] [CrossRef]
- Syed Alwi, S.A.R.; Rafidah, E.; Zurraini, A.H.; Juslina, O.; Brohi, I.B.; Lukas, S. A survey on COVID-19 vaccine acceptance and concern among Malaysians. BMC Public Health 2021, 21, 1129. [Google Scholar] [CrossRef]
- Tam, C.C.; Qiao, S.; Li, X. Factors associated with decision making on COVID-19 vaccine acceptance among college students in South Carolina. Psychol Health Med. 2021. [Google Scholar] [CrossRef]
- Enhancing Public Trust in COVID-19 Vaccination: The Role of Governments. Available online: https://www.oecd.org/coronavirus/policy-responses/enhancing-public-trust-in-covid-19-vaccination-the-role-of-governments-eae0ec5a/ (accessed on 18 November 2021).
- Machingaidze, S.; Wiysonge, C.S. Understanding COVID-19 vaccine hesitancy. Nat. Med. 2021, 27, 1338–1344. [Google Scholar] [CrossRef]
- Gao, Y. COVID-19: Risk factors for critical illness. EClinicalMedicine 2020, 25, 100507. [Google Scholar] [CrossRef]
- Wolff, D.; Nee, S.; Hickey, N.S.; Marschollek, M. Risk factors for COVID-19 severity and fatality: A structured literature review. Infection 2021, 49, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. [Google Scholar] [CrossRef]
- Budd, J.; Miller, B.S.; Manning, E.M.; Lampos, V.; Zhuang, M.; Edelstein, M.; Rees, G.; Emery, V.C.; Stevens, M.M.; Keegan, N.; et al. Digital technologies in the public-health response to COVID-19. Nature Medicine. Nat. Res. 2020, 19, 1183–1192. [Google Scholar] [CrossRef]
- Zhang, M.; Smith, H.E. Digital tools to ameliorate psychological symptoms associated with COVID-19: Scoping review. J. Med. Internet Res. 2020, 22, e19706. [Google Scholar] [CrossRef] [PubMed]
- El-Elimat, T.; AbuAlSamen, M.M.; Almomani, B.A.; Al-Sawalha, N.A.; Alali, F.Q. Acceptance and attitudes toward COVID-19 vaccines: A cross-sectional study from Jordan. PLoS ONE 2021, 16, e0250555. [Google Scholar] [CrossRef]
- Rader, B.; White, L.F.; Burns, M.R.; Chen, J.; Brilliant, J.; Cohen, J.; Shaman, J.; Brilliant, L.; Kraemer, M.U.G.; Hawkins, J.B.; et al. Mask-wearing and control of SARS-CoV-2 transmission in the USA: A cross-sectional study. Lancet Digit Health 2021, 3, e148–e157. [Google Scholar] [CrossRef]
- Gee, J.; Marquez, P.; Su, J.; Calvert, G.M.; Liu, R.; Myers, T.; Nair, N.; Martin, S.; Clark, T.; Markowitz, L.; et al. First Month of COVID-19 Vaccine Safety Monitoring—United States, December 14, 2020–January 13, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 283–288. [Google Scholar] [CrossRef]
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and vaccine hesitancy: A longitudinal study. PLoS ONE 2021, 16, e0250123. [Google Scholar] [CrossRef]
- Latkin, C.A.; Dayton, L.; Yi, G.; Colon, B.; Kong, X. Mask usage, social distancing, racial, and gender correlates of COVID-19 vaccine intentions among adults in the US. PLoS ONE 2021, 16, e0246970. [Google Scholar] [CrossRef]
- Burki, T. The online anti-vaccine movement in the age of COVID-19. Lancet Digit. Health 2020, 2, e504–e505. [Google Scholar] [CrossRef]
- Managing the COVID-19 infodemic: Promoting Healthy Behaviours and Mitigating the Harm from Misinformation and Disinformation. Available online: https://www.who.int/news/item/23-09-2020-managing-the-covid-19-infodemic-promoting-healthy-behaviours-and-mitigating-the-harm-from-misinformation-and-disinformation (accessed on 26 March 2021).
- On the Importance of Human-Centricity and Data Preface. Available online: http://www3.weforum.org/docs/WEF_On_the_Importance_of_Human_Centricity_2021.pdf (accessed on 26 March 2021).
- Kretzschmar, M.E.; Rozhnova, G.; Bootsma, M.C.J.; van Boven, M.; van de Wijgert, J.H.H.M.; Bonten, M.J.M. Impact of delays on effectiveness of contact tracing strategies for COVID-19: A modelling study. Lancet Public Health 2020, 5, e452–e459. [Google Scholar] [CrossRef]
- Digital Engagement Platform. Available online: https://www.iesaistos.lv/ (accessed on 29 March 2021).
- Chatterjee, R.; Bajwa, S.; Dwivedi, D.; Kanji, R.; Ahammed, M.; Shaw, R. COVID-19 Risk Assessment Tool: Dual application of risk communication and risk governance. Prog. Disaster Sci. 2020, 7, 100109. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Agarwala, N.; Kundu, P.; Harvey, B.; Zhang, Y.; Wallace, E.; Chatterjee, N. Individual and community-level risk for COVID-19 mortality in the United States. Nat. Med. 2020, 27, 264–269. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Version 26.0; IBM Corp.: Armonk, NY, USA, 2019. [Google Scholar]
- Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the Protection of Natural Persons with Regard to the Processing of Personal Data and on the Free Movement of Such Data, and Repealing Directive 95/46/EC. Gen. Da. Off. J. 2016, 119, 1–88. Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj/eng# (accessed on 18 November 2021).
- Benis, A.; Khodos, A.; Ran, S.; Levner, E.; Ashkenazi, S. Social Media Engagement and Influenza Vaccination During the COVID-19 Pandemic: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e25977. [Google Scholar] [CrossRef] [PubMed]
- Benis, A.; Seidmann, A.; Ashkenazi, S. Reasons for Taking the COVID-19 Vaccine by US Social Media Users. Vaccines 2021, 9, 315. [Google Scholar] [CrossRef]
- Hyland, P.; Vallières, F.; Hartman, T.K.; McKay, R.; Butter, S.; Bentall, R.P.; McBride, O.; Shevlin, M.; Bennett, K.; Mason, L.; et al. Detecting and describing stability and change in COVID-19 vaccine receptibility in the United Kingdom and Ireland. PLoS ONE 2021, 16, e0258871. [Google Scholar] [CrossRef]
- Edwards, B.; Biddle, N.; Gray, M.; Sollis, K. COVID-19 vaccine hesitancy and resistance: Correlates in a nationally representative longitudinal survey of the Australian population. PLoS ONE 2021, 16, e0248892. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Country Readiness and Delivery. Available online: https://www.who.int/initiatives/act-accelerator/covax/covid-19-vaccine-country-readiness-and-delivery (accessed on 26 March 2021).
- Gelfand, M.J.; Jackson, J.C.; Pan, X.; Nau, D.; Pieper, D.; Denison, E.; Dagher, M.; Lange, P.A.M.V.; Chiu, C.-Y.; Wang, M. The relationship between cultural tightness–looseness and COVID-19 cases and deaths: A global analysis. Lancet Planet Health 2021, 5, 135–179. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef]
- König, R.; Seifert, A.; Doh, M. Internet use among older Europeans: An analysis based on SHARE data. Univ. Access Inf. Soc. 2018, 17, 621–633. [Google Scholar] [CrossRef]
- Merkel, S.; Kucharski, A. Participatory Design in Gerontechnology: A Systematic Literature Review. Gerontologist 2019, 59, e16–e25. [Google Scholar] [CrossRef] [PubMed]
- Van Jaarsveld, G.M. The Effects of COVID-19 Among the Elderly Population: A Case for Closing the Digital Divide. Front. Psychiatry 2020, 11, 577427. [Google Scholar] [CrossRef] [PubMed]
- Bidmon, S.; Terlutter, R. Gender differences in searching for health information on the internet and the virtual patient-physician relationship in Germany: Exploratory results on how men and women differ and why. J. Med. Internet Res. 2015, 17, e156. [Google Scholar] [CrossRef] [PubMed]
- Longenesis Curator Tool. Available online: www.longenesis.com/curator (accessed on 18 November 2021).
| Variable | Category | N = 467 |
|---|---|---|
| Gender, N (%) | 333 (71.3) | |
| 5 (1.1) | ||
| Age, median (IQR) | 34.0 (28.0–42.0) | |
| Marital status, N (%) | Single | 121 (25.9) |
| Married/civil union | 306 (65.5) | |
| Separated or divorced | 17 (3.6) | |
| Widowed | 4 (0.9) | |
| Number of children, N (%) | 0 | 238 (51.1) |
| 1 | 88 (18.8) | |
| 2 | 86 (18.5) | |
| 3 | 38 (8.2) | |
| 4 and more | 11 (2.4) | |
| Education, N (%) | Less than high school | 5 (1.1) |
| High school | 116 (24.9) | |
| Bachelor’s degree | 147 (31.5) | |
| Master’s degree | 193 (41.4) | |
| Location | Capital city | 289 (62.3) |
| Other cities | 49 (10.6) | |
| Rural areas | 126 (27.2) | |
| Type of dwelling | Apartment | 358 (76.7) |
| Private home | 104 (22.3) | |
| Dormitory | 4 (0.9) | |
| Nursing home | 1 (0.2) | |
| Number of people at home, median (IQR) | 2.0 (2.0–4.0) | |
| Number of rooms, median (IQR) | 3.0 (2.0–4.0) |
| Vaccination Readiness | ||||
|---|---|---|---|---|
| Variable | Category/Factor Affecting Motivation | Yes N = 401 (85.9%) | No/Not Sure N = 66 (14.1%) | p |
| Smoking status, N (%) | Never | 203 (84.9) | 36 (15.1) | 0.59 |
| Not a smoker < 2 years | 42 (82.4) | 9 (16.4) | ||
| Smoker < 5 years | 26 (92.9) | 2 (7.1) | ||
| Smoker ≥ 5 years | 56 (87.5) | 8 (12.5) | ||
| BMI (kg/m2), median (IQR) | 23.9 (21.5–27.6) | 24.8 (22.1–29.7) | 0.24 | |
| Having chronic disease, N (%) | No | 334 (85.4) | 57 (14.6) | 0.59 |
| Yes | 67 (88.2) | 9 (11.8) | ||
| Transport, N (%) | Stay at home | 55 (88.7) | 7 (11.3) | 0.09 |
| Walking | 96 (88.9) | 12 (11.1) | ||
| Private transport | 203 (86.4) | 32 (13.6) | ||
| Public transport | 47 (75.8) | 15 (24.2) | ||
| Profession, N (%) | Health care | 51 (98.1) | 1 (1.9) | 0.05 |
| Direct with people | 46 (80.7) | 11 (19.3) | ||
| Indirect with people | 23 (85.2) | 4 (14.8) | ||
| Other | 281 (84.9) | 50 (15.1) | ||
| Use of disinfecting solution, N (%) | No | 92 (76.0) | 29 (24.0) | <0.01 |
| Sometimes | 158 (89.3) | 19 (10.7) | ||
| Yes | 151 (89.3) | 18 (10.7) | ||
| Disinfection of surfaces, N (%) | Very often | 250 (89.9) | 28 (10.1) | <0.01 |
| Often | 132 (86.8) | 20 (13.2) | ||
| Sometimes | 19 (51.4) | 18 (48.6) | ||
| Social distancing, N (%) | No/sometimes | 53 (75.7) | 17 (24.3) | 0.01 |
| Yes | 348 (87.7) | 49 (12.3) | ||
| Anxiety, N (%) | Never | 9 (40.9) | 13 (59.1) | <0.01 |
| Sometimes | 118 (76.1) | 37 (23.9) | ||
| Often | 171 (92.4) | 14 (7.6) | ||
| Very often | 103 (98.1) | 2 (1.9) | ||
| Risk of infection, median (IQR) | 36.7 (32.4–45.3) | 38.9 (34.5–45.3) | 0.08 | |
| Risk to get severe disease, median (IQR) | 22.7 (16.5–28.9) | 24.8 (18.6–31.0) | 0.05 | |
| Variable | Factors | Odds Ratio, OR | 95% Confidence Interval, CI | p |
|---|---|---|---|---|
| Education | 1.26 | 0.82; 1.93 | 0.29 | |
| Anxiety | 3.09 | 1.88; 5.09 | <0.01 | |
| Risk of infection | 1.01 | 0.97; 1.06 | 0.63 | |
| Risk of severe disease | 0.99 | 0.96; 1.03 | 0.66 | |
| Factors affecting the motivation to be vaccinated | Fear of COVID-19 | 1.23 | 0.91; 1.68 | 0.18 |
| To protect family | 0.81 | 0.54; 1.20 | 0.29 | |
| Trust in health care | 1.18 | 0.80; 1.75 | 0.41 | |
| Trust in pharmaceutical companies | 1.53 | 1.03; 2.27 | 0.03 | |
| Innovative vaccine | 1.02 | 0.72; 1.45 | 0.89 | |
| Employer recommendation | 1.22 | 0.92; 1.62 | 0.16 | |
| Trust in government | 1.14 | 0.81; 1.62 | 0.45 | |
| Social responsibility | 1.61 | 1.16; 2.22 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syundyukov, E.; Mednis, M.; Zaharenko, L.; Pildegovica, E.; Danovska, I.; Kistkins, S.; Seidmann, A.; Benis, A.; Pirags, V.; Tzivian, L. Data-Driven Decision Making and Proactive Citizen–Scientist Communication: A Cross-Sectional Study on COVID-19 Vaccination Adherence. Vaccines 2021, 9, 1384. https://doi.org/10.3390/vaccines9121384
Syundyukov E, Mednis M, Zaharenko L, Pildegovica E, Danovska I, Kistkins S, Seidmann A, Benis A, Pirags V, Tzivian L. Data-Driven Decision Making and Proactive Citizen–Scientist Communication: A Cross-Sectional Study on COVID-19 Vaccination Adherence. Vaccines. 2021; 9(12):1384. https://doi.org/10.3390/vaccines9121384
Chicago/Turabian StyleSyundyukov, Emil, Martins Mednis, Linda Zaharenko, Eva Pildegovica, Ieva Danovska, Svjatoslavs Kistkins, Abraham Seidmann, Arriel Benis, Valdis Pirags, and Lilian Tzivian. 2021. "Data-Driven Decision Making and Proactive Citizen–Scientist Communication: A Cross-Sectional Study on COVID-19 Vaccination Adherence" Vaccines 9, no. 12: 1384. https://doi.org/10.3390/vaccines9121384
APA StyleSyundyukov, E., Mednis, M., Zaharenko, L., Pildegovica, E., Danovska, I., Kistkins, S., Seidmann, A., Benis, A., Pirags, V., & Tzivian, L. (2021). Data-Driven Decision Making and Proactive Citizen–Scientist Communication: A Cross-Sectional Study on COVID-19 Vaccination Adherence. Vaccines, 9(12), 1384. https://doi.org/10.3390/vaccines9121384