
Health Literacy among Older Adults in Portugal and Associated Sociodemographic, Health and Healthcare-Related Factors

 ,
,  ,
,  ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling
2.2. Data Collection
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Sample Characterisation
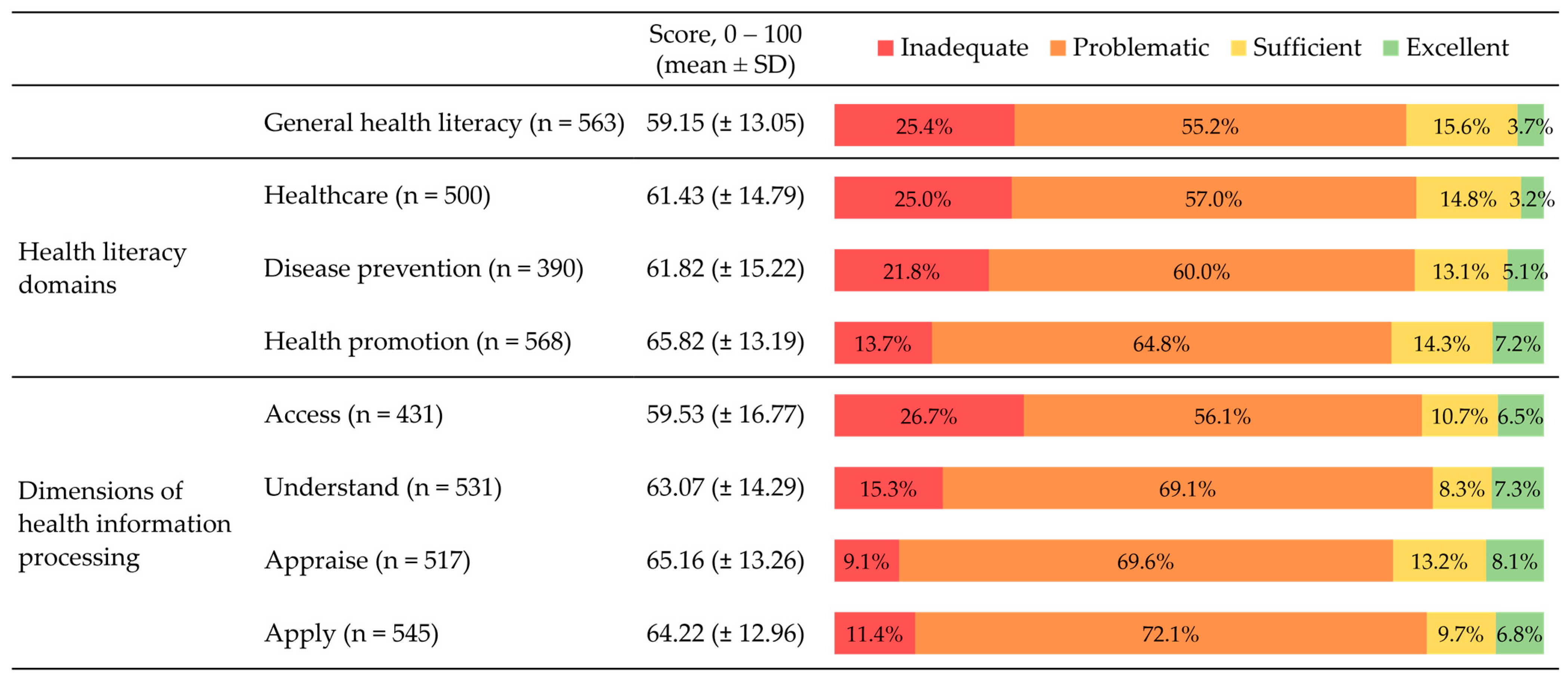
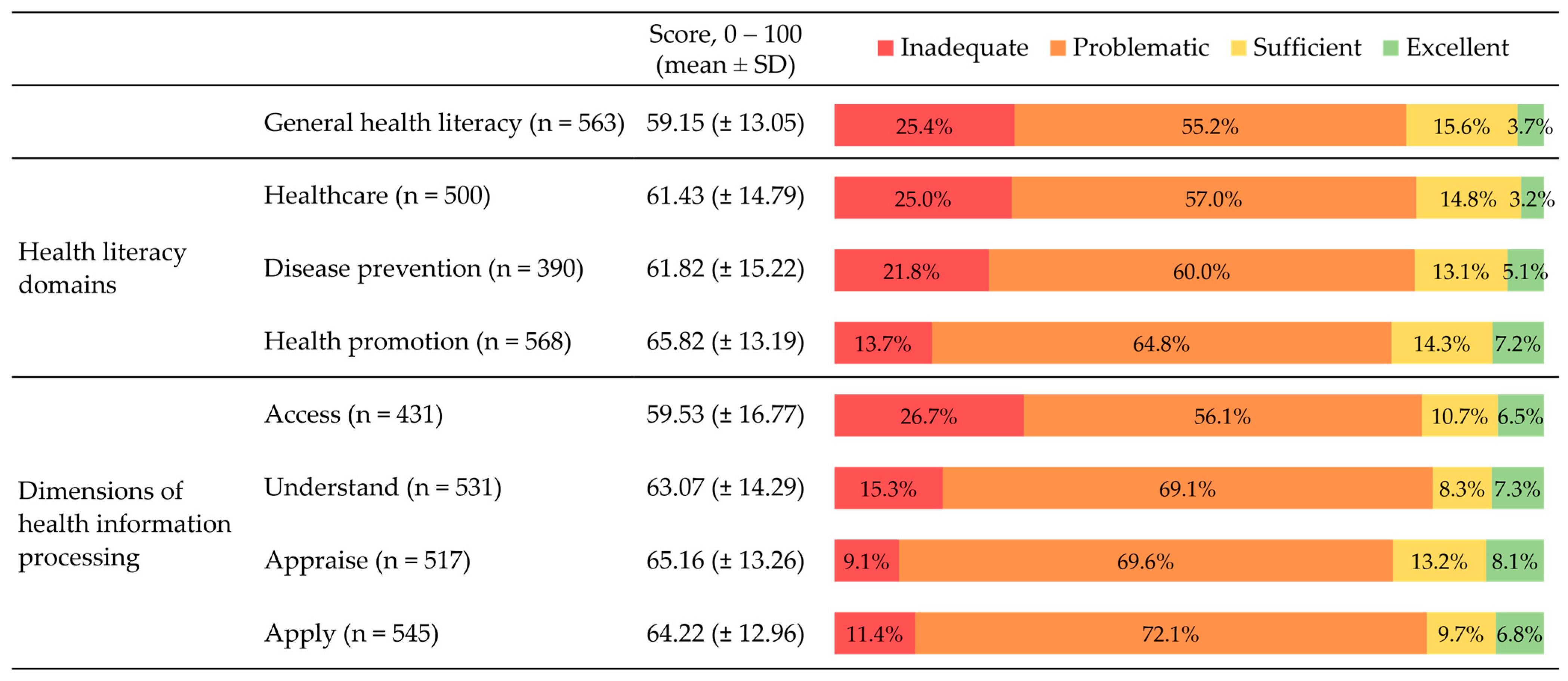
3.2. Health Literacy Measures
3.3. Limited Health Literacy Distribution within Sample Subgroups
3.4. Determinants of Limited Health Literacy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eurostat. Ageing Europe—Looking at the Lives of Older People in the EU, 2020 ed.; Products Statistical Books–Eurostat. Ageing Europe–Looking at the Lives of Older People in the EU, 1–184. Available online: https://ec.europa.eu/eurostat/en/web/products-statistical-books/-/ks-02-20-655 (accessed on 30 December 2022).
- Kassebaum, N.J. Global, regional, and national burden of diseases and injuries for adults 70 years and older: Systematic analysis for the Global Burden of Disease 2019 Study. BMJ 2022, 376, e068208. [Google Scholar] [CrossRef]
- Costa, A.; Câmara, G.; de Arriaga, M.T.; Nogueira, P.; Miguel, J.P. Active and Healthy Aging After COVID-19 Pandemic in Portugal and Other European Countries: Time to Rethink Strategies and Foster Action. Front. Public Health 2021, 9, 886. [Google Scholar] [CrossRef] [PubMed]
- Kehler, D.S. Age-related disease burden as a measure of population ageing. Lancet Public Health 2019, 4, e123–e124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, A.Y.; Skirbekk, V.F.; Tyrovolas, S.; Kassebaum, N.J.; Dieleman, J.L. Measuring population ageing: An analysis of the Global Burden of Disease Study 2017. Lancet Public Health 2019, 4, e159–e167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.-P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [Green Version]
- Abud, T.; Kounidas, G.; Martin, K.R.; Werth, M.; Cooper, K.; Myint, P.K. Determinants of healthy ageing: A systematic review of contemporary literature. Aging Clin. Exp. Res. 2022, 34, 1215–1223. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; (HLS-EU) Consortium Health Literacy Project European. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-J.; Son, Y.-J. Associated Factors and Health Outcomes of Health Literacy and Physical Frailty Among Older Adults: A Systematic Review. Res. Gerontol. Nurs. 2022, 15, 39–52. [Google Scholar] [CrossRef]
- Smith, G.D.; Ho, K.H.M.; Poon, S.; Chan, S.W. Beyond the tip of the iceberg: Health literacy in older people. J. Clin. Nurs. 2021, 31, E3–E5. [Google Scholar] [CrossRef]
- Costa, A.S.; Arriaga, M.; Mendes, R.V.; Miranda, D.; Barbosa, P.; Sakellarides, C.; Peralta, A.; Lopes, N.A.; Roque, C.; Ribeiro, S. A Strategy for the Promotion of Health Literacy in Portugal, Centered around the Life-Course Approach: The Importance of Digital Tools. Port. J. Public Health 2019, 37, 50–54. [Google Scholar] [CrossRef]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The HLS19 Consortium of the WHO Action Network M-POHL. International Report on the Methodology, Results, and Recommendations of the European Health Literacy Population Survey 2019-2021 (HLS19) of M-POHL. Vienna. 2021. Available online: https://m-pohl.net/Results (accessed on 30 December 2022).
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Zamora, H.; Clingerman, E.M. Health Literacy Among Older Adults: A Systematic Literature Review. J. Gerontol. Nurs. 2011, 37, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Chesser, A.K.; Woods, N.K.; Smothers, K.; Rogers, N. Health Literacy and Older Adults: A Systematic Review. Gerontol. Geriatr. Med. 2016, 2, 2333721416630492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Do, B.N.; Nguyen, P.-A.; Pham, K.M.; Nguyen, H.C.; Nguyen, M.H.; Tran, C.Q.; Nguyen, T.T.P.; Tran, T.V.; Pham, L.V.; Tran, K.V.; et al. Determinants of Health Literacy and Its Associations With Health-Related Behaviors, Depression Among the Older People With and Without Suspected COVID-19 Symptoms: A Multi-Institutional Study. Front. Public Health 2020, 8, 581746. [Google Scholar] [CrossRef]
- Van Hoa, H.; Giang, H.T.; Vu, P.T.; Van Tuyen, D.; Khue, P.M. Factors Associated with Health Literacy among the Elderly People in Vietnam. BioMed Res. Int. 2020, 2020, 3490635. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.-B.; Liu, L.; Li, Y.-F.; Chen, Y.-L. Relationship between Health Literacy, Health-Related Behaviors and Health Status: A Survey of Elderly Chinese. Int. J. Environ. Res. Public Health 2015, 12, 9714–9725. [Google Scholar] [CrossRef] [Green Version]
- Arriaga, M.; Francisco, R.; Nogueira, P.; Oliveira, J.; Silva, C.; Câmara, G.; Sørensen, K.; Dietscher, C.; Costa, A. Health Literacy in Portugal: Results of the Health Literacy Population Survey Project 2019–2021. Int. J. Environ. Res. Public Health 2022, 19, 4225. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Dean, A.; Sullivan, K.; Soe, M. OpenEpi: Open Source Epidemiologic Statistics for Public Health, Versão 3.01. Available online: https://www.openepi.com (accessed on 14 February 2023).
- Pelikan, J.M.; Link, T.; Straßmayr, C.; Waldherr, K.; Alfers, T.; Bøggild, H.; Griebler, R.; Lopatina, M.; Mikšová, D.; Nielsen, M.G.; et al. Measuring Comprehensive, General Health Literacy in the General Adult Population: The Development and Validation of the HLS19-Q12 Instrument in Seventeen Countries. Int. J. Environ. Res. Public Health 2022, 19, 14129. [Google Scholar] [CrossRef]
- Pelikan, J.M.; Ganahl, K.; Roethlin, F. Health literacy as a determinant, mediator and/or moderator of health: Empirical models using the European Health Literacy Survey dataset. Glob. Health Promot. 2018, 25, 57–66. [Google Scholar] [CrossRef]
- Gibney, S.; Bruton, L.; Ryan, C.; Doyle, G.; Rowlands, G. Increasing Health Literacy May Reduce Health Inequalities: Evidence from a National Population Survey in Ireland. Int. J. Environ. Res. Public Health 2020, 17, 5891. [Google Scholar] [CrossRef]
- Espanha, R.; Ávila, P.; Mendes, R.V.; CIES/IUL Centro de Investigação e Estudos de Sociologia. Literacia em Saúde em Portugal. Relatório Síntese. Lisboa. Available online: https://cdn.gulbenkian.pt/wp-content/uploads/2021/05/87Est_Lieracia_Saude.pdf (accessed on 30 January 2023).
- Meier, C.; Vilpert, S.; Borrat-Besson, C.; Jox, R.J.; Maurer, J. Health literacy among older adults in Switzerland: Cross-sectional evidence from a nationally representative population-based observational study. Swiss Med Wkly. 2022, 152, w30158. [Google Scholar] [CrossRef]
- Gustafsdottir, S.S.; Sigurdardottir, A.K.; Mårtensson, L.; Arnadottir, S.A. Making Europe health literate: Including older adults in sparsely populated Arctic areas. BMC Public Health 2022, 22, 511. [Google Scholar] [CrossRef]
- Bozkurt, H.; Demirci, H. Health literacy among older persons in Turkey. Aging Male 2018, 22, 272–277. [Google Scholar] [CrossRef]
- Lopatina, M.; Popovich, M.; Kontsevaya, A.; Drapkina, O. Determinants of health literacy: The results of the first population survey in the Russian Federation. Profil. Meditsina 2021, 24, 57–64. [Google Scholar] [CrossRef]
- Garcia-Codina, O.; Juvinyà-Canal, D.; Amil-Bujan, P.; Bertran-Noguer, C.; González-Mestre, M.A.; Masachs-Fatjo, E.; Santaeugènia, S.J.; Magrinyà-Rull, P.; Saltó-Cerezuela, E. Determinants of health literacy in the general population: Results of the Catalan health survey. BMC Public Health 2019, 19, 1122. [Google Scholar] [CrossRef] [Green Version]
- Schaeffer, D.; Berens, E.-M.; Vogt, D.; Gille, S.; Griese, L.; Klinger, J.; Hurrelmann, K. Health Literacy in Germany—Findings of a Representative Follow-up Survey. Dtsch. Arztebl. Int. 2021, 118, 723–729. [Google Scholar] [CrossRef]
- Von Wagner, C.; Knight, K.; Steptoe, A.; Wardle, J. Functional health literacy and health-promoting behaviour in a national sample of British adults. J. Epidemiol. Community Health 2007, 61, 1086–1090. [Google Scholar] [CrossRef]
- Coughlin, S.S.; Vernon, M.; Hatzigeorgiou, C.; George, V. Health Literacy, Social Determinants of Health, and Disease Prevention and Control. J. Environ. Health Sci. 2020, 6, 3061. [Google Scholar]
- Laine, J.E.; Baltar, V.T.; Stringhini, S.; Gandini, M.; Chadeau-Hyam, M.; Kivimaki, M.; Severi, G.; Perduca, V.; Hodge, A.M.; Dugué, P.A.; et al. Reducing socioeconomic inequalities in all-cause mortality: A counterfactual mediation approach. Int. J. Epidemiol. 2020, 49, 497. [Google Scholar] [CrossRef] [PubMed]
- Cockerham, W.C.; Hamby, B.W.; Oates, G.R. The Social Determinants of Chronic Disease. Am. J. Prev. Med. 2017, 52, S5–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minkler, M.; Fuller-Thomson, E.; Guralnik, J.M. Gradient of Disability across the Socioeconomic Spectrum in the United States. N. Engl. J. Med. 2006, 355, 695–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Public Health England. Local Action on Health Inequalities: Improving Health Literacy to Reduce Health Inequalities; Public Health England: London, UK, 2015; Available online: https://www.instituteofhealthequity.org/resources-reports/local-action-on-health-inequalities-health-literacy-to-reduce-health-inequalities/health-literacy-improving-health-literacy-to-reduce-health-inequalities-full.pdf (accessed on 20 January 2023).
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2013; Volume 398. [Google Scholar]
- Geboers, B.; Reijneveld, S.A.; Jansen, C.J.; de Winter, A.F. Health Literacy Is Associated With Health Behaviors and Social Factors Among Older Adults: Results from the LifeLines Cohort Study. J. Health Commun. 2016, 21 (Suppl. 2), 45–53. [Google Scholar] [CrossRef] [Green Version]
- Goldman, D.P.; Smith, J.P. Can patient self-management help explain the SES health gradient? Proc. Natl. Acad. Sci. USA 2002, 99, 10929–10934. [Google Scholar] [CrossRef] [Green Version]
- Maitra, S. Can patient self-management explain the health gradient? Goldman and Smith’s “Can patient self-management help explain the SES health gradient?” (2002) revisited. Soc. Sci. Med. 2010, 70, 802–812. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Health Literacy: The Solid Facts; WHO Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Paiva, D.; Silva, S.; Severo, M.; Moura-Ferreira, P.; Lunet, N.; Azevedo, A. Limited Health Literacy in Portugal Assessed with the Newest Vital Sign. Acta Med. Port. 2017, 30, 861–869. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Estatística. Censos 2021. XVI Recenseamento Geral da População. VI Recenseamento Geral da Habitação: Resultados definitivos. Lisboa. Available online: https://www.ine.pt/xurl/pub/65586079 (accessed on 20 January 2023).

{kind=link}
| Sociodemographic Characteristics | |
|---|---|
| Age (mean ± SD 1) | 72.84 ± 5.79 |
| Age groups | n (%) |
| 65–74 years | 405 (66.1%) |
| 75+ years | 208 (33.9%) |
| Gender | |
| Male | 320 (52.2%) |
| Female | 293 (47.8%) |
| Household living arrangement | |
| Living alone | 182 (29.7%) |
| Living with others | 431 (70.3%) |
| Country of birth | |
| Portugal | 578 (94.3%) |
| Other country | 35 (5.7%) |
| Place of residence (based on nomenclature of territorial units for statistics, level II region) | |
| North | 164 (26.8%) |
| Centre | 134 (21.9%) |
| Lisbon Metropolitan Area | 246 (40.1%) |
| Alentejo | 37 (6.0%) |
| Algarve | 32 (5.2%) |
| Employment status | |
| Working professionally | 38 (6.2%) |
| Not working professionally | 574 (93.6%) |
| Do not know/Did not answer | 1 (0.2%) |
| Educational level | |
| Up to 2nd cycle of primary education | 210 (34.3%) |
| 3rd cycle of primary education | 83 (13.5%) |
| High school | 131 (21.4%) |
| University education | 189 (30.8%) |
| Perceived household financial situation | |
| Comfortable or very comfortable | 173 (28.2%) |
| Enough for needs | 255 (41.6%) |
| Difficult or very difficult | 180 (29.4%) |
| Do not know/Did not answer | 5 (0.8%) |
| Health status and healthcare-related variables | |
| Self-perceived health status | |
| Good or very good | 194 (31.6%) |
| Fair | 305 (49.8%) |
| Bad or very bad | 114 (18.6%) |
| Self-reported chronic disease or disability | |
| Yes | 287 (46.8%) |
| No | 326 (53.2%) |
| Registered in a primary healthcare centre | |
| Yes | 584 (95.3%) |
| No | 29 (4.7%) |
| Primary healthcare medical consultation within the previous six months, at least once (n = 584) | |
| No | 186 (31.8%) |
| Yes | 398 (68.2%) |
| Primary healthcare evaluation, previous six months (n = 584) | |
| Bad or very bad | 74 (12.7%) |
| Fair | 184 (31.5%) |
| Good or very good | 271 (46.4%) |
| Do not know/Did not answer | 55 (9.4%) |
| General HL Mean (±SD) | Limited HL n (%) | p-Value 1 | |
|---|---|---|---|
| Total (n = 563) | 59.15 (±13.05) | 454 (80.6%) | |
| Sociodemographic characteristics | |||
| Age groups | |||
| 65–74 years | 59.79 (±13.64) | 295 (78.2%) | 0.042 |
| 75+ years | 57.84 (±11.70) | 159 (85.5%) | |
| Gender | |||
| Male | 59.87 (±12.68) | 239 (81.0%) | 0.831 |
| Female | 58.35 (±13.43) | 215 (80.2%) | |
| Household living arrangement | |||
| Living alone | 58.21 (±13.71) | 137 (83.5%) | 0.292 |
| Living with others | 59.53 (±12.77) | 317 (79.4%) | |
| Country of birth | |||
| Portugal | 58.83 (±12.91) | 432 (81.4%) | 0.103 |
| Other country | 64.50 (±14.40) | 22 (68.8%) | |
| Place of residence (based on NUTS II region) | |||
| North | 59.41 (±13.81) | 116 (77.9%) | |
| Centre | 56.13 (±12.47) | 106 (87.6%) | |
| Lisbon Metropolitan Area | 60.41 (±13.12) | 182 (78.8%) | 0.174 |
| Alentejo | 60.68 (±12.58) | 24 (75.0%) | |
| Algarve | 58.61 (±9.93) | 26 (86.7%) | |
| Employment status | |||
| Working professionally | 65.05 (±11.89) | 24 (66.7%) | 0.047 |
| Not working professionally | 58.76 (±13.05) | 429 (81.6%) | |
| Educational level | |||
| Up to 2nd cycle of primary education | 53.16 (±12.16) | 165 (91.7%) | |
| 3rd cycle of primary education | 58.56 (±11.94) | 64 (86.5%) | <0.000 |
| High school | 59.06 (±11.85) | 104 (81.9%) | |
| University education | 65.37 (±12.37) | 121 (66.5%) | |
| Perceived household financial situation | |||
| Comfortable or very comfortable | 65.69 (±12.74) | 106 (64.2%) | |
| Enough for needs | 59.74 (±11.34) | 193 (82.1%) | <0.000 |
| Difficult or very difficult | 51.56 (±11.91) | 152 (95.0%) | |
| Health status and healthcare-related variables | |||
| Self-perceived health status | |||
| Good or very good | 65.14 (±12.41) | 125 (68.7%) | |
| Fair | 58.52 (±11.61) | 226 (82.5%) | <0.000 |
| Bad or very bad | 50.57 (±12.51) | 103 (96.3%) | |
| Self-reported chronic disease or disability | |||
| Yes | 56.59 (±12.73) | 231 (86.2%) | 0.002 |
| No | 61.47 (±12.93) | 223 (75.6%) | |
| Registered in primary healthcare | |||
| Yes | 58.97 (±13.07) | 432 (80.9%) | 0.474 |
| No | 62.36 (±12.48) | 22 (75.9%) | |
| Primary healthcare medical consultation last six months, at least once (n = 534) | |||
| No | 61.63 (±13.22) | 128 (75.3%) | 0.033 |
| Yes | 57.73 (±12.83) | 304 (83.5%) | |
| Primary healthcare evaluation, last six months (n = 487) | |||
| Bad or very bad | 54.29 (±13.43) | 60 (88.2%) | |
| Fair | 55.20 (±12.48) | 146 (90.1%) | 0.001 |
| Good or very good | 61.57 (±12.16) | 196 (76.3%) |
| Crude OR (95% CI) 1 | Adjusted OR, 1st bloc (95% CI) 2 | Adjusted OR, 2nd bloc (95% CI) 3 | |
|---|---|---|---|
| Age groups | |||
| 65–74 years | 1 | 1 | 1 |
| 75+ years | 1.64 (1.02–2.63) | 1.89 (1.06–3.35) | 1.78 (0.99–3.23) |
| Employment status | |||
| Working professionally | 1 | - | - |
| Not working professionally | 2.21 (1.07–4.58) | - | - |
| Educational level | |||
| University education | 1 | - | 1 |
| High school | 2.28 (1.32–3.94) | - | 1.91 (0.98–3.74) |
| 3rd cycle of primary education | 3.23 (1.55–6.72) | - | 1.86 (0.75–4.65) |
| Up to 2nd cycle of primary education | 5.55 (3.01–10.22) | - | 1.84 (0.87–3.90) |
| Perceived household financial situation | |||
| Comfortable or very comfortable | 1 | 1 | 1 |
| Enough for needs | 2.56 (1.61–4.06) | 1.85 (1.07–3.20) | 1.78 (0.995–3.17) |
| Difficult or very difficult | 10.58 (4.85–23.05) | 4.95 (2.11–11.61) | 4.17 (1.64–10.57) |
| Self-perceived health status | |||
| Good or very good | 1 | 1 | 1 |
| Fair | 2.15 (1.38–3.34) | 1.56 (0.92–2.64) | 1.41 (0.80–2.48) |
| Bad or very bad | 11.74 (4.12–33.45) | 8.29 (2.40–28.69) | 7.12 (2.02–25.09) |
| Self-reported chronic disease or disability | |||
| Yes | 1 | - | - |
| No | 2.02 (1.30–3.12) | - | - |
| Primary healthcare medical consultation last 6 months, at least once (n = 534) | |||
| No | 1 | - | - |
| Yes | 1.66 (1.07–2.60) | - | - |
| Primary healthcare evaluation, last six months (n = 487) | |||
| Good or very good | 1 | 1 | 1 |
| Fair | 2.84 (1.57–5.13) | 2.64 (1.42–4.91) | 2.75 (1.46–5.19) |
| Bad or very bad | 2.33 (1.06–5.15) | 1.68 (0.73–3.90) | 1.74 (0.74–4.09) |
| Gender | |||
| Male | - | - | 1 |
| Female | - | - | 0.87 (0.51–1.47) |
| Place of residence (based on NUTS II region) | |||
| North | - | - | 1 |
| Centre | - | - | 1.74 (0.81–3.76) |
| Lisbon Metropolitan Area | - | - | 1.27 (0.67–2.40) |
| Alentejo | - | - | 1.05 (0.36–3.12) |
| Algarve | - | - | 4.41 (0.87–22.49) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, A.; Feteira-Santos, R.; Alarcão, V.; Henriques, A.; Madeira, T.; Virgolino, A.; Arriaga, M.; Nogueira, P.J. Health Literacy among Older Adults in Portugal and Associated Sociodemographic, Health and Healthcare-Related Factors. Int. J. Environ. Res. Public Health 2023, 20, 4172. https://doi.org/10.3390/ijerph20054172
Costa A, Feteira-Santos R, Alarcão V, Henriques A, Madeira T, Virgolino A, Arriaga M, Nogueira PJ. Health Literacy among Older Adults in Portugal and Associated Sociodemographic, Health and Healthcare-Related Factors. International Journal of Environmental Research and Public Health. 2023; 20(5):4172. https://doi.org/10.3390/ijerph20054172
Chicago/Turabian StyleCosta, Andreia, Rodrigo Feteira-Santos, Violeta Alarcão, Adriana Henriques, Teresa Madeira, Ana Virgolino, Miguel Arriaga, and Paulo J. Nogueira. 2023. "Health Literacy among Older Adults in Portugal and Associated Sociodemographic, Health and Healthcare-Related Factors" International Journal of Environmental Research and Public Health 20, no. 5: 4172. https://doi.org/10.3390/ijerph20054172
APA StyleCosta, A., Feteira-Santos, R., Alarcão, V., Henriques, A., Madeira, T., Virgolino, A., Arriaga, M., & Nogueira, P. J. (2023). Health Literacy among Older Adults in Portugal and Associated Sociodemographic, Health and Healthcare-Related Factors. International Journal of Environmental Research and Public Health, 20(5), 4172. https://doi.org/10.3390/ijerph20054172