
The Role of Diffusion Tensor MR Imaging (DTI) of the Brain in Diagnosing Autism Spectrum Disorder: Promising Results

 ,
,  ,
,  ,
,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
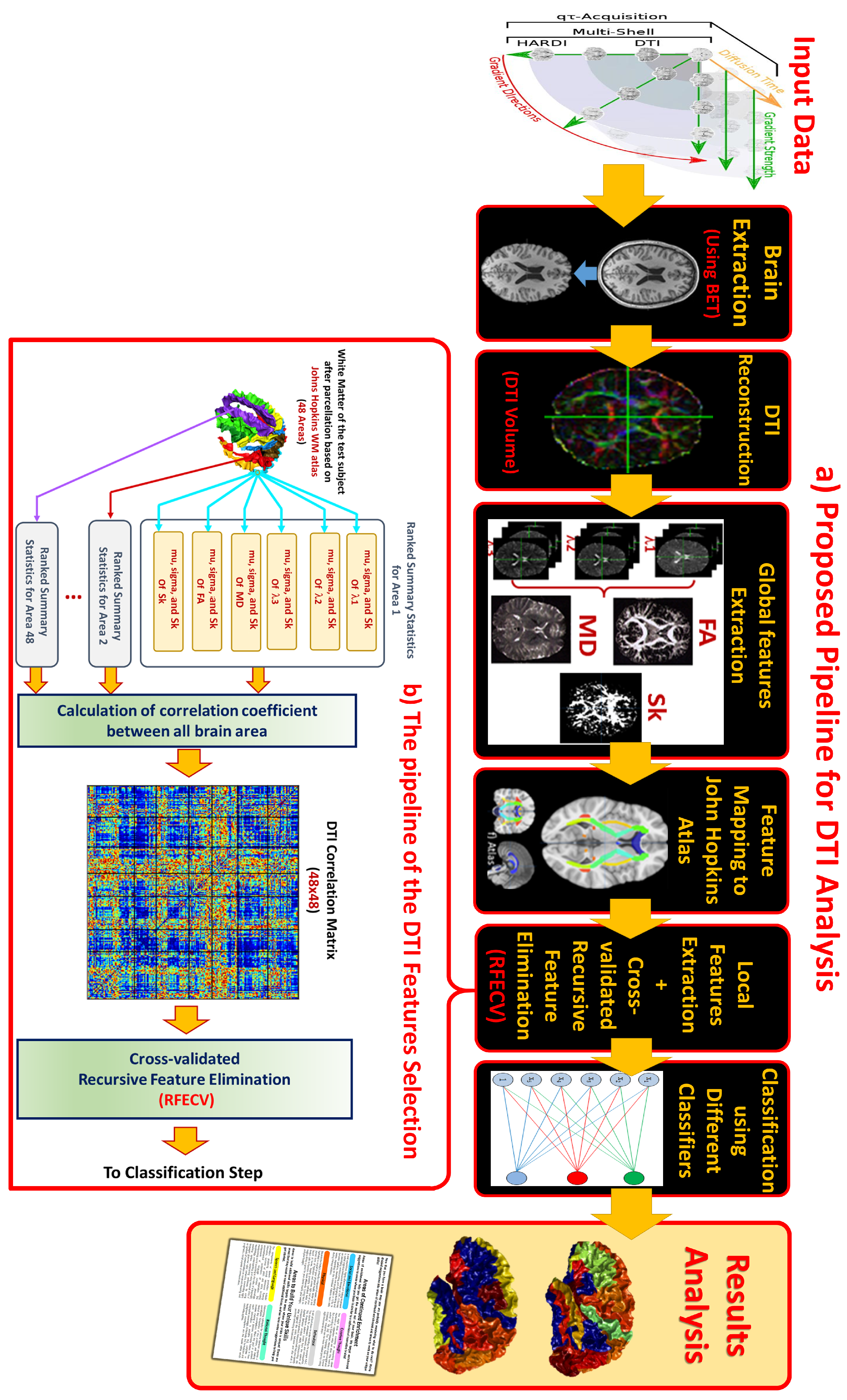
2. Methodology
2.1. Data Used
2.2. Pre-Processing
2.2.1. Input Image Preparation
2.2.2. Skull Stripping
2.2.3. Eddy Current Correction
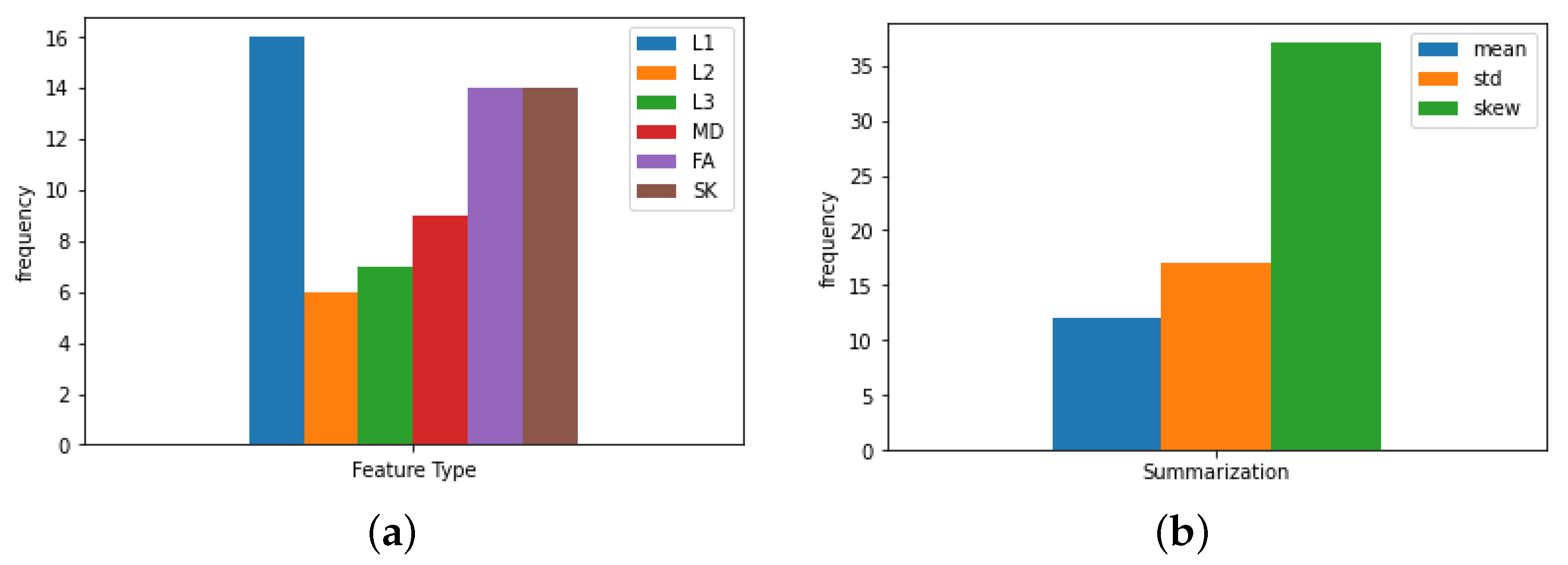
2.3. Feature Calculation
- 1.
- Fractional anisotropy (FA): Measures the degree of anisotropy of the diffusion, with zero representing completely isotropic diffusion, and one representing a directional diffusion [33];
- 2.
- Mean diffusivity (MD): Average magnitude of diffusion at each point, independent of the direction. ;
- 3.
- Axial diffusivity (AD): Magnitude of diffusion along the major axis; ;
- 4.
- & 5. Radial diffusivities: Magnitude of diffusion along the two perpendicular axes to AD: RDs = [λ2, λ3];
- 6.
- Tensor skewness: A higher order moment of diffusion, revealing more information not captured by lower order ones. [14];.
Data Cleaning
2.4. Atlas-Based Segmentation
2.5. Feature Representation
2.5.1. Feature Engineering
2.5.2. Feature Reduction: RFE-CV
2.6. Classification
| Algorithm 1 Diffusion tensor autism diagnosis algorithm. |
|
3. Results
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DTI | Diffusion tensor imaging |
| MRI | Magnetic resonance imaging |
| ASD | Autism spectrum disorder |
| ADOS | Autism Diagnostic Observation Schedule |
| ADI-R | Autism Diagnostic Interview-Revised |
| ABIDE | Autism Brain Imaging Data Exchange |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5); American Psychiatric Association: Arlington, TX, USA, 2013. [Google Scholar]
- Casanova, M.F.; El-Baz, A.; Suri, J.S. Autism Imaging and Devices; CRC Press: Boca Raton, FL, USA, 2017. [Google Scholar]
- Ismail, M.M.; Keynton, R.S.; Mostapha, M.M.; ElTanboly, A.H.; Casanova, M.F.; Gimel’farb, G.L.; El-Baz, A. Studying autism spectrum disorder with structural and diffusion magnetic resonance imaging: A survey. Front. Hum. Neurosci. 2016, 10, 211. [Google Scholar] [CrossRef] [Green Version]
- Muhle, R.; Trentacoste, S.V.; Rapin, I. The genetics of autism. Pediatrics 2004, 113, e472–e486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef] [PubMed]
- Falkmer, T.; Anderson, K.; Falkmer, M.; Horlin, C. Diagnostic procedures in autism spectrum disorders: A systematic literature review. Eur. Child Adolesc. Psychiatry 2013, 22, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.; Ford, T.; McCabe, R.; Russell, G. Autism diagnosis as a social process. Autism 2021. [Google Scholar] [CrossRef]
- Brieber, S.; Neufang, S.; Bruning, N.; Kamp-Becker, I.; Remschmidt, H.; Herpertz-Dahlmann, B.; Fink, G.R.; Konrad, K. Structural brain abnormalities in adolescents with autism spectrum disorder and patients with attention deficit/hyperactivity disorder. J. Child Psychol. Psychiatry 2007, 48, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Alexander, A.L.; Lee, J.E.; Lazar, M.; Boudos, R.; DuBray, M.B.; Oakes, T.R.; Miller, J.N.; Lu, J.; Jeong, E.K.; McMahon, W.M.; et al. Diffusion tensor imaging of the corpus callosum in Autism. Neuroimage 2007, 34, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Barnea-Goraly, N.; Kwon, H.; Menon, V.; Eliez, S.; Lotspeich, L.; Reiss, A.L. White matter structure in autism: Preliminary evidence from diffusion tensor imaging. Biol. Psychiatry 2004, 55, 323–326. [Google Scholar] [CrossRef]
- O’Donnell, L.J.; Westin, C.F. An introduction to diffusion tensor image analysis. Neurosurg. Clin. 2011, 22, 185–196. [Google Scholar] [CrossRef] [Green Version]
- Shukla, D.K.; Keehn, B.; Müller, R.A. Tract-specific analyses of diffusion tensor imaging show widespread white matter compromise in autism spectrum disorder. J. Child Psychol. Psychiatry 2011, 52, 286–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basser, P.J. New histological and physiological stains derived from diffusion-tensor MR images. Ann. N. Y. Acad. Sci. 1997, 820, 123–138. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.J.; Gu, H.; Gerig, G.; Elison, J.T.; Styner, M.; Gouttard, S.; Botteron, K.N.; Dager, S.R.; Dawson, G.; Estes, A.M.; et al. Differences in white matter fiber tract development present from 6 to 24 months in infants with autism. Am. J. Psychiatry 2012, 169, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.E.; Bigler, E.D.; Alexander, A.L.; Lazar, M.; DuBray, M.B.; Chung, M.K.; Johnson, M.; Morgan, J.; Miller, J.N.; McMahon, W.M.; et al. Diffusion tensor imaging of white matter in the superior temporal gyrus and temporal stem in autism. Neurosci. Lett. 2007, 424, 127–132. [Google Scholar] [CrossRef]
- Mostapha, M.; Casanova, M.F.; Gimel’farb, G.; El-Baz, A. Towards non-invasive image-based early diagnosis of autism. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Berlin/Heidelberg, Germany, 2015; pp. 160–168. [Google Scholar]
- Sundaram, S.K.; Kumar, A.; Makki, M.I.; Behen, M.E.; Chugani, H.T.; Chugani, D.C. Diffusion tensor imaging of frontal lobe in autism spectrum disorder. Cereb. Cortex 2008, 18, 2659–2665. [Google Scholar] [CrossRef]
- Ingalhalikar, M.; Parker, D.; Bloy, L.; Roberts, T.P.; Verma, R. Diffusion based abnormality markers of pathology: Toward learned diagnostic prediction of ASD. Neuroimage 2011, 57, 918–927. [Google Scholar] [CrossRef] [Green Version]
- Heinsfeld, A.S.; Franco, A.R.; Craddock, R.C.; Buchweitz, A.; Meneguzzi, F. Identification of autism spectrum disorder using deep learning and the ABIDE dataset. NeuroImage Clin. 2018, 17, 16–23. [Google Scholar] [CrossRef]
- Khosla, M.; Jamison, K.; Kuceyeski, A.; Sabuncu, M.R. 3D convolutional neural networks for classification of functional connectomes. In Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support; Springer: Berlin/Heidelberg, Germany, 2018; pp. 137–145. [Google Scholar]
- Dekhil, O.; Ali, M.; El-Nakieb, Y.; Shalaby, A.; Soliman, A.; Switala, A.; Mahmoud, A.; Ghazal, M.; Hajjdiab, H.; Casanova, M.F.; et al. A personalized autism diagnosis cad system using a fusion of structural mri and resting-state functional mri data. Front. Psychiatry 2019, 10, 392. [Google Scholar] [CrossRef] [PubMed]
- Elnakieb, Y.A.; Ali, M.T.; Soliman, A.; Mahmoud, A.H.; Shalaby, A.M.; Alghamdi, N.S.; Ghazal, M.; Khalil, A.; Switala, A.; Keynton, R.S.; et al. Computer Aided Autism Diagnosis Using Diffusion Tensor Imaging. IEEE Access 2020, 8, 191298–191308. [Google Scholar] [CrossRef]
- Lu, L.; Chen, T.; Chen, Y.; Yuan, M.; Gerstein, M.; Li, T.; Liang, H.; Froehlich, T. Towards developing a practical artificial intelligence tool for diagnosing and evaluating autism spectrum disorder: A study using multicenter ABIDE II datasets. JMIR Med. Inform. 2020, 8, e15767. [Google Scholar] [CrossRef]
- Farooq, H.; Chen, Y.; Georgiou, T.T.; Tannenbaum, A.; Lenglet, C. Network curvature as a hallmark of brain structural connectivity. Nat. Commun. 2019, 10, 4937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fredo, A.J.; Jahedi, A.; Reiter, M.; Müller, R.A. Diagnostic classification of autism using resting-state fMRI data and conditional random forest. Age 2018, 12, 6–41. [Google Scholar]
- Crimi, A.; Dodero, L.; Murino, V.; Sona, D. Case-control discrimination through effective brain connectivity. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 970–973. [Google Scholar]
- Bellman, R. Dynamic programming. Science 1966, 153, 34–37. [Google Scholar] [CrossRef]
- Haar, S.; Berman, S.; Behrmann, M.; Dinstein, I. Anatomical abnormalities in autism? Cereb. Cortex 2016, 26, 1440–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sen, B.; Borle, N.C.; Greiner, R.; Brown, M.R. A general prediction model for the detection of ADHD and Autism using structural and functional MRI. PLoS ONE 2018, 13, e0194856. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M. Fast robust automated brain extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef]
- Bodammer, N.; Kaufmann, J.; Kanowski, M.; Tempelmann, C. Eddy current correction in diffusion-weighted imaging using pairs of images acquired with opposite diffusion gradient polarity. Magn. Reson. Med. 2004, 51, 188–193. [Google Scholar] [CrossRef]
- Alexander, A.L.; Lee, J.E.; Lazar, M.; Field, A.S. Diffusion tensor imaging of the brain. Neurotherapeutics 2007, 4, 316–329. [Google Scholar] [CrossRef] [Green Version]
- Mori, S.; Wakana, S.; Van Zijl, P.C.; Nagae-Poetscher, L.M. MRI Atlas of Human White Matter; Elsevier: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Wang, Y.; Gupta, A.; Liu, Z.; Zhang, H.; Escolar, M.L.; Gilmore, J.H.; Gouttard, S.; Fillard, P.; Maltbie, E.; Gerig, G.; et al. DTI registration in atlas based fiber analysis of infantile Krabbe disease. Neuroimage 2011, 55, 1577–1586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyon, I.; Weston, J.; Barnhill, S.; Vapnik, V. Gene selection for cancer classification using support vector machines. Mach. Learn. 2002, 46, 389–422. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. Mach. Learn. 2011, 12, 2825–2830. [Google Scholar]
- Di Martino, A.; O’connor, D.; Chen, B.; Alaerts, K.; Anderson, J.S.; Assaf, M.; Balsters, J.H.; Baxter, L.; Beggiato, A.; Bernaerts, S.; et al. Enhancing studies of the connectome in autism using the autism brain imaging data exchange II. Sci. Data 2017, 4, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Panesar, S.S.; Yeh, F.C.; Deibert, C.P.; Fernandes-Cabral, D.; Rowthu, V.; Celtikci, P.; Celtikci, E.; Hula, W.D.; Pathak, S.; Fernández-Miranda, J.C. A diffusion spectrum imaging-based tractographic study into the anatomical subdivision and cortical connectivity of the ventral external capsule: Uncinate and inferior fronto-occipital fascicles. Neuroradiology 2017, 59, 971–987. [Google Scholar] [CrossRef]
- Kleinhans, N.M.; Pauley, G.; Richards, T.; Neuhaus, E.; Martin, N.; Corrigan, N.M.; Shaw, D.W.; Estes, A.; Dager, S.R. Age-related abnormalities in white matter microstructure in autism spectrum disorders. Brain Res. 2012, 1479, 1–16. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, K.; Travers, B.G.; Dadalko, O.I.; Dean III, D.C.; Tromp, D.; Adluru, N.; Destiche, D.; Freeman, A.; Prigge, M.D.; Froehlich, A.; et al. Longitudinal development of thalamic and internal capsule microstructure in autism spectrum disorder. Autism Res. 2018, 11, 450–462. [Google Scholar] [CrossRef]
- Saaybi, S.; AlArab, N.; Hannoun, S.; Saade, M.; Tutunji, R.; Zeeni, C.; Shbarou, R.; Hourani, R.; Boustany, R.M. Pre-and post-therapy assessment of clinical outcomes and white matter integrity in autism Spectrum disorder: Pilot study. Front. Neurol. 2019, 10, 877. [Google Scholar] [CrossRef] [Green Version]
- Vogan, V.; Morgan, B.; Leung, R.; Anagnostou, E.; Doyle-Thomas, K.; Taylor, M. Widespread white matter differences in children and adolescents with autism spectrum disorder. J. Autism Dev. Disord. 2016, 46, 2138–2147. [Google Scholar] [CrossRef]
- Bashat, D.B.; Kronfeld-Duenias, V.; Zachor, D.A.; Ekstein, P.M.; Hendler, T.; Tarrasch, R.; Even, A.; Levy, Y.; Sira, L.B. Accelerated maturation of white matter in young children with autism: A high b value DWI study. Neuroimage 2007, 37, 40–47. [Google Scholar] [CrossRef]
- Shukla, D.K.; Keehn, B.; Lincoln, A.J.; Müller, R.A. White matter compromise of callosal and subcortical fiber tracts in children with autism spectrum disorder: A diffusion tensor imaging study. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 1269–1278. [Google Scholar]
- Yamagata, B.; Itahashi, T.; Nakamura, M.; Mimura, M.; Hashimoto, R.I.; Kato, N.; Aoki, Y. White matter endophenotypes and correlates for the clinical diagnosis of autism spectrum disorder. Soc. Cogn. Affect. Neurosci. 2018, 13, 765–773. [Google Scholar] [CrossRef] [Green Version]
- Brito, A.R.; Vasconcelos, M.M.; Domingues, R.C.; Hygino da Cruz Jr, L.C.; Rodrigues, L.d.S.; Gasparetto, E.L.; Calçada, C.A.B.P. Diffusion tensor imaging findings in school-aged autistic children. J. Neuroimaging 2009, 19, 337–343. [Google Scholar] [CrossRef]
- Sivaswamy, L.; Kumar, A.; Rajan, D.; Behen, M.; Muzik, O.; Chugani, D.; Chugani, H. A diffusion tensor imaging study of the cerebellar pathways in children with autism spectrum disorder. J. Child Neurol. 2010, 25, 1223–1231. [Google Scholar] [CrossRef]
- Cheng, Y.; Chou, K.H.; Chen, I.Y.; Fan, Y.T.; Decety, J.; Lin, C.P. Atypical development of white matter microstructure in adolescents with autism spectrum disorders. Neuroimage 2010, 50, 873–882. [Google Scholar] [CrossRef]
- Barnea-Goraly, N.; Lotspeich, L.J.; Reiss, A.L. Similar white matter aberrations in children with autism and their unaffected siblings: A diffusion tensor imaging study using tract-based spatial statistics. Arch. Gen. Psychiatry 2010, 67, 1052–1060. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.W.; Lee, A.; Choi, T.K.; Kim, B.; Lee, K.S.; Bang, M.; Lee, S.H. White matter abnormalities of the tapetum and their associations with duration of untreated psychosis and symptom severity in first-episode psychosis. Schizophr. Res. 2018, 201, 437–438. [Google Scholar] [CrossRef]
- Payabvash, S.; Palacios, E.M.; Owen, J.P.; Wang, M.B.; Tavassoli, T.; Gerdes, M.; Brandes-Aitken, A.; Cuneo, D.; Marco, E.J.; Mukherjee, P. White matter connectome edge density in children with autism spectrum disorders: Potential imaging biomarkers using machine-learning models. Brain Connect. 2019, 9, 209–220. [Google Scholar] [CrossRef]
- Groen, W.B.; Buitelaar, J.K.; Van Der Gaag, R.J.; Zwiers, M.P. Pervasive microstructural abnormalities in autism: A DTI study. J. Psychiatry Neurosci. JPN 2011, 36, 32. [Google Scholar] [CrossRef] [Green Version]
- Karahanoğlu, F.I.; Baran, B.; Nguyen, Q.T.H.; Meskaldji, D.E.; Yendiki, A.; Vangel, M.; Santangelo, S.L.; Manoach, D.S. Diffusion-weighted imaging evidence of altered white matter development from late childhood to early adulthood in autism spectrum disorder. Neuroimage Clin. 2018, 19, 840–847. [Google Scholar] [CrossRef]
- Itahashi, T.; Yamada, T.; Nakamura, M.; Watanabe, H.; Yamagata, B.; Jimbo, D.; Shioda, S.; Kuroda, M.; Toriizuka, K.; Kato, N.; et al. Linked alterations in gray and white matter morphology in adults with high-functioning autism spectrum disorder: A multimodal brain imaging study. NeuroImage Clin. 2015, 7, 155–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rane, P.; Cochran, D.; Hodge, S.M.; Haselgrove, C.; Kennedy, D.; Frazier, J.A. Connectivity in autism: A review of MRI connectivity studies. Harv. Rev. Psychiatry 2015, 23, 223. [Google Scholar] [CrossRef] [Green Version]
- Vasa, R.A.; Mostofsky, S.H.; Ewen, J.B. The disrupted connectivity hypothesis of autism spectrum disorders: Time for the next phase in research. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2016, 1, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Classifier | Hyper-Parameter | Range/ Values |
|---|---|---|
| (1) LSVM | Regularization (C) | 0.1, 1, 5, 10 |
| Loss function (loss) | L1, L2 | |
| Penalization strategy (penalty) | squared_hinge, hinge | |
| (2) LR | Penalization strategy (penalty) | L1, L2 elastic |
| Regularization (C) | 0.1, 1, 5, 10 | |
| Solver algorithm (solver) | newton-cg, lbfgs, liblinear, sag, saga | |
| (3) PassiveAgressive | Regularization (C) | 0.1, 1, 5, 10 |
| N idle iteration before stop (n_iter_no_change) | 1, 5, 10 | |
| (4) Nonlinear-SVM | Regularization (C) | 0.1, 1, 5, 10 |
| Kernel used (kernel) | rbf, poly, sigmoid | |
| Polynomial kernel degree (degree) | 2–6 | |
| Kernel coefficient (gamma) | scale, auto | |
| Independent term in kernel function (coef0) | 0.0, 0.01, 0.1, 1, 5, 10, 50, 100 | |
| (5) GNB | Default parameters | priors = None, var_smoothing = |
| (6) RF | Number of features to consider when looking for the best split (max_features) | auto, sqrt, log2 |
| Number of trees in the forest (n_estimators) | 50, 100, 200, 500, 1000 | |
| Function to measure the quality of a split (criterion) | gini, entropy | |
| Bootstrap samples when building trees (bootstrap) | True, False | |
| Min # of samples required to split an internal node (min_samples) | 1, 2, 5, 10 | |
| (7) XGB | Which booster to use (booster) | gbtree, gblinear, dart |
| Learning rate (learning_rate) | 0.001, 0.01, 0.1, 0.3, 0.5, 1 | |
| Min loss reduction required to make a further partition on a leaf node (gamma) | 0, 0.1, 0.5, 1, 1.5, 2, 5, 20, 50, 100 | |
| Min sum of instance weight needed in a child (min_child_weight) | 0.1,0.5, 1, 5, 10 | |
| Subsample ratio of columns when constructing each tree (colsample_bytree) | 0.6, 0.8, 1.0 | |
| L2 regularization term on weights (lambda) | 0, 0.001, 0.5, 1, 10 | |
| L1 regularization term on weights (alpha) | 0, 0.001, 0.5, 1, 10 | |
| (8) NN | Hidden layer sizes (hidden_layer_sizes) | (150,100,50,), (100,50,25,), (100,) |
| Activation function (activation) | tanh, relu, logistic | |
| Solver used for weight optimization (solver) | lbfgs, sgd, adam | |
| L2 regularization penalty (alpha) | 0.0001,0.001,0.01, 0.05, 0.1, 0.5 | |
| Initial learning rate (learning_rate) | constant, adaptive | |
| Exponential decay rate for estimates of first moment vector in adam (beta_1) | 0, 0.001, 0.01, 0.1, 0.3, 0.5, 0.9 | |
| Exponential decay rate for estimates of second moment vector in adam (beta_2) | 0, 0.001, 0.01, 0.1, 0.3, 0.5, 0.9 |
| lSVM | {‘penalty’: ‘l2’, ‘loss’: ‘hinge’, ‘C’: 1} |
| pagg | {‘n_iter_no_change’: 5, ‘C’: 0.1} |
| LR | {‘solver’: ‘newton-cg’, ‘penalty’: ‘none’, ‘C’: 0.1} |
| XGB | {‘reg_lambda’: 0.001, ‘reg_alpha’: 0, ‘min_child_weight’: 10, ‘learning_rate’: 1, ‘gamma’: 0.1, ‘colsample_bytree’: 0.6, ‘booster’: ‘gblinear’} |
| GNB | defaults |
| SVC | {‘kernel’: ‘poly’, ‘gamma’: ‘scale’, ‘degree’: 3, ‘coef0’: 5, ‘C’: 0.1} |
| Rf | {n_estimators’: 50, ‘min_samples_split’: 2, ‘min_samples_leaf’: 0.1, ‘max_features’: ‘sqrt’, ‘criterion’: ‘entropy’, ‘bootstrap’: False} |
| nn | {‘solver’: ‘adam’, ‘learning_rate’: ‘adaptive’, ‘hidden_layer_sizes’: (100,), ‘beta_2’: 0.5, ‘beta_1’: 0.5, ‘alpha’: 0.0001, ‘activation’: ‘logistic’} |
| k = 2 | k = 4 | k = 5 | k = 10 | |
|---|---|---|---|---|
| LSVM | 0.92 ± 0.018 | 0.991 ± 0.015 | 0.999 ± 0.002 | 0.999 ± 0.002 |
| pagg | 0.893 ± 0.018 | 0.951 ± 0.037 | 0.96 ± 0.026 | 0.982 ± 0.03 |
| LR | 0.902 ± 0.0 | 0.964 ± 0.018 | 0.978 ± 0.02 | 0.991 ± 0.018 |
| XGB | 0.556 ± 0.011 | 0.604 ± 0.021 | 0.591 ± 0.041 | 0.609 ± 0.119 |
| GNB | 0.644 ± 0.025 | 0.618 ± 0.079 | 0.613 ± 0.08 | 0.684 ± 0.133 |
| RBF-SVM | 0.511 ± 0.038 | 0.529 ± 0.021 | 0.573 ± 0.022 | 0.582 ± 0.076 |
| RF | 0.609 ± 0.02 | 0.591 ± 0.04 | 0.591 ± 0.05 | 0.596 ± 0.054 |
| NN | 0.871 ± 0.004 | 0.969 ± 0.019 | 0.973 ± 0.026 | 0.964 ± 0.034 |
| k = 2 | k = 4 | k = 5 | k = 10 | |
|---|---|---|---|---|
| LSVM | 0.919 | 0.991 | 0.999 | 0.999 |
| pagg | 0.891 | 0.948 | 0.959 | 0.982 |
| LR | 0.9 | 0.962 | 0.977 | 0.991 |
| XGB | 0.543 | 0.593 | 0.583 | 0.606 |
| GNB | 0.644 | 0.618 | 0.608 | 0.683 |
| RBF-SVM | 0.509 | 0.529 | 0.565 | 0.575 |
| RF | 0.571 | 0.549 | 0.548 | 0.552 |
| NN | 0.873 | 0.969 | 0.975 | 0.963 |
| Retrolenticular Part of Internal Capsule L | & | Fornix Cres/Stria Terminalis |
| Anterior Limb of Internal Capsule L | & | Uncinate Fasciculus R |
| Body of Corpus Callosum | & | Tapetum L |
| Corticospinal Tract R | & | Posterior Corona Radiata R |
| Posterior Limb of Internal Capsule R | & | Retrolenticular Part Of Internal Capsule R |
| External Capsule R | & | Tapetum L |
| Middle Cerebellar Peduncle | & | Inferior Cerebellar Peduncle R |
| Anterior Limb of Internal Capsule R | & | Tapetum R |
| Middle Cerebellar Peduncle | & | Cingulum Cingulate Gyrus L |
| Anterior Limb of Internal Capsule R | & | Fornix Cres /StriaTerminalis R |
| Inferior Cerebellar Peduncle R | & | Retrolenticular Part Of Internal Capsule R |
| Cingulum Hippocampus L | & | Superior Fronto-occipital Fasciculus R |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
ElNakieb, Y.; Ali, M.T.; Elnakib, A.; Shalaby, A.; Soliman, A.; Mahmoud, A.; Ghazal, M.; Barnes, G.N.; El-Baz, A. The Role of Diffusion Tensor MR Imaging (DTI) of the Brain in Diagnosing Autism Spectrum Disorder: Promising Results. Sensors 2021, 21, 8171. https://doi.org/10.3390/s21248171
ElNakieb Y, Ali MT, Elnakib A, Shalaby A, Soliman A, Mahmoud A, Ghazal M, Barnes GN, El-Baz A. The Role of Diffusion Tensor MR Imaging (DTI) of the Brain in Diagnosing Autism Spectrum Disorder: Promising Results. Sensors. 2021; 21(24):8171. https://doi.org/10.3390/s21248171
Chicago/Turabian StyleElNakieb, Yaser, Mohamed T. Ali, Ahmed Elnakib, Ahmed Shalaby, Ahmed Soliman, Ali Mahmoud, Mohammed Ghazal, Gregory Neal Barnes, and Ayman El-Baz. 2021. "The Role of Diffusion Tensor MR Imaging (DTI) of the Brain in Diagnosing Autism Spectrum Disorder: Promising Results" Sensors 21, no. 24: 8171. https://doi.org/10.3390/s21248171
APA StyleElNakieb, Y., Ali, M. T., Elnakib, A., Shalaby, A., Soliman, A., Mahmoud, A., Ghazal, M., Barnes, G. N., & El-Baz, A. (2021). The Role of Diffusion Tensor MR Imaging (DTI) of the Brain in Diagnosing Autism Spectrum Disorder: Promising Results. Sensors, 21(24), 8171. https://doi.org/10.3390/s21248171