
Evaluation of E-Health Applications for Paediatric Patients with Refractory Epilepsy and Maintained on Ketogenic Diet

 ,
,  , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Caregivers
2.3. Questionnaire
2.4. Booklets
2.5. Website
2.6. App
2.7. Videos
2.8. Statistical Analysis
3. Results
3.1. Characterisation of Paediatric Patients and Their Families
3.2. The Design of an Italian Website about the Ketogenic Diet
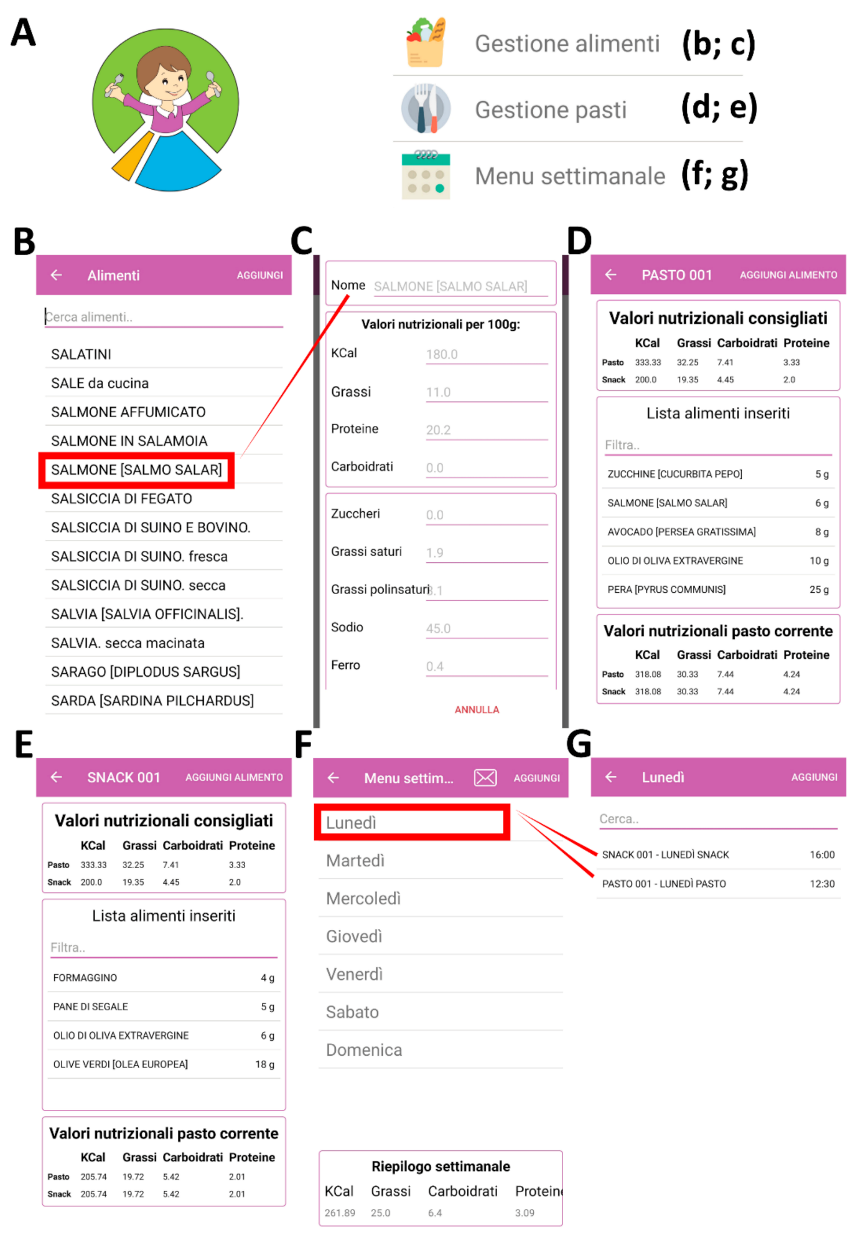
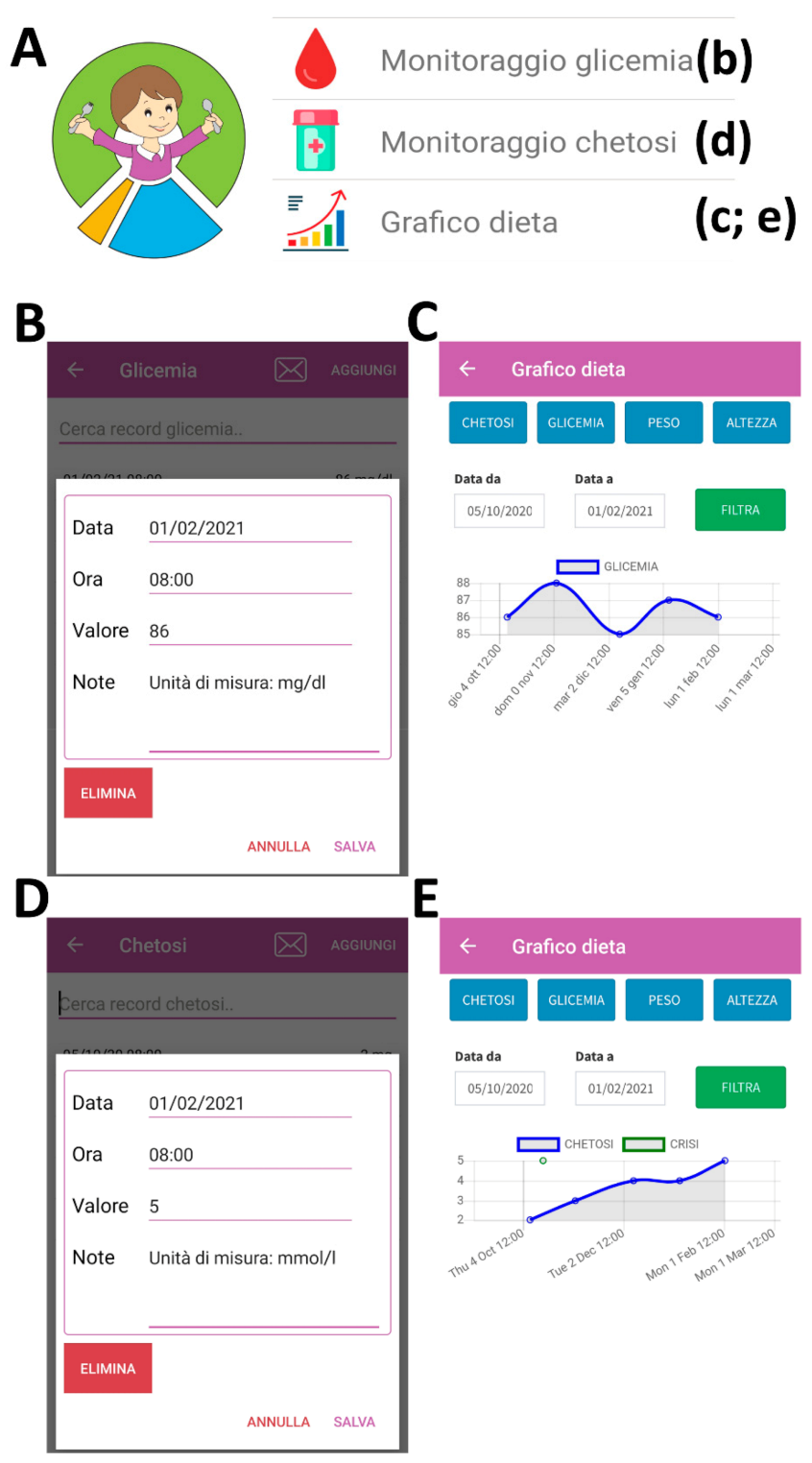
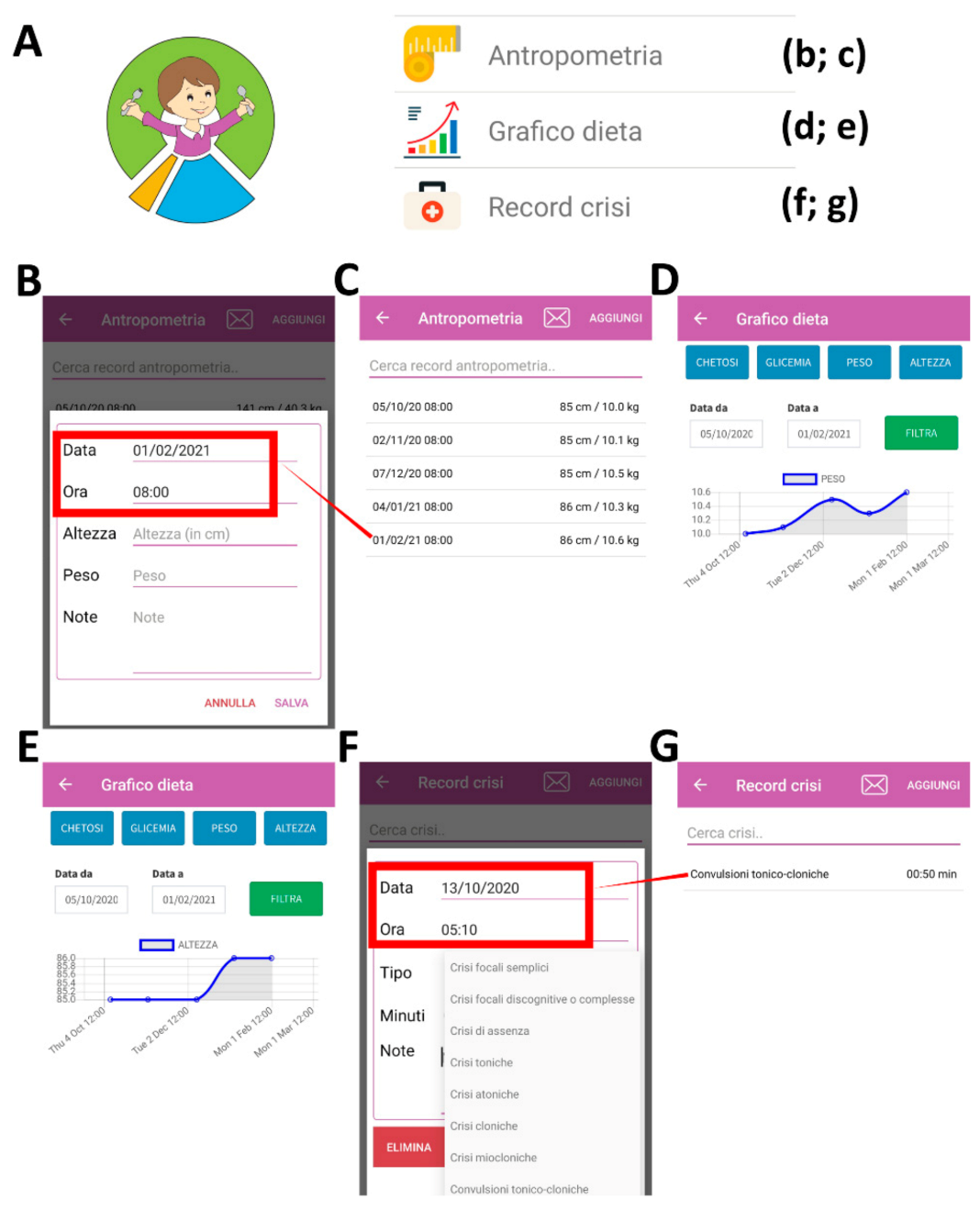
3.3. The Design of an Italian App for the Management of the Ketogenic Diet
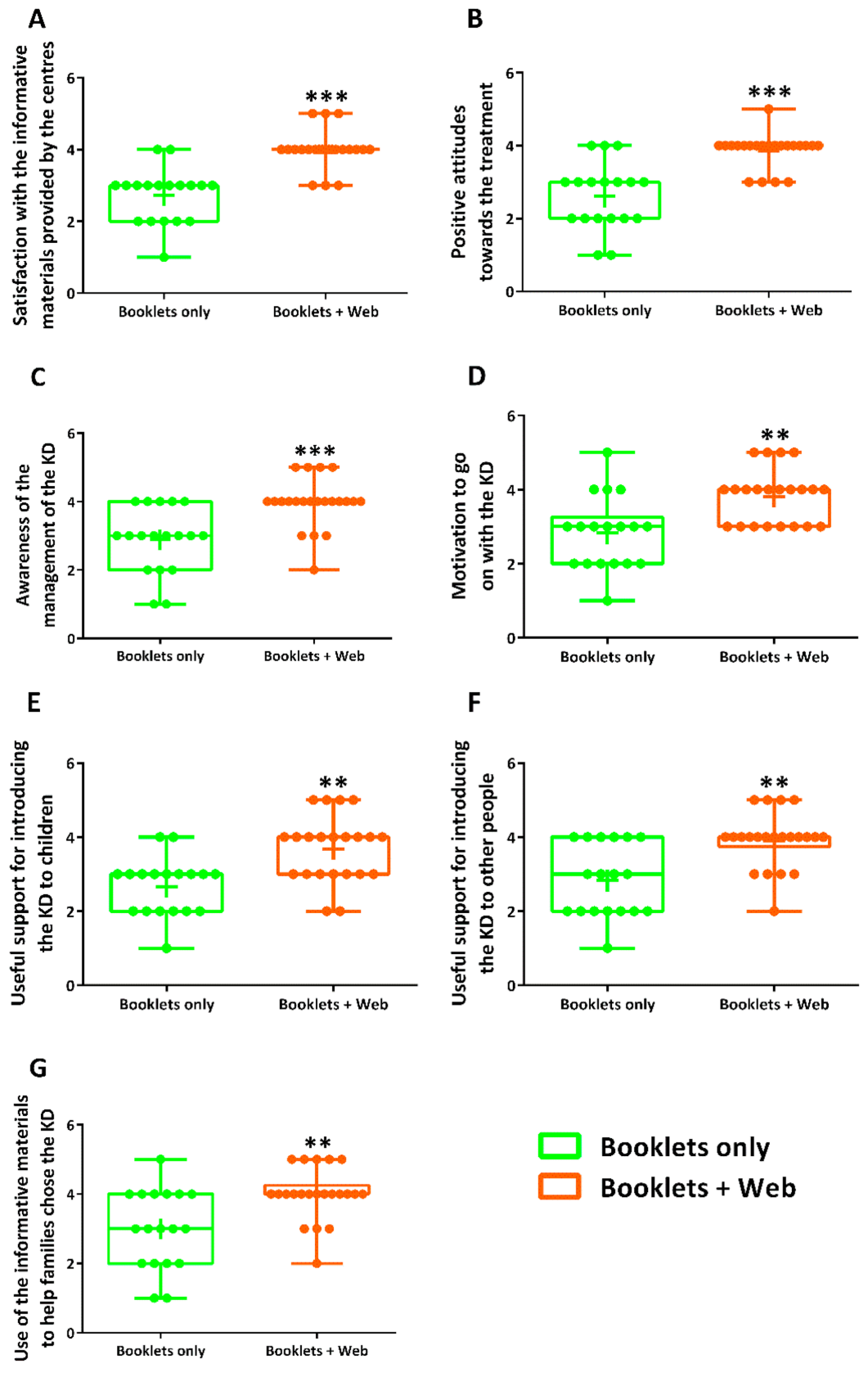
3.4. Different Channels of Communication through Which Caregivers Had Received Information about the Ketogenic Diet
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blaya, J.A.; Fraser, H.S.F.; Holt, B. E-Health Technologies Show Promise in Developing Countries. Health Aff. 2010, 29, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Ricci, G.; Baldanzi, S.; Seidita, F.; Proietti, C.; Carlini, F.; Peviani, S.; Antonini, G.; Vianello, A.; Siciliano, G.; Musumeci, O.; et al. A Mobile App for Patients with Pompe Disease and Its Possible Clinical Applications. Neuromuscul. Disord. 2018, 28, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Semprino, M.; Fasulo, L.; Fortini, S.; Martorell Molina, C.I.; González, L.; Ramos, P.A.; Martínez, C.; Caraballo, R. Telemedicine, Drug-Resistant Epilepsy, and Ketogenic Dietary Therapies: A Patient Survey of a Pediatric Remote-Care Program during the COVID-19 Pandemic. Epilepsy Behav. 2020, 112, 107493. [Google Scholar] [CrossRef] [PubMed]
- Lo, M.D.; Gospe, S.M. Telemedicine and Child Neurology. J. Child. Neurol. 2019, 34, 22–26. [Google Scholar] [CrossRef]
- Liu, X.; Wang, R.; Zhou, D.; Hong, Z. Feasibility and Acceptability of Smartphone Applications for Seizure Self-Management in China: Questionnaire Study among People with Epilepsy. Epilepsy Behav. 2016, 55, 57–61. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Glidden, A.M.; Holloway, M.R.; Birbeck, G.L.; Schwamm, L.H. Teleneurology and Mobile Technologies: The Future of Neurological Care. Nat. Rev. Neurol. 2018, 14, 285–297. [Google Scholar] [CrossRef]
- Kossoff, E.H.; Turner, Z.; Adams, J.; Bessone, S.K.; Avallone, J.; McDonald, T.J.W.; Diaz-Arias, L.; Barron, B.J.; Vizthum, D.; Cervenka, M.C. Ketogenic Diet Therapy Provision in the COVID-19 Pandemic: Dual-Center Experience and Recommendations. Epilepsy Behav. 2020, 111, 107181. [Google Scholar] [CrossRef]
- Kondylakis, H.; Katehakis, D.G.; Kouroubali, A.; Logothetidis, F.; Triantafyllidis, A.; Kalamaras, I.; Votis, K.; Tzovaras, D. COVID-19 Mobile Apps: A Systematic Review of the Literature. J. Med. Internet Res. 2020, 22, e23170. [Google Scholar] [CrossRef]
- Ross, J.; Stevenson, F.; Lau, R.; Murray, E. Factors That Influence the Implementation of E-Health: A Systematic Review of Systematic Reviews (an Update). Implement. Sci. 2016, 11, 1–12. [Google Scholar] [CrossRef]
- Pandher, P.S.; Bhullar, K.K. Smartphone Applications for Seizure Management. Health Inform. J. 2016, 22, 209–220. [Google Scholar] [CrossRef]
- Le, S.; Shafer, P.O.; Bartfeld, E.; Fisher, R.S. An Online Diary for Tracking Epilepsy. Epilepsy Behav. 2011, 22, 705–709. [Google Scholar] [CrossRef]
- Zarnowska, I.M. Therapeutic Use of the Ketogenic Diet in Refractory Epilepsy: What We Know and What Still Needs to Be Learned. Nutrients 2020, 12, 2616. [Google Scholar] [CrossRef]
- Wells, J.; Swaminathan, A.; Paseka, J.; Hanson, C. Efficacy and Safety of a Ketogenic Diet in Children and Adolescents with Refractory Epilepsy—A Review. Nutrients 2020, 12, 1809. [Google Scholar] [CrossRef]
- Martin-McGill, K.J.; Bresnahan, R.; Levy, R.G.; Cooper, P.N. Ketogenic Diets for Drug-Resistant Epilepsy. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Pasca, L.; Varesio, C.; Ferraris, C.; Guglielmetti, M.; Trentani, C.; Tagliabue, A.; Veggiotti, P.; De Giorgis, V. Families’ Perception of Classic Ketogenic Diet Management in Acute Medical Conditions: A Web-Based Survey. Nutrients 2020, 12, 2920. [Google Scholar] [CrossRef]
- Zini, E.M.; Tagliabue, A.; Trentani, C.; Ferraris, C.; Boninsegna, R.; Quaglini, S.; Lanzola, G. An MHealth Application for Educating and Monitoring Patients Treated with a Ketogenic Diet Regimen. Stud. Health Technol. Inf. 2018, 247, 481–485. [Google Scholar]
- Marchiò, M.; Roli, L.; Lucchi, C.; Costa, A.M.; Borghi, M.; Iughetti, L.; Trenti, T.; Guerra, A.; Biagini, G. Ghrelin Plasma Levels After 1 Year of Ketogenic Diet in Children with Refractory Epilepsy. Front. Nutr. 2019, 6, 112. [Google Scholar] [CrossRef] [PubMed]
- Marchiò, M.; Roli, L.; Giordano, C.; Trenti, T.; Guerra, A.; Biagini, G. Decreased Ghrelin and Des-Acyl Ghrelin Plasma Levels in Patients Affected by Pharmacoresistant Epilepsy and Maintained on the Ketogenic Diet. Clin. Nutr. 2018, 38, 954–957. [Google Scholar] [CrossRef]
- Leone, A.; De Amicis, R.; Lessa, C.; Tagliabue, A.; Trentani, C.; Ferraris, C.; Battezzati, A.; Veggiotti, P.; Foppiani, A.; Ravella, S.; et al. Food and Food Products on the Italian Market for Ketogenic Dietary Treatment of Neurological Diseases. Nutrients 2019, 11, 1104. [Google Scholar] [CrossRef]
- Ferraris, C.; Guglielmetti, M.; Tamagni, E.; Trentani, C.; De Giorgis, V.; Pasca, L.; Varesio, C.; Ferraro, O.E.; Tagliabue, A. Use of Remote Monitoring by E-Mail for Long-Term Management of the Classic Ketogenic Diet. Nutrients 2020, 12, 1833. [Google Scholar] [CrossRef]
- Cavalieri, S.; Marchiò, M.; Bondi, M.; Biagini, G. Assessing Caregiver Informative Materials on the Ketogenic Diet in Italy: A Textual Ethnographic Approach. Token 2019. [Google Scholar] [CrossRef]
- Karakis, I.; Cole, A.J.; Montouris, G.D.; San Luciano, M.; Meador, K.J.; Piperidou, C. Caregiver Burden in Epilepsy: Determinants and Impact. Epilepsy Res. Treat. 2014, 2014, 1–9. [Google Scholar] [CrossRef]
- Loblaw, D.A.; Bezjak, A.; Bunston, T. Development and Testing of a Visit-Specific Patient Satisfaction Questionnaire: The Princess Margaret Hospital Satisfaction with Doctor Questionnaire. J. Clin. Oncol. 1999, 17, 1931–1938. [Google Scholar] [CrossRef]
- Weissenstein, A.; Straeter, A.; Villalon, G.; Luchter, E.; Bittmann, S. Parent Satisfaction with a Pediatric Practice in Germany: A Questionnaire-Based Study. Ital. J. Pediatrics 2011, 37, 31. [Google Scholar] [CrossRef]
- Lin, K.-L.; Lin, J.-J.; Wang, H.-S. Application of Ketogenic Diets for Pediatric Neurocritical Care. Biomed. J. 2020, 43, 218–225. [Google Scholar] [CrossRef]
- Kossoff, E.H.; Zupec-Kania, B.A.; Auvin, S.; Ballaban-Gil, K.R.; Christina Bergqvist, A.G.; Blackford, R.; Buchhalter, J.R.; Caraballo, R.H.; Cross, J.H.; Dahlin, M.G.; et al. Optimal Clinical Management of Children Receiving Dietary Therapies for Epilepsy: Updated Recommendations of the International Ketogenic Diet Study Group. Epilepsia Open 2018, 3, 175–192. [Google Scholar] [CrossRef]
- Testa, F.; Marchiò, M.; Belli, M.; Giovanella, S.; Ligabue, G.; Cappelli, G.; Biagini, G.; Magistroni, R. A Pilot Study to Evaluate Tolerability and Safety of a Modified Atkins Diet in ADPKD Patients. PharmaNutrition 2019, 9, 100154. [Google Scholar] [CrossRef]
- Rezaei, S.; Abdurahman, A.A.; Saghazadeh, A.; Badv, R.S.; Mahmoudi, M. Short-Term and Long-Term Efficacy of Classical Ketogenic Diet and Modified Atkins Diet in Children and Adolescents with Epilepsy: A Systematic Review and Meta-Analysis. Nutr. Neurosci. 2019, 22, 317–334. [Google Scholar] [CrossRef]
- Kossoff, E.; Cervenka, M. Ketogenic Dietary Therapy Controversies for Its Second Century. Epilepsy Curr. 2020, 20, 125–129. [Google Scholar] [CrossRef]
- Costa, A.-M.; Lucchi, C.; Malkoç, A.; Rustichelli, C.; Biagini, G. Relationship between Delta Rhythm, Seizure Occurrence and Allopregnanolone Hippocampal Levels in Epileptic Rats Exposed to the Rebound Effect. Pharmaceuticals 2021, 14, 127. [Google Scholar] [CrossRef]
- Lucchi, C.; Marchiò, M.; Caramaschi, E.; Giordano, C.; Giordano, R.; Guerra, A.; Biagini, G. Electrographic Changes Accompanying Recurrent Seizures under Ketogenic Diet Treatment. Pharmaceuticals 2017, 10, 82. [Google Scholar] [CrossRef]
- Goswami, J.N.; Sharma, S. Current Perspectives on The Role of The Ketogenic Diet in Epilepsy Management. Neuropsychiatr. Dis. Treat. 2019, 15, 3273–3285. [Google Scholar] [CrossRef]
- Li, H.; Jauregui, J.L.; Fenton, C.; Chee, C.M.; Bergqvist, A.G.C. Epilepsy Treatment Simplified through Mobile Ketogenic Diet Planning. J. Mob. Technol. Med. 2014, 3, 11–15. [Google Scholar] [CrossRef]
- Tao, D.; LeRouge, C.; Smith, K.J.; De Leo, G. Defining Information Quality into Health Websites: A Conceptual Framework of Health Website Information Quality for Educated Young Adults. JMIR Hum. Factors 2017, 4, e25. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, A.-M.; Marchiò, M.; Bruni, G.; Bernabei, S.M.; Cavalieri, S.; Bondi, M.; Biagini, G. Evaluation of E-Health Applications for Paediatric Patients with Refractory Epilepsy and Maintained on Ketogenic Diet. Nutrients 2021, 13, 1240. https://doi.org/10.3390/nu13041240
Costa A-M, Marchiò M, Bruni G, Bernabei SM, Cavalieri S, Bondi M, Biagini G. Evaluation of E-Health Applications for Paediatric Patients with Refractory Epilepsy and Maintained on Ketogenic Diet. Nutrients. 2021; 13(4):1240. https://doi.org/10.3390/nu13041240
Chicago/Turabian StyleCosta, Anna-Maria, Maddalena Marchiò, Giulia Bruni, Silvia Maria Bernabei, Silvia Cavalieri, Marina Bondi, and Giuseppe Biagini. 2021. "Evaluation of E-Health Applications for Paediatric Patients with Refractory Epilepsy and Maintained on Ketogenic Diet" Nutrients 13, no. 4: 1240. https://doi.org/10.3390/nu13041240
APA StyleCosta, A.-M., Marchiò, M., Bruni, G., Bernabei, S. M., Cavalieri, S., Bondi, M., & Biagini, G. (2021). Evaluation of E-Health Applications for Paediatric Patients with Refractory Epilepsy and Maintained on Ketogenic Diet. Nutrients, 13(4), 1240. https://doi.org/10.3390/nu13041240