
Longwise Cluster Analysis for the Prediction of COVID-19 Severity within 72 h of Admission: COVID-DATA-SAVE-LIFES Cohort

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Database
2.2. Data Collection and Definitions
2.3. Statistical Analysis
3. Results
3.1. Study Sample Description
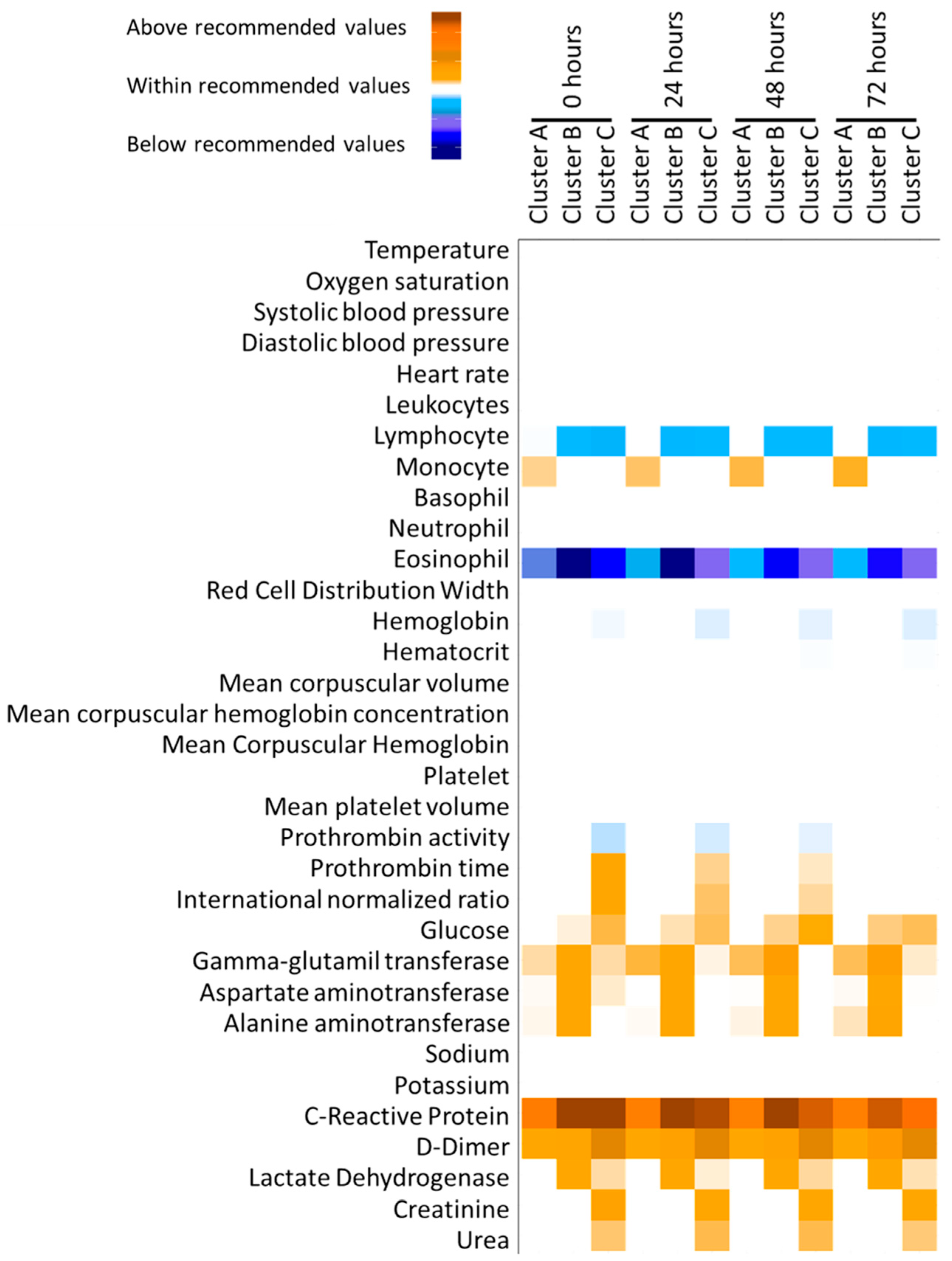
3.2. Patient Clusterization
3.3. Logistic Regression Models to Predict Severe Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.L.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.; Oh, M.D.; Sall, A.A.; et al. COVID-19: Towards controlling of a pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Freidin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varsavsky, T.; Cardoso, M.J.; El-Sayed Moustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Lee, K.A.; Lochlainn, M.N.; Varsavsky, T.; Murray, B.; Graham, M.S.; Menni, C.; Modat, M.; Bowyer, R.C.E.; Nguyen, L.H.; et al. Symptom clusters in COVID-19: A potential clinical prediction tool from the COVID Symptom Study app. Sci. Adv. 2021, 7, eabd4177. [Google Scholar] [CrossRef]
- Faes, C.; Abrams, S.; Van Beckhoven, D.; Meyfroidt, G.; Vlieghe, E.; Hens, N.; Belgian Collaborative Group on COVID-19 Hospital Surveillance. Time between Symptom Onset, Hospitalisation and Recovery or Death: Statistical Analysis of Belgian COVID-19 Patients. Int. J. Environ. Res. Public Health 2020, 17, 7560. [Google Scholar] [CrossRef]
- Pellis, L.; Scarabel, F.; Stage, H.B.; Overton, C.E.; Chappell, L.H.K.; Fearon, E.; Bennett, E.; Lythgoe, K.A.; House, T.A.; Hall, I.; et al. Challenges in control of COVID-19: Short doubling time and long delay to effect of interventions. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2021, 376, 20200264. [Google Scholar] [CrossRef]
- Martinez-Urbistondo, M.; Mora-Vargas, A.; Exposito-Palomo, E.; Castejon, R.; Citores, M.J.; Rosado, S.; de Mendoza, C.; Banos, I.; Fernandez-Cruz, A.; Daimiel, L.; et al. Inflammatory-Related Clinical and Metabolic Outcomes in COVID-19 Patients. Mediat. Inflamm. 2020, 2020, 2914275. [Google Scholar] [CrossRef]
- Moreno-Torres, V.; de Mendoza, C.; de la Fuente, S.; Sanchez, E.; Martinez-Urbistondo, M.; Herraiz, J.; Gutierrez, A.; Gutierrez, A.; Hernandez, C.; Callejas, A.; et al. Bacterial infections in patients hospitalized with COVID-19. Intern. Emerg. Med. 2021, 17, 431–438. [Google Scholar] [CrossRef]
- Martinez Urbistondo, M.; Mora Vargas, A.; Exposito Palomo, E.; Aparicio de Miguel, M.; Castejon Diaz, R.; Daimiel, L.; Ramos Lopez, O.; San Cristobal, R.; Martinez, J.A.; Vargas Nunez, J.A. Evolution of patients infected with SARS-CoV-2 according to previous metabolic status. Nutr. Hosp. 2021, 38, 1068–1074. [Google Scholar] [CrossRef]
- Ramos-Lopez, O.; San-Cristobal, R.; Martinez-Urbistondo, D.; Mico, V.; Colmenarejo, G.; Villares-Fernandez, P.; Daimiel, L.; Martinez, J.A. Proinflammatory and Hepatic Features Related to Morbidity and Fatal Outcomes in COVID-19 Patients. J. Clin. Med. 2021, 10, 3112. [Google Scholar] [CrossRef] [PubMed]
- Yokota, S.; Miyamae, T.; Kuroiwa, Y.; Nishioka, K. Novel Coronavirus Disease 2019 (COVID-19) and Cytokine Storms for More Effective Treatments from an Inflammatory Pathophysiology. J. Clin. Med. 2021, 10, 801. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli, A.; Pezzati, L.; Conti, F.; Bernacchia, D.; Siano, M.; Oreni, L.; Rusconi, S.; Gervasoni, C.; Ridolfo, A.L.; Rizzardini, G.; et al. Self-reported Olfactory and Taste Disorders in Patients with Severe Acute Respiratory Coronavirus 2 Infection: A Cross-sectional Study. Clin. Infect. Dis. 2020, 71, 889–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C.; et al. Clinical Characteristics of COVID-19 Patients with Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. Am. J. Gastroenterol. 2020, 115, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Moradian, N.; Ochs, H.D.; Sedikies, C.; Hamblin, M.R.; Camargo, C.A., Jr.; Martinez, J.A.; Biamonte, J.D.; Abdollahi, M.; Torres, P.J.; Nieto, J.J.; et al. The urgent need for integrated science to fight COVID-19 pandemic and beyond. J. Transl. Med. 2020, 18, 205. [Google Scholar] [CrossRef]
- Crisci, C.D.; Ardusso, L.R.F.; Mossuz, A.; Muller, L. A Precision Medicine Approach to SARS-CoV-2 Pandemic Management. Curr. Treat. Options Allergy 2020, 7, 422–440. [Google Scholar] [CrossRef]
- Russell, S.M.; Alba-Patino, A.; Baron, E.; Borges, M.; Gonzalez-Freire, M.; de la Rica, R. Biosensors for Managing the COVID-19 Cytokine Storm: Challenges Ahead. ACS Sens. 2020, 5, 1506–1513. [Google Scholar] [CrossRef]
- Man, M.A.; Rajnoveanu, R.M.; Motoc, N.S.; Bondor, C.I.; Chis, A.F.; Lesan, A.; Puiu, R.; Lucaciu, S.R.; Dantes, E.; Gergely-Domokos, B.; et al. Neutrophil-to-lymphocyte ratio, platelets-to-lymphocyte ratio, and eosinophils correlation with high-resolution computer tomography severity score in COVID-19 patients. PLoS ONE 2021, 16, e0252599. [Google Scholar] [CrossRef]
- Lamadrid, P.; Alonso-Pena, M.; San Segundo, D.; Arias-Loste, M.; Crespo, J.; Lopez-Hoyos, M. Innate and Adaptive Immunity Alterations in Metabolic Associated Fatty Liver Disease and Its Implication in COVID-19 Severity. Front. Immunol. 2021, 12, 651728. [Google Scholar] [CrossRef]
- Garip Ustaoglu, S.; Kaygusuz, H.; Bilgin, M.D.; Severcan, F. Novel approaches for COVID-19 diagnosis and treatment: A nonsystematic review. Turk. J. Biol. 2021, 45, 358–371. [Google Scholar] [CrossRef]
- Guan, J.; Wei, X.; Qin, S.; Liu, X.; Jiang, Y.; Chen, Y.; Chen, Y.; Lu, H.; Qian, J.; Wang, Z.; et al. Continuous tracking of COVID-19 patients’ immune status. Int. Immunopharmacol. 2020, 89, 107034. [Google Scholar] [CrossRef] [PubMed]
- Falzone, L.; Gattuso, G.; Tsatsakis, A.; Spandidos, D.A.; Libra, M. Current and innovative methods for the diagnosis of COVID19 infection (Review). Int. J. Mol. Med. 2021, 47, 100. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Genolini, C.; Pingault, J.B.; Driss, T.; Cote, S.; Tremblay, R.E.; Vitaro, F.; Arnaud, C.; Falissard, B. KmL3D: A non-parametric algorithm for clustering joint trajectories. Comput. Methods Programs Biomed. 2013, 109, 104–111. [Google Scholar] [CrossRef]
- Chatterjee, A.; Gerdes, M.W.; Martinez, S.G. Identification of Risk Factors Associated with Obesity and Overweight-A Machine Learning Overview. Sensors 2020, 20, 2734. [Google Scholar] [CrossRef]
- DeGregory, K.W.; Kuiper, P.; DeSilvio, T.; Pleuss, J.D.; Miller, R.; Roginski, J.W.; Fisher, C.B.; Harness, D.; Viswanath, S.; Heymsfield, S.B.; et al. A review of machine learning in obesity. Obes. Rev. 2018, 19, 668–685. [Google Scholar] [CrossRef]
- Alzoughool, F.; Alanagreh, L.; Abumweis, S.; Atoum, M. Cerebrovascular comorbidity, high blood levels of C-reactive protein and D-dimer are associated with disease outcomes in COVID-19 patients. Clin. Hemorheol. Microcirc. 2021, 77, 311–322. [Google Scholar] [CrossRef]
- Chahar, S.; Roy, P.K. COVID-19: A Comprehensive Review of Learning Models. Arch. Comput. Methods Eng. 2021, 29, 1915–1940. [Google Scholar] [CrossRef]
- Su, C.; Xu, Z.; Hoffman, K.; Goyal, P.; Safford, M.M.; Lee, J.; Alvarez-Mulett, S.; Gomez-Escobar, L.; Price, D.R.; Harrington, J.S.; et al. Identifying organ dysfunction trajectory-based subphenotypes in critically ill patients with COVID-19. Sci. Rep. 2021, 11, 15872. [Google Scholar] [CrossRef]
- Ramos-Lopez, O.; Milton-Laskibar, I.; Martinez, J.A.; Collaborators Rodrigo, S.-C.; Maria, P.P. Precision nutrition based on phenotypical traits and the (epi)genotype: Nutrigenetic and nutrigenomic approaches for obesity care. Curr. Opin. Clin. Nutr. Metab. Care 2021, 24, 315–325. [Google Scholar] [CrossRef]
- Chaudhary, L.; Singh, B. Community detection using unsupervised machine learning techniques on COVID-19 dataset. Soc. Netw. Anal. Min. 2021, 11, 28. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, E.; Yeghiazaryan, K.; Ahmad, A.; Giordano, F.A.; Frohlich, H.; Golubnitschaja, O. Optimal multiparametric set-up modelled for best survival outcomes in palliative treatment of liver malignancies: Unsupervised machine learning and 3 PM recommendations. EPMA J. 2020, 11, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Senia, P.; Vella, F.; Mucci, N.; Dounias, G.; Trovato, A.; Marconi, A.; Ledda, C.; Rapisarda, V.; Vitale, E. Survey on COVID-19-related mortality associated with occupational infection during the first phase of the pandemic: A systematic review. Exp. Ther. Med. 2022, 23, 10. [Google Scholar] [CrossRef] [PubMed]
- Vahabi, N.; Salehi, M.; Duarte, J.D.; Mollalo, A.; Michailidis, G. County-level longitudinal clustering of COVID-19 mortality to incidence ratio in the United States. Sci. Rep. 2021, 11, 3088. [Google Scholar] [CrossRef] [PubMed]
- Migrino, J.R., Jr.; Batangan, A.R.U. Using machine learning to create a decision tree model to predict outcomes of COVID-19 cases in the Philippines. West. Pac. Surveill. Response J. 2021, 12, 56–64. [Google Scholar] [CrossRef]
- Wanyan, T.; Honarvar, H.; Jaladanki, S.K.; Zang, C.; Naik, N.; Somani, S.; De Freitas, J.K.; Paranjpe, I.; Vaid, A.; Zhang, J.; et al. Contrastive learning improves critical event prediction in COVID-19 patients. Patterns 2021, 2, 100389. [Google Scholar] [CrossRef]
- Li, W.T.; Ma, J.; Shende, N.; Castaneda, G.; Chakladar, J.; Tsai, J.C.; Apostol, L.; Honda, C.O.; Xu, J.; Wong, L.M.; et al. Using machine learning of clinical data to diagnose COVID-19: A systematic review and meta-analysis. BMC Med. Inform. Decis. Mak. 2020, 20, 247. [Google Scholar] [CrossRef]
- Taneri, P.E.; Gomez-Ochoa, S.A.; Llanaj, E.; Raguindin, P.F.; Rojas, L.Z.; Roa-Diaz, Z.M.; Salvador, D., Jr.; Groothof, D.; Minder, B.; Kopp-Heim, D.; et al. Anemia and iron metabolism in COVID-19: A systematic review and meta-analysis. Eur. J. Epidemiol. 2020, 35, 763–773. [Google Scholar] [CrossRef]
- Rostami, M.; Mansouritorghabeh, H. D-dimer level in COVID-19 infection: A systematic review. Expert. Rev. Hematol. 2020, 13, 1265–1275. [Google Scholar] [CrossRef]
- Wool, G.D.; Miller, J.L. The Impact of COVID-19 Disease on Platelets and Coagulation. Pathobiology 2021, 88, 15–27. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Levi, M.; Thachil, J. Coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Paz, L.; Capodanno, D.; Montalescot, G.; Angiolillo, D.J. Coronavirus Disease 2019-Associated Thrombosis and Coagulopathy: Review of the Pathophysiological Characteristics and Implications for Antithrombotic Management. J. Am. Heart Assoc. 2021, 10, e019650. [Google Scholar] [CrossRef]
- Hartl, L.; Jachs, M.; Simbrunner, B.; Bauer, D.J.M.; Semmler, G.; Gompelmann, D.; Szekeres, T.; Quehenberger, P.; Trauner, M.; Mandorfer, M.; et al. Cirrhosis-Associated RAS-Inflammation-Coagulation Axis Anomalies: Parallels to Severe COVID-19. J. Pers. Med. 2021, 11, 1264. [Google Scholar] [CrossRef] [PubMed]
- Hanff, T.C.; Mohareb, A.M.; Giri, J.; Cohen, J.B.; Chirinos, J.A. Thrombosis in COVID-19. Am. J. Hematol. 2020, 95, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Mertoglu, C.; Huyut, M.T.; Arslan, Y.; Ceylan, Y.; Coban, T.A. How do routine laboratory tests change in coronavirus disease 2019? Scand. J. Clin. Lab. Investig. 2021, 81, 24–33. [Google Scholar] [CrossRef]
- Oikonomou, E.; Paraskevas, T.; Velissaris, D. Cardiac biomarkers alterations in patients with SARS-CoV-2 infection. Rom. J. Intern. Med. 2022, 60, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Caruso, F.P.; Scala, G.; Cerulo, L.; Ceccarelli, M. A review of COVID-19 biomarkers and drug targets: Resources and tools. Brief. Bioinform. 2021, 22, 701–713. [Google Scholar] [CrossRef]
- Carobene, A.; Milella, F.; Famiglini, L.; Cabitza, F. How is test laboratory data used and characterised by machine learning models? A systematic review of diagnostic and prognostic models developed for COVID-19 patients using only laboratory data. Clin. Chem. Lab. Med. 2022. [Google Scholar] [CrossRef]
- Bhargava, A.; Bansal, A.; Goyal, V. Machine learning-based automatic detection of novel coronavirus (COVID-19) disease. Multimed. Tools Appl. 2022, 81, 13731–13750. [Google Scholar] [CrossRef]
- Vaishya, R.; Javaid, M.; Khan, I.H.; Haleem, A. Artificial Intelligence (AI) applications for COVID-19 pandemic. Diabetes Metab. Syndr. 2020, 14, 337–339. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Overall | ≤3 Points | >3 Points | p | |
|---|---|---|---|---|
| n | 1039 | 533 | 506 | |
| Age | 68.5 (15.5) | 58.0 (11.9) | 79.5 (10.3) | <0.001 |
| Sex (male (%)) | 626 (60.3) | 328 (61.5) | 298 (58.9) | 0.419 |
| Hospitalization (days) | 10.1 (8.6) | 8.9 (7.7) | 11.3 (9.3) | <0.001 |
| ICU stay (yes (%)) | 56 (5.4) | 29 (5.4) | 27 (5.3) | 1 |
| Mechanical ventilation (yes (%)) | 650 (62.6) | 295 (55.3) | 355 (70.2) | <0.001 |
| Cause of discharge (%) | <0.001 | |||
| Voluntary discharge | 1 (0.1) | 0 (0.0) | 1 (0.2) | |
| Home | 816 (78.5) | 476 (89.3) | 340 (67.2) | |
| Death | 120 (11.5) | 15 (2.8) | 105 (20.8) | |
| Health center transfer | 31 (3.0) | 3 (0.6) | 28 (5.5) | |
| Hospital transfer | 33 (3.2) | 19 (3.6) | 14 (2.8) | |
| Not registered | 38 (3.7) | 20 (3.8) | 18 (3.6) | |
| CCI | 3.58 (2.53) | 1.58 (1.11) | 5.68 (1.81) | <0.001 |
| Myocardial infarction (yes (%)) | 79 (7.6) | 3 (0.6) | 76 (15.0) | <0.001 |
| Congestive heart failure (yes (%)) | 54 (5.2) | 1 (0.2) | 53 (10.5) | <0.001 |
| Peripheral vascular disease (yes (%)) | 32 (3.1) | 0 (0.0) | 32 (6.3) | <0.001 |
| Cerebrovascular accident (yes (%)) | 22 (2.1) | 1 (0.2) | 21 (4.2) | <0.001 |
| Dementia (yes (%)) | 42 (4.0) | 1 (0.2) | 41 (8.1) | <0.001 |
| COPD (yes (%)) | 131 (12.6) | 30 (5.6) | 101 (20.0) | <0.001 |
| Connective tissue disease (yes (%)) | 13 (1.3) | 4 (0.8) | 9 (1.8) | 0.226 |
| Peptic ulcer disease (yes (%)) | 2 (0.2) | 0 (0.0) | 2 (0.4) | 0.456 |
| Liver disease (yes (%)) | 35 (3.4) | 2 (0.4) | 33 (6.5) | <0.001 |
| Diabetes mellitus (yes (%)) | 194 (18.7) | 36 (6.8) | 158 (31.2) | <0.001 |
| Hemiplegia (yes (%)) | 2 (0.2) | 1 (0.2) | 1 (0.2) | 1 |
| Moderate to severe CKD (yes (%)) | 153 (14.7) | 4 (0.8) | 149 (29.4) | <0.001 |
| Solid tumor (yes (%)) | 44 (4.2) | 1 (0.2) | 43 (8.5) | <0.001 |
| Lymphoma (yes (%)) | 16 (1.5) | 0 (0.0) | 16 (3.2) | <0.001 |
| Leukemia (yes (%)) | 8 (0.8) | 0 (0.0) | 8 (1.6) | 0.01 |
| AIDS (yes (%)) | 2 (0.2) | 0 (0.0) | 2 (0.4) | 0.456 |
| Stratified by Cluster | ||||
|---|---|---|---|---|
| A | B | C | p | |
| n | 496 | 403 | 147 | |
| Age | 66.1 (15.8) | 66.1 (13.7) | 83.1 (9.9) | <0.001 |
| Sex (male (%)) | 252 (50.8) | 287 (71.2) | 92 (62.6) | <0.001 |
| Hospitalization (days) | 7.6 (5.6) | 13.7 (11.9) | 10.1 (7.9) | <0.001 |
| ICU stay (yes (%)) | 0.10 (1.57) | 1.36 (5.08) | 0.17 (1.51) | <0.001 |
| Mechanical ventilation (yes (%)) | 258 (52.0) | 287 (71.2) | 112 (76.2) | <0.001 |
| Cause of discharge (%) | <0.001 | |||
| Voluntary discharge | 0 (0.0) | 1 (0.2) | 0 (0.0) | |
| Home | 433 (87.3) | 313 (77.7) | 75 (51.0) | |
| Death | 8 (1.6) | 58 (14.4) | 55 (37.4) | |
| Health center transfer | 18 (3.6) | 3 (0.7) | 10 (6.8) | |
| Hospital transfer | 14 (2.8) | 16 (4.0) | 3 (2.0) | |
| Not registered | 23 (4.6) | 12 (3.0) | 4 (2.7) | |
| CCI | 3.2 (2.4) | 3.1 (2.2) | 6.2 (2.2) | <0.001 |
| Myocardial infarction (yes (%)) | 40 (8.1) | 17 (4.3) | 22 (15.1) | <0.001 |
| Congestive heart failure (yes (%)) | 19 (3.8) | 11 (2.8) | 24 (16.4) | <0.001 |
| Peripheral vascular disease (yes (%)) | 18 (3.6) | 3 (0.8) | 11 (7.5) | <0.001 |
| Cerebrovascular accident (yes (%)) | 8 (1.6) | 5 (1.3) | 9 (6.2) | 0.001 |
| Dementia (yes (%)) | 23 (4.6) | 8 (2.0) | 11 (7.5) | 0.01 |
| COPD (yes (%)) | 67 (13.5) | 35 (8.8) | 29 (19.9) | 0.002 |
| Connective tissue disease (yes (%)) | 8 (1.6) | 1 (0.3) | 4 (2.7) | 0.041 |
| Peptic ulcer disease (yes (%)) | 1 (0.2) | 0 (0.0) | 1 (0.7) | 0.271 |
| Liver disease (yes (%)) | 17 (3.4) | 16 (4.0) | 2 (1.4) | 0.314 |
| Diabetes mellitus (yes (%)) | 89 (18.0) | 59 (14.8) | 46 (31.5) | <0.001 |
| Hemiplegia (yes (%)) | 1 (0.2) | 1 (0.3) | 0 (0.0) | 0.837 |
| Moderate to severe CKD (yes (%)) | 44 (8.9) | 46 (11.6) | 63 (43.2) | <0.001 |
| Solid tumor (yes (%)) | 12 (2.4) | 15 (3.8) | 17 (11.6) | <0.001 |
| Lymphoma (yes (%)) | 8 (1.6) | 5 (1.3) | 3 (2.1) | 0.784 |
| Leukemia (yes (%)) | 4 (0.8) | 2 (0.5) | 2 (1.4) | 0.586 |
| AIDS (yes (%)) | 0 (0.0) | 2 (0.5) | 0 (0.0) | 0.199 |
| OR (95% CI) | p | AUC | ||
|---|---|---|---|---|
| Model 1 | 0.801 | |||
| Age-independent CCI | 1.09 | (0.97–1.21) | 0.126 | |
| Sex (male) | 2.66 | (1.69–4.25) | 0.000 | |
| Age | 1.09 | (1.07–1.11) | 0.000 | |
| Model 2 | 0.810 | |||
| Age-independent CCI | 1.10 | (0.98–1.23) | 0.087 | |
| Oxygen saturation | 0.94 | (0.9–0.98) | 0.007 | |
| Temperature | 1.12 | (0.82–1.54) | 0.469 | |
| Sex (male) | 2.55 | (1.63–4.09) | 0.000 | |
| Age | 1.09 | (1.07–1.11) | 0.000 | |
| Model 3 | 0.871 | |||
| Cluster (Cluster B) | 12.83 | (6.11–30.54) | 0.000 | |
| Cluster (Cluster C) | 14.29 | (6.66–34.43) | 0.000 | |
| Age-independent CCI | 1.05 | (0.93–1.18) | 0.431 | |
| Oxygen saturation | 0.96 | (0.92–1) | 0.071 | |
| Temperature | 0.81 | (0.58–1.13) | 0.231 | |
| Sex (male) | 2.12 | (1.31–3.52) | 0.003 | |
| Age | 1.08 | (1.06–1.11) | 0.000 | |
| OR (95% CI) | p | AUC | ||
|---|---|---|---|---|
| Model 1 | 0.775 | |||
| Age-independent CCI | 1.18 | (1.08–1.29) | 0.000 | |
| Sex (male) | 1.17 | (0.9–1.53) | 0.246 | |
| Age | 1.02 | (1.01–1.03) | 0.000 | |
| Model 2 | 0.749 | |||
| Age-independent CCI | 1.20 | (1.1–1.32) | 0.000 | |
| Oxygen saturation | 1.01 | (0.98–1.05) | 0.467 | |
| Temperature | 1.49 | (1.22–1.83) | 0.000 | |
| Sex (male) | 1.16 | (0.88–1.51) | 0.291 | |
| Age | 1.02 | (1.01–1.03) | 0.000 | |
| Model 3 | 0.807 | |||
| Cluster (Cluster B) | 2.22 | (1.64–3.01) | 0.000 | |
| Cluster (Cluster C) | 1.71 | (1.08–2.76) | 0.024 | |
| Age-independent CCI | 1.21 | (1.1–1.33) | 0.000 | |
| Oxygen saturation | 1.02 | (0.99–1.06) | 0.205 | |
| Temperature | 1.28 | (1.04–1.59) | 0.021 | |
| Sex (male) | 1.00 | (0.75–1.32) | 0.980 | |
| Age | 1.02 | (1.01–1.03) | 0.000 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
San-Cristobal, R.; Martín-Hernández, R.; Ramos-Lopez, O.; Martinez-Urbistondo, D.; Micó, V.; Colmenarejo, G.; Villares Fernandez, P.; Daimiel, L.; Martínez, J.A. Longwise Cluster Analysis for the Prediction of COVID-19 Severity within 72 h of Admission: COVID-DATA-SAVE-LIFES Cohort. J. Clin. Med. 2022, 11, 3327. https://doi.org/10.3390/jcm11123327
San-Cristobal R, Martín-Hernández R, Ramos-Lopez O, Martinez-Urbistondo D, Micó V, Colmenarejo G, Villares Fernandez P, Daimiel L, Martínez JA. Longwise Cluster Analysis for the Prediction of COVID-19 Severity within 72 h of Admission: COVID-DATA-SAVE-LIFES Cohort. Journal of Clinical Medicine. 2022; 11(12):3327. https://doi.org/10.3390/jcm11123327
Chicago/Turabian StyleSan-Cristobal, Rodrigo, Roberto Martín-Hernández, Omar Ramos-Lopez, Diego Martinez-Urbistondo, Víctor Micó, Gonzalo Colmenarejo, Paula Villares Fernandez, Lidia Daimiel, and Jose Alfredo Martínez. 2022. "Longwise Cluster Analysis for the Prediction of COVID-19 Severity within 72 h of Admission: COVID-DATA-SAVE-LIFES Cohort" Journal of Clinical Medicine 11, no. 12: 3327. https://doi.org/10.3390/jcm11123327
APA StyleSan-Cristobal, R., Martín-Hernández, R., Ramos-Lopez, O., Martinez-Urbistondo, D., Micó, V., Colmenarejo, G., Villares Fernandez, P., Daimiel, L., & Martínez, J. A. (2022). Longwise Cluster Analysis for the Prediction of COVID-19 Severity within 72 h of Admission: COVID-DATA-SAVE-LIFES Cohort. Journal of Clinical Medicine, 11(12), 3327. https://doi.org/10.3390/jcm11123327