
A Multilingual App for Providing Information to SARS-CoV-2 Vaccination Candidates with Limited Language Proficiency: Development and Pilot


Abstract
:1. Introduction
Objectives
2. Materials and Methods
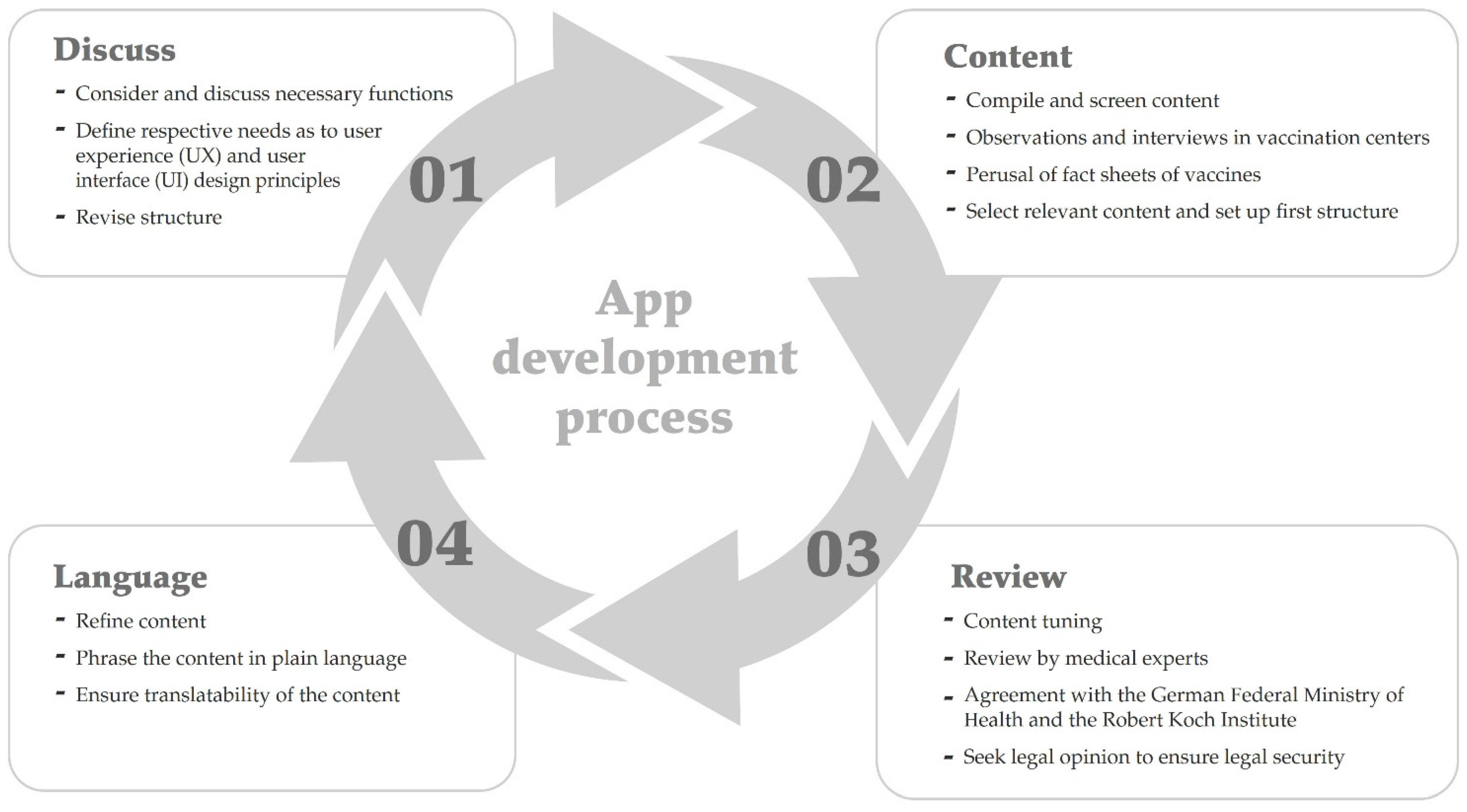
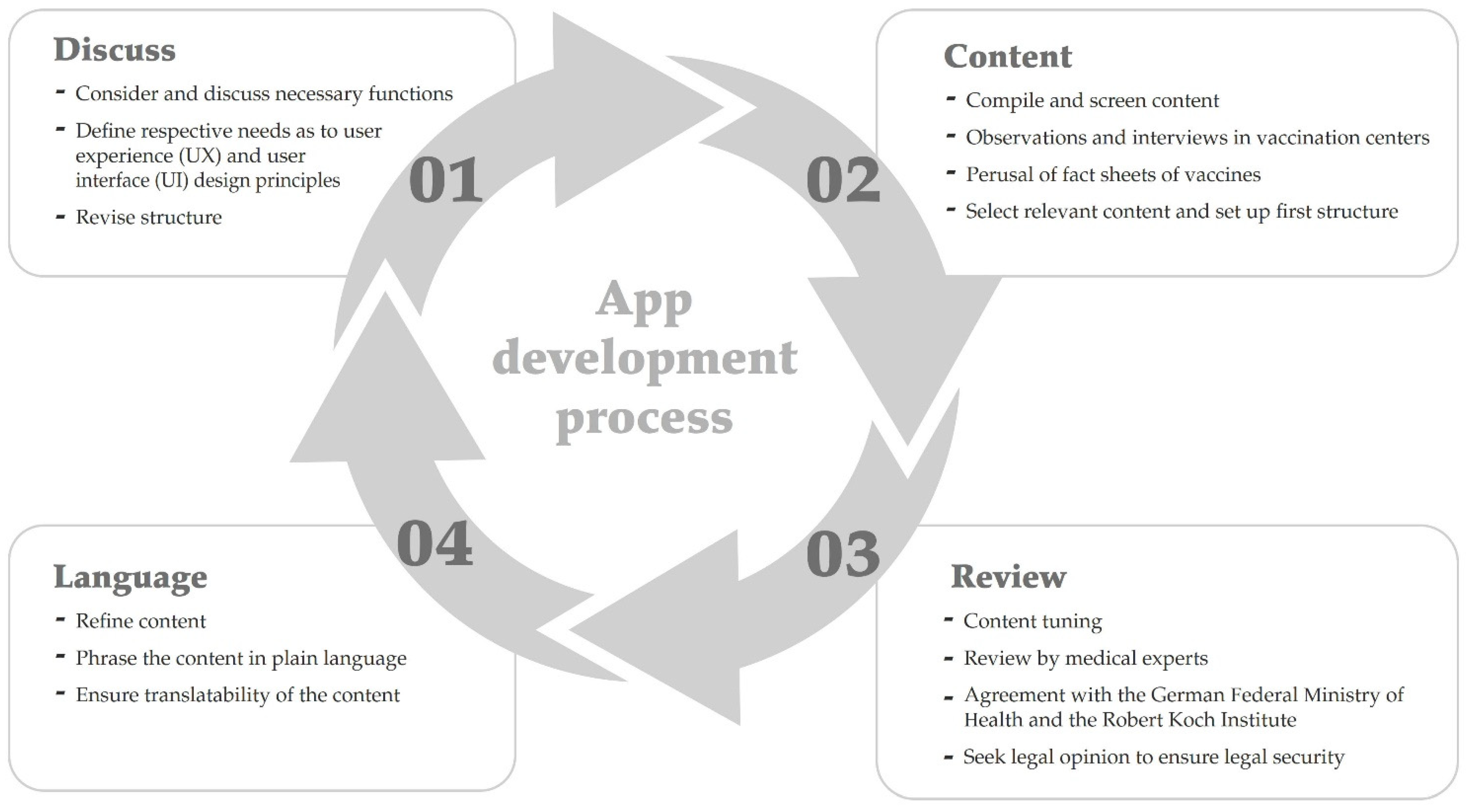
2.1. Framework of the Development Process: The STAR Steps
2.2. Pilot Test
3. Results
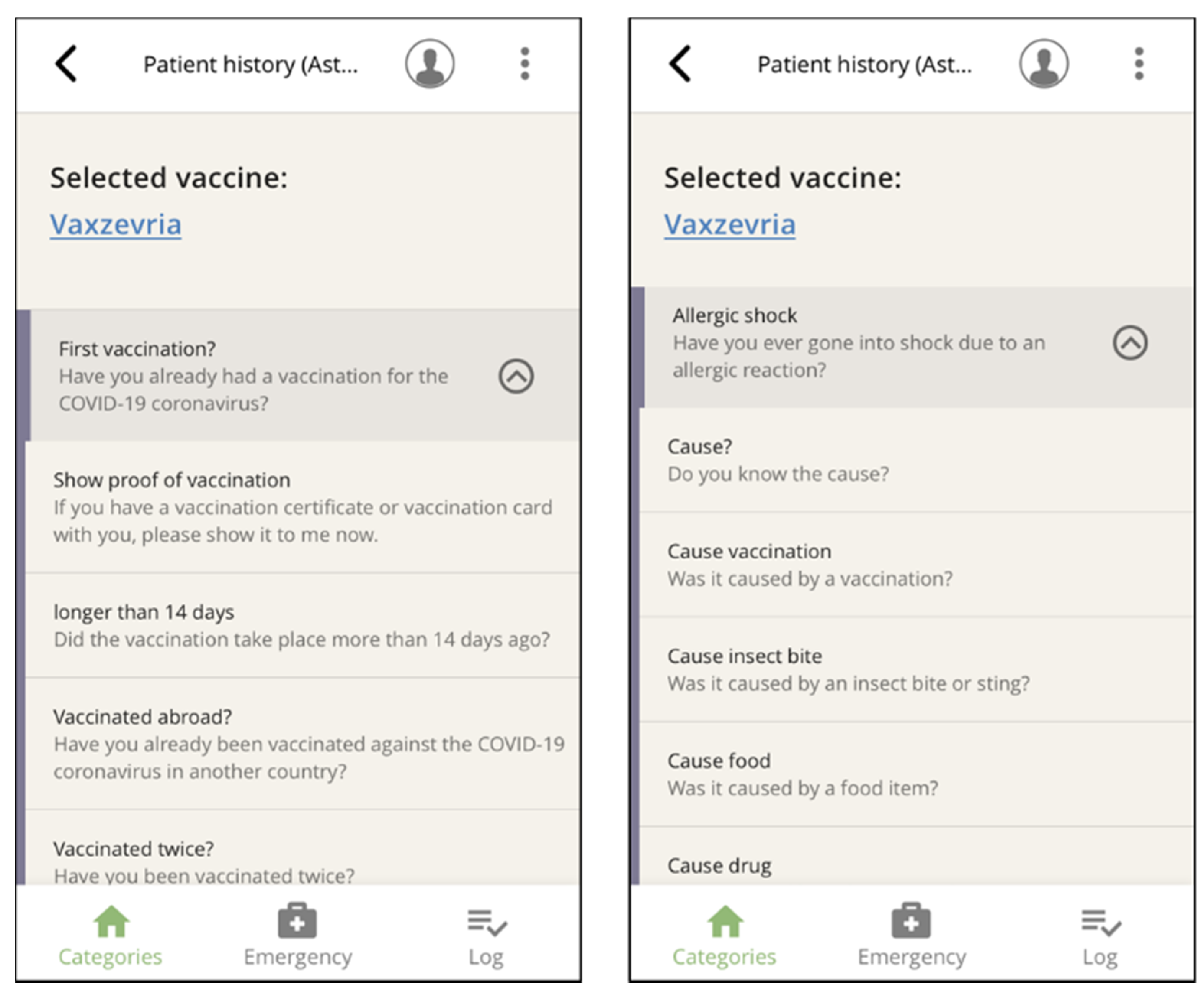
3.1. Content and Structure
3.2. Languages, Functions, and Navigation
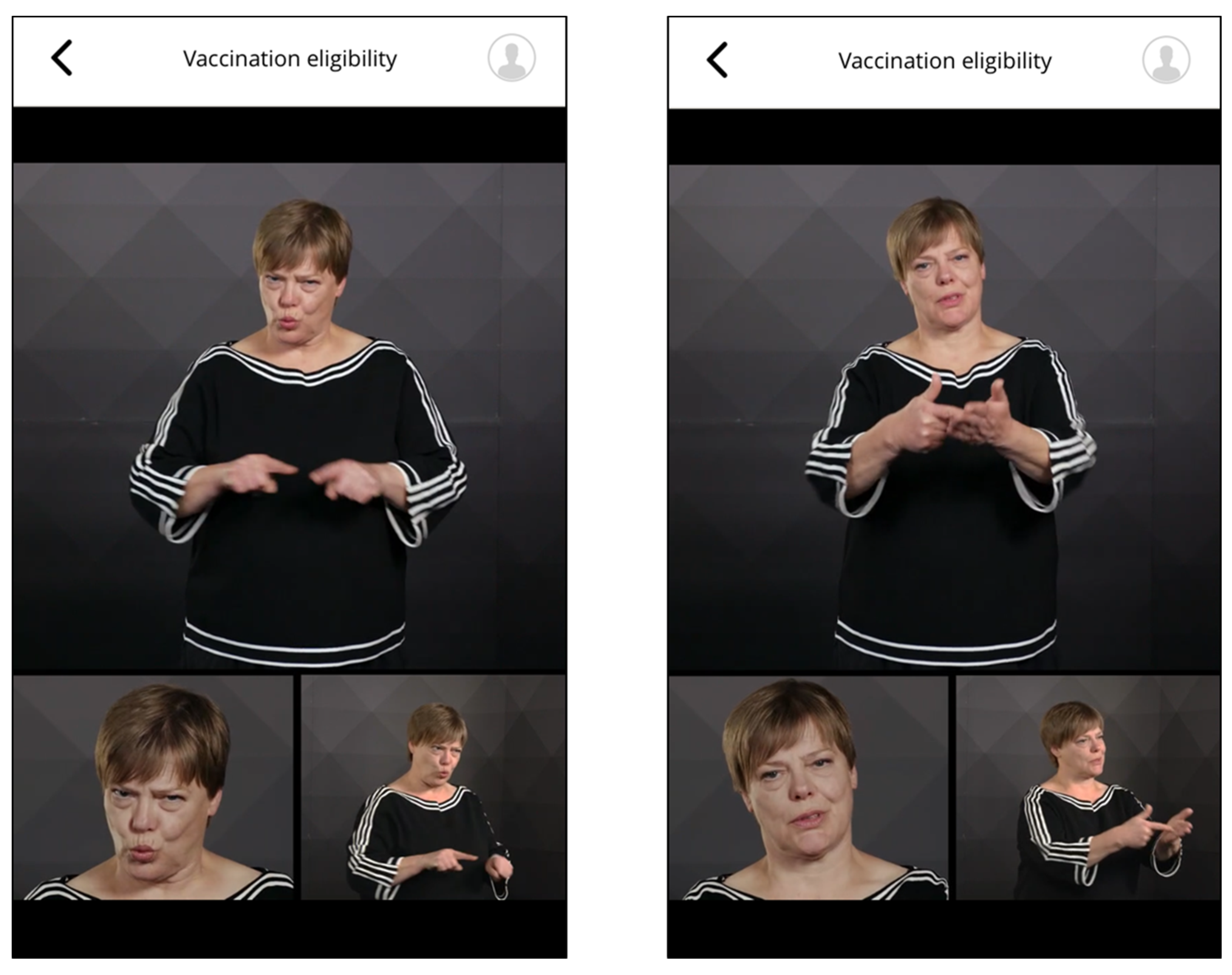
3.2.1. Supported Languages
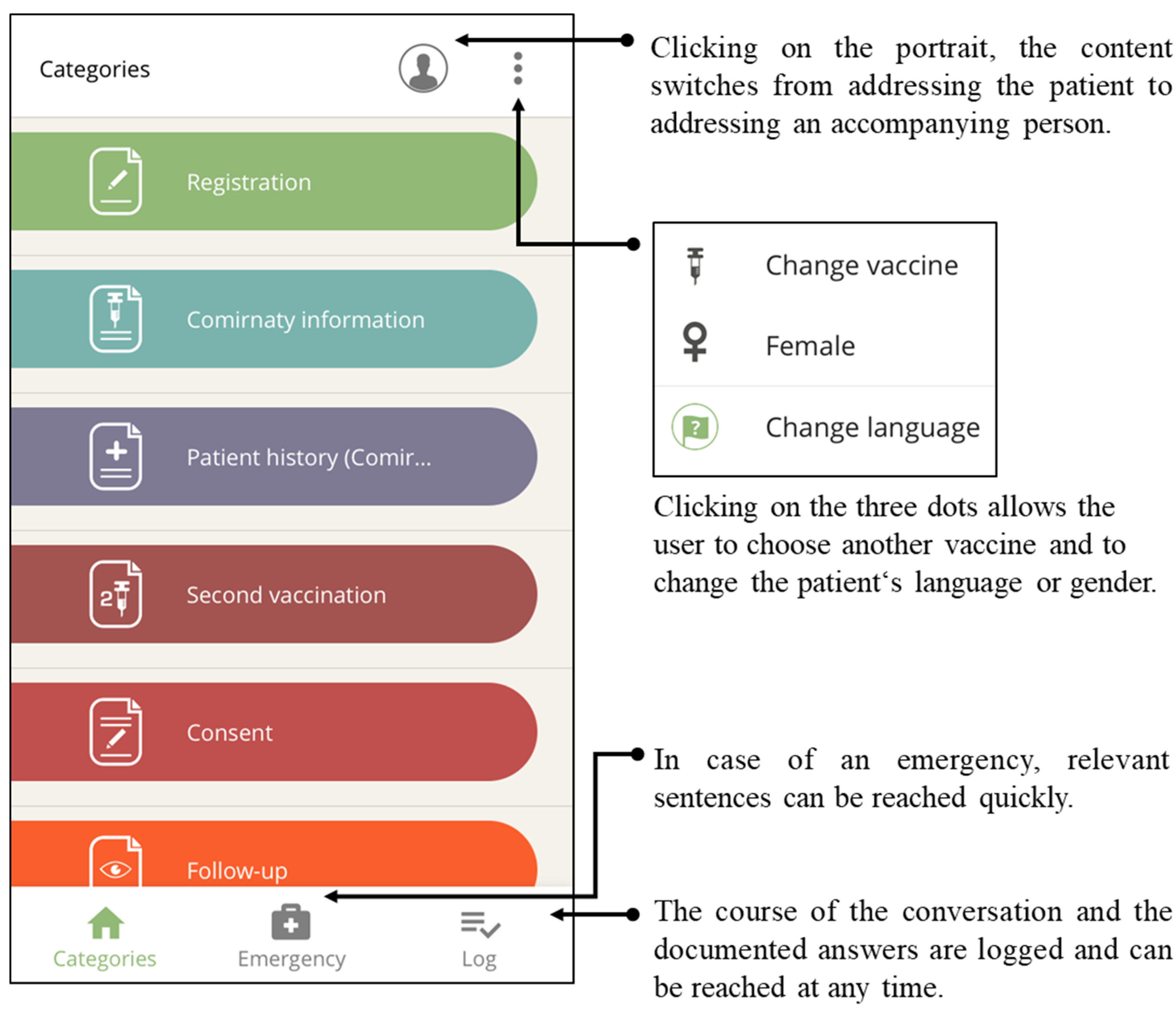
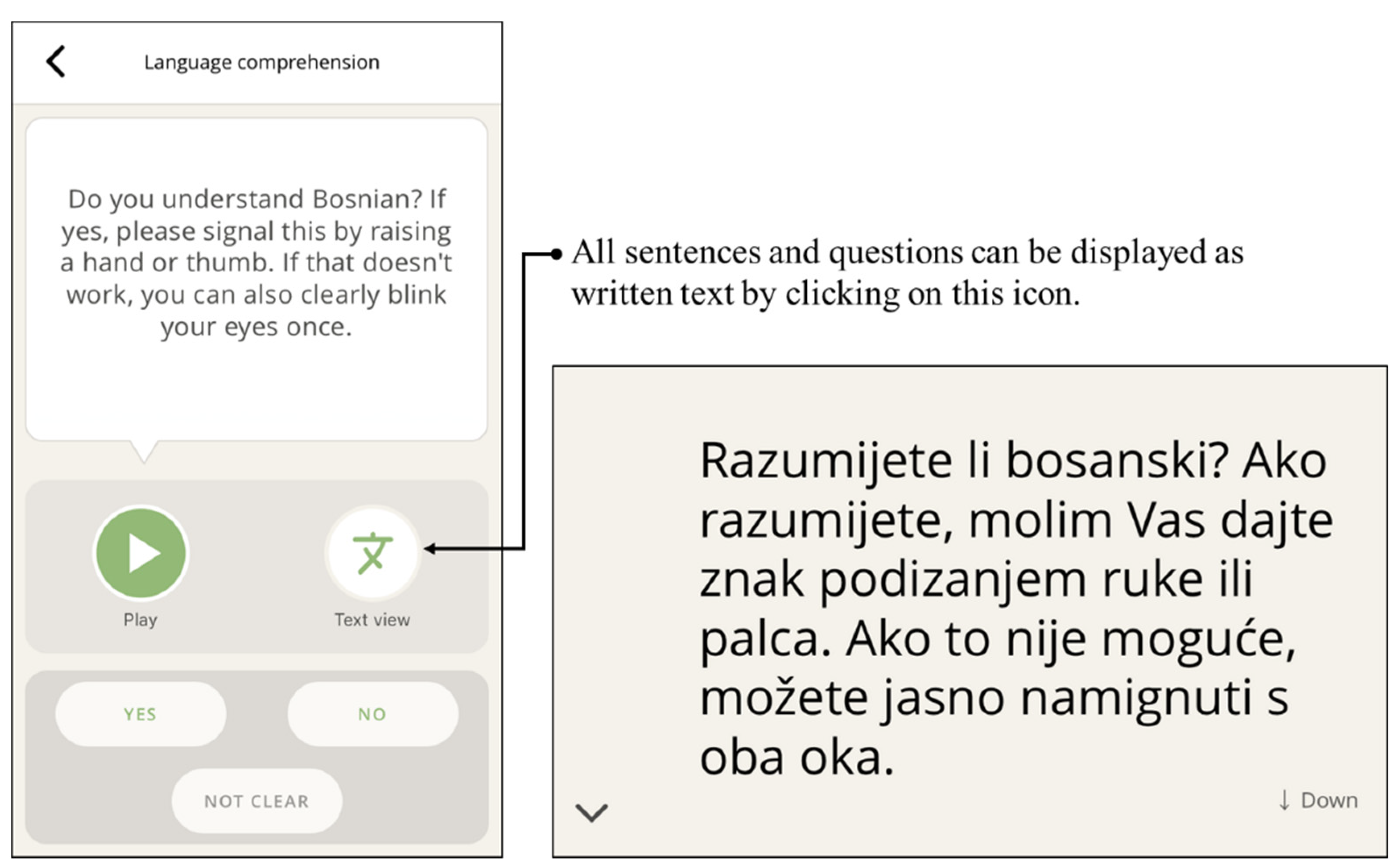
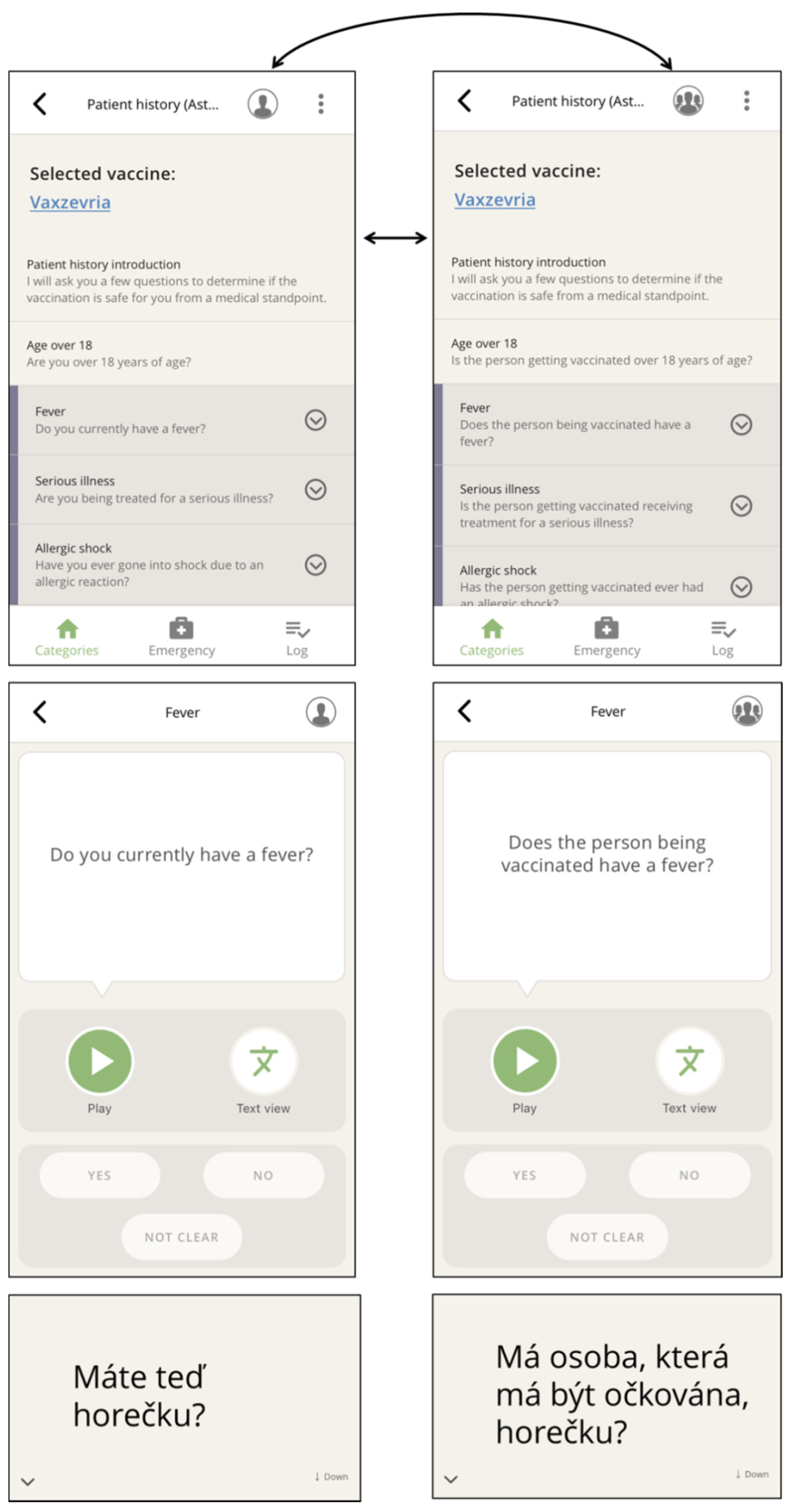
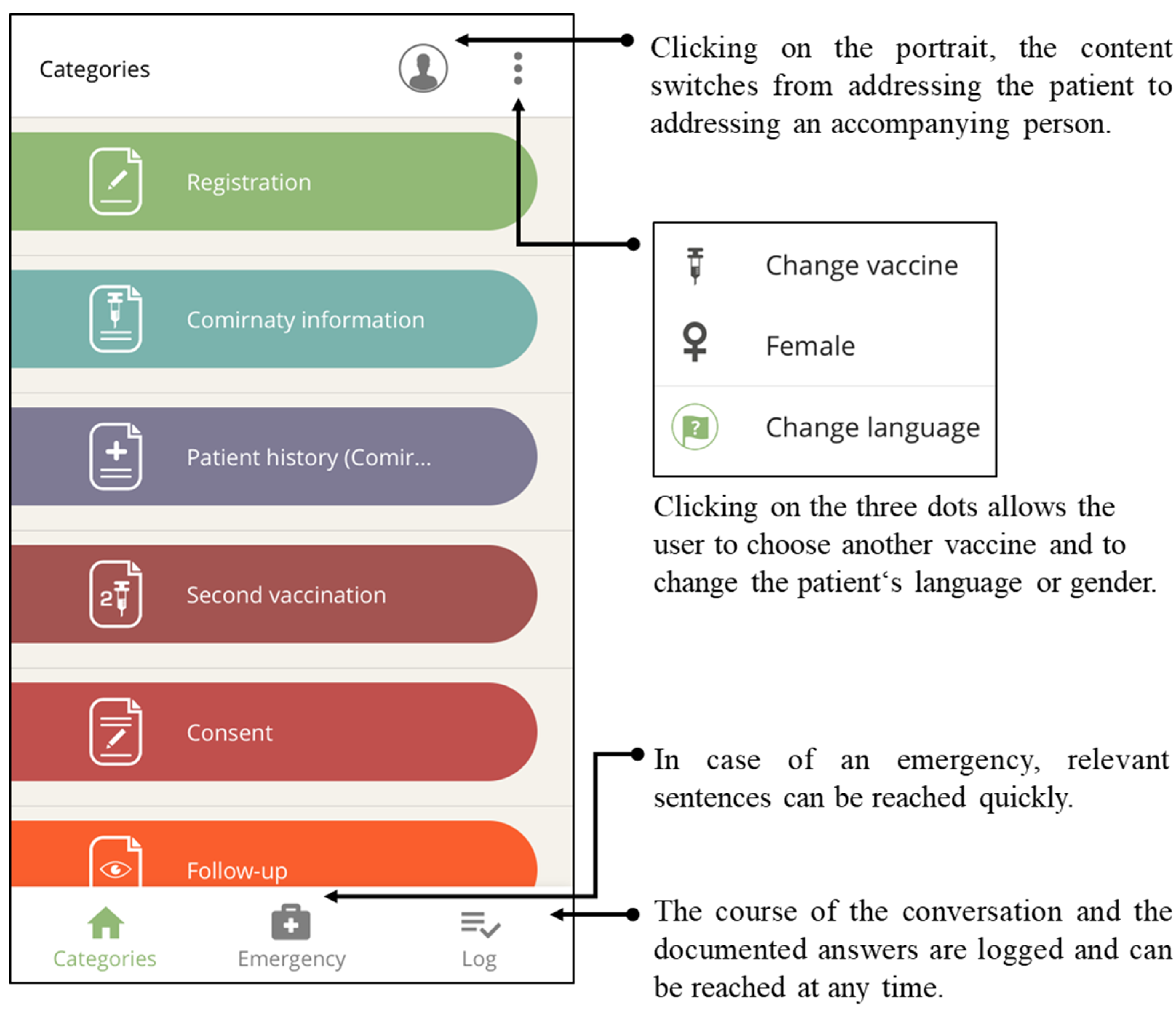
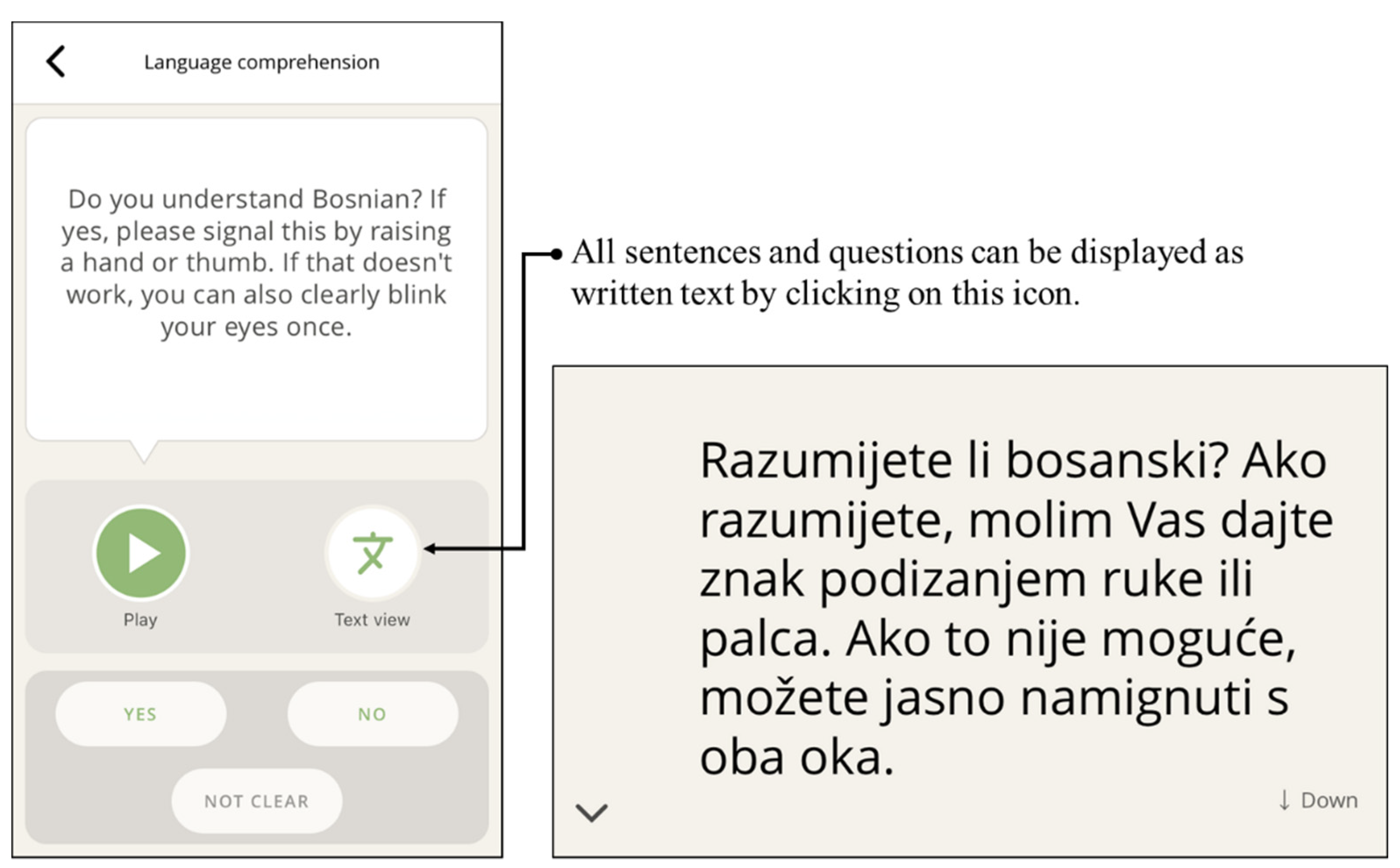
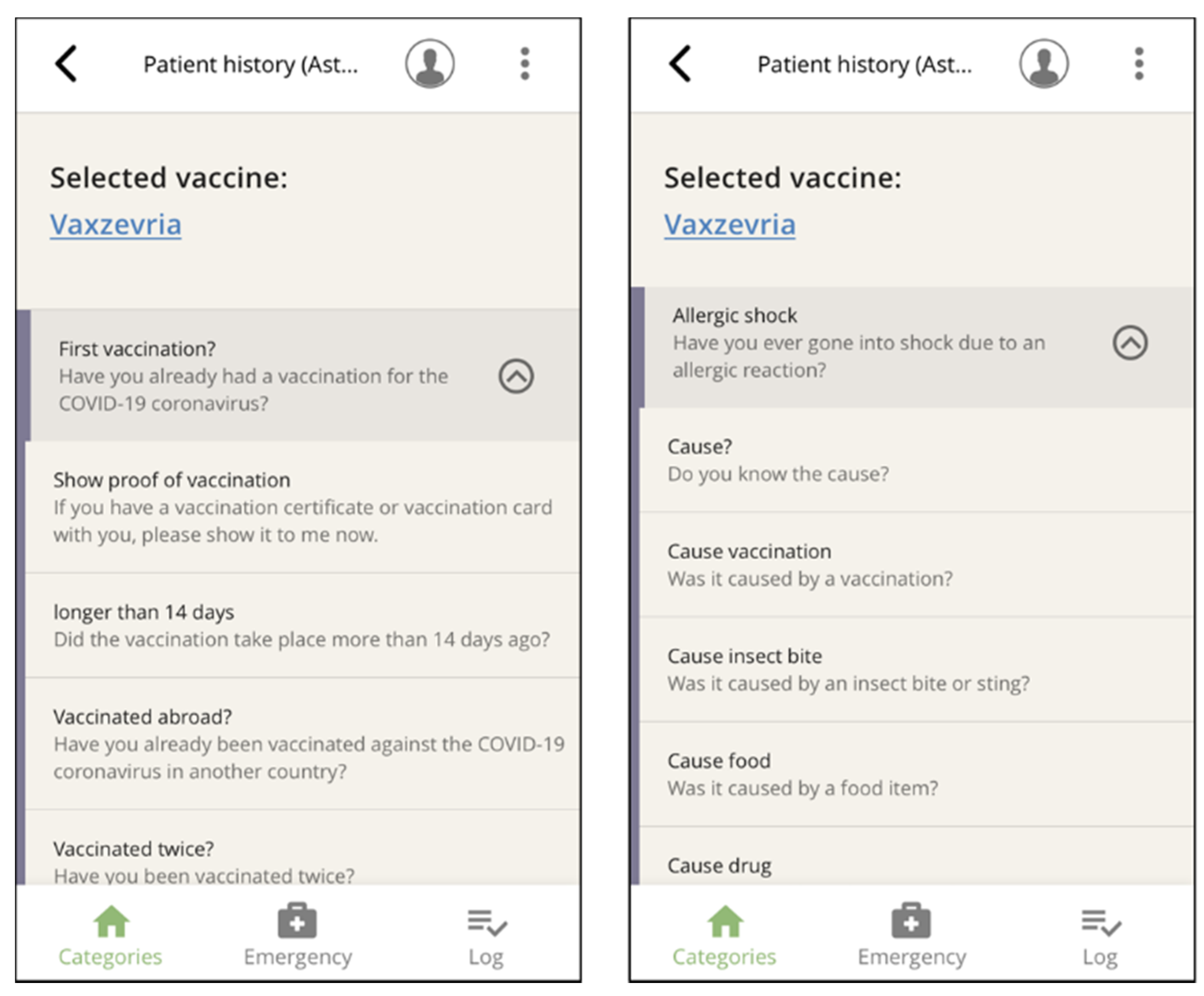
3.2.2. Functions and Navigation Features
3.3. Pilot Test
4. Discussion
4.1. Discussion of the Results
4.2. Limitations and Strengths
4.3. Outlook
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Observed Category | Phrases Used | n (%) | Mean (SD) |
|---|---|---|---|
| Registration process | Spoken | 2 (10) | |
| Played | 1.5 (0.7) | ||
| Quality of communication | 1 (0) | ||
| Informed consent talk | Spoken | 20 (100) | |
| Played | 4.6 (5.0) | ||
| Risks and side effects | 15 (75) | ||
| Information on COVID-19 | 3 (15) | ||
| Protective efficacy of vaccination | 6 (30) | ||
| Process of vaccination admission (e.g., need for 2nd vaccination) | 5 (25) | ||
| After vaccination | 6 (30) | ||
| If vaccination candidate has more questions | 10 (50) | ||
| Quality of communication | 1.2 (0.4) | ||
| Medical history taking | Spoken | 15 (75) | |
| Played phrases | 5.1 (3.3) | ||
| Fever | 11 (55) | ||
| Pre-existing conditions | 9 (45) | ||
| Allergies and history of allergic shock | 12 (60) | ||
| Problems with previous immunizations | 6 (30) | ||
| Drug therapy (e.g., anticoagulation) | 8 (40) | ||
| Quality of communication | 1.1 (0.4) | ||
| Obtaining consent | Spoken | 15 (75) | |
| Mean played phrases | 1.3 (0.6) | ||
| Asked for consent to vaccinate | 8 (40) | ||
| Asked if vaccination candidate has additional questions or concerns | 5 (25) | ||
| Vaccination candidate refused vaccination | 0 (0) | ||
| Quality of communication | 1.13 (0.4) | ||
| Additional phrases | Communication in a medical emergency | 0 (0) | |
| History of breast cancer or thrombosis | 0 (0) | ||
| Handedness and side preference of the vaccinated arm | 16 (80) | ||
| Further instructions | 2 (10) | ||
| Global assessment | General compliance of vaccination candidate | 1.2 (0.4) | |
| General compliance of vaccination candidate with app | 1.4 (0.5) | ||
| Vaccination candidate’s German language proficiency | 3.8 (1.3) |
| Detailed Category | Content |
|---|---|
| Missing phrases | Inform the vaccination candidate that he/she should stay in the waiting area for 15 min or 30 min for follow-up. |
| Provision of information for follow-up appointments or location on the second vaccination | |
| It was not possible to give appropriate information to vaccination candidates who had already had a COVID-19 infection. This mainly concerns information on a positive coronavirus PCR test, the vaccination intervals after infection, and whether they would receive one or two vaccinations. | |
| Information about how vaccine candidates could get a digital vaccination certificate, what it meant, and where to get it. | |
| In the information about the vaccines, it is mentioned that you can take fever-reducing and painkilling medication. However, it was also desired to make a recommendation about what these could be (paracetamol and ibuprofen). | |
| Vaccine candidates could not be told where polyethylene glycol could be found as an additional ingredient in other food or drug sources. It was also not possible to ask vaccination candidates about general allergies. | |
| There was a lack of information on cases of myocarditis that occurred after vaccination with an mRNA vaccine. | |
| Usability | It occurred that the explanation on how to use the app could not be played at the beginning of the informed consent talk. |
| The question about pregnancy was not playable in Vietnamese. | |
| It was noticeable that the navigation was very confusing due to fold-out filter questions. | |
| The question about the handedness of the vaccination candidates is listed, but it is so hidden that the doctors could not find it without support. | |
| It is not clear how the recording and printing of the log will be implemented in actual vaccination practice. | |
| Communication problems | There were difficulties in determining whether people understand the German language or not. Therefore, the app was used even though the person understood at least some German. |
| In Romanian, there were communication difficulties with the question about handedness (mimicking expression of the vaccination candidate indicated that he did not understand the question). | |
| The question was asked whether the person would prefer to be vaccinated lying down or sitting up. However, this question cannot be answered with yes or no. | |
| Communication and acceptance of the app by HCPs | Some HCPs were not familiar with the app, they tended to perceive it as a burden rather than a time saver. |
| Because some phrases were missing or not up to date, some HCPs did not fully trust the app. | |
| Communication and acceptance of the app by vaccine candidates | One accompanying daughter gave feedback that the app helped ease her mother’s fear of vaccination. |
| Not up-to-date contents | In some cases, the app gave the wrong information that there was no need to take special care after vaccination. Indeed, the vaccination candidate should refrain from physical exertion after vaccination with an mRNA vaccine. |
| Extra tools | One HCP usually used a Bluetooth box for giving information to the vaccination candidates. |
| Other particulars | Although the vaccine candidate understood English very well, “with his consent, the app was used in Azerbaijani.” |
| The vaccinating doctor decided against using the app during the interview because she preferred to use her own language resources. However, these were not sufficient. |
References
- Bermejo, I.; Hölzel, L.P.; Kriston, L.; Härter, M. Subjektiv erlebte Barrieren von Personen mit Migrationshintergrund bei der Inanspruchnahme von Gesundheitsmaßnahmen. Bundesgesundheitsblatt Gesundh. Gesundh. 2012, 55, 944–953. [Google Scholar] [CrossRef] [PubMed]
- Green, M. Language Barriers and Health of Syrian Refugees in Germany. Am. J. Public Health 2017, 107, 486. [Google Scholar] [CrossRef] [PubMed]
- Brand, T.; Kleer, D.; Samkange-Zeeb, F.; Zeeb, H. Prävention bei Menschen mit Migrationshintergrund: Teilnahme, migrationssensible Strategien und Angebotscharakteristika. Bundesgesundheitsblatt Gesundh. Gesundh. 2015, 58, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.; Knesebeck, O. von dem. Inequalities in health care utilization among migrants and non-migrants in Germany: A systematic review. Int. J. Equity Health 2018, 17, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayward, S.E.; Deal, A.; Cheng, C.; Crawshaw, A.F.; Orcutt, M.; Vandrevala, T.F.; Norredam, M.; Carballo, M.; Ciftci, Y.; Requena-Mendez, A.; et al. Clinical outcomes and risk factors for COVID-19 among migrant populations in high-income countries: A systematic review. J. Migr. Health 2020, 3, 10041. [Google Scholar] [CrossRef] [PubMed]
- Hintermeier, M.; Gencer, H.; Kajikhina, K.; Rohleder, S.; Santos-Hövener, C.; Tallarek, M.; Spallek, J.; Bozorgmehr, K. SARS-CoV-2 among migrants and forcibly displaced populations: A rapid systematic review. J. Migr. Health 2020, 4, 100056. [Google Scholar] [CrossRef] [PubMed]
- Knights, F.; Carter, J.; Deal, A.; Crawshaw, A.F.; Hayward, S.E.; Jones, L.; Hargreaves, S. Impact of COVID-19 on migrants’ access to primary care and implications for vaccine roll-out: A national qualitative study. Br. J. Gen. Pract. 2021, 71, e583–e595. [Google Scholar] [CrossRef] [PubMed]
- Green, M.S.; Abdullah, R.; Vered, S.; Nitzan, D. A study of ethnic, gender and educational differences in attitudes toward COVID-19 vaccines in Israel-implications for vaccination implementation policies. Isr. J. Health Policy Res. 2021, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Jones, A.; Lesser, I.; Daly, M. International estimates of intended uptake and refusal of COVID-19 vaccines: A rapid systematic review and meta-analysis of large nationally representative samples. Vaccine 2021, 39, 2024–2034. [Google Scholar] [CrossRef] [PubMed]
- Deal, A.; Hayward, S.E.; Huda, M.; Knights, F.; Crawshaw, A.F.; Carter, J.; Hassan, O.B.; Farah, Y.; Ciftci, Y.; Rowland-Pomp, M.; et al. Strategies and action points to ensure equitable uptake of COVID-19 vaccinations: A national qualitative interview study to explore the views of undocumented migrants, asylum seekers, and refugees. J. Migr. Health 2021, 4, 100050. [Google Scholar] [CrossRef] [PubMed]
- Razai, M.S.; Kankam, H.K.N.; Majeed, A.; Esmail, A.; Williams, D.R. Mitigating ethnic disparities in covid-19 and beyond. BMJ 2021, 372, m4921. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch-Institut. Epidemiologisches Bulletin 34/2021. Available online: https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2021/Ausgaben/34_21.pdf?__blob=publicationFile (accessed on 1 November 2021).
- Skinner, H.A.; Maley, O.; Norman, C.D. Developing internet-based eHealth promotion programs: The Spiral Technology Action Research (STAR) model. Health Promot. Pract. 2006, 7, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Langley, G.; Nolan, K.; Nolan, T.; Norman, G.; Provest, L. The Improvement Guide: A Practical Approach to Enhance Organizational Performance; Jossey-Bass: San Francisco, CA, USA, 1996. [Google Scholar]
- Skinner, H.A. Promoting Health through Organizational Change; Benjamin Cummings: San Francisco, CA, USA, 2002. [Google Scholar]
- Noack, E.M.; Schulze, J.; Müller, F. Designing an App to Overcome Language Barriers in the Delivery of Emergency Medical Services: Participatory Development Process. JMIR Mhealth Uhealth 2021, 9, e21586. [Google Scholar] [CrossRef] [PubMed]
- Müller, F.; Hummers, E.; Schulze, J.; Noack, E.M. Nutz- und Bedienbarkeit einer App zur Überwindung von Sprachbarrieren im Rettungsdienst. Notfall Rett. 2021. [Google Scholar] [CrossRef] [PubMed]
- AstraZeneca. COVID-19 Vaccine AstraZeneca: Product Information as Approved by the CHMP on 29 January 2021. 2020. Available online: https://www.ema.europa.eu/en/documents/product-information/covid-19-vaccine-astrazeneca-product-information-approved-chmp-29-january-2021-pending-endorsement_en.pdf (accessed on 23 December 2021).
- BioNTech Manufacturing GmbH. Comirnaty, INN-Tozinameran: Product Information. 2020. Available online: https://www.ema.europa.eu/en/documents/product-information/comirnaty-epar-product-information_en.pdf (accessed on 23 December 2021).
- Moderna Biotech Spain S.L. Spikevax (Previously COVID-19 Vaccine Moderna): Product Information. 2020. Available online: https://www.ema.europa.eu/en/documents/product-information/spikevax-previously-covid-19-vaccine-moderna-epar-product-information_en.pdf (accessed on 23 December 2021).
- Paul-Ehrlich-Institut. Sicherheitsbericht: Verdachtsfälle von Nebenwirkungen und Impfkomplikationen nach Impfung zum Schutz vor COVID-19. 2021. Available online: https://www.pei.de/SharedDocs/Downloads/DE/newsroom/dossiers/sicherheitsberichte/sicherheitsbericht-27-12-20-bis-31-12-21.pdf (accessed on 30 December 2021).
- Robert Koch-Institut. Aufklärungsbogen und Anamnese- und Einwilligungsbogen zur COVID-19-Impfung: Aktuelle Daten und Informationen zu Infektionskrankheiten und Public Health. Available online: https://www.rki.de/DE/Content/Infekt/Impfen/ImpfungenAZ/COVID-19/Aufklaerungsbogen-Tab.html (accessed on 1 November 2021).
- Noack, E.M.; Kleinert, E.; Müller, F. Overcoming language barriers in paramedic care: A study protocol of the interventional trial ’DICTUM rescue’ evaluating an app designed to improve communication between paramedics and foreign-language patients. BMC Health Serv. Res. 2020, 20, 223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, S.; Saliba, V.; Ramsay, M.; Mounier-Jack, S. What have we learnt from measles outbreaks in 3 English cities? A qualitative exploration of factors influencing vaccination uptake in Romanian and Roma Romanian communities. BMC Public Health 2020, 20, 381. [Google Scholar] [CrossRef] [PubMed]
- Schouten, B.C.; Meeuwesen, L. Cultural differences in medical communication: A review of the literature. Patient Educ. Couns. 2006, 64, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Schouten, B.C.; Meeuwesen, L.; Harmsen, H.A.M. The impact of an intervention in intercultural communication on doctor-patient interaction in The Netherlands. Patient Educ. Couns. 2005, 58, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Schouten, B.C.; Meeuwesen, L.; Harmsen, H.A.M. GPs’ interactional styles in consultations with Dutch and ethnic minority patients. J. Immigr. Minor. Health 2009, 11, 468–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawshaw, A.F.; Deal, A.; Rustage, K.; Forster, A.S.; Campos-Matos, I.; Vandrevala, T.; Würz, A.; Pharris, A.; Suk, J.E.; Kinsman, J.; et al. What must be done to tackle vaccine hesitancy and barriers to COVID-19 vaccination in migrants? J. Travel Med. 2021, 28, taab048. [Google Scholar] [CrossRef] [PubMed]

| Language/Dialect | ||
|---|---|---|
| Albanian | French | Romanian |
| Arabic | German (incl. sign language 1) | Russian |
| Bosnian | Greek | Serbian |
| Bulgarian | Hebrew | Slovakian |
| Chinese (China) | Hindi | Sorani (Central Kurdish) |
| Chinese (Taiwan) | Hungarian | Spanish (Spain) |
| Croatian | Italian | Spanish (Latin America) |
| Czech | Kurdish-Sorani | Swedish |
| Danish | Lithuanian | Tamil |
| Dari (Persian) | Pashto (Afghani) | Thai |
| Dutch | Polish | Turkish |
| English | Portuguese (Portugal) | Ukrainian |
| Farsi (Persian) | Portuguese (Brazil) | Vietnamese |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noack, E.M.; Schäning, J.; Müller, F. A Multilingual App for Providing Information to SARS-CoV-2 Vaccination Candidates with Limited Language Proficiency: Development and Pilot. Vaccines 2022, 10, 360. https://doi.org/10.3390/vaccines10030360
Noack EM, Schäning J, Müller F. A Multilingual App for Providing Information to SARS-CoV-2 Vaccination Candidates with Limited Language Proficiency: Development and Pilot. Vaccines. 2022; 10(3):360. https://doi.org/10.3390/vaccines10030360
Chicago/Turabian StyleNoack, Eva Maria, Jennifer Schäning, and Frank Müller. 2022. "A Multilingual App for Providing Information to SARS-CoV-2 Vaccination Candidates with Limited Language Proficiency: Development and Pilot" Vaccines 10, no. 3: 360. https://doi.org/10.3390/vaccines10030360
APA StyleNoack, E. M., Schäning, J., & Müller, F. (2022). A Multilingual App for Providing Information to SARS-CoV-2 Vaccination Candidates with Limited Language Proficiency: Development and Pilot. Vaccines, 10(3), 360. https://doi.org/10.3390/vaccines10030360