
Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies



 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection-Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment of Included Studies
2.5. Statistical Analysis
3. Results
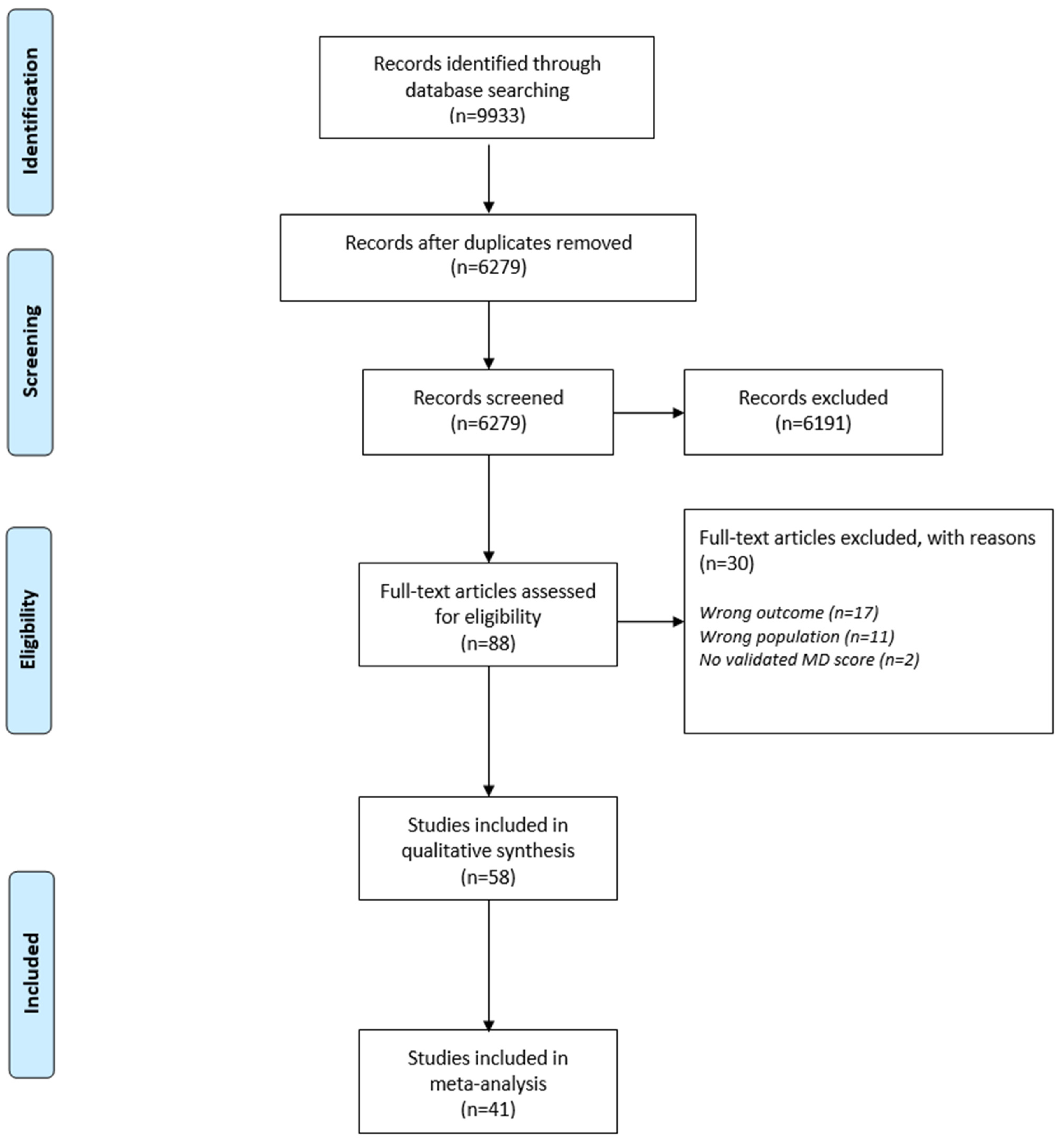
3.1. Search Results
3.2. Quality Assessment
3.3. Publication Bias
3.4. Study Characteristics
3.5. Result on Components of MetS
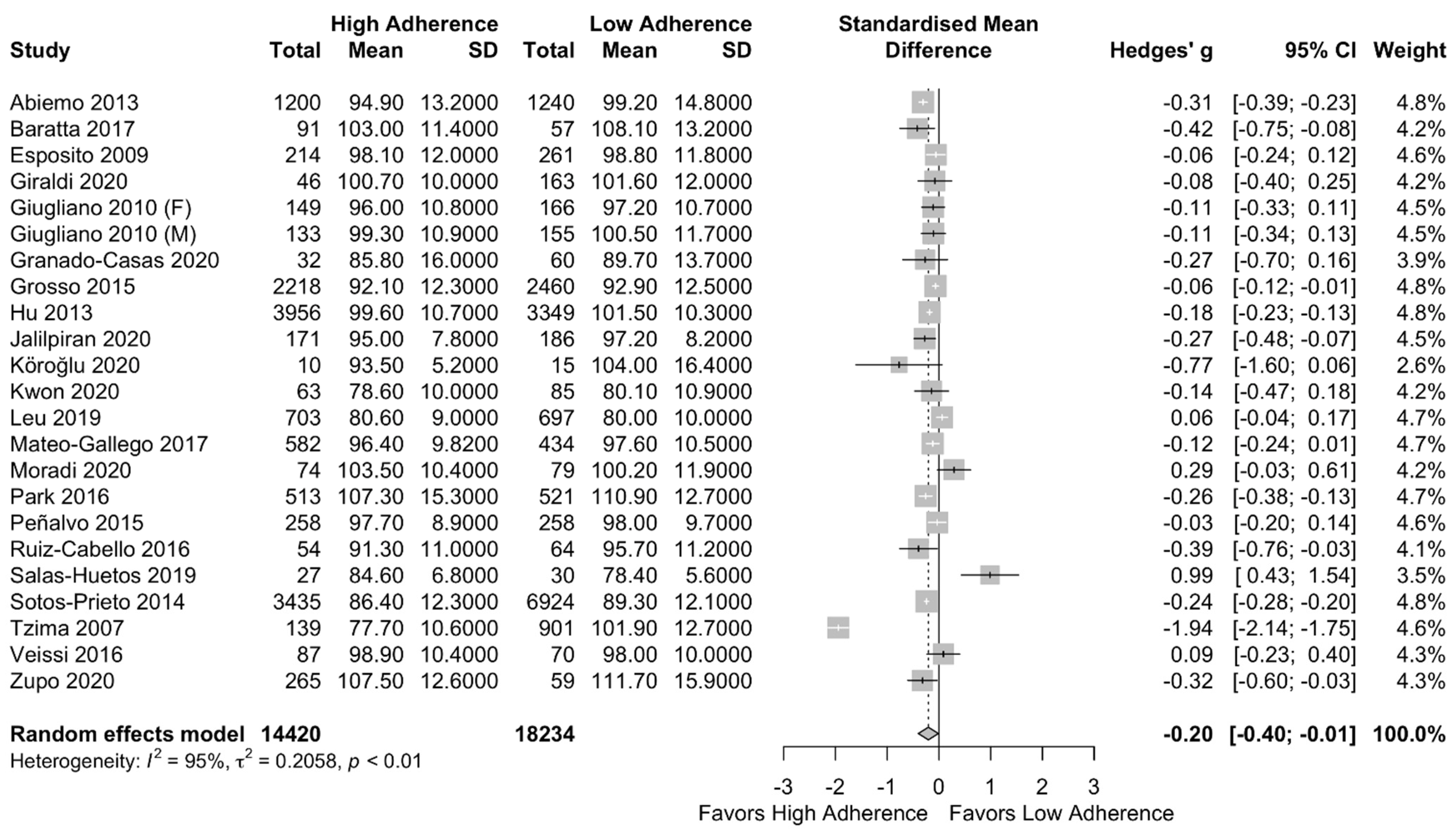
3.5.1. Waist Circumference (WC)
3.5.2. HDL Cholesterol
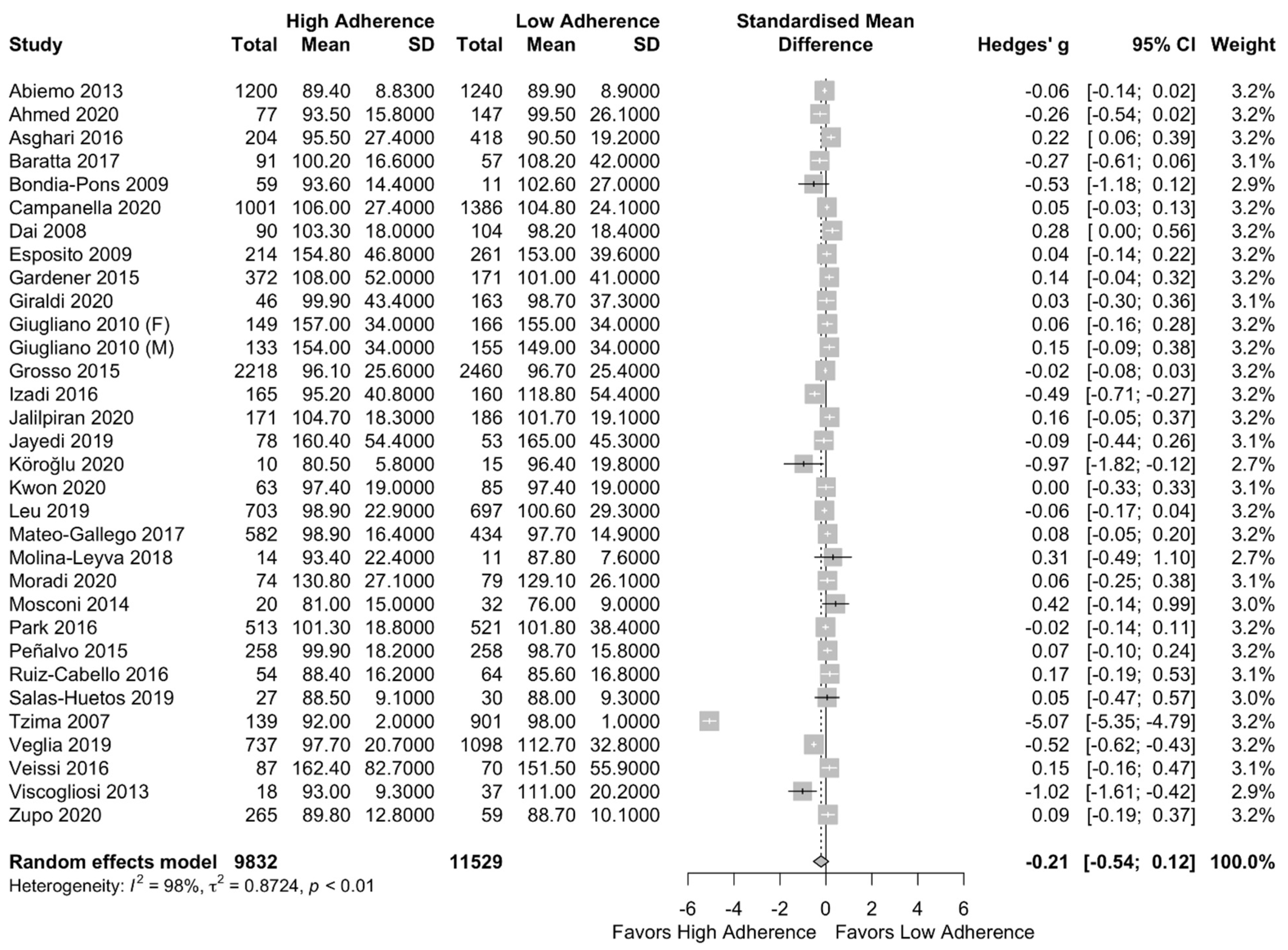
3.5.3. Serum Triglycerides
3.5.4. Fasting Blood Glucose
3.5.5. Systolic Blood Pressure (SBP)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BP | Blood Pressure |
| CI | Confidence Interval |
| CVD | Cardiovascular Disease |
| DBP | Diastolic Blood Pressure |
| FFQs | Food Frequency Questionnaires |
| FG | Fasting Glucose |
| GLP-1 | Glucagon-Like Peptide-1 |
| HbA1c | Glycohemoglobin |
| HDL | High-Density Lipoprotein |
| IDF | International Diabetes Federation |
| MD | Mediterranean Diet |
| MDS | Mediterranean Diet Score |
| MEDAS | Mediterranean Diet Adherence Screener |
| MetS | Metabolic Syndrome |
| MSDPS | Mediterranean-Style Dietary Pattern Score |
| MOOSE | Meta-analyses Of Observational Studies in Epidemiology |
| N-3 FAs | Omga-3-Fatty Acids |
| NAFLD | Non-Alcoholic Fatty Liver Disease |
| NCDs | Non-Communicable Diseases |
| NCEP ATP III | National Cholesterol Program in Adult Treatment Panel III |
| NHNES | National Health and Nutrition Examination Survey |
| NOS | New Castle Ottawa Scale |
| OR | Odds Ration |
| RCT | Randomized Controlled Trial |
| SD | Standard Deviation |
| SBP | Systolic Blood Pressure |
| SMD | Standardized Mean Difference |
| T2DM | Type 2 Diabetes Mellitus |
| TG | Triglycerides |
| UK | United Kingdom |
| US | United States |
| WC | Waist Circumference |
| WHO | World Health Organization |
References
- Cordain, L.; Eaton, S.B.; Sebastian, A.; Mann, N.; Lindeberg, S.; Watkins, B.A.; O’Keefe, J.H.; Brand-Miller, J. Origins and evolution of the Western diet: Health implications for the 21st century. Am. J. Clin. Nutr. 2005, 81, 341–354. [Google Scholar] [CrossRef]
- Misra, A.; Khurana, L. Obesity and the Metabolic Syndrome in Developing Countries. J. Clin. Endocrinol. Metab. 2008, 93 (Suppl. 1), s9–s30. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.X.; Chaudhary, N.; Akinyemiju, T. Metabolic Syndrome Prevalence by Race/Ethnicity and Sex in the United States, National Health and Nutrition Examination Survey, 1988–2012. Prev. Chronic Dis. 2017, 14, E24. [Google Scholar] [CrossRef] [PubMed]
- van Vliet-Ostaptchouk, J.V.; Nuotio, M.L.; Slagter, S.N.; Doiron, D.; Fischer, K.; Foco, L.; Gaye, A.; Gögele, M.; Heier, M.; Hiekkalinna, T.; et al. The prevalence of metabolic syndrome and metabolically healthy obesity in Europe: A collaborative analysis of ten large cohort studies. BMC Endocr. Disord. 2014, 14, 9. [Google Scholar] [CrossRef]
- Kassi, E.; Pervanidou, P.; Kaltsas, G.; Chrousos, G. Metabolic syndrome: Definitions and controversies. BMC Med. 2011, 9, 48. [Google Scholar] [CrossRef]
- Pérez-Martínez, P.; Mikhailidis, D.P.; Athyros, V.G.; Bullo, M.; Couture, P.; Covas, M.I.; De Koning, L.; Delgado-Lista, J.; Díaz-López, A.; Drevon, C.A.; et al. Lifestyle recommendations for the prevention and management of metabolic syndrome: An international panel recommendation. Nutr. Rev. 2017, 75, 307–326. [Google Scholar] [CrossRef] [PubMed]
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef]
- Steckhan, N.; Hohmann, C.-D.; Kessler, C.; Dobos, G.; Michalsen, A.; Cramer, H. Effects of different dietary approaches on inflammatory markers in patients with metabolic syndrome: A systematic review and meta-analysis. Nutrients 2016, 32, 338–348. [Google Scholar] [CrossRef] [PubMed]
- Gami, A.S.; Witt, B.J.; Howard, D.E.; Erwin, P.J.; Gami, L.A.; Somers, V.K.; Montori, V.M. Metabolic syndrome and risk of incident cardiovascular events and death: A systematic review and meta-analysis of longitudinal studies. J. Am. Coll. Cardiol. 2007, 49, 403–414. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- National Cholesterol Education Program (U.S.). Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. In Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III); The Program: Berkeley, CA, USA, 2002. [Google Scholar]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic syndrome-a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Hoyas, I.; Leon-Sanz, M. Nutritional Challenges in Metabolic Syndrome. J. Clin. Med. 2019, 8, 1301. [Google Scholar] [CrossRef] [PubMed]
- Lăcătușu, C.-M.; Grigorescu, E.-D.; Floria, M.; Onofriescu, A.; Mihai, B.-M. The Mediterranean Diet: From an Environment-Driven Food Culture to an Emerging Medical Prescription. Int. J. Environ. Res. Public Health 2019, 16, 942. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Murphy, K.J. Definition of the Mediterranean Diet—A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Lagiou, P. Healthy Traditional Mediterranean Diet: An Expression of Culture, History, and Lifestyle. Nutr. Rev. 1997, 55, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Zaragoza-Martí, A.; Cabañero-Martínez, M.J.; Hurtado-Sánchez, J.A.; Laguna-Pérez, A.; Ferrer-Cascales, R. Evaluation of Mediterranean diet adherence scores: A systematic review. BMJ Open 2018, 8, e019033. [Google Scholar] [CrossRef] [PubMed]
- Bamia, C.; Martimianaki, G.; Kritikou, M.; Trichopoulou, A. Indexes for Assessing Adherence to a Mediterranean Diet from Data Measured through Brief Questionnaires: Issues Raised from the Analysis of a Greek Population Study. Curr. Dev. Nutr. 2017, 1, e000075. [Google Scholar] [CrossRef]
- A Benítez-Arciniega, A.; Mendez, M.A.; Baena-Díez, J.M.; Martori, M.-A.R.; Soler, C.; Marrugat, J.; Covas, M.-I.; Sanz, H.; Llopis, A.; Schröder, H. Concurrent and construct validity of Mediterranean diet scores as assessed by an FFQ. Public Health Nutr. 2011, 14, 2015–2021. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Martínez-González, M.; García-López, M.; Bes-Rastrollo, M.; Toledo, E.; Martínez-Lapiscina, E.; Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J. Mediterranean diet and the incidence of cardiovascular disease: A Spanish cohort. Nutr. Metab. Cardiovasc. Dis. 2010, 21, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Tognon, G.; Lissner, L.; Sæbye, D.; Walker, K.Z.; Heitmann, B.L. The Mediterranean diet in relation to mortality and CVD: A Danish cohort study. Br. J. Nutr. 2013, 111, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.; Georgousopoulou, E.; Pitsavos, C.; Chrysohoou, C.; Skoumas, I.; Pitaraki, E.; Georgiopoulos, G.; Ntertimani, M.; Christou, A.; Stefanadis, C. Exploring the path of Mediterranean diet on 10-year incidence of cardiovascular disease: The ATTICA study (2002–2012). Nutr. Metab. Cardiovasc. Dis. 2015, 25, 327–335. [Google Scholar] [CrossRef]
- Martínez-González, M.Á.; De La Fuente-Arrillaga, C.; Nunez-Cordoba, J.M.; Basterra-Gortari, F.J.; Beunza, J.J.; Vazquez, Z.; Benito, S.; Tortosa, A.; Bes-Rastrollo, M. Adherence to Mediterranean diet and risk of developing diabetes: Prospective cohort study. BMJ 2008, 336, 1348–1351. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Missbach, B.; König, J.; Hoffmann, G. Adherence to a Mediterranean diet and risk of diabetes: A systematic review and meta-analysis. Public Health Nutr. 2015, 18, 1292–1299. [Google Scholar] [CrossRef]
- Franquesa, M.; Pujol-Busquets, G.; García-Fernández, E.; Rico, L.; Shamirian-Pulido, L.; Aguilar-Martínez, A.; Medina, F.-X.; Serra-Majem, L.; Bach-Faig, A. Mediterranean Diet and Cardiodiabesity: A Systematic Review through Evidence-Based Answers to Key Clinical Questions. Nutrients 2019, 11, 655. [Google Scholar] [CrossRef]
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean Diet, its Components, and Cardiovascular Disease. Am. J. Med. 2015, 128, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Zappalà, G.; Bernardini, S.; Giambini, I.; Bes-Rastrollo, M.; Martinez-Gonzalez, M. Adherence to the Mediterranean diet is inversely associated with metabolic syndrome occurrence: A meta-analysis of observational studies. Int. J. Food Sci. Nutr. 2017, 68, 138–148. [Google Scholar] [CrossRef]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: A Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- A Martínez-González, M.; Fernández-Jarne, E.; Serrano-Martínez, M.; Wright, M.; Gomez-Gracia, E. Development of a short dietary intake questionnaire for the quantitative estimation of adherence to a cardioprotective Mediterranean diet. Eur. J. Clin. Nutr. 2004, 58, 1550–1552. [Google Scholar] [CrossRef] [PubMed]
- Monteagudo, C.; Mariscal-Arcas, M.; Rivas, A.; Lorenzo-Tovar, M.L.; Tur, J.A.; Olea-Serrano, F. Proposal of a Mediterranean Diet Serving Score. PLoS ONE 2015, 10, e0128594. [Google Scholar]
- Rumawas, M.E.; Dwyer, J.T.; McKeown, N.M.; Meigs, J.B.; Rogers, G.; Jacques, P.F. The Development of the Mediterranean-Style Dietary Pattern Score and Its Application to the American Diet in the Framingham Offspring Cohort. J. Nutr. 2009, 139, 1150–1156. [Google Scholar] [CrossRef]
- Patterson, R.E.; Haines, P.S.; Popkin, B.M. Diet quality index: Capturing a multidimensional behavior. J. Am. Diet. Assoc. 1994, 94, 57–64. [Google Scholar] [CrossRef]
- Buckland, G.; González, C.A.; Agudo, A.; Vilardell, M.; Berenguer, A.; Amiano, P.; Ardanaz, E.; Arriola, L.; Barricarte, A.; Basterretxea, M.; et al. Adherence to the Mediterranean Diet and Risk of Coronary Heart Disease in the Spanish EPIC Cohort Study. Am. J. Epidemiol. 2009, 170, 1518–1529. [Google Scholar] [CrossRef] [PubMed]
- León, E.Á.; Henríquez, P.; Serra-Majem, L. Mediterranean diet and metabolic syndrome: A cross-sectional study in the Canary Islands. Public Health Nutr. 2006, 9, 1089–1098. [Google Scholar] [CrossRef]
- Huang, X.; Jiménez-Moleón, J.J.; Lindholm, B.; Cederholm, T.; Ärnlöv, J.; Risérus, U.; Sjögren, P.; Carrero, J.J. Mediterranean Diet, Kidney Function, and Mortality in Men with CKD. Clin. J. Am. Soc. Nephrol. 2013, 8, 1548–1555. [Google Scholar] [CrossRef]
- Fung, T.T.; McCullough, M.L.; Newby, P.; Manson, J.E.; Meigs, J.B.; Rifai, N.; Willett, W.C.; Hu, F.B. Diet-quality scores and plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2005, 82, 163–173. [Google Scholar] [CrossRef]
- Sánchez-Villegas, A.; Martínez, J.A.; De Irala, J.; Martínez-González, M.A. Determinants of the adherence to an “a priori” defined Mediterranean dietary pattern. Eur. J. Nutr. 2002, 41, 249–257. [Google Scholar] [CrossRef]
- Yang, J.; Farioli, A.; Korre, M.; Kales, S.N. Modified Mediterranean Diet Score and Cardiovascular Risk in a North American Working Population. PLoS ONE 2014, 9, e87539. [Google Scholar] [CrossRef] [PubMed]
- Steffen, L.M.; Van Horn, L.; Daviglus, M.L.; Zhou, X.; Reis, J.P.; Loria, C.M.; Jacobs, D.R.; Duffey, K.J. A modified Mediterranean diet score is associated with a lower risk of incident metabolic syndrome over 25 years among young adults: The CARDIA (Coronary Artery Risk Development in Young Adults) study. Br. J. Nutr. 2014, 112, 1654–1661. [Google Scholar] [CrossRef] [PubMed]
- Abiemo, E.E.; Alonso, A.; Nettleton, J.A.; Steffen, L.M.; Bertoni, A.G.; Jain, A.; Lutsey, P.L. Relationships of the Mediterranean dietary pattern with insulin resistance and diabetes incidence in the Multi-Ethnic Study of Atherosclerosis (MESA). Br. J. Nutr. 2012, 109, 1490–1497. [Google Scholar] [CrossRef]
- Grosso, G.; Stepaniak, U.; Micek, A.; Topor-Mądry, R.; Stefler, D.; Szafraniec, K.; Bobak, M.; Pająk, A. A Mediterranean-type diet is associated with better metabolic profile in urban Polish adults: Results from the HAPIEE study. Metabolism 2015, 64, 738–746. [Google Scholar] [CrossRef]
- Veglia, F.; Baldassarre, D.; De Faire, U.; Kurl, S.; Smit, A.J.; Rauramaa, R.; Giral, P.; Amato, M.; Di Minno, A.; Ravani, A.; et al. A priori-defined Mediterranean-like dietary pattern predicts cardiovascular events better in north Europe than in Mediterranean countries. Int. J. Cardiol. 2019, 282, 88–92. [Google Scholar] [CrossRef]
- Martín-Peláez, S.; Fito, M.; Castaner, O. Mediterranean Diet Effects on Type 2 Diabetes Prevention, Disease Progression, and Related Mechanisms. A Review. Nutrients 2020, 12, 2236. [Google Scholar] [CrossRef]
- Vitale, M.; Masulli, M.; Calabrese, I.; Rivellese, A.A.; Bonora, E.; Signorini, S.; Perriello, G.; Squatrito, S.; Buzzetti, R.; Sartore, G.; et al. Impact of a Mediterranean Dietary Pattern and Its Components on Cardiovascular Risk Factors, Glucose Control, and Body Weight in People with Type 2 Diabetes: A Real-Life Study. Nutrients 2018, 10, 1067. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of non Randomised Studies in Meta-Analyses; University of Liverpool: Liverpool, UK, 2000. [Google Scholar]
- Cox, D.R.; Snell, E.J. Analysis of Binary Data; CRC Press: Boca Raton, FL, USA, 1989. [Google Scholar]
- da Costa, B.R.; Rutjes, A.W.; Johnston, B.C.; Reichenbach, S.; Nüesch, E.; Tonia, T.; Gemperli, A.; Guyatt, G.H.; Jüni, P. Methods to convert continuous outcomes into odds ratios of treatment response and numbers needed to treat: Meta-epidemiological study. Int. J. Epidemiol. 2012, 41, 1445–1459. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [PubMed]
- Omni Calculator. Available online: https://www.omnicalculator.com/ (accessed on 5 March 2021).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Moorthy, M.V.; Demler, O.V.; Hu, F.B.; Ridker, P.M.; Chasman, D.I.; Mora, S. Assessment of Risk Factors and Biomarkers Associated With Risk of Cardiovascular Disease Among Women Consuming a Mediterranean Diet. JAMA Netw. Open 2018, 1, e185708. [Google Scholar] [CrossRef]
- Ahmed, F.S.; Wade, A.T.; Guenther, B.A.; Murphy, K.J.; Elias, M.F. Adherence to a Mediterranean diet associated with lower blood pressure in a US sample: Findings from the Maine-Syracuse Longitudinal Study. J. Clin. Hypertens. 2020, 22, 2276–2284. [Google Scholar] [CrossRef] [PubMed]
- Asghari, G.; Farhadnejad, H.; Mirmiran, P.; Dizavi, A.; Yuzbashian, E.; Azizi, F. Adherence to the Mediterranean diet is associated with reduced risk of incident chronic kidney diseases among Tehranian adults. Hypertens. Res. 2017, 40, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Baratta, F.; Pastori, D.; Polimeni, L.; Bucci, T.; Ceci, F.; Calabrese, C.; Ernesti, I.; Pannitteri, G.; Violi, F.; Angelico, F.; et al. Adherence to Mediterranean Diet and Non-Alcoholic Fatty Liver Disease: Effect on Insulin Resistance. Am. J. Gastroenterol. 2017, 112, 1832–1839. [Google Scholar] [CrossRef] [PubMed]
- Bondia-Pons, I.; Mayneris-Perxachs, J.; Serra-Majem, L.; Castellote, A.I.; Mariné, A.; López-Sabater, M.C. Diet quality of a population sample from coastal north-east Spain evaluated by a Mediterranean adaptation of the Diet Quality Index (DQI). Public Health Nutr. 2009, 13, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Campanella, A.; Misciagna, G.; Mirizzi, A.; Caruso, M.G.; Bonfiglio, C.; Aballay, L.R.; Silveira, L.V.D.A.; Bianco, A.; Franco, I.; Sorino, P.; et al. The effect of the Mediterranean Diet on lifespan: A treatment-effect survival analysis of a population-based prospective cohort study in Southern Italy. Int. J. Epidemiol. 2021, 50, 245–255. [Google Scholar] [CrossRef]
- Dai, J.; Miller, A.H.; Bremner, J.D.; Goldberg, J.; Jones, L.; Shallenberger, L.; Buckham, R.; Murrah, N.V.; Veledar, E.; Wilson, P.W.; et al. Adherence to the mediterranean diet is inversely associated with circulating interleukin-6 among middle-aged men: A twin study. Circulation 2008, 117, 169–175. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Di Palo, C.; Giugliano, D.; Campanian Postprandial Hyperglycemia Study Group. Adherence to a Mediterranean diet and glycaemic control in Type 2 diabetes mellitus. Diabet. Med. 2009, 26, 900–907. [Google Scholar] [CrossRef] [PubMed]
- Gardener, H.; Wright, C.B.; Cabral, D.; Scarmeas, N.; Gu, Y.; Cheung, K.; Elkind, M.S.; Sacco, R.L.; Rundek, T. Mediterranean diet and carotid atherosclerosis in the Northern Manhattan Study. Atheroscler. 2014, 234, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Giraldi, L.; Miele, L.; Aleksovska, K.; Manca, F.; Leoncini, E.; Biolato, M.; Arzani, D.; Pirro, M.A.; Marrone, G.; Cefalo, C.; et al. Mediterranean diet and the prevention of non-alcoholic fatty liver disease: Results from a case-control study. Eur. Rev. Med Pharmacol. Sci. 2020, 24, 7391–7398. [Google Scholar] [PubMed]
- Giugliano, F.; Maiorino, M.I.; Bellastella, G.; Autorino, R.; De Sio, M.; Giugliano, D.; Esposito, K. ERECTILE DYSFUNCTION: Adherence to Mediterranean Diet and Erectile Dysfunction in Men with Type 2 Diabetes. J. Sex. Med. 2010, 7, 1911–1917. [Google Scholar] [CrossRef]
- Giugliano, F.; Maiorino, M.I.; Di Palo, C.; Autorino, R.; De Sio, M.; Giugliano, D.; Esposito, K. ORIGINAL RESEARCH—WOMEN’S SEXUAL HEALTH: Adherence to Mediterranean Diet and Sexual Function in Women with Type 2 Diabetes. J. Sex. Med. 2010, 7, 1883–1890. [Google Scholar] [CrossRef]
- Granado-Casas, M.; Martin, M.; Martínez-Alonso, M.; Alcubierre, N.; Hernández, M.; Alonso, N.; Castelblanco, E.; Mauricio, D. The Mediterranean Diet is Associated with an Improved Quality of Life in Adults with Type 1 Diabetes. Nutrients 2020, 12, 131. [Google Scholar] [CrossRef]
- Hu, E.; Toledo, E.; Diez-Espino, J.; Estruch, R.; Corella, D.; Salas-Salvado, J.; Vinyoles, E.; Gomez-Gracia, E.; Aros, F.; Fiol, M.; et al. Lifestyles and risk factors associated with baseline adherence to the mediterranean diet in the predimed trial. Ann. Nutr. Metab. 2013, 63 (Suppl. 1), 912. [Google Scholar] [CrossRef]
- Izadi, V.; Tehrani, H.; Haghighatdoost, F.; Dehghan, A.; Surkan, P.J.; Azadbakht, L. Adherence to the DASH and Mediterranean diets is associated with decreased risk for gestational diabetes mellitus. Nutrients 2016, 32, 1092–1096. [Google Scholar] [CrossRef]
- Jalilpiran, Y.; Mofrad, M.D.; Mozaffari, H.; Bellissimo, N.; Azadbakht, L. Adherence to dietary approaches to stop hypertension (DASH) and Mediterranean dietary patterns in relation to cardiovascular risk factors in older adults. Clin. Nutr. ESPEN 2020, 39, 87–95. [Google Scholar] [CrossRef]
- Jayedi, A.; Mirzaei, K.; Rashidy-Pour, A.; Yekaninejad, M.S.; Zargar, M.-S.; Eidgahi, M.R.A. Dietary approaches to stop hypertension, mediterranean dietary pattern, and diabetic nephropathy in women with type 2 diabetes: A case-control study. Clin. Nutr. ESPEN 2019, 33, 164–170. [Google Scholar] [CrossRef]
- Köroğlu, Ö.; Adıgüzel, K.T. Cardiometabolic risk parameters of individuals with lower extremity amputation: What is the effect of adherence to DASH diet and Mediterranean diet? Turk. J. Phys. Med. Rehabil. 2020, 66, 291–298. [Google Scholar] [CrossRef]
- Kwon, Y.-J.; Lee, H.; Yoon, Y.; Kim, H.M.; Chu, S.H.; Lee, J.-W. Development and Validation of a Questionnaire to Measure Adherence to the Mediterranean Diet in Korean Adults. Nutrients 2020, 12, 1102. [Google Scholar] [CrossRef]
- Lavados, P.M.; Mazzon, E.; Rojo, A.; Brunser, A.M.; Olavarría, V.V. Pre-stroke adherence to a Mediterranean diet pattern is associated with lower acute ischemic stroke severity: A cross-sectional analysis of a prospective hospital-register study. BMC Neurol. 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Leu, H.-B.; Chung, C.-M.; Chen, J.-W.; Pan, W.-H. The Mediterranean diet reduces the genetic risk of chromosome 9p21 for myocardial infarction in an Asian population community cohort. Sci. Rep. 2019, 9, 1–8. [Google Scholar] [CrossRef]
- Mateo-Gallego, R.; Uzhova, I.; Moreno-Franco, B.; León-Latre, M.; Casasnovas, J.A.; Laclaustra, M.; Peñalvo, J.L.; Civeira, F. Adherence to a Mediterranean diet is associated with the presence and extension of atherosclerotic plaques in middle-aged asymptomatic adults: The Aragon Workers’ Health Study. J. Clin. Lipidol. 2017, 11, 1372–1382.e4. [Google Scholar] [CrossRef] [PubMed]
- Molina-Leyva, A.; Cuenca-Barrales, C.; Vega-Castillo, J.; Ruiz-Carrascosa, J.; Ruiz-Villaverde, R. Adherence to Mediterranean diet in Spanish patients with psoriasis: Cardiovascular benefits? Dermatol. Ther. 2019, 32, e12810. [Google Scholar] [CrossRef] [PubMed]
- Moradi, M.; Daneshzad, E.; Najafabadi, M.M.; Bellissimo, N.; Suitor, K.; Azadbakht, L. Association between adherence to the Mediterranean diet and renal function biomarkers and cardiovascular risk factors among diabetic patients with nephropathy. Clin. Nutr. ESPEN 2020, 40, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Mosconi, L.; Murray, J.; Tsui, W.H.; Li, Y.; Davies, M.; Williams, S.; Pirraglia, E.; Spector, N.; Osorio, R.S.; Glodzik, L.; et al. Mediterranean Diet and Magnetic Resonance Imaging-Assessed Brain Atrophy in Cognitively Normal Individuals at Risk for Alzheimer’s Disease. J. Prev. Alzheimers Dis. 2014, 1, 23–32. [Google Scholar]
- Park, Y.-M.; Steck, S.E.; Fung, T.T.; Zhang, J.; Hazlett, L.J.; Han, K.; Merchant, A.T. Mediterranean diet and mortality risk in metabolically healthy obese and metabolically unhealthy obese phenotypes. Int. J. Obes. 2016, 40, 1541–1549. [Google Scholar] [CrossRef]
- Peñalvo, J.L.; Oliva, B.; Sotos-Prieto, M.; Uzhova, I.; Moreno-Franco, B.; León-Latre, M.; Ordovás, J.M. Greater Adherence to a Mediterranean Dietary Pattern Is Associated With Improved Plasma Lipid Profile: The Aragon Health Workers Study Cohort. Revista Española de Cardiología (English Edition) 2015, 68, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Pocovi-Gerardino, G.; Correa-Rodríguez, M.; Callejas-Rubio, J.-L.; Ríos-Fernández, R.; Martín-Amada, M.; Cruz-Caparros, M.-G.; Rueda-Medina, B.; Ortego-Centeno, N. Beneficial effect of Mediterranean diet on disease activity and cardiovascular risk in systemic lupus erythematosus patients: A cross-sectional study. Rheumatology 2021, 60, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Cabello, P.; Coll-Risco, I.; Acosta-Manzano, P.; Borges-Cosic, M.; Gallo-Vallejo, F.; Aranda, P.; López-Jurado, M.; Aparicio, V. Influence of the degree of adherence to the Mediterranean diet on the cardiometabolic risk in peri and menopausal women. The Flamenco project. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Salas-Huetos, A.; Babio, N.; Carrell, D.T.; Bulló, M.; Salas-Salvadó, J. Adherence to the Mediterranean diet is positively associated with sperm motility: A cross-sectional analysis. Sci. Rep. 2019, 9, 3389. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Luben, R.; Khaw, K.-T.; Wareham, N.J.; Forouhi, N.G. The association between Mediterranean Diet Score and glucokinase regulatory protein gene variation on the markers of cardiometabolic risk: An analysis in the European Prospective Investigation into Cancer (EPIC)-Norfolk study. Br. J. Nutr. 2014, 112, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Casuccio, A.; Buttà, C.; Pecoraro, R.; Di Raimondo, D.; Della Corte, V.; Arnao, V.; Clemente, G.; Maida, C.; Simonetta, I.; et al. Mediterranean Diet in patients with acute ischemic stroke: Relationships between Mediterranean Diet score, diagnostic subtype, and stroke severity index. Atherosclerosis 2015, 243, 260–267. [Google Scholar] [CrossRef]
- Tuttolomondo, A.; Di Raimondo, D.; Casuccio, A.; Velardo, M.; Salamone, G.; Cataldi, M.; Corpora, F.; Restivo, V.; Pecoraro, R.; Della Corte, V.; et al. Mediterranean diet adherence and congestive heart failure: Relationship with clinical severity and ischemic pathogenesis. Nutrition 2020, 70, 110584. [Google Scholar] [CrossRef]
- Tzima, N.; Pitsavos, C.; Panagiotakos, D.B.; Skoumas, J.; Zampelas, A.; Chrysohoou, C.; Stefanadis, C. Mediterranean diet and insulin sensitivity, lipid profile and blood pressure levels, in overweight and obese people; The Attica study. Lipids Health Dis. 2007, 6, 22. [Google Scholar] [CrossRef]
- Veissi, M.; Anari, R.; Amani, R.; Shahbazian, H.; Latifi, S.M. Mediterranean diet and metabolic syndrome prevalence in type 2 diabetes patients in Ahvaz, southwest of Iran. Diabetes Metab. Syndr. Clin. Res. Rev. 2016, 10, S26–S29. [Google Scholar] [CrossRef]
- Viscogliosi, G.; Cipriani, E.; Liguori, M.L.; Marigliano, B.; Saliola, M.; Ettorre, E.; Andreozzi, P. Mediterranean Dietary Pattern Adherence: Associations with Prediabetes, Metabolic Syndrome, and Related Microinflammation. Metab. Syndr. Relat. Disord. 2013, 11, 210–216. [Google Scholar] [CrossRef]
- Zupo, R.; Castellana, F.; Panza, F.; Lampignano, L.; Murro, I.; Di Noia, C.; Triggiani, V.; Giannelli, G.; Sardone, R.; De Pergola, G. Adherence to a Mediterranean Diet and Thyroid Function in Obesity: A Cross-Sectional Apulian Survey. Nutrients 2020, 12, 3173. [Google Scholar] [CrossRef]
- Aridi, Y.S.; Walker, J.L.; Roura, E.; Wright, O.R.L. Adherence to the Mediterranean Diet and Chronic Disease in Australia: National Nutrition and Physical Activity Survey Analysis. Nutrients 2020, 12, 1251. [Google Scholar] [CrossRef]
- Barnaba, L.; Intorre, F.; Azzini, E.; Ciarapica, D.; Venneria, E.; Foddai, M.S.; Maiani, F.; Raguzzini, A.; Polito, A. Evaluation of adherence to Mediterranean diet and association with clinical and biological markers in an Italian population. Nutrition 2020, 77, 110813. [Google Scholar] [CrossRef]
- Karayiannis, D.; Kontogianni, M.D.; Mendorou, C.; Douka, L.; Mastrominas, M.; Yiannakouris, N. Association between adherence to the Mediterranean diet and semen quality parameters in male partners of couples attempting fertility. Hum. Reprod. 2016, 32, 215–222. [Google Scholar] [CrossRef]
- Kesse-Guyot, E.; Ahluwalia, N.; Lassale, C.; Hercberg, S.; Fezeu, L.; Lairon, D. Adherence to Mediterranean diet reduces the risk of metabolic syndrome: A 6-year prospective study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Je, Y. A modified Mediterranean diet score is inversely associated with metabolic syndrome in Korean adults. Eur. J. Clin. Nutr. 2018, 72, 1682–1689. [Google Scholar] [CrossRef] [PubMed]
- Mahdavi-Roshan, M.; Salari, A.; Ashouri, A.; Alizadeh, I. Association between depression symptoms and Mediterian dietary adherence in adults with cardiovascular disease risk factors in the north of Iran in 2016. Pol. Ann. Med. 2018, 26, 1–7. [Google Scholar] [CrossRef]
- Mattei, J.; Sotos-Prieto, M.; Bigornia, S.J.; Noel, S.E.; Tucker, K.L. The Mediterranean Diet Score Is More Strongly Associated with Favorable Cardiometabolic Risk Factors over 2 Years Than Other Diet Quality Indexes in Puerto Rican Adults. J. Nutr. 2017, 147, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Mayr, H.L.; Itsiopoulos, C.; Tierney, A.C.; Kucianski, T.; Radcliffe, J.; Garg, M.; Willcox, J.; Thomas, C.J. Ad libitum Mediterranean diet reduces subcutaneous but not visceral fat in patients with coronary heart disease: A randomised controlled pilot study. Clin. Nutr. ESPEN 2019, 32, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, P.; Moslehi, N.; Mahmoudof, H.; Sadeghi, M.; Azizi, F. A Longitudinal Study of Adherence to the Mediterranean Dietary Pattern and Metabolic Syndrome in a Non-Mediterranean Population. Int. J. Endocrinol. Metab. 2015, 13, e26128. [Google Scholar] [CrossRef]
- Mohamed, M.; Denis, L.; Rekia, B. Mediterranean Diet and Metabolic Syndrome in Adult Moroccan Women. J. Res. Obes. 2015, 2015, 15–32. [Google Scholar] [CrossRef][Green Version]
- Roldan, C.C.; Marcos, M.L.T.; Marcos, F.M.; Albero, J.S.; Rios, R.S.; Rodriguez, A.C.; Royo, J.M.P.; López, P.J.T. Adhesion to the Mediterranean diet in diabetic patients with poor control. Clinica e Investigacion en Arteriosclerosis 2019, 31, 210–217. [Google Scholar] [CrossRef]
- Rumawas, M.E.; Meigs, J.B.; Dwyer, J.T.; McKeown, N.M.; Jacques, P.F. Mediterranean-style dietary pattern, reduced risk of metabolic syndrome traits, and incidence in the Framingham Offspring Cohort. Am. J. Clin. Nutr. 2009, 90, 1608–1614. [Google Scholar] [CrossRef] [PubMed]
- Tortosa, A.; Bes-Rastrollo, M.; Sanchez-Villegas, A.; Basterra-Gortari, F.J.; Nuñez-Cordoba, J.M.; Martinez-Gonzalez, M.A. Mediterranean Diet Inversely Associated With the Incidence of Metabolic Syndrome: The SUN prospective cohort. Diabetes Care 2007, 30, 2957–2959. [Google Scholar] [CrossRef] [PubMed]
- Tsartsou, E.; Proutsos, N.; Castanas, E.; Kampa, M. Network Meta-Analysis of Metabolic Effects of Olive-Oil in Humans Shows the Importance of Olive Oil Consumption With Moderate Polyphenol Levels as Part of the Mediterranean Diet. Front. Nutr. 2019, 6, 6. [Google Scholar] [CrossRef]
- Fontana, L.; Eagon, J.C.; Trujillo, M.E.; Scherer, P.E.; Klein, S. Visceral Fat Adipokine Secretion Is Associated With Systemic Inflammation in Obese Humans. Diabetes 2007, 56, 1010–1013. [Google Scholar] [CrossRef] [PubMed]
- Phillips, L.K.; Prins, J.B. The link between abdominal obesity and the metabolic syndrome. Curr. Hypertens. Rep. 2008, 10, 156–164. [Google Scholar] [CrossRef]
- Howard, B.V. Insulin resistance and lipid metabolism. Am. J. Cardiol. 1999, 84 (Suppl. 1), 28–32. [Google Scholar] [CrossRef]
- Huo, R.; Du, T.; Xu, Y.; Xu, W.; Chen, X.; Sun, K.; Yu, X. Effects of Mediterranean-style diet on glycemic control, weight loss and cardiovascular risk factors among type 2 diabetes individuals: A meta-analysis. Eur. J. Clin. Nutr. 2014, 69, 1200–1208. [Google Scholar] [CrossRef]
- Mitjavila, M.T.; Fandos, M.; Salas-Salvadó, J.; Covas, M.-I.; Borrego, S.; Estruch, R.; Lamuela-Raventós, R.; Corella, D.; Martínez-Gonzalez, M.Á.; Sánchez, J.M.; et al. The Mediterranean diet improves the systemic lipid and DNA oxidative damage in metabolic syndrome individuals. A randomized, controlled, trial. Clin. Nutr. 2013, 32, 172–178. [Google Scholar] [CrossRef]
- Julibert, A.; Bibiloni, M.D.M.; Gallardo-Alfaro, L.; Abbate, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Fitó, M.; Martínez, J.A.; Alonso-Gómez, Á.M.; et al. Metabolic Syndrome Features and Excess Weight Were Inversely Associated with Nut Consumption after 1-Year Follow-Up in the PREDIMED-Plus Study. J. Nutr. 2020, 150, 3161–3170. [Google Scholar] [CrossRef]
- Hołowko-Ziółek, J.; Cięszczyk, P.; Biliński, J.; Basak, G.W.; Stachowska, E. What Model of Nutrition Can Be Recommended to People Ending Their Professional Sports Career? An Analysis of the Mediterranean Diet and the CRON Diet in the Context of Former Athletes. Nutrients 2020, 12, 3604. [Google Scholar] [CrossRef] [PubMed]
- Damasceno, N.R.; Sala-Vila, A.; Cofán, M.; Pérez-Heras, A.M.; Fitó, M.; Ruiz-Gutiérrez, V.; Martínez-González, M.Á.; Corella, D.; Arós, F.; Estruch, R.; et al. Mediterranean diet supplemented with nuts reduces waist circumference and shifts lipoprotein subfractions to a less atherogenic pattern in subjects at high cardiovascular risk. Atherosclerosis 2013, 230, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Hernáez, Á.; Castañer, O.; Fitó, M. Response to Letter Regarding Article, “Mediterranean Diet Improves High-Density Lipoprotein Function in High-Cardiovascular-Risk Individuals: A Randomized Controlled Trial”. Circulation 2017, 136, 342–343. [Google Scholar] [CrossRef]
- Notario-Barandiaran, L.; Project, O.B.O.T.I.; Valera-Gran, D.; Gonzalez-Palacios, S.; Garcia-De-La-Hera, M.; Fernández-Barrés, S.; Pereda-Pereda, E.; Fernández-Somoano, A.; Guxens, M.; Iñiguez, C.; et al. High adherence to a mediterranean diet at age 4 reduces overweight, obesity and abdominal obesity incidence in children at the age of 8. Int. J. Obes. 2020, 44, 1906–1917. [Google Scholar] [CrossRef]
- Mata, P.; Alvarez-Sala, L.A.; Rubio, M.J.; Nuño, J.; De Oya, M. Effects of long-term monounsaturated- vs polyunsaturated-enriched diets on lipoproteins in healthy men and women. Am. J. Clin. Nutr. 1992, 55, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Ghobadi, S.; Hassanzadeh-Rostami, Z.; Mohammadian, F.; Nikfetrat, A.; Ghasemifard, N.; Dehkordi, H.R.; Faghih, S. Comparison of blood lipid-lowering effects of olive oil and other plant oils: A systematic review and meta-analysis of 27 randomized placebo-controlled clinical trials. Crit. Rev. Food Sci. Nutr. 2018, 59, 2110–2124. [Google Scholar] [CrossRef]
- Abia, R.; Perona, J.S.; Pacheco, Y.M.; Montero, E.; Muriana, F.J.G.; Ruiz-Gutierrez, V. Postprandial triacylglycerols from dietary virgin olive oil are selectively cleared in humans. J. Nutr. 1999, 129, 2184–2191. [Google Scholar] [CrossRef]
- Berglund, L.; Lefevre, M.; Ginsberg, H.N.; Kris-Etherton, P.M.; Elmer, P.J.; Stewart, P.W.; Ershow, A.; Pearson, T.A.; Dennis, B.H.; Roheim, P.S.; et al. Comparison of monounsaturated fat with carbohydrates as a replacement for saturated fat in subjects with a high metabolic risk profile: Studies in the fasting and postprandial states. Am. J. Clin. Nutr. 2007, 86, 1611–1620. [Google Scholar] [CrossRef]
- Poudyal, H.; Panchal, S.K.; Diwan, V.; Brown, L. Omega-3 fatty acids and metabolic syndrome: Effects and emerging mechanisms of action. Prog. Lipid Res. 2011, 50, 372–387. [Google Scholar] [CrossRef]
- Sleiman, D.; Al-Badri, M.R.; Azar, S.T. Effect of Mediterranean Diet in Diabetes Control and Cardiovascular Risk Modification: A Systematic Review. Front. Public Health 2015, 3, 69. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Ceriello, A.; Giugliano, D. Prevention and control of type 2 diabetes by Mediterranean diet: A systematic review. Diabetes Res. Clin. Pr. 2010, 89, 97–102. [Google Scholar] [CrossRef]
- Elhayany, A.; Lustman, A.; Abel, R.; Attal-Singer, J.; Vinker, S. A low carbohydrate Mediterranean diet improves cardiovascular risk factors and diabetes control among overweight patients with type 2 diabetes mellitus: A 1-year prospective randomized intervention study. Diabetes Obes. Metab. 2010, 12, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Georgoulis, M.; Kontogianni, M.D.; Yiannakouris, N. Mediterranean Diet and Diabetes: Prevention and Treatment. Nutrients 2014, 6, 1406–1423. [Google Scholar] [CrossRef]
- Ajala, O.; English, P.; Pinkney, J. Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes. Am. J. Clin. Nutr. 2013, 97, 505–516. [Google Scholar] [CrossRef] [PubMed]
- Shimbo, D.; Muntner, P.; Mann, D.; Viera, A.J.; Homma, S.; Polak, J.F.; Barr, R.G.; Herrington, D.; Shea, S. Endothelial dysfunction and the risk of hypertension: The multi-ethnic study of atherosclerosis. Hypertension 2010, 55, 1210–1216. [Google Scholar] [CrossRef]
- Tuttolomondo, A.; Simonetta, I.; Daidone, M.; Mogavero, A.; Ortello, A.; Pinto, A. Metabolic and Vascular Effect of the Mediterranean Diet. Int. J. Mol. Sci. 2019, 20, 4716. [Google Scholar] [CrossRef] [PubMed]
- Bendinelli, B.; Masala, G.; Bruno, R.M.; Caini, S.; Saieva, C.; Boninsegni, A.; Ungar, A.; Ghiadoni, L.; Palli, D. A priori dietary patterns and blood pressure in the EPIC Florence cohort: A cross-sectional study. Eur. J. Nutr. 2019, 58, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Psaltopoulou, T.; Naska, A.; Orfanos, P.; Trichopoulos, D.; Mountokalakis, T.; Trichopoulou, A. Olive oil, the Mediterranean diet, and arterial blood pressure: The Greek European Prospective Investigation into Cancer and Nutrition (EPIC) study. Am. J. Clin. Nutr. 2004, 80, 1012–1018. [Google Scholar] [CrossRef] [PubMed]
- Cowell, O.R.; Mistry, N.; Deighton, K.; Matu, J.; Griffiths, A.; Minihane, A.M.; Mathers, J.C.; Shannon, O.M.; Siervo, M. Effects of a Mediterranean diet on blood pressure: A systematic review and meta-analysis of randomized controlled trials and observational studies. J. Hypertens. 2021, 39, 729–739. [Google Scholar] [PubMed]
- Filippou, C.D.; Thomopoulos, C.G.; Kouremeti, M.M.; Sotiropoulou, L.I.; Nihoyannopoulos, P.I.; Tousoulis, D.M.; Tsioufis, C.P. Mediterranean diet and blood pressure reduction in adults with and without hypertension: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2021. [Google Scholar] [CrossRef]
- Medina-Remón, A.; Tresserra-Rimbau, A.; Pons, A.; Tur, J.; Martorell, M.; Ros, E.; Buil-Cosiales, P.; Sacanella, E.; Covas, M.; Corella, D.; et al. Effects of total dietary polyphenols on plasma nitric oxide and blood pressure in a high cardiovascular risk cohort. The PREDIMED randomized trial. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Castro-Barquero, S.; Ruiz-León, A.M.; Sierra-Pérez, M.; Estruch, R.; Casas, R. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients 2020, 12, 2983. [Google Scholar] [CrossRef] [PubMed]
- Fontalba-Romero, M.I.; López-Enriquez, S.; Lago-Sampedro, A.; Garcia-Escobar, E.; Pastori, R.L.; Domínguez-Bendala, J.; Alvarez-Cubela, S.; Valdés, S.; Rojo-Martinez, G.; García-Fuentes, E.; et al. Association between the Mediterranean Diet and Metabolic Syndrome with Serum Levels of miRNA in Morbid Obesity. Nutrients 2021, 13, 436. [Google Scholar] [CrossRef]
- Reguero, M.; de Cedrón, M.G.; Wagner, S.; Reglero, G.; Quintela, J.; de Molina, A.R. Precision Nutrition to Activate Thermogenesis as a Complementary Approach to Target Obesity and Associated-Metabolic-Disorders. Cancers 2021, 13, 866. [Google Scholar] [CrossRef]
- Papadaki, A.; Nolen-Doerr, E.; Mantzoros, C.S. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients 2020, 12, 3342. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo-Mora, J.J.; Cortés-Sierra, L.; García-Pérez, M.Á.; Tarín, J.J.; Cano, A. Diet to Reduce the Metabolic Syndrome Associated with Menopause. The Logic for Olive Oil. Nutrients 2020, 12, 3184. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organization | Criteria |
|---|---|
| WHO (1998) [10] | Impaired glucose intolerance or diabetes and insulin resistance Two or more of the following risk markers:
|
| NCEP-ATP III (2002) [11] | Three or more of the following risk markers:
|
| IDF (2006) [12] | Central adiposity a Plus two or more of the following markers
|
| Study ID (Country) | No of Participants (F/M) | Mean Age (Years) | Population | MD Assessment Tool | WC (cm) | HDL Cholesterol (mg/dL) | TG (mg/dL) | FBG (mg/dL) | SBP (mmHg) | Measure of Effect |
|---|---|---|---|---|---|---|---|---|---|---|
| Alvarez-Leon 2006 (Canary Islands) [39] | 578 (329/249) | ≥18 1 | General population | Semi-quant FFQ 81 to calculate Specific food item score (10-item) [39] | L = 1 H = 0.77 [0.38–1.56] | L = 1 H = 0.90 [0.56–1.42] | L = 1 H = 1.05 [0.63–1.75] | L = 1 H = 2.46 [1.13–5.37] * | L = 1 H = 0.58 [0.34–0.99] * | OR [95%CI] |
| Aridi 2020 (Australia) [95] | 3245 (1753/1492) | 48.6 (17.6) | General population | Trichopoulou MDS [21] | L = 94.5 (14.7) H = 90.7 (13.3) * | L = 88.7% H= 89.9% | L = 83.1% H = 85.8% | L = 6.1% H = 5.7% | L = 123.6 (18.8) H = 122.1 (18.4) | Mean (SD)/ %Prevalence |
| Barnaba 2020 (Italy) [96] | 349 (228/121) | 18–86 1 | General population | MD serving score [35] | No info | L + M = 52.2 (11.1) H = 52.2 (13.4) | L + M = 107.5 (54.4) H = 110 (43.42) | L + M = 98.1 (12.2) H = 103.5 (11.76) | No info | Mean (SD) |
| Huang 2013 (Sweden) [40] | 187 (0/187) | 70 | Elderly population with CKD | Modified Trichopoulou MDS 14-item [21] | L = 97 (10) H = 97 (11) | L = 47 (14) H = 48 (14) | L = 127.8 (59.9) H = 122.2 (70.8) | L = 103 (20) H = 106 (28) | L = 149 (19) H = 148 (19) | Mean (SD) |
| Karayiannis 2017 (Greece) [97] | 142 (0/142) | 37.8 (5.4) | Subjects without systemic diseases, cryptorchidism or varicocele, microorchidism, vasectomy or hormonal treatment in the last six months | MDS by Panagiotakos 0–55 points [31] | No info | L = 49.4 (11.3) H = 50.4 (10.6) | L = 107.9 (39.3) H = 84.3 (27.1) | L = 89.6 (9.1) H = 86.4 (8.3) | No info | Mean (SD) |
| Kesse-Geyot 2013 (France) [98] | 1881 (668/1213) | 49.7 (6.2) | General population | Trichopoulou MDS—9 points [21] | L = 84.21 (0.9) H = 82.8 (0.96) | L = 58 (1.19) H = 58.8 (1.2) | L = 88.5 (35.4) H = 84.07 (2.65) | L = 90.7 (0.4) H = 90.4 (0.7) | L = 128.7 (1.4) H = 127.67 (1.42) | Mean (SD) |
| Kim 2018 (Korea) [99] | 2349 (1159/1190) | 19–65 1 | General population | Modified MDS -9 points [41] | L = 1 H = 0.45 [0.31–0.66] * | L = 1 H = 0.89 [0.70–1.13] * | L = 1 H = 0.72 [0.55–0.94] * | L = 1 H = 0.83 [0.63–1.10] * | L = 1 H = 0.99 [0.74–1.34] * | OR |
| Mahdavi-Roshnan 2017 (Iran) [100] | 344 (154/190) | L = 59.0 (8.30) H = 58.0 (9.36) | Subjects with CVD risk factors | PREDIMED MEDAS score -14 points [33] | No info | L = 42.81 (8.34) H = 43.3 (8.23) | L = 209.61 (399.33) H = 155.83 (87.63) | L = 116.4 (66.9) H = 105.9 (66.1) | No info | OR/ Mean (SD) |
| Mattei 2017 (US) [101] | 1194 (No info) | L = 56.6 (7.9) H = 57.2 (7.7) | Subjects with no severe health conditions or cognitive impairments | Trichopoulou MDS—9 points [21] | L = 103 (14) H = 102 (13) * | L = 46.3 (12.5) H = 45.96 (12.3) | L = 163 (93) H = 165 (127) | L = 115 (53) H = 112 (36) * | L = 135 (19) H = 137 (20) | Mean (SD) |
| Mayr 2019 (Australia) [102] | 37 (No info) | No info | Patients with coronary heart disease | PREDIMED MEDAS score 14—item [33] | L = 103.5 (3.4) H = 100.7 (3.3) * | L = 48.7 (6.5) H = 46.02 (6.1) | L = 102.75 (33.9) H = 115.15 (36.8) | L = 91.6 (13.40) H = 99 (13.30) | L = 136.5 (10.4) H = 133.4 (10.2) | Mean (SD) |
| Mirmiran 2015 (Iran) [103] | 1683 (927/756) | L = 36.3 (13.3) H = 41.3 (13.8) | General population | Trichopoulou MDS—8 points [21] | L = 1 H = 0.74 [0.48–1.13] | L = 1 H = 0.82 [0.48–1.40] * | L = 1 H = 0.81 [0.56–1.17] * | L = 1 H = 1.01 [0.73–1.39] | L = 1 H = 0.86 [0.64–1.22] | OR |
| Mziwira 2015 (Morocco) [104] | 90 (90/0) | 39.9 (0.66) | General non-pregnant population | Specific MDS- 0%–100% [42] | L = 1 H = 0.54 [0.13–2.27] | L = 1 H = 0.29 [0.02–3.02] | L = 1 H = 0.47 [0.04–4.94] | L = 1 H = 0.27 [0.05–1.49] | L = 1 H = 0.77 [0.19–3.15] | OR |
| Roldan 2019 (Spain) [105] | 107 (58/49) | 61.16 (23) | Overweight/Obese T2DM patients with poor glycemic control | PREDIMED MEDAS score—14 points [33] | Νo info | L = 48.29 H = 52.45 * | L = 223.56 H = 171.23 ** | L = 201.14 H = 132.88 * | Νo info | Mean |
| Rumawas 2009 (US) [106] | 1069 (608/461) | L = 52.4 (9.9) H = 54.8 (9.6) | Non-diabetic general population | The MSDPS—100 points [36] | L = 98.5 H = 97.1 ** | L = 53.3 H = 54 * | L = 114 H = 103 ** | L= 98.5 H = 97.1 * | L = 122 H = 121 | Geometric mean |
| Steffen 2014 (US) [44] | 865 (511/354) | L = 24.3 H = 25.7 | General population | Modified Trichopoulou MDS—22 points [21] | L = 59.4% H = 41.9% ** | L = 68.4% H = 59.3% * | L = 37.3% H = 21.6% ** | L= 21.3% H = 19.1% * | L= 49.2% H = 40.4% * | %Prevalence |
| Tortosa 2007 (Spain) [107] | 1040 (No info) | No info | Graduate students | Trichopoulou MDS—9 points [21] | L = 82.5 (12) H = 82 (12) * | L = 63.8 (15) H = 64.1 (19) * | L = 80.0 (38) H = 78 (40) | L = 86.1 (11) H = 87.3 (17) | L = 112.5 (14) H = 113.3 (13) | Mean (SD) |
| Yang 2014 (US) [43] | 395 (0/395) | L = 38.2 (8.6) H = 37.1 (8.4) | General population | Study Specific MDS—42 points [43] | No info | L = 41.7 (1.3) H = 46.6 (1.3) | L = 140.4 (1.8) H = 115.8 (1.8) | L = 93.2 (1.2) H = 91.1 (1.2) | L = 122.4 (12.6) H = 122.8 (13.3) | Geometric mean (SD) |
| Study ID (Country) | No Participants (F/M) | Age (Years) | Population | MD Assessment Tool |
|---|---|---|---|---|
| Abiemo 2013 (US) [45] | 2440 (1305/1135) | L = 60.0 (10.3) H = 63.0 (10.3) | General population | Study Specific Alternate MDS—10 points [45] |
| Ahmad 2018 (US) [58] | 16,623 (16,623/0) | L = 52.6 (6.7) H = 54.9 (8.1) | General population | Trichopoulou MDS—9 points [21] |
| Ahmed 2020 (US) [59] | 224 (133/91) | L = 56.2 (12.6) H = 66.7 (11.6) | Community-dweling adults | Sofi MDS—12 points [32] |
| Asghari 2016 (Iran) [60] | 622 (308/314) | L = 43.0 (9.1) H = 43.7 (9.7) | Subjects without CKD | Trichopoulou MDS—8 points [108] |
| Baratta 2017 (Italy) [61] | 148 (47/101) | L = 51.7 (11.3) H = 57.7 (11.9) | Outpatients presenting with T2DM, HBP, Overweight/Obese, Dyslipedemia or MetS | Short MDS—9 points [34] |
| Bondia-Pons 2009 (Spain) [62] | 70 (41/29) | 47 (15.3) | General population | MD Quality Index—14 point % adherence [37] |
| Campanella 2020 (Italy) [63] | 2387 (1183/1204) | L = 45.5(15.5) H = 54.6 (15.5) | General population | Relative MD system—18 points [38] |
| Dai 2008 (US) [64] | 194 (0/194) | L = 53.8 (0.3) H = 54.8 (0.3) | Middle aged twins who have served in the Vietman War | Trichopoulou MDS—9 points [21] |
| Esposito 2009 (Italy) [65] | 475 (232/243) | L = 58.0 (7.0) H = 58.3 (7.0) | T2DM patients | Trichopoulou MDS—9 points [21] |
| Gardener 2015 (US) [66] | 543 (308/235) | L = 69.0 (8.0) H = 65.0 (9.0) | Population never diagnosed with stroke | Trichopoulou MDS—9 points [21] |
| Giraldi 2020 (Italy) [67] | 209 (61/148) | L = 41.7 (13.3) H = 49.9 (16.4) | Patients with NAFLD | Sofi MDS—12 points [32] |
| Giugliano 2010a (Italy) [69] | 315 (315/0) | L = 57.7 (6.7) H = 58.0 (6.8) | T2DM patients | Trichopoulou MDS—9 points [21] |
| Giugliano 2010b (Italy) [68] | 288 (0/288) | L = 54.7 (6.9) H = 58.7 (7.0) | T2DM patients | Trichopoulou MDS- 9 points [21] |
| Granado-Casas 2020 (Spain) [70] | 92 (52/40) | L = 41.9 (10.6) H = 45.1 (10.9) | T1DM patients | Trichopoulou MDS—9 points [21] |
| Grosso 2015 (Poland) [46] | 4678 (2408/2270) | 45–69 * | General population | Modified Panagiotakos MDS—60 points [31] |
| Hu 2013 (Spain) [71] | 7305 (4188/3117) | L = 67.2 (6.2) H = 67.0 (6.2) | Adults with high risk of CVD, with T2DM or at least 3/6 CVD risk factors | PREDIMED MEDAS Score—14 points [33] |
| Izadi 2016 (Iran) [72] | 325 (325/0) | L = 28.0 (6.2) H = 27.2 (5.2) | Pregnant carrying singleton fetuses with/without GDM | Trichopoulou MDS—9 points [21] |
| Jalilpiran 2020 (Iran) [73] | 357 (0/357) | L = 66.5 (6.7) H = 63.3 (5.8) | General population | Trichopoulou MDS—9 points [21] |
| Jayedi 2019 (Iran) [74] | 131 (131/0) | L = 54.7 (6.8) H = 54.9 (7.5) | Females with prevalent T2DM or with history of 3–10 yrs T2DM and with/without DN | Trichopoulou MDS—9 points [21] |
| Köroğlu 2020 (Turkey) [75] | 25 (0/25) | 18–65 * | Patients with lower limb amputation | PREDIMED MEDAS Score—14 points [33] |
| Kwon 2020 (Korea) [76] | 148 (84/64) | L = 43.6 (9.1) H = 53.3 (8.3) | General Population | PREDIMED MEDAS Score—14 points [33] |
| Lavados 2020 (Leu) [77] | 368 (158/210) | L = 67.2 (18.7) H = 69.9 (16.9) | Patients with acute ischemic stroke | PREDIMED MEDAS Score—14 points [33] |
| Leu 2019 (Taiwan) [78] | 1400 (807/593) | L = 48.4 (12.7) H = 50.6 (11.4) | General Population | Trichopoulou MDS—9 points [21] |
| Mateo-Gallego 2017 (Spain) [79] | 1016 (54/962) | L = 50.9 (4.0) H = 51.7 (3.7) | Employees of car assembly plant | Trichopoulou MDS—9 points [21] |
| Molina-Leyva 2018 (Spain) [80] | 25 (No info) | L = 43.7 (10.9) H = 50.8 (13.5) | Patients with psoriasis | PREDIMED MEDAS Score—14 points [33] |
| Moradi 2020 (Iran) [81] | 153 (95/58) | L = 64.7 (9.3) H = 67.2 (9.8) | Diabetic patients with nephropathy | Trichopoulou MDS—9 points [21] |
| Mosconi 2014 (US) [82] | 52 (37/15) | L = 53.0 (13) H = 55.0 (12) | Cognitive-normal individuals | Study Specific MDS—9 points [82] |
| Park 2016 (US) [83] | 1034 (572/462) | L = 40.8 (0.9) H = 40.8 (1.3) | Metabolicaly healthy and unhealthy obese population | Panagiotakos MDS—55 points [31] |
| Peñalvo 2015 (Spain) [84] | 516 (18/498) | L = 50.8 (3.8) H = 51.5 (3.4) | General population | MEDAS Score [33] Alternative MD index [41] |
| Pocovi-Gerardino 2020 (Spain) [85] | 159 (143/16) | L = 38.6 (9.7) H = 28.3 (12.8) | Patients with SLE | PREDIMED MEDAS Score—14 points [33] |
| Ruiz-Cabello 2016 (Spain) [86] | 118 (118/0) | L = 52.0 (4.8) H = 52.9 (4.1) | Peri- and menopausal females | Panagiotakos MDS—55 points [31] |
| Salas-Huetos 2019 (Spain) [87] | 57 (0/57) | L = 24.1 (4.5) H = 26.3 (4.8) | Healthy subjects | Trichopoulou MDS—9 points [21] |
| Sotos-Prieto 2014 (UK) [88] | 10,359 (5593/4766) | L = 59.0 (9.4) H = 59.3 (9.3) | General population | Trichopoulou MDS—9 points [21] |
| Tuttolomondo 2015 (Italy) [89] | 288 (162/126) | L = 72.9 (14.8) H = 72.4 (13.2) | Patients with ischemic heart disease | Trichopoulou MDS—9 points [21] |
| Tuttolomondo 2020 (Italy) [90] | 409 (250/159) | L = 70.2 (12.6) H = 72.0 (10.4) | Patients with congestive heart failure | Trichopoulou MDS—9 points [21] |
| Tzima 2007 (Greece) [91] | 1040 (333/707) | L = 55.0 (13) H = 35.0 (10) | Obese and Overweight population | Panagiotakos MDS—55 points [31] |
| Veglia 2019 (Finland, Sweden, Netherlands, France, Italy) [47] | 1835 (980/855) | L = 64.8 (5.4) H = 63.9 (5.7) | Patients with >3 vascular risk factors | Study Specific MDS—7 points [47] |
| Veissi 2016 (Iran) [92] | 157 (104/53) | L = 54.3 (9.9) H = 54.6 (8.9) | T2DM patients | Study Specific MDS—4 points [92] |
| Viscogliosi 2013 (Italy) [93] | 55 (33/22) | L = 59.6 (10.2) H = 60.0 (9.4) | High CVD risk population | PREDIMED MEDAS Score—14 points [33] |
| Vitale 2018 (Italy) [49] | 1539 (606/933) | No info | T2DM patients with HbA1c 7%–9% | Modified Trichopoulou MDS—18 points [21] |
| Zupo 2020 (Italy) [94] | 324 (228/96) | L = 38.0 (13.1) H = 42.5 (13.1) | General population | PREDIMED MEDAS Score—14 points [33] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakaloudi, D.R.; Chrysoula, L.; Kotzakioulafi, E.; Theodoridis, X.; Chourdakis, M. Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2021, 13, 1514. https://doi.org/10.3390/nu13051514
Bakaloudi DR, Chrysoula L, Kotzakioulafi E, Theodoridis X, Chourdakis M. Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients. 2021; 13(5):1514. https://doi.org/10.3390/nu13051514
Chicago/Turabian StyleBakaloudi, Dimitra Rafailia, Lydia Chrysoula, Evangelia Kotzakioulafi, Xenophon Theodoridis, and Michail Chourdakis. 2021. "Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies" Nutrients 13, no. 5: 1514. https://doi.org/10.3390/nu13051514
APA StyleBakaloudi, D. R., Chrysoula, L., Kotzakioulafi, E., Theodoridis, X., & Chourdakis, M. (2021). Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients, 13(5), 1514. https://doi.org/10.3390/nu13051514