
Sodium Intake and Proteinuria/Albuminuria in the Population—Observational, Cross-Sectional Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Calculations
2.2. Statistics
3. Results
3.1. Descriptive Statistics
3.2. Linear Regression
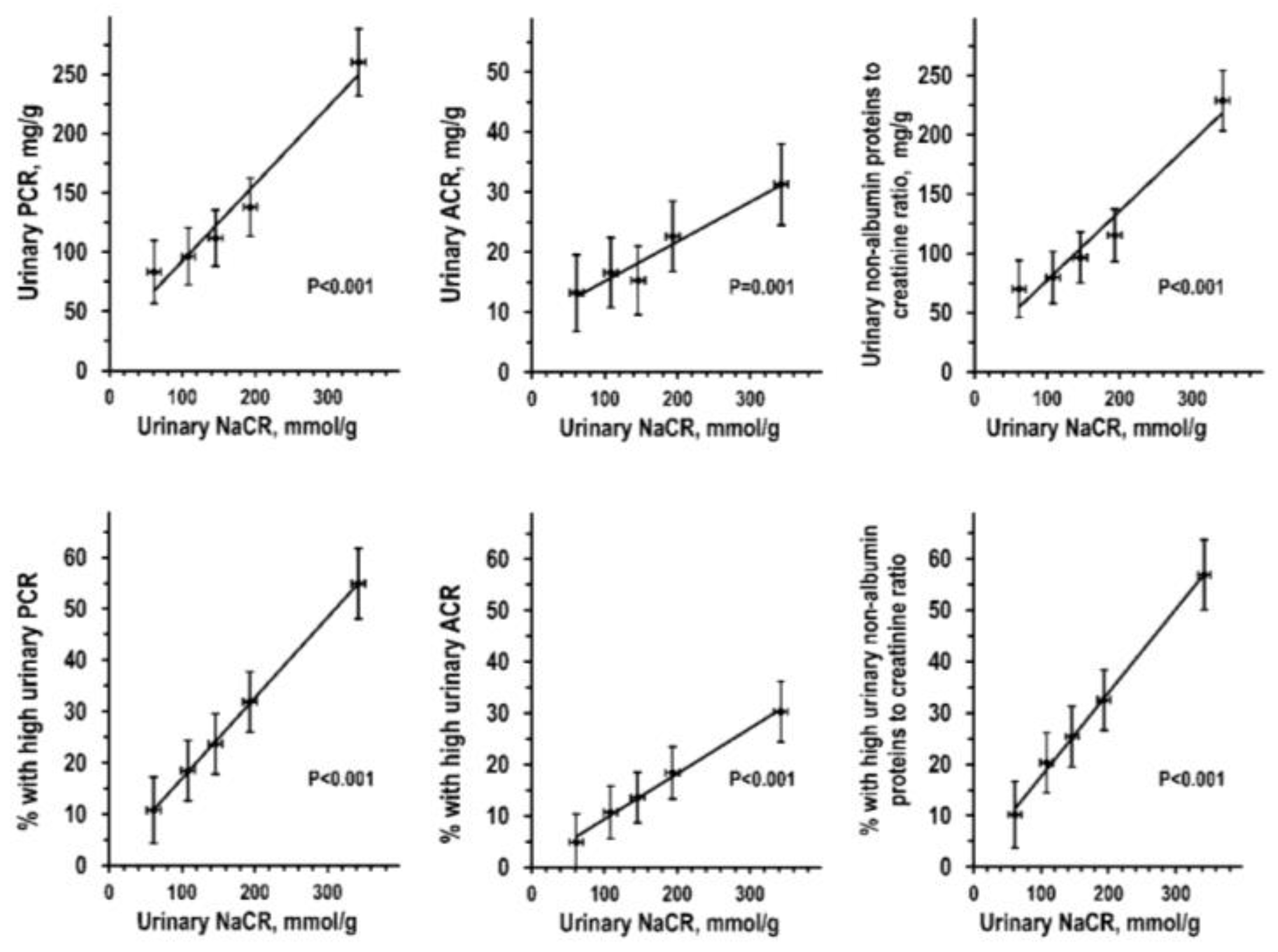
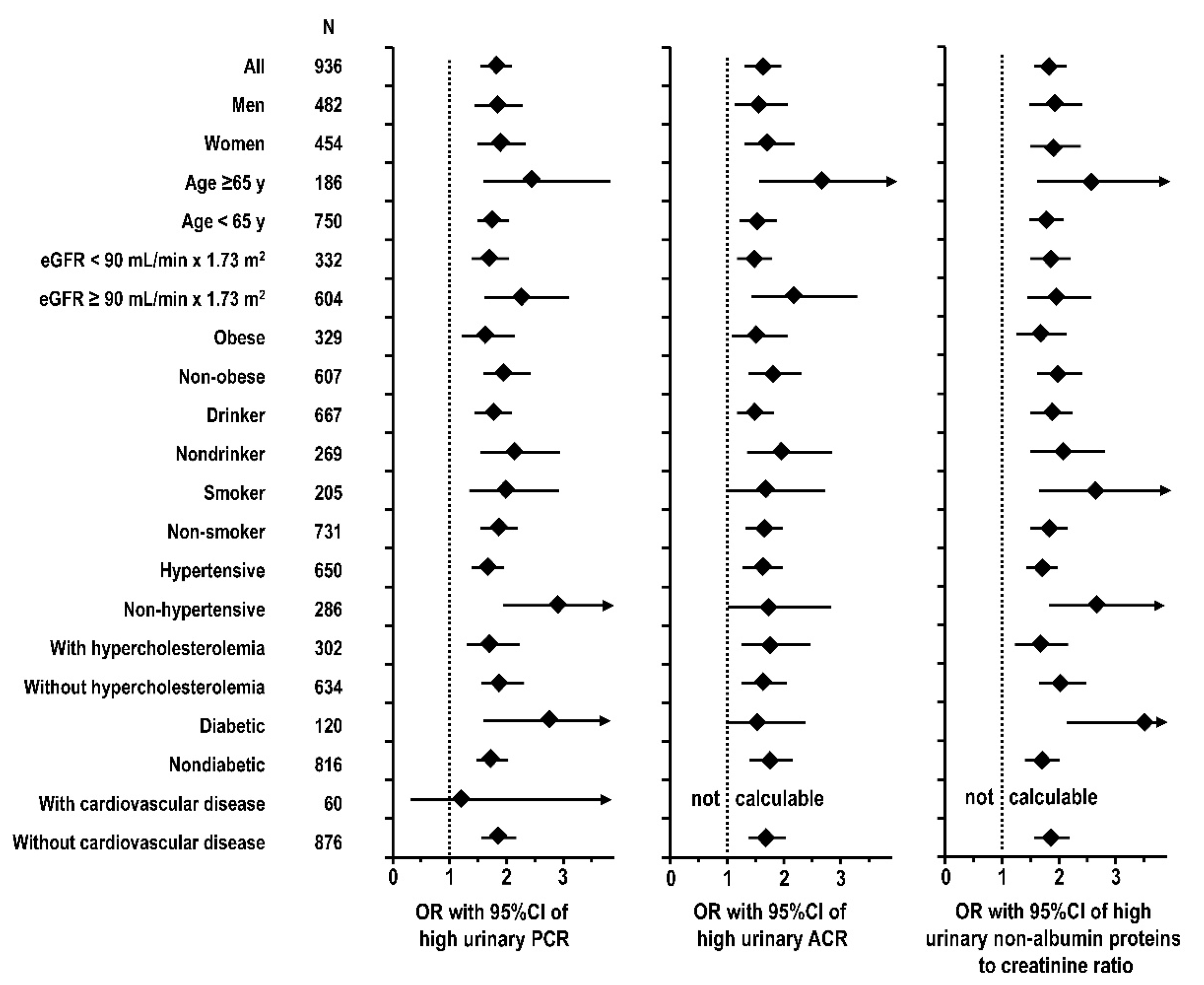
3.3. Quintile Analyses and Logistic Regression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group. KDIGO Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. Suppl. 2012, 2, 337–414. [Google Scholar]
- Nomura, M.; Asayama, K.; Jacobs, L.; Thijs, L.; Staessen, J.A. Renal function in relation to sodium intake: A quantitative review of the literature. Kidney Int. 2017, 92, 67–78. [Google Scholar] [PubMed] [Green Version]
- McMahon, E.J.; Bauer, J.D.; Hawley, C.M.; Isbel, N.M.; Stowasser, M.; Johnson, D.W.; Campbell, K.L. A Randomized trial of dietary sodium restriction in CKD. J. Am. Soc. Nephrol. 2013, 24, 2096–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, E.J.; Campbell, K.L.; Bauer, J.D.; Mudge, D.W. Altered dietary salt intake for people with chronic kidney disease. Cochrane Database Syst. Rev. 2015, 18, CD010070. [Google Scholar] [CrossRef] [Green Version]
- Di Castelnuovo, A.; Costanzo, S.; Persichillo, M.; Olivieri, M.; De Curtis, A.; Zito, F.; Donati, M.B.; De Gaetano, G.; Iacoviello, L. Distribution of short and lifetime risks for cardiovascular disease in Italians. Eur. J. Prev. Cardiol. 2012, 19, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Bonaccio, M.; Di Castelnuovo, A.; Costanzo, S.; Persichillo, M.; De Curtis, A.; Donati, M.B.; De Gaetano, G.; Iacoviello, L. Adherence to the traditional Mediterranean diet and mortality in subjects with diabetes. Prospective results from the MOLI-SANI study. Eur. J. Prev. Cardiol. 2016, 23, 400–407. [Google Scholar] [CrossRef]
- Iacoviello, L.; De Curtis, A.; Donati, M.B.; de Gaetano, G. Biobanks for cardiovascular epidemiology and prevention. Future Cardiol. 2014, 10, 243–254. [Google Scholar] [CrossRef]
- Zeller, T.; Hughes, M.; Tuovinen, T.; Schillert, A.; Conrads-Frank, A.; den Ruijter, H.; Schnabel, R.B.; Kee, F.; Salomaa, V.; Siebert, U.; et al. BiomarCaRE: Rationale and design of the European BiomarCaRE project including 300,000 participants from 13 European countries. Eur. J. Epidemiol. 2014, 29, 777–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirillo, M.; Bilancio, G.; Guarino, E.; Cavallo, P.; Lombardi, C.; Costanzo, S.; De Curtis, A.; Di Castelnuovo, A.; Iacoviello, L. Vitamin D Status and indices of mineral homeostasis in the population: Differences between 25-hydroxyvitamin D and 1.;25-dihydroxyvitamin D. Nutrients 2019, 11, 1777. [Google Scholar]
- Pauli, D.; Seyfarth, M.; Dibbelt, L. The Abbott Architect c8000: Analytical performance and productivity characteristics of a new analyzer applied to general chemistry testing. Clin. Lab. 2005, 51, 31–41. [Google Scholar] [PubMed]
- Myers, G.L.; Miller, W.G.; Coresh, J.; Fleming, J.; Greenberg, N.; Greene, T.; Hostetter, T.; Levey, A.S.; Panteghini, M.; Welch, M.; et al. Recommendations for improving serum creatinine measurement: A report from the Laboratory Working Group of the National Kidney Disease Education Program. Clin. Chem. 2006, 52, 5–18. [Google Scholar] [CrossRef]
- Valcour, A.; Zierold, C.; Podgorski, A.L.; Olson, G.T.; Wall, J.V.; DeLuca, H.F.; Bonelli, F. A novel, fully-automated, chemiluminescent assay for the detection of 1,25-dihydroxyvitamin D in biological samples. J. Steroid Biochem. Mol. Biol. 2016, 164, 120–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de la Hunty, A.; Wallace, A.M.; Gibson, S.; Viljakainen, H.; Lamberg-Allardt, C.; Ashwell, M. UK Food Standards Agency Workshop Consensus Report: The choice of method for measuring 25-hydroxyvitamin D to estimate vitamin D status for the UK National Diet and Nutrition Survey. Br. J. Nutr. 2010, 104, 612–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phinney, K.W.; Bedner, M.; Tai, S.S.-C.; Vamathevan, V.V.; Sander, L.C.; Sharpless, K.E.; Wise, S.A.; Yen, J.H.; Schleicher, R.L.; Chaudhary-Webb, M.; et al. Development and certification of a standard reference material for vitamin D metabolites in human serum. Anal. Chem. 2012, 84, 956–962. [Google Scholar] [CrossRef] [Green Version]
- Cogswell, M.E.; Maalouf, J.; Elliott, P.; Loria, C.M.; Patel, S.; Bowman, B.A. Use of urine biomarkers to assess sodium intake: Challenges and opportunities. Annu. Rev. Nutr. 2015, 35, 349–387. [Google Scholar] [CrossRef] [Green Version]
- Campbell, N.R.C.; He, F.J.; Tan, M.; Cappuccio, F.P.; Neal, B.; Woodward, M.; Cogswell, M.E.; McLean, R.; Arcand, J.; MacGregor, G.; et al. The International Consortium for Quality Research on Dietary Sodium/Salt (TRUE) position statement on the use of 24-hour, spot, and short duration (<24 hours) timed urine collections to assess dietary sodium intake. J. Clin. Hypertens. 2019, 21, 700–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirillo, M.; Bilancio, G.; Cavallo, P.; Palladino, R.; Terradura-Vagnarelli, O.; Laurenzi, M. Sodium intake and kidney function in the general population: An observational population-based study. Clin. Kidney J. 2021, 14, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.M.; Fraser, S.D.S.; Bradley, J.A.; Bradley, C.; Draper, H.; Metcalfe, W.; Oniscu, G.C.; Tomson, C.R.; Ravanan, R.; Roderick, P.J. A systematic review of the prevalence and associations of limited health literacy in CKD. Clin. J. Am. Soc. Nephrol. 2017, 12, 1070–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roshanravan, B.; Gamboa, J.; Wilund, K. Exercise and CKD: Skeletal muscle dysfunction and practical application of exercise to prevent and treat physical impairments in CKD. Am. J. Kidney Dis. 2017, 69, 837–852. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.R.; Grams, M.E.; Ballew, S.H.; Bilo, H.; Correa, A.; Evans, M.; Gutierrez, O.M.; Hosseinpanah, F.; Iseki, K.; Kenealy, T.; et al. Adiposity and risk of decline in glomerular filtration rate: Meta-analysis of individual participant data in a global Consortium. BMJ 2019, 364, k5301. [Google Scholar] [CrossRef] [Green Version]
- Cirillo, M.; Laurenzi, M.; Mancini, M.; Zanchetti, A.; de Santo, N.G. Low muscular mass and overestimation of microalbuminuria by urinary albumin/creatinine ratio. Hypertension 2006, 47, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Metcalf, P.A.; Baker, J.; Scragg, R.; Dryson, E.; Scott, A.J.; Wild, C.J. Albuminuria in people at least 40 years old: Effect of alcohol consumption, regular exercise, and cigarette smoking. Clin. Chem. 1993, 39, 1793–1797. [Google Scholar] [CrossRef] [PubMed]
- Cirillo, M.; Senigalliesi, L.; Laurenzi, M.; Alfieri, R.; Stamler, J.; Stamler, R.; Panarelli, W.; De Santo, N.G. Microalbuminuria in nondiabetic adults–Relation of blood pressure, body mass index, plasma cholesterol levels, and smoking: The Gubbio population study. Arch. Intern. Med. 1998, 158, 1933–1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravid, M.; Brosh, D.; Ravid-Safran, D.; Levy, Z.; Rachmani, R. Main risk factors for nephropathy in type 2 diabetes mellitus are plasma cholesterol levels, mean blood pressure, and hyperglycemia. Arch. Intern. Med. 1998, 158, 998–1004. [Google Scholar] [CrossRef] [PubMed]
- Sarnak, M.J.; Amann, K.; Bangalore, S.; Cavalcante, J.L.; Charytan, D.M.; Craig, J.C.; Gill, J.S.; Hlatky, M.A.; Jardine, A.G.; Landmesser, U.; et al. Chronic kidney disease and coronary artery disease. J. Am. Coll. Cardiol. 2019, 74, 1823–1838. [Google Scholar] [CrossRef]
- Wang, S.-Y.; Cai, G.-Y.; Chen, Z.-M. Energy restriction in renal protection. Br. J. Nutr. 2018, 120, 1149–1158. [Google Scholar] [CrossRef] [Green Version]
- Snelson, M.; Clarke, R.E.; Coughlan, M.T. Stirring the pot: Can dietary modification alleviate the burden of CKD? Nutrients 2017, 9, 265. [Google Scholar] [CrossRef] [PubMed]
- Gritter, M.; Rotmans, J.I.; Hoorn, E.J. Role of dietary K+ in natriuresis, blood pressure reduction, cardiovascular protection, and renoprotection. Hypertension 2019, 73, 15–23. [Google Scholar] [CrossRef]
- Chang, A.R.; Anderson, C. Dietary phosphorus intake and the kidney. Annu. Rev. Nutr. 2017, 37, 321–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheungpasitporn, W.; Thongprayoon, C.; Kittanamongkolchai, W.; Brabec, B.A.; O’Corragain, O.A.; Edmonds, P.J.; Erickson, S.B. High alcohol consumption and the risk of renal damage: A systematic review and meta-analysis. QJM 2015, 108, 539–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humalda, J.K.; Goldsmith, D.J.A.; Thadhani, R.; de Borst, M.H. Vitamin D analogues to target residual proteinuria: Potentiual impact on cardiorenal outcomes. Nephrol. Dial. Transplant. 2015, 30, 1988–1994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonaccio, M.; Di Castelnuovo, A.; Costanzo, S.; De Lucia, F.; Olivieri, M.; Donati, M.B.; De Gaetano, G.; Iacoviello, L.; Bonanni, A. Mass media information and adherence to Mediterranean diet: Results from the Moli-sani study. Int. J. Public Health 2012, 57, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32 (Suppl. S9), 498–504. [Google Scholar] [CrossRef] [Green Version]
- Ix, J.H.; Wassel, C.L.; Stevens, L.A.; Beck, G.J.; Froissart, M.; Navis, G.; Rodby, R.; Torres, V.E.; Zhang, Y. (Lucy); Greene, T.; et al. Equations to estimate creatinine excretion rate: The CKD Epidemiology Collaboration. Clin. J. Am. Soc. Nephrol. 2011, 6, 184–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirillo, M.; Lombardi, C.; Luciano, M.G.; Bilancio, G.; Anastasio, P.; De Santo, N.G. Estimation of GFR: A comparison of new and established equations. Am. J. Kidney Dis. 2010, 56, 802–804. [Google Scholar] [CrossRef]
- Sharma, S.; McFann, K.; Chonchol, M.; de Boer, I.H.; Kendrick, J. Association between dietary sodium and potassium intake with chronic kidney disease in US adults: A cross-sectional study. Am. J. Nephrol. 2013, 37, 526–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirillo, M. Determinants of kidney dysfunction: Is vasopressin a new player in the arena? Kidney Int. 2010, 77, 5–6. [Google Scholar] [CrossRef] [Green Version]
- Tasevska, I.; Enhörning, S.; Burri, P.; Melander, O. High salt intake increases copeptin but salt sensitivity is associated with fluid induced reduction of copeptin in women. Int. J. Hypertens. 2014, 2014, 641587. [Google Scholar] [CrossRef] [Green Version]
- Thornton, S.N. Sodium intake.; cardiovascular disease, and physiology. Nat. Rev. 2018, 15, 497. [Google Scholar] [CrossRef]
- Meijer, E.; Bakker, S.J.L.; Halbesma, N.; de Jong, P.E.; Struck, J.; Gansevoort, R.T. Copeptin, a surrogate marker of vasopressin is associated with microalbuminuria in a large population cohort. Kidney Int. 2010, 77, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardoux, P.; Bichet, D.G.; Martin, H.; Gallois, Y.; Marre, M.; Arthus, M.-F.; Lonergan, M.; Ruel, N.; Bouby, N.; Bankir, L. Vasopressin increases urinary albumin excretion in rats and humans: Involvement of V2 receptors and the renin-angiotensin system. Nephrol. Dial. Transplant. 2003, 18, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.M.; Nawaz, A.; Evans, M. Renal outcomes in type 2 diabetes: A review of cardiovascular and renal outcome trials. Diabetes Ther. 2020, 11, 369–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumida, K.; Nadkarni, G.N.; Grams, M.E.; Sang, Y.; Ballew, S.H.; Coresh, J.; Matsushita, K.; Surapaneni, A.; Brunskill, N.; Chadban, S.J.; et al. Conversion of urine protein–creatinine ratio or urine dipstick protein to urine albumin–creatinine ratio for use in chronic kidney disease screening and prognosis-An individual participant–based meta-analysis. Ann. Intern. Med. 2020, 173, 426–435. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Women | Men | pa | |
|---|---|---|---|
| n | 454 | 482 | |
| Age, years | 60.0 ± 10.0 | 60 ± 10 | 0.801 |
| Education, % with high school or higher | 38.9% | 46.4% | 0.021 |
| Physical activity, MET-d | |||
| total | 40.6 (39.5–42.3) | 40.7 (39.2–44.0) | |
| log-transformed | 1.62 ± 0.05 | 1.63 ± 0.08 | 0.001 |
| leisure | 1.7 (0.3–3.4) | 3.4 (1.1–6.8) | |
| log-transformed | 0.25 ± 0.40 | 0.46 ± 0.46 | 0.001 |
| Body mass index, kg-m2 | 28.7 ± 5.5 | 28.6 ± 4.2 | 0.793 |
| Waist-hip ratio | 0.90 ± 0.08 | 0.95 ± 0.06 | <0.001 |
| Estimated urinary creatinine, g-d | 1.00 ± 0.17 | 1.52 ± 0.18 | <0.001 |
| Current smoking, % | 16.1% | 26.6% | <0.001 |
| Systolic pressure, mmHg | 144 ± 21 | 147 ± 19 | 0.018 |
| Diastolic pressure, mmHg | 82 ± 10 | 85 ± 9 | <0.001 |
| Antihypertensive drug, % | 41.4% | 31.9% | 0.003 |
| Inhibitor-blocker renin-angiotensin system, % | 31.8% | 24.6% | 0.014 |
| Diuretic, % | 20.3% | 12.8% | 0.002 |
| Serum total cholesterol, mg-100 mL | 218 ± 39 | 208 ± 40 | <0.001 |
| Statin, % | 9.6% | 10.6% | 0.697 |
| Serum glucose, mg-100 mL | 98 ± 23 | 107 ± 30 | <0.001 |
| Oral antidiabetic drug, % | 5.4% | 9.2% | 0.034 |
| Insulin treatment, % | 1.5% | 1.4% | 0.929 |
| Diabetes, % | 9.2% | 16.0% | 0.002 |
| Cardiovascular disease history, % | 3.3% | 9.4% | <0.001 |
| Serum creatinine, mg-100 mL | 0.74 ± 0.14 | 0.91 ± 0.19 | <0.001 |
| Serum cystatin C, mg-L | 1.01 ± 0.23 | 1.03 ± 0.21 | 0.122 |
| eGFR, mL-min × 1.73 m2 | 82 ± 16 | 85 ± 16 | 0.003 |
| Energy intake, kcal-d | 1844 ± 558 | 2227 ± 692 | <0.001 |
| Urinary creatinine, mg-100 mL | 31 (16–64) | 66 (31–110) | |
| log-transformed | 1.48 ± 0.42 | 1.74 ± 0.43 | <0.001 |
| Urinary NaCR, mmol-g | 169 (115–232) | 124 (89–181) | |
| log-transformed | 2.21 ± 0.26 | 2.10 ± 0.27 | <0.001 |
| Urinary urea nitrogen-creatinine ratio, g-g | 9.8 (8.1–11.6) | 7.7 (6.3–9.2) | |
| log-transformed | 0.99 ± 0.13 | 0.88 ± 0.14 | <0.001 |
| Urinary potassium-creatinine ratio, mmol-g | 82 (61–106) | 63 (47–83) | |
| log-transformed | 1.91 ± 0.17 | 1.80 ± 0.17 | <0.001 |
| Urinary phosphorus-creatinine ratio, mg-g | 493 (364–621) | 417 (296–564) | |
| log-transformed | 2.67 ± 0.20 | 2.60 ± 0.216 | <0.001 |
| Alcohol intake, g-d | 2 (0–12) | 27 (7–48) | |
| log-transformed | 0.48 ± 0.55 | 1.18 ± 0.63 | <0.001 |
| Serum 25-OH vitamin D, ng-mL | 21 ± 13 | 22 ± 12 | |
| log-transformed | 1.25 ± 0.27 | 1.28 ± 0.24 | 0.030 |
| Urinary total proteins-creatinine ratio, mg-g | 103 (48–198) | 59 (29–131) | |
| log-transformed | 1.99 ± 0.52 | 1.79 ± 0.48 | <0.001 |
| Urinary albumin-creatinine ratio, mg-g | 11 (5–23) | 6 (3–17) | |
| log-transformed | 1.05 ± 0.49 | 0.86 ± 0.56 | <0.001 |
| Urinary non-albumin proteins-creatinine ratio, mg-g | 83 (37–170) | 51 (23–108) | |
| log-transformed | 1.87 ± 0.61 | 1.68 ± 0.53 | <0.001 |
| Dependent Variable | Women n = 454 | Men n = 482 | |
|---|---|---|---|
| Simple regression | Urinary PCR, log mg/g | 0.432 (0.35/0.51) <0.001 | 0.369 (0.29/0.45) <0.001 |
| Urinary ACR, log mg/g | 0.753 (0.59/0.91) <0.001 | 0.328 (0.24/0.41) <0.001 | |
| Urinary non/albumin proteins to creatinine ratio, log mg/g | 0.392 (0.31/0.47) <0.001 | 0.344 (0.26/0.43) <0.001 | |
| Multivariable regression * | Urinary PCR, log mg/g | 0.280 (0.17/0.39) <0.001 | 0.242 (0.13/0.35) <0.001 |
| Urinary ACR, log mg/g | 0.310 (0.20/0.42) <0.001 | 0.265 (0.16/0.38) <0.001 | |
| Urinary non/albumin proteins to creatinine ratio, log mg/g | 0.247 (0.14/0.36) <0.001 | 0.209 (0.09/0.33) <0.001 | |
| Independent Variables | Dependent Variable | ||
|---|---|---|---|
| Urinary PCR log mg/g | Urinary ACR log mg/g | Urinary Non−Albumin Proteins to Creatinine Ratio log mg/g | |
| Age, years | −0.157 (−0.27/−0.05) 0.007 | −0.121 (−0.23/−0.01) 0.035 | −0.142 (−0.26/−0.02) 0.017 |
| Systolic pressure, mmHg | 0.129 (0.04/0.22) 0.005 | 0.170 (0.08/0.26) <0.001 | 0.111 (0.02/0.20) 0.018 |
| Diabetes, yes/no = 1/0 | 0.064 (0.01/0.12) 0.048 | 0.158 (0.10/0.22) <0.001 | 0.026 (−0.02/0.09) n.s. |
| eGFR, mL/min × 1.73 m2 | −0.077 (−0.15/0.01) n.s. | −0.094 (−0.17/−0.02) 0.022 | −0.067 (−0.15/0.02) n.s. |
| uNaCR, log mmol/g | 0.267 (0.19/0.35) <0.001 | 0.290 (0.21/0.37) <0.001 | 0.234 (0.16/0.32) <0.001 |
| Urinary potassium/creatinine ratio, log mmol/g | 0.150 (0.08/0.22) <0.001 | 0.116 (0.04/0.16) 0.002 | 0.144 (0.07/0.21) <0.001 |
| Urinary phosphorus/creatinine ratio, log mg/g | 0.075 (0.01/0.14) 0.034 | 0.055 (−0.02/0.12) n.s. | 0.074 (0.01/0.15) 0.035 |
| Serum 25−OH vitamin D, log ng/mL | −0.058 (−0.11/0.01) not significant | −0.075 (−0.14/−0.02) 0.017 | −0.055 (−0.11/0.01) not significant |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirillo, M.; Cavallo, P.; Zulli, E.; Villa, R.; Veneziano, R.; Costanzo, S.; Magnacca, S.; Di Castelnuovo, A.; Iacoviello, L.; on behalf of Moli-Sani Study Investigators. Sodium Intake and Proteinuria/Albuminuria in the Population—Observational, Cross-Sectional Study. Nutrients 2021, 13, 1255. https://doi.org/10.3390/nu13041255
Cirillo M, Cavallo P, Zulli E, Villa R, Veneziano R, Costanzo S, Magnacca S, Di Castelnuovo A, Iacoviello L, on behalf of Moli-Sani Study Investigators. Sodium Intake and Proteinuria/Albuminuria in the Population—Observational, Cross-Sectional Study. Nutrients. 2021; 13(4):1255. https://doi.org/10.3390/nu13041255
Chicago/Turabian StyleCirillo, Massimo, Pierpaolo Cavallo, Enrico Zulli, Rachele Villa, Rosangela Veneziano, Simona Costanzo, Sara Magnacca, Augusto Di Castelnuovo, Licia Iacoviello, and on behalf of Moli-Sani Study Investigators. 2021. "Sodium Intake and Proteinuria/Albuminuria in the Population—Observational, Cross-Sectional Study" Nutrients 13, no. 4: 1255. https://doi.org/10.3390/nu13041255