
Trust in Science as a Possible Mediator between Different Antecedents and COVID-19 Booster Vaccination Intention: An Integration of Health Belief Model (HBM) and Theory of Planned Behavior (TPB)

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Literature Background
2.1. Health Behavior Theories
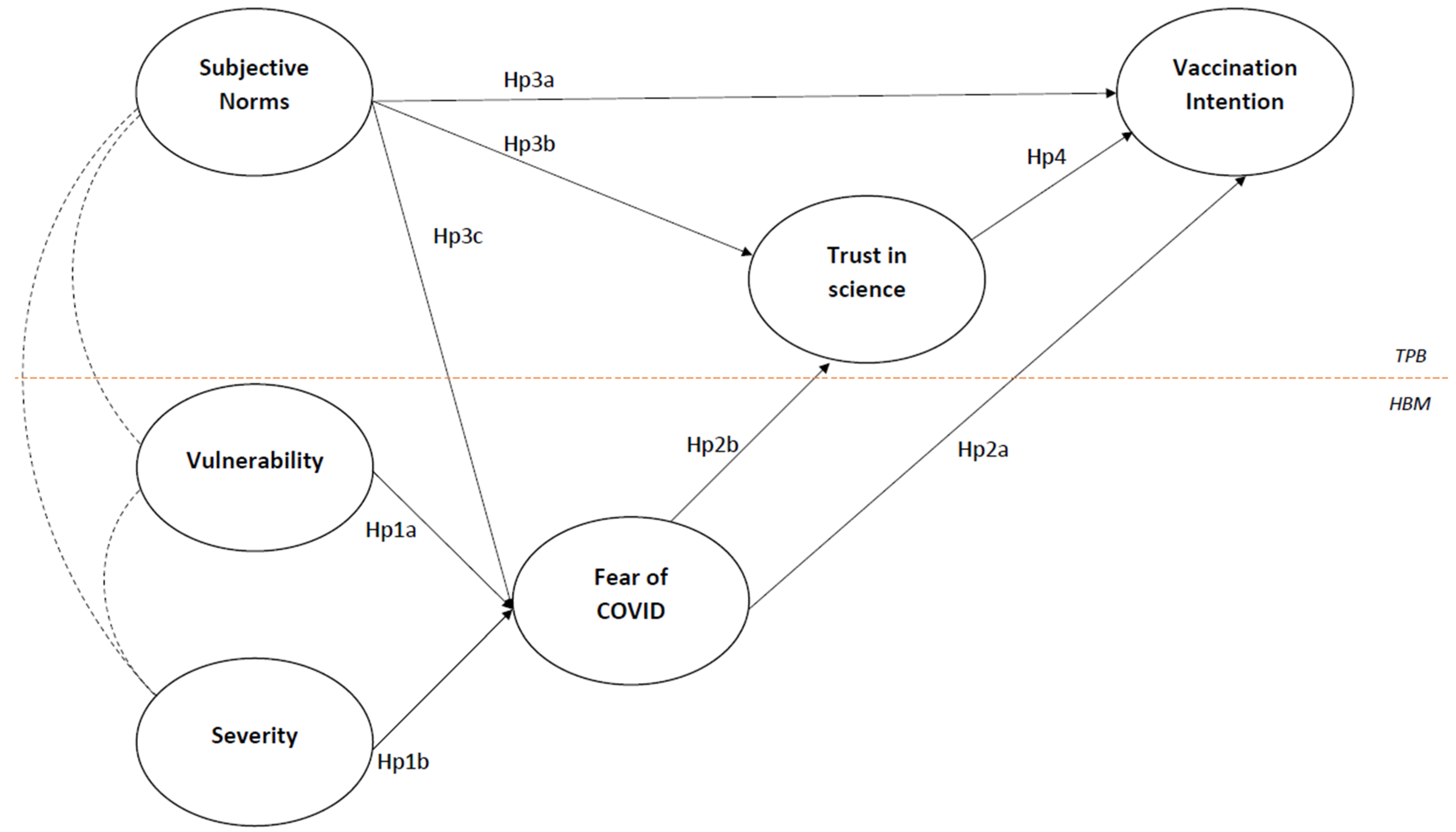
- Hp 1a and Hp 1b: a higher risk perception (higher vulnerability and severity) will be positively related to fear of COVID-19; Hp 2a: a higher fear of COVID-19 will be associated with a lower intention to receive the booster;
- Hp 2b: a higher fear of COVID-19 will be associated with lower Trust in Science.
2.2. Theory of Planned Behavior
- Hp 3a: Subjective norms will be positively related to intention to get the booster;
- Hp 3b: Subjective norms will be positively related to trust in science;
- Hp 4: Trust in science will be positively related to intention to get the booster.
- Hp 3c: Subjective norms will be positively related to fear of COVID-19.
2.3. 5C Model
- Hp 5: Trust mediates the relationship between subjective norms and intention to get vaccinated.
- Hp 6: Trust mediates the relationship between fear of COVID-19 and intention to get vaccinated.
2.4. Socio-Demographic Factors
3. Study Aim
4. Materials and Methods
4.1. Method
4.2. Participants
4.3. Measures
4.4. Data Analysis
5. Results
5.1. Predictors and Clusters for Vaccination Intention
5.2. Measurement Model
5.3. Tested Model
6. Discussion
6.1. Limitations and Future Directions
6.2. Theoretical Implications
6.3. Practical Implications
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hornsey, M.J.; Harris, E.A.; Fielding, K.S. The psychological roots of anti-vaccination attitudes: A 24-nation investigation. Health Psychol. 2018, 37, 307–315. [Google Scholar] [CrossRef] [PubMed]
- De Giorgio, A. COVID-19 is not just a flu. Learn from Italy and act now. Travel Med. Infect. Dis. 2020, 35, 101655. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Du, J.; Du, Z. Government Communication, Perceptions of COVID-19, and Vaccination Intention: A Multi-Group Comparison in China. Front. Psychol. 2022, 12, 783374. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, N.; Costa, D.; Costa, D.; Keating, J.; Arantes, J. Predicting COVID-19 Vaccination Intention: The Determinants of Vaccine Hesitancy. Vaccines 2021, 9, 1161. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, Y. Multilevel determinants of COVID-19 vaccination hesitancy in the United States: A rapid systematic review. Prev. Med. Rep. 2021, 25, 101673. [Google Scholar] [CrossRef]
- Borah, P.; Hwang, J.; Hsu, Y. COVID-19 Vaccination Attitudes and Intention: Message Framing and the Moderating Role of Perceived Vaccine Benefits. J. Health Commun. 2021, 26, 523–533. [Google Scholar] [CrossRef]
- Gerretsen, P.; Kim, J.; Caravaggio, F.; Quilty, L.; Sanches, M.; Wells, S.; Brown, E.E.; Agic, B.; Pollock, B.G.; Graff-Guerrero, A. Individual determinants of COVID-19 vaccine hesitancy. PLoS ONE 2021, 16, e0258462. [Google Scholar] [CrossRef]
- Sombultawee, K.; Boon-itt, S.; Bussanit, V. The Adoption of Protective Health Behaviors During the COVID-19 Pandemic in Thailand. J. Behav. Sci. 2021, 16, 72–83. [Google Scholar]
- Pivetti, M.; Di Battista, S.; Paleari, F.G.; Hakoköngäs, E. Conspiracy beliefs and attitudes toward COVID-19 vaccinations: A conceptual replication study in Finland. J. Pac. Rim Psychol. 2021, 15, 18344909211039893. [Google Scholar] [CrossRef]
- Loomba, S.; De Figueiredo, A.; Piatek, S.J.; De Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef]
- Thaker, J.; Ganchoudhuri, S. The Role of Attitudes, Norms, and Efficacy on Shifting COVID-19 Vaccine Intentions: A Longitudinal Study of COVID-19 Vaccination Intentions in New Zealand. Vaccines 2021, 9, 1132. [Google Scholar] [CrossRef]
- Jin, Q.; Raza, S.H.; Yousaf, M.; Zaman, U.; Siang, J.M.L.D. Can Communication Strategies Combat COVID-19 Vaccine Hesitancy with Trade-Off between Public Service Messages and Public Skepticism? Experimental Evidence from Pakistan. Vaccines 2021, 9, 757. [Google Scholar] [CrossRef]
- Petersen, M.B.; Bor, A.; Jørgensen, F.; Lindholt, M.F. Transparent communication about negative features of COVID-19 vaccines decreases acceptance but increases trust. Proc. Natl. Acad. Sci. USA 2021, 118, e2024597118. [Google Scholar] [CrossRef]
- Wynen, J.; Op de Beeck, S.; Verhoest, K.; Glavina, M.; Six, F.; Van Damme, P.; Beutels, P.; Hendrickx, G.; Pepermans, K. Taking a COVID-19 Vaccine or Not? Do Trust in Government and Trust in Experts Help us to Understand Vaccination Intention? Adm. Soc. 2022, 1–27. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Zheng, H.; Jiang, S.; Wu, Q. Factors influencing COVID-19 vaccination intention: The roles of vaccine knowledge, vaccine risk perception, and doctor-patient communication. Patient Educ. Couns. 2022, 105, 277–283. [Google Scholar] [CrossRef]
- Dubé, E.; Gagnon, D.; Nickels, E.; Jeram, S.; Schuster, M. Mapping vaccine hesitancy—Country-specific characteristics of a global phenomenon. Vaccine 2014, 32, 6649–6654. [Google Scholar] [CrossRef] [Green Version]
- Kwok, K.O.; Li, K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Chu, H.; Liu, S. Integrating health behavior theories to predict American’s intention to receive a COVID-19 vaccine. Patient Educ. Couns. 2021, 104, 1878–1886. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Soveri, A.; Lewandowsky, S.; Karlsson, L.; Karlsson, H.; Nolvi, S.; Karukivi, M.; Lindfelt, M.; Antfolk, J. Fearing the disease or the vaccine: The case of COVID-19. Personal. Individ. Differ. 2021, 172, 110590. [Google Scholar] [CrossRef]
- Machingaidze, S.; Wiysonge, C.S. Understanding COVID-19 vaccine hesitancy. Nat. Med. 2021, 27, 1338–1344. [Google Scholar] [CrossRef]
- Noar, S.M.; Zimmerman, R.S. Health behavior theory and cumulative knowledge regarding health behaviors: Are we moving in the right direction? Health Educ. Res. 2005, 20, 275–290. [Google Scholar] [CrossRef] [Green Version]
- Rosental, H.; Shmueli, L. Integrating Health Behavior Theories to Predict COVID-19 Vaccine Acceptance: Differences between Medical Students and Nursing Students. Vaccines 2021, 9, 783. [Google Scholar] [CrossRef]
- Carpenter, C.J. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [Green Version]
- Zampetakis, L.A.; Melas, C. The health belief model predicts vaccination intentions against COVID-19: A survey experiment approach. Appl. Psychol. Health Well-Being 2021, 13, 469–484. [Google Scholar] [CrossRef]
- Bosnjak, M.; Ajzen, I.; Schmidt, P. The Theory of Planned Behavior: Selected Recent Advances and Applications. Eur. J. Psychol. 2020, 16, 352–356. [Google Scholar] [CrossRef]
- Wolff, K. COVID-19 Vaccination Intentions: The Theory of Planned Behavior, Optimistic Bias, and Anticipated Regret. Front. Psychol. 2021, 12, 648289. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The theory of planned behavior: Frequently asked questions. Hum. Behav. Emerg. Technol. 2020, 2, 314–324. [Google Scholar] [CrossRef]
- Hossain, M.B.; Alam, M.Z.; Islam, M.S.; Sultan, S.; Faysal, M.M.; Rima, S.; Hossain, M.A.; Mamun, A.A. Health Belief Model, Theory of Planned Behavior, or Psychological Antecedents: What Predicts COVID-19 Vaccine Hesitancy Better Among the Bangladeshi Adults? Front. Public Health 2021, 9, 711066. [Google Scholar] [CrossRef]
- Patwary, M.M.; Bardhan, M.; Disha, A.S.; Hasan, M.; Haque, Z.; Sultana, R.; Hossain, R.; Browning, M.H.E.M.; Alam, A.; Sallam, M. Determinants of COVID-19 Vaccine Acceptance among the Adult Population of Bangladesh Using the Health Belief Model and the Theory of Planned Behavior Model. Vaccines 2021, 9, 1393. [Google Scholar] [CrossRef] [PubMed]
- An, P.L.; Nguyen, H.; Dang, H.; Huynh, Q.; Pham, B.; Huynh, G. Integrating Health Behavior Theories to Predict Intention to Get a COVID-19 Vaccine. Health Serv. Insights 2021, 14, 11786329211060130. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I.M. Health Belief Model. In Encyclopedia of Psychology; Kazdin, A.E., Ed.; American Psychological Association: New York, NY, USA, 2000; Volume 4, pp. 78–80. [Google Scholar]
- Campion, V.L.; Skinner, C.S. The Health Belief Model. In Health Behavior & Health Education, 4th ed.; Kasprzyk, D., Ed.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 45–64. [Google Scholar]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Haque, A.; Pant, A.B. Mitigating COVID-19 in the face of emerging virus variants, breakthrough infections and vaccine hesitancy. J. Autoimmun. 2022, 127, 102792. [Google Scholar] [CrossRef]
- Lai, X.; Zhu, H.; Wang, J.; Huang, Y.; Jing, R.; Lyu, Y.; Zhang, H.; Feng, H.; Guo, J.; Fang, H. Public Perceptions and Acceptance of COVID-19 Booster Vaccination in China: A Cross-Sectional Study. Vaccines 2021, 9, 1461. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; Van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Mahmud, I.; Kabir, R.; Rahman, M.A.; Alradie-Mohamed, A.; Vinnakota, D.; Al-Mohaimeed, A. The Health Belief Model Predicts Intention to Receive the COVID-19 Vaccine in Saudi Arabia: Results from a Cross-Sectional Survey. Vaccines 2021, 9, 864. [Google Scholar] [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 37, 1080–1086. [Google Scholar] [CrossRef]
- Suess, C.; Maddock, J.E.; Dogru, T.; Mody, M.; Lee, S. Using the Health Belief Model to examine travelers’ willingness to vaccinate and support for vaccination requirements prior to travel. Tour Manag. 2022, 88, 104405. [Google Scholar] [CrossRef]
- Maraqa, B.; Nazzal, Z.; Rabi, R.; Sarhan, N.; Al-Shakhra, K. COVID-19 vaccine hesitancy among health care workers in Palestine: A call for action. Prev. Med. 2021, 149, 106618. [Google Scholar] [CrossRef]
- Chen, H.; Li, X.; Gao, J.; Liu, X.; Mao, Y.; Wang, R.; Zheng, P.; Xiao, Q.; Jia, Y.; Fu, H.; et al. Health Belief Model Perspective on the Control of COVID-19 Vaccine Hesitancy and the Promotion of Vaccination in China: Web-Based Cross-sectional Study. J. Med. Internet Res. 2021, 23, e29329. [Google Scholar] [CrossRef]
- Coco, M.; Guerrera, C.S.; Santisi, G.; Riggio, F.; Grass, R.; Di Corrado, D.; Di Nuovo, S.; Ramaci, T. Psychosocial Impact and Role of Resilience on Healthcare Workers during COVID-19 Pandemic. Sustainability 2021, 13, 7096. [Google Scholar] [CrossRef]
- Scrima, F.; Miceli, S.; Caci, B.; Cardaci, M. The relationship between fear of COVID-19 and intention to get vaccinated. The serial mediation roles of existential anxiety and conspiracy beliefs. Pers. Individ. Differ. 2022, 184, 111188. [Google Scholar] [CrossRef]
- Birhanu, Z.; Ambelu, A.; Fufa, D.; Mecha, M.; Zeynudin, A.; Abafita, J.; Belay, A.; Doyore, F.; Oljira, L.; Bacha, E.; et al. Risk perceptions and attitudinal responses to COVID-19 pandemic: An online survey in Ethiopia. BMC Public Health 2021, 21, 981. [Google Scholar] [CrossRef]
- Clavel, N.; Badr, J.; Gautier, L.; Lavoie-Tremblay, M.; Paquette, J. Risk Perceptions, Knowledge and Behaviors of General and High-Risk Adult Populations Towards COVID-19: A Systematic Scoping Review. Public Health Rev. 2021, 42, 1603979. [Google Scholar] [CrossRef]
- González-Castro, J.L.; Ubillos-Landa, S.; Puente-Martínez, A.; Gracia-Leiva, M. Perceived Vulnerability and Severity Predict Adherence to COVID-19 Protection Measures: The Mediating Role of Instrumental Coping. Front. Psychol. 2021, 12, 674032. [Google Scholar] [CrossRef]
- Hilverda, F.; Vollmann, M. The Role of Risk Perception in Students’ COVID-19 Vaccine Uptake: A Longitudinal Study. Vaccines 2022, 10, 22. [Google Scholar] [CrossRef]
- Wake, A.D. The Willingness to Receive COVID-19 Vaccine and Its Associated Factors: “Vaccination Refusal Could Prolong the War of This Pandemic”—A Systematic Review. Risk Manag. Healthc. Policy 2021, 14, 2609–2623. [Google Scholar] [CrossRef]
- Sekizawa, Y.; Hashimoto, S.; Denda, K.; Ochi, S.; So, M. Association between COVID-19 vaccine hesitancy and generalized trust, depression, generalized anxiety, and fear of COVID-19. BMC Public Health 2022, 22, 126. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Xiao, X.; Wong, R.M. Vaccine hesitancy and perceived behavioral control: A meta-analysis. Vaccine 2020, 38, 5131–5138. [Google Scholar] [CrossRef]
- La Barbera, F.; Ajzen, I. Control Interactions in the Theory of Planned Behavior: Rethinking the Role of Subjective Norm. Eur. J. Psychol. 2020, 16, 401–417. [Google Scholar] [CrossRef]
- Wolff, K.; Nordin, K.; Brun, W.; Berglund, G.; Kvale, G. Affective and cognitive attitudes, uncertainty avoidance and intention to obtain genetic testing: An extension of the theory of planned Behaviour. Psychol. Health 2011, 26, 1143–1155. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, V. A/H1N1 vaccine intentions in college students: An application of the theory of planned behavior. J. Am. Coll. Health 2014, 6, 416–424. [Google Scholar] [CrossRef]
- Catalano, P.H.; Richards, K.; Hawkins, H.K. Theory of planned behavior-based correlates of HPV vaccination intentions and series completion among University Students in the Southeastern United States. Health Educ. 2017, 49, 35–44. [Google Scholar] [CrossRef]
- Gagnon, M.; Godin, G. Young Adults and HIV Vaccine: Determinants of the Intention of Getting Immunized. Can. J. Public Health 2000, 91, 432–434. [Google Scholar] [CrossRef]
- Fan, Y.V.; Jiang, P.; Hemzal, M.; Klemeš, J.J. An update of COVID-19 influence on waste management. Sci. Total Environ. 2021, 275, 142014. [Google Scholar] [CrossRef]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2020, 17, 1612–1621. [Google Scholar] [CrossRef]
- Yahaghi, R.; Ahmadizade, S.; Fotuhi, R.; Taherkhani, E.; Ranjbaran, M.; Buchali, Z.; Jafari, R.; Zamani, N.; Shahbazkhania, A.; Simiari, H.; et al. Fear of COVID-19 and Perceived COVID-19 Infectability Supplement Theory of Planned Behavior to Explain Iranians’ Intention to Get COVID-19 Vaccinated. Vaccines 2021, 9, 684. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, K.; Van Dongen, A.; Hagger, M. An extended theory of planned behavior for parent-for-child health behaviors: A metaanalysis. Health Psychol. 2020, 39, 863–878. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.Q.; Zhou, X.; Wang, Z. Parental Acceptability of COVID-19 Vaccination for Children under the Age of 18 Years: Cross-Sectional Online Survey. JMIR Pediatr. Parent. 2020, 3, e24827. Available online: https://preprints.jmir.org/preprint/24827 (accessed on 21 April 2021). [CrossRef] [PubMed]
- Sniehotta, F.F.; Presseau, J.; Ara jo-Soares, V. Time to retire the theory of planned behaviour. Health Psychol. 2014, 8, 1–7. [Google Scholar] [CrossRef]
- Winter, K.; Pummerer, L.; Hornsey, M.J.; Sassenberg, K. Pro-vaccination subjective norms moderate the relationship between conspiracy mentality and vaccination intentions. Br. J. Health Psychol. 2022, 27, 390–405. [Google Scholar] [CrossRef]
- Husain, F.; Shahnawaz, M.G.; Khan, N.H.; Parveen, H.; Savani, K. Intention to get COVID-19 vaccines: Exploring the role of attitudes, subjective norms, perceived behavioral control, belief in COVID-19 misinformation, and vaccine confidence in Northern India. Hum. Vaccines Immunother. 2021, 17, 3941–3953. [Google Scholar] [CrossRef]
- Rad, R.E.; Kahnouji, K.; Mohseni, S.; Shahabi, N.; Noruziyan, F.; Farshidi, H.; Hosseinpoor, M.; Kashani, S.; Takhti, H.K.; Azad, M.H.; et al. Predicting the COVID-19 vaccine receive intention based on the theory of reasoned action in the south of Iran. BMC Public Health 2022, 22, 229. [Google Scholar] [CrossRef]
- Visser, O.; Hulscher, M.E.; Antonise-Kamp, L.; Akkermans, R.; Van der Velden, K.; Ruiter, R.A.; Hautvast, J.L. Assessing determinants of the intention to accept a pertussis cocooning vaccination: A survey among healthcare workers in maternity and paediatric care. Vaccine 2018, 36, 736–743. [Google Scholar] [CrossRef]
- Xiao, X.; Borah, P. Do norms matter? Examining norm-based messages in HPV vaccination promotion. Health Commun. 2020, 36, 1476–1484. [Google Scholar] [CrossRef]
- Shmueli, L. The Role of Incentives in Deciding to Receive the Available COVID-19 Vaccine in Israel. Vaccines 2022, 10, 77. [Google Scholar] [CrossRef]
- Brambilla, M.; Sacchi, S.; Rusconi, P.; Goodwin, G. The primacy of morality in impression development: Theory, research, and future directions. Adv. Exp. Soc. Psychol. 2021, 64, 187–262. [Google Scholar] [CrossRef]
- Chu, A.; Gupta, V.; Unni, E.J. Utilizing the Theory of Planned Behavior to determine the intentions to receive the influenza vaccine during COVID-19: A cross-sectional survey of US adults. Prev. Med. Rep. 2021, 23, 101417. [Google Scholar] [CrossRef]
- Lewandowsky, S.; Gignac, G.E.; Oberauer, K. The role of conspiracist ideation and worldviews in predicting rejection of science. PLoS ONE 2013, 8, e75637. [Google Scholar] [CrossRef] [Green Version]
- Baumgaertner, B.; Carlisle, J.E.; Justwan, F. The influence of political ideology and trust on willingness to vaccinate. PLoS ONE 2018, 13, e0191728. [Google Scholar] [CrossRef] [Green Version]
- Pagliaro, S.; Sacchi, S.; Pacilli, M.G.; Brambilla, M.; Lionetti, F.; Bettache, K.; Bianchi, M.; Biella, M.; Bonnot, V.; Boza, M.; et al. Trust predicts COVID-19 prescribed and discretionary behavioral intentions in 23 countries. PLoS ONE 2021, 16, e0248334. [Google Scholar] [CrossRef]
- Ramaci, T.; Pagliaro, S.; Teresi, M.; Barattucci, M. Job Demands and Negative Outcomes after the Lockdown: The Moderating Role of Stigma towards Italian Supermarket Workers. Sustainability 2021, 13, 7507. [Google Scholar] [CrossRef]
- Sturgis, P.; Brunton-Smith, I.; Jackson, J. Trust in science, social consensus and vaccine confidence. Nat. Hum. Behav. 2021, 5, 1528–1534. [Google Scholar] [CrossRef]
- Kerr, J.R.; Schneider, C.R.; Recchia, G.; Dryhurst, S.; Sahlin, U.; Dufouil, C.; Arwidson, P.; Freeman, A.L.; Van der Linden, S. Correlates of intended COVID-19 vaccine acceptance across time and countries: Results from a series of cross-sectional surveys. BMJ Open 2021, 11, e048025. [Google Scholar] [CrossRef]
- Bronfman, N.; Repetto, P.; Cisternas, P.; Castañeda, J.; Cordón, P. Government Trust and Motivational Factors on Health Protective Behaviors to Prevent COVID-19 Among Young Adults. Int. J. Public Health 2022, 67, 1604290. [Google Scholar] [CrossRef]
- Barattucci, M.; Chirico, A.; Kuvačić, G.; De Giorgio, A. Rethinking the Role of Affect in Risk Judgment: What We Have Learned from COVID-19 During the First Week of Quarantine in Italy. Front. Psychol. 2020, 11, 554561. [Google Scholar] [CrossRef]
- Liu, M.; Chen, Y.; Shi, D.; Yan, T. The Public’s Risk Information Seeking and Avoidance in China During Early Stages of the COVID-19 Outbreak. Front. Psychol. 2021, 12, 649180. [Google Scholar] [CrossRef]
- Godbersen, H.; Hofmann, L.A.; Ruiz-Fernández, S. How People Evaluate Anti-Corona Measures for Their Social Spheres: Attitude, Subjective Norm, and Perceived Behavioral Control. Front. Psychol. 2020, 11, 567405. [Google Scholar] [CrossRef]
- Brewer, N.T.; Hall, M.E.; Malo, T.L.; Gilkey, M.B.; Quinn, B.; Lathren, C. Announcements versus conversations to improve HPV vaccination coverage: A randomized trial. Pediatrics 2017, 139, e20161764. [Google Scholar] [CrossRef] [Green Version]
- Mohamed Ghazy, R.; Abd ElHafeez, S.; Shaaban, R.; Elbarazi, I.; Shawky Abdou, M.; Ramadan, A.; Kheirallah, K.A. Determining the Cutoff Points of the 5C Scale for Assessment of COVID-19Vaccines Psychological Antecedents among the Arab Population: A Multinational Study. J. Prim. Care Community Health 2021, 12, 21501327211018568. [Google Scholar] [CrossRef]
- Jaffe, A.E.; Graupensperger, S.; Blayney, J.A.; Duckworth, J.C.; Stappenbeck, C.A. The Role of Perceived Social Norms in College Student Vaccine Hesitancy: Implications for COVID-19 Prevention Strategies. Vaccine 2022, 40, 1888–1895. [Google Scholar] [CrossRef]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Ransing, R.; Kukreti, P.; Raghuveer, P.; Puri, M.; Paranjape, A.D.; Patil, S.; Hegde, P.; Padma, K.; Kumar, P.; Kishore, J.; et al. A brief psycho-social intervention for COVID-19 vaccine hesitancy among perinatal women in low-and middle-income countries: Need of the hour. Asian J. Psychiatry 2022, 67, 102929. [Google Scholar] [CrossRef]
- Thomson, A.; Robinson, K.; Vallée-Tourangeau, G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
- Plohl, N.; Musil, B. Modeling compliance with COVID-19 prevention guidelines: The critical role of trust in science. Psychol. Health Med. 2021, 26, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Akther, T.; Nur, T. A model of factors influencing COVID.19 vaccine acceptance: A synthesis of the theory of reasoned action, conspiracy theory belief, awareness, perceived usefulness, and perceived ease of use. PLoS ONE 2022, 17, e0261869. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, M.; Ichino, A.; Bonomi, A.; Martoni, R.; Cammino, S.; Gorini, A. Who Is Willing to Get Vaccinated? A Study into the Psychological, Socio-Demographic, and Cultural Determinants of COVID-19 Vaccination Intentions. Vaccines 2021, 9, 810. [Google Scholar] [CrossRef] [PubMed]
- Bucchi, M.; Fattorini, E.; Saracino, B. Public Perception of COVID-19 Vaccination in Italy: The Role of Trust and Experts’ Communication. Int. J. Public Health 2022, 67, 1604222. [Google Scholar] [CrossRef]
- De Giorgio, A.; Kuvacic, G.; Maleš, D.; Vecchio, I.; Tornali, C.; Ishac, W.; Ramaci, T.; Barattucci, M.; Milavi’c, B. Willingness to Receive COVID-19 Booster Vaccine: Associations between Green-Pass, Social Media Information, Anti-Vax Beliefs, and Emotional Balance. Vaccines 2022, 10, 481. [Google Scholar] [CrossRef]
- Flanagan, P.; Dowling, M.; Gethin, G. Barriers and Facilitators to Seasonal Influenza Vaccination Uptake among Nurses: A Mixed Methods Study. J. Adv. Nurs. 2020, 76, 1746–1764. Available online: https://publons.com/publon/10.1111/jan.14360 (accessed on 11 March 2021). [CrossRef]
- Ramaci, T.; Barattucci, M.; Ledda, C.; Rapisarda, V. Social Stigma during COVID-19and its Impact on HCWs Outcomes. Sustainability 2020, 12, 3834. [Google Scholar] [CrossRef]
- Zhang, J.; While, A.E.; Norman, I.J. Nurses’ Vaccination against Pandemic H1N1 Influenza and Their Knowledge and Other Factors. Vaccine 2012, 30, 4813–4819. [Google Scholar] [CrossRef]
- Nan, X. Communicating to young adults about HPV vaccination: Consideration of message framing, motivation, and gender. Health Commun. 2012, 27, 10–18. [Google Scholar] [CrossRef]
- Chapman, G.B.; Coups, E.J. Predictors of influenza vaccine acceptance among healthy adults. Prev. Med. 1999, 29, 249–262. [Google Scholar] [CrossRef]
- Kumar, S.; Quinn, S.C.; Kim, K.H.; Musa, D.; Hilyard, K.M.; Freimuth, V.S. The social ecological model as a framework for determinants of 2009 H1N1 influenza vaccine uptake in the United States. Health Educ. Behav. 2012, 39, 229–243. [Google Scholar] [CrossRef] [Green Version]
- Machida, M.; Nakamura, I.; Kojima, T.; Saito, R.; Nakaya, T.; Hanibuchi, T.; Takamiya, T.; Odagiri, Y.; Fukushima, N.; Kikuchi, H.; et al. Trends in COVID-19 vaccination intent from pre- to post-COVID-19 vaccine distribution and their associations with the 5C psychological antecedents of vaccination by sex and age in Japan. Hum. Vaccines Immunother. 2021, 17, 3954–3962. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Rhodes, A.; Hoq, M.; Measey, M.-A.; Danchin, M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020, 21, e110. [Google Scholar] [CrossRef]
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine hesitancy: Causes, consequences, and a call to action. Am. J. Prev. Med. 2015, 49 (Suppl. S4), S391–S398. [Google Scholar] [CrossRef]
- Breslin, G.; Dempster, M.; Berry, E.; Cavanagh, M.; Nicola, C.; Armstrong, N.C. COVID-19 vaccine uptake and hesitancy survey in Northern Ireland and Republic of Ireland: Applying the theory of planned behaviour. PLoS ONE 2021, 16, e0259381. [Google Scholar] [CrossRef]
- Cafagna, D.; Barattucci, M. Risk perception and personality: A study in the transportation sector. G. Ital. Med. Lav. Ergon. 2019, 41, 211–220. [Google Scholar]
- Savadori, L.; Rumiati, R.; Bonini, N.; Pedon, A. Percezione del rischio: Esperti vs non esperti. Arch. Psicol. Neurol. Psichiatr. 1998, 59, 387–405. [Google Scholar]
- Keller, C.; Bostrom, A.; Kuttschreuter, M.; Savadori, L.; Spence, A.; White, M. Bringing appraisal theory to environmental risk perception: A review of conceptual approaches of the past 40 years and suggestions for future research. J. Risk Res. 2012, 15, 237–256. [Google Scholar] [CrossRef]
- Fishbein, M.; Ajzen, I. Predicting and Changing Behavior: The Reasoned Action Approach; Psychology Press: New York, NY, USA, 2010. [Google Scholar]
- Istituto Superiore di Sanità. Relazione dell’Istituto Superiore di Sanità sui Risultati Dell’attività Svolta nel 2011; Istituto Superiore di Sanità: Roma, Italy, 2012. [Google Scholar]
- Tamburrano, A.; Mellucci, C.; Galletti, C.; Vitale, D.; Vallone, D.; Barbara, A.; Sguera, A.; Zega, M.; Damiani, G.; Laurenti, P. Improving Nursing Staff Attitudes toward Vaccinations through Academic Detailing: The HProImmune Questionnaire as a Tool for Medical Management. Int. J. Environ. Res. Public Health 2019, 16, 2006. [Google Scholar] [CrossRef] [Green Version]
- Slovic, P.; Finucane, M.L.; Peters, E.; MacGregor, D.G. Risk as analysis and risk as feelings: Some thoughts about affect, reason, risk, and rationality. Risk Anal. 2004, 24, 311–322. [Google Scholar] [CrossRef]
- Brown, V.J. Risk perception: It’s personal. Environ. Health Perspect. 2014, 122, A276–A279. [Google Scholar] [CrossRef] [Green Version]
- Slovic, P.E. The Perception of Risk; Earthscan Publications: London, UK, 2000. [Google Scholar]
- Podsakoff, P.; MacKenzie, S.B.; Lee, J.-Y.; Podsakoff, N.P. Common Method Biases in Behavioral Research: A Critical Review of the Literature and Recommended Remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Richardson, H.M.; Simmering, M.J.; Sturman, M. A Tale of Three Perspectives. Organ. Res. Methods 2009, 12, 762–800. [Google Scholar] [CrossRef]
- AlShurman, B.A.; Khan, A.F.; Mac, C.; Majeed, M.; Butt, Z.A. What Demographic, Social, and Contextual Factors Influence the Intention to Use COVID-19 Vaccines: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 9342. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef]
- Patwary, M.M.; Alam, M.A.; Bardhan, M.; Disha, A.S.; Haque, M.Z.; Billah, S.M.; Kabir, M.P.; Browning, M.; Rahman, M.M.; Parsa, A.D.; et al. COVID-19 Vaccine Acceptance among Low- and Lower-Middle-Income Countries: A Rapid Systematic Review and Meta-Analysis. Vaccines 2022, 10, 427. [Google Scholar] [CrossRef]
- Corace, K.M.; Srigley, J.A.; Hargadon, D.P.; Yu, D.; MacDonald, T.K.; Fabrigar, L.R.; Garber, G.E. Using Behavior Change Frameworks to Improve Healthcare Worker Influenza Vaccination Rates: A Systematic Review. Vaccine 2016, 34, 3235–3242. [Google Scholar] [CrossRef] [Green Version]
- Hopman, C.E.; Riphagen-Dalhuisen, J.; Looijmans-van den Akker, I.; Frijstein, G.; Van der Geest-Blankert, A.D.J.; Danhof-Pont, M.B.; De Jager, H.J.; Bos, A.A.; Smeets, E.; De Vries, M.J.T.; et al. Determination of Factors Required to Increase Uptake of Influenza Vaccination among Hospital-Based Healthcare Workers. J. Hosp. Infect. 2011, 77, 327–331. [Google Scholar] [CrossRef]
- Folcarelli, L.; Miraglia del Giudice, G.; Corea, F.; Angelillo, I.F. Intention to Receive the COVID-19 Vaccine Booster Dose in a University Community in Italy. Vaccines 2022, 10, 146. [Google Scholar] [CrossRef] [PubMed]
- Santirocchi, A.; Spataro, P.; Costanzi, M.; Doricchi, F.; Rossi-Arnaud, C.; Cestari, V. Predictors of the Intention to Be Vaccinated against COVID-19 in a Sample of Italian Respondents at the Start of the Immunization Campaign. J. Pers. Med. 2022, 12, 111. [Google Scholar] [CrossRef] [PubMed]
- French, J.; Deshpande, S.; Evans, W.; Obregon, R. Key guidelines in developing a pre-emptive COVID-19 vaccination uptake promotion strategy. Int. J. Environ. Res. 2020, 17, 5893. [Google Scholar] [CrossRef] [PubMed]
- Simione, L.; Vagni, M.; Gnagnarella, C.; Bersani, G.; Pajardi, D. Mistrust and Beliefs in Conspiracy Theories Differently Mediate the Effects of Psychological Factors on Propensity for COVID-19 Vaccine. Front. Psychol. 2021, 12, 683684. [Google Scholar] [CrossRef] [PubMed]
- Bliese, P.D.; Edwards, J.R.; Sonnentag, S. Stress and well-being at work: A century of empirical trends reflecting theoretical and societal influences. J. Appl. Psychol. 2017, 102, 389–402. [Google Scholar] [CrossRef]
- Morgeson, F.P.; Mitchell, T.R.; Liu, D. Event System Theory: An Event-Oriented Approach to the Organizational Sciences. Acad. Manag. Rev. 2015, 40, 515–537. [Google Scholar] [CrossRef] [Green Version]
- Egede, L.E.; Ellis, C. Development and testing of the multidimensional trust in health care systems scale. Gen. Intern. Med. 2008, 23, 808–815. [Google Scholar] [CrossRef] [Green Version]
- Griva, K.; Tan, K.; Chan, F.; Periakaruppan, R.; Ong, B.; Soh, A.; Chen, M.I. Evaluating Rates and Determinants of COVID-19 Vaccine Hesitancy for Adults and Children in the Singapore Population: Strengthening Our Community’s Resilience against Threats from Emerging Infections (SOCRATEs) Cohort. Vaccines 2021, 9, 1415. [Google Scholar] [CrossRef]
- Maftei, A.; Holman, A.C. SARS-CoV-2 Threat Perception and Willingness to Vaccinate: The Mediating Role of Conspiracy Beliefs. Front. Psychol. 2021, 12, 672634. [Google Scholar] [CrossRef]
- Bruder, M.; Haffke, P.; Neave, N.; Nouripanah, N.; Imhoff, R. Measuring individual differences in generic beliefs in conspiracy theories across cultures: Conspiracy Mentality Questionnaire. Front. Psychol. 2013, 4, 225. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Guo, Y.; Zhou, Q.; Tan, Z.; Cao, J. The Mediating Roles of Medical Mistrust, Knowledge, Confidence and Complacency of Vaccines in the Pathways from Conspiracy Beliefs to Vaccine Hesitancy. Vaccines 2021, 9, 1342. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| M (SD) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Vulnerability | 4.44 (1.5) | - | ||||||||
| 2. Severity | 4.65 (1.4) | 0.250 *** | - | |||||||
| 3. Fear of COVID-19 | 5.52 (1.4) | 0.290 *** | 0.522 *** | - | ||||||
| 4. Fear of vaccine | 3.06 (1.9) | –0.059 | –0.121 ** | –0.183 ** | - | |||||
| 5. COVID-19 knowledge | 4.70 (1.3) | 0.059 | 0.093 ** | 0.096 ** | 0.039 | - | ||||
| 6. Subjective norm | 5.58 (1.7) | 0.170 ** | 0.276 *** | –0.340 *** | –0.268 *** | 0.041 | - | |||
| 7. Trust in science | 5.72 (1.4) | 0.137 ** | 0.275 *** | 0.369 *** | –0.585 *** | –0.006 | 0.407 *** | - | ||
| 8. Trust in vaccine | 5.52 (1.4) | 0.116 ** | 0.331 *** | 0.368 *** | –0.719 *** | –0.017 | 0.389 *** | 0.763 *** | - | |
| 9. Intention to vaccine | 5.86 (1.9) | 0.119 ** | 0.206 ** | 0.271 *** | –0.482*** | 0.092 ** | 0.322 *** | 0.585 *** | 0.638 *** | - |
| Chi-Square | df | RMSEA | CFI | IFI | SRMR | |
|---|---|---|---|---|---|---|
| Model 1: one factor | 3510.733 | 170 | 0.134 | 0.751 | 0.742 | 0.110 |
| Model 2: three factors | 3464.783 | 167 | 0.123 | 0.756 | 0.793 | 0.096 |
| Model 3: six factors | 3155.012 | 164 | 0.109 | 0.830 | 0.809 | 0.089 |
| Model 4: nine factors | 2250.771 | 161 | 0.083 | 0.921 | 0.909 | 0.078 |
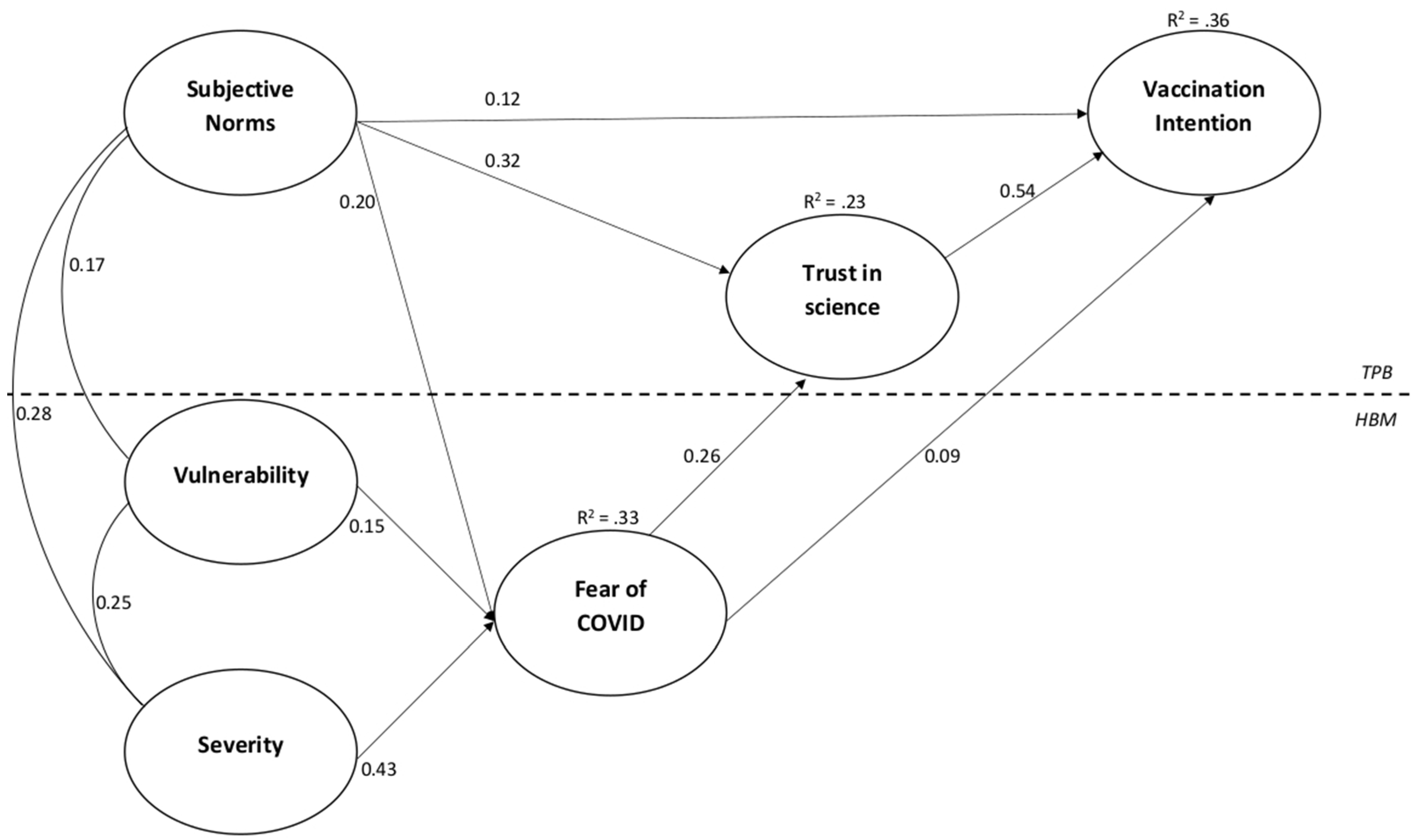
| Direct Effects | |
|---|---|
| Vulnerability → fear of COVID-19 | 0.149 |
| Severity → fear of COVID-19 | 0.430 |
| Subjective norm → fear of COVID-19 | 0.197 |
| Subjective norm → trust | 0.319 |
| Subjective norm → vaccination intention | 0.120 |
| Fear of COVID-19 → trust | 0.260 |
| Fear of COVID-19 → vaccination intention | 0.086 |
| Trust → vaccination intention | 0.541 |
| Indirect Effects via Trust | |
| Fear of COVID-19 → vaccination intention | 0.140 |
| Subjective norm → vaccination intention | 0.217 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barattucci, M.; Pagliaro, S.; Ballone, C.; Teresi, M.; Consoli, C.; Garofalo, A.; De Giorgio, A.; Ramaci, T. Trust in Science as a Possible Mediator between Different Antecedents and COVID-19 Booster Vaccination Intention: An Integration of Health Belief Model (HBM) and Theory of Planned Behavior (TPB). Vaccines 2022, 10, 1099. https://doi.org/10.3390/vaccines10071099
Barattucci M, Pagliaro S, Ballone C, Teresi M, Consoli C, Garofalo A, De Giorgio A, Ramaci T. Trust in Science as a Possible Mediator between Different Antecedents and COVID-19 Booster Vaccination Intention: An Integration of Health Belief Model (HBM) and Theory of Planned Behavior (TPB). Vaccines. 2022; 10(7):1099. https://doi.org/10.3390/vaccines10071099
Chicago/Turabian StyleBarattucci, Massimiliano, Stefano Pagliaro, Chiara Ballone, Manuel Teresi, Carlo Consoli, Alice Garofalo, Andrea De Giorgio, and Tiziana Ramaci. 2022. "Trust in Science as a Possible Mediator between Different Antecedents and COVID-19 Booster Vaccination Intention: An Integration of Health Belief Model (HBM) and Theory of Planned Behavior (TPB)" Vaccines 10, no. 7: 1099. https://doi.org/10.3390/vaccines10071099
APA StyleBarattucci, M., Pagliaro, S., Ballone, C., Teresi, M., Consoli, C., Garofalo, A., De Giorgio, A., & Ramaci, T. (2022). Trust in Science as a Possible Mediator between Different Antecedents and COVID-19 Booster Vaccination Intention: An Integration of Health Belief Model (HBM) and Theory of Planned Behavior (TPB). Vaccines, 10(7), 1099. https://doi.org/10.3390/vaccines10071099