

Effects of Adding Extracorporeal Shockwave Therapy (ESWT) to Platelet-Rich Plasma (PRP) among Patients with Rotator Cuff Partial Tear: A Prospective Randomized Comparative Study

 ,
,  , , , , ,
, , , , ,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
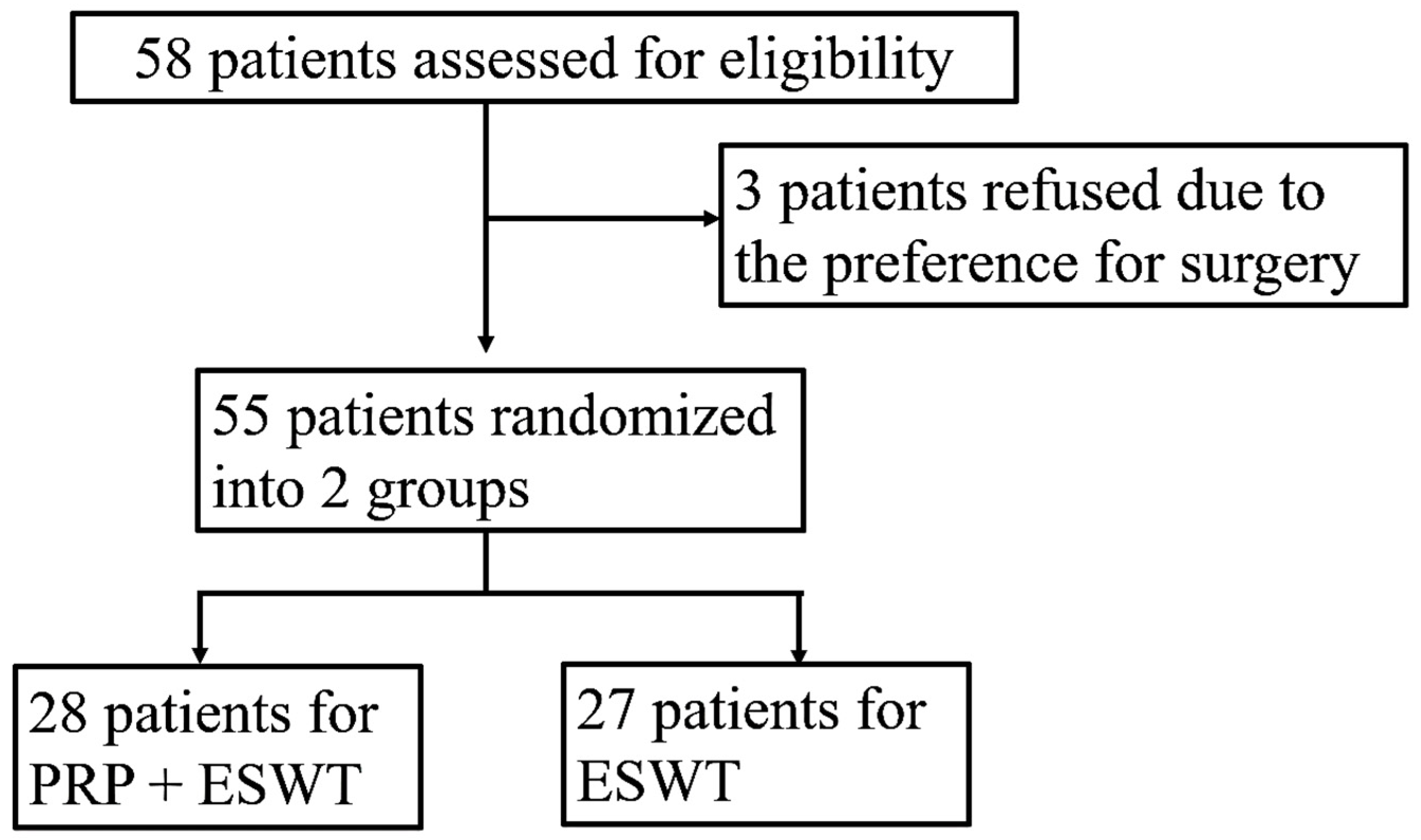
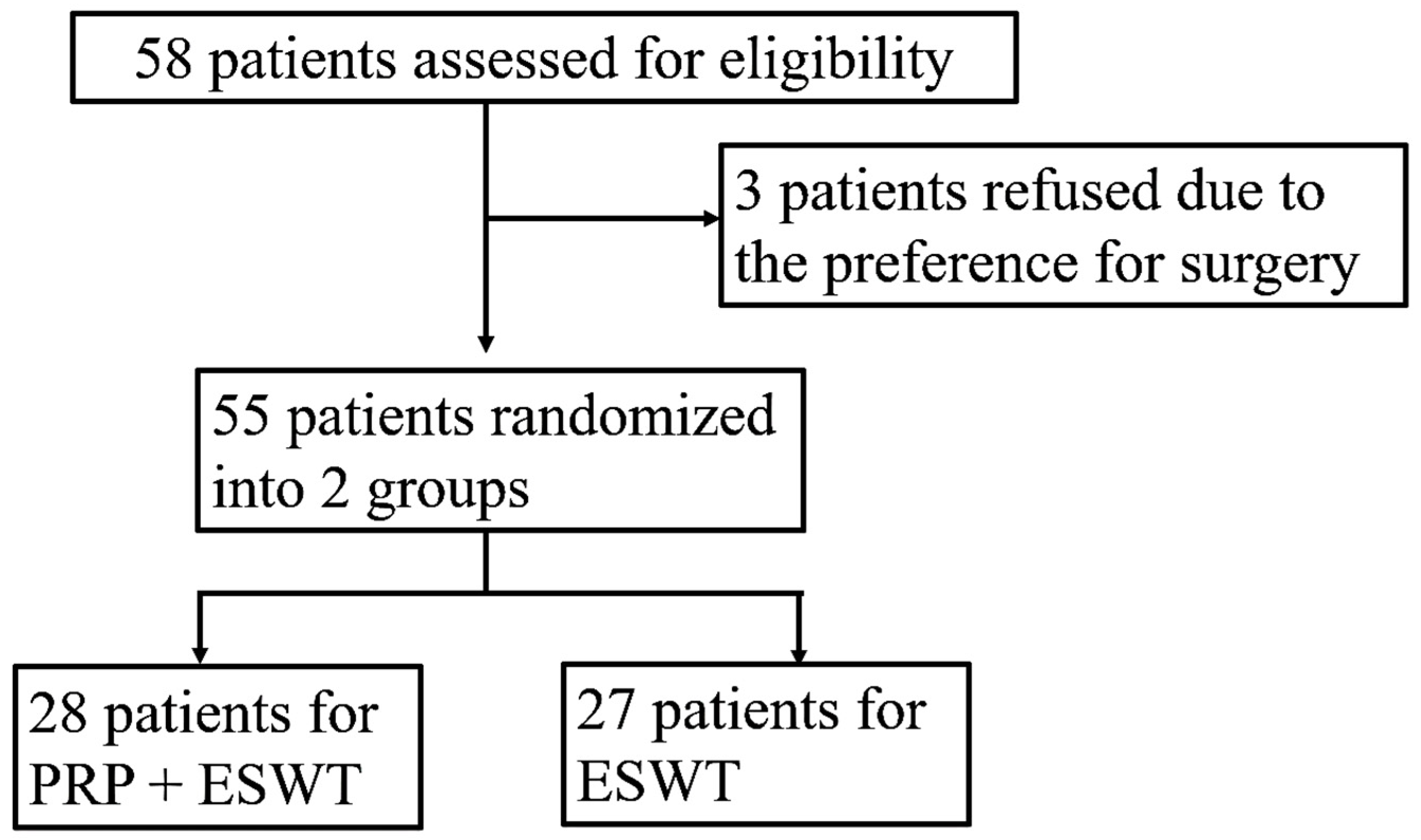
2.1. Recruitment of Participants
2.2. Imaging Diagnosis of Rotator Cuff (RC) Lesions
2.3. Platelet-Rich Plasma (PRP) Injection
2.4. Extracorporeal Shockwave (ESWT) Therapy
2.5. Clinical Assessments
2.6. Assessments of Isobaric Tag for Relative and Absolute Quantitation (iTRAQ)
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yamaura, K.; Mifune, Y.; Inui, A.; Nishimoto, H.; Mukohara, S.; Yoshikawa, T.; Shinohara, I.; Kato, T.; Furukawa, T.; Hoshino, Y.; et al. Sex Is Associated with the Success or Failure of Manipulation Alone for Joint Stiffness Associated with Rotator Cuff Repair. J. Clin. Med. 2022, 11, 7192. [Google Scholar] [CrossRef]
- Ko, J.-Y.; Chen, S.-H.; Wu, R.-W.; Wu, K.-T.; Hsu, C.-C.; Kuo, S.-J. Decreased Expression of Leptin among Patients with Shoulder Stiffness. Life 2022, 12, 1588. [Google Scholar] [CrossRef] [PubMed]
- Pogorzelski, J.; Rupp, M.-C.; Scheiderer, B.; Lacheta, L.; Schliemann, B.; Schanda, J.; Heuberer, P.; Schneider, M.; Hackl, M.; Aga Shoulder Committee-Rotator Cuff; et al. Management of Irreparable Posterosuperior Rotator Cuff Tears—A Current Concepts Review and Proposed Treatment Algorithm by the AGA Shoulder Committee. J. Pers. Med. 2023, 13, 191. [Google Scholar] [CrossRef] [PubMed]
- Fieseler, G.; Laudner, K.; Cornelius, J.; Schulze, S.; Delank, K.-S.; Schwesig, R. Longitudinal Analysis of the ASES and Constant–Murley Scores, and the Internal Rotation/Shift and Jobe Tests following Arthroscopic Repair of Supraspinatus Lesions. J. Pers. Med. 2023, 13, 1304. [Google Scholar] [CrossRef]
- Zhao, J.; Luo, M.; Liang, G.; Wu, M.; Pan, J.; Zeng, L.-F.; Yang, W.; Liu, J. Risk Factors for Supraspinatus Tears: A Meta-analysis of Observational Studies. Orthop. J. Sports Med. 2021, 9. [Google Scholar] [CrossRef]
- Liu, J.; Dai, S.; Deng, H.; Qiu, D.; Liu, L.; Li, M.; Chen, Z.; Kang, J.; Tao, J. Evaluation of the prognostic value of the anatomical characteristics of the bony structures in the shoulder in bursal-sided partial-thickness rotator cuff tears. Front. Public Health 2023, 11, 1189003. [Google Scholar] [CrossRef]
- De Castro, R.L.B.; Antonio, B.P.; Giovannetti, G.A.; Annichino-Bizzacchi, J.M. Total Healing of a Partial Rupture of the Supraspinatus Tendon Using Barbotage Technique Associated with Platelet-Rich Plasma: A Randomized, Controlled, and Double-Blind Clinical Trial. Biomedicines 2023, 11, 1849. [Google Scholar] [CrossRef] [PubMed]
- Strauss, E.J.; Salata, M.J.; Kercher, J.; Barker, J.U.; McGill, K.; Bach, B.R., Jr.; Romeo, A.A.; Verma, N.N. The Arthroscopic Management of Partial-Thickness Rotator Cuff Tears: A Systematic Review of the Literature. Arthroscopy 2011, 27, 568–580. [Google Scholar] [CrossRef]
- Popov, V.L.; Poliakov, A.M.; Pakhaliuk, V.I. In silico evaluation of the mechanical stimulation effect on the regenerative rehabilitation for the articular cartilage local defects. Front. Med. 2023, 10, 1134786. [Google Scholar] [CrossRef]
- Notarnicola, A.; Ladisa, I.; Lanzilotta, P.; Bizzoca, D.; Covelli, I.; Bianchi, F.P.; Maccagnano, G.; Farì, G.; Moretti, B. Shock Waves and Therapeutic Exercise in Greater Trochanteric Pain Syndrome: A Prospective Randomized Clinical Trial with Cross-Over. J. Pers. Med. 2023, 13, 976. [Google Scholar] [CrossRef]
- Simplicio, C.L.; Purita, J.; Murrell, W.; Santos, G.S.; dos Santos, R.G.; Lana, J. Extracorporeal shock wave therapy mechanisms in musculoskeletal regenerative medicine. J. Clin. Orthop. Trauma 2020, 11, S309–S318. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.-Y.; Siu, K.-K.; Wang, F.-S.; Wang, C.-J.; Chou, W.-Y.; Huang, C.-C.; Kuo, S.-J. The Therapeutic Effects of Extracorporeal Shock Wave Therapy (ESWT) on the Rotator Cuff Lesions with Shoulder Stiffness: A Prospective Randomized Study. BioMed Res. Int. 2020, 2020, 6501714. [Google Scholar] [CrossRef] [PubMed]
- Shams, A.; El-Sayed, M.; Gamal, O.; Ewes, W. Subacromial injection of autologous platelet-rich plasma versus corticosteroid for the treatment of symptomatic partial rotator cuff tears. Eur. J. Orthop. Surg. Traumatol. 2016, 26, 837–842. [Google Scholar] [CrossRef]
- Kuo, S.-J.; Siu, K.-K.; Wu, K.-T.; Ko, J.-Y.; Wang, F.-S. The Differential Systemic Biological Effects between Computer Navigation and Conventional Total Knee Arthroplasty (TKA) Surgeries: A Prospective Study. J. Pers. Med. 2022, 12, 1835. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.J.; Chou, W.Y.; Hsu, C.C.; Chang-Chien, G.P.; Lin, S.F.; Siu, K.K.; Tsai, T.C.; Ko, J.Y.; Sun, Y.C. Systemic effects of platelet-rich plasma local injection on serum and urinary anabolic metabolites: A prospective randomized study. Chin. J. Physiol. 2020, 63, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Natali, S.; Screpis, D.; Patania, E.; De Berardinis, L.; Benoni, A.; Piovan, G.; Iacono, V.; Magnan, B.; Gigante, A.P.; Zorzi, C. Efficacy and Long-Term Outcomes of Intra-Articular Autologous Micro-Fragmented Adipose Tissue in Individuals with Glenohumeral Osteoarthritis: A 36-Month Follow-Up Study. J. Pers. Med. 2023, 13, 1309. [Google Scholar] [CrossRef] [PubMed]
- Zaha, I.A.; Huniadi, A.; Bodog, F.; Seles, L.; Toma, M.C.; Maghiar, L.; Szulay-Bimbo, E.; Bodog, A.; Sachelarie, L.; Florea, M.; et al. Autologous Platelet-Rich Plasma (PRP) in Infertility—Infusion versus Injectable PRP. J. Pers. Med. 2023, 13, 1676. [Google Scholar] [CrossRef] [PubMed]
- Gregori, P.; Perricone, G.; Franceschetti, E.; Giurazza, G.; Papalia, G.F.; Zà, P.; Papalia, R. Allograft Prosthesis Composite (APC) for Proximal Humeral Bone Loss: Outcomes and Perspectives. J. Pers. Med. 2023, 13, 1301. [Google Scholar] [CrossRef]
- Kanto, K.; Lähdeoja, T.; Paavola, M.; Aronen, P.; Järvinen, T.L.N.; Jokihaara, J.; Ardern, C.L.; Karjalainen, T.V.; Taimela, S. Minimal important difference and patient acceptable symptom state for pain, Constant-Murley score and Simple Shoulder Test in patients with subacromial pain syndrome. BMC Med. Res. Methodol. 2021, 21, 45. [Google Scholar] [CrossRef]
- Wiese, S.; Reidegeld, K.A.; Meyer, H.E.; Warscheid, B. Protein labeling by iTRAQ: A new tool for quantitative mass spectrometry in proteome research. Proteomics 2007, 7, 340–350. [Google Scholar] [CrossRef]
- Omar, M.A.; Omran, M.M.; Farid, K.; Tabll, A.A.; Shahein, Y.E.; Emran, T.M.; Petrovic, A.; Lucic, N.R.; Smolic, R.; Kovac, T.; et al. Biomarkers for Hepatocellular Carcinoma: From Origin to Clinical Diagnosis. Biomedicines 2023, 11, 1852. [Google Scholar] [CrossRef]
- Yang, X.; Jiang, Z.; He, J.; Shen, L. iTRAQ-Based Quantitative Proteomics Unveils Protein Dynamics in the Root of Solanum melongena L. under Waterlogging Stress Conditions. Life 2023, 13, 1399. [Google Scholar] [CrossRef]
- Chiu, Y.-K.; Yin, T.; Lee, Y.-T.; Chen, S.-J.; Wang, Y.-C.; Ma, K.-H. Proteomic Profiling of Outer Membrane Vesicles Released by Escherichia coli LPS Mutants Defective in Heptose Biosynthesis. J. Pers. Med. 2022, 12, 1301. [Google Scholar] [CrossRef] [PubMed]
- Kusama, K.; Bai, R.; Matsuno, Y.; Ideta, A.; Sakurai, T.; Nagaoka, K.; Hori, M.; Imakawa, K. Characterization of Serum Metabolome and Proteome Profiles Identifies SNX5 Specific for Pregnancy Failure in Holstein Heifers. Life 2022, 12, 309. [Google Scholar] [CrossRef] [PubMed]
- Weng, K.-P.; Chien, K.-J.; Huang, S.-H.; Huang, L.-H.; Lin, P.-H.; Lin, Y.; Chang, W.-H.; Chen, C.-Y.; Li, S.-C. iTRAQ Proteomics Identified the Potential Biomarkers of Coronary Artery Lesion in Kawasaki Disease and In Vitro Studies Demonstrated That S100A4 Treatment Made HCAECs More Susceptible to Neutrophil Infiltration. Int. J. Mol. Sci. 2022, 23, 12770. [Google Scholar] [CrossRef]
- Unwin, R.D. Quantification of proteins by iTRAQ. Methods Mol. Biol. 2010, 658, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Li, S.-C.; Tsai, K.-W.; Huang, L.-H.; Weng, K.-P.; Chien, K.-J.; Lin, Y.; Tu, C.-Y.; Lin, P.-H. Serum proteins may facilitate the identification of Kawasaki disease and promote in vitro neutrophil infiltration. Sci. Rep. 2020, 10, 15645. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.-J.; Chen, C.-L.; Chen, S.-H.; Ko, J.-Y. Changes in Serum Bone Metabolism Markers after Living Donor Liver Transplantation (LDLT) and Their Association with Fracture Occurrences. Life 2023, 13, 1438. [Google Scholar] [CrossRef]
- Van Lent, P.L.; Grevers, L.; Blom, A.B.; Sloetjes, A.; Mort, J.S.; Vogl, T.; Nacken, W.; van den Berg, W.B.; Roth, J. Myeloid-related proteins S100A8/S100A9 regulate joint inflammation and cartilage destruction during antigen-induced arthritis. Ann. Rheum. Dis. 2008, 67, 1750–1758. [Google Scholar] [CrossRef]
- Averill, M.M.; Kerkhoff, C.; Bornfeldt, K.E. S100A8 and S100A9 in Cardiovascular Biology and Disease. Arter. Thromb. Vasc. Biol. 2012, 32, 223–229. [Google Scholar] [CrossRef]
- Chou, W.-Y.; Wang, C.-J.; Wu, K.-T.; Yang, Y.-J.; Cheng, J.-H.; Wang, S.-W. Comparative outcomes of extracorporeal shockwave therapy for shoulder tendinitis or partial tears of the rotator cuff in athletes and non-athletes: Retrospective study. Int. J. Surg. 2018, 51, 184–190. [Google Scholar] [CrossRef]
- Dankova, I.; Pyrgidis, N.; Tishukov, M.; Georgiadou, E.; Nigdelis, M.P.; Solomayer, E.-F.; Marcon, J.; Stief, C.G.; Hatzichristou, D. Efficacy and Safety of Platelet-Rich Plasma Injections for the Treatment of Female Sexual Dysfunction and Stress Urinary Incontinence: A Systematic Review. Biomedicines 2023, 11, 2919. [Google Scholar] [CrossRef]
- Everts, P.A.; Lana, J.F.; Onishi, K.; Buford, D.; Peng, J.; Mahmood, A.; Fonseca, L.F.; van Zundert, A.; Podesta, L. Angiogenesis and Tissue Repair Depend on Platelet Dosing and Bioformulation Strategies Following Orthobiological Platelet-Rich Plasma Procedures: A Narrative Review. Biomedicines 2023, 11, 1922. [Google Scholar] [CrossRef] [PubMed]
- Giaccari, L.G.; Coppolino, F.; Aurilio, C.; Pace, M.C.; Passavanti, M.B.; Pota, V.; Alicino, D.; Pulito, G.; Sansone, P. Pulsed Radiofrequency and Platelet Rich Plasma in Degenerative Joint Arthritis: Two Case Reports and Literature Analyses. Life 2023, 13, 1334. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Xing, F.; Yan, T.; Zhang, S.; Chen, F. Multiple Injections of Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Current Evidence in Randomized Controlled Trials. J. Pers. Med. 2023, 13, 429. [Google Scholar] [CrossRef]
- Ivković, A.; Glavčić, M.; Vuletić, F.; Janković, S. Core Decompression Combined with Intraosseous Autologous Conditioned Plasma Injections Decreases Pain and Improves Function in Patients with Symptomatic Knee Bone Marrow Lesions. Biomedicines 2023, 11, 1799. [Google Scholar] [CrossRef]
- Gupta, A.; Jeyaraman, M.; Potty, A.G. Leukocyte-Rich vs. Leukocyte-Poor Platelet-Rich Plasma for the Treatment of Knee Osteoarthritis. Biomedicines 2023, 11, 141. [Google Scholar] [CrossRef] [PubMed]
- Vali, S.; Saso, S.; Bracewell Milnes, T.; Nicopoullos, J.; Thum, M.-Y.; Smith, J.R.; Jones, B.P. The Clinical Application of Platelet-Rich Plasma in the Female Reproductive System: A Narrative Review. Life 2023, 13, 2348. [Google Scholar] [CrossRef]
- Machado, E.S.; Soares, F.P.; Vianna de Abreu, E.; de Souza, T.A.d.C.; Meves, R.; Grohs, H.; Ambach, M.A.; Navani, A.; de Castro, R.B.; Pozza, D.H.; et al. Systematic Review of Platelet-Rich Plasma for Low Back Pain. Biomedicines 2023, 11, 2404. [Google Scholar] [CrossRef]
- Saginova, D.; Tashmetov, E.; Kamyshanskiy, Y.; Tuleubayev, B.; Rimashevskiy, D. Evaluation of Bone Regenerative Capacity in Rabbit Femoral Defect Using Thermally Disinfected Bone Human Femoral Head Combined with Platelet-Rich Plasma, Recombinant Human Bone Morphogenetic Protein 2, and Zoledronic Acid. Biomedicines 2023, 11, 1729. [Google Scholar] [CrossRef]
- Vladulescu, D.; Scurtu, L.G.; Simionescu, A.A.; Scurtu, F.; Popescu, M.I.; Simionescu, O. Platelet-Rich Plasma (PRP) in Dermatology: Cellular and Molecular Mechanisms of Action. Biomedicines 2024, 12, 7. [Google Scholar] [CrossRef]
- Costa, F.R.R.; Santos, M.d.S.d.S.; Martins, R.A.A.; Costa, C.B.B.; Hamdan, P.C.C.; Silva, M.B.D.B.; Azzini, G.O.M.O.M.; Pires, L.; Menegassi, Z.; Santos, G.S.S.; et al. The Synergistic Effects of Hyaluronic Acid and Platelet-Rich Plasma for Patellar Chondropathy. Biomedicines 2024, 12, 6. [Google Scholar] [CrossRef]
- Tanpowpong, T.; Thepsoparn, M.; Numkarunarunrote, N.; Itthipanichpong, T.; Limskul, D.; Thanphraisan, P. Effects of Platelet-Rich Plasma in Tear Size Reduction in Partial-Thickness Tear of the Supraspinatus Tendon Compared to Corticosteroids Injection. Sports Med. Open 2023, 9, 11. [Google Scholar] [CrossRef]
- Von Wehren, L.; Blanke, F.; Todorov, A.; Heisterbach, P.; Sailer, J.; Majewski, M. The effect of subacromial injections of autologous conditioned plasma versus cortisone for the treatment of symptomatic partial rotator cuff tears. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3787–3792. [Google Scholar] [CrossRef] [PubMed]
- Damjanov, N.; Barac, B.; Colic, J.; Stevanovic, V.; Zekovic, A.; Tulic, G. The efficacy and safety of autologous conditioned serum (ACS) injections compared with betamethasone and placebo injections in the treatment of chronic shoulder joint pain due to supraspinatus tendinopathy: A prospective, randomized, double-blind, controlled study. Med. Ultrason. 2018, 20, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Sari, A.; Eroglu, A. Comparison of ultrasound-guided platelet-rich plasma, prolotherapy, and corticosteroid injections in rotator cuff lesions. J. Back Musculoskelet. Rehabil. 2020, 33, 387–396. [Google Scholar] [CrossRef]
- Cai, Y.U.; Sun, Z.; Liao, B.; Song, Z.; Xiao, T.; Zhu, P. Sodium Hyaluronate and Platelet-Rich Plasma for Partial-Thickness Rotator Cuff Tears. Med. Sci. Sports Exerc. 2019, 51, 227–233. [Google Scholar] [CrossRef]
- Oppenheim, J.J.; Yang, D. Alarmins: Chemotactic activators of immune responses. Curr. Opin. Immunol. 2005, 17, 359–365. [Google Scholar] [CrossRef]
- Yang, D.; Han, Z.; Oppenheim, J.J. Alarmins and immunity. Immunol. Rev. 2017, 280, 41–56. [Google Scholar] [CrossRef]
- Wolf, M.; Joseph, R.; Austermann, J.; Scharrnbeck-Davis, C.; Hermann, S.; Roth, J.; Vogl, T. S100A8/S100A9 Integrates F-Actin and Microtubule Dynamics to Prevent Uncontrolled Extravasation of Leukocytes. Biomedicines 2023, 11, 835. [Google Scholar] [CrossRef]
- Furci, F.; Murdaca, G.; Pelaia, C.; Imbalzano, E.; Pelaia, G.; Caminati, M.; Allegra, A.; Senna, G.; Gangemi, S. TSLP and HMGB1: Inflammatory Targets and Potential Biomarkers for Precision Medicine in Asthma and COPD. Biomedicines 2023, 11, 437. [Google Scholar] [CrossRef] [PubMed]
- Crowe, L.A.N.; McLean, M.; Kitson, S.M.; Melchor, E.G.; Patommel, K.; Cao, H.M.; Reilly, J.H.; Leach, W.J.; Rooney, B.P.; Spencer, S.J.; et al. S100A8 & S100A9: Alarmin mediated inflammation in tendinopathy. Sci. Rep. 2019, 9, 1463. [Google Scholar] [CrossRef] [PubMed]
- Aly, A.-R.; Rajasekaran, S.; Ashworth, N. Ultrasound-guided shoulder girdle injections are more accurate and more effective than landmark-guided injections: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1042–1049. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion criteria | Exclusion criteria |
| VAS score surpassing 3 | Rheumatic diseases |
| Positive impingement sign | Glenohumeral osteoarthritis |
| Pain during Hawkins’ test or empty can test | Full-thickness RC tear |
| MRI evidence of a supraspinatus lesion without a complete tear | Fractures |
| Pain and/or stiffness resistance to modifications in physical activity and/or therapeutic interventions under professional therapists for at least 3 months | Infections |
| Aged between 35 and 80 years | Neoplasms |
| Pregnancy | |
| Subacromial injections within the preceding 3 weeks | |
| Not submitting valid written informed consent |
| PRP + ESWT | PRP | p-Value | |
|---|---|---|---|
| Male/female | 8/20 | 13/14 | 0.135 |
| Age | 57.5 (53.0, 66.5) | 57.0 (51.5, 64.5) | 0.826 |
| Left/right | 11/17 | 11/16 | 0.912 |
| Body mass index | 24.2 (23.0, 26.8) | 24.4 (22.7, 28.4) | 0.976 |
| Medical comorbidities a | 10 | 14 | 0.228 |
| VAS | 5.5 (4.5,7.5) | 6.0 (4.0, 7.0) | 0.936 |
| 5.46 ± 2.17 | 5.37 ± 2.34 | ||
| Muscle power (lb) | 14.5 (12.0, 20.0) | 16.0 (13.5, 20.5) | 0.093 |
| 18.20 ± 9.45 | 21.10 ± 11.78 | ||
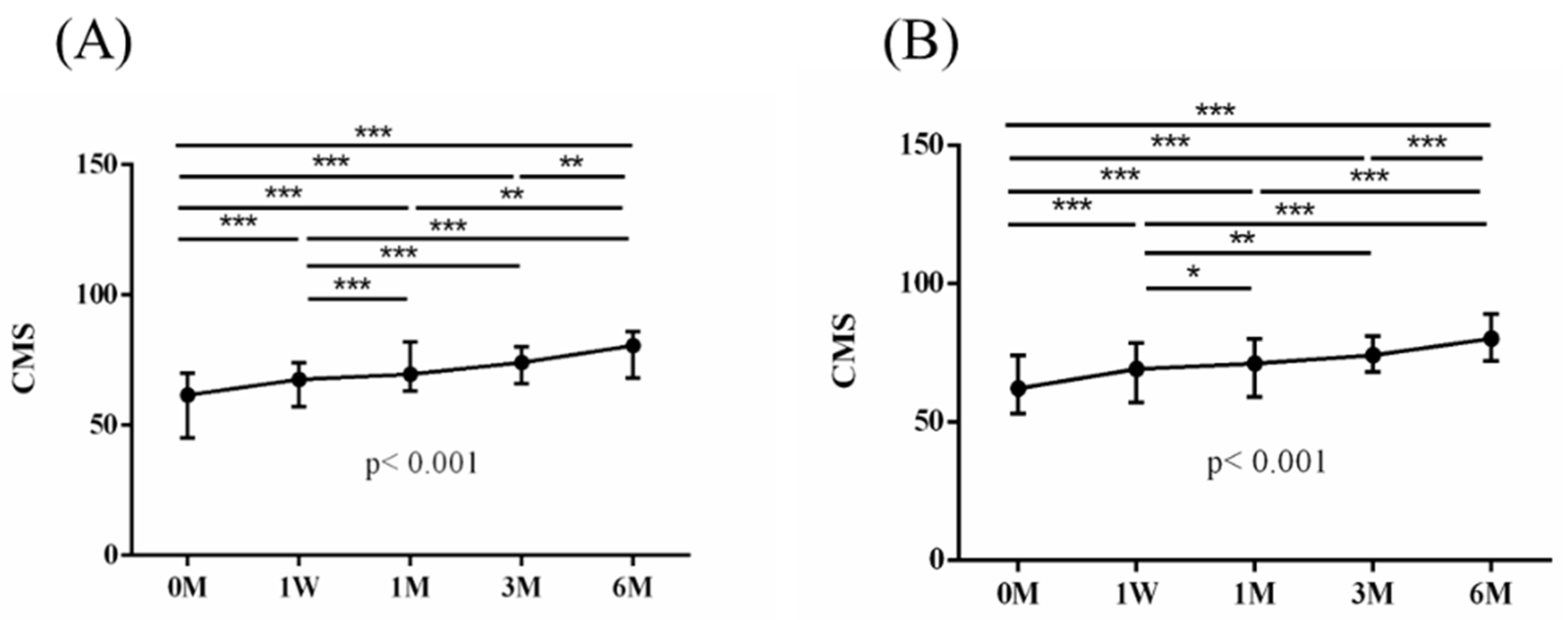
| CMS | 61.5 (45.0, 69.5) | 62.0 (53.0, 73.5) | 0.412 |
| 59.30 ± 14.20 | 62.69 | ||
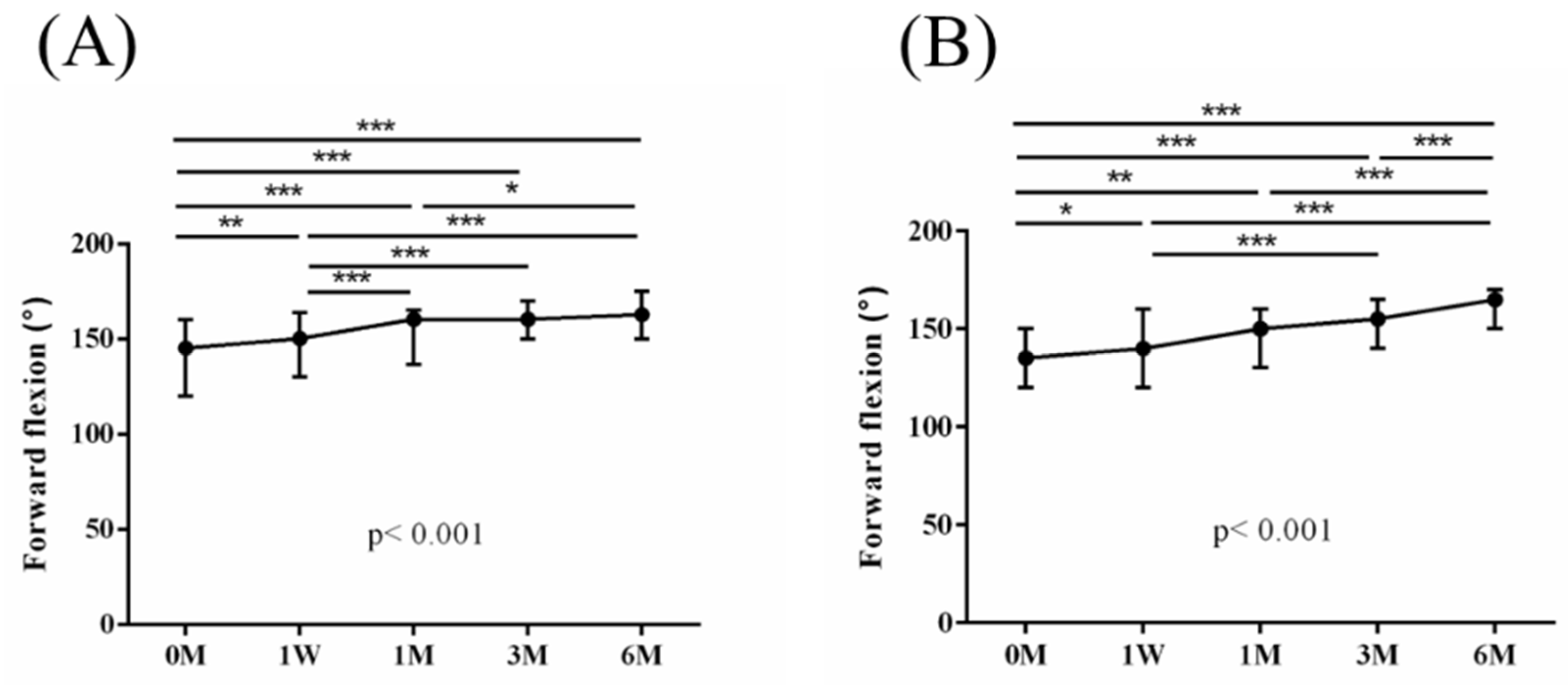
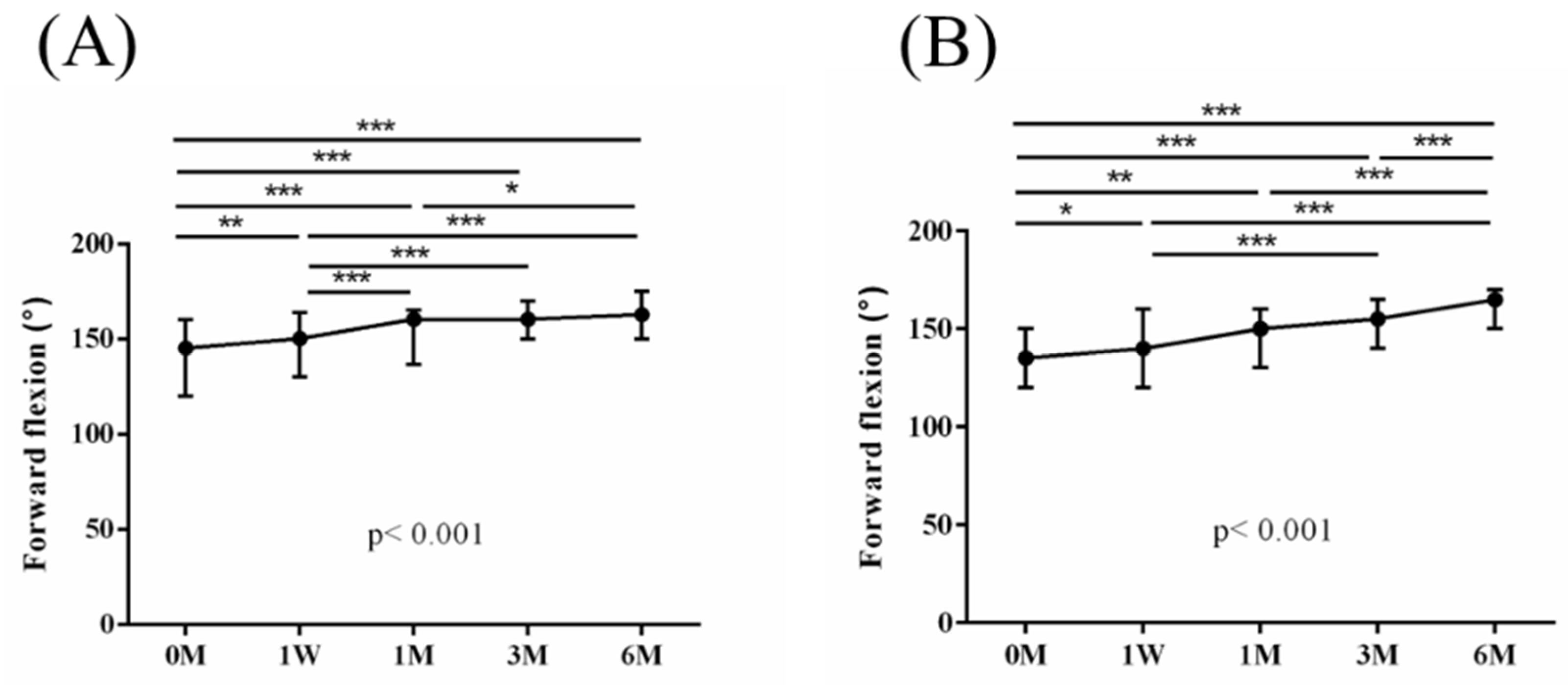
| Forward flexion (°) | 145.0 (120.0, 160.0) | 135.0 (120.0, 150.0) | 0.435 |
| 136.11 ± 26.94 | 133.70 | ||
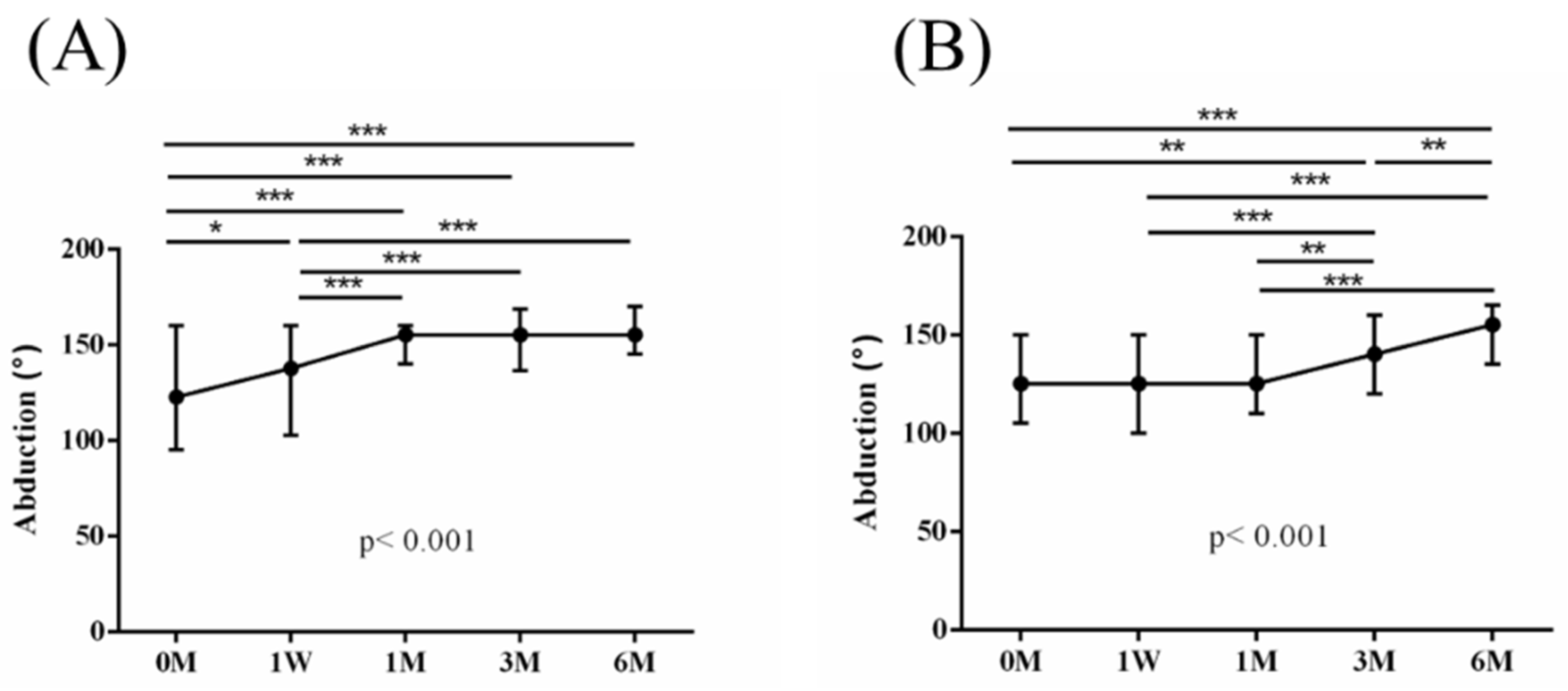
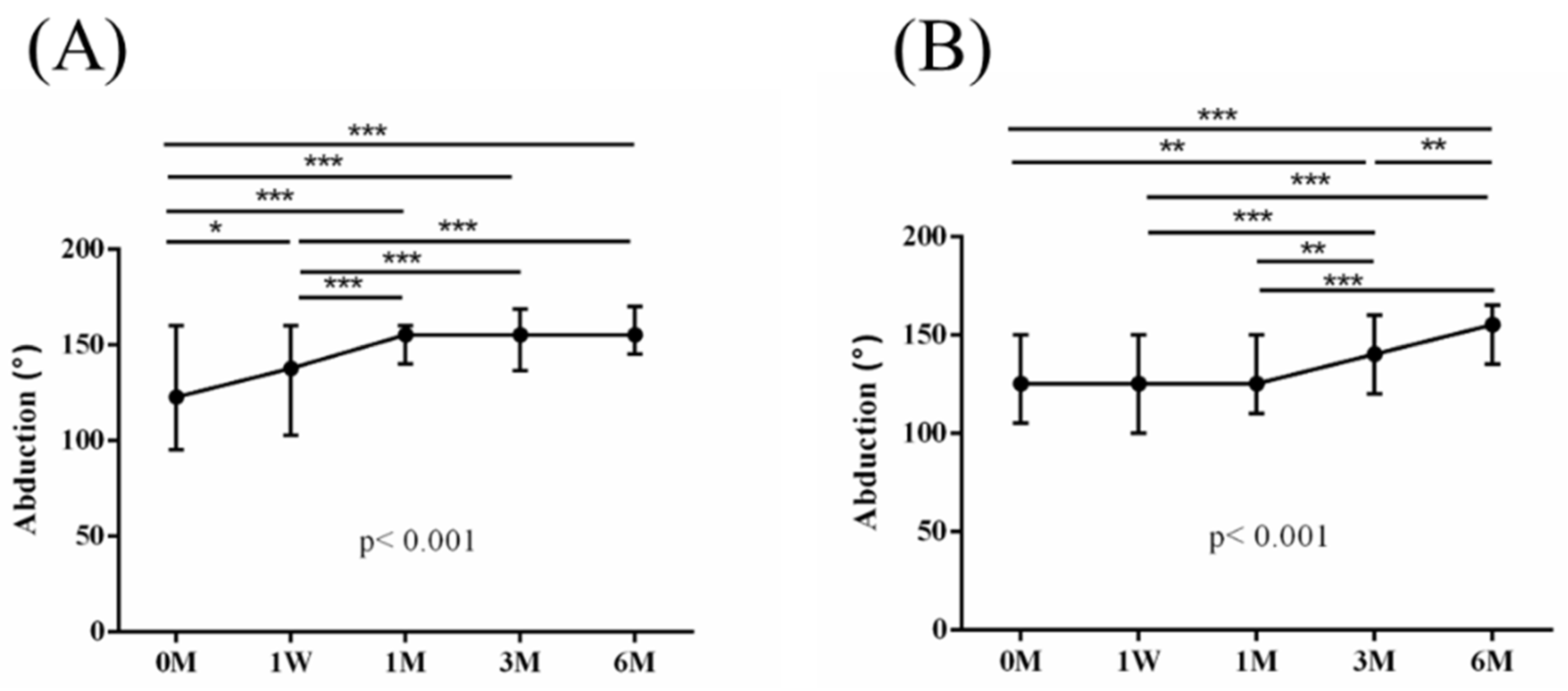
| Abduction (°) | 122.5 (95.0, 160.0) | 125.0 (107.5, 150.0) | 0.968 |
| 123.39 | 124.63 | ||
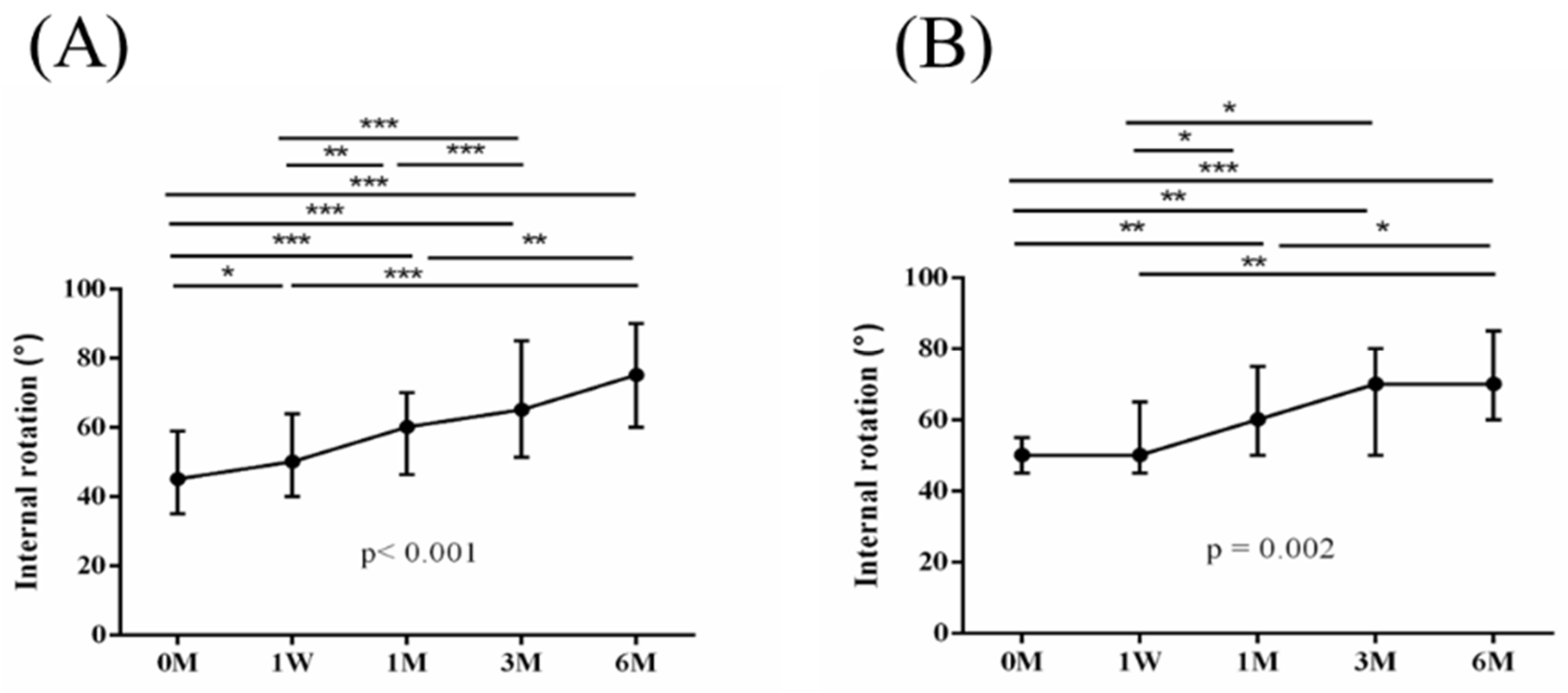
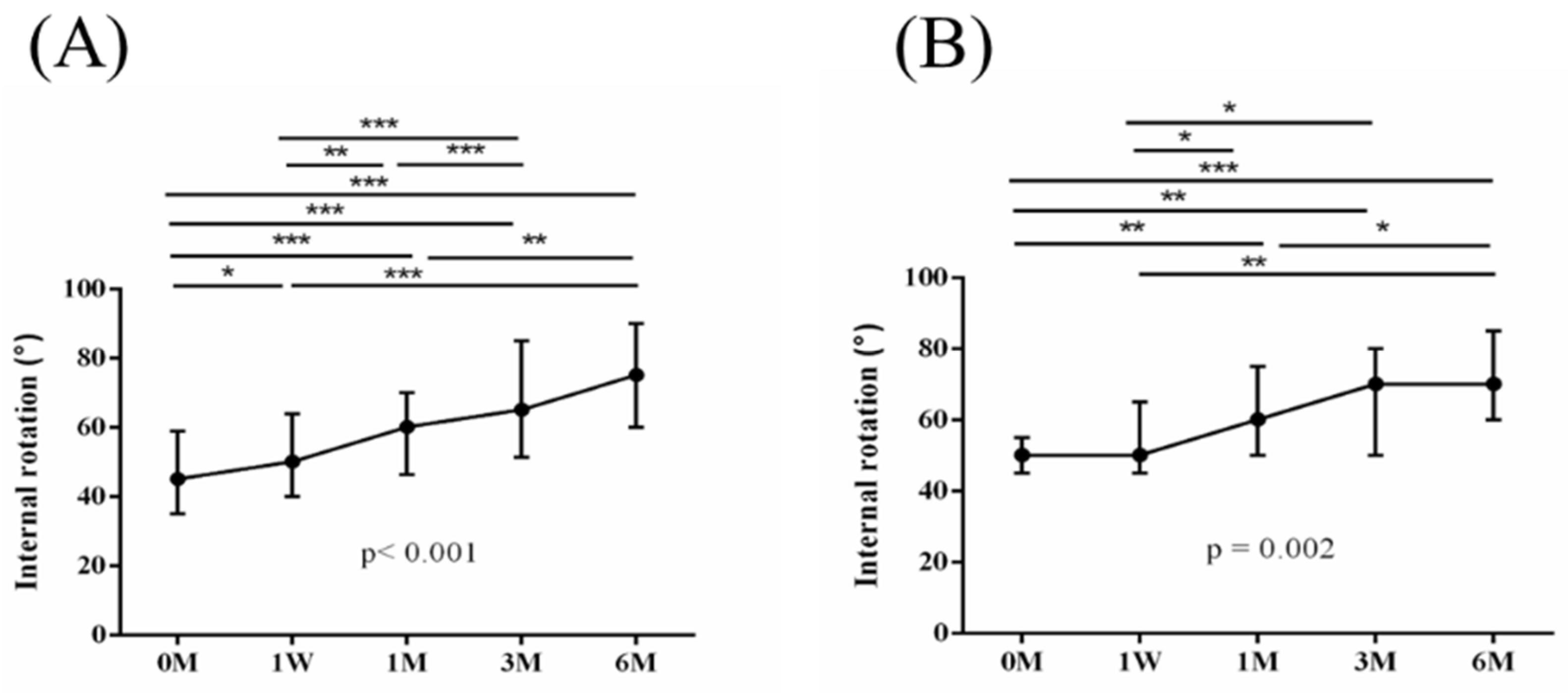
| IR (°) | 45.0 (35.0, 56.3) | 50.0 (45.0, 55.0) | 0.162 |
| 46.07 19.64 | 52.41 | ||
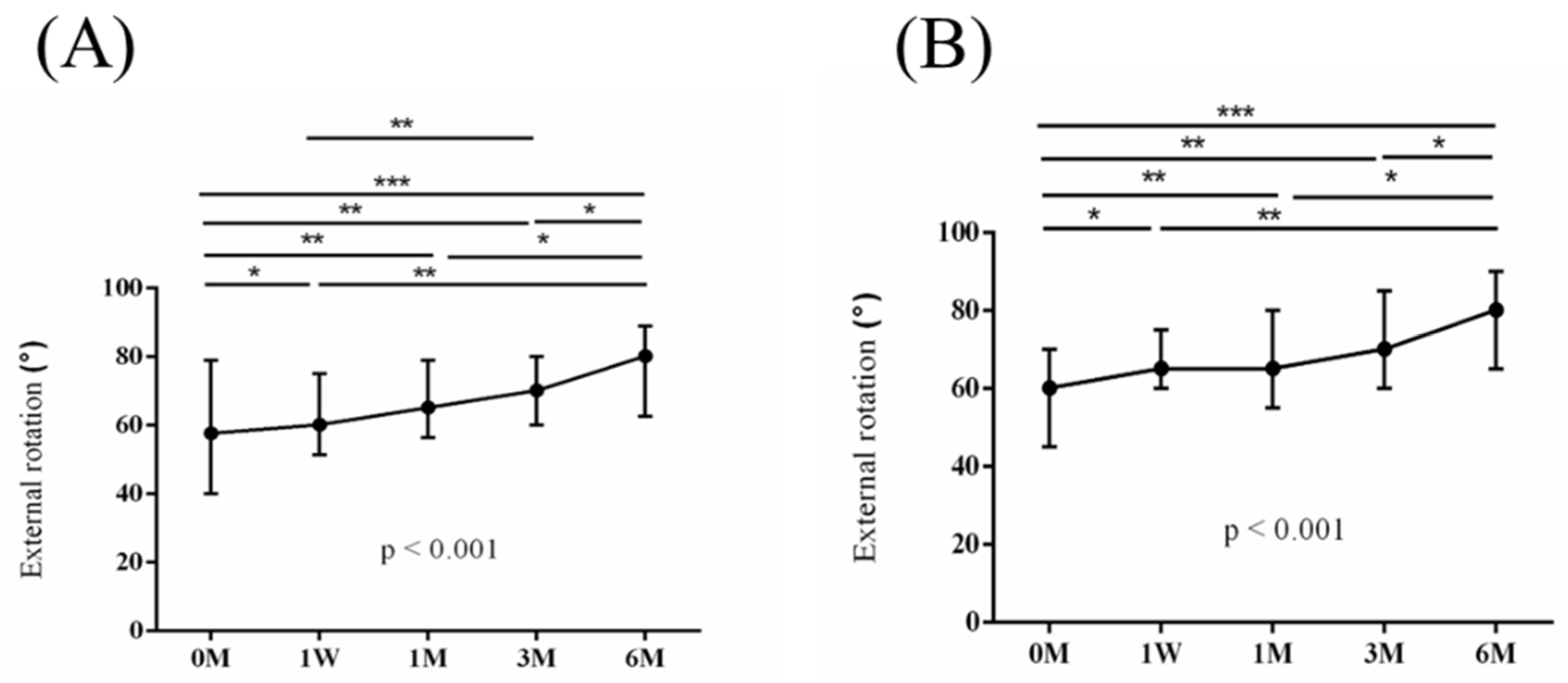
| ER (°) | 57.5 (40.0, 76.3) | 60.0 (47.5, 70.0) | 0.711 |
| 58.93 | 61.11 | ||
| SROM (°) | 390.0 (288.8, 425.0) | 385.0 (327.5, 425.0) | 0.992 |
| 365.36 ± 84.11 | 371.85 |
| PRP + ESWT | PRP | p-Value | |
|---|---|---|---|
| Baseline profiles | |||
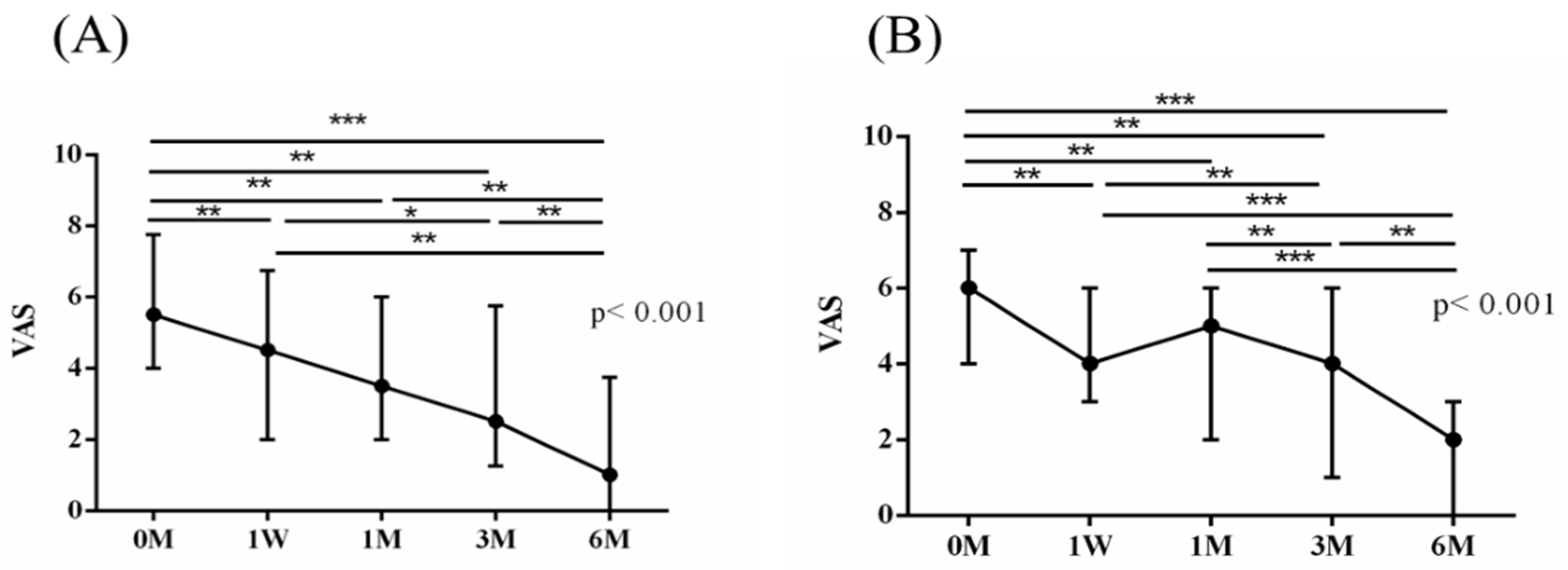
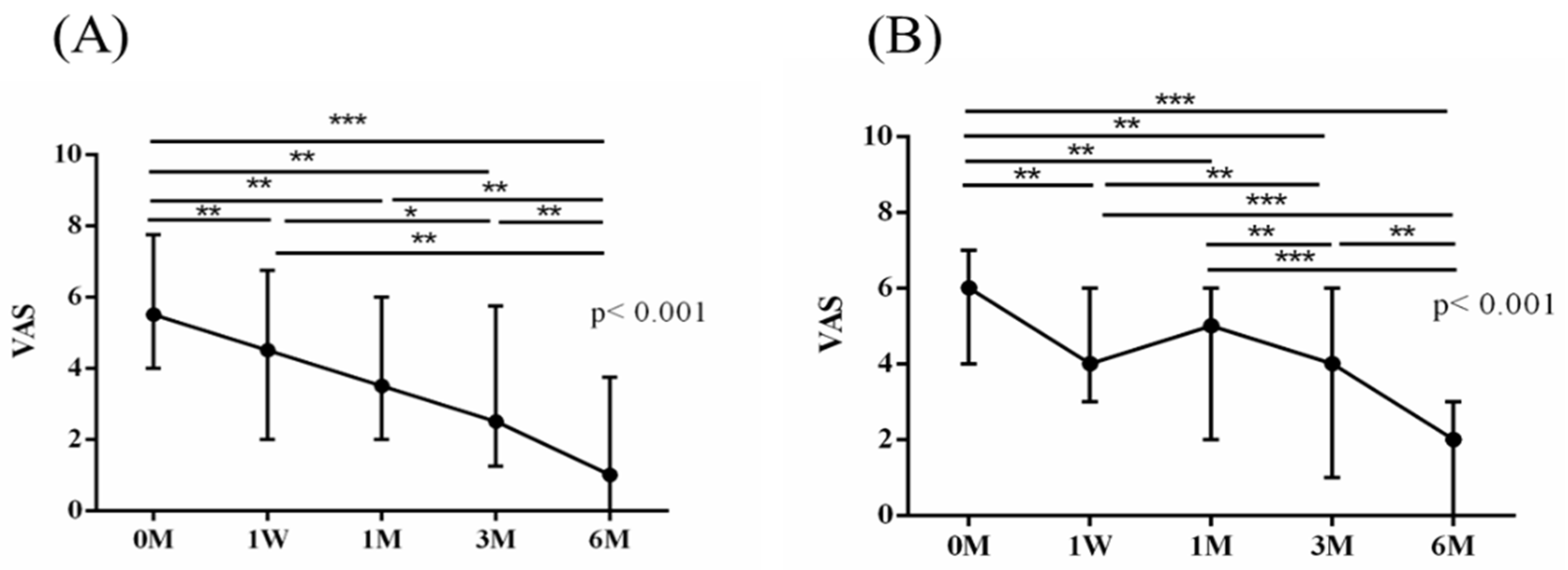
| VAS | 5.5 (4.5,7.5) | 6.0 (4.0, 7.0) | 0.936 |
| 5.46 2.17 | 5.37 2.34 | ||
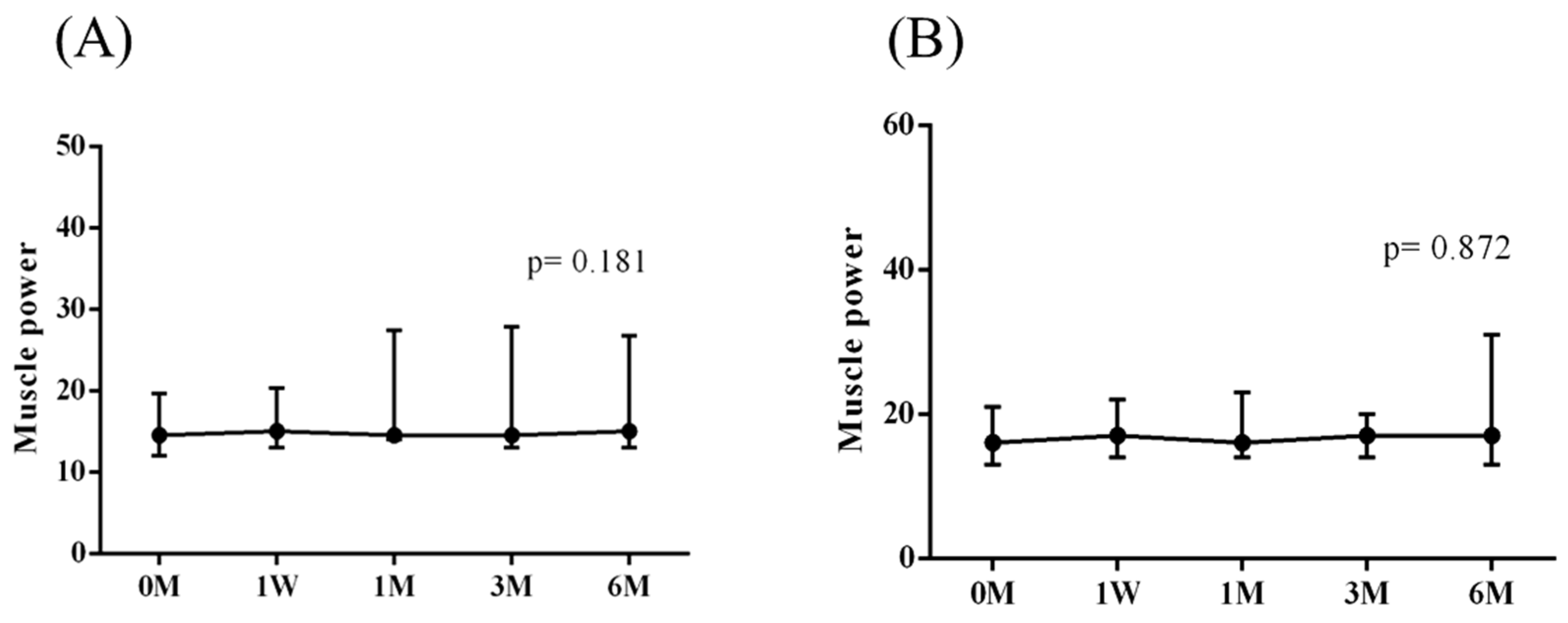
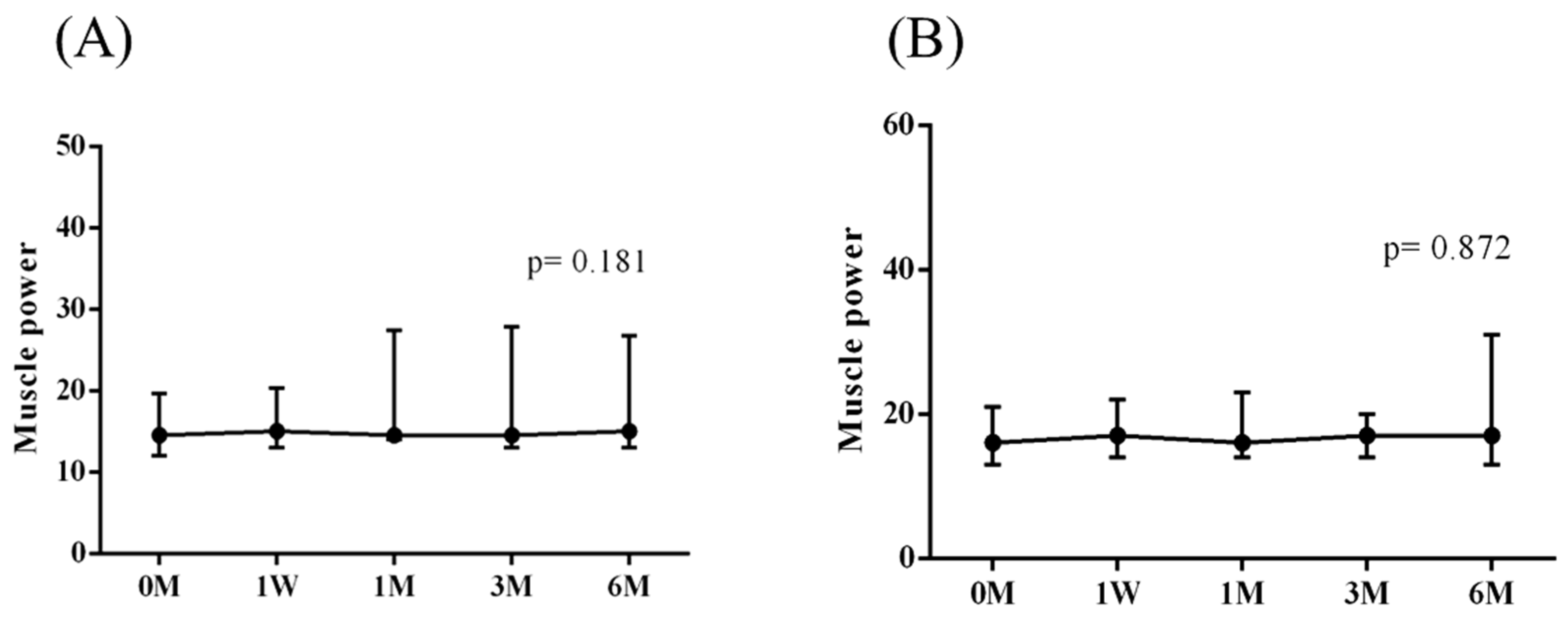
| Muscle power (lb) | 14.5 (12.0, 20.0) | 16.0 (13.5, 20.5) | 0.093 |
| 18.20 | 21.10 | ||
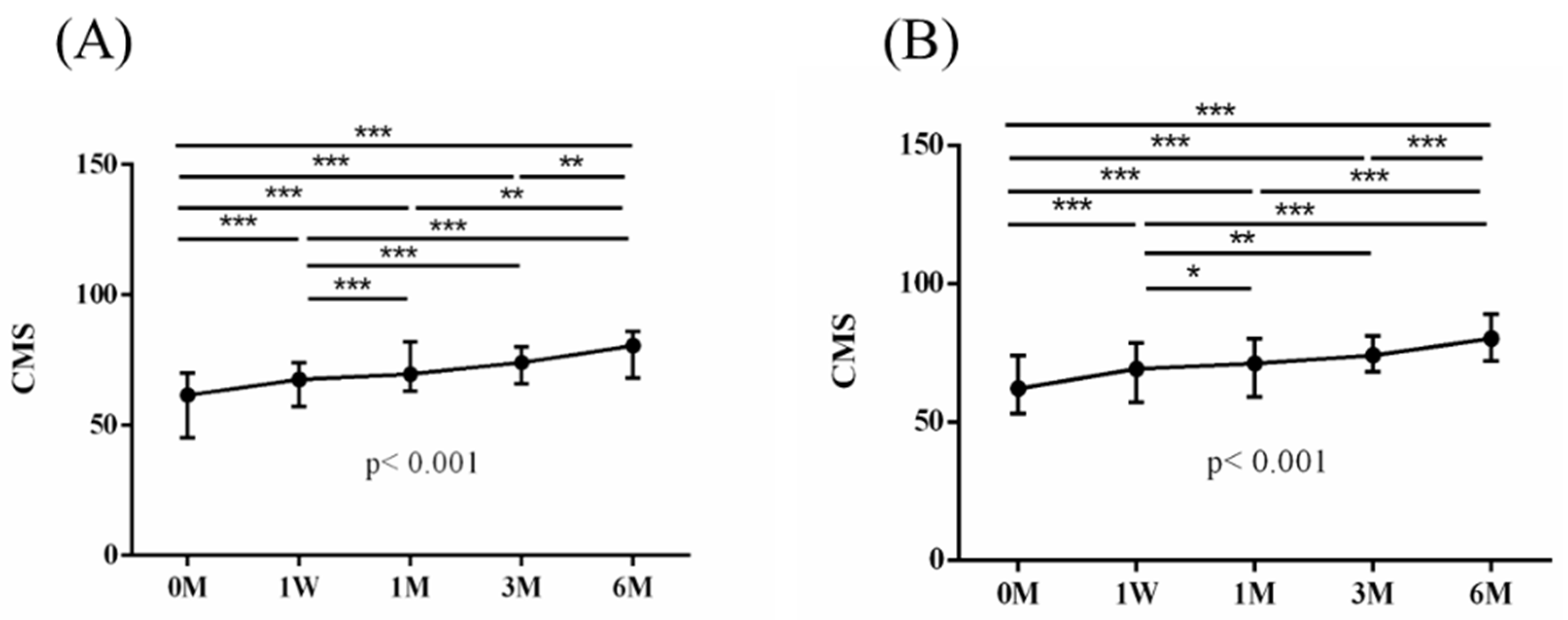
| CMS | 61.5 (45.0, 69.5) | 62.0 (53.0, 73.5) | 0.412 |
| 59.30 | 62.69 | ||
| One week | |||
| VAS | 5.5 (5.0, 10.0) | 5.0 (5.0, 10.0) | 0.976 |
| 4.32 2.44 | 4.26 2.33 | ||
| Muscle power (lb) | 15.0 (13.0, 20.4) | 17.0 (14.0, 22.0) | 0.234 |
| 18.88 | 21.64 ± 11.96 | ||
| CMS | 67.5 (57.0, 73.5) | 69.0 (57.0, 78.5) | 0.529 |
| 65.77 12.06 | 67.22 | ||
| One month | |||
| VAS | 3.5 (2.0, 6.0) | 5.0 (2.0, 6.0) | 0.787 |
| 3.89 2.40 | 4.11 2.52 | ||
| Muscle power (lb) | 14.5 (14.0, 27.0) | 16.0 (14.0, 23.0) | 0.322 |
| 19.67 9.42 | 21.55 11.01 | ||
| CMS | 69.5 (63.0, 81.5) | 71.0 (59.0, 80.0) | 0.697 |
| 71.29 | 69.69 | ||
| Three months | |||
| VAS | 2.5 (2.0, 5.0) | 4.0 (1.0, 6.0) | 0.873 |
| 3.57 2.53 | 3.48 2.59 | ||
| Muscle power (lb) | 14.5 (13.0, 26.0) | 17.0 (14.0, 20.0) | 0.313 |
| 19.26 | 21.09 ± 11.33 | ||
| CMS | 74.0 (67.3. 79.4) | 74.0 (68.5, 80.5) | 0.873 |
| 72.32 | 72.04 | ||
| Six months | |||
| VAS | 1.0 (0.5, 3.5) | 2.0 (0.5, 3.0) | 0.912 |
| 2.25 2.53 | 2.04 1.91 | ||
| Muscle power (lb) | 15.0 (13.0, 26.7) | 17.0 (13.5, 28/0) | 0.352 |
| 19.68 | 22.59 | ||
| CMS | 81.0 (71.0, 86.0) | 80.0 (72.0, 87.3) | 0.719 |
| 76.75 | 79.33 |
| MCID | PASS | |||
|---|---|---|---|---|
| PRP + ESWT | PRP | PRP + ESWT | PRP | |
| N = 28 | N = 27 | N = 28 | N = 27 | |
| 1 week | ||||
| VAS | 9 | 10 | 0 | 3 |
| CMS | 8 | 4 | 3 | 4 |
| 1 month | ||||
| VAS | 14 | 9 | 0 | 4 |
| CMS | 17 | 8 | 8 | 7 |
| 3 months | ||||
| VAS | 16 | 17 | 1 | 4 |
| CMS | 13 | 15 | 7 | 9 |
| 6 months | ||||
| VAS | 19 | 21 | 8 | 7 |
| CMS | 20 | 22 | 15 | 15 |
| PRP + ESWT | PRP | p-Value | |
|---|---|---|---|
| Baseline profiles | |||
| Forward flexion (°) | 145.0 (120.0, 160.0) | 135.0 (120.0, 150.0) | 0.435 |
| 136.11 | 133.70 | ||
| Abduction (°) | 122.5 (95.0, 160.0) | 125.0 (107.5, 150.0) | 0.968 |
| 123.39 | 124.63 | ||
| IR (°) | 45.0 (35.0, 56.3) | 50.0 (45.0, 55.0) | 0.162 |
| 46.07 19.64 | 52.41 | ||
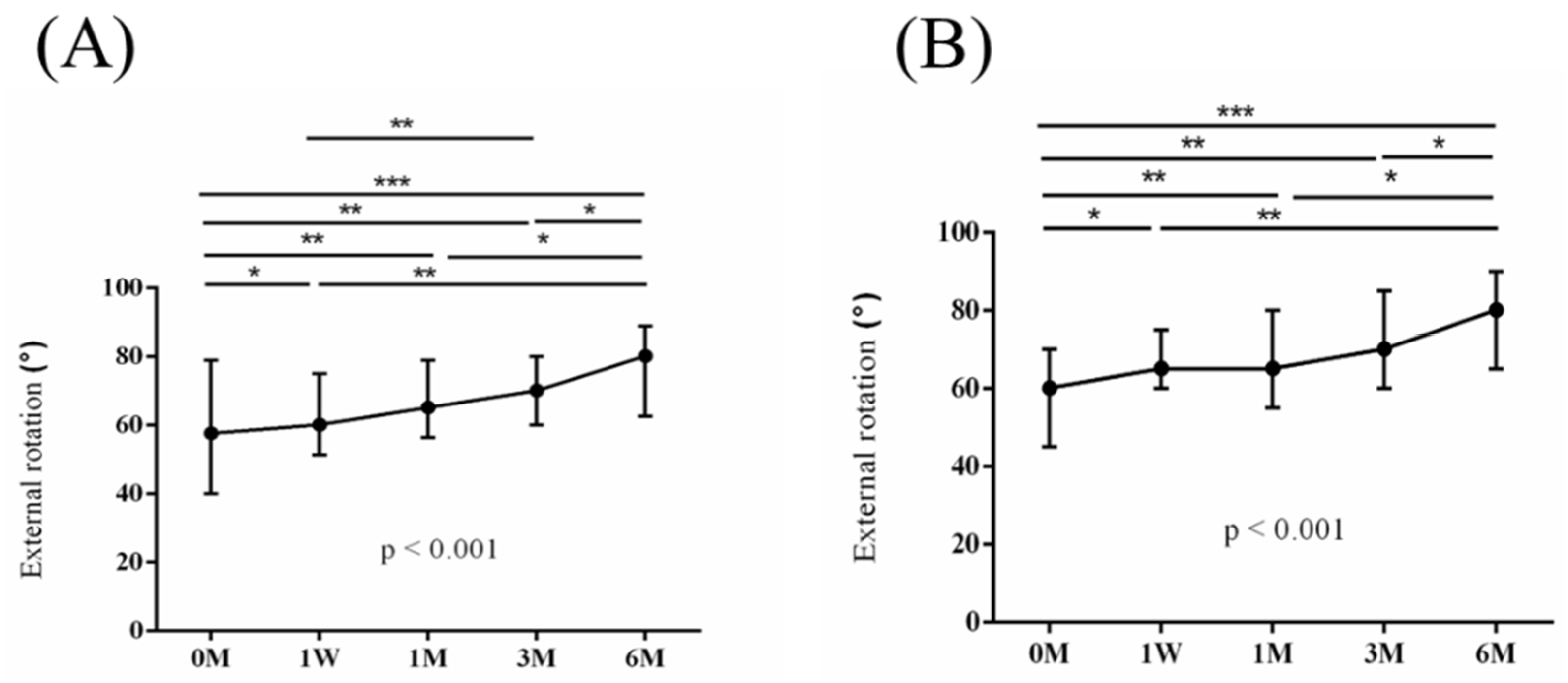
| ER (°) | 57.5 (40.0, 76.3) | 60.0 (47.5, 70.0) | 0.711 |
| 58.93 | 61.11 | ||
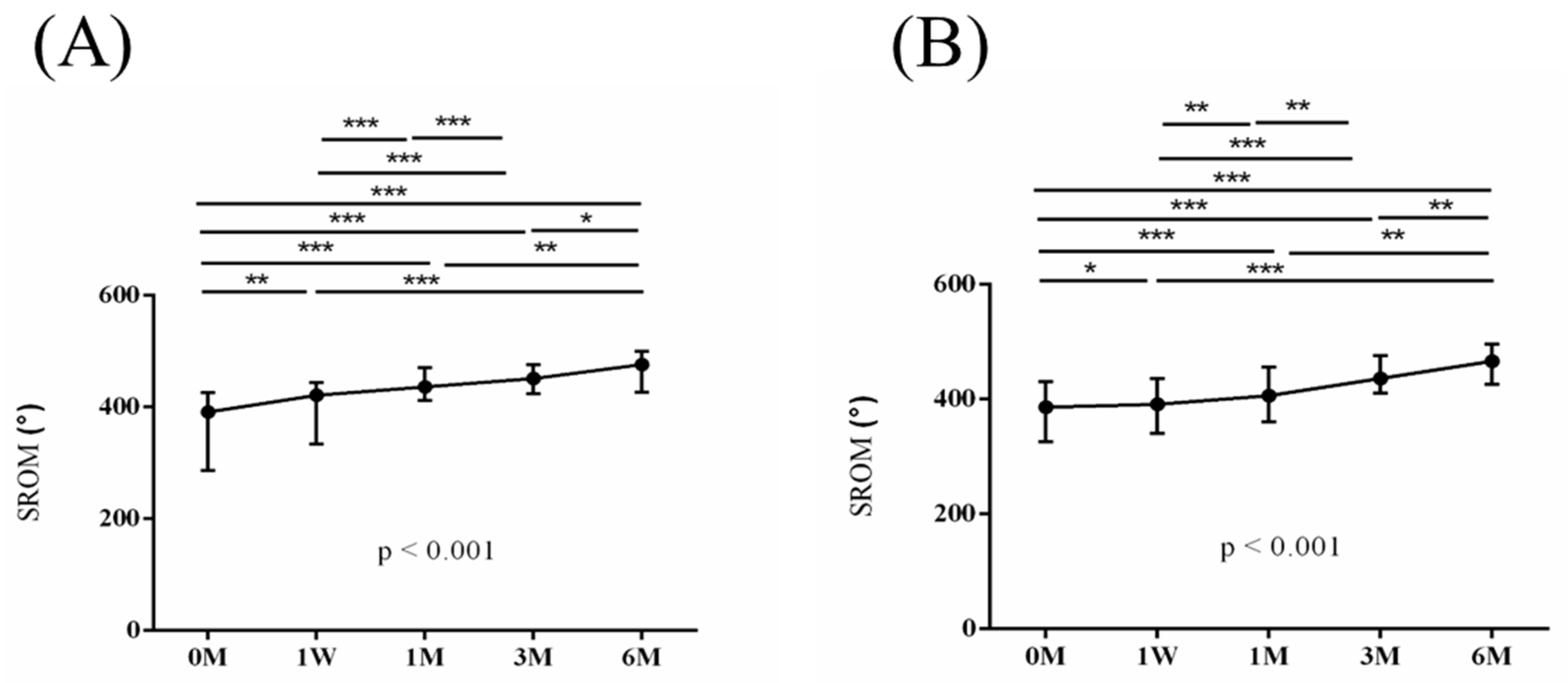
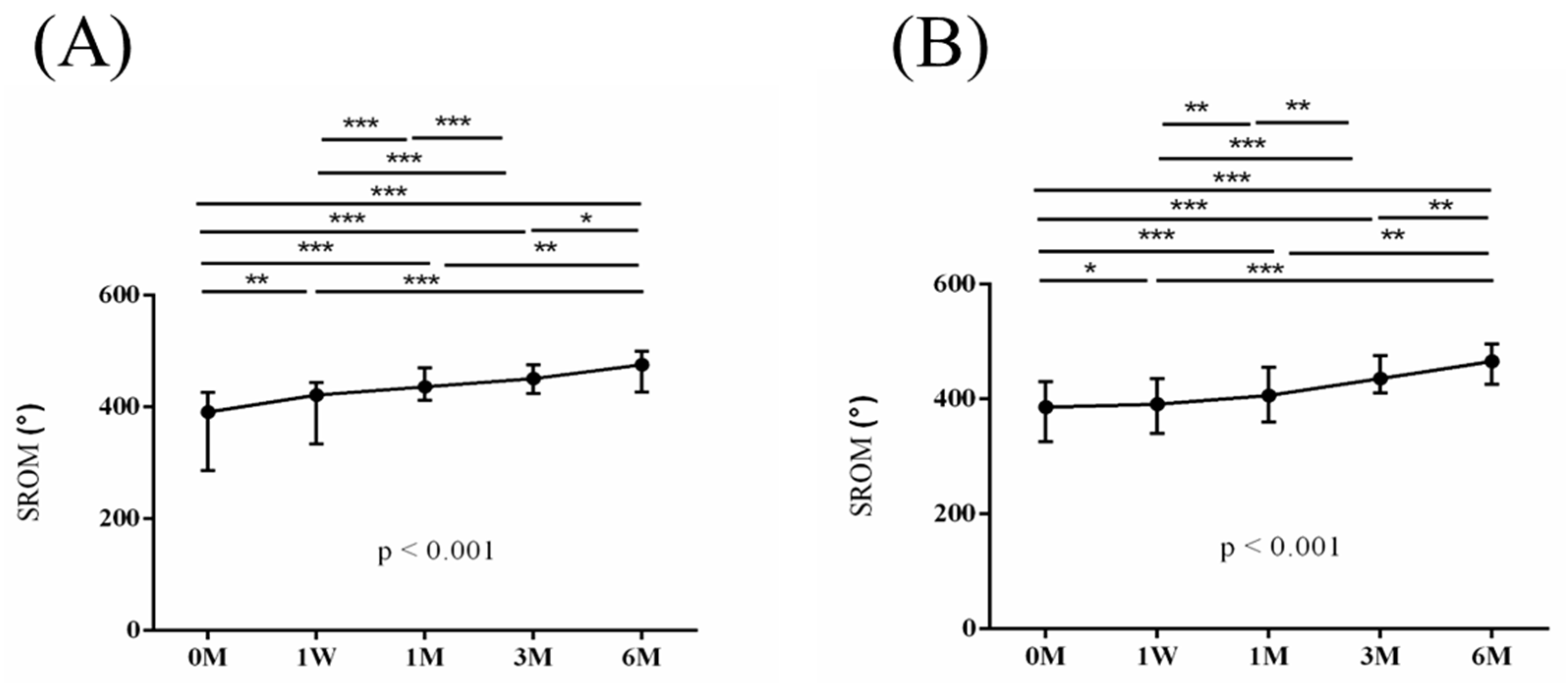
| SROM (°) | 390.0 (288.8, 425.0) | 385.0 (327.5, 425.0) | 0.992 |
| 365.36 84.11 | 371.85 | ||
| One week | |||
| Forward flexion (°) | 150.0 (122.5, 160.0) | 140.0 (125.0, 150.0) | 0.401 |
| 142.41 | 138.70 21.82 | ||
| Abduction (°) | 135.0 (96.3, 158.8) | 125.0 (100.0, 150.0) | 0.497 |
| 130.89 | 125.74 | ||
| IR (°) | 50.0 (35.0, 60.0) | 50.0 (45.0, 62.5) | 0.478 |
| 52.68 | 55.19 | ||
| ER (°) | 60.0 (45.0, 75.0) | 65.0 (51.5, 75.0) | 0.509 |
| 63.57 | 66.11 15.46 | ||
| SROM (°) | 405.0 (330.0, 430.0) | 385.0 (337.5, 427.5) | 0.728 |
| 390.00 | 385.74 | ||
| One month | |||
| Forward flexion (°) | 160.0 (136.3, 165.0) | 150.0 (130.0, 160.0) | 0.033 |
| 153.70 | 142.22 | ||
| Abduction (°) | 155.0 (140.0, 160.0) | 125.0 (110.0, 150.0) | 0.015 |
| 144.82 | 129.44 | ||
| IR (°) | 60.0 (46.3, 70.0) | 60.0 (50.0, 75.0) | 0.787 |
| 60.36 | 61.48 | ||
| ER (°) | 65.0 (56.3, 78.8) | 65.0 (57.5, 80.0) | 0.928 |
| 66.79 | 67.59 | ||
| SROM (°) | 435.0 (411.3, 470.0) | 405.0 (362.5, 452.5) | 0.089 |
| 425.89 | 400.74 | ||
| Three months | |||
| Forward flexion (°) | 160.0 (150.0, 170.0) | 155.0 (142.5, 165.0) | 0.267 |
| 156.67 | 150.74 | ||
| Abduction (°) | 155.0 (138.8, 166.3) | 140.0 (120.0, 160.0) | 0.091 |
| 149.46 20.74 | 139.26 22.86 | ||
| IR (°) | 65.0 (53.8, 85.0) | 70.0 (52.5, 80.0) | 0.711 |
| 67.50 | 65.00 | ||
| ER (°) | 70.0 (60.0, 80.0) | 70.0 (62.5, 85.0) | 0.719 |
| 69.29 | 69.63 | ||
| SROM (°) | 450.0 (427.5, 475.0) | 435.0 (412.5, 472.5) | 0.610 |
| 443.39 | 424.63 | ||
| Six months | |||
| Forward flexion (°) | 165.0 (150.0, 175.0) | 165.0 (152.5, 170.0) | 0.728 |
| 158.89 | 159.63 | ||
| Abduction (°) | 155.0 (145.0, 170.0) | 155.0 (137.5, 165.0) | 0.596 |
| 152.14 | 148.89 | ||
| IR (°) | 75.0 (62.5, 90.0) | 70.0 (60.0, 85.0) | 0.610 |
| 71.43 | 69.63 | ||
| ER (°) | 80.0 (70.0, 87.5) | 80.0 (67.5, 90.0) | 0.897 |
| 73.21 | 74.81 | ||
| SROM (°) | 475.0 (450.0, 497.5) | 465.0 (412.5, 495.0) | < 0.001 |
| 455.36 | 452.96 |
| Protein | PRP + ESWT/PRP Ratio | p-Value |
|---|---|---|
| Apolipoprotein C4 | 0.866 | <0.001 |
| Adhesion G protein-coupled receptor G6 | 0.741 | 0.013 |
| YWHAE | 0.842 | 0.013 |
| Phosphatidylethanolamine-binding protein 4 | 0.786 | 0.014 |
| Lactoferrin | 0.767 | 0.021 |
| CD5-like molecule | 0.893 | 0.023 |
| Fermitin family homolog 3 | 0.914 | 0.023 |
| Mannan-binding lectin serine protease 1 | 0.948 | 0.024 |
| H4 clustered histone 1 | 1.305 | 0.024 |
| Paraoxonase 3 | 1.046 | 0.027 |
| Apolipoprotein A2 | 1.047 | 0.028 |
| Keratin 9 | 0.443 | 0.035 |
| S100 calcium-binding protein A9 | 0.573 | 0.042 |
| Intercellular adhesion molecule 2 | 1.110 | 0.043 |
| Apolipoprotein H | 0.972 | 0.045 |
| PRP + ESWT | PRP | p-Value | |
|---|---|---|---|
| S100A8 | 12.53 (3.21, 15.77) | 22.45 (10.33, 35.11) | 0.042 |
| S100A9 | 34.32 (20.71. 47.73) | 57.67 (51.06, 119.70) | 0.034 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, S.-J.; Su, Y.-H.; Hsu, S.-C.; Huang, P.-H.; Hsia, C.-C.; Liao, C.-Y.; Chen, S.-H.; Wu, R.-W.; Hsu, C.-C.; Lai, Y.-C.; et al. Effects of Adding Extracorporeal Shockwave Therapy (ESWT) to Platelet-Rich Plasma (PRP) among Patients with Rotator Cuff Partial Tear: A Prospective Randomized Comparative Study. J. Pers. Med. 2024, 14, 83. https://doi.org/10.3390/jpm14010083
Kuo S-J, Su Y-H, Hsu S-C, Huang P-H, Hsia C-C, Liao C-Y, Chen S-H, Wu R-W, Hsu C-C, Lai Y-C, et al. Effects of Adding Extracorporeal Shockwave Therapy (ESWT) to Platelet-Rich Plasma (PRP) among Patients with Rotator Cuff Partial Tear: A Prospective Randomized Comparative Study. Journal of Personalized Medicine. 2024; 14(1):83. https://doi.org/10.3390/jpm14010083
Chicago/Turabian StyleKuo, Shu-Jui, Yu-Hsiang Su, Shih-Chan Hsu, Po-Hua Huang, Chia-Chun Hsia, Chin-Yi Liao, Sung-Hsiung Chen, Re-Wen Wu, Chieh-Cheng Hsu, Yen-Chun Lai, and et al. 2024. "Effects of Adding Extracorporeal Shockwave Therapy (ESWT) to Platelet-Rich Plasma (PRP) among Patients with Rotator Cuff Partial Tear: A Prospective Randomized Comparative Study" Journal of Personalized Medicine 14, no. 1: 83. https://doi.org/10.3390/jpm14010083
APA StyleKuo, S.-J., Su, Y.-H., Hsu, S.-C., Huang, P.-H., Hsia, C.-C., Liao, C.-Y., Chen, S.-H., Wu, R.-W., Hsu, C.-C., Lai, Y.-C., Liu, D.-Y., Ku, N.-E., Chen, J.-F., & Ko, J.-Y. (2024). Effects of Adding Extracorporeal Shockwave Therapy (ESWT) to Platelet-Rich Plasma (PRP) among Patients with Rotator Cuff Partial Tear: A Prospective Randomized Comparative Study. Journal of Personalized Medicine, 14(1), 83. https://doi.org/10.3390/jpm14010083