
Maternal Fatigue after Postpartum Anemia Treatment with Intravenous Ferric Carboxymaltose vs. Intravenous Ferric Derisomaltose vs. Oral Ferrous Sulphate: A Randomized Controlled Trial

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
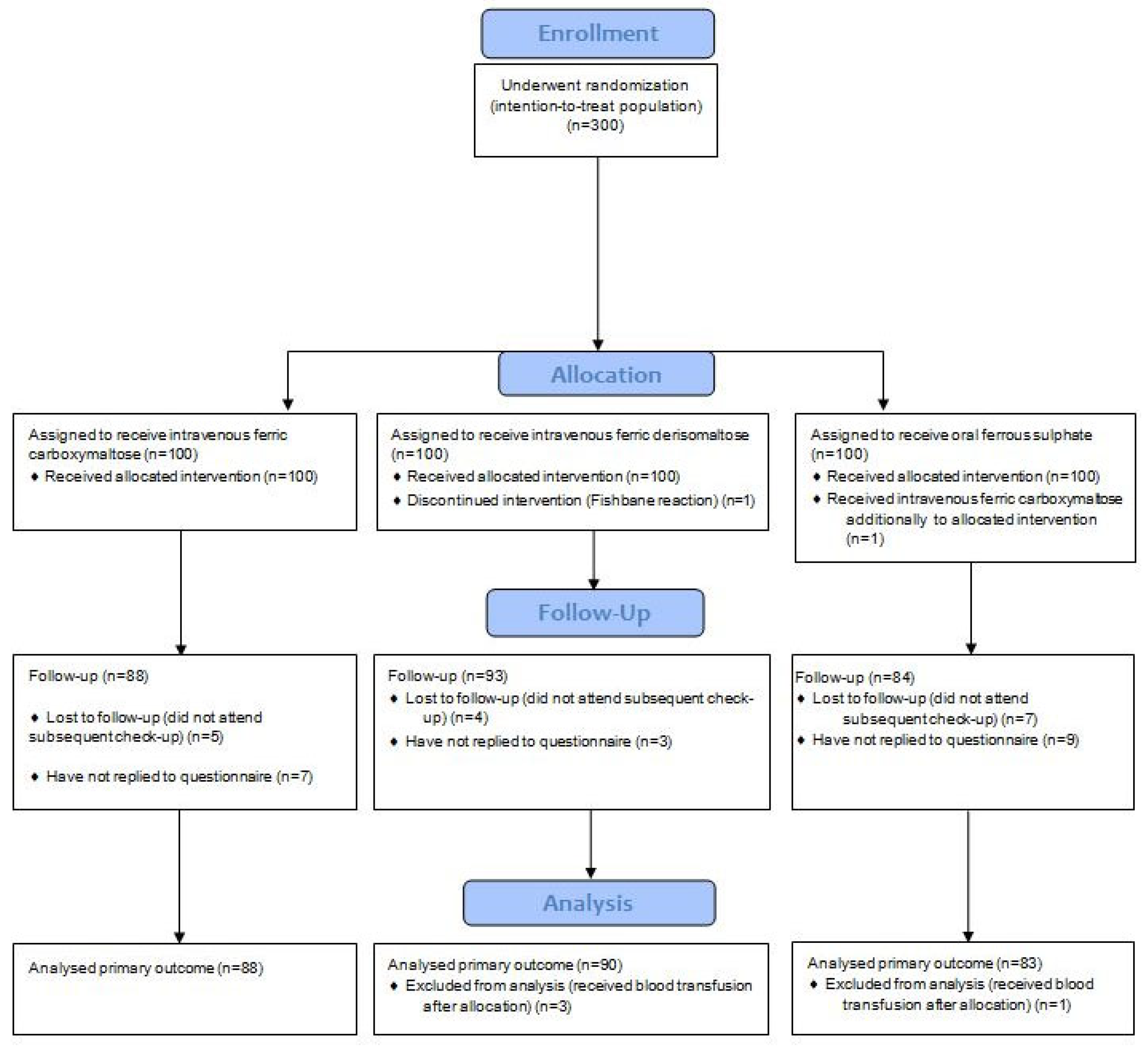
2.1. Study Design and Participants
2.2. Randomization and Blinding
2.3. Study Outcomes
- MFI physical fatigue score (fatigue score assessed by the physical fatigue domain of the MFI questionnaire) six weeks postpartum;
- Proportion of participants with a high MFI physical fatigue score (physical fatigue score > 15) six weeks postpartum;
- Hb concentration six weeks postpartum;
- Change in Hb concentration from study inclusion to six weeks postpartum;
- Ferritin concentration six weeks postpartum;
- Change in ferritin concentration from study inclusion to six weeks postpartum;
- Transferrin saturation six weeks postpartum;
- Change in transferrin concentration from study inclusion to six weeks postpartum.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Milman, N. Postpartum anemia I: Definition, prevalence, causes, and consequences. Ann. Hematol. 2011, 90, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Cogswell, M.E.; McDonald, T. Have we forgotten the significance of postpartum iron deficiency? Am. J. Obstet. Gynecol. 2005, 193, 36–44. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Iron Supplementation in Postpartum Women. 2016. Available online: http://www.who.int (accessed on 20 January 2024).
- Lee, K.A.; Zaffke, M.E. Longitudinal changes in fatigue and energy during pregnancy and the postpartum period. J. Obstet. Gynecol. Neonatal. Nurs. 1999, 28, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Ando, K.; Morita, S.; Higashi, T.; Fukuhara, S.; Watanabe, S.; Park, J.; Kikuchi, M.; Kawano, K.; Wasada, I.; Hotta, T. Health-related quality of life among Japanese women with iron-deficiency anemia. Qual. Life Res. 2006, 15, 1559–1563. [Google Scholar] [CrossRef] [PubMed]
- Holm, C.; Thomsen, L.L.; Nørgaard, A.; Langhoff-Roos, J. Single-dose intravenous iron infusion or oral iron for treatment of fatigue after postpartum haemorrhage: A randomized controlled trial. Vox Sang. 2017, 112, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Moya, E.; Phiri, N.; Choko, A.T.; Mwangi, M.N.; Phiri, K.S. Effect of postpartum anaemia on maternal health-related quality of life: A systematic review and meta-analysis. BMC Public Health 2022, 22, 364. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.L.; Hendricks, M.K.; Perez, E.M.; Murray-Kolb, L.E.; Berg, A.; Vernon-Feagans, L.; Irlam, J.; Isaacs, W.; Sive, A.; Tomlinson, M. Maternal iron deficiency anaemia affects postpartum emotions and cognitions. J. Nutr. 2005, 135, 267–272. [Google Scholar] [CrossRef]
- Corwin, E.J.; Murray-Kolb, L.E.; Beard, J.L. Low hemoglobin level is a risk factor for post partum depression. J. Nutr. 2003, 133, 4139–4142. [Google Scholar] [CrossRef]
- Rioux, F.M.; Savoie, N.; Allard, J. Is there a link between postpartum anemia and discontinuation of breastfeeding? Can. J. Diet. Pract. Res. 2006, 67, 72–76. [Google Scholar] [CrossRef]
- Milman, N. Postpartum anemia II: Prevention and treatment. Ann. Hematol. 2012, 91, 143–154. [Google Scholar] [CrossRef]
- Evstatiev, R.; Marteau, P.; Iqbal, T.; Khalif, I.L.; Stein, J.; Bokemeyer, B.; Chopey, I.V.; Gutzwiller, F.S.; Riopel, L.; Gasche, C.; et al. FERGIcor, a randomized controlled trial on ferric carboxymaltose for iron deficiency anemia in inflammatory bowel disease. Gastroenterology 2011, 141, 846–853. [Google Scholar] [CrossRef]
- Bhandari, S.; Kalra, P.A.; Kothari, J.; Ambühl, P.M.; Christensen, J.H.; Essaian, A.M.; Thomsen, L.L.; Macdougall, I.C.; Coyne, D.W. A randomized, open-label trial of iron isomaltoside 1000 (Monofer®) compared with iron sucrose (Venofer®) as maintenance therapy in haemodialysis patients. Nephrol. Dial. Transplant. 2015, 30, 1577–1589. [Google Scholar] [CrossRef]
- Derman, R.; Roman, E.; Modiano, M.R.; Achebe, M.M.; Thomsen, L.L.; Auerbach, M. A randomized trial of iron isomaltoside versus iron sucrose in patients with iron deficiency anemia. Am. J. Hematol. 2017, 92, 286–291. [Google Scholar] [CrossRef]
- Rozen-Zvi, B.; Gafter-Gvili, A.; Paul, M.; Leibovici, L.; Shpilberg, O.; Gafter, U. Intravenous versus oral iron supplementation for the treatment of anemia in CKD: Systematic review and meta-analysis. Am. J. Kidney Dis. 2008, 52, 897–906. [Google Scholar] [CrossRef]
- Auerbach, M.; Macdougall, I.C. Oral Iron Therapy: After Three Centuries, It Is Time for a Change. Am. J. Kidney Dis. 2016, 68, 665–666. [Google Scholar] [CrossRef]
- Bhandal, N.; Russell, R. Intravenous versus oral iron therapy for postpartum anaemia. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 1248–1252. [Google Scholar] [CrossRef] [PubMed]
- Sultan, P.; Bampoe, S.; Shah, R.; Guo, N.; Estes, J.; Stave, C.; Goodnough, L.T.; Halpern, S.; Butwick, A.J. Oral vs intravenous iron therapy for postpartum anemia: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2019, 221, 19–29.e3. [Google Scholar] [CrossRef]
- Ganzoni, A.M. Intravenous iron-dextran: Therapeutic and experimental possibilities. Schweiz. Med. Wochenschr. 1970, 100, 301–303. (In German) [Google Scholar] [PubMed]
- Smets, E.M.A.; Garssen, B.; Bonke, B.; De Haes, J.C.J.M. The multidimensional fatigue inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosomat. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef]
- Lin, J.M.S.; Brimmer, D.J.; Maloney, E.M. Further validation of the Multidimensional Fatigue Inventory in a US adult population sample. Popul. Health Metr. 2009, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Jansen, A.J.; Essink-Bot, M.L.; Duvekot, J.J.; van Rhenen, D.J. Psychometric evaluation of health-related quality of life measures in women after different types of delivery. J. Psychosom. Res. 2007, 63, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.; Afif, W.; Knowles, S.; Lim, G.; Lin, Y.; Mothersill, C.; Nistor, I.; Rehman, F.; Song, C.; Xenodemetropoulos, T. Canadian expert consensus: Management of hypersensitivity reactions to intravenous iron in adults. Vox Sang. 2019, 114, 363–373. [Google Scholar] [CrossRef]
- Van Wyck, D.B.; Martens, M.G.; Seid, M.H.; Baker, J.B.; Mangione, A. Intravenous ferric carboxymaltose compared with oral iron in the treatment of postpartum anemia: A randomized controlled trial. Obstet. Gynecol. 2007, 110 Pt 1, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Westad, S.; Backe, B.; Salvesen, K.A.; Nakling, J.; Økland, I.; Borthen, I.; Rognerud Jensen, O.H.; Kolås, T.; Løkvik, B.; Smedvig, E. A 12-week randomised study comparing intravenous iron sucrose versus oral ferrous sulphate for treatment of postpartum anemia. Acta Obstet. Gynecol. Scand. 2008, 87, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Rathod, S.; Samal, S.K.; Mahapatra, P.C.; Samal, S. Ferric carboxymaltose: A revolution in the treatment of postpartum anemia in Indian women. Int. J. Appl. Basic Med. Res. 2015, 5, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Vanobberghen, F.; Lweno, O.; Kuemmerle, A.; Mwebi, K.D.; Asilia, P.; Issa, A.; Simon, B.; Mswata, S.; Schmidlin, S.; Glass, T.R.; et al. Efficacy and safety of intravenous ferric carboxymaltose compared with oral iron for the treatment of iron deficiency anaemia in women after childbirth in Tanzania: A parallel-group, open-label, randomised controlled phase 3 trial. Lancet Glob. Health. 2021, 9, e189–e198. [Google Scholar] [CrossRef] [PubMed]
- Seid, M.H.; Butcher, A.D.; Chatwani, A. Ferric Carboxymaltose as Treatment in Women with Iron-Deficiency Anemia. Anemia 2017, 2017, 9642027. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.F.; Stepanek, R.; Kothmann, M.; Wilson-Jimenez, M.; McCoy, L.; Aguillon, B.; Salazar, A.; Saade, G.R. Intravenous Iron Compared With Oral Iron Supplementation for the Treatment of Postpartum Anemia: A Randomized Controlled Trial. Obstet. Gynecol. 2023, 141, 1052–1055. [Google Scholar] [CrossRef]
- Badr, H.A.; Zauszniewski, J.A. Meta-analysis of the predictive factors of postpartum fatigue. Appl. Nurs. Res. 2017, 36, 122–127. [Google Scholar] [CrossRef]
- Troy, N.W. Is the significance of postpartum fatigue being overlooked in the lives of women? MCN Am. J. Matern. Child. Nurs. 2003, 28, 252–259. [Google Scholar] [CrossRef]
- Moretti, D.; Goede, J.S.; Zeder, C.; Jiskra, M.; Chatzinakou, V.; Tjalsma, H.; Melse-Boonstra, A.; Brittenham, G.; Swinkels, D.W.; Zimmermann, M.B. Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in iron-depleted young women. Blood 2015, 126, 1981–1989. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Statistics/Category | Treatment Group | p Value | ||
|---|---|---|---|---|
| Intravenous Ferric Carboxymaltose (n = 88) | Intravenous Ferric Derisomaltose (n = 90) | Oral Ferrous Sulphate (n = 83) | ||
| Maternal age, years | 32 (28–36) | 30 (27–35) | 31 (28–36) | 0.237 |
| Prepregnancy BMI, kg/m2 | 24 (21–27) | 24 (22–27) | 23 (21–27) | 0.631 |
| BMI at delivery, kg/m2 | 28 (27–32) | 30 (27–32) | 29 (26–32) | 0.485 |
| Multiple gestation | 6 (2) | 6 (2) | 2 (1) | 0.351 |
| Nulliparity | 58 (22) | 64 (25) | 46 (18) | 0.092 |
| Gestational age at childbirth, completed weeks | 39 (38–40) | 39 (38–40) | 39 (38–40) | 0.590 |
| Transfusion of RBC before intervention | 5 (2) | 5 (2) | 7 (3) | 0.691 |
| Cesarean section | 28 (11) | 22 (8) | 28 (11) | 0.365 |
| Maternal level of education * | 8 (5–9) | 8 (5–9) | 8 (5–9) | 0.465 |
| Calculated iron deficit †, g | 1422 (1281–1567) | 1449 (1346–1586) | / | 0.191 |
| Hemoglobin, g/L | 92 (87–97) | 91 (87–95) | 95 (91–98) | 0.006 |
| Ferritin, µ/L | 29 (11–47) | 20 (12–30) | 22 (13–41) | 0.106 |
| Transferrin saturation, % | 9 (7–14) | 10 (7–15) | 10 (7–16) | 0.301 |
| Plasma iron µmol/L | 6 (4–8) | 8 (5–12) | 7 (5–11) | 0.163 |
| TIBC, µmol/L | 71 (64–77) | 73 (67–80) | 71 (65–80) | 0.334 |
| CRP, mg/L | 57 (36–94) | 53 (35–78) | 48 (34–76) | 0.576 |
| Total MFI score | 49 (41–62) | 48 (34–60) | 51 (37–62) | 0.340 |
| Physical fatigue MFI score | 12 (8–15) | 11 (8–15) | 12 (8–15) | 0.816 |
| Physical fatigue MFI score > 15 ‡ | 27 (31) | 23 (28) | 20 (26) | 0.713 |
| Statistics/Category | Treatment Group | p Value | ||
|---|---|---|---|---|
| Intravenous Ferric Carboxymaltose (n = 88) | Intravenous Ferric Derisomaltose (n = 90) | Oral Ferrous Sulphate (n = 83) | ||
| Total MFI score six weeks postpartum | 38 (29–47) | 34 (26–42) | 36 (25–47) | 0.26 |
| Decrease in total MFI score from study inclusion to six weeks postpartum | 12 (4–22) | 12 (4–20) | 11 (1–21) | 0.76 |
| Physical fatigue MFI score six weeks postpartum | 8 (5–11) | 7 (5–10) | 8 (5–11) | 0.10 |
| Decrease in physical fatigue MFI score from study inclusion to six weeks postpartum | 3 (0–6) | 3 (0–6) | 3 (0–6) | 0.78 |
| Physical fatigue MFI score > 15 * six weeks postpartum | 7 (8) | 5 (6) | 5 (6) | 0.79 |
| Decrease in proportion of participants with physical fatigue MFI score > 15 from study inclusion to six weeks postpartum | 20 (23) | 18 (20) | 15 (18) | 0.75 |
| Statistics/Category | Treatment Group | p Value | ||
|---|---|---|---|---|
| Intravenous Ferric Carboxymaltose (n = 88) | Intravenous Ferric Derisomaltose (n = 90) | Oral Ferrous Sulphate (n = 83) | ||
| Hemoglobin at six weeks postpartum, g/L | 135 (131–139) | 134 (129–139) | 131 (125–137) | 0.008 |
| Change in hemoglobin from study inclusion to six weeks postpartum, g/L | 43 (37–51) | 45 (38–50) | 36 (31–44) | <0.001 |
| Ferritin at six weeks postpartum, µg/L | 273 (198–377) | 187 (155–246) | 24 (17–37) | <0.001 |
| Change in ferritin from study inclusion to six weeks postpartum, µg/L | 240 (173–336) | 163 (127–219) | 0 (−10–12) | <0.001 |
| Transferrin saturation at six weeks postpartum, % | 34 (28–38) | 30 (23–37) | 24 (17–37) | <0.001 |
| Change in transferrin saturation from study inclusion to six weeks postpartum, % | 23 (18–28) | 19 (10–28) | 12 (5–24) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bombač Tavčar, L.; Hrobat, H.; Gornik, L.; Preložnik Zupan, I.; Vidmar Šimic, M.; Pečlin, P.; Kavšek, G.; Lučovnik, M. Maternal Fatigue after Postpartum Anemia Treatment with Intravenous Ferric Carboxymaltose vs. Intravenous Ferric Derisomaltose vs. Oral Ferrous Sulphate: A Randomized Controlled Trial. J. Clin. Med. 2024, 13, 758. https://doi.org/10.3390/jcm13030758
Bombač Tavčar L, Hrobat H, Gornik L, Preložnik Zupan I, Vidmar Šimic M, Pečlin P, Kavšek G, Lučovnik M. Maternal Fatigue after Postpartum Anemia Treatment with Intravenous Ferric Carboxymaltose vs. Intravenous Ferric Derisomaltose vs. Oral Ferrous Sulphate: A Randomized Controlled Trial. Journal of Clinical Medicine. 2024; 13(3):758. https://doi.org/10.3390/jcm13030758
Chicago/Turabian StyleBombač Tavčar, Lea, Hana Hrobat, Lea Gornik, Irena Preložnik Zupan, Marijana Vidmar Šimic, Polona Pečlin, Gorazd Kavšek, and Miha Lučovnik. 2024. "Maternal Fatigue after Postpartum Anemia Treatment with Intravenous Ferric Carboxymaltose vs. Intravenous Ferric Derisomaltose vs. Oral Ferrous Sulphate: A Randomized Controlled Trial" Journal of Clinical Medicine 13, no. 3: 758. https://doi.org/10.3390/jcm13030758
APA StyleBombač Tavčar, L., Hrobat, H., Gornik, L., Preložnik Zupan, I., Vidmar Šimic, M., Pečlin, P., Kavšek, G., & Lučovnik, M. (2024). Maternal Fatigue after Postpartum Anemia Treatment with Intravenous Ferric Carboxymaltose vs. Intravenous Ferric Derisomaltose vs. Oral Ferrous Sulphate: A Randomized Controlled Trial. Journal of Clinical Medicine, 13(3), 758. https://doi.org/10.3390/jcm13030758