
Design and Validation of a Scale of Knowledge of Cardiovascular Risk Factors and Lifestyle after Coronary Event

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
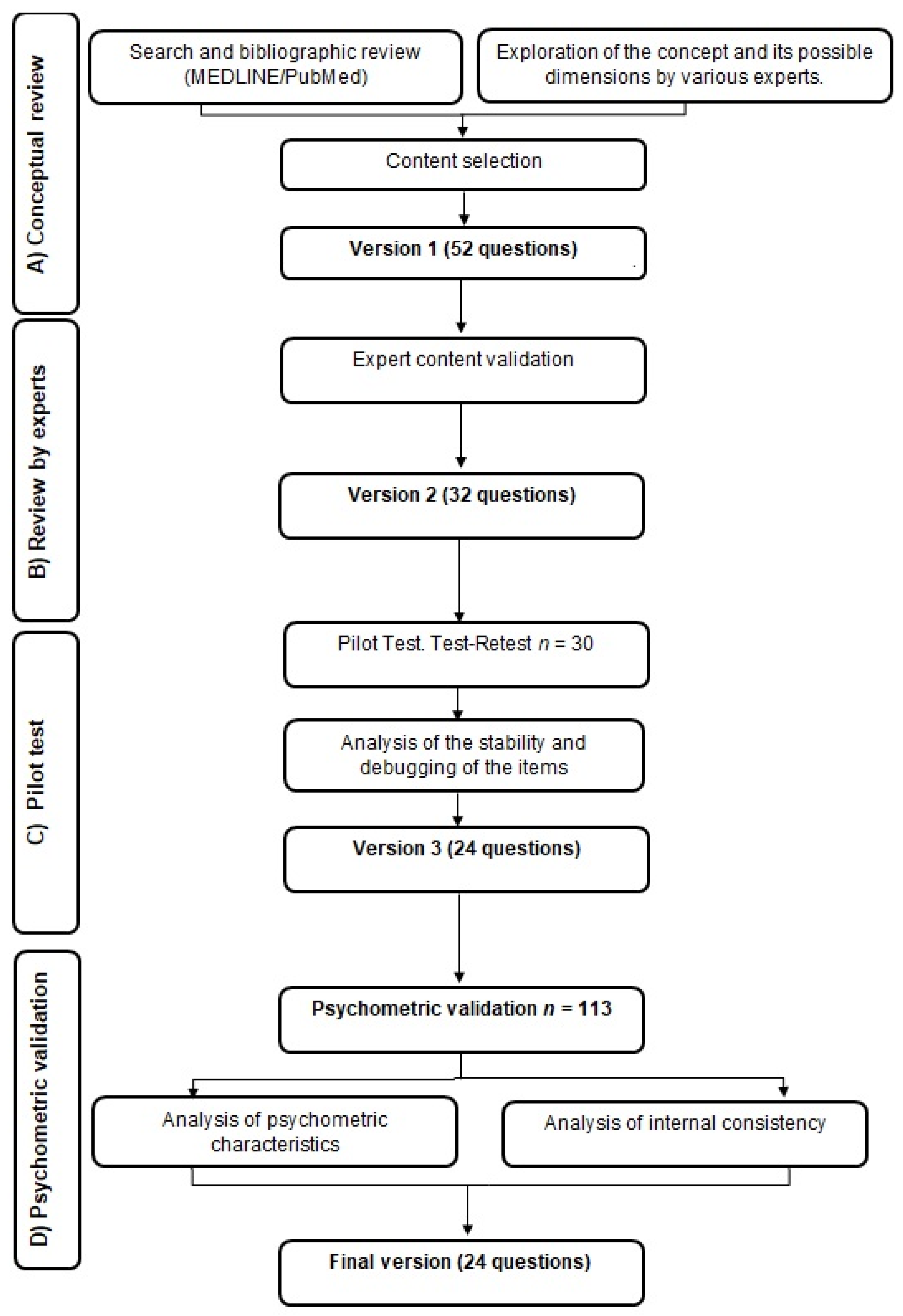
2.1. Study Design
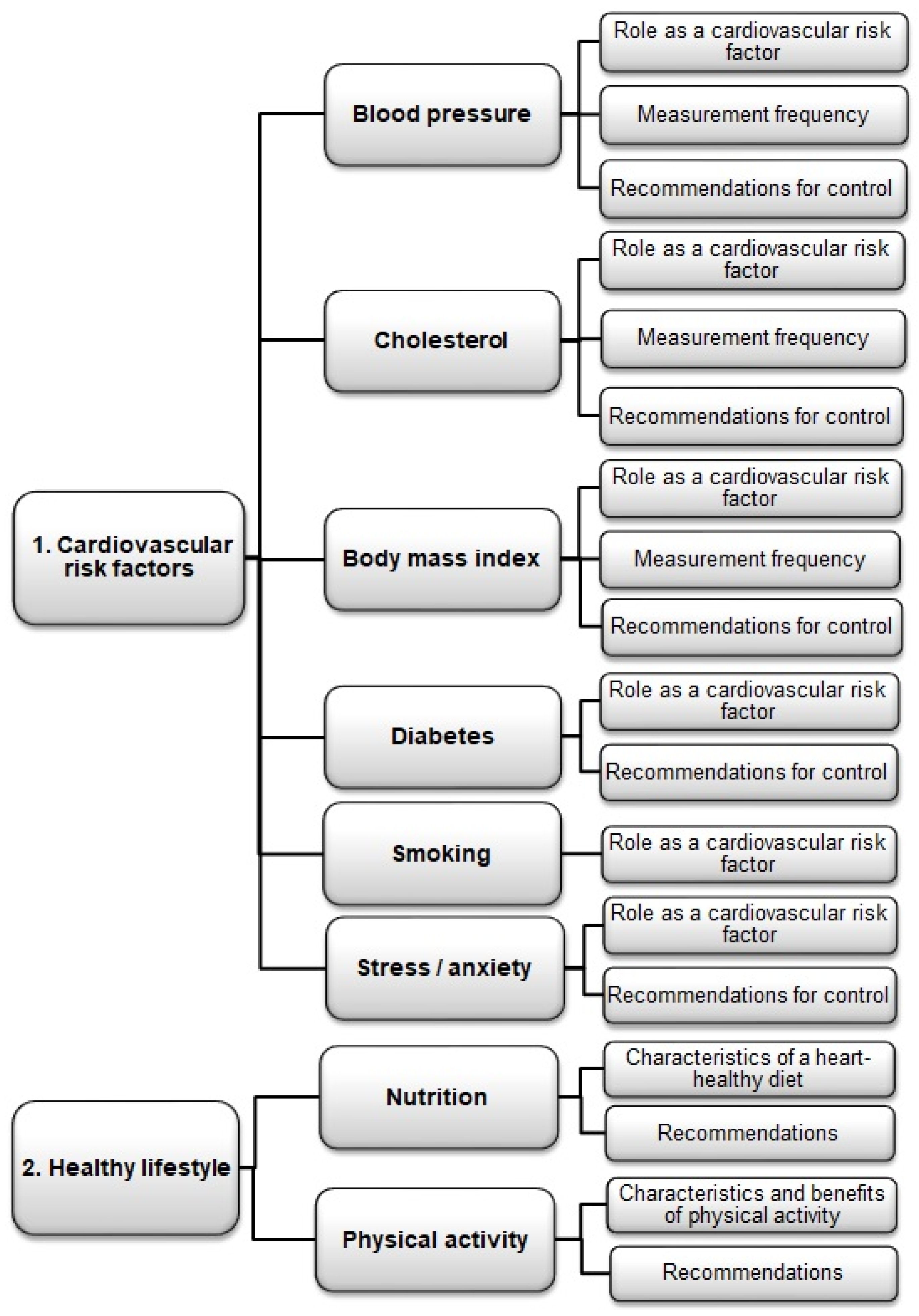
2.2. Conceptual Review
Design of the Scale
2.3. Review by Experts
Validation of Content by Experts
2.4. Pilot Test: Test–Retest
2.4.1. Stability Analysis
2.4.2. Applicability of the Instrument and Refining the Items
2.5. Psychometric Validation
2.5.1. Participants
Inclusion Criteria
Exclusion Criteria
2.5.2. Sample Size
2.5.3. Psychometric Characteristics
2.6. Clinical Variables Studied
2.7. Statistical Analysis of the Data
2.8. Ethical and Legal Aspects
3. Results
3.1. Pilot Test

{kind=link}
{kind=link}
| Test | Retest | ||
|---|---|---|---|
| Cronbach’s Alpha | 0.695 | 0.756 | |
| Reliability/Internal Consistency | Stability | ||
| Questions | Item-Total Correlation | Pearson Correlation Coefficient | |
| Test | Retest | Test–Retest | |
| Q 1 | 0.458 | 0.450 | 0.537 |
| Q 2 | 0.201 | 0.236 | 0.545 |
| Q 3 | −0.113 | 0.260 | 0.406 |
| Q 4 | 0.419 | 0.273 | 0.580 |
| Q 5 | 0.331 | 0.126 | 0.447 |
| Q 6 | 0.076 | 0.069 | 0.734 |
| Q 7 | 0.519 | 0.402 | 0.447 |
| Q 8 | 0.194 | 0.344 | 0.659 |
| Q 9 | 0.530 | 0.195 | 0.272 |
| Q 10 | 0.301 | 0.456 | 0.547 |
| Q 11 | 0.504 | 0.561 | 0.660 |
| Q 12 | 0.516 | 0.508 | 0.705 |
| Q 13 | −0.147 | −0.039 | 0.324 |
| Q 14 | 0.348 | 0.243 | 0.605 |
| Q 15 | 0.320 | 0.657 | 0.403 |
| Q 16 | 0.216 | 0.171 | 0.076 |
| Q 17 | 0.435 | 0.321 | 0.405 |
| Q 18 | 0.509 | 0.381 | 0.663 |
| Q 19 | 0.031 | 0.345 | 0.227 |
| Q 20 | 0.187 | 0.429 | 0.267 |
| Q 21 | 0.582 | 0.576 | 0.459 |
| Q 22 | 0.268 | 0.374 | 0.454 |
| Q 23 | 0.556 | 0.411 | 0.557 |
| Q 24 | 0.365 | 0.588 | 0.447 |
| Q 25 | 0.070 | 0.565 | 0.407 |
| Q 26 | 0.357 | 0.166 | 0.465 |
| Q 27 | 0.357 | 0.553 | 0.639 |
| Q 28 | 0.351 | 0.530 | 0.715 |
| Q 29 | 0.325 | 0.319 | 0.501 |
| Q 30 | 0.642 | 0.597 | 0.662 |
| Q 31 | 0.405 | 0.289 | 0.245 |
| Q 32 | 0.088 | 0.419 | 0.131 |
3.2. Psychometric Validation
| Gender % (n) | |
| Men % (n) | 68.1 (77) |
| Women % (n) | 31.9 (36) |
| Age mean ± SD | 60.25 ± 9.04 |
| Men mean ± SD | 58.48 ± 9.18 |
| Women mean ± SD | 64.03 ± 7.57 |
| Obesity % (n) | 42.5 (48) |
| BMI (kg/m2) mean ± SD | 29.28 ± 4.94 |
| Waist circumference (cm) mean ± SD | 104.57 ± 10.52 |
| HTN % (n) | 57.5 (65) |
| SBP (mmHg) mean ± SD | 132.12 ± 19.26 |
| DBP (mmHg) mean ± SD | 75.24 ± 10.57 |
| Heart rate (beats/minute) mean ± SD | 73.78 ± 12.44 |
| Diabetes % (n) | 33.6 (38) |
| Dyslipidemia % (n) | 53.1 (60) |
| Total Cholesterol (mg/dL) mean ± DE | 188.03 ± 51.47 |
| LDLc (mg/dL) mean ± DE | 121.35 ± 43.12 |
| HDLc (mg/dL) mean ± DE | 41.51 ± 12.16 |
| Smokers % (n) | 37.2 (42) |
| Former smoker % (n) | 31.9 (36) |
| Number of cardiovascular risk factors mean ± SD | 2.22 ± 1.15 |
| Cardiovascular risk (%) mean ± SD | 6.82 ± 3.43 |
| Personal history CVD % (n) | 6.2 (7) |
| NSTEMI % (n) | 0.9 (1) |
| STEMI % (n) | 3.5 (4) |
| Stable angina % (n) | 1.8 (2) |
| Family history | |
| Angina % (n) | 4.4 (5) |
| Heart attack % (n) | 27.4 (31) |
| Current reason PCI | |
| Stable angina % (n) | 27.4 (31) |
| Unstable angina % (n) | 17.7 (20) |
| NSTEMI % (n) | 21.2 (24) |
| STEMI % (n) | 33.6 (38) |
| Previous Treatment | |
| Anticoagulants % (n) | 1.8 (2) |
| Antiplatelet % (n) | 31.0 (35) |
| B-blockers % (n) | 22.1 (25) |
| Calcium channel blockers % (n) | 17.7 (20) |
| ACE-I % (n) | 21.2 (24) |
| ARB II % (n) | 28.3 (32) |
| Nitrates % (n) | 7.1 (8) |
| Diuretics % (n) | 19.5 (22) |
| Insulin % (n) | 8.8 (10) |
| Oral Antidiabetics % (n) | 27.4 (31) |
| Estatins % (n) | 46.0 (52) |
| Omeprazole % (n) | 35.4 (40) |
| Other % (n) | 46.0 (52) |
| Questions | ||
|---|---|---|
| Cronbach’s Alpha | 0.887 | |
| Reliability Internal Consistency. | ||
| Item-Total Correlation | ||
| Q 1 | I consider that only adults with high blood pressure should measure their blood pressure regularly. | 0.410 |
| Q 2 | High blood pressure increases the risk of cardiovascular disease. | 0.485 |
| Q 3 | Diet and doing physical exercise help to lower blood pressure. | 0.546 |
| Q 4 | All adults should have a regular blood test to monitor blood cholesterol levels. | 0.582 |
| Q 5 | Following a diet and doing physical exercise is not a very effective way to lower blood cholesterol levels. | 0.687 |
| Q 6 | Having high blood cholesterol levels increases the chances of suffering from cardiovascular diseases. | 0.567 |
| Q 7 | Bodyweight has little influence on cardiovascular health. | 0.665 |
| Q 8 | I consider that it is NOT necessary to measure body weight regularly. | 0.518 |
| Q 9 | Overweight and obesity increase the risk of cardiovascular disease. | 0.566 |
| Q 10 | Weight loss in obese people helps to control diabetes. | 0.470 |
| Q 11 | Diet is a part of the treatment of diabetes. | 0.569 |
| Q 12 | High blood sugar hardly increases the risk of cardiovascular disease. | 0.548 |
| Q 13 | Tobacco is harmful to cardiovascular health. | 0.391 |
| Q 14 | Being a passive smoker hardly increases the risk of suffering from cardiovascular disease. | 0.399 |
| Q 15 | Being a light smoker is NOT harmful to your health. | 0.433 |
| Q 16 | Stress hardly influences cardiovascular health. | 0.728 |
| Q 17 | Doing exercise reduces stress. | 0.643 |
| Q 18 | Stress is harmful to cardiovascular health. | 0.541 |
| Q 19 | Food has little influence on cardiovascular health. | 0.512 |
| Q 20 | It is better to eat fresh food than ready-made food. | 0.508 |
| Q 21 | Eating fruit and vegetables every day is recommended. | 0.469 |
| Q 22 | People should walk for 30–45 min every day. | 0.409 |
| Q 23 | Doing physical activity hardly improves cardiovascular health. | 0.718 |
| Q 24 | Lack of physical exercise makes you more likely to suffer from cardiovascular diseases. | 0.563 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. Fact Sheets [Internet]. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 18 October 2021).
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Rydén, L.; Hoes, A.; Grobbee, D.; Maggioni, A.P.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Primary prevention efforts are poorly developed in people at high cardiovascular risk: A report from the European Society of Cardiology EURObservational Research Programme EUROASPIRE V survey in 16 European countries. Eur. J. Prev. Cardiol. 2020, 28, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2022, 75, 429. [Google Scholar] [CrossRef]
- Marquina, C.; Zomer, E.; Vargas-Torres, S.; Zoungas, S.; Ofori-Asenso, R.; Liew, D.; Ademi, Z. Novel Treatment Strategies for Secondary Prevention of Cardiovascular Disease: A Systematic Review of Cost-Effectiveness. PharmacoEconomics 2020, 38, 1095–1113. [Google Scholar] [CrossRef] [PubMed]
- Ghisi, G.L.; Abdallah, F.; Grace, S.L.; Thomas, S.; Oh, P. A systematic review of patient education in cardiac patients: Do they increase knowledge and promote health behavior change? Patient Educ. Couns. 2014, 95, 160–174. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Brown, J.P.; Clark, A.M.; Dalal, H.; Rossau, H.; Bridges, C.; Taylor, R.S. Patient education in the management of coronary heart disease. Cochrane Database Syst. Rev. 2017, 2021, CD008895. [Google Scholar] [CrossRef]
- Nolan, M.T.; Mckee, G. Is Knowledge level of coronary heart disease and risk factors among post-percutaneous coronary intervention patients adequate? J. Cardiovas Nurs. 2016, 31, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Hassen, H.Y.; Aerts, N.; Demarest, S.; Manzar, D.; Abrams, S.; Bastiaens, H. Validation of the Dutch-Flemish translated ABCD questionnaire to measure cardiovascular diseases knowledge and risk perception among adults. Sci. Rep. 2021, 11, 8952. [Google Scholar] [CrossRef] [PubMed]
- Woringer, M.; Nielsen, J.J.; Zibarras, L.; Evason, J.; Kassianos, A.; Harris, M.; Majeed, A.; Soljak, M. Development of a questionnaire to evaluate patients’ awareness of cardiovascular disease risk in England’s National Health Service Health Check preventive cardiovascular programme. BMJ Open 2017, 7, e014413. [Google Scholar] [CrossRef]
- Wagner, J.; Lacey, K.; Chyun, D.; Abbott, G. Development of a questionnaire to measure heart disease risk knowledge in people with diabetes: The Heart Disease Fact Questionnaire. Patient Educ. Couns. 2005, 58, 82–87. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Giornale Ital. Cardiol. (Rome) 2018, 19, 3S–73S. [Google Scholar]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, D.V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Bernal-Jiménez, M.; Calle-Pérez, G.; Gutiérrez-Barrios, A.; Gheorghe, L.; Solano-Mulero, A.; Rodríguez-Martín, A.; Tur, J.; Vázquez-García, R.; Santi-Cano, M. Lifestyle and Treatment Adherence Intervention after a Coronary Event Based on an Interactive Web Application (EVITE): Randomized Controlled Clinical Trial Protocol. Nutrients 2021, 13, 1818. [Google Scholar] [CrossRef] [PubMed]
- Ghisi, G.L.D.M.; Grace, S.L.; Thomas, S.; Evans, M.F.; Oh, P. Development and psychometric validation of the second version of the Coronary Artery Disease Education Questionnaire (CADE-Q II). Patient Educ. Couns. 2015, 98, 378–383. [Google Scholar] [CrossRef]
- Hair, J.F. Anderson RE. Multivariate Data Analysis; Prentice Hall: Hoboken, NJ, USA, 1998. [Google Scholar]
- Nunnally, J.C. Psychometric Theory, 2nd ed.; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Potvin, L.; Richard, L.; Edwards, A.C. Knowledge of cardiovascular disease risk factors among the Canadian population: Relationships with indicators of socioeconomic status. Can. Med. Assoc. J. 2000, 162, S5–S11. [Google Scholar]
- Marrugat, J.; Vila, J.; Baena-Díez, J.M.; Grau, M.; Sala, J.; Ramos, R.; Subirana, I.; Fitó, M.; Elosua, R. Relative validity of the 10-year cardiovascular risk estimate in a population cohort of the REGICOR study. Rev. Esp. Cardiol. 2012, 64, 385–394. [Google Scholar] [CrossRef]
- Alm-Roijer, C.; Stagmo, M.; Udén, G.; Erhardt, L.R. Better Knowledge Improves Adherence to Lifestyle Changes and Medication in Patients with Coronary Heart Disease. Eur. J. Cardiovasc. Nurs. 2004, 3, 321–330. [Google Scholar] [CrossRef]
- Alm-Roijer, C.; Fridlund, B.; Stagmo, M.; Erhardt, L. Knowing Your Risk Factors for Coronary Heart Disease Improves Adherence to Advice on Lifestyle Changes and Medication. J. Cardiovasc. Nurs. 2006, 21, E24–E31. [Google Scholar] [CrossRef]
- Amariles, P.; Faus, M.J.; Machuca, M.; Gonzalez-Zapata, L.; Baena, M.I.; Quesada, F. Evaluation of a knowledge questionnaire about cardiovascular disease in Spanish community pharmacies. Aten Farm. 2009, 11, 101–109. [Google Scholar]
- Amariles, P.; Pino-Marín, D.; Sabater-Hernández, D.; García-Jiménez, E.; Roig-Sánchez, I.; Faus, M.J. Fiabilidad y validez externa de un cuestionario de conocimiento sobre riesgo y enfermedad cardiovascular en pacientes que acuden a farmacias comunitarias de España. Aten Prim. 2016, 48, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Huang, Y.-J.; Zhao, L.; Wang, W.; Liu, S.; He, G.-P.; Liao, L.; Zeng, Y. Association between knowledge and risk for cardiovascular disease among older adults: A cross-sectional study in China. Int. J. Nurs. Sci. 2020, 7, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, E.; Romate, J. Behavioural Risk Factors, Hypertension Knowledge, and Hypertension in Rural India. Int. J. Hypertens. 2020, 2020, 8108202–8108207. [Google Scholar] [CrossRef] [PubMed]
- Mifsud, J.L.; Galea, J.; Garside, J.; Stephenson, J.; Astin, F. Motivational interviewing to support modifiable risk factor change in individuals at increased risk of cardiovascular disease: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0241193. [Google Scholar] [CrossRef]
- Kayaniyil, S.; Ardern, C.I.; Winstanley, J.; Parsons, C.; Brister, S.; Oh, P.; Stewart, D.E.; Grace, S.L. Degree and correlates of cardiac knowledge and awareness among cardiac inpatients. Patient Educ. Couns. 2009, 75, 99–107. [Google Scholar] [CrossRef] [Green Version]
- Boateng, D.; Wekesah, F.; Browne, J.L.; Agyemang, C.; Agyei-Baffour, P.; Aikins, A.D.-G.; Smit, H.A.; Grobbee, D.E.; Klipstein-Grobusch, K. Knowledge and awareness of and perception towards cardiovascular disease risk in sub-Saharan Africa: A systematic review. PLoS ONE 2017, 12, e0189264. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Chair, S.Y.; Wong, E.M.-L.; Taylor-Piliae, R.E.; Qiu, X.C.H.; Li, X.M. Metabolic Syndrome Knowledge among Adults with Cardiometabolic Risk Factors: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 159. [Google Scholar] [CrossRef] [Green Version]
- Mullie, P.; Clarys, P. Association between Cardiovascular Disease Risk Factor Knowledge and Lifestyle. Food Nutr. Sci. 2011, 2, 1048–1053. [Google Scholar] [CrossRef] [Green Version]
| Variance (%) | Cronbach’s Alpha—Dimension | Dimension—Total Correlation | Item—Dimension Correlation | ||
|---|---|---|---|---|---|
| Factor 1 Knowledge of lifestyle habits | 14.695 | 0.821 | 0.844 | ||
| Q 16. | Stress hardly influences cardiovascular health. | 0.866 | |||
| Q 17. | Doing exercise reduces stress. | 0.735 | |||
| Q 19. | Food has little influence on cardiovascular health. | 0.703 | |||
| Q 23. | Doing physical activity hardly improves cardiovascular health. | 0.835 | |||
| Q 24. | Lack of physical exercise makes you more likely to suffer from cardiovascular diseases. | 0.709 | |||
| Factor 2 Knowledge of control of cholesterol and blood pressure | 12.916 | 0.829 | 0.746 | ||
| Q 2. | High blood pressure increases the risk of cardiovascular disease. | 0.760 | |||
| Q 3. | Diet and doing physical exercise help to lower blood pressure. | 0.755 | |||
| Q 4. | All adults should have a regular blood test to monitor blood cholesterol levels. | 0.844 | |||
| Q 5. | Following a diet and doing physical exercise is not a very effective way to lower blood cholesterol levels. | 0.703 | |||
| Q 6. | Having high blood cholesterol levels increases the chances of suffering from cardiovascular diseases. | 0.864 | |||
| Factor 3 Knowledge of lifestyle recommendations | 12.441 | 0.725 | 0.660 | ||
| Q 13. | Tobacco is harmful to cardiovascular health. | 0.516 | |||
| Q 18. | Stress is harmful to cardiovascular health. | 0.749 | |||
| Q 20. | It is better to eat fresh food than ready-made food. | 0.803 | |||
| Q 21. | Eating fruit and vegetables every day is recommended. | 0.814 | |||
| Q 22. | People should walk for 30–45 min every day. | 0.672 | |||
| Factor 4 Knowledge of cardiovascular risks | 8.650 | 0.505 | 0.582 | ||
| Q 1. | I consider that only adults with high blood pressure should measure their blood pressure regularly. | 0.657 | |||
| Q 9. | Overweight and obesity increase the risk of cardiovascular disease. | ||||
| Q 14. | Being a passive smoker hardly increases the risk of suffering from cardiovascular disease. | 0.759 | |||
| Q 15. | Being a light smoker is NOT harmful to your health. | 0.729 | |||
| Factor 5 Knowledge of diabetes mellitus | 8.340 | 0.696 | 0.683 | ||
| Q 10. | Weight loss in obese people helps to control diabetes. | 0.782 | |||
| Q 11. | Diet is a part of the treatment of diabetes. | 0.838 | |||
| Q 12. | High blood sugar hardly increases the risk of cardiovascular disease. | 0.777 | |||
| Total | 57.041 | 0.887 | |||
| Knowledge Level | ||
|---|---|---|
| Mean ± SD (CI 95%) | p | |
| Sex | ||
| Men | 105.97 ± 9.54 (0.07–7.76) | 0.046 |
| Women | 102.96 ± 9.77 (0.07–7.76) | |
| Education level | ||
| Low | 99.20 ± 11.93 (93.61–104.79) | 0.003 |
| Moderate | 105.92 ± 7.85 (103.30–108.54) | |
| High | 109.78 ± 8.76 (105.42–114.13) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernal-Jiménez, M.Á.; Calle-Pérez, G.; Gutiérrez-Barrios, A.; Gheorghe, L.; Solano-Mulero, A.M.; Trujillo-Garrido, N.; Rodríguez-Martín, A.; Tur, J.A.; Vázquez-García, R.; Santi-Cano, M.J. Design and Validation of a Scale of Knowledge of Cardiovascular Risk Factors and Lifestyle after Coronary Event. J. Clin. Med. 2022, 11, 2773. https://doi.org/10.3390/jcm11102773
Bernal-Jiménez MÁ, Calle-Pérez G, Gutiérrez-Barrios A, Gheorghe L, Solano-Mulero AM, Trujillo-Garrido N, Rodríguez-Martín A, Tur JA, Vázquez-García R, Santi-Cano MJ. Design and Validation of a Scale of Knowledge of Cardiovascular Risk Factors and Lifestyle after Coronary Event. Journal of Clinical Medicine. 2022; 11(10):2773. https://doi.org/10.3390/jcm11102773
Chicago/Turabian StyleBernal-Jiménez, María Ángeles, Germán Calle-Pérez, Alejandro Gutiérrez-Barrios, Livia Gheorghe, Ana María Solano-Mulero, Nuria Trujillo-Garrido, Amelia Rodríguez-Martín, Josep A. Tur, Rafael Vázquez-García, and María José Santi-Cano. 2022. "Design and Validation of a Scale of Knowledge of Cardiovascular Risk Factors and Lifestyle after Coronary Event" Journal of Clinical Medicine 11, no. 10: 2773. https://doi.org/10.3390/jcm11102773
APA StyleBernal-Jiménez, M. Á., Calle-Pérez, G., Gutiérrez-Barrios, A., Gheorghe, L., Solano-Mulero, A. M., Trujillo-Garrido, N., Rodríguez-Martín, A., Tur, J. A., Vázquez-García, R., & Santi-Cano, M. J. (2022). Design and Validation of a Scale of Knowledge of Cardiovascular Risk Factors and Lifestyle after Coronary Event. Journal of Clinical Medicine, 11(10), 2773. https://doi.org/10.3390/jcm11102773