




Effect of Supervised and Unsupervised Exercise Training in Outdoor Gym on the Lifestyle of Elderly People
 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
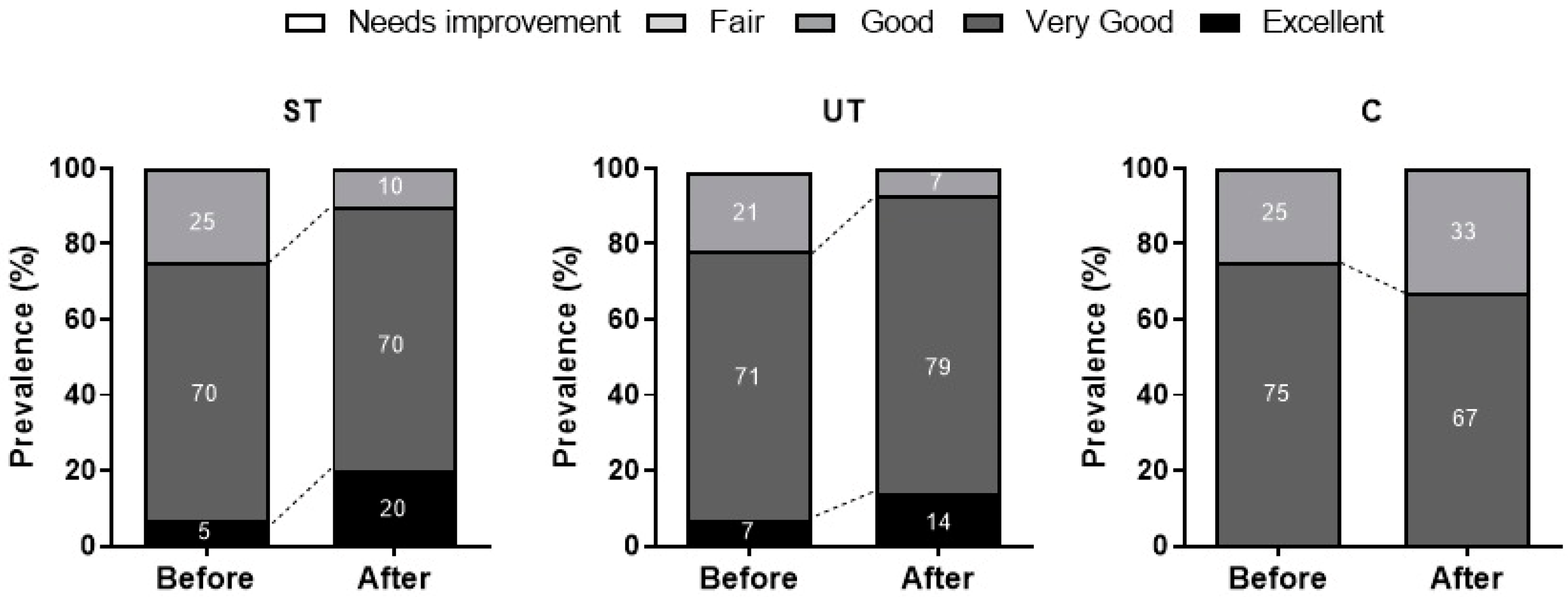
- Supervised Trained (ST, n: 20; 66 ± 5 years old): Elderly participants subjected to training with controlled cadence and supervised by a Physical Education professional throughout the training program.
- Unsupervised Trained (UT, n: 20; 68 ± 7 years old): Elderly participants who exercised freely without the supervision of a Physical Education professional throughout the program.
- Control (C, n: 20; 68 ± 5 years old): Elderly participants who did not engage in exercise but received support to maintain their daily routines throughout the entire investigation period.
2.1. Intervention
2.2. Evaluated Parameters
Lifestyle Questionnaire
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Guidelines on Physical Activity and Sedentary Behaviour. 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK566045/ (accessed on 27 January 2021).
- Oliveira, J.G.; França, S.P. Barreiras percebidas para a prática regular de atividade física de idosos. Geriatr. Gerontol. Aging 2014, 8, 165–170. [Google Scholar]
- De Oliveira, D.V.; Da Silva, T.P.D.S.; Scherer, F.C.; Do Nascimento, J.R.A., Jr.; Antunes, M.D. O tipo de exercício físico interfere na frequência da prática de atividade física, comportamento sedentário, composição corporal e estado nutricional do idoso? RBNE-Rev. Bras. Nutr. Esportiva 2019, 13, 3–16. [Google Scholar]
- Morais, M.; Passos, G.; Cintra, R.; Santana, M. Efeito de video games ativos sobre a capacidade funcional e o humor de idosos: Revisão sistemática e meta-análise. Rev. Bras. Atividade Física Saúde 2017, 22, 523–532. [Google Scholar] [CrossRef]
- Rica, R.L.; Shimojo, G.L.; Gomes, M.C.; Alonso, A.C.; Pitta, R.M.; Santa-Rosa, F.A.; Bocalini, D.S. Effects of a Kinect-based physical training program on body composition, functional fitness and depression in institutionalized older adults. Geriatr. Gerontol. Int. 2020, 20, 195–200. [Google Scholar] [CrossRef] [PubMed]
- de Macedo, R.M.; de Oliveira, M.D.R.P.; Cilião, M.R.; Prosdócimo, A.C.G.; de Macedo, A.C.B.; França, D.; Belemer, A.; Costantini, C.O.; Costantini, C.R. Nível de atividade física de idosos participantes de um programa de prevenção de doença cardiovascular. ASSOBRAFIR Ciênc. 2019, 6, 10–20. [Google Scholar]
- Pinheiro, W.L.; Coelho Filho, J.M. Perfil dos idosos usuários das academias ao ar livre para a terceira idade. Rev. Bras. Promoção Saúde 2017, 30, 93–101. [Google Scholar] [CrossRef][Green Version]
- Costa, B.G.G.; Freitas, C.R.; Silva, K.S. Atividade física e uso de equipamentos entre usuários de duas academias ao ar livre. Rev. Bras. Ativ. Fís. Saúde 2016, 21, 29–38. [Google Scholar] [CrossRef][Green Version]
- Salin, M.D.S.; Virtuoso, J.F.; Nepomuceno, A.S.N.; Weiers, G.G.; Mazo, G.Z. Golden Age Gym: Reasons for entry, permanence and satisfaction among participating older adults. Rev. Bras. Cineantropometria Desempenho Hum. 2014, 16, 152–160. [Google Scholar]
- Barbosa, R.R.N.; dos Santos Valente, A.M.; Machado, F.A.; do Nascimento, J.G.C.; Fortes, M.D.S.R.; Marson, R.A. O efeito agudo da cadência de execução sobre o número máximo de repetições no exercício de flexão de braços sobre o solo. Rev. Min. Educ. Fís. 2014, 23, 7–21. [Google Scholar]
- Mazo, G.Z.; Cardoso, F.L.; Aguiar, D.D. Programa de hidroginástica para idosos: Motivação, auto-estima e auto-imagem. Rev. Bras. Cineantropom Desempenho Hum. 2006, 8, 67–72. [Google Scholar]
- Fernandes, A.P.; Martins-Costa, H.C.; Vidigal, J.M.S.; Fermino, R.C. Estrutura, perfil dos frequentadores e padrão de utilização de Academias a Céu Aberto em Belo Horizonte, Minas Gerais. Rev. Bras. Atividade Fís. Saúde 2022, 27, 1–9. [Google Scholar] [CrossRef]
- Mathias, N.G.; Filho, J.M.; Szkudlarek, A.C.; Gallo, L.H.; Fermino, R.C.E.; Gomes, A.R.S. Motivos para a prática de atividades físicas em uma academia ao ar livre de paranaguá-pr. Rev. Bras. Ciênc. Esporte 2019, 4, 222–228. [Google Scholar] [CrossRef]
- Liu, Y.C.; Yang, W.W.; Fang, I.Y.; Pan, H.L.; Chen, W.H.; Liu, C. Training program with outdoor fitness equipment in parks offers no substantial benefits for functional fitness in active seniors: A randomized controlled trial. J. Aging Phys. Act. 2020, 29, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, W.A.; Rica, R.L.; Pontes, F.L., Jr.; Reis, V.M.; Bergamin, V.; Bocalini, D.S. Psychophysiological effects of different execution speeds of single bout exercise in outdoor fitness equipment performed by older men. Motriz 2022, 28, 1–8. [Google Scholar] [CrossRef]
- Barnett, A.G.; Van Der Pols, J.C.; Dobson, A.J. Regression to the mean: What it is and how to deal with it. Int. J. Epidemiol. 2005, 34, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez Añez, C.R.; Reis, R.S.; Petroski, E.L. Versão brasileira do questionário “estilo de vida fantástico”: Tradução e validação para adultos jovens. Arq. Bras. Cardiol. 2008, 91, 102–109. [Google Scholar] [CrossRef]
- Basso, M.S.R.; Schonardie, F.L.; Roncaglio, G. Perfil do estilo de vida de uma amostra de senhoras integrantes do PITI/UNIJUÍ. Salão Conhecimento 2021, 7, 3–9. [Google Scholar]
- Ferreira, L.K.; Meireles, J.F.F.; Ferreira, M.E.C. Evaluation of lifestyle and quality of life in the elderly: A literature review. Rev. Bras. Geriatr. E Gerontol. 2018, 21, 616–627. [Google Scholar] [CrossRef]
- Naughton, M.J.; Brunner, R.L.; Hogan, P.E.; Danhauer, S.C.; Brenes, G.A.; Bowen, D.J.; Shumaker, S.A. Global quality of life among whi women aged 80 years and older. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, S72–S78. [Google Scholar] [CrossRef][Green Version]
- Marques, J.F.; Sahb, N.A.; Ferreira, L.; Ferreira, M.E.C. Avaliação do estilo de vida de idosos residentes no município de juiz de fora–mg. Estud. Interdiscip. Sobre O Envelhec. 2021, 26, 29–46. [Google Scholar]
- Souza, C.A.; Fermino, R.C.; Anez, C.R.R.; Reis, R.S. Perfil dos frequentadores e padrão de uso das academias ao ar livre em bairros de baixa e alta renda de Curitiba-PR. Rev. Bras. Ativ. Fis. Saúde 2014, 19, 86–97. [Google Scholar] [CrossRef]
- Cerqueira, H.S.C.; Ulian, L.V. Avaliação do estilo de vida de idosos praticantes de musculação através do questionário estilo de vida fantástico. REGRASP-Rev. Para Grad. IFSP-Câmpus São Paulo 2021, 6, 75–94. [Google Scholar]
- De Macedo, M.G.; De Sales Ferreira, J.C. The health risks associated with the consumption of food supplements without nutritional guidance. Res. Soc. Dev. 2021, 10, e45610313593. [Google Scholar]
- Chatziralli, I.; Mitropoulos, P.; Parikakis, E.; Niakas, D.; Labiris, G. Risk factors for poor quality of life among patients with age-related macular degeneration. Semin. Ophthalmol. 2016, 32, 772–780. [Google Scholar] [CrossRef]
- Costa, I.M.; dos Reis Lopes, P.H.; Silveira, B.B.; Melo, L.D.C.; dos Santos, J.A.; Ferreira, E.B.; Guerra, E.N.S.; dos Reis, P.E.D. Dispositivos Eletrônicos para Fumar: Aliados ou adversários ao tabagismo? Concilium 2022, 22, 757–768. [Google Scholar] [CrossRef]
- Kirsch Micheletti, J.; Bláfoss, R.; Sundstrup, E.; Bay, H.; Pastre, C.M.; Andersen, L.L. Association between lifestyle and musculoskeletal pain: Cross-sectional study among 10,000 adults from the general working population. BMC Musculoskelet. Disord. 2019, 20, 609. [Google Scholar] [CrossRef]
- Visser, M.; Wijnhoven, H.A.; Comijs, H.C.; Thomése, F.G.; Twisk, J.W.; Deeg, D.J. A healthy lifestyle in old age and prospective change in four domains of functioning. J. Aging Health 2019, 31, 1297–1314. [Google Scholar] [CrossRef]
- Goulart, D.; Engroff, P.; Ely, L.S.; Sgnaolin, V.; Santos, E.F.D.; Terra, N.L.; De Carli, G.A. Tabagismo em idosos. Rev. Bras. Geriatr. Gerontol. 2010, 13, 313–320. [Google Scholar] [CrossRef]
- Pimenta, F.B.; Pinho, L.; Silveira, M.F.; Botelho, A.C.C. Fatores associados a doenças crônicas em idosos atendidos pela Estratégia de Saúde da Família. Ciênc Saúde Colet. 2015, 20, 2489–2498. [Google Scholar] [CrossRef]
- da Silva Santos, Á.; Viana, D.A.; de Souza, M.C.; Meneguci, J.; da Silveira, R.E.; Silvano, C.M.; Rodrigues, L.R.; Damião, R. Atividade física, álcool e tabaco entre idosos. Rev. Família Ciclos Vida Saúde Contexto Soc. 2014, 2, 6–13. [Google Scholar]
- Coutinho, L.S.B.; Tomasi, E. Déficit de autocuidado em idosos: Características, fatores associados e recomendações às equipes de Estratégia Saúde da Família. Interface-Comun. Saúde Educ. 2020, 24, e190578. [Google Scholar] [CrossRef]
- Ferrari, T.K.; Cesar, C.L.G.; Alves, M.C.G.P.; Barros, M.B.D.A.; Goldbaum, M.; Fisberg, R.M. Estilo de vida saudável em São Paulo, Brasil. Cad. Saúde Pública 2017, 33, e00188015. [Google Scholar] [CrossRef] [PubMed]
- Salonna, F.; Van Dijk, J.P.; Geckova, A.M.; Sleskova, M.; Groothoff, J.W.; Reijneveld, A.S. Social inequalities in changes in health-related behaviour among Slovak adolescents aged between 15 and 19: A longitudinal study. BMC Public Health 2008, 8, 57. [Google Scholar] [CrossRef]
- Freire, M.Q.; Firmo, J.D.R.; Firmo, I.D.R.; De Carvalho, K.C.N. Hidroginástica: Uma avaliação de seus benefícios sobre os transtornos de depressão, ansiedade e distúrbios do sono em idosos. Cipeex 2022, 3, 1–4. [Google Scholar]
- Moreno-Vecino, B.; Arija-Blázquez, A.; Pedrero-Chamizo, R.; Gómez-Cabello, A.; Alegre, L.M.; Perez-Lopez, F.R.; González-Gross, M.; Casajús, J.A.; Ara, I.; EXERNET Group. Sleep disturbance, obesity, physical fitness and quality of life in older women: EXERNET study group. Climacteric 2017, 20, 72–79. [Google Scholar] [CrossRef]
- Duran, S.; Mattar, P.; Bravo, N.; Moreno, C.; Reyes, S. Asociación entre calidad de vida y cantidad de sueño em adultos mayores de la Región Metropolitana y Región de Valparaíso, Chile. Rev. Med. Chile 2014, 142, 1371–1376. [Google Scholar] [CrossRef]
- dos Santos Silva, D.; Aidar, F.J.; Mendonça, T.P.; Souza, L.M.V.; dos Santos, J.L.; de Oliveira, J.U.; de Gama, D.M.; de Souza, R.F.; dos Santos, M.D.; Marçal, A.C.; et al. Glicemia e qualidade do sono em idosos participantes de um programa de exercício físico: Estudo piloto. Motricidade 2019, 15, 164–170. [Google Scholar]
- Reid, K.J.; Baron, K.G.; Lu, B.; Naylor, E.; Wolfe, L.; Zee, P.C. Aerobic exercise improves self-reported sleep and quality of life in older adults with insomnia. Sleep Med. 2010, 1, 934–940. [Google Scholar] [CrossRef]
- Alves, H.B.; Alves, H.B.; Vasconcelos, K.P.; Silva, C.T.L.; de Souza Silva, M.N.; Patrício, D.F.; Dantas, R.R.; de Melo, P.Y.B. Alterações da qualidade do sono em idosos e sua relação com doenças crônicas. Braz. J. Health Rev. 2020, 3, 5030–5042. [Google Scholar] [CrossRef]
- De Oliveira, D.V.; Antunes, M.D.; Oliveira, J. Ansiedade e sua relação com a qualidade de vida em idosos: Revisão narrativa. Cinergis 2017, 18, 316–322. [Google Scholar]
- Mcphee, J.S.; French, D.P.; Jac Kson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Agostino, D.; Daskalopoulou, C.; Wu, Y.T.; Koukounari, A.; Haro, J.M.; Tyrovolas, S.; Panagiotakos, D.B.; Prince, M.; Prina, A.M. The impact of physical activity on healthy ageing trajectories: Evidence from eight cohort studies. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, F.A.; Pirajá, W.C.; Silva, A.P.; Primo CP, F. Benefícios da prática de atividade física sistematizada no lazer de idosos: Algumas considerações. LICERE-Rev. Programa Pós-Grad. Interdiscip. Estud. Lazer 2015, 18, 262–304. [Google Scholar] [CrossRef]
- Marques, L.P.; Schneider, I.J.C.; D’orsi, E. Quality of life and its association with work, the Internet, participation in groups and physical activity among the elderly from the EpiFloripa survey, Florianópolis, Santa Catarina State, Brazil. Cad. Saúde Pública 2016, 32, e00143615. [Google Scholar] [CrossRef] [PubMed]
- Antunes, M.H.; More, C.L.O. Aposentadoria, saúde do idoso e saúde do trabalhador: Revisão integrativa da produção brasileira. Rev. Psicol. Organ. Trab. 2016, 16, 248–258. [Google Scholar] [CrossRef]
- Lu, C.; Yuan, L.; Lin, W.; Zhou, Y.; Pan, S. Depression and resilience mediates the effect of family function on quality of life of the elderly. Arch. Gerontol. Geriatr. 2017, 71, 34–42. [Google Scholar] [CrossRef] [PubMed]
- French, E.; Jones, J.B. Health, health insurance, and retirement: A survey. Annu. Rev. Econ. 2017, 9, 383–409. [Google Scholar] [CrossRef]
- Ilmakunnas, P.; Ilmakunnas, S. Health and retirement age: Comparison of expectations and actual retirement. Scand. J. Public Health 2018, 46, 18–31. [Google Scholar] [CrossRef]


{kind=link}
| Domain | Before | After | MD | 95% IC | ES | ANOVA | ||
|---|---|---|---|---|---|---|---|---|
| Time | TimexGroup | |||||||
| p | F | p | ||||||
| Family | ||||||||
| ST | 5.60 ± 2.39 | 6.15 ± 1.95 | −0.55 | −1.118–0.017 | 0.23 | =0.0606 | 0.3430 | =0.0711 |
| UT | 5.85 ± 2.44 | 6.35 ± 1.86 | −0.50 | −1.179–0.178 | 0.20 | =0.2203 | ||
| C | 5.83 ± 2.48 | 6.08 ± 2.39 | −0.25 | −0.983–0.483 | 0.10 | >0.9999 | ||
| Physical activity | ||||||||
| ST | 4.90 ± 2.07 | 6.10 ± 1.41 | −1.20 | −2.118–−0.282 | 0.57 | =0.0066 | 0.5394 | =0.5870 |
| UT | 4.92 ± 1.97 | 5.64 ± 1.86 | −0.71 | −1.811–0.382 | 0.36 | =0.3362 | ||
| C | 4.66 ± 2.10 | 5.33 ± 1.61 | −0.66 | −1.852–0.518 | 0.31 | =0.5045 | ||
| Nutrition | ||||||||
| ST | 8.80 ± 1.85 | 9.25 ± 2.14 | −0.45 | −0.992–0.092 | 0.24 | =0.1341 | 1.133 | =0.3315 |
| UT | 9.21 ± 1.62 | 9.50 ± 1.95 | −0.28 | −0.933–0.362 | 0.17 | =0.8343 | ||
| C | 9.08 ± 2.35 | 9.00 ± 2.25 | 0.08 | −0.616–0.783 | 0.03 | >0.9999 | ||
| Smoking | ||||||||
| ST | 13.95 ± 1.73 | 14.05 ± 1.79 | −0.10 | −0.391–0.191 | 0.05 | >0.9999 | 2.219 | =0.1211 |
| UT | 14.21 ± 1.12 | 14.35 ± 1.21 | −0.14 | −0.491–0.205 | 0.12 | =0.9376 | ||
| C | 14.00 ± 1.70 | 13.75 ± 1.81 | 0.25 | −0.126–0.626 | −0.14 | =0.3152 | ||
| Alcohol | ||||||||
| ST | 11.75 ± 1.11 | 11.80 ± 0.89 | −0.05 | −0.260–0.160 | 1.11 | >0.9999 | 2.981 | =0.0613 |
| UT | 11.64 ± 1.33 | 11.71 ± 1.06 | −0.07 | −0.322–0.179 | 0.05 | >0.9999 | ||
| C | 14.00 ± 1.70 | 13.75 ± 1.81 | 0.25 | −0.0215–0.521 | −0.15 | =0.0802 | ||
| Sleep | ||||||||
| ST | 13.40 ± 0.13 | 14.35 ± 2.08 | −0.95 | −1.789–−0.111 | 0.44 | =0.0216 | 1.022 | =0.0368 |
| UT | 13.71 ± 0.05 | 14.42 ± 1.86 | −0.71 | −1.717–0.288 | 0.34 | =0.2489 | ||
| C | 13.16 ± 2.69 | 13.33 ± 2.87 | −0.16 | −1.249–0.916 | 0.06 | >0.9999 | ||
| Behavior | ||||||||
| ST | 4.00 ± 2.20 | 4.75 ± 1.94 | −0.75 | −1.348–−0.152 | 0.34 | =0.0095 | 0.395 | =0.6758 |
| UT | 3.35 ± 2.30 | 4.07 ± 2.16 | −0.71 | −1.429–0.000 | 0.31 | =0.0501 | ||
| C | 3.16 ± 1.99 | 3.58 ± 1.56 | −0.41 | −1.188–0.355 | 0.21 | =0.5571 | ||
| Introspection | ||||||||
| ST | 7.60 ± 2.47 | 7.90 ± 2.65 | −0.30 | −0.780–0.180 | 0.12 | =0.3812 | 0.2661 | =0.7676 |
| UT | 7.92 ± 2.46 | 8.21 ± 2.66 | −0.28 | −0.859–0.288 | 0.11 | =0.6654 | ||
| C | 7.25 ± 2.09 | 7.33 ± 1.77 | −0.08 | −0.703–0.536 | 0.03 | >0.9999 | ||
| Work | ||||||||
| ST | 3.60 ± 0.50 | 3.70 ± 0.47 | −0.10 | −0.388–0.188 | 0.20 | >0.9999 | 0.2575 | =0.7742 |
| UT | 3.57 ± 0.51 | 3.71 ± 0.46 | −0.14 | −0.487–0.201 | 0.27 | =0.9222 | ||
| C | 3.58 ± 1.16 | 3.58 ± 0.79 | 0.00 | −0.372–0.372 | 0.00 | >0.9999 | ||
| Overall score | ||||||||
| ST | 73.60 ± 7.07 | 78.05 ± 6.69 | −4.45 | −6.222–−2.678 | 0.62 | <0.0001 | 4.270 | =0.0204 |
| UT | 74.42 ± 6.59 | 78.00 ± 5.69 | −3.57 | −5.690–−1.453 | 0.54 | =0.0004 | ||
| C | 72.91 ± 6.35 | 74.00 ± 5.08 | −1.08 | −3.371–1.205 | 0.17 | =0.7341 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbosa, W.A.; Leite, C.D.F.C.; Reis, C.H.O.; Machado, A.F.; Bullo, V.; Gobbo, S.; Bergamin, M.; Lima-Leopoldo, A.P.; Vancini, R.L.; Baker, J.S.; et al. Effect of Supervised and Unsupervised Exercise Training in Outdoor Gym on the Lifestyle of Elderly People. Int. J. Environ. Res. Public Health 2023, 20, 7022. https://doi.org/10.3390/ijerph20217022
Barbosa WA, Leite CDFC, Reis CHO, Machado AF, Bullo V, Gobbo S, Bergamin M, Lima-Leopoldo AP, Vancini RL, Baker JS, et al. Effect of Supervised and Unsupervised Exercise Training in Outdoor Gym on the Lifestyle of Elderly People. International Journal of Environmental Research and Public Health. 2023; 20(21):7022. https://doi.org/10.3390/ijerph20217022
Chicago/Turabian StyleBarbosa, Welmo A., Carine Danielle F. C. Leite, Carlos H. O. Reis, Alexandre F. Machado, Valentina Bullo, Stefano Gobbo, Marco Bergamin, Ana Paula Lima-Leopoldo, Rodrigo L. Vancini, Julien S. Baker, and et al. 2023. "Effect of Supervised and Unsupervised Exercise Training in Outdoor Gym on the Lifestyle of Elderly People" International Journal of Environmental Research and Public Health 20, no. 21: 7022. https://doi.org/10.3390/ijerph20217022
APA StyleBarbosa, W. A., Leite, C. D. F. C., Reis, C. H. O., Machado, A. F., Bullo, V., Gobbo, S., Bergamin, M., Lima-Leopoldo, A. P., Vancini, R. L., Baker, J. S., Rica, R. L., & Bocalini, D. S. (2023). Effect of Supervised and Unsupervised Exercise Training in Outdoor Gym on the Lifestyle of Elderly People. International Journal of Environmental Research and Public Health, 20(21), 7022. https://doi.org/10.3390/ijerph20217022