
Effects of a Mediterranean Diet Intervention on Maternal Stress, Well-Being, and Sleep Quality throughout Gestation—The IMPACT-BCN Trial

 , , , , , ,
, , , , , ,  , , ,
, , ,  ,
,  ,
,  , and add
Show full author list
, and add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Population and Ethics
2.2. Interventions and Measurements
2.2.1. Mediterranean Diet Program
2.2.2. Usual Care (Control Group)
2.3. Outcomes
2.4. Data Collection
2.5. Sample Collection
2.6. Statistical Analysis
3. Results
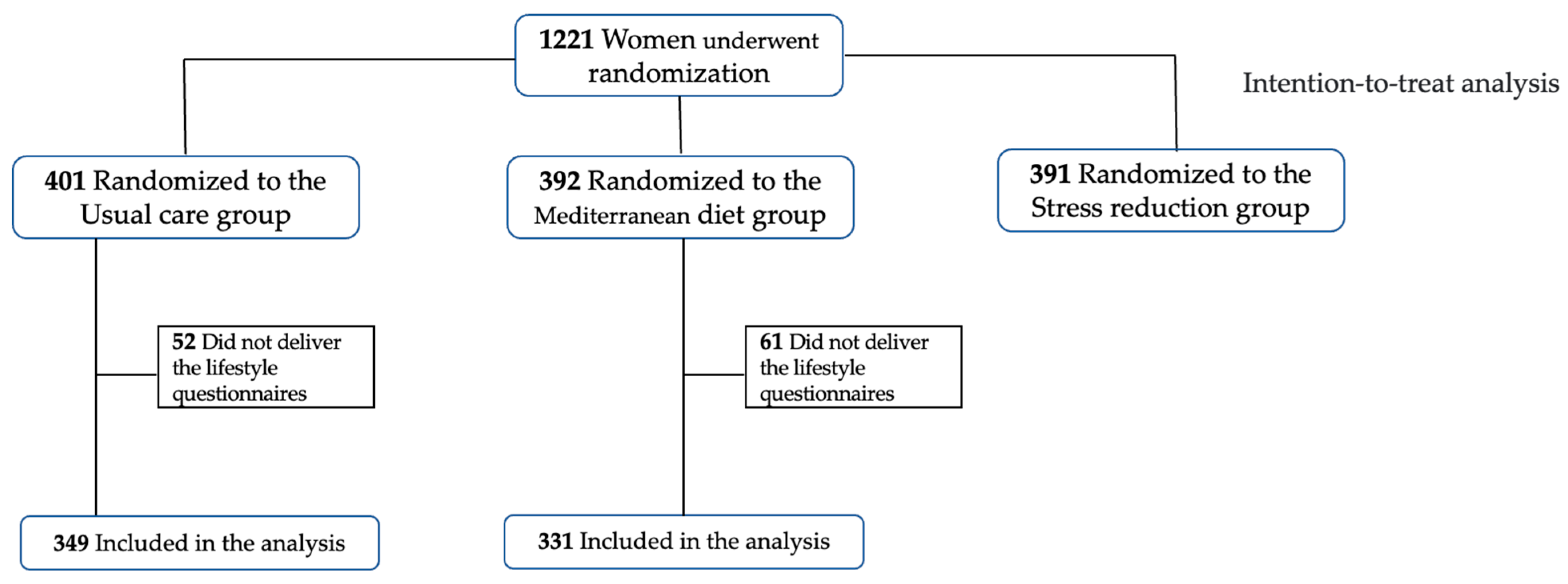
3.1. Study Population and Pregnancy Outcomes
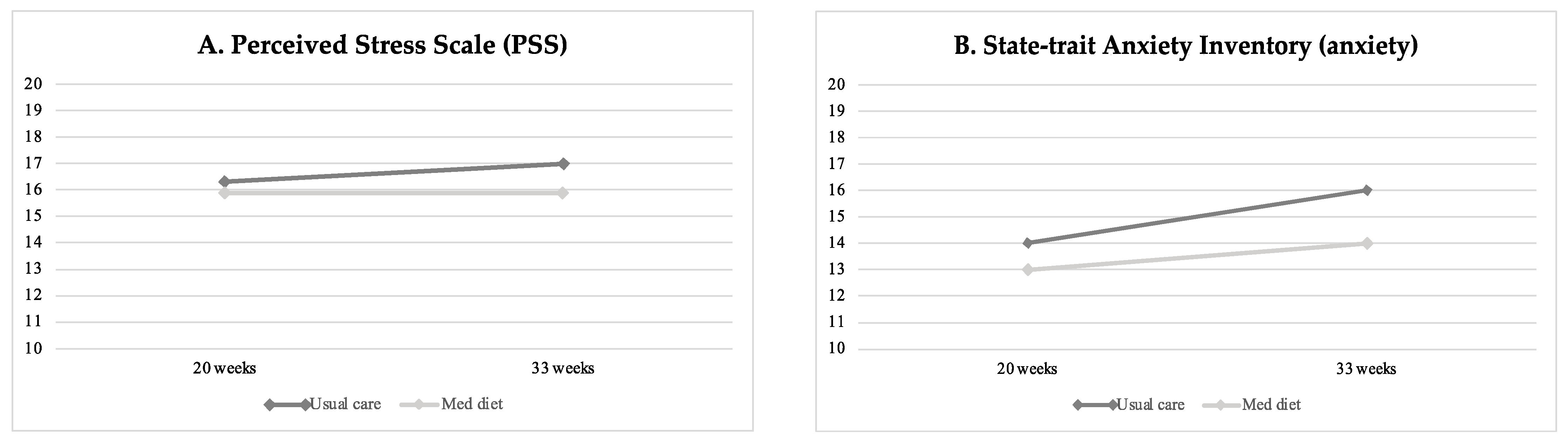
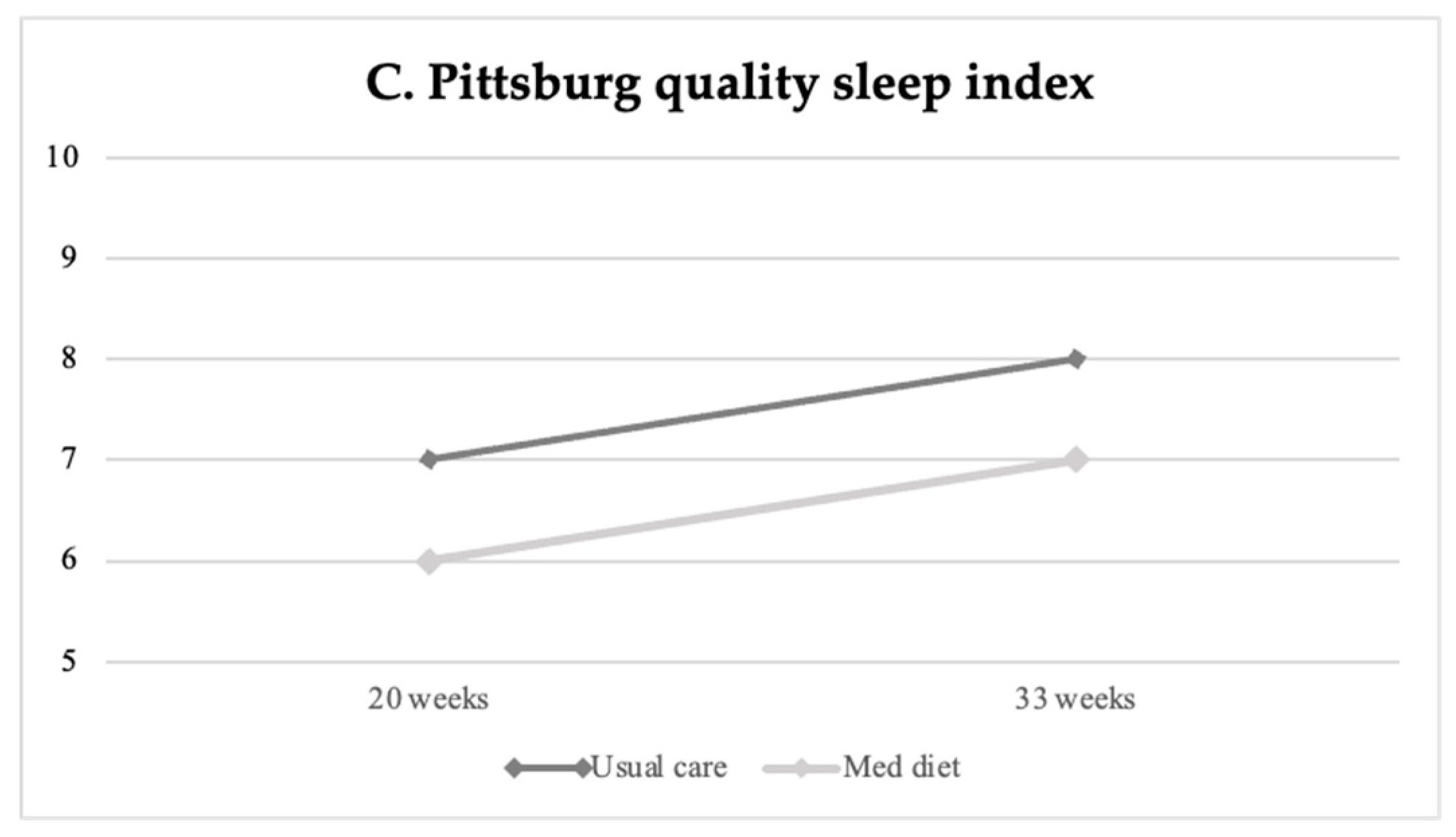
3.2. Effects of Mediterranean Diet on Stress, Anxiety, Well-Being, Sleep Quality and Mindful State
3.2.1. Life-Style Questionnaires
3.2.2. Cortisol Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Salas-Salvadó, J.; Díaz-López, A.; Ruiz-Canela, M.; Basora, J.; Fitó, M.; Corella, D.; Serra-Majem, L.; Wärnberg, J.; Romaguera, D.; Estruch, R.; et al. Effect of a Lifestyle Intervention Program With Energy-Restricted Mediterranean Diet and Exercise on Weight Loss and Cardiovascular Risk Factors: One-Year Results of the PREDIMED-Plus Trial. Diabetes Care 2019, 42, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Valls-Pedret, C.; Sala-Vila, A.; Serra-Mir, M.; Corella, D.; De La Torre, R.; Martínez-González, M.Á.; Martínez-Lapiscina, E.H.; Fitó, M.; Pérez-Heras, A.; Salas-Salvadó, J.; et al. Mediterranean Diet and Age-Related Cognitive Decline: A Randomized Clinical Trial. JAMA Intern. Med. 2015, 175, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Toledo, E.; Salas-Salvado, J.; Donat-Vargas, C.; Buil-Cosiales, P.; Estruch, R.; Ros, E.; Corella, D.; Fito, M.; Hu, F.B.; Aros, F.; et al. Mediterranean Diet and Invasive Breast Cancer Risk Among Women at High Cardiovascular Risk in the PREDIMED Trial: A Randomized Clinical Trial. JAMA Intern. Med. 2015, 175, 1752–1760. [Google Scholar] [CrossRef]
- Ventriglio, A.; Sancassiani, F.; Contu, M.P.; Latorre, M.; Di Slavatore, M.; Fornaro, M.; Bhugra, D. Mediterranean Diet and Its Benefits on Health and Mental Health: A Literature Review. Clin. Pract. Epidemiol. Ment. Health 2020, 16, 156. [Google Scholar] [CrossRef]
- Ventriglio, A.; Gentile, A.; Stella, E.; Bellomo, A. Metabolic Issues in Patients Affected by Schizophrenia: Clinical Characteristics and Medical Management. Front. Neurosci. 2015, 9, 297. [Google Scholar] [CrossRef]
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B.; et al. A Mediterranean-Style Dietary Intervention Supplemented with Fish Oil Improves Diet Quality and Mental Health in People with Depression: A Randomized Controlled Trial (HELFIMED). Nutr. Neurosci. 2017, 22, 474–487. [Google Scholar] [CrossRef]
- Cano-Ibáñez, N.; Serra-Majem, L.; Martín-Peláez, S.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella Piquer, M.D.; Lassale, C.; Martínez Hernandez, J.A.; Alonso-Gómez, Á.M.; Wärnberg, J.; et al. Association between the Prime Diet Quality Score and Depressive Symptoms in a Mediterranean Population with Metabolic Syndrome. Cross-Sectional and 2-Year Follow-up Assessment from PREDIMED-PLUS Study. Br. J. Nutr. 2022, 128, 1170–1179. [Google Scholar] [CrossRef]
- Sánchez-Villegas, A.; Martínez-González, M.A.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Covas, M.I.; Arós, F.; Romaguera, D.; Gómez-Gracia, E.; Lapetra, J.; et al. Mediterranean Dietary Pattern and Depression: The PREDIMED Randomized Trial. BMC Med. 2013, 11, 208. [Google Scholar] [CrossRef]
- Bayes, J.; Schloss, J.; Sibbritt, D. Effects of Polyphenols in a Mediterranean Diet on Symptoms of Depression: A Systematic Literature Review. Adv. Nutr. 2020, 11, 602–615. [Google Scholar] [CrossRef]
- Taylor, A.M.; Holscher, H.D. A Review of Dietary and Microbial Connections to Depression, Anxiety, and Stress. Nutr. Neurosci. 2018, 23, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Moylan, S.; Berk, M.; Dean, O.M.; Samuni, Y.; Williams, L.J.; O’Neil, A.; Hayley, A.C.; Pasco, J.A.; Anderson, G.; Jacka, F.N.; et al. Oxidative & Nitrosative Stress in Depression: Why so Much Stress? Neurosci. Biobehav. Rev. 2014, 45, 46–62. [Google Scholar] [CrossRef] [PubMed]
- Berk, M.; Williams, L.J.; Jacka, F.N.; O’Neil, A.; Pasco, J.A.; Moylan, S.; Allen, N.B.; Stuart, A.L.; Hayley, A.C.; Byrne, M.L.; et al. So Depression Is an Inflammatory Disease, but Where Does the Inflammation Come from? BMC Med. 2013, 11, 200. [Google Scholar] [CrossRef]
- Fawcett, E.J.; Fairbrother, N.; Cox, M.L.; White, I.R.; Fawcett, J.M. The Prevalence of Anxiety Disorders During Pregnancy and the Postpartum Period: A Multivariate Bayesian Meta-Analysis. J. Clin. Psychiatry 2019, 80, 1181. [Google Scholar] [CrossRef] [PubMed]
- Traylor, C.S.; Johnson, J.D.; Kimmel, M.C.; Manuck, T.A. Effects of Psychological Stress on Adverse Pregnancy Outcomes and Nonpharmacologic Approaches for Reduction: An Expert Review. Am. J. Obstet. Gynecol. MFM 2020, 2, 100229. [Google Scholar] [CrossRef] [PubMed]
- Flor-Alemany, M.; Baena-García, L.; Migueles, J.H.; Henriksson, P.; Löf, M.; Aparicio, V.A. Associations of Mediterranean Diet with Psychological Ill-Being and Well-Being throughout the Pregnancy Course: The GESTAFIT Project. Qual. Life Res. 2022, 31, 2705–2716. [Google Scholar] [CrossRef]
- Crovetto, F.; Crispi, F.; Casas, R.; Martín-Asuero, A.; Borràs, R.; Vieta, E.; Estruch, R.; Gratacós, E. Effects of Mediterranean Diet or Mindfulness-Based Stress Reduction on Prevention of Small-for-Gestational Age Birth Weights in Newborns Born to At-Risk Pregnant Individuals: The IMPACT BCN Randomized Clinical Trial. JAMA 2021, 326, 2150–2160. [Google Scholar] [CrossRef]
- Crovetto, F.; Crispi, F.; Borras, R.; Paules, C.; Casas, R.; Martín, R.; Arranz, A.; Vieta, E.; Estruch, R.G.E. Mediterranean Diet, Mindfulness Based Stress Reduction and Usual Care during Pregnancy for Reducing Fetal Growth Restriction and Adverse Perinatal Outcomes: IMPACT BCN (Improving Mothers for a Better PrenAtal Care Trial Barcelona): A Study Protocol for Randomized Controlled Trial. Trials 2021, 22, 1–14. [Google Scholar]
- Royal College of Obstetricians and Gynaecologist. The Investigation and Management of the Small for Gestational Age Fetus. Green-Top Guidel. 2013, 31, 1–34. [Google Scholar]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Juton, C.; Castro-barquero, S.; Casas, R.; Freitas, T.; Ruiz-león, A.M.; Crovetto, F.; Domenech, M.; Crispi, F.; Vieta, E.; Gratacós, E.; et al. Reliability and Concurrent and Construct Validity of a Food Frequency Questionnaire for Pregnant Women at High Risk to Develop Fetal Growth Restriction. Nutrients 2021, 13, 1629. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Vagg, P.R. Psychometric Properties of the STAI: A Reply to Ramanaiah, Franzen, and Schill. J. Pers. Assess. 1984, 48, 95–97. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Bech, P.; Olsen, L.R.; Kjoller, M.; Rasmussen, N.K. Measuring Well-Being Rather than the Absence of Distress Symptoms: A Comparison of the SF-36 Mental Health Subscale and the WHO-Five Well-Being Scale. Int. J. Methods Psychiatr. Res. 2003, 12, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using Self-Report Assessment Methods to Explore Facets of Mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Bonnín, C.M.; Yatham, L.N.; Michalak, E.E.; Martínez-Arán, A.; Dhanoa, T.; Torres, I.; Santos-Pascual, C.; Valls, E.; Carvalho, A.F.; Sánchez-Moreno, J.; et al. Psychometric Properties of the Well-Being Index (WHO-5) Spanish Version in a Sample of Euthymic Patients with Bipolar Disorder. J. Affect. Disord. 2018, 228, 153–159. [Google Scholar] [CrossRef]
- Marcos, J.; Renau, N.; Casals, G.; Segura, J.; Ventura, R.; Pozo, O.J. Investigation of Endogenous Corticosteroids Profiles in Human Urine Based on Liquid Chromatography Tandem Mass Spectrometry. Anal. Chim. Acta 2014, 812, 92–104. [Google Scholar] [CrossRef]
- Jacka, F.N.; O’Neil, A.; Opie, R.; Itsiopoulos, C.; Cotton, S.; Mohebbi, M.; Castle, D.; Dash, S.; Mihalopoulos, C.; Chatterton, M.L.; et al. A Randomised Controlled Trial of Dietary Improvement for Adults with Major Depression (the “SMILES” Trial). BMC Med. 2017, 15, 23. [Google Scholar] [CrossRef]
- Papandreou, P.; Amerikanou, C.; Vezou, C.; Gioxari, A.; Kaliora, A.C.; Skouroliakou, M. Improving Adherence to the Mediterranean Diet in Early Pregnancy Using a Clinical Decision Support System; A Randomised Controlled Clinical Trial. Nutrients 2023, 15, 432. [Google Scholar] [CrossRef]
- Huang, P.; Wei, D.; Xiao, W.; Yuan, M.; Chen, N.; Wei, X.; Xie, J.; Lu, J.; Xia, X.; Lu, M.; et al. Maternal Dietary Patterns and Depressive Symptoms during Pregnancy: The Born in Guangzhou Cohort Study. Clin. Nutr. 2021, 40, 3485–3494. [Google Scholar] [CrossRef] [PubMed]
- Miyake, Y.; Tanaka, K.; Okubo, H.; Sasaki, S.; Furukawa, S.; Arakawa, M. Dietary Patterns and Depressive Symptoms during Pregnancy in Japan: Baseline Data from the Kyushu Okinawa Maternal and Child Health Study. J. Affect. Disord. 2018, 225, 552–558. [Google Scholar] [CrossRef]
- Tokumitsu, K.; Tokumitsu, K.; Sugawara, N.; Sugawara, N.; Maruo, K.; Suzuki, T.; Shimoda, K.; Yasui-Furukori, N.; Yasui-Furukori, N. Prevalence of Perinatal Depression among Japanese Women: A Meta-Analysis. Ann. Gen. Psychiatry 2020, 19, 41. [Google Scholar] [CrossRef]
- Paskulin, J.T.A.; Drehmer, M.; Olinto, M.T.; Hoffmann, J.F.; Pinheiro, A.P.; Schmidt, M.I.; Nunes, M.A. Association between Dietary Patterns and Mental Disorders in Pregnant Women in Southern Brazil. Braz. J. Psychiatry 2017, 39, 208. [Google Scholar] [CrossRef] [PubMed]
- Fowles, E.R.; Stang, J.; Bryant, M.; Kim, S.H. Stress, Depression, Social Support, and Eating Habits Reduce Diet Quality in the First Trimester in Low-Income Women: A Pilot Study. J. Acad. Nutr. Diet. 2012, 112, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Agostino, D.; Caballero, F.F.; Martín-María, N.; Tyrovolas, S.; López-García, P.; Rodríguez-Artalejo, F.; Haro, J.M.; Ayuso-Mateos, J.L.; Miret, M. Mediterranean Diet and Wellbeing: Evidence from a Nationwide Survey. Psychol. Health 2019, 34, 321–335. [Google Scholar] [CrossRef]
- Flor-Alemany, M.; Nestares, T.; Alemany-Arrebola, I.; Marín-Jiménez, N.; Borges-Cosic, M.; Aparicio, V.A. Influence of Dietary Habits and Mediterranean Diet Adherence on Sleep Quality during Pregnancy. The GESTAFIT Project. Nutrients 2020, 12, 3569. [Google Scholar] [CrossRef]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean Diet Pyramid Today. Science and Cultural Updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef]
- Dash, S.; Clarke, G.; Berk, M.; Jacka, F.N. The Gut Microbiome and Diet in Psychiatry: Focus on Depression. Curr. Opin. Psychiatry 2015, 28, 1–6. [Google Scholar] [CrossRef]
- Jacka, F.N.; Cherbuin, N.; Anstey, K.J.; Sachdev, P.; Butterworth, P. Western Diet Is Associated with a Smaller Hippocampus: A Longitudinal Investigation. BMC Med. 2015, 13, 215. [Google Scholar] [CrossRef]
- Bocchio-Chiavetto, L.; Bagnardi, V.; Zanardini, R.; Molteni, R.; Gabriela Nielsen, M.; Placentino, A.; Giovannini, C.; Rillosi, L.; Ventriglia, M.; Riva, M.A.; et al. Serum and Plasma BDNF Levels in Major Depression: A Replication Study and Meta-Analyses. World J. Biol. Psychiatry 2010, 11, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Kriengtuntiwong, T.; Zaw, Y.H.; Taneepanichskul, N. Brain-Derived Neurotrophic Factor (BDNF) Depression and Subjective Sleep Quality in the First Trimester of Pregnancy Among Migrant Workers in Thailand. J. Multidiscip. Healthc. 2021, 2549–2556. [Google Scholar] [CrossRef]
- Sánchez-Villegas, A.; Galbete, C.; Martinez-González, M.A.; Martinez, J.A.; Razquin, C.; Salas-Salvadó, J.; Estruch, R.; Buil-Cosiales, P.; Martí, A. The Effect of the Mediterranean Diet on Plasma Brain-Derived Neurotrophic Factor (BDNF) Levels: The PREDIMED-NAVARRA Randomized Trial. Nutr. Neurosci. 2013, 14, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Sinn, N.; Milte, C.; Howe, P.R.C. Oiling the Brain: A Review of Randomized Controlled Trials of Omega-3 Fatty Acids in Psychopathology across the Lifespan. Nutrients 2010, 2, 128–170. [Google Scholar] [CrossRef]
- Stahl, L.A.; Begg, D.P.; Weisinger, R.S.; Sinclair, A.J. The Role of Omega-3 Fatty Acids in Mood Disorders. Curr. Opin. Investig. Drugs 2008, 9, 57–64. [Google Scholar]
- Parletta, N.; Milte, C.M.; Meyer, B.J. Nutritional Modulation of Cognitive Function and Mental Health. J. Nutr. Biochem. 2013, 24, 725–743. [Google Scholar] [CrossRef]
- Nielsen-Scott, M.; Fellmeth, G.; Opondo, C.; Alderdice, F. Prevalence of Perinatal Anxiety in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2022, 306, 71–79. [Google Scholar] [CrossRef]
- Coelho, H.F.; Murray, L.; Royal-Lawson, M.; Cooper, P.J. Antenatal Anxiety Disorder as a Predictor of Postnatal Depression: A Longitudinal Study. J. Affect. Disord. 2011, 129, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Glasheen, C.; Richardson, G.A.; Fabio, A. A Systematic Review of the Effects of Postnatal Maternal Anxiety on Children. Arch. Womens Ment. Health 2010, 13, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Grigoriadis, S.; Graves, L.; Peer, M.; Mamisashvili, L.; Tomlinson, G.; Vigod, S.N.; Dennis, C.L.; Steiner, M.; Brown, C.; Cheung, A.; et al. A Systematic Review and Meta-Analysis of the Effects of Antenatal Anxiety on Postpartum Outcomes. Arch. Womens Ment. Health 2019, 22, 543–556. [Google Scholar] [CrossRef]
- Dennis, C.L.; Falah-Hassani, K.; Shiri, R. Prevalence of Antenatal and Postnatal Anxiety: Systematic Review and Meta-Analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E.; Berk, M. Early intervention comes late. Eur. Neuropsychopharmacol. 2022, 59, 1–3. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Usual Care | Mediterranean Diet | p Value |
|---|---|---|---|
| n = 349 | n = 331 | ||
| Age at recruitment (years) | 37.1 (33.3–40.5) | 37.3 (34.7–40.4) | 0.28 |
| Ethnicity | |||
| White | 281 (80.5%) | 269 (81.3%) | 0.80 |
| Latin | 50 (14.3%) | 44 (13.3%) | 0.70 |
| Afro-American | 6 (1.7%) | 5 (1.5%) | 0.83 |
| Asian | 6 (1.7%) | 7 (2.1%) | 0.70 |
| Others | 6 (1.7%) | 6 (1.8%) | 0.93 |
| Socio-economic status a | |||
| Low | 20 (5.7%) | 15 (4.5%) | 0.48 |
| Medium | 106 (30.4%) | 86 (26.0%) | 0.20 |
| High | 223 (63.9%) | 230 (69.5%) | 0.12 |
| BMI before pregnancy (Kg/m2) | 23.7 (4.8) | 24.0 (4.7) | 0.60 |
| BMI > 30 kg/m2 before pregnancy | 39 (11.2%) | 38 (11.5%) | 0.90 |
| Medical history before pregnancy | |||
| Autoimmune disease | 48 (13.8%) | 39 (11.8%) | 0.44 |
| Thyroid disorders | 20 (5.7%) | 29 (8.8%) | 0.13 |
| Chronic hypertension | 15 (4.3%) | 8 (2.4%) | 0.18 |
| Diabetes Mellitus | 12 (3.4%) | 16 (4.8%) | 0.36 |
| Psychiatric disorders | 11 (3.2%) | 8 (2.4%) | 0.56 |
| Chronic kidney disease | 5 (1.4%) | 6 (1.8%) | 0.70 |
| Obstetric history | |||
| Nulliparous | 143 (41.0%) | 145 (43.8%) | 0.46 |
| Previous placental disease | 68 (19.5%) | 66 (19.9%) | 0.88 |
| Previous preterm birth | 9 (2.6%) | 10 (3.0%) | 0.73 |
| Use of assisted reproductive technologies | 92 (26.4%) | 85 (25.7%) | 0.84 |
| Cigarette smoking during pregnancy | 28 (8.0%) | 22 (6.6%) | 0.49 |
| Alcohol intake during pregnancy | 8 (2.3%) | 4 (1.2%) | 0.27 |
| Drug consumption during pregnancy | 1 (0.3%) | 2 (0.6%) | 0.77 |
| Sports practice during pregnancy | 78 (22.3%) | 71 (21.5%) | 0.94 |
| Yoga or Pilates during pregnancy | 73 (20.9%) | 63 (19.0%) | 0.54 |
| Within-Group Mean Changes | p § | Between-Group Changes | |||
|---|---|---|---|---|---|
| Usual Care | MedDiet | MedDiet vs. Usual Care | |||
| n = 349 | n = 331 | Difference | |||
| (95% CI) | |||||
| Perceived stress scale score | Baseline † | 16.3 ± 7.8 | 15.9 ± 7.6 | ||
| Final ‡ | 17.0 ± 0.4 * | 15.9 ± 0.4 | 0.035 | −0.85 (−1.63 to −0.06) | |
| State-trait Anxiety Inventory (anxiety) | Baseline † | 14.1 ± 8.8 | 12.9 ± 8.3 | ||
| Final ‡ | 15.8 ± 0.5 ** | 13.6 ± 0.4 * | 0.004 | −1.35 (−2.28 to −0.43) | |
| State-trait Anxiety Inventory (personality) | Baseline † | 15.8. ± 9.0 | 14.2 ± 7.9 | ||
| Final ‡ | 15.8 ± 0.5 | 14.0 ± 0.5 | 0.100 | −0.68 (−1.48 to 0.13) | |
| WHO Five Well-being index | Baseline † | 62.7 ± 17.3 | 67.5 ± 15.2 | ||
| Final ‡ | 62.9 ± 0.9 | 66.6 ± 0.8 | 0.587 | 0.51 (−1.32 to 2.33) | |
| Pittsburgh Sleep Quality Index | Baseline † | 6.7 ± 2.4 | 6.4 ± 2.1 | ||
| Final ‡ | 7.9 ± 0.2 ** | 7.0 ± 0.2 ** | 0.001 | −0.73 (−1.15 to −0.31) | |
| FFMQ 1: Observation | Baseline † | 23.3 ± 5.9 | 24.2 ± 5.6 | ||
| Final ‡ | 24.0 ± 0.3 | 24.6 ± 0.3 | 0.729 | 0.12 (−0.57 to 0.81) | |
| FFMQ 2: Description | Baseline † | 32.1 ± 5.5 | 32.7 ± 4.8 | ||
| Final ‡ | 31.7 ± 0.3 | 32.4 ± 0.3 | 0.273 | 0.35 (−0.27 to 1.37) | |
| FFMQ 3: Awareness | Baseline † | 31.3 ± 6.0 | 31.3 ± 6.3 | ||
| Final ‡ | 30.6 ± 0.4 * | 30.0 ± 0.4 ** | 0.280 | −0.51 (−1.43 to 0.41) | |
| FFMQ 4: Non-judgmental | Baseline † | 29.9 ± 5.6 | 30.1 ± 5.2 | ||
| Final ‡ | 30.0 ± 0.3 | 30.0 ± 0.3 | 0.994 | 0.00 (−0.64 to 0.64) | |
| FFMQ 5: Non-reactivity | Baseline † | 22.5 ± 4.8 | 22.6 ± 4.8 | ||
| Final ‡ | 22.9 ± 0.2 | 22.5 ± 0.3 | 0.091 | −0.55 (−1.05 to 0.08) | |
| Final Scores | Usual Care | Mediterranean Diet | p Value |
|---|---|---|---|
| n = 349 | n = 331 | ||
| Perceived Stress Scale score > p75 | 85 (24.4%) | 80 (24.2%) | 0.96 |
| State-trait Anxiety Inventory (anxiety) score > p75 a | 82 (23.9%) | 75 (23.1%) | 0.82 |
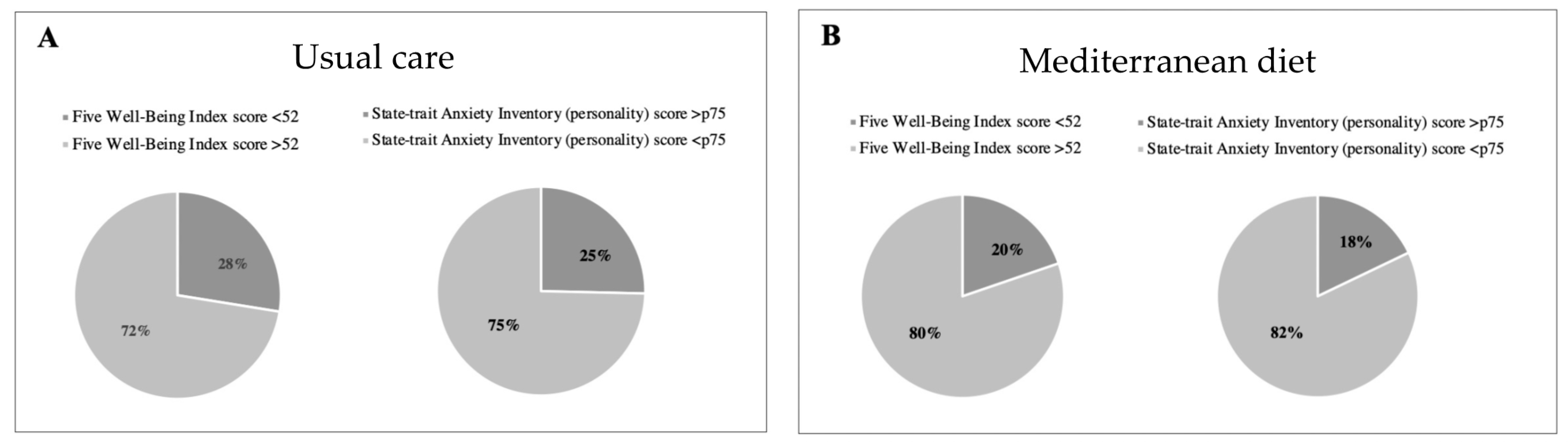
| State-trait Anxiety Inventory (personality) score > p75 a | 87 (25.4%) | 58 (17.9%) | 0.02 |
| WHO Five Well-Being Index score < 52 b | 95 (27.5%) | 65 (19.8%) | 0.02 |
| Pittsburgh Sleep Quality Index score > p75 c | 62 (21.8%) | 44 (16.8%) | 0.14 |
| Within-Group Mean Changes | p § | Between-Group Changes | |||
|---|---|---|---|---|---|
| Usual Care | MedDiet | MedDiet vs. Usual Care | |||
| n = 52 | n = 54 | Difference | |||
| (95% CI) | |||||
| Total Cortisone/Total Cortisol | Baseline † | 1.0 ± 0.6 | 1.2 ± 0.8 | ||
| Final ‡ | 1.3 ± 0.1 ** | 1.7 ± 0.1 ** | 0.015 | 0.26 (0.05 to 0.47) | |
| Total cortisol | Baseline † | 89.9 ± 42.6 | 81.6 ± 36.1 | ||
| Final ‡ | 89.8 ± 4.8 | 84.9 ± 5.3 | 0.619 | 2.66 (−7.83 to 13.16) | |
| Total cortisol % | Baseline † | 2.0 ± 0.8 | 2.0 ± 0.8 | ||
| Final ‡ | 2.1 ± 0.1 | 2.0 ± 0.1 | 0.536 | −0.08 (−0.33 to 0.17) | |
| 5β-tetrahydrocortisol | Baseline † | 823.1 ± 419.3 | 734.4 ± 304.2 | ||
| Final ‡ | 777.8 ± 54.6 | 766.3 ± 55.3 | 0.279 | 64.9 (−52.60 to 182.42) | |
| 5β-THF/Cortisol | Baseline † | 10.0 ± 5.2 | 10.9 ± 5.0 | ||
| Final ‡ | 9.1 ± 0.6 | 9.6 ± 0.7 | 0.774 | 0.19 (−1.13 to 1.52) | |
| Total cortisone | Baseline † | 85.6 ± 52.5 | 87.0 ± 50.1 | ||
| Final ‡ | 111.5 ± 7.7 * | 134.7 ± 8.3 ** | 0.012 | 24.3 (5.45 to 43.3) | |
| Total cortisone % | Baseline † | 1.9 ± 1.0 | 1.9 ± 0.7 | ||
| Final ‡ | 2.4 ± 0.1 ** | 2.9 ± 0.1 ** | 0.002 | 0.47 (0.18 to 0.78) | |
| 5β-tetrahydrocortisone % | Baseline † | 2185.2 ± 1189.3 | 1961.1 ± 973.2 | ||
| Final ‡ | 2209.3 ± 171.2 | 2196.5 ± 184.4 | 0.627 | 111.0 (−336.96 to 558.99) | |
| 5β-THE/Cortisone | Baseline † | 29.8 ± 15.5 | 26.3 ± 14.8 | ||
| Final ‡ | 21.4 ± 1.4 ** | 16.8 ± 1.2 ** | 0.032 | −3.39 (−6.49 to −0.30) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casas, I.; Nakaki, A.; Pascal, R.; Castro-Barquero, S.; Youssef, L.; Genero, M.; Benitez, L.; Larroya, M.; Boutet, M.L.; Casu, G.; et al. Effects of a Mediterranean Diet Intervention on Maternal Stress, Well-Being, and Sleep Quality throughout Gestation—The IMPACT-BCN Trial. Nutrients 2023, 15, 2362. https://doi.org/10.3390/nu15102362
Casas I, Nakaki A, Pascal R, Castro-Barquero S, Youssef L, Genero M, Benitez L, Larroya M, Boutet ML, Casu G, et al. Effects of a Mediterranean Diet Intervention on Maternal Stress, Well-Being, and Sleep Quality throughout Gestation—The IMPACT-BCN Trial. Nutrients. 2023; 15(10):2362. https://doi.org/10.3390/nu15102362
Chicago/Turabian StyleCasas, Irene, Ayako Nakaki, Rosalia Pascal, Sara Castro-Barquero, Lina Youssef, Mariona Genero, Leticia Benitez, Marta Larroya, Maria Laura Boutet, Giulia Casu, and et al. 2023. "Effects of a Mediterranean Diet Intervention on Maternal Stress, Well-Being, and Sleep Quality throughout Gestation—The IMPACT-BCN Trial" Nutrients 15, no. 10: 2362. https://doi.org/10.3390/nu15102362
APA StyleCasas, I., Nakaki, A., Pascal, R., Castro-Barquero, S., Youssef, L., Genero, M., Benitez, L., Larroya, M., Boutet, M. L., Casu, G., Gomez-Gomez, A., Pozo, O. J., Morilla, I., Martínez-Àran, A., Vieta, E., Gómez-Roig, M. D., Casas, R., Estruch, R., Gratacos, E., ... Crovetto, F. (2023). Effects of a Mediterranean Diet Intervention on Maternal Stress, Well-Being, and Sleep Quality throughout Gestation—The IMPACT-BCN Trial. Nutrients, 15(10), 2362. https://doi.org/10.3390/nu15102362