Appendix A. Detailed Country Data
Bangladesh
First case: 23 February 2020
Restrictions on in-person learning: 16 March 2020 to 30 September
Restrictions to on-site work: 19 March 2020 to 10 August 2021
Public events canceled: 16 March 2020 to 16 July 2021; 23 July 2021 through 30 September 2021
Gatherings restricted: 19 March 2020 to 16 July 2021; 23 July 2021 through 30 September 2021
Public transport closed: 19 March 2020 to 16 July 2021; 23 July 2021 to 11 August 2021
Stay-at-home restrictions: 19 March 2020 to 15 July 2021; 23 July 2021 through 30 September 2021
Internal movement restricted: 19 March 2020 to 31 May 2020; 16 June 2020 to 24 May 2021; 31 May 2021 to 15 July 2021; 23 July 2021 to 6 August 2021
International travel restrictions: 22 January 2020 through 30 September 2021
Income support: 13 April 2020 to 14 May 2020
Debt/contract relief: 19 March 2020 to 31 May 2021; 26 August 2021 to 19 September 2021
Fiscal measures: 25 March 2020 (USD 595,000,000); 5 April 2020 (USD 8,564,857,500); 13 April 2020 (USD 91,000,000)
International support: 22 March 2020 (USD 1,500,000); 5 April 2020 (USD 500,000,000)
Public information campaigns: 21 January 2020 through 30 September 2021
COVID testing becomes available: 1 March 2020
Contact tracing begins: 24 January 2020
Emergency healthcare investment: 18 March 2020 (USD 29,550,000); 13 April 2020 (USD 100,320,307)
Investment in vaccines: none
Mask first recommended: 30 May 2020
Vaccine available to high-risk populations: 14 December 2020
Protection of elderly begins: 26 January 2020
Barbados
First case: 3 March 2020
Restrictions on in-person learning: 19 March 2020 through 30 September 2021
Restrictions to on-site work: 28 March 2020 through 30 September 2021
Public events canceled: 17 March 2020 through 30 September 2021
Gatherings restricted: 17 March 2020 to 25 July 2020; 29 October 2020 through 30 September 2021
Public transport closed: 8 April 2020 to 9 October 2020; 29 October 2020 to 6 June 2021; 11 September 2021 through 30 September 2021
Stay-at-home restrictions: 28 March 2020 to 21 August 2020; 31 December 2020 to 29 June 2021; 25 July 2021 through 30 September 2021
Internal movement restricted: 3 April 2020 to 21 August 2020; 26 April 2021 to 17 May 2021
International travel restrictions: 26 January 2020 through 30 September 2021
Income support: 1 April 2020 through 30 September 2021
Debt/contract relief: 1 April 2020 through 30 September 2021
Fiscal measures: 22 March 2020 (USD 10,000,000); 23 April 2020 (USD 1,000,000,000)
International support: 19 June 2020 (USD 15000)
Public information campaigns: 22 January 2020 through 30 September 2021
COVID testing becomes available: 26 January 2020
Contact tracing begins: 17 March 2020
Emergency healthcare investment: 29 October 2020 (USD 11,613,382)
Investment in vaccines: none
Mask first recommended: 11 April 2020
Vaccine available to high-risk populations: 16 February 2021
Protection of elderly begins: 17 March 2020
Belgium
First case: 21 January 2020
Restrictions on in-person learning: 14 March 2020 through 30 September 2021
Restrictions to on-site work: 13 March 2020 through 30 September 2021
Public events canceled: 10 March 2020 through 30 September 2021
Gatherings restricted: 18 March 2020 through 30 September 2021
Public transport closed: 3 April 2021 to 19 April 2021
Stay-at-home restrictions: 18 March 2020 to 8 June 2020; 29 July 2020 to 27 August 2020; 19 October 2020 to 30 July 2021
Internal movement restricted: 14 March 2020 to 8 June 2020; 28 July 2020 to 12 August 2020
International travel restrictions: 4 March 2020
Income support: 6 March 2020 through 30 September 2021
Debt/contract relief: 6 March 2020 through 30 September 2021
Fiscal measures: 19 March 2020 (USD 260,000,000); 20 March 2020 (USD 9,608,192,466); 22 April 2020 (USD 320,000,000); 3 June 2020 (USD 505,000,000); 6 June 2020 (USD 3,950,000,000); 12 June 2020 (USD 123,000,000); 9 July 2020 (USD 63,000,000); 22 July 2020 (USD 588,000); 9 Sepetember 2020 (USD 66,000,000); 24 September 2020 (USD 61,818,321.78); 21 January 2021 (USD 90,035,800)
International support: none
Public information campaigns: 28 January 2020 through 30 September 2021
COVID testing becomes available: 1 March 2020
Contact tracing begins: 25 February 2020
Emergency healthcare investment: 20 March 2020 (USD 1,076,350,000); 6 June 2020 (USD 565,000,000)
Investment in vaccines: 5 April 2020 (USD 5,427,500); 10 May 2020 (USD 22,000,000)
Mask first recommended: 24 April 2020
Vaccine available to high-risk populations: 28 December 2020
Protection of elderly begins: 11 March 2020
Bolivia
First case: 26 February 2020
Restrictions on in-person learning: 12 March 2020 through 30 September 2021
Restrictions to on-site work: 18 March 2020 to 5 January 2021; 13 July 2021 through 30 September 2021
Public events canceled: 12 March 2020 to 5 January 2021; 13 July 2021 through 30 September 2021
Gatherings restricted: 12 March 2020 to 1 December 2020; 13 July 2021 through 30 September 2021
Public transport closed: 16 March 2020 to 1 December 2020; 13 July 2021 through 30 September 2021
Stay-at-home restrictions: 17 March 2020 to 5 January 2021; 8 June 2021 to 28 September 2021
Internal movement restricted: 21 March 2020 to 5 January 2021; 13 July 2021 to 28 September 2021
International travel restrictions: 13 March 2020
Income support: 31 March 2020 to 21 September 2021
Debt/contract relief: 31 March 2020 to 1 July 2020; 1 January 2021 to 21 September 2021
Fiscal measures: 31 March 2020 (USD 169,813,247); 9 April 2020 (USD 187,000); 14 April 2020 (USD 215,500,000); 15 April 2020 (USD 201,000,000); 3 November 2020 (USD 584,000,000)
International support: none
Public information campaigns: 10 March 2020 through 30 September 2021
COVID testing becomes available: 7 April 2020
Contact tracing begins: 2 June 2020
Emergency healthcare investment: 28 April 2020 (USD 23,000,000); 22 July 2020 (USD 101,387,930); 26 July 2020 (USD 89,914); 5 January 2021 (USD 38,858,400); 30 May 2021 (USD 961,877.46); 4 June 2021 (USD 2,044,298.55); 5 June 2021 (USD 306,541.30)
Investment in vaccines: none
Mask first recommended: 1 May 2020
Vaccine available to high-risk populations: 29 January 2021
Protection of elderly begins: 1 January 2020
Denmark
First case: 13 February 2020
Restrictions on in-person learning: 13 March 2020 to 21 October 2020; 9 November 2020 through 30 September 2021
Restrictions to on-site work: 11 March 2020 through 30 September 2021
Public events canceled: 6 March 2020 to 10 September 2021
Gatherings restricted: 13 March 2020 to 1 September 2021
Public transport closed: 10 March 2020 to 10 October 2020
Stay-at-home restrictions: 3 March 2020 to 21 October 2020; 9 November 2020 to 19 November 2020; 23 November 2020 to 21 May 2021
Internal movement restricted: 13 March 2020 to 22 May 2020; 9 November 2020 to 19 November 2020
International travel restrictions: 3 March 2020
Income support: 9 March 2020 to 7 September 2021
Debt/contract relief: 18 April 2020 to 15 January 2021
Fiscal measures: 13 March 2020 (USD 1,112,519,936); 26 March 2020 (USD 42,066,226,711); 22 April 2020 (USD 2,175,900); 29 May 2020 (USD 3,219,069,854); 28 August 2020 (USD 15,993,841)
International support: 2 April 2020 (USD 94,575,000); 8 April 2020 (USD 1,091,655)
Public information campaigns: 27 February 2020 through 30 September 2021
COVID testing becomes available: 11 March 2020
Contact tracing begins: 27 February 2020
Emergency healthcare investment: 2 April 2020 (USD 94,575,000); 8 April 2020 (USD 1,142,352)
Investment in vaccines: 16 November 2020 (USD 3,000,000)
Mask first recommended: 9 July 2020
Vaccine available to high-risk populations: 27 December 2020
Protection of elderly begins: 17 March 2020
Estonia
First case: 13 February 2020
Restrictions on in-person learning: 16 March 2020 to 26 September 2021
Restrictions to on-site work: 27 March 2020 to 6 July 2021
Public events canceled: 12 March 2020 to 6 July 2021; 26 August 2021 through 30 September 2021
Gatherings restricted: 25 March 2020 through 30 September 2021
Public transport closed: none
Stay-at-home restrictions: 29 March 2020 to 18 May 2020; 11 March 2021 to 9 May 2021
Internal movement restricted: 14 March 2020 to 8 May 2020
International travel restrictions: 12 March 2020
Income support: 1 March 2020 to 1 July 2020; 8 March 2021 to 6 July 2021
Debt/contract relief: 13 March 2020 to 9 May 2021
Fiscal measures: 16 March 2020 (USD 434); 19 March 2020 (USD 2,160,000,000); 24 April 2020 (USD 569,170,000); 28 April 2020 (USD 37,815,296); 6 May 2020 (USD 11,884,807); 14 May 2020 (USD 76,600,000); 21 May 2020 (USD 161,260,000); 17 December 2020 (USD 6,134,750); 23 December 2020 (USD 28,039,300); 7 January 2021 (USD 5,226,713)
International support: 12 April 2020 (USD 111,000); 17 April 2020 (USD 220,000)
Public information campaigns: 12 March 2020 through 30 September 2021
COVID testing becomes available: 12 March 2020
Contact tracing begins: 20 August 2020
Emergency healthcare investment: 16 April 2020 (USD 325,949); 3 November 2020 (USD 1,044,942)
Investment in vaccines: none
Mask first recommended: 8 May 2020
Vaccine available to high-risk populations: 27 December 2020
Protection of elderly begins: 12 March 2020
Finland
First case: 15 January 2020
Restrictions on in-person learning: 18 March 2020 through 30 September 2021
Restrictions to on-site work: 12 March 2020 through 30 September 2021
Public events canceled: 12 March 2020 to 28 September 2021
Gatherings restricted: 12 March 2020 to 14 August 2020; 11 October 2020 to 28 September 2020
Public transport closed: none
Stay-at-home restrictions: 16 March 2020 to 1 June 2020; 7 12 2020 through 30 September 2021
Internal movement restricted: 16 March 2020 to 29 May 2020
International travel restrictions: 6 February 2020
Income support: 16 March 2020 through 30 September 2021
Debt/contract relief: 5 June 2020 through 30 September 2021
Fiscal measures: 19 March 2020 (USD 536,507); 5 June 2020 (USD 346,000,000); 11 June 2020 (USD 95,000,000); 3 September 2020 (USD 70,830,360)
International support: 16 April 2020 (USD 6,011,700); 6 May 2021 (USD 3,615,208)
Public information campaigns: 27 January 2020 through 30 September 2021
COVID testing becomes available: 26 February 2020
Contact tracing begins: 28 February 2020
Emergency healthcare investment: 9 July 2020 (USD 112,986,734.90)
Investment in vaccines: 12 March 2020 (USD 5,543,828)
Mask first recommended: 13 August 2020
Vaccine available to high-risk populations: 27 December 2020
Protection of elderly begins: 16 March 2020
Germany
First case: 13 January 2020
Restrictions on in-person learning: 26 February 2020 through 30 September 2021
Restrictions to on-site work: 22 March 2020 through 30 September 2021
Public events canceled: 29 February 2020 through 30 September 2021
Gatherings restricted: 10 March 2020 through 30 September 2021
Public transport closed: 30 November 2020 through 30 September 2021
Stay-at-home restrictions: 9 March 2020 to 6 May 2020; 15 October 2020 through 30 September 2021
Internal movement restricted: 18 March 2020 to 4 September 2020; 15 October 2020 to 3 August 2021
International travel restrictions: 28 February 2020
Income support: 16 March 2020 through 30 September 2021
Debt/contract relief: 1 April 2020 to 1 July 2020
Fiscal measures: 23 March 2020 (USD 68,442,949,673); 17 June 2020 (USD 28,000,000,000); 2 November 2020 (USD 11,791,900,000)
International support: 4 May 2020 (USD 2,023,000,000); 17 June 2020 (USD 1,740,000,000); 17 December 2020 (USD 342,890)
Public information campaigns: 24 January 2020 through 30 September 2021
COVID testing becomes available: 27 January 2020
Contact tracing begins: 22 January 2020
Emergency healthcare investment: 23 March 2020 (USD 62,997,723,800); 27 March 2020 (USD 3,100,000,000); 29 April 2020 (USD 54,269,511)
Investment in vaccines: 6 February 2020 (USD 8,010,337); 23 March 2020 (USD 156,510,825); 4 May 2020 (USD 545,000,000); 11 May 2020 (USD 812,000,000); 17 June 2020 (USD 340,000,000)
Mask first recommended: 1 April 2020
Vaccine available to high-risk populations: 27 December 2020
Protection of elderly begins: 28 February 2020
Iceland
First case: 14 February 2020
Restrictions on in-person learning: 16 March 2020 through 30 September 2021
Restrictions to on-site work: 16 March 2020 to 25 May 2020; 31 July 2020 to 26 June 2021; 25 July 2021 through 30 September 2021
Public events canceled: 16 March 2020 to 26 June 2021; 25 July 2021 through 30 September 2021
Gatherings restricted: 15 March 2020 to 26 June 2021; 25 July 2021 through 30 September 2021
Public transport closed: 25 March 2021 to 10 May 2021
Stay-at-home restrictions: none
Internal movement restricted: none
International travel restrictions: 29 January 2020
Income support: 21 March 2020 through 30 September 2021
Debt/contract relief: 10 March 2020 through 30 September 2021
Fiscal measures: 21 March 2020 (USD 1,600,000,000); 21 April 2020 (USD 2,884,140); 27 May 2020 (USD 580,000,000)
International support: none
Public information campaigns: 23 January 2020 through 30 September 2021
COVID testing becomes available: 9 March 2020
Contact tracing begins: 9 March 2020
Emergency healthcare investment: none
Investment in vaccines: none
Mask first recommended: 31 July 2020
Vaccine available to high-risk populations: 29 December 2020
Protection of elderly begins: 6 March 2020
Lithuania
First case: 5 March 2020
Restrictions on in-person learning: 13 March 2020 to 24 August 2021
Restrictions to on-site work: 16 March 2020 to 17 June 2020; 7 August 2020 to 30 August 2021; 29 September 2021 through 30 September 2021
Public events canceled: 12 March 2020 to 1 July 2020; 9 October 2020 through 30 September 2021
Gatherings restricted: 12 March 2020 to 1 July 2021; 24 August 2021 through 30 September 2021
Public transport closed: 16 March 2020 to 7 August 2020; 9 October 2020 to 7 November 2020; 23 May 2021 to 27 May 2021
Stay-at-home restrictions: 16 March 2020 to 17 June 2020; 7 August 2020 to 19 April 2021
Internal movement restricted: 16 March 2020 to 17 June 2020; 28 October 2020 to 13 April 2021; 23 May 2021 to 27 May 2021
International travel restrictions: 13 March 2020
Income support: 7 April 2020 through 30 September 2021
Debt/contract relief: 17 March 2020 through 30 September 2021
Fiscal measures: 16 March 2020 (USD 2,244,535,000); 10 June 2020 (USD 2,476,881,000); 3 September 2020 (USD 22,712,991); 16 October 2020 (USD 14,052,000); 16 November 2020 (USD 5,900,000); 18 November 2020 (USD 118,600,000); 18 December 2020 (USD 164,700,000); 22 December 2020 (USD 109,530,000); 23 December 2020 (USD 219,420,000); 12 April 2021 (USD 142,820,000);
International support: 25 February 2020 (USD 92,008); 9 April 2020 (USD 91,481); 20 May 2020 (USD 91,082); 3 June 2020 (USD 56,682.50)
Public information campaigns: 26 February 2020 through 30 September 2021
COVID testing becomes available: 29 January 2020
Contact tracing begins: 7 April 2020
Emergency healthcare investment: 16 March 2020 (USD 550,832,500)
Investment in vaccines: 19 August 2020 (USD 1,784,956); 16 September 2020 (USD 2,947,137.50)
Mask first recommended: 7 August 2020
Vaccine available to high-risk populations: 27 December 2020
Protection of elderly begins: 12 March 2020
New Zealand
First case: 14 February 2020
Restrictions on in-person learning: 21 March 2020 to 8 June 2020; 12 August 2020 to 7 October 2020; 15 February 2021 to 18 February 2021; 28 February 2021 to 7 March 2021; 17 August 2021 through 30 September 2021
Restrictions to on-site work: 21 March 2020 to 14 May 2020; 12 August 2020 to 7 October 2020; 15 February 2021 to 23 February 2021; 28 February 2021 to 12 March 2021; 17 August 2021 through 30 September 2021
Public events canceled: 16 March 2020 to 8 June 2020; 12 August 2020 to 7 October 2020; 15 February 2021 to 23 February 2021; 28 February 2021 to 12 March 2021; 17 August 2021 through 30 September 2021
Gatherings restricted: 16 March 2020 to 8 June 2020; 12 August 2020 to 7 October 2020; 15 February 2021 to 23 February 2021; 28 February 2021 to 12 March 2021; 17 August 2021 through 30 September 2021
Public transport closed: 23 March 2020 to 14 May 2020; 17 August 2021 through 30 September 2021
Stay-at-home restrictions: 21 March 2020 to 14 May 2020; 12 August 2020 to 31 August 2020; 17 August 2021 through 30 September 2021
Internal movement restricted: 21 March 2020 to 14 May 2020; 12 August 2020 to 31 August 2020; 15 February 2021 to 18 February 2021; 28 February 2021 to 7 March 2021; 17 August 2021 through 30 September 2021
International travel restrictions: 2 February 2020
Income support: 17 March 2020 through 30 September 2021
Debt/contract relief: 24 March 2020 through 30 September 2021
Fiscal measures: 17 March 2020 (USD 11,500,000,000); 22 January 2021 (USD 2,147,618.72)
International support: none
Public information campaigns: 22 January 2020 through 30 September 2021
COVID testing becomes available: 28 February 2020
Contact tracing begins: 28 February 2020
Emergency healthcare investment: 17 March 2020 (USD 297,228,142)
Investment in vaccines: 27 May 2020 (USD 23,870,000)
Mask first recommended: 12 August 2020
Vaccine available to high-risk populations: 19 February 2021
Protection of elderly begins: 25 March 2020
Norway
First case: 12 February 2020
Restrictions on in-person learning: 12 March 2020 through 30 September 2021
Restrictions to on-site work: 10 March 2020 to 25 September 2021
Public events canceled: 24 March 2020 to 2 June 2020; 26 October 2020 to 25 September 2021
Gatherings restricted: 11 March 2020 to 13 August 2021
Public transport closed: 9 March 2020 to 14 May 2020; 16 January 2021 to 25 September 2021
Stay-at-home restrictions: 5 November 2020 to 25 September 2021
Internal movement restricted: 16 March 2020 to 21 September 2020; 5 November 2020 to 27 May 2021
International travel restrictions: 14 March 2020
Income support: 20 March 2020 through 30 September 2021
Debt/contract relief: none
Fiscal measures: 16 March 2020 (USD 9,729,500,000); 18 March 2020 (USD 81,041,400); 20 March 2020 (USD 8,666,000,000); 30 March 2020 (USD 664,363); 3 April 2020 (USD 241,066,800); 7 April 2020 (USD 14,641,200); 9 April 2020 (USD 1,952,160); 14 April 2020 (USD 58,224,000); 19 April 2020 (USD 145,414,500); 20 April 2020 (USD 593,278,200); 21 April 2020 (USD 9,428,100); 22 April 2020 (USD 18,525,800); 29 May 2020 (USD 1,613,290,761)
International support: 26 March 2020 (USD 1,438,898.70); 23 December 2020 (USD 232,000,000)
Public information campaigns: 31 January 2020 through 30 September 2021
COVID testing becomes available: 26 February 2020
Contact tracing begins: 1 April 2020
Emergency healthcare investment: 14 February 2020 (USD 1,080,950); 31 March 2020 (USD 14,115,450); 2 April 2020 (USD 9,638,900); 11 April 2020 (USD 2,943,480)
Investment in vaccines: 14 February 2020 (USD 3,891,420); 27 March 2020 (USD 190,372,000); 20 October 2020 (USD 500,000,000)
Mask first recommended: 14 August 2020
Vaccine available to high-risk populations: 18 December 2020
Protection of elderly begins: 3 December 2020
Serbia
First case: 21 February 2020
Restrictions on in-person learning: 16 March 2020 through 30 September 2021
Restrictions to on-site work: 16 March 2020 to 6 June 2020; 1 July 2020 to 1 June 2021; 7 June 2021 through 30 September 2021
Public events canceled: 15 March 2020 through 30 September 2021
Gatherings restricted: 11 March 2020 to 6 June 2020; 17 July 2020 through 30 September 2021
Public transport closed: 21 March 2020 to 17 May 2020; 26 April 2021 to 24 May 2021; 22 September 2021 through 30 September 2021
Stay-at-home restrictions: 15 March 202 to 7 June 2021; 12 July 2021 through 30 September 2021
Internal movement restricted: 18 March 2020 to 17 May 2020; 10 July 2020 to 8 March 2021; 22 September 2021 through 30 September 2021
International travel restrictions: 22 January 2020
Income support: 31 March 2020 through 30 September 2021
Debt/contract relief: 31 March 2020 through 30 September 2021
Fiscal measures: none
International support: none
Public information campaigns: 25 February 2020 through 30 September 2021
COVID testing becomes available: 27 February 2020
Contact tracing begins: 6 March 2020
Emergency healthcare investment: 31 March 2020 (USD 16,518,385); 11 May 2020 (USD 109,000,000); 5 December 2020 (USD 96,921,120)
Investment in vaccines: none
Mask first recommended: 1 July 2020
Vaccine available to high-risk populations: 30 December 2020
Protection of elderly begins: 15 March 2020
Taiwan
First case: 10 January 2020
Restrictions on in-person learning: 2 February 2020 to 1 December 2020; 16 May 2021 to 1 September 2021
Restrictions to on-site work: 15 May 2021 through 30 September 2021
Public events canceled: 5 March 2020 to 8 May 2020; 21 January 2021 through 30 September 2021
Gatherings restricted: 15 May 2021 through 30 September 2021
Public transport closed: 7 September 2021 to 28 September 2021
Stay-at-home restrictions: 19 May 2021 to 27 July 2021
Internal movement restricted: 15 May 2021 through 30 September 2021
International travel restrictions: 1 January 2020
Income support: 21 April 2020 through 30 September 2021
Debt/contract relief: 10 March 2020 to 1 June 2021
Fiscal measures: 25 February 2020 (USD 1,417,589,723); 2 April 2020 (USD 32,761,907,413); 31 May 2021 (USD 15,200,000,000)
International support: none
Public information campaigns: 2 January 2020 through 30 September 2021
COVID testing becomes available: 20 January 2020
Contact tracing begins: 21 January 2020
Emergency healthcare investment: 27 February 2020 (USD 560,790,000); 7 June 2021 (USD 142,796,240)
Investment in vaccines: 27 February 2020 (USD 1,733,514)
Mask first recommended: 24 January 2020
Vaccine available to high-risk populations: 22 March 2021
Protection of elderly begins: 4 May 2020







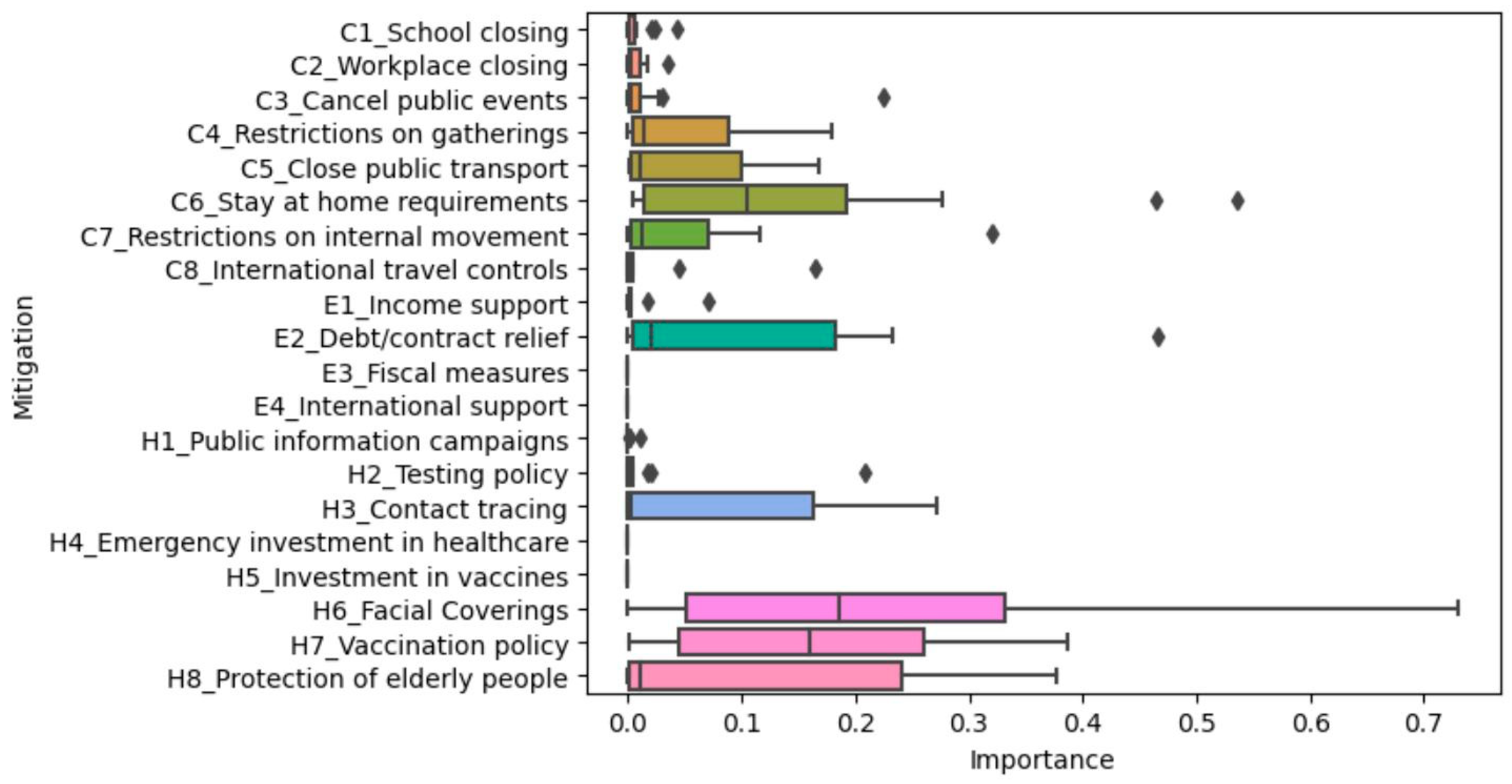
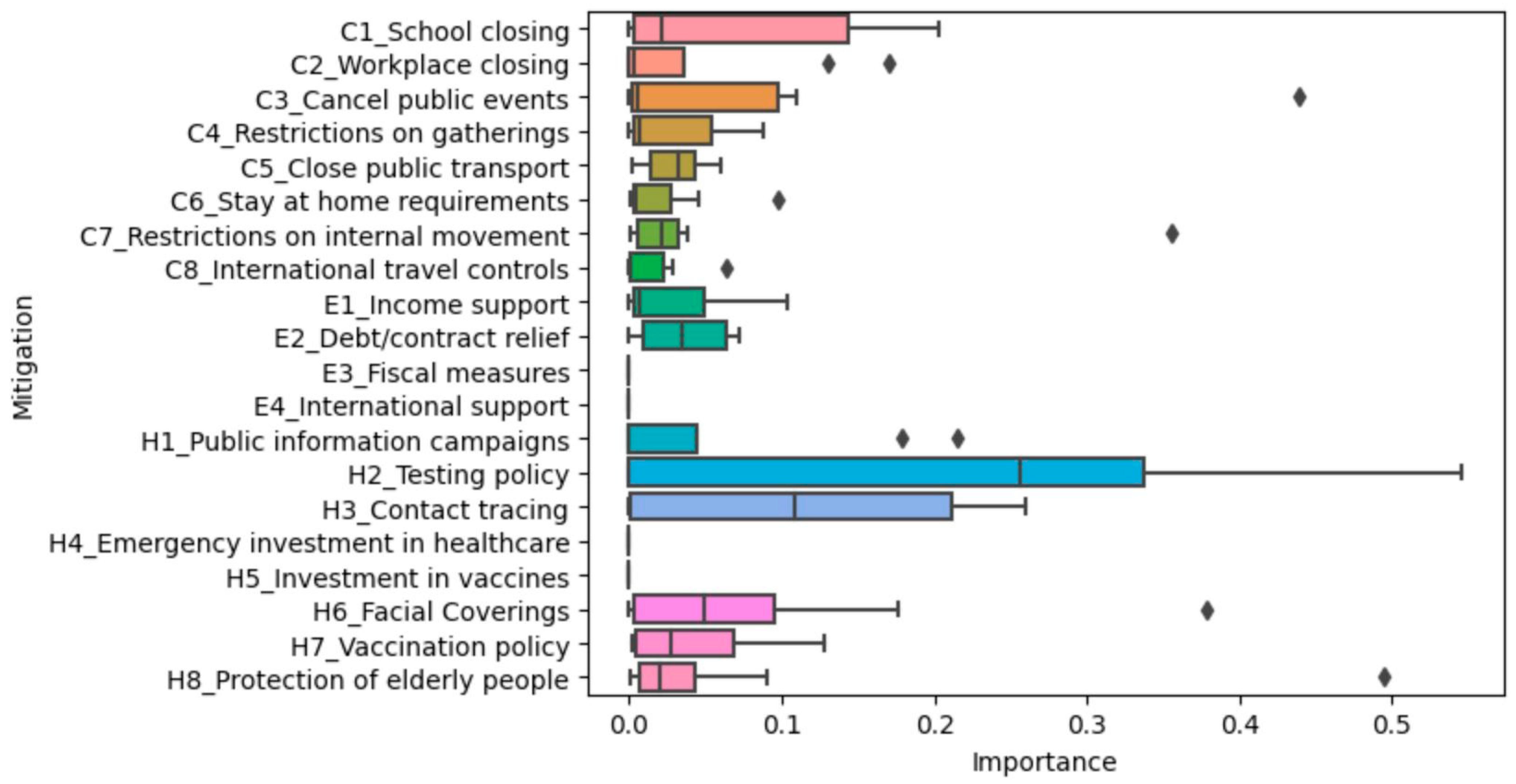
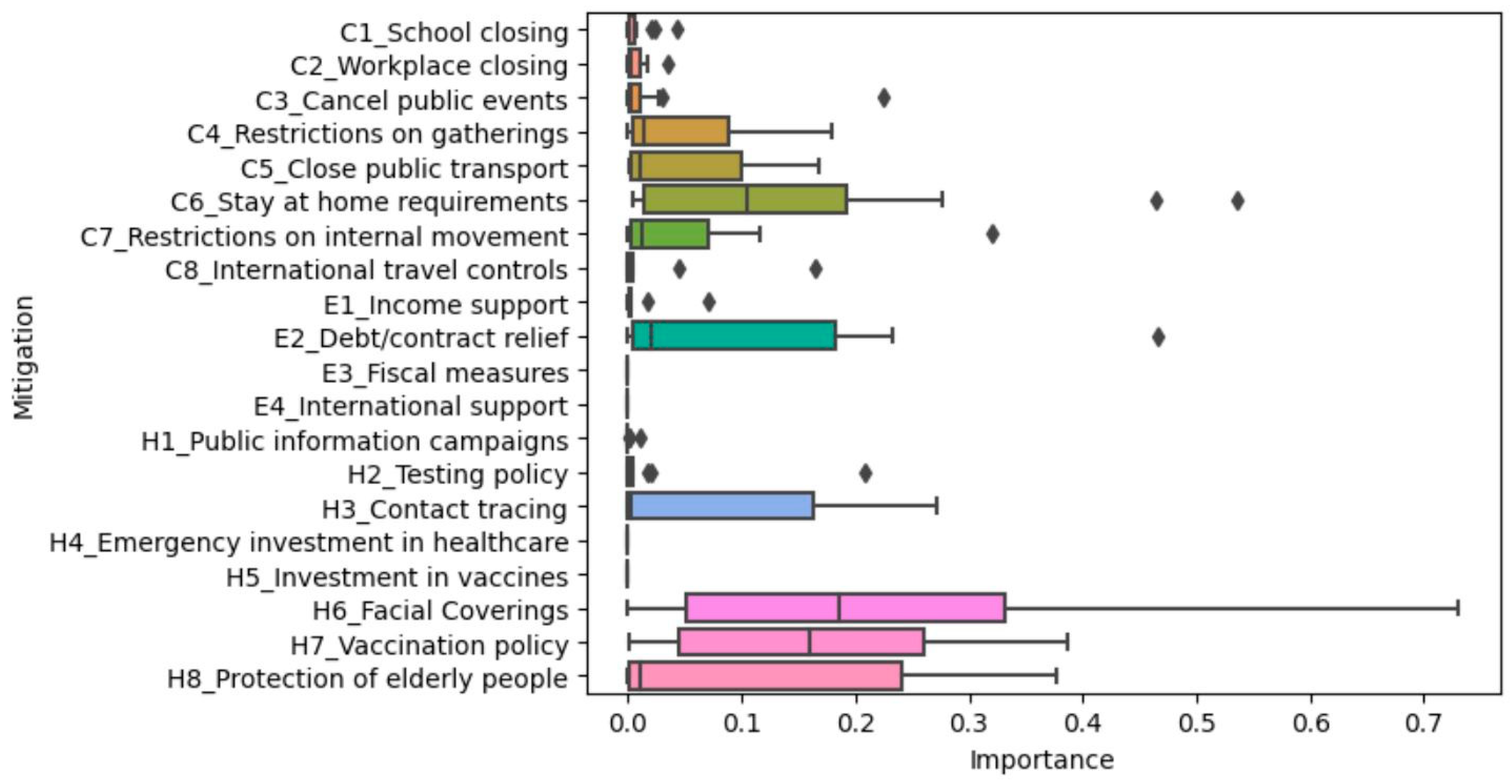
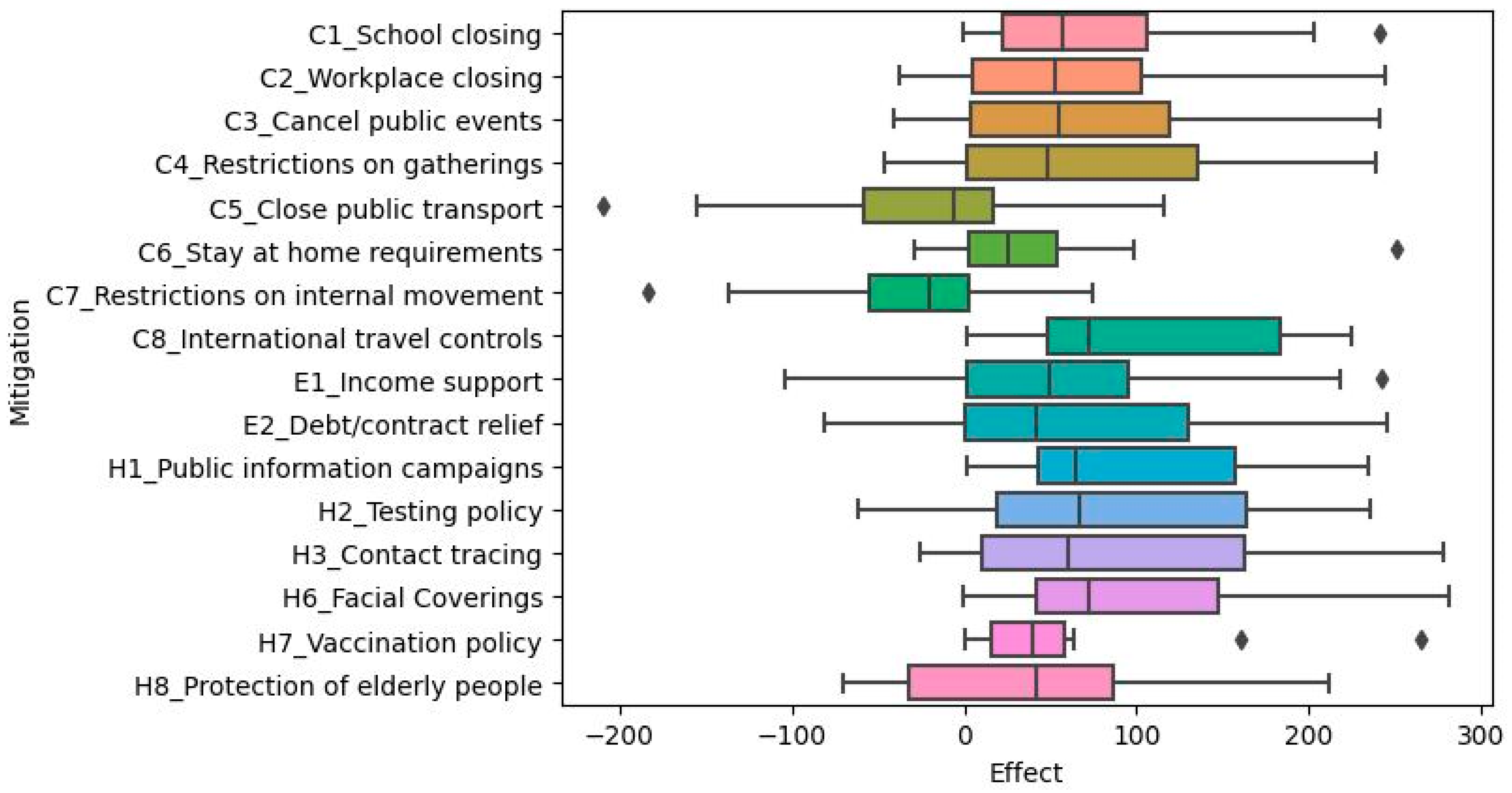
 represents outliers.
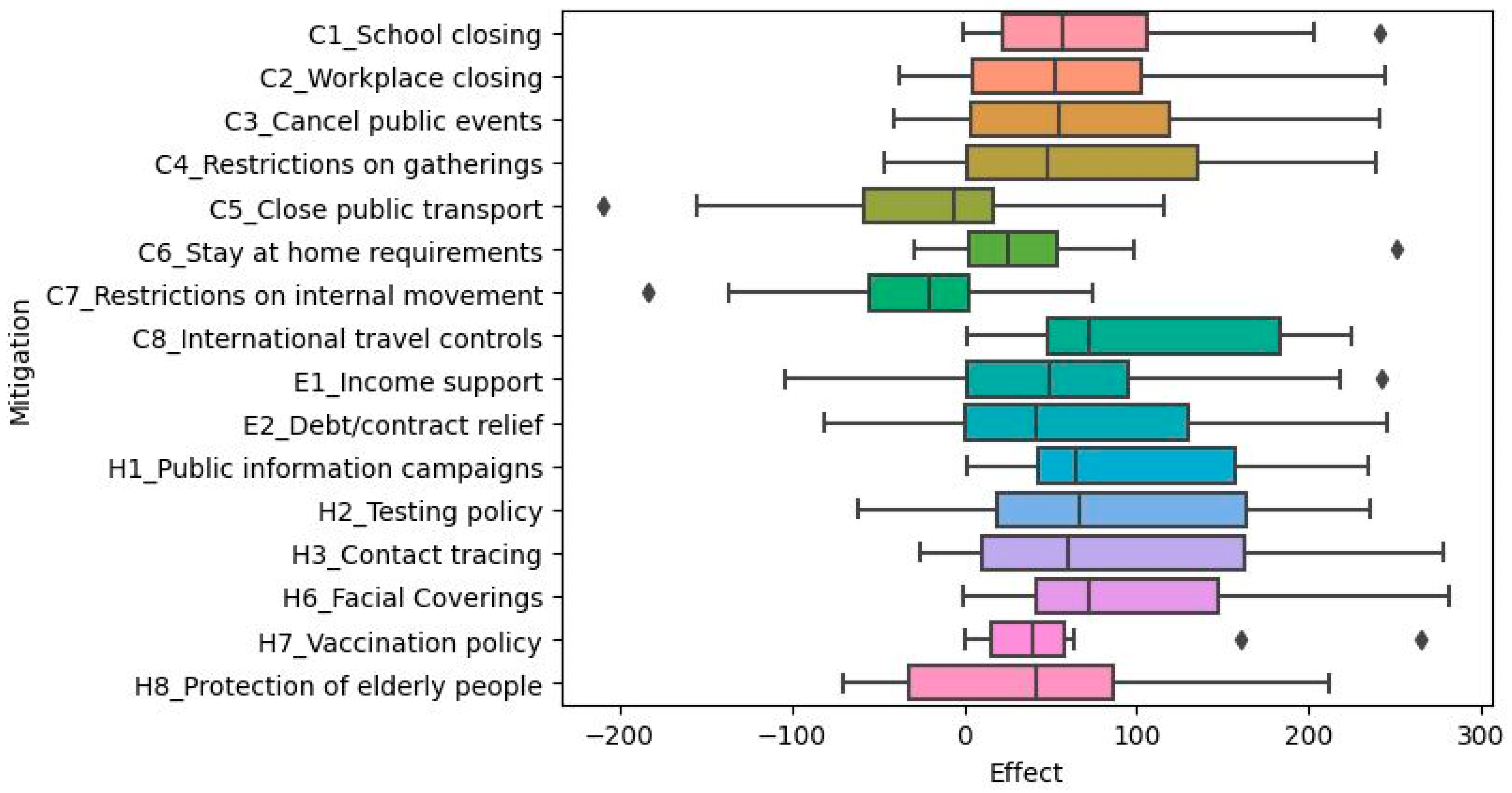
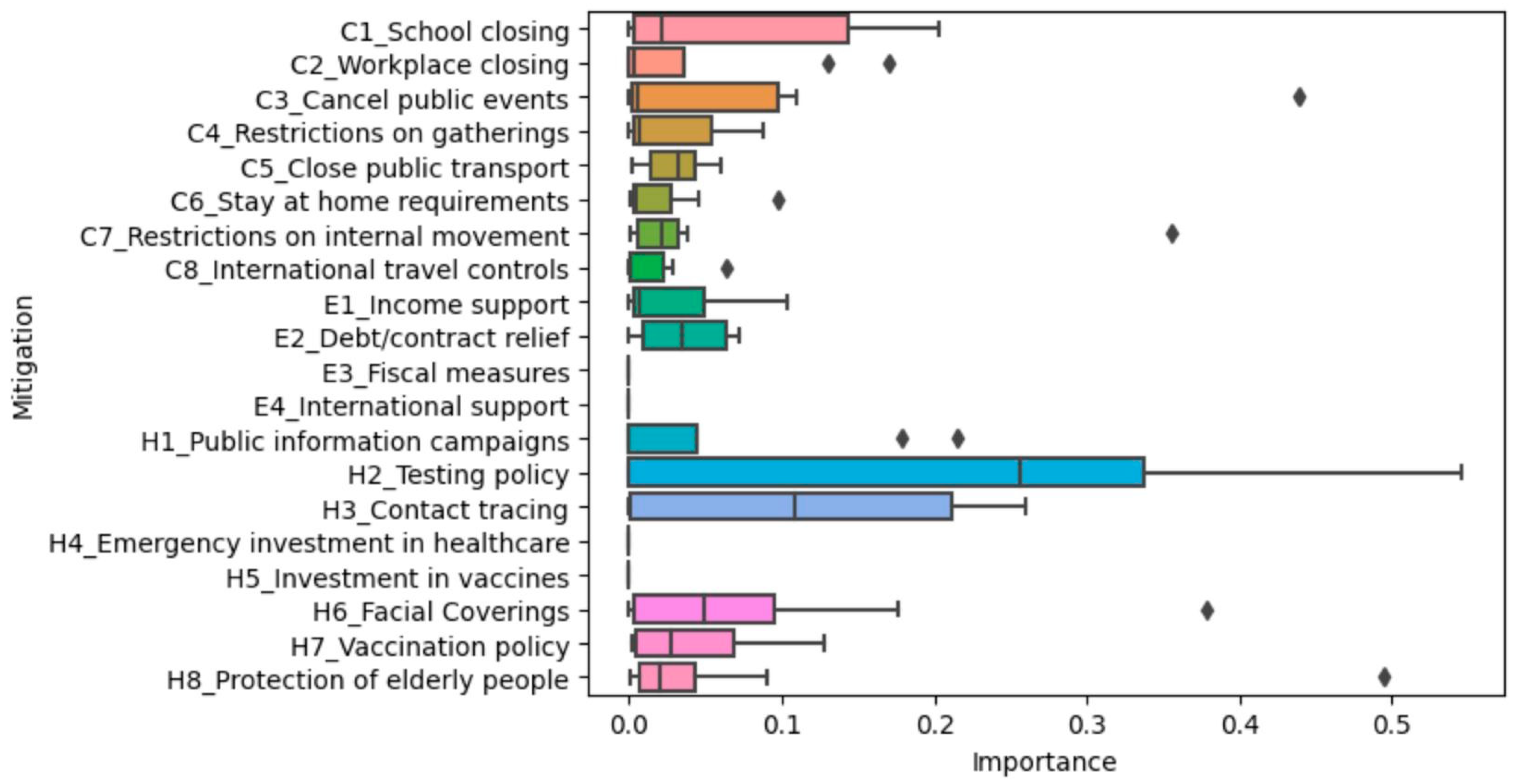
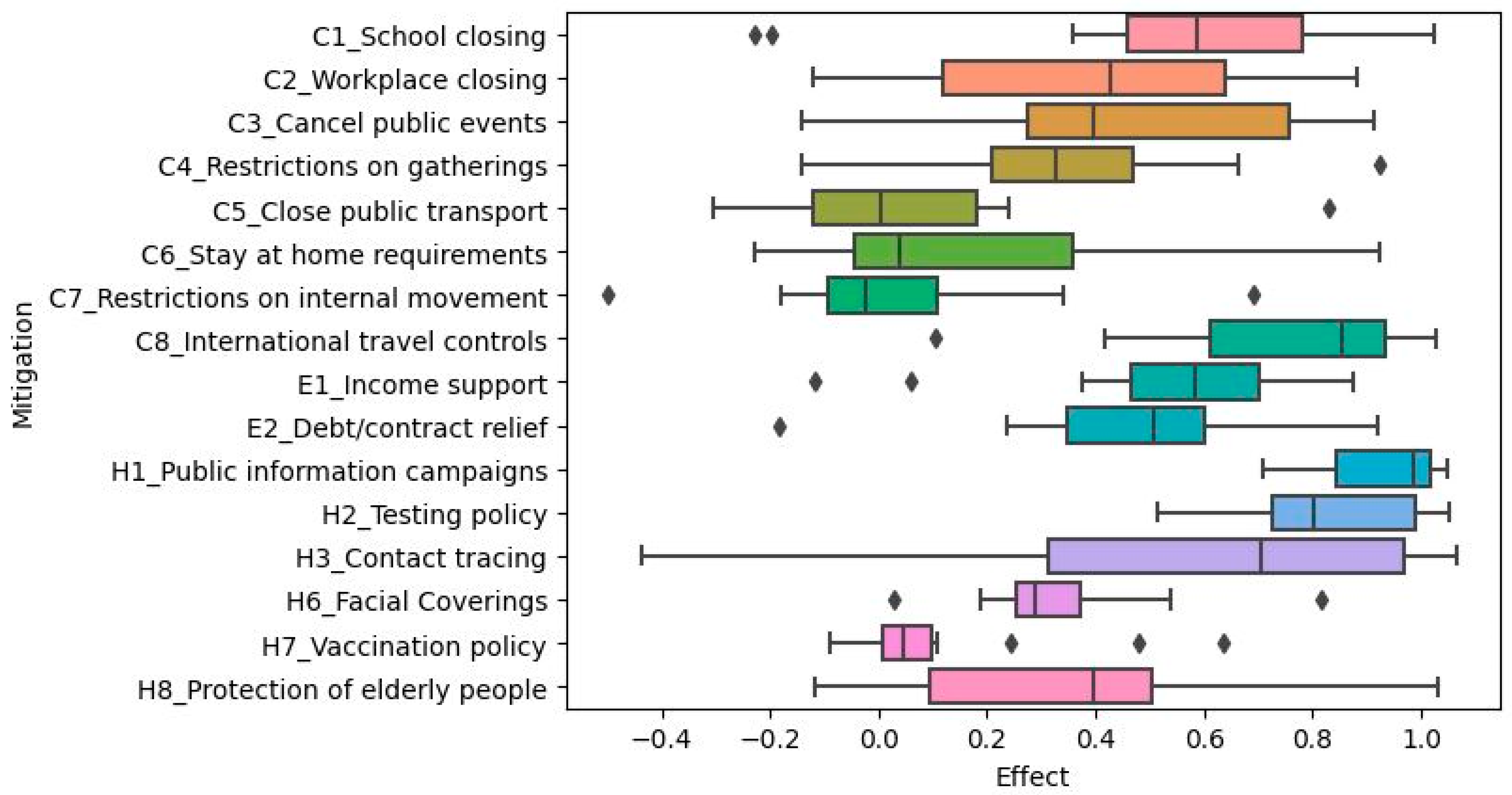
represents outliers.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}