
The Relationship between Prevention and Panic from COVID-19, Ethical Principles, Life Expectancy, Anxiety, Depression and Stress



Abstract
:1. Introduction
2. Theoretical Foundations and Hypotheses Development
Explaining the Relationship between COVID-19 Prevention and Panic, Ethical Principles, Life Expectancy, Anxiety, Depression, and Stress
3. Methodology
3.1. Population and Sample
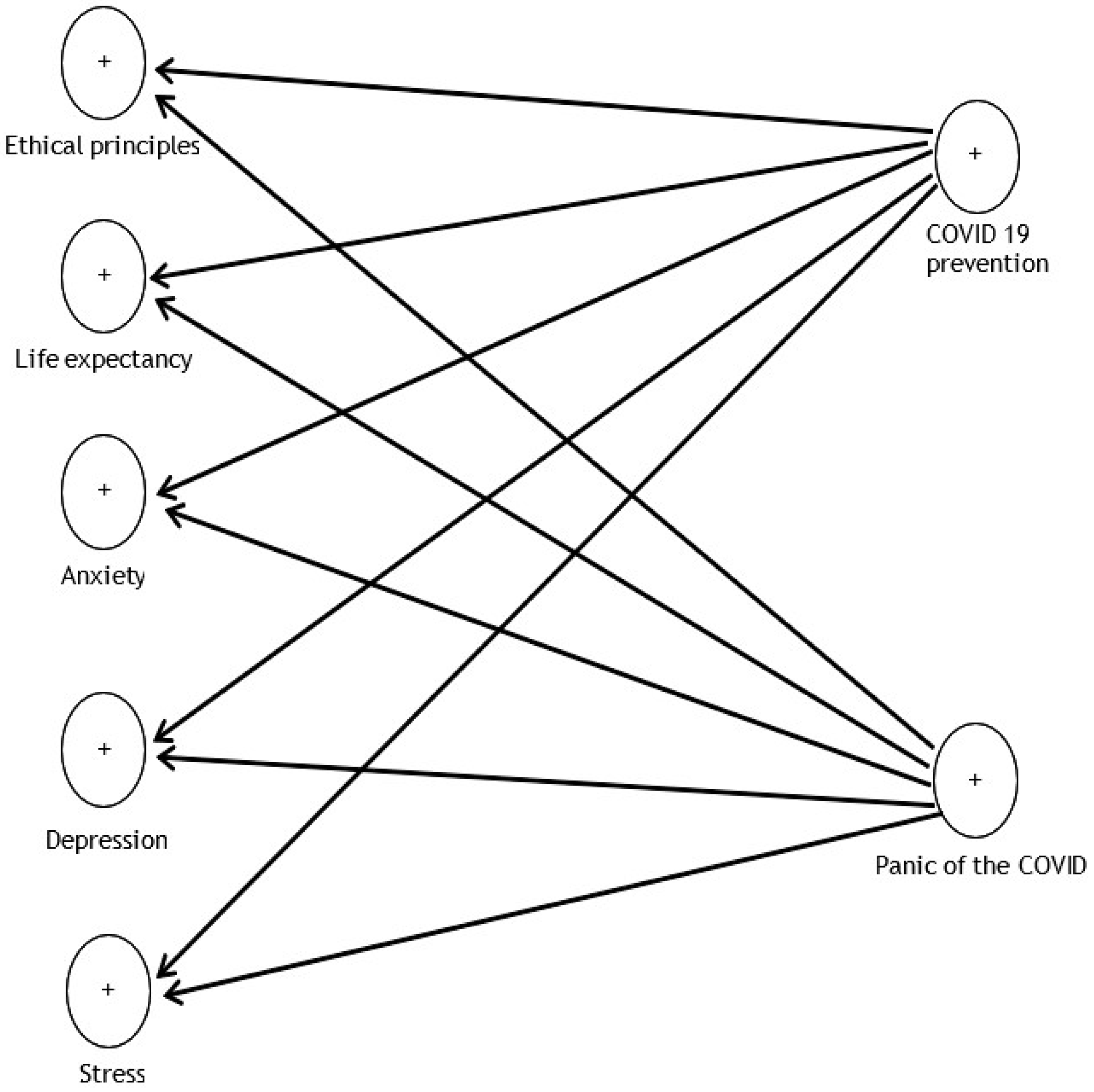
3.2. Research Model and Variables
4. Results
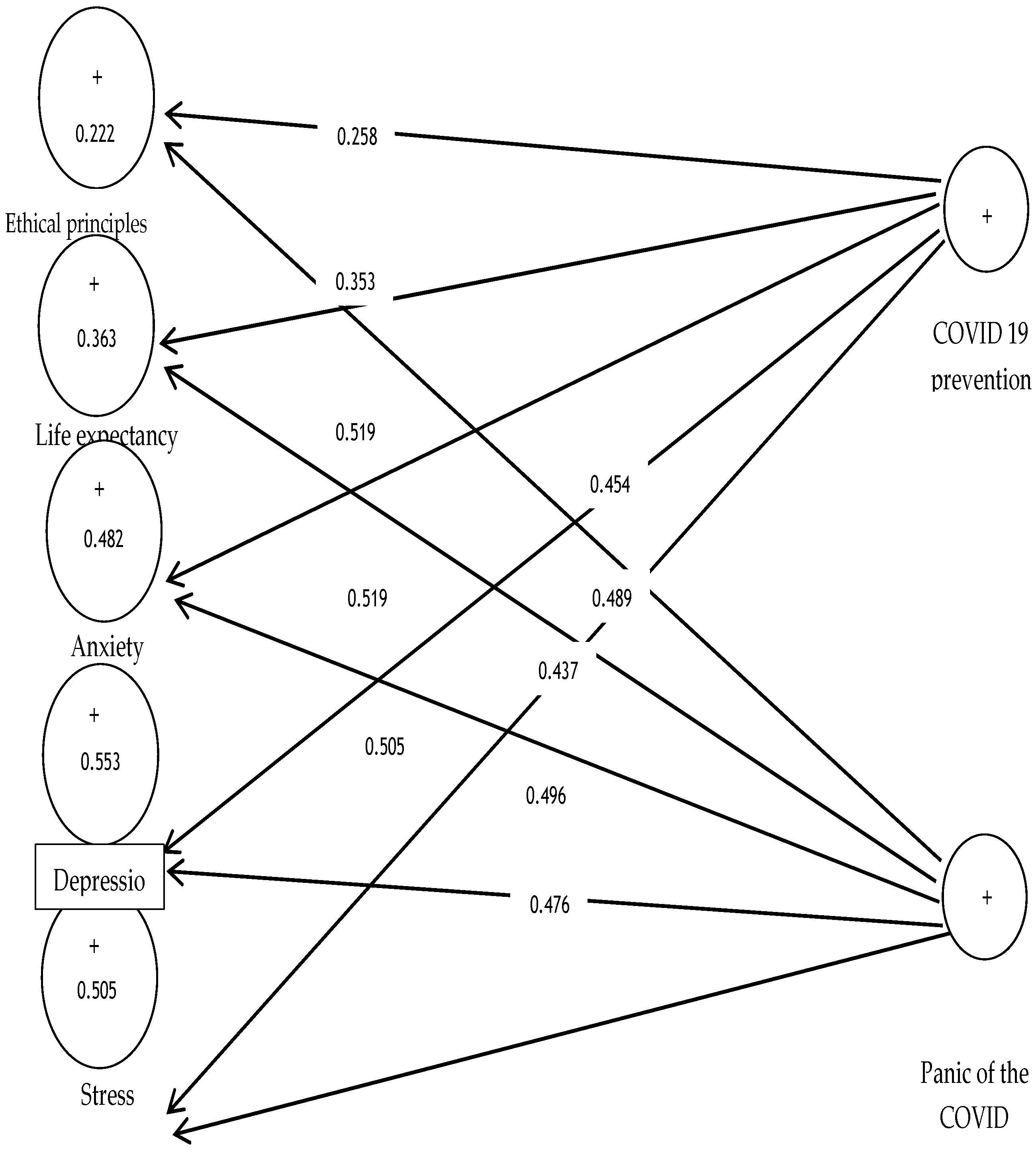
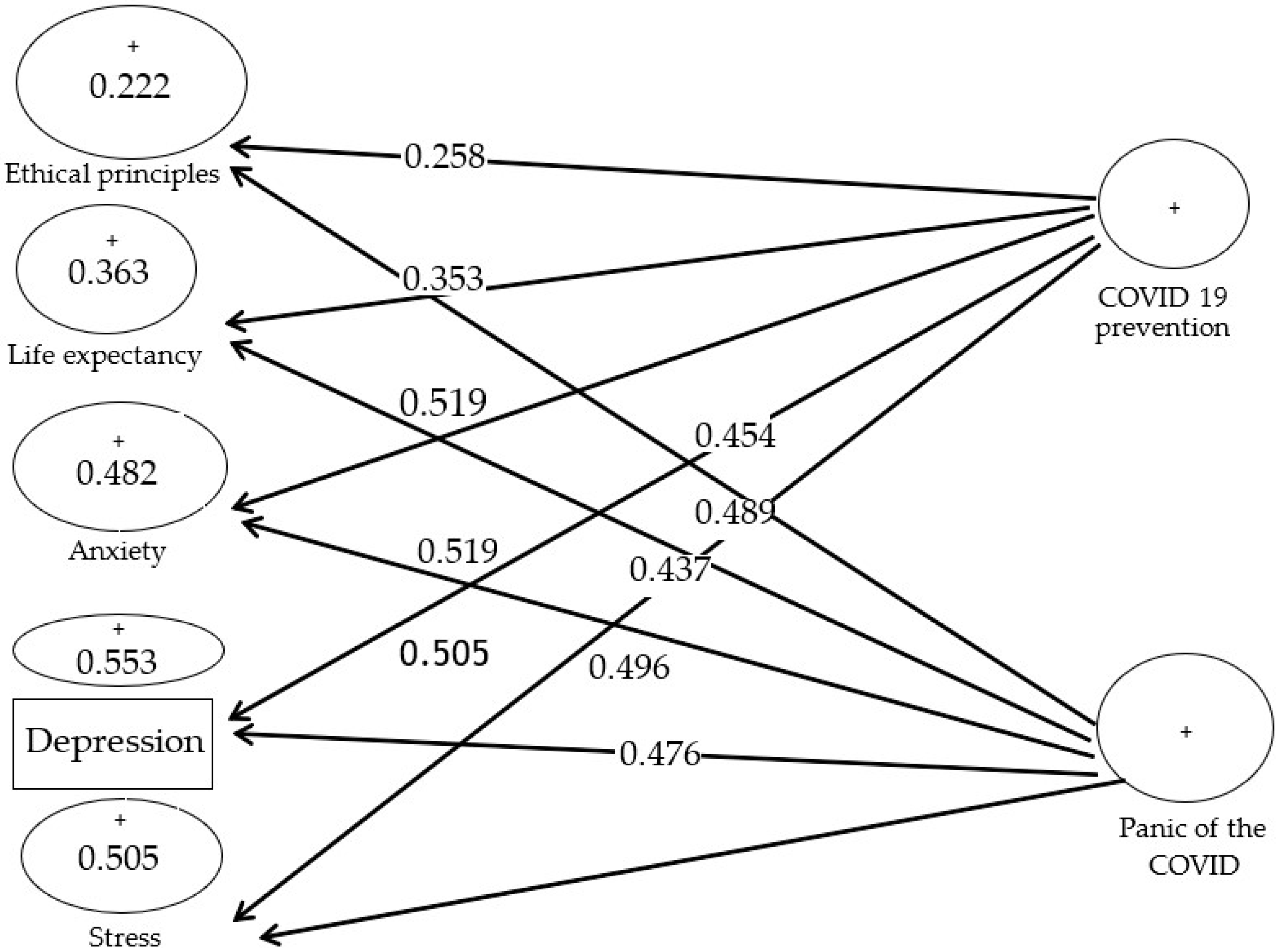
Hypotheses Testing
5. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Worldometer 2022. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 30 January 2022).
- Clampit, J.; Hasija, D.; Dugan, M.; Gamble, J. The Effect of Risk, R&D Intensity, Liquidity, and Inventory on Firm Performance during COVID-19: Evidence from US Manufacturing Industry. J. Risk Financ. Manag. 2021, 14, 499. [Google Scholar] [CrossRef]
- Zimon, G.; Tarighi, H. Effects of the COVID-19 Global Crisis on the Working Capital Management Policy: Evidence from Poland. J. Risk Financ. Manag. 2021, 14, 169. [Google Scholar] [CrossRef]
- Sadowski, A.; Galar, Z.; Walasek, R.; Zimon, G.; Engelseth, P. Big data insight on global mobility during the Covid-19 pandemic lockdown. J. Big Data 2021, 8, 78. [Google Scholar] [CrossRef]
- Garfin, D.R.; Silver, R.C.; Holman, E.A. he novel coronavirus (COVID-2019) outbreak: Amplification of public health consequences by media exposure. Health Psychol. 2020, 39, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Jia, J.S.; Lu, X.; Yuan, Y.; Xu, G.; Jia, J.; Christakis, N.A. Population flow drives Spatio-temporal distribution of COVID-19 in China. Nature 2020, 582, 389–394. [Google Scholar] [CrossRef]
- Chen, B.; Sun, J.; Feng, Y. How have COVID-19 isolation policies affected young people’s mental health?—Evidence from Chinese college students. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Zhou, X.; Xu, S.; Huang, H.; Song, J. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Feng, S.; Shen, C.; Xia, N.; Song, W.; Fan, M.; Cowling, B.J. Rational use of face masks in the COVID-19 pandemic. Lancet Respir. Med. 2020, 8, 434–436. [Google Scholar] [CrossRef]
- Horwell, C.J.; McDonald, F. The Conversation; 2020, May 5. Why You Need to Wear a Face Mask in France, but Not in the UK. Available online: https://theconversation.com/coronavirus-why-you-need-to-wear-a-face-mask-in-france-but-not-in-the-uk-137856 (accessed on 1 May 2022).
- Barcenilla-Guitard, M.; Espart, A. Influence of Gender, Age and Field of Study on Hand Hygiene in Young Adults: A Cross-Sectional Study in the COVID-19 Pandemic Context. Int. J. Environ. Res. Public Health 2021, 18, 13016. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Lo, N.C. Scientific and ethical basis for social-distancing interventions against COVID-19. Lancet Infect. Dis. 2020, 20, 631–633. [Google Scholar] [CrossRef] [Green Version]
- Precel, N.; Colangelo, A. “That Is a Concern”: People Flout distaNcing Guidelines over Easter. 2020. Available online: https://www.theage.com.au/national/victoria/that-is-a-concern-people-flout-distancing-guidelines-over-easter-20200411-p54j2o.html (accessed on 17 March 2020).
- Graham, J.; Haidt, J.; Nosek, B.A. Liberals and conservatives rely on different sets of moral foundations. J. Personal. Soc. Psychol. 2009, 96, 1029–1046. [Google Scholar] [CrossRef] [PubMed]
- Strimling, P.; Vartanova, I.; Jansson, F.; Eriksson, K. The connection between moral positions and moral arguments drives opinion change. Nat. Hum. Behav. 2019, 3, 922–930. [Google Scholar] [CrossRef]
- Waytz, A.; Iyer, R.; Young, L.; Haidt, J.; Graham, J. Ideological differences in the expanse of the moral circle. Nat. Commun. 2019, 10, 4389. [Google Scholar] [CrossRef] [PubMed]
- Haidt, J. The emotional dog and its rational tail: A social intuitionist approach to moral judgment. Psychol. Rev. 2001, 108, 814–834. [Google Scholar] [CrossRef] [PubMed]
- Hauser, M.; Cushman, F.; Young, L.; Kang-Xing Jin, R.; Mikhail, J. A dissociation between moral judgments and justifications. Mind Lang. 2008, 22, 1–21. [Google Scholar] [CrossRef]
- Major, B.; Schmader, T. Stigma, Social Identity Threat, and Health. In The Oxford Handbook of Stigma, Discrimination and Health; Major, B., Dovidio, J.F., Link, B.G., Eds.; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Kahneman, D.A. Perspective on judgment and choice: Mapping bounded rationality. Am. Psychol. 2003, 58, 697–720. [Google Scholar] [CrossRef] [Green Version]
- Dunham, A.M.; Rieder, T.N.; Humbyrd, C.J. A bioethical perspective for navigating moral dilemmas amidst the COVID-19 Pandemic. J. Am. Acad. Orthop. Surg. 2020, 28, 471–476. [Google Scholar] [CrossRef]
- Turner, L.; Munsie, M.; Levine, A.D.; Ikonomou, L. Ethical issues and public communication in the development of cell-based treatments for COVID-19: Lessons from the pandemic. Stem Cell Rep. 2021, 16, 2567–2576. [Google Scholar] [CrossRef]
- Sinnott-Armstrong, W. Moral realisms and moral dilemmas. J. Philos. 1987, 84, 263–276. [Google Scholar] [CrossRef]
- Tasso, A.; Sarlo, M.; Lotto, L. Emotions associated with counterfactual comparisons drive decision-making in Footbridge-type moral dilemmas. Motiv. Emot. 2017, 41, 410–418. [Google Scholar] [CrossRef]
- Palmiotti, G.P.; Del Popolo Cristaldi, F.; Cellini, N.; Lotto, L.; Sarlo, M. Framing the outcome of moral dilemmas: Effects of emotional information. Ethics Behav. 2020, 30, 213–229. [Google Scholar] [CrossRef]
- McCarthy, J.; Deady, R. Moral distress reconsidered. Nurs. Ethics. 2008, 15, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Dean, W.; Talbot, S.G.; Caplan, A. Clarifying the language of clinician distress. JAMA 2020, 323, 923–924. [Google Scholar] [CrossRef]
- Lützen, K.; Blom, T.; Ewalds-Kvist, B.; Winch, S. Moral stress, moralclimate and moral sensitivity among psychiatric professionals. Nurs. Ethics 2010, 17, 213–224. [Google Scholar] [CrossRef]
- Starcke, K.; Brand, M. Decision making under stress: A selective review. Neurosci. Biobehav. Rev. 2012, 36, 1228–1248. [Google Scholar] [CrossRef]
- Starcke, K.; Polzer, C.; Wolf, O.T.; Brand, M. Does stress alter everyday moral decision-making? Psych. Neuroendocrinol. 2011, 36, 210–219. [Google Scholar] [CrossRef]
- Youssef, F.F.; Dookeeram, K.; Basdeo, V.; Francis, E.; Doman, M.; Mamed, D. Stress alters personal moral decision making. Psychneuroendocrinology 2012, 37, 491–498. [Google Scholar] [CrossRef]
- Romero-Rivas, C.; Rodríguez-Cuadrado, S. Moral decision-makingand mental health during the COVID-19 pandemic. PsyArXiv 2020, 1–33. [Google Scholar] [CrossRef]
- Unützer, J.; Kimmel, R.J.; Snowden, M. Psychiatry in the age of COVID-19. World Psychiatry 2020, 19, 130. [Google Scholar] [CrossRef]
- Francis, K.; McNabb, C. Moral Decision-Making during COVID-19: Moral judgments, moralisation, and everyday behavior. Front. Psychol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mill, J.S. Utilitarianism; Parker Son Bourn: London, UK, 1863. [Google Scholar]
- Singer, P. Famine, Affluence, and Morality; Philosophy &Public Affairs: Hoboken, NJ, USA, 1972; Volume 1, pp. 229–243. [Google Scholar]
- Scanlon, T.M. The Difficulty of Tolerance: Essays in Political Philosophy; Cambridge University Press: Cambridge, UK, 2003. [Google Scholar]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Young, L.; Camprodon, J.A.; Hauser, M.; Pascual-Leone, A.; Saxe, R. Disruption of the right temporoparietal junction with transcranial magneticstimulation reduces the role of beliefs in moral judgments. Proc. Natl. Acad. Sci. USA 2010, 107, 6753–6758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaller, U.M.; Biscaldi, M.; Fangmeier, T.; van Elst, L.T.; Rauh, R. Intuitive moral reasoning in high-functioning Autism Spectrum disorder: A matter of social schemas? J. Autism Dev. Disord. 2019, 49, 1807–1824. [Google Scholar] [CrossRef] [PubMed]
- Empathy, Social Cognition, and Moral Action. In Handbook of Moral Behavior and Development; Kurtines, W.M.; Gewirtz, J.; Lamb, J.L. (Eds.) Erlbaum: New York, NY, USA, 1991; Volume 1, pp. 275–301. [Google Scholar]
- Baez, S.; García, A.M.; Santamaría-García, H. Moral cognition and moral emotions. In Neuroscience and Social Science; Ibáñez, A., Sedeño, L., García, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 169–197. [Google Scholar]
- Forbes, C.E.; Grafman, J. The role of the human prefrontal cortex in social cognition and moral judgment. Annu. Rev. Neurosci. 2010, 33, 299–324. [Google Scholar] [CrossRef] [Green Version]
- Del Casale, A.; Kotzalidis, G.D.; Rapinesi, C.; Janiri, D.; Aragona, M.; Puzella, A. Neural functional correlates of empathic face processing. Neurosci. Lett. 2017, 655, 68–75. [Google Scholar] [CrossRef]
- Eres, R.; Louis, W.R.; Molenberghs, P. Common and distinct neural networks involved in fMRI studies investigating morality: An ALEmeta-analysis. Soc. Neurosci. 2018, 13, 384–398. [Google Scholar] [CrossRef]
- Greene, J.D.; Morelli, S.A.; Lowenberg, K.; Nystrom, L.E.; Cohen, J.D. Cognitive load selectively interferes with utilitarian moral judgment. Cognition 2008, 107, 1144–1154. [Google Scholar] [CrossRef] [Green Version]
- Greene, J.D.; Nystrom, L.E.; Engell, A.D.; Darley, J.M.; Cohen, J.D. The neural bases of cognitive conflict and control in moral judgment. Neuron 2004, 44, 389–400. [Google Scholar] [CrossRef] [Green Version]
- Greene, J.D.; Sommerville, R.B.; Nystrom, L.E.; Darley, J.M.; Cohen, J.D. An fMRI investigation of emotional engagement in moral judgment. Science 2001, 293, 2105–2108. [Google Scholar] [CrossRef] [Green Version]
- Patil, I.; Zucchelli, M.M.; Kool, W.; Campbell, S.; Fornasier, F.; Calò, M. Reasoning supports utilitarian resolutions to moral dilemmas acrossdiverse measures. J. Pers. Soc. Psychol. 2020, 120, 443–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moll, J.; de Oliveira-Souza, R.; Eslinger, P.J.; Bramati, I.E.; Mourão-Miranda, J.; Andreiuolo, P.A. The neural correlates of moral sensitivity: A functional magnetic resonance imaging investigation of basic and moral emotions. J. Neurosci. 2002, 22, 2730–2736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, J.M.; Young, L.L.; Saxe, R.; Lee, S.M.; O’Young, D.; Mavros, P.L. Impaired theory of mind for moral judgment in high-functioningautism. Proc. Natl. Acad. Sci. USA 2011, 108, 2688–2692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bzdok, D.; Schilbach, L.; Vogeley, K.; Schneider, K.; Laird, A.R.; Langner, R. Parsing the neural correlates of moral cognition: ALE meta-analysis on morality, theory of mind, and empathy. Brain Struct. Funct. 2012, 217, 783–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hovenkamp-Hermelink, J.H.; Jeronimus, B.F.; Spinhoven, P.; Penninx, B.W.; Schoevers, R.A.; Riese, H. Differential associations of locus of control with anxiety, depression and life-events: A five-wave, nine-year study to test stability and change. J. Affect. Disord. 2019, 253, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, J.; Yoeli, E.; Rand, D. Don’t get it or don’t spread it? Comparing self-interested versus prosocially framed COVID-19 prevention messaging. PsyArXi. 2020, 1–60. [Google Scholar] [CrossRef] [Green Version]
- Pfattheicher, S.; Nockur, L.; Böhm, R.; Sassenrath, C.; Petersen, M.B. The emotional path to action: Empathy promotes physical distancing during the COVID-19 pandemic. PsyArXiv 2020, 31. [Google Scholar] [CrossRef] [Green Version]
- Oosterhoff, B.; Palmer, C. Psychological correlates of news monitoring, social distancing, disinfecting, and hoarding behaviors among US adolescents during the COVID-19 pandemic. PsyArXiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Elmer, T.; Mepham, K.; Stadtfeld, C. Students under lockdown:comparisons of students’ social networks and mental health before and during the COVID-19 Crisis in Switzerland. PLoS ONE 2020, 15, e0236337. [Google Scholar] [CrossRef]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Dai, J. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]
- Ornelas, I.J.; Tornberg-Belanger, S.; Balkus, J.E.; Bravo, P.; Perez Solorio, S.A.; Perez, G.E.; Tran, A.N. Coping With COVID-19: The Impact of the Pandemic on Latina Immigrant Women’s Mental Health and Well-being. Health Educ. Behav. 2021, 48, 733–738. [Google Scholar] [CrossRef]
- Li, S.; Wang, Y.; Xue, J.; Zhao, N.; Zhu, T. The impact of COVID-19epidemic declaration on psychological consequences: A study on active Weibo users. Int. J. Environ. Res. Public Health 2020, 17, 2032. [Google Scholar] [CrossRef] [Green Version]
- Alyami, M.; Henning, M.; Krägeloh, C.U.; Alyami, H. Psychometric evaluation of the Arabic version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2021, 19, 2219–2232. [Google Scholar] [CrossRef]
- Sakib, N.; Bhuiyan, A.K.M.I.; Hossain, S.; Al Mamun, F.; Hosen, I.; Abdullah, A.H. Psychometric validation of the Bangla Fear of COVID-19 Scale: Confirmatory factor analysis and rsearch analysis. Int. J. Ment. Health Addict. 2020, 1–12. [Google Scholar] [CrossRef]
- Satici, B.; Gocet-Tekin, E.; Deniz, M.E.; Satici, S.A. Adaptation of the Fear of COVID-19 Scale: Its association with psychological distress and life satisfaction in Turkey. Int. J. Ment. Health Addict. 2020, 19, 1980–1988. [Google Scholar] [CrossRef]
- Reznik, A.; Gritsenko, V.; Konstantinov, V.; Khamenka, N.; Isralowitz, R. COVID-19 fear in Eastern Europe: Validation of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–6. [Google Scholar] [CrossRef]
- Tzur Bitan, D.; Grossman-Giron, A.; Bloch, Y.; Mayer, Y.; Shiffman, N.; Mendlovic, S. Fear of COVID-19 Scale: Psychometric characteristics, reliability and validity in the Israeli population. Psychiatry Res. 2020, 289, 113100. [Google Scholar] [CrossRef]
- Huarcaya-Victoria, J.; Villarreal-Zegarra, D.; Podestà, A.; Luna-Cuadros, M.A. Psychometric properties of a Spanish version of the Fear of COVID-19 Scale in general population of Lima, Peru. Int. J. Ment. Health Addict. 2020, 20, 249–262. [Google Scholar] [CrossRef]
- Barrios, I.; Ríos-González, C.; O’Higgins, M.; González, I.; García, O.; Díaz, N.R. Psychometric properties of the Spanish version of the Fear of COVID-19 Scale (FCV-19S). Int. J. Ment. Health Addict. 2020, 20, 249–262. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamun, M.A.; Griffiths, M.D. First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: Possible suicide prevention strategies. Asian J. Psychiatr. 2020, 51, 102073. [Google Scholar] [CrossRef] [PubMed]
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalised anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Dong, L.; Freedman, V.A.; de Leon, C.F.M. The association of comorbid depression and anxiety symptoms with disability onset in older adults. Psychosom. Med. 2020, 82, 158–164. [Google Scholar] [CrossRef]
- Fiske, A.; McLennan, S.; Buyx, A. Ethical insights from the COVID-19 pandemic in Germany: Considerations for building resilient healthcare systems in Europe. Lancet Reg. Health–Eur. 2021, 9, 100213. [Google Scholar] [CrossRef]
- Nuggerud-Galeas, S.; Oliván Blázquez, B.; Perez Yus, M.C.; Valle-Salazar, B.; Aguilar-Latorre, A.; Magallón Botaya, R. Factors associated with depressive episode recurrences in primary care: A retrospective, descriptive study. Front. Psychol. 2020, 11, 1230. [Google Scholar] [CrossRef]
- Mak, I.W.C.; Chu, C.M.; Pan, P.C.; Yiu, M.G.C.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef]
- Lee, S.M.; Kang, W.S.; Cho, A.R.; Kim, T.; Park, J.K. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef]
- Morganstein, J.C.; Ursano, R.J. Ecological disasters and mental health: Causes, consequences, and interventions. Front. Psychol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cheung, Y.T.; Chau, P.H.; Yip, P.S.F. A revisit on older adults suicides and Severe Acute Respiratory Syndrome (SARS) epidemic in Hong Kong. Int. J. Geriatr. Psychiatry 2008, 23, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- Zou, P.; Sun, L.; Yang, W.; Zeng, Y.; Chen, Q.; Yang, H. Associations between negative life events and anxiety, depressive, and stress symptoms: A cross-sectional study among Chinese male senior college students. Psychiatry Res. 2018, 270, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, S.P.; Meng, S.; Wu, Y.J.; Mao, Y.P.; Ye, R.X.; Wang, Q.Z. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [Green Version]
- Orellana, C.I.; Orellana, L.M. Predictores de síntomas emocionales durante la cuarentena domiciliar por pandemia de COVID-19 en El Salvador. Actual. Psicol. 2020, 34, 103–120. [Google Scholar] [CrossRef]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. “Pandemic fear” and COVID-19: Mental health burden and strategies. Braz. J. Psychiatry 2020, 42, 232–235. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Rey, R.; Garrido-Hernansaiz, H.; Collado, S. Psychological impact and associated factors during the initial stage of the Coronavirus (COVID-19) pandemic among the general population in Spain. Front. Psychol. 2020, 11, 1540. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.; Hu, G.; Xiong, H.; Qiu, H.; Yuan, X. Psychological impact of the coronavirus disease 2019 (COVID-19) outbreak on healthcare workers in China. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Galea, S.; Merchant, R.M.; Lurie, N. The mental health consequences of COVID19 and physical distancing: The need for prevention and early intervention. JAMA Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [Green Version]
- Goyal, K.; Chauhan, P.; Chhikara, K.; Gupta, P.; Singh, M.P. Fear of COVID 2019: First suicidal case in India. Asian J. Psychiatry 2020, 49, 101989. [Google Scholar] [CrossRef]
- Gaudine, A.; Thorne, L. Emotion and ethical decision-making in organizations. J. Bus. Ethics 2001, 31, 175–187. [Google Scholar] [CrossRef]
- Ho, J.T.; Dupasquier, J.R.; Scarfe, M.L.; Moscovitch, D.A. Fears of Receiving Compassion from Others Predict Safety Behaviour Use in Social Anxiety Disorder Over and Above Fears of Negative Self-Portrayal. J. Anxiety Disord. 2021, 80, 102387. [Google Scholar] [CrossRef] [PubMed]
- Jizheng, H.; Mingfeng, H.; Tengda, L.; Ake, R.; Xiaoping, Z. A survey of mental health of medical staff in new-type coronavirus pneumonia hospitals. Chin. J. Ind. Hyg. Occup. Dis. 2020, 17, 475–480. [Google Scholar] [CrossRef]
- Xiang, Y.T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wu, W.; Zhao, X.; Zhang, W. Recommended psychological crisis intervention response to the 2019 novel coronavirus pneumonia outbreak in China: A model of West China Hospital. Precis. Clin. Med. 2020, 3, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.W.; Song, H.R. Structural relationships among public’s risk characteristics, trust, risk perception and preventive behavioral intention: The case of MERS in Korea. Crisisnomy 2017, 13, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Tausczik, Y.; Faasse, K.; Pennebaker, J.W.; Petrie, K.J. Public anxiety and information seeking following the H1N1 outbreak: Blogs, newspaper articles, and Wikipedia visits. Health Commun. 2012, 27, 179–185. [Google Scholar] [CrossRef]
- Maunder, R.; Hunter, J.; Vincent, L. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. CMAJ 2003, 168, 1245–1251. [Google Scholar]
- Somma, A.; Gialdi, G.; Krueger, R.F.; Markon, K.E.; Frau, C.; Lovallo, S.; Fossati, A. Dysfunctional personality features, non-scientifically supported causal beliefs, and emotional problems during the first month of the COVID-19 pandemic in Italy. Personal. Individ. Differ. 2020, 165, 110139. [Google Scholar] [CrossRef]
- Bavel, J.J.V.; Baicker, K.; Boggio, P.S. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.K.T.; Carvalho, P.M.; Lima, I.; Nunes, J.V.A.; Saraiva, J.S.; Souza, R.I.; Neto, M.L.R. The emotional impact of coronavirus 2019- Ncov (New Coronavirus Disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef]
- Román, F.; Santibáñez, P.; Vinet, E.V. Uso de las Escalas de Depresión Ansiedad Estrés (DASS-21) como Instrumento de Tamizaje en Jóvenes con Problemas Clínicos. Acta Investig. Psicol. 2016, 6, 2325–2336. [Google Scholar] [CrossRef]
- Sandín, B.; Valiente, R.M.; García-Escalera, J.; Chorot, P. Impacto psicológico de la pandemia de COVID-19: Efectos negativos y positivos en población española asociados al periodo de confinamiento nacional. Rev. Psicopatol. Y Psicol. Clin. 2020, 25, 1–22. [Google Scholar] [CrossRef]
- Mertens, G.; Gerritsen, L.; Duijndam, S.; Salemink, E.; Engelhard, I.M. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. J. Anxiety Disord. 2020, 74, 102258. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, N.C.; Newman, M.G. Anxiety and depression as bidirectional risk factors for one another: A meta-analysis of longitudinal studies. Psychol. Bull. 2017, 143, 1155–1200. [Google Scholar] [CrossRef] [PubMed]
- Jansson-Fröjmark, M.; Lindblom, K. A bidirectional relationship between anxiety and depression, and insomnia? A prospective study in the general population. J. Psychosom. Res. 2008, 64, 443–449. [Google Scholar] [CrossRef]
- Marquez, N.M.; Littman, A.M.; Rossi, V.E.; Everett, M.C.; Tyagi, E.; Johnson, H.C.; Dolovich, S.L. Life Expectancy and COVID-19 in Florida State Prisons. Am. J. Prev. Med. 2022, 1–4. [Google Scholar] [CrossRef]
- Fjermestad, K.W.; Orm, S.; Silverman, W.K.; Cogo-Moreira, H. COVID-19-related anxiety is associated with mental health problems among adults with rare disorders. Res. Dev. Disabil. 2022, 123, 104181. [Google Scholar] [CrossRef]
- Bridgland, V.M.E.; Moeck, E.K.; Green, D.M.; Swain, T.L.; Nayda, D.M.; Matson, L.A.; Hutchison, N.P.; Takarangi, M.K.T. Why the COVID-19 pandemic is a traumatic stressor. PLoS ONE 2021, 16, e0240146. [Google Scholar] [CrossRef]
- Stewart, D.E.; Appelbaum, P.S. COVID-19 and psychiatrists’ responsibilities: A WPA position paper. World Psychiatry 2020, 19, 406. [Google Scholar] [CrossRef]
- McDaid, D. Investing in strategies to support mental health recovery from the COVID-19 pandemic. Eur. Psychiatry 2021, 64, e32. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Combined Reliability Coefficient |
|---|---|
| COVID-19 prevention | 0.805 |
| Panic of COVID-19 | 0.892 |
| Ethical principles | 0.782 |
| Life expectancy | 0.751 |
| Anxiety | 0.903 |
| Depression | 0.744 |
| Stress | 0.825 |
| Structures | Stress | Anxiety | Depression | Life Expectancy | Ethical Principles | Panic of COVID-19 | COVID-19 Prevention |
|---|---|---|---|---|---|---|---|
| Stress | 0.721 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Anxiety | 0.469 | 0.708 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Depression | 0.627 | 0.645 | 0.632 | 0.000 | 0.000 | 0.000 | 0.000 |
| Life expectancy | 0.276 | 0.293 | 0.321 | 0.615 | 0.000 | 0.000 | 0.000 |
| Ethical principles | 0.611 | 0.444 | 0.535 | 0.273 | 0.608 | 0.000 | 0.000 |
| Panic of COVID-19 | 0.671 | 0.568 | 0.628 | 0.387 | 0.510 | 0.604 | 0.000 |
| COVID-19 prevention | 0.449 | 0.570 | 0.571 | 0.338 | 0.548 | 0.519 | 0.588 |
| Structure | R Square |
|---|---|
| Ethical principles | 0.222 |
| Life expectancy | 0.363 |
| Anxiety | 0.482 |
| Depression | 0.553 |
| Stress | 0.505 |
| Information | Status | No. | Percentage |
|---|---|---|---|
| Gender | Male | 163 | 82.3 |
| Female | 35 | 17.7 | |
| Education | Bachelor | 124 | 62.6 |
| M.A. | 39 | 19.7 | |
| PhD. | 4 | 2 | |
| Age | 20 < 30 | 21 | 10.6 |
| 31 < 40 | 137 | 69.2 | |
| 41 < 50 | 24 | 12.1 | |
| >51 | 16 | 8.1 | |
| Job grade | Audit supervisor | 12 | 6.1 |
| Senior audit supervisor | 28 | 14.1 | |
| Auditor | 6 | 3 | |
| Senior auditor | 152 | 76.8 | |
| Professional experience | <5 | 24 | 12.1 |
| 6 < 10 | 123 | 62.1 | |
| 11 < 15 | 16 | 8.1 | |
| 16 < 20 | 28 | 14.1 | |
| >21 | 7 | 3.5 |
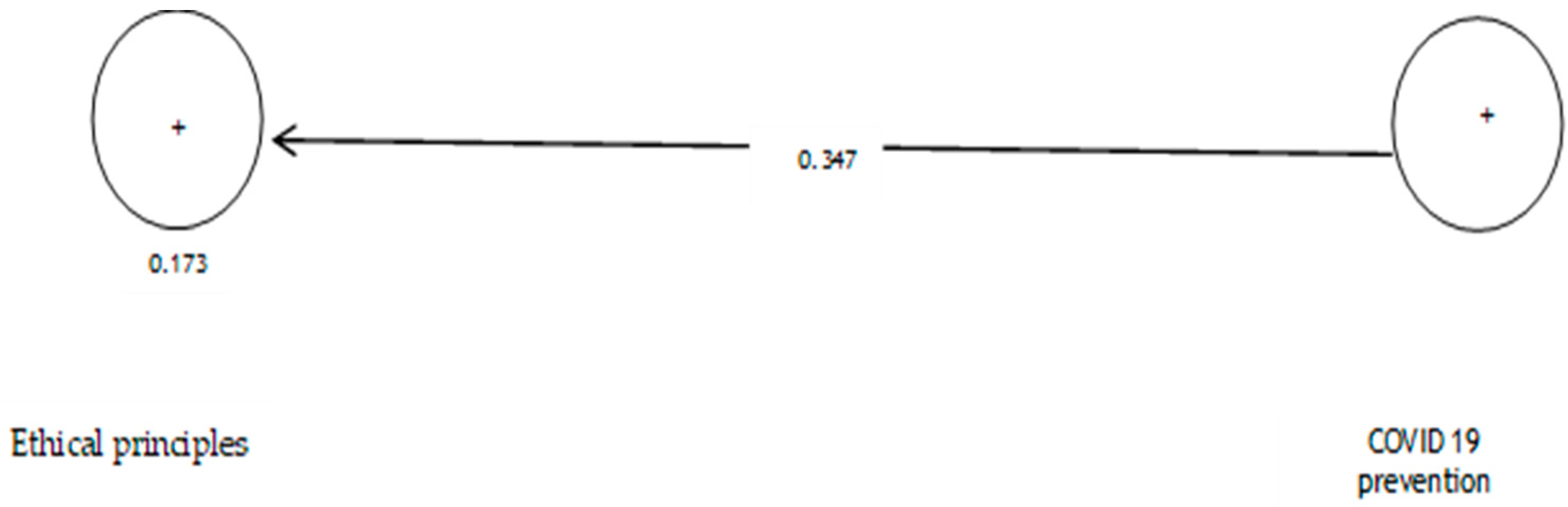
| The Relationship of Variables | Path Coefficient (β) | Test Value t | Significance Level | Results |
|---|---|---|---|---|
| COVID-19 prevention—Ethical principles | 0.347 | 1.719 | 0.086 | Confirmed |
| The Relationship of Variables | Path Coefficient (β) | Test Value t | Significance Level | |
|---|---|---|---|---|
| COVID-19 prevention—Life expectancy | 0.312 | 1.383 | 0.000 | Confirmation |
| The Relationship of Variables | Path Coefficient (β) | Test Value t | Significance Level | |
|---|---|---|---|---|
| COVID-19 prevention—Anxiety | 0.696 | 14.514 | 0.000 | Confirmed |
| The Relationship of Variables | Path Coefficient (β) | Test Value t | Significance Level | |
|---|---|---|---|---|
| COVID-19 prevention—Depression | 0.705 | 14.149 | 0.000 | Confirmed |
| The Relationship of Variables | Path Coefficient (β) | Test Value t | Significance Level | |
|---|---|---|---|---|
| COVID-19 prevention—Stress | 0.630 | 6.656 | 0.000 | Confirmed |
| The Relationship of Variables | Path Coefficient (β) | Test Value t | Significance Level | |
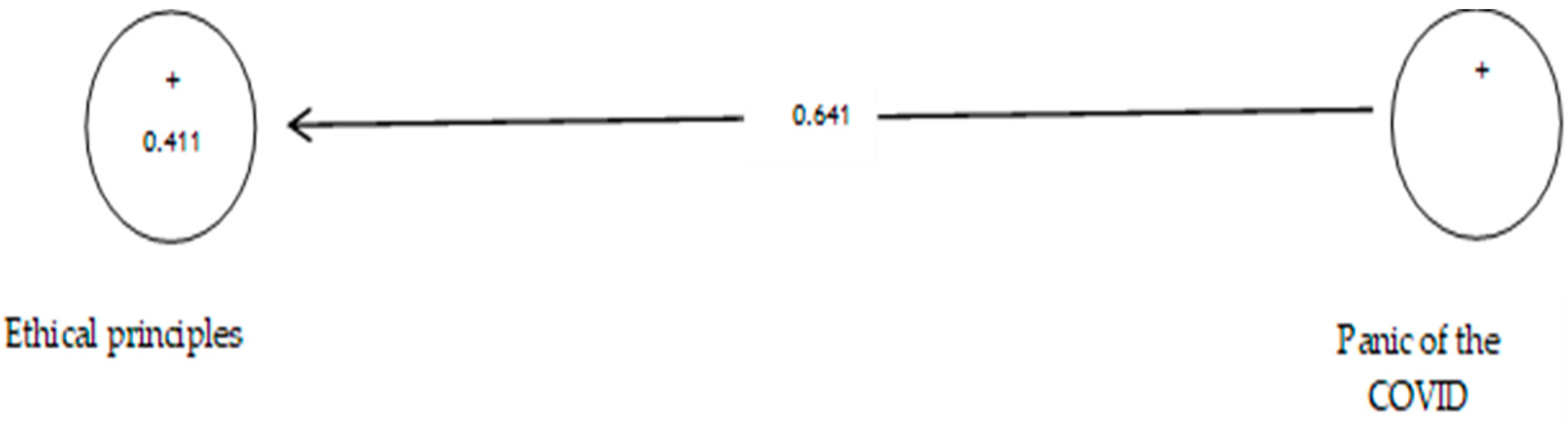
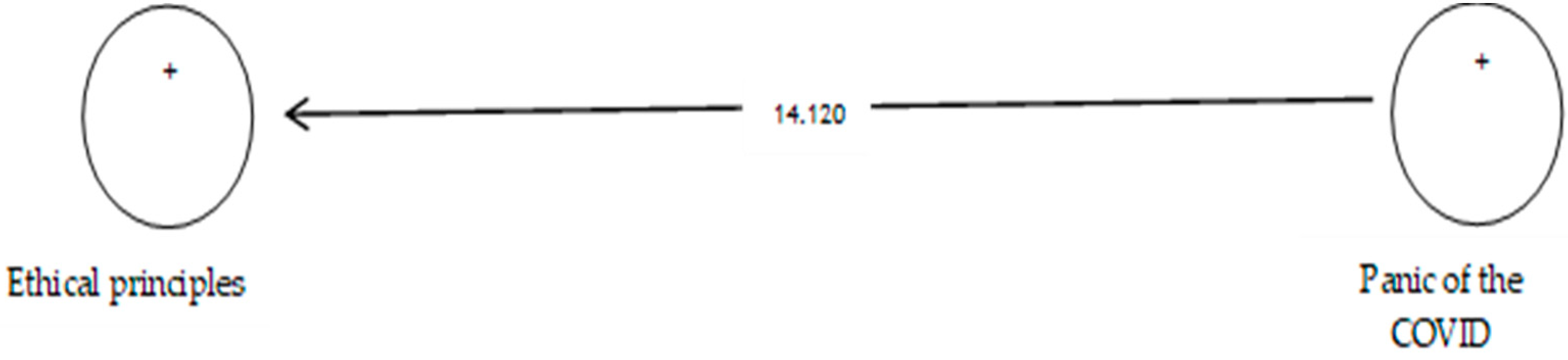
|---|---|---|---|---|
| Panic of COVID-19—Ethical principles | 0.641 | 14.120 | 0.000 | Confirmed |
| The Relationship of Variables | Path Coefficient (β) | Test Value t | Significance Level | |
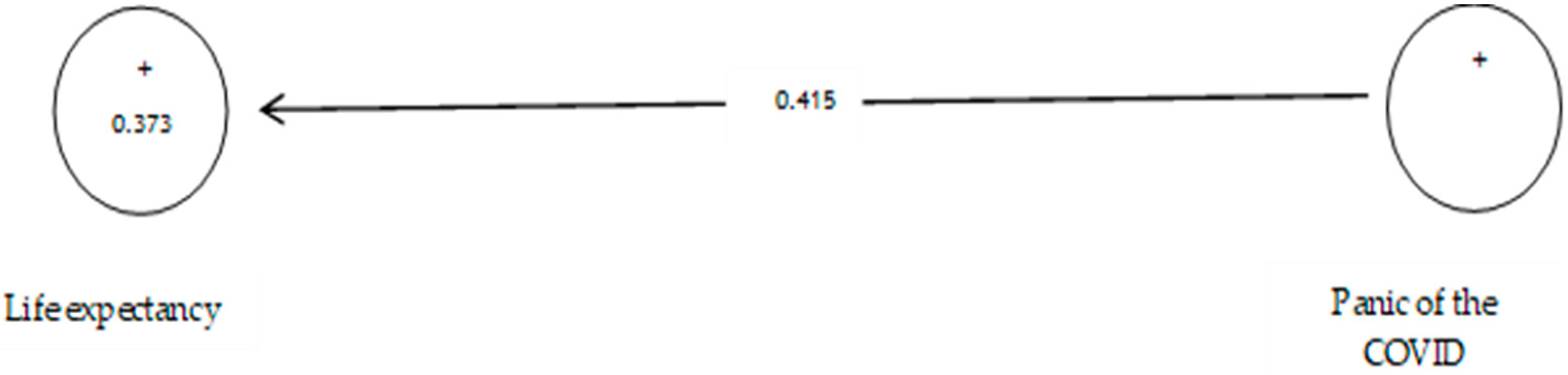
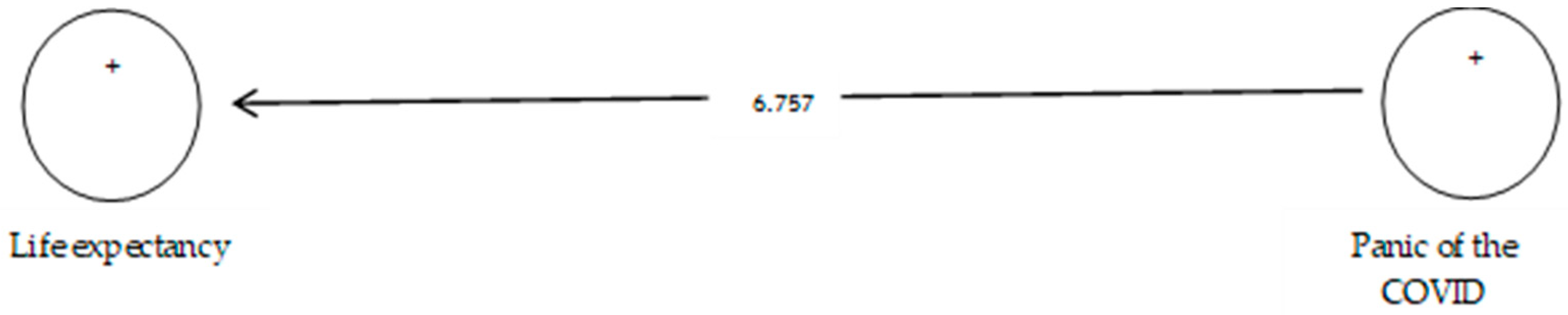
|---|---|---|---|---|
| Panic of COVID-19—Life expectancy | 0.415 | 6.757 | 0.000 | Confirmed |
| The Relationship of Variables | Path Coefficient (β) | Test Value t | Significance Level | |
|---|---|---|---|---|
| Panic of COVID-19—Anxiety | 0.585 | 10.297 | 0.000 | Confirmed |
| The Relationship of Variables | Path Coefficient (β) | Test Value t | Significance Level | |
|---|---|---|---|---|
| Panic of COVID-19—Depression | 0.654 | 11.986 | 0.000 | Confirmed |
| The Relationship of Variables | Path Coefficient (β) | Test Value t | Significance Level | |
|---|---|---|---|---|
| Panic of COVID-19—Stress | 0.682 | 14.416 | 0.000 | Confirmed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salehi, M.; Zimon, G.; Ghaderi, A.R.; Hasan, Z.A. The Relationship between Prevention and Panic from COVID-19, Ethical Principles, Life Expectancy, Anxiety, Depression and Stress. Int. J. Environ. Res. Public Health 2022, 19, 5841. https://doi.org/10.3390/ijerph19105841
Salehi M, Zimon G, Ghaderi AR, Hasan ZA. The Relationship between Prevention and Panic from COVID-19, Ethical Principles, Life Expectancy, Anxiety, Depression and Stress. International Journal of Environmental Research and Public Health. 2022; 19(10):5841. https://doi.org/10.3390/ijerph19105841
Chicago/Turabian StyleSalehi, Mahdi, Grzegorz Zimon, Ali Reza Ghaderi, and Zinab Ahmed Hasan. 2022. "The Relationship between Prevention and Panic from COVID-19, Ethical Principles, Life Expectancy, Anxiety, Depression and Stress" International Journal of Environmental Research and Public Health 19, no. 10: 5841. https://doi.org/10.3390/ijerph19105841
APA StyleSalehi, M., Zimon, G., Ghaderi, A. R., & Hasan, Z. A. (2022). The Relationship between Prevention and Panic from COVID-19, Ethical Principles, Life Expectancy, Anxiety, Depression and Stress. International Journal of Environmental Research and Public Health, 19(10), 5841. https://doi.org/10.3390/ijerph19105841