Abstract
Genetic variants of severe acute respiratory syndrome coronavirus (SARS-CoV-2) have been globally surging and devastating many countries around the world. There are at least eleven reported variants dedicated with inevitably catastrophic consequences. In 2021, the most dominant Delta and Omicron variants were estimated to lead to more severity and deaths than other variants. Furthermore, these variants have some contagious characteristics involving high transmissibility, more severe illness, and an increased mortality rate. All outbreaks caused by the Delta variant have been rapidly skyrocketing in infection cases in communities despite tough restrictions in 2021. Apart from it, the United States, the United Kingdom and other high-rate vaccination rollout countries are still wrestling with this trend because the Delta variant can result in a significant number of breakthrough infections. However, the pandemic has changed since the latest SARS-CoV-2 variant in late 2021 in South Africa, Omicron. The preliminary data suggest that the Omicron variant possesses 100-fold greater than the Delta variant in transmissibility. Therefore, this paper aims to review these characteristics based on the available meta-data and information from the first emergence to recent days. Australia and the five most affected countries, including the United States, India, Brazil, France, as well as the United Kingdom, are selected in order to review the transmissibility, severity and fatality due to Delta and Omicron variants. Finally, the vaccination programs for each country are also reviewed as the main factor in prevention.
1. Introduction
There is no doubt that the entire world’s population has been suffering from coronavirus disease (COVID-19) pandemic since the first infection of a new coronavirus, recently known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was recorded in Wuhan, China in December 2019 [1,2,3]. More importantly, it has caused unimaginable damages to societies and economies worldwide due to its increased transmissibility and high mortality rate [4,5,6,7,8]. In general, air pollutants with micro-particle (PM10, PM2.5, and other pollutants in the atmosphere) can go deep into the alveolar region of the human lung and lead to severe respiratory diseases. However, the amount of this particle deposition is based on the lung sizes (human age), daily physical activities (causing different airflow rates), and micro-particle sizes [9,10,11,12,13,14,15,16]. For SARS-CoV-2, it is classified as a nano-particle at 120 nm and can be up to 1000 nm [17,18,19]. Several researchers proved that toxic nano-particles lead to a greater negative impact on the respiratory system compared to toxic micro-particles [20,21,22,23].
According to the latest updated data from the World Health Organization (WHO) [24] on 26 March 2022, the world has recorded over 480 million COVID-19 cases, and it has been responsible for over 6 million deaths around the world. Unfortunately, since the pandemic, SARS-CoV-2 has been dramatically evolving in a wide range of variants dedicated to devastating characteristics [25,26,27,28]. Apart from this, the term “variant” refers to a group of viruses that have mutated from the original lineages with additional changes to the characteristic spike protein [29]. According to The United States Department of Health and Human Services (HHS) and SARS-CoV-2 Interagency Group (SIG) [30], there are three main types of variant classifications, including Variant of Interest (VOI), Variant of Concern (VOC) and Variant of High Consequence (VOHC). In terms of VOCs, many countries have been struggling with the emergence and spread of ongoing variants, including in Southeast Asia, Middle East, Europe and North America. A group of experts at the World Health Organization (WHO) decided to name these variants using the Greek alphabet, such as Alpha, Beta, Gamma and Delta, which is easier for non-scientific people to discuss [31]. According to WHO [32], some of the VOCs are listed in Table 1 below:

Table 1.
Recently designed Variants of Concern by WHO [32].
In terms of the Delta variant of SARS-CoV-2, it has caused the latest wave of infection resulting in socio-economic setbacks across many countries around the world [33]. In December 2020, the first case of the Delta infection was detected in India [34,35,36,37,38]. Since then, the Delta variant has been drastically spreading across many unvaccinated countries with tremendous numbers of cases, increasing hospitalizations and mortality rates [34,39,40,41]. However, Del Rio et al. [34] also presented that the emergence of the Delta variant in the UK and US have created a massive wave of new infections despite their high vaccination rate [34]. Noticeably, the most affected areas are highly located at unvaccinated or delayed second-dose communities. Generally speaking, some main factors should be taken into account to discuss the characteristics of the Delta variant. First, its transmissibility is highly infectious, which is more than double compared to previous lineages. Second, Sheikh et al. [42] and Fisman [43] claim that in unvaccinated patients, the infections of the Delta variant potentially cause more severe sickness than previous variants [42,43]. Additionally, these patients are highly likely to be monitored under the intensive care unit (ICU) than from the Alpha and original strains. Moreover, Riemersma et al. [44] and Nasreen et al. [45] analysed the impacts of the Delta variant on fully vaccinated people, and they agree that although there are breakthrough infections among the vaccinated people, the infections tend to reduce faster than unvaccinated people.
Regarding the outbreaks in Australia, Australia has undoubtedly succeeded in preventing the initial wave of infection (March–June 2020) and second wave (June–September 2020) in the south-eastern state of Victoria (VIC) by their effective actions, including quick and immediate management in contact tracing and local lockdowns, travel restrictions, and social distancing [46,47,48]. Despite the trigger of social distancing restrictions and business shutdowns involving retailers and construction work, the number of confirmed cases has significantly risen to 100 and 439, within 10 days and 23 days, respectively, since the first case was detected [49]. It is evident that the Delta variant is more transmissible than previous variants, regardless of if it can result in more severity and mortality. First, many studies suggest that unvaccinated people are the most vulnerable because they tend to be sicker quickly and more severely during the infection. An instance illustrating this point is that the UK study asserts that Delta cases have double the risk of hospitalization than Alpha cases among over 40,000 SARS-CoV-2 cases [40]. Furthermore, a study in Canada also claims that infected people by the Delta variant escalate the probability of hospitalization and fatality by twofold [47]. Consequently, transmissibility and mortality are the most concerning characteristics of the Delta variant.
Conversely, the detection of a new and greatly mutated SAR-CoV-2 variant in South Africa, Omicron, has been causing global grave concern. First, the Omicron variant is designated as a variant of concern, B.1.1529, by The World Health Organization (WHO) [50], and it was first reported in Botswana on 11 November 2021. Since the initial detection, the Omicron variant has spread in over 20 countries across the globe within a week, including in Hong Kong, the UK, the US and Australia. Thus, Omicron is globally recognized as a high-risk variant. Omicron has currently become the most predominant variant detected in SARS-CoV-2 cases in various South African countries, such as Botswana and Zimbabwe, and in Israel and Hong Kong. According to Rao and Singh [51], the Omicron variant is 100-fold greater, as compared to the Delta variant, in the rate of infection. In detail, a few recent studies were conducted to analyse the mutational profile of the Omicron variant [52,53]. Therefore, Venkatakrishnan et al. [52] claim that after the comparison between Omicron and previous variants of concern (Delta, Alpha, Gamma, Delta), the Omicron variant possesses up to 37 mutations in its spike protein involving 26 unique mutations which make Omicron a “step function” of the SARS-CoV-2 strains’ evolution. The summary of the mutational profile of the spike mutations in the SARS-CoV-2 variants of concern can be found in Table 2.
Table 2.
Summary of mutational profile of spike mutations in the SARS-CoV-2 variants of concern (Alpha, Beta, Gamma, Delta and Omicron).
Furthermore, there is a well-established fact that the Omicron variant has higher transmissibility and infectivity than the Delta variant [54,55,56]. However, there is no available evidence that the Omicron variant can cause more severe sickness or that it can reduce vaccine effectiveness. In brief, due to the deadly continuing spread of Omicron and Delta VOCs worldwide, many countries, including the United States (US), Canada, and the United Kingdom (UK) have been conducting several studies to investigate national and global trends of these two VOCs infected waves. However, there are limited studies conducted to analyse not only the highlighted characteristics but also the differences between Omicron and Delta VOCs, in terms of transmissibility and severity.
Therefore, this review paper aims to summarize the differences between Delta and Omicron variants by focusing on the impact of Omicron and Delta variants on vaccine effectiveness, transmissibility, severity, mortality. To provide more details, Australia and the most affected countries including Brazil, France, India, the US and the UK will be selected for this review. In addition, this paper also summarizes the current preventions that have been used to deal with SARS-CoV-2 variants.
2. SARS-CoV-2, Delta Variant and Omicron Variant
2.1. Chemical Composition
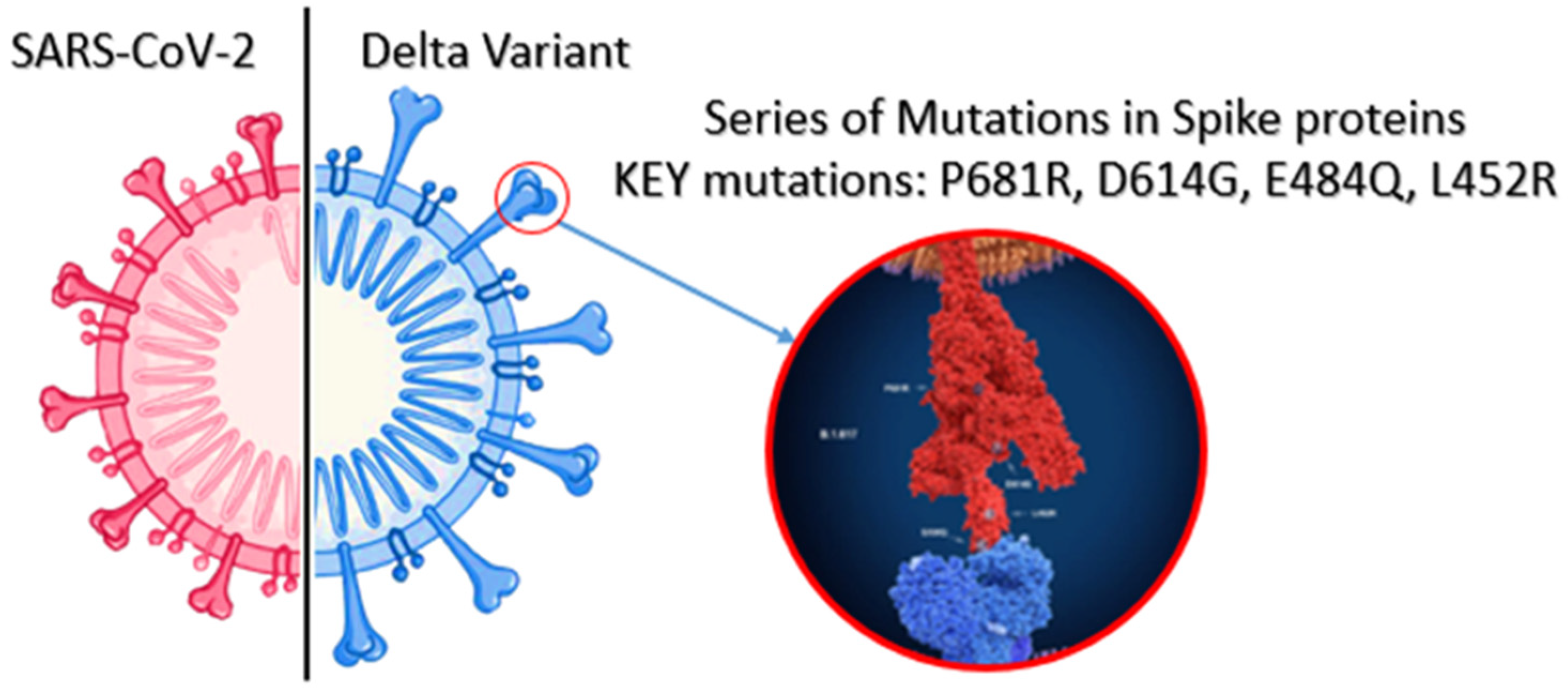
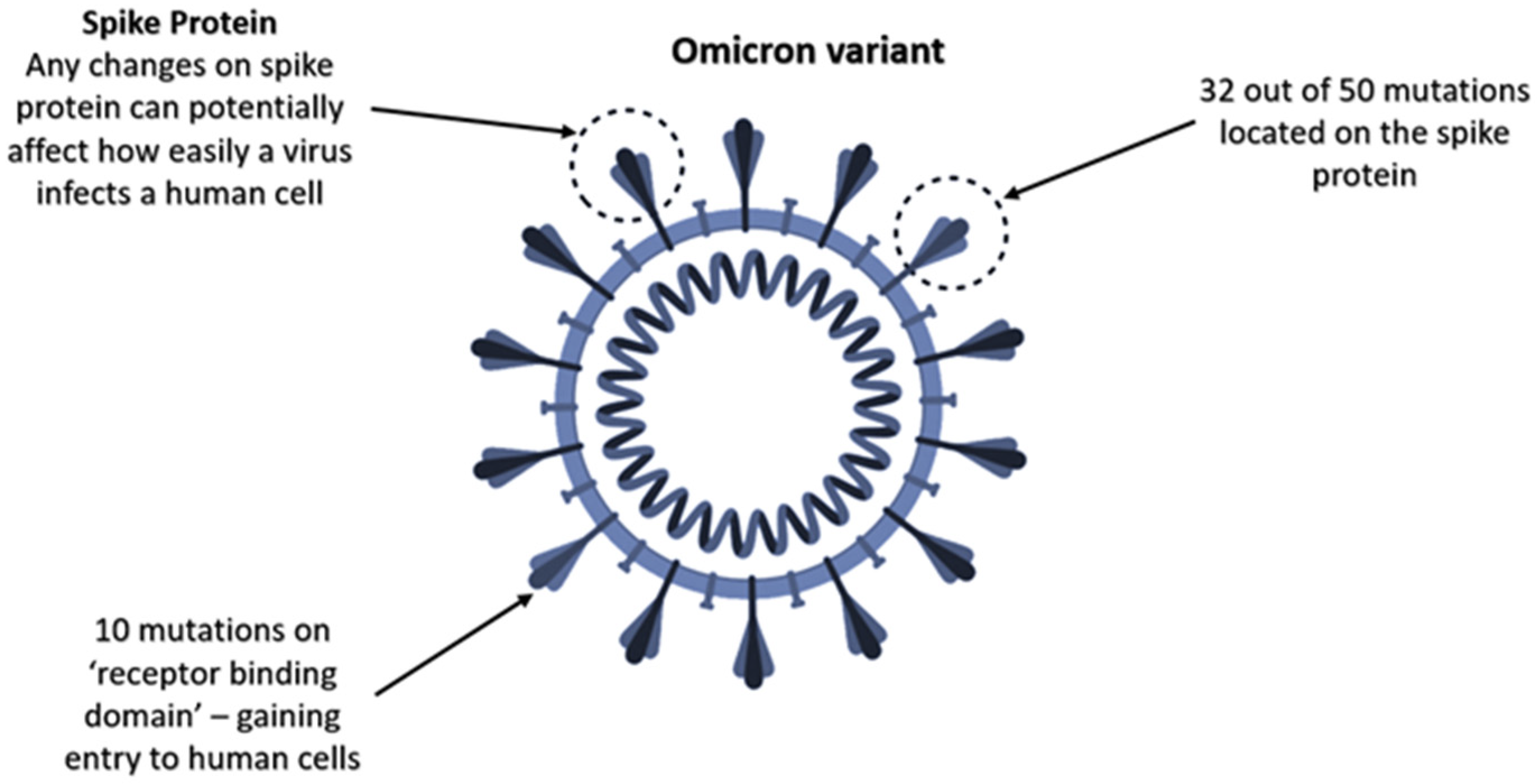
Many countries have been experiencing the global emergence of SARS-CoV-2 (VOCs), predominantly Delta variant, since December 2020. Therefore, several studies have been conducted to analyse the mutated spike variants of SARS-CoV-2 [25,26,27,28]. According to the Centers for Disease Control and Prevention [31], SARS-CoV-2 viruses have constantly been changing over time, and this process is called mutation [57]. Moreover, it normally results in the emergence of new variants. In simple terms, this process can be described as the growth of trees and branches. When the tree grows up, branches also grow up together. Additionally, while some of the branches grow and die off, others may be strong enough to overcome blocks and spread quickly [57]. Similarly, COVID-19 mutates into emerging new variants, and some of the variants pose new mutated characteristics, such as easier binding to human cells, rapid reproduction and resisting antibodies or treatment. When it comes to the Delta variant, it has been determined that it has some significant mutations in the spike protein of the virus structure compared with the original lineages [58,59,60,61,62,63]. In Figure 1, there are some main mutations in the spike proteins of the Delta variant, including E484Q, L452R, P681R and D614G [59]. More importantly, these mutations play a crucial role in making the Delta variant more transmissible. It can be explained by the fact that these mutations can unlock the human cells and even evade natural human immunity. However, due to the recent emergence of the Omicron variant in late 2021, there are limited studies investigating the mutation profile of this variant. Specifically, Venkatakrishnan et al. [52] claim that the Omicron variant possesses up to 26 unique mutations and seven overlapped mutations between the Omicron and Alpha variants after comparing 37 mutations in the Omicron variant to other variants (Figure 2). Furthermore, although variants with a higher number of mutations are not potentially more dangerous, the Omicron variant with 32 out of 50 mutations located on the spike protein is more likely able to affect how easily it infects a human cell.
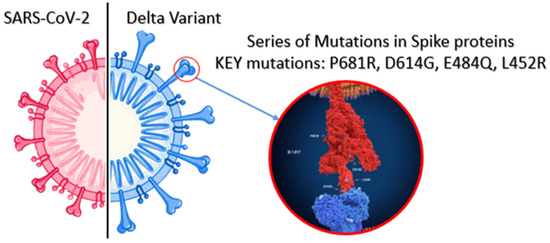
Figure 1.
Comparison structure of SARS-CoV-2 and Delta variant.
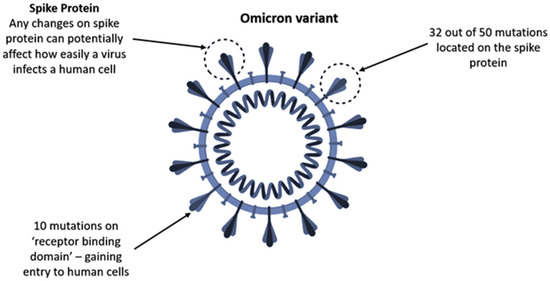
Figure 2.
The new COVID-19 variant: Omicron (B.1.1.529).
2.2. Delta Variant and Omicron Variant Outbreaks
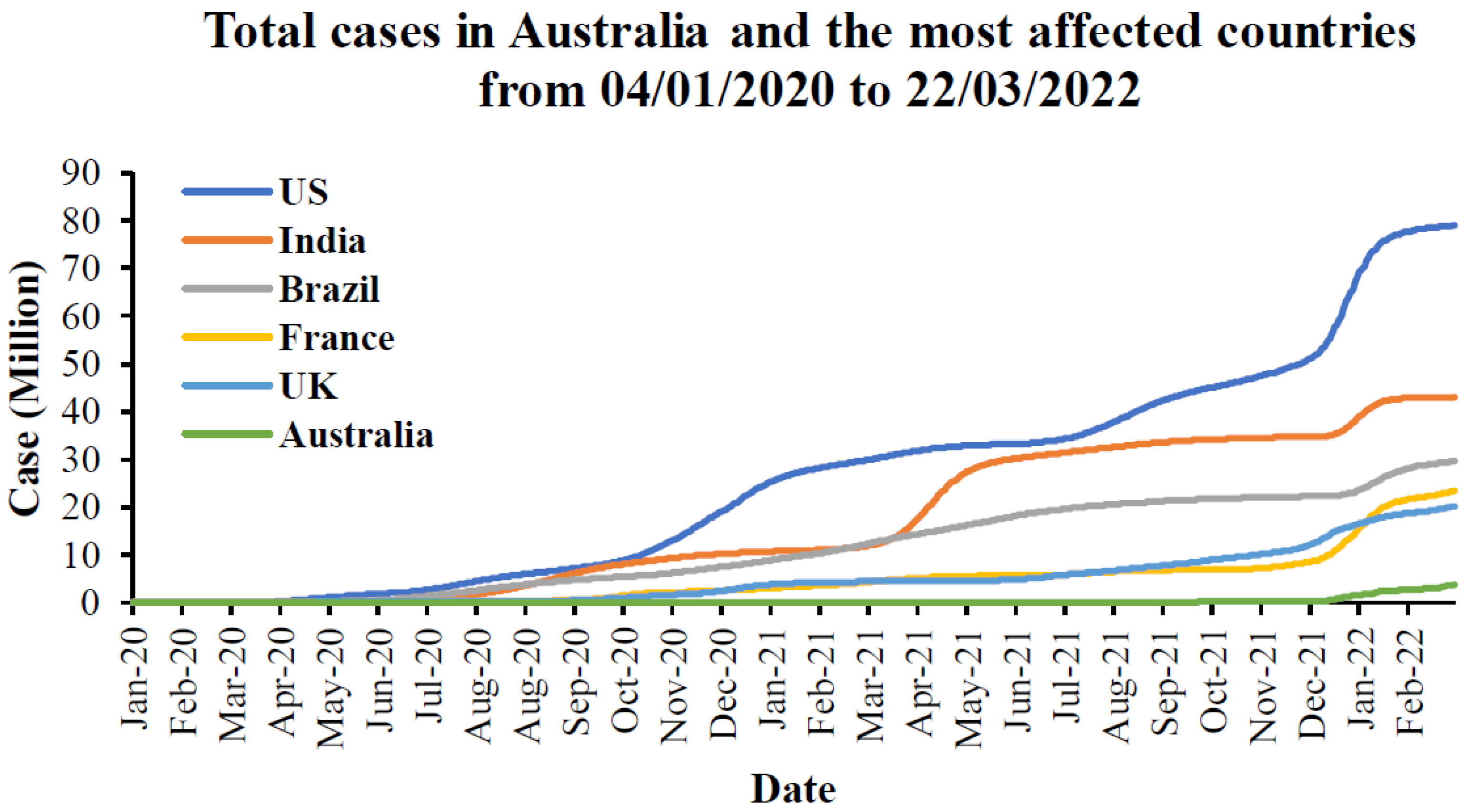
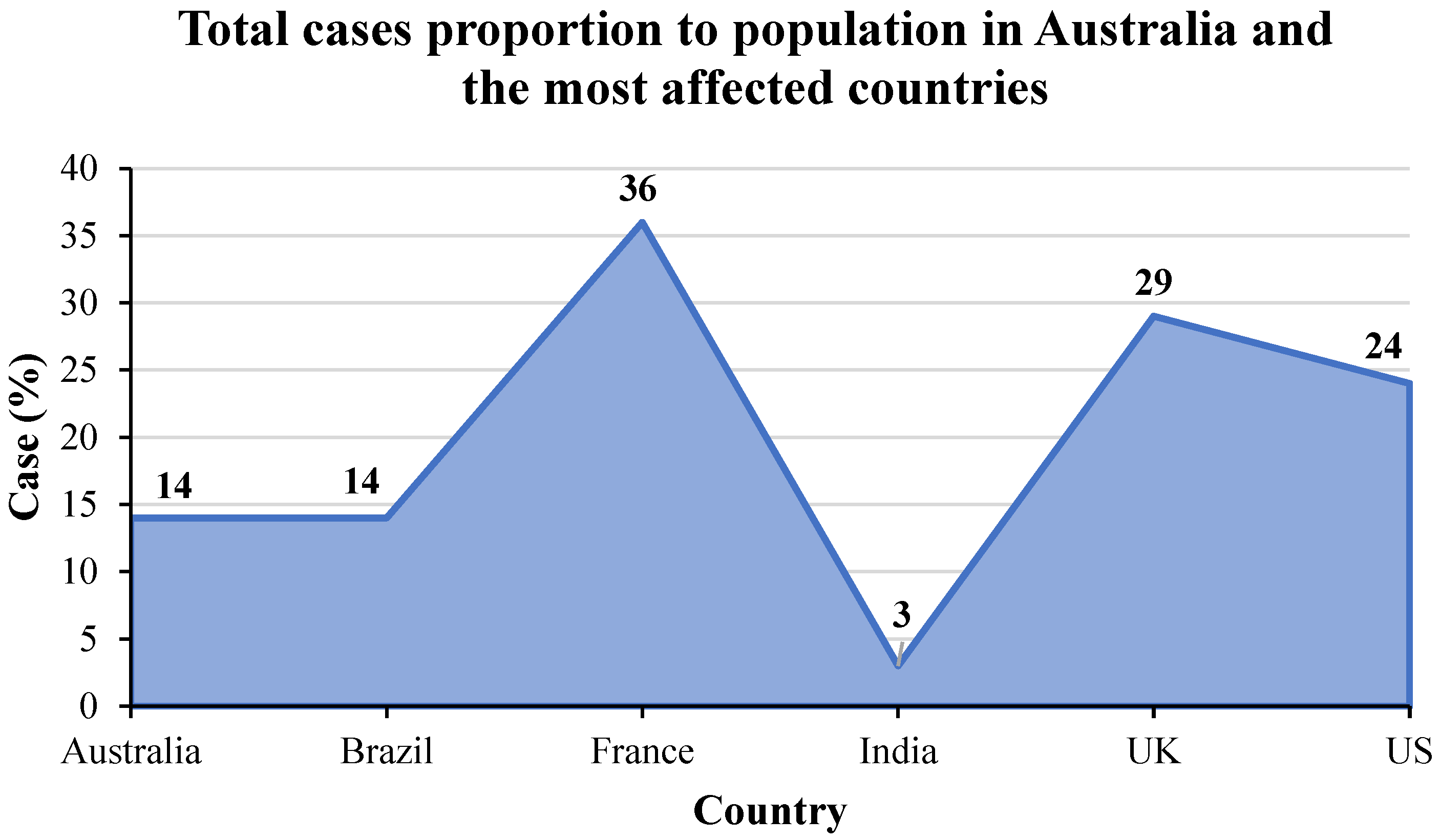
The total cases in Australia and the most affected countries from the first emergence to March 2022 are provided in Figure 3 based on the latest updated data from the WHO [64]. From this Figure, it can be seen that the US is the most affected country by SARS-CoV-2, followed by India, Brazil, France, and the UK, in order. Australia is the least affected country compared to the total cases since the first to recent days. The cumulative cases in the US are approximately 80 million, while there are around 30 to 20 million cases in other countries except for Australia. For Australia, there are around 4 million cases that have been caused by this pandemic. When focusing on the proportion of the total cases to the population in these countries in Figure 4, France is the most affected country followed by the UK and the US, while Brazil and Australia have the proportion of the same cases to population. India has the lowest number of cases compared to other countries.
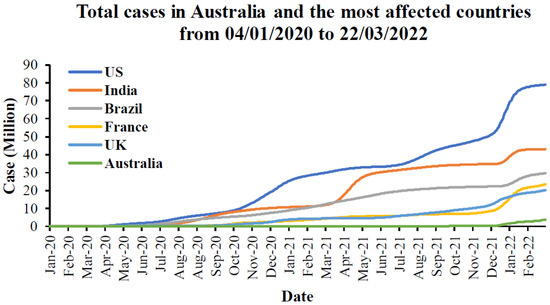
Figure 3.
Total cases in Australia and the most affected countries from 4 January 2020 to 22 March 2022 [64].
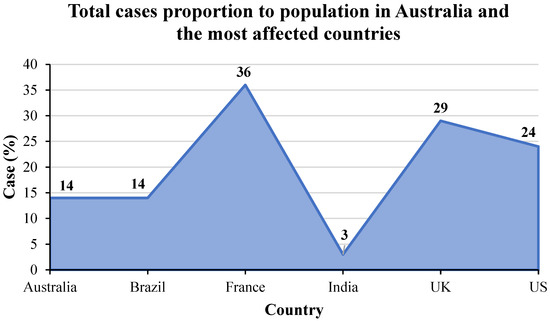
Figure 4.
Total cases in proportion to population in Australia and the most affected countries from the first emergence to March 2022.
Focusing on the Delta variant, it is evident that the infected wave of the coronavirus epidemic is predominantly attributed to the emergence of the Delta variant of SARS-CoV-2 across 98 countries, such as India, the UK, the US and Southeast Asian countries in 2021. The main reason for the rapid spread of the Delta variant is its transmissibility, which is estimated at approximately more than 60% compared with the Alpha variant. Meanwhile, since the first discovery of the Omicron variant in South Africa in November 2021, Omicron has been circulating in over 63 countries, and has become dominant in Australia, the United Kingdom and the United States. Consequently, to control the current spread, it is necessary to understand the transmissibility of the Delta and Omicron variants by analysing recent outbreaks throughout the world [65].
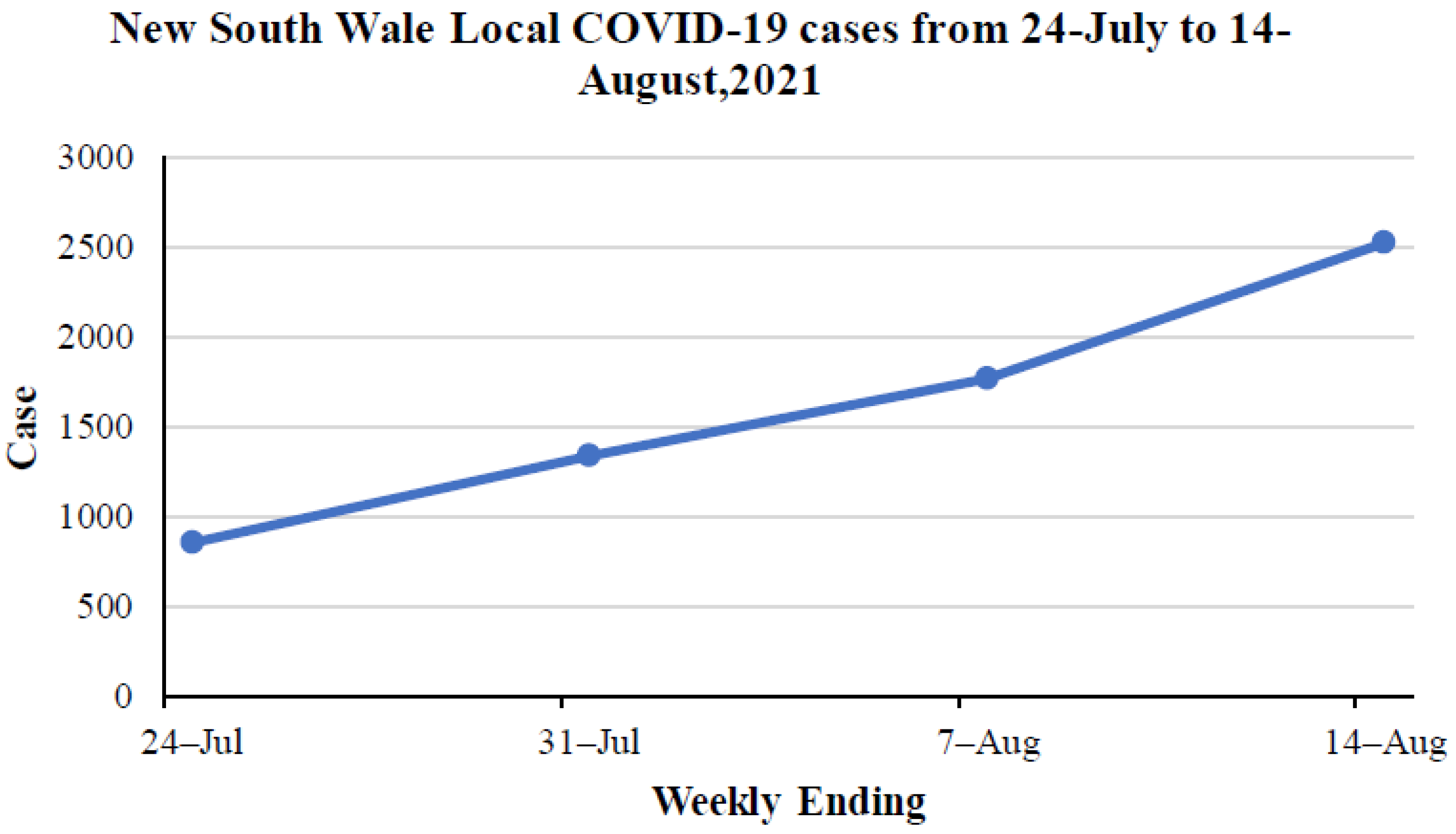
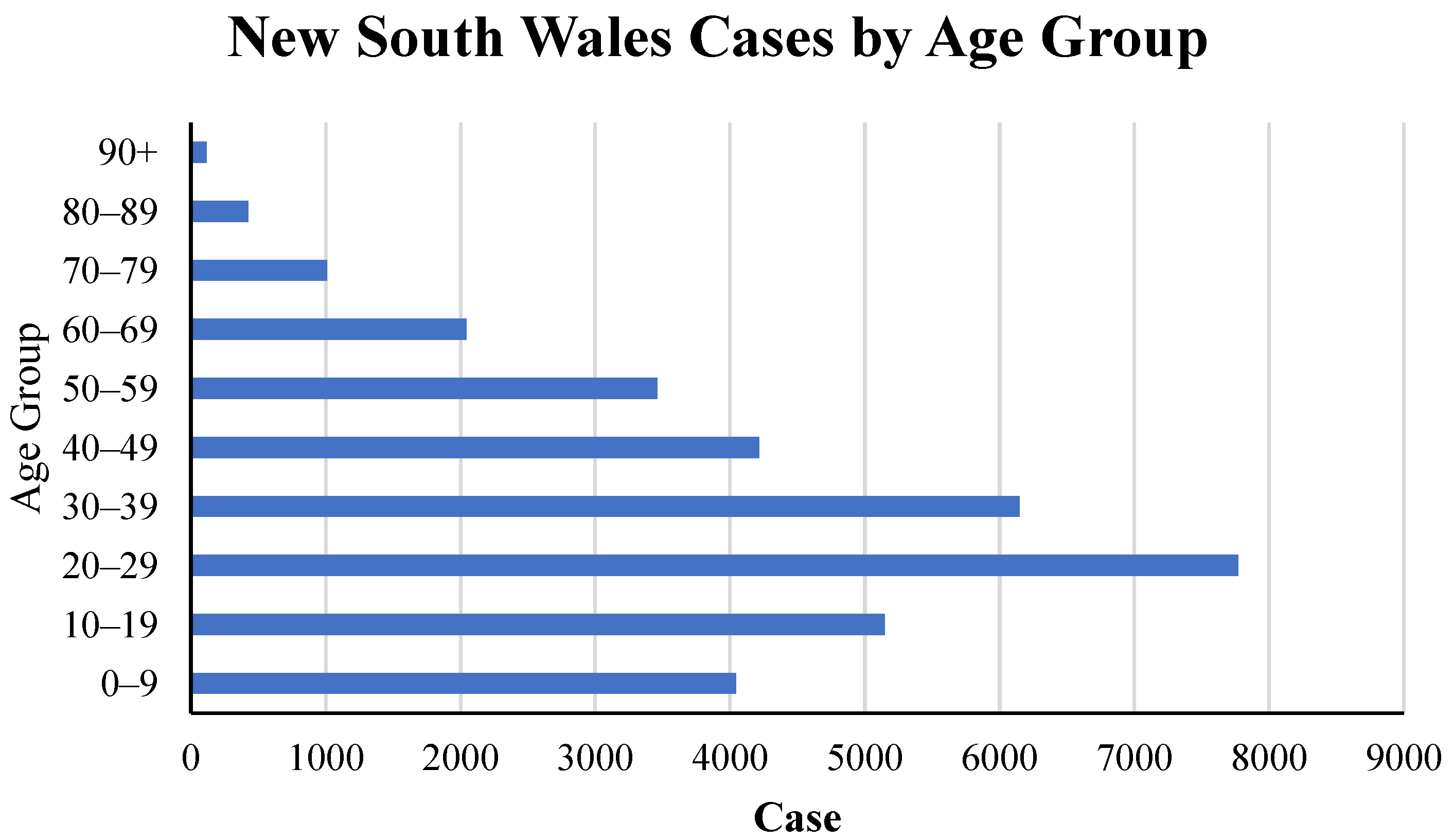
When it comes to Australia, Sydney has been suffering from a wave of Delta variant infections since July 2021. Australia’s latest outbreak was caused by the Delta variant, with the first case detected in Sydney on June 16. The outbreak then quickly spread to other states. According to the recorded data from NSW Health [66], which is the official NSW government website, the specific period was selected and is provided in Figure 5. This figure illustrates that 2521 locally acquired cases have been reported since 14 August 2021. As can be seen from that time, the number of confirmed cases has suddenly increased. In terms of time, the further in time, the more obvious the upward trend is. During the first week (from 24 to 31 July), the number of cases increased to 484, while in the second week (from 31 July to 7 August), the case numbers were 429, and in the third week (from 7 to 14 August), it skyrocketed to 754 cases. From this period, it is obvious to see that the transmission rate is fast. Conversely, in Sydney, during the current Delta infection, the number of cases in young people, with ages involving 10–19, 20–29 and 30–39, account for the highest infections, at approximately 5000, 8000 and 6000, respectively (Figure 6). Similarly, the 0–9 age group also has a great number of cases, which is around 4000 (Figure 6). In simple terms, the higher transmissibility of the Delta variant is demonstrated by the dramatic infections of the younger ages, even in the 0–9 age group, which is certainly believed to be immunized to the original lineage.
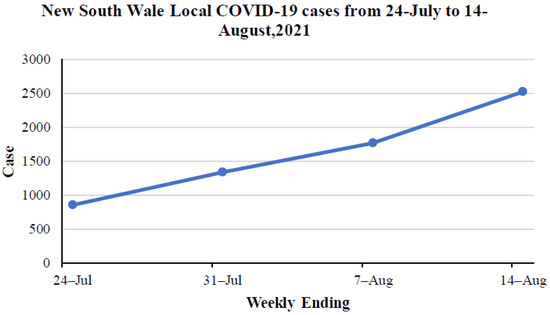
Figure 5.
New South Wales local COVID-19 cases from 7 to 14 August 2021 (accessed 14 August 2021) [66].
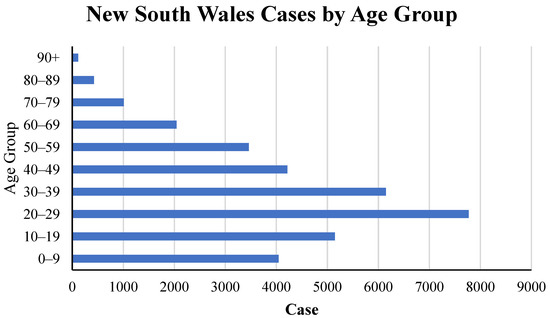
Figure 6.
New South Wales cases by different age groups (accessed 8 September 2021) [66].
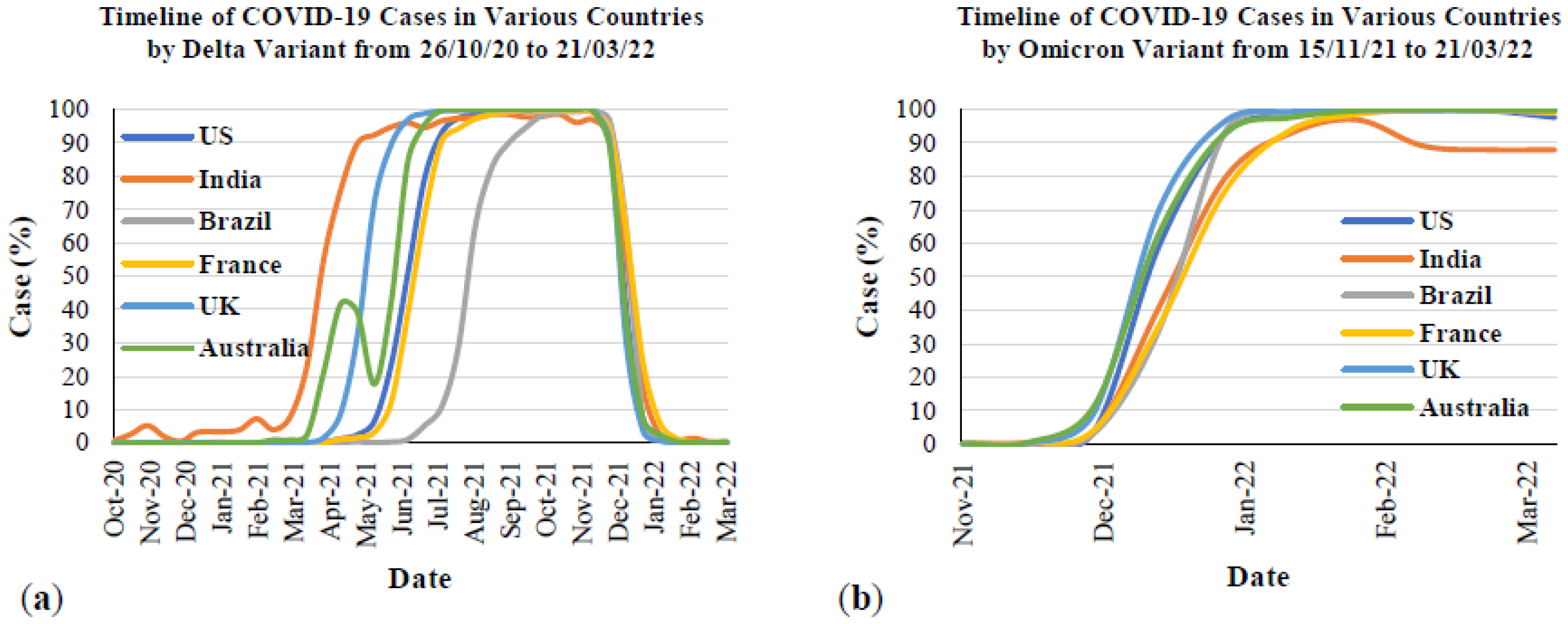
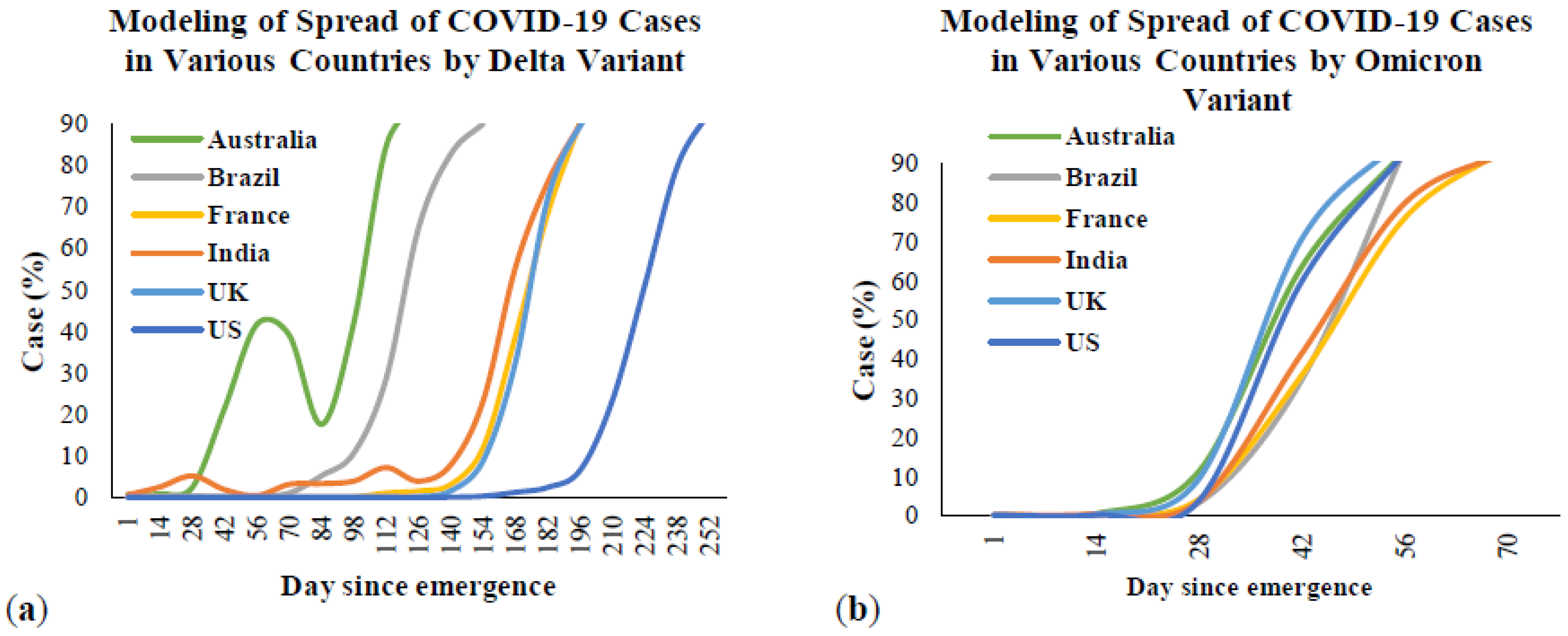
Figure 7 presents the timeline of the Delta and Omicron outbreaks in Australia and the five most affected countries from the first emergence to March 2022. This figure was created based on the timeline for each variant from the beginning until obtaining 100% of the total cases in each country. Figure 7a is the timeline of the Delta variant, and Figure 7b presents the timeline of the Omicron variant. The data from this figure were taken and recreated from Our World in Data [67]. This organization is a collaborative effort between researchers at the University of Oxford and the non-profit organization, Global Change Data Lab. From Figure 7a, the Delta variant was first detected in India in October 2020 and rapidly spread by May 2021. After that, the COVID-19 cases caused by this variant were stable and rapidly decreased by December 2021. Other countries were also affected by the Delta variant in different periods. However, the trends from all countries were similar to India, in that they rapidly increased and remained stable until December 2021. Regarding Figure 7b, COVID-19 cases by the Omicron variant rapidly increased within a month starting from December 2021, which is the end of the COVID-19 cases caused by the Delta variant. More information will be provided in the transmission section. For more analysis, if considering the timeline of COVID-19 cases caused by the Delta variant in all six countries (Figure 7a), it can be seen that the total number of cases (Figure 3) significantly increased, with a 100% case rate of this variant. However, if compared to the timeline of COVID-19 cases by the Omicron variant (Figure 7b), between December 2021 and January 2022, the total cases (Figure 3) rapidly increased in this period, which is the same time as when this variant reached 100% of total cases.
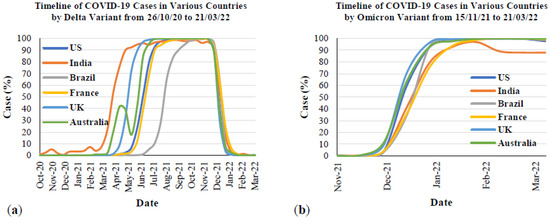
Figure 7.
The timeline of SAR-CoV-2 cases in Australia and the most affected countries from 26 October 2020 to 21 March 2022: (a) Delta variant; (b) Omicron variant.
2.3. Transmission
2.3.1. Respiratory Droplet Transmission
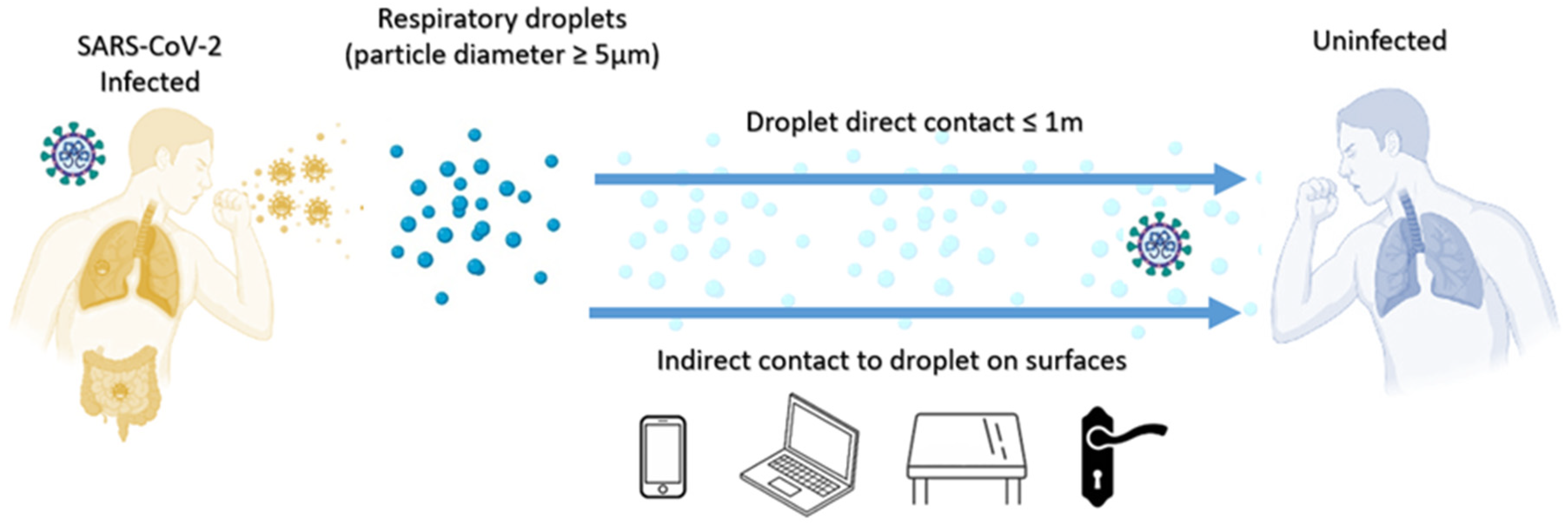
Reports show that the virus can survive on the surface of respiratory droplets, secretions, and contaminated bodies for a while. When a patient coughs or expects sputum, the droplets usually contain many viruses, which can stay on the surface for a while, such as elevator buttons, stair handrails, or the surface of express parcels (Figure 8). When healthy people touch these contaminated objects, if they do not wash their hands properly and touch their eyes, nose, and mouth, they will be infected. For example, someone who touched the surface of an object touched by a confirmed patient with his hand would then be infected with the virus when touching his mouth, eyes, or nose. When people sneeze, cough or even talk, the virus they carry can infect people who are in close contact with them. It is easier for air to flow in outdoor spaces, and it is difficult for outdoor spaces to form air circulation. These minimize the theoretical risk of aerosol transmission through smaller respiratory droplets. Outdoor spaces usually allow for more physical distances, thus reducing the risk of transmission of the virus through large respiratory droplets [68]. The main way humans are infected with the Delta variant is through contact with respiratory fluids that carry infectious viruses. The risk of spreading the SARS-CoV-2 Delta variant in an outdoor environment is low [69].
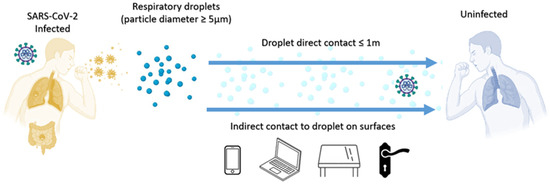
Figure 8.
Delta variant droplet transmission.
2.3.2. Transmission by Exposure to Contaminants
The Delta variant can be spread through objects. In patients infected with the Delta variant, the virus appears earlier in the body, the amount of virus is higher, and the amount of virus is higher than the original new coronavirus. The virus remains positive in the patient’s body for a longer time than the original virus strain [70]. Therefore, all these factors can greatly increase the speed of the Delta virus spreading through surfaces.
2.3.3. Airborne or Aerosol Transmission
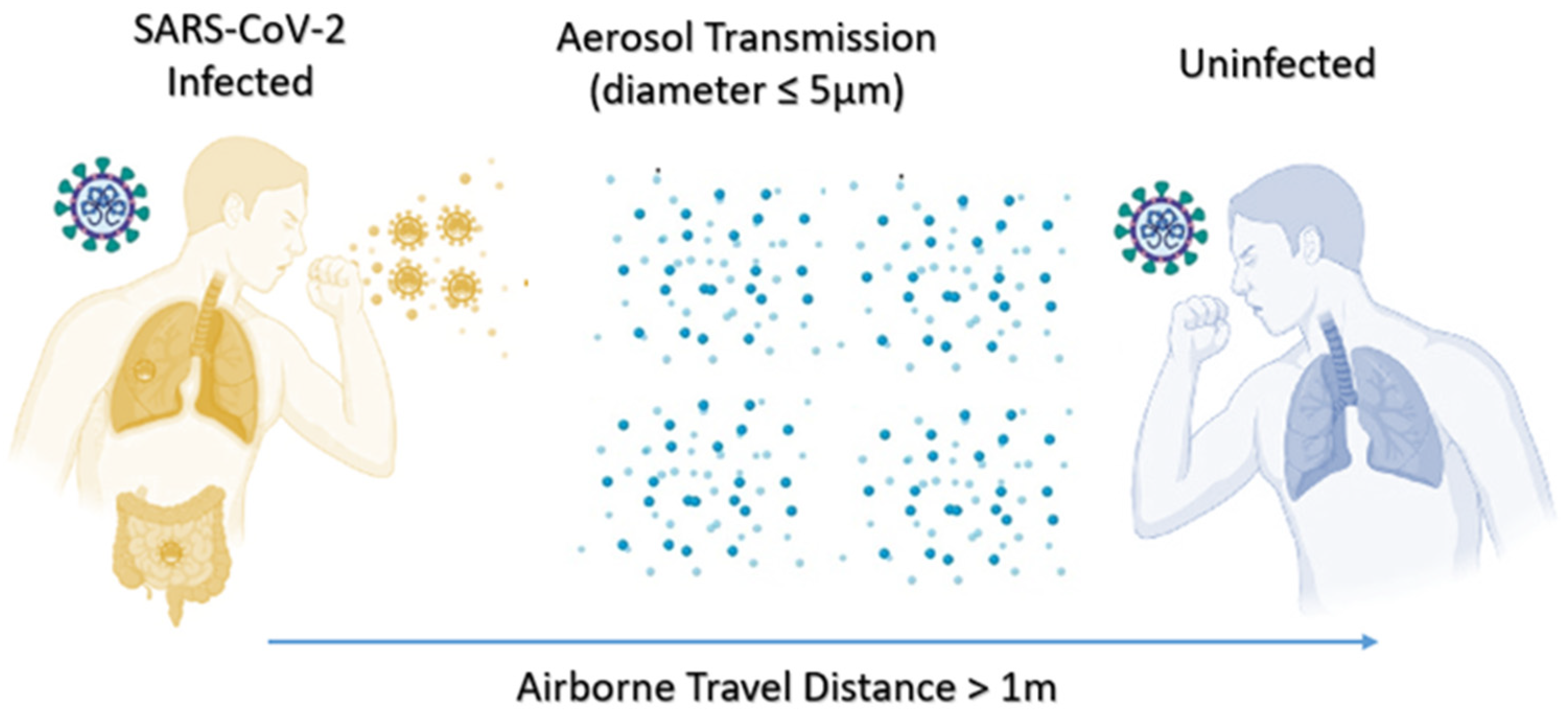
Airborne transmission is also called “aerosol transmission”. People should pay special attention, especially indoors, in closed and unventilated narrow spaces [71]. If an infected person coughs or sneezes, small respiratory secretion particles will form (Figure 9). These particles can be suspended in the air. Inhalation can cause infection. Although the transmission of aerosols in the community environment is controversial, new data show that indoor circulating air can transmit SARS-CoV-2, for example: an incident of spreading at an indoor choir practice in Washington State, USA [72], a meat processing plant in the US [73], and a nursing home in the Netherlands [74]. In low-ventilated areas, the atomized droplets can stay suspended longer before being inhaled or falling onto a surface, which may lead to the spread of contaminants. In a closed environment, low humidity, air conditioning, and low ultraviolet light may all help the virus particles survive longer [68]. Especially for the ventilation of small indoor spaces, if someone coughs or sneezes, small particles of respiratory secretions can be formed and suspended in the air. Conversely, it may cause infection or even remove the virus and leave the space. The virus in the air still exists for a certain time, causing other people to be infected. The proven effective anti-SARS-CoV-2-Delta transmission strategy also includes diluting the air through maximize ventilation and filtration [69].
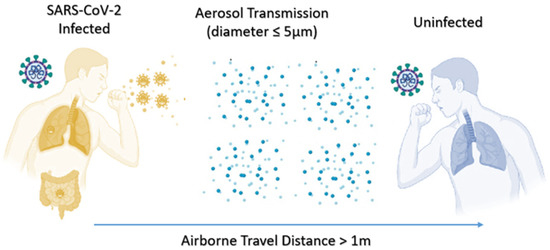
Figure 9.
Delta variant aerosol transmission.
2.3.4. Animal to Human
The spread of the virus depends on the host, and the infection of the virus to the host is selective. Viruses are classified into plant viruses, animal viruses and bacterial viruses according to the organisms they live in. Viruses that live exclusively in plant cells are called plant viruses, such as tobacco mosaic virus; viruses that live in animal and human cells are called animal viruses, such as influenza viruses and coronaviruses; viruses that specialize in bacteria are called bacteria viruses (also called bacteriophages), such as caliphates. In other words, a virus cannot infect every species. It depends on whether the virus can complete one generation in that species to produce a new generation of viruses. The virus itself has only a long string of nucleic acids and a protein shell. To complete the replication, transcription and translation of its genetic information, it must be carried out in the host cell, which requires the host cell to provide the material and energy it needs. Otherwise, the virus cannot complete replication and will not be able to infect.
In order to infect the host, the virus first needs to be able to bind to the host cell’s receptors such that it can use the host cell’s material and energy to synthesize its material. However, this is not always easy. Generally speaking, the closer the related species are, the more likely they are to combine, while the further the species are, the less likely it is to be infected. This is why plant viruses generally cannot infect animals.
2.3.5. Human Behaviours—Sneezing without Wearing a Mask
Because the Delta virus load is high and the spread speed is fast, and the Delta virus can be spread through pollutants and air, droplets from sneezing, coughing and even talking may carry the virus and infect people who are in close contact with the virus [75]. Thus, when people do not wear masks and are in the same small, confined space as the confirmed patient, they are susceptible to transmission. The proven effective anti-SARS-CoV-2 Delta transmission strategy always includes the correct use of masks [68]. The CDC recommends that the community uses multilayer cloth masks or non-medical disposable masks. When it is not possible to maintain a physical distance of ≥6 feet, it is vital to use masks in indoor spaces and outdoors. In the family, masks should be used when family members are infected or have recent potential SARS-CoV-2 -Delta exposure (for example, known close contact or potential exposure related to occupations, crowded public places, travel, or non-family members) [70].
2.4. The Difference in Transmissibility between the Delta Variant and Omicron Variant
Alpha (B.1.1.7): the first variant of attention described in the UK in late December 2020. Beta (B.1.351): first reported in South Africa in December 2020. Gamma (P.1): first reported in Brazil in early January 2021. Delta (B.1.617.2): first reported in India in December 2020. Among these variants, symptoms of the Delta variant in infected patients may be slightly different. For example, headache, fever, sore throat and runny nose are common, but cough and loss of smell are not. Hearing loss is one of the new symptoms noticed among Delta variant patients [76].
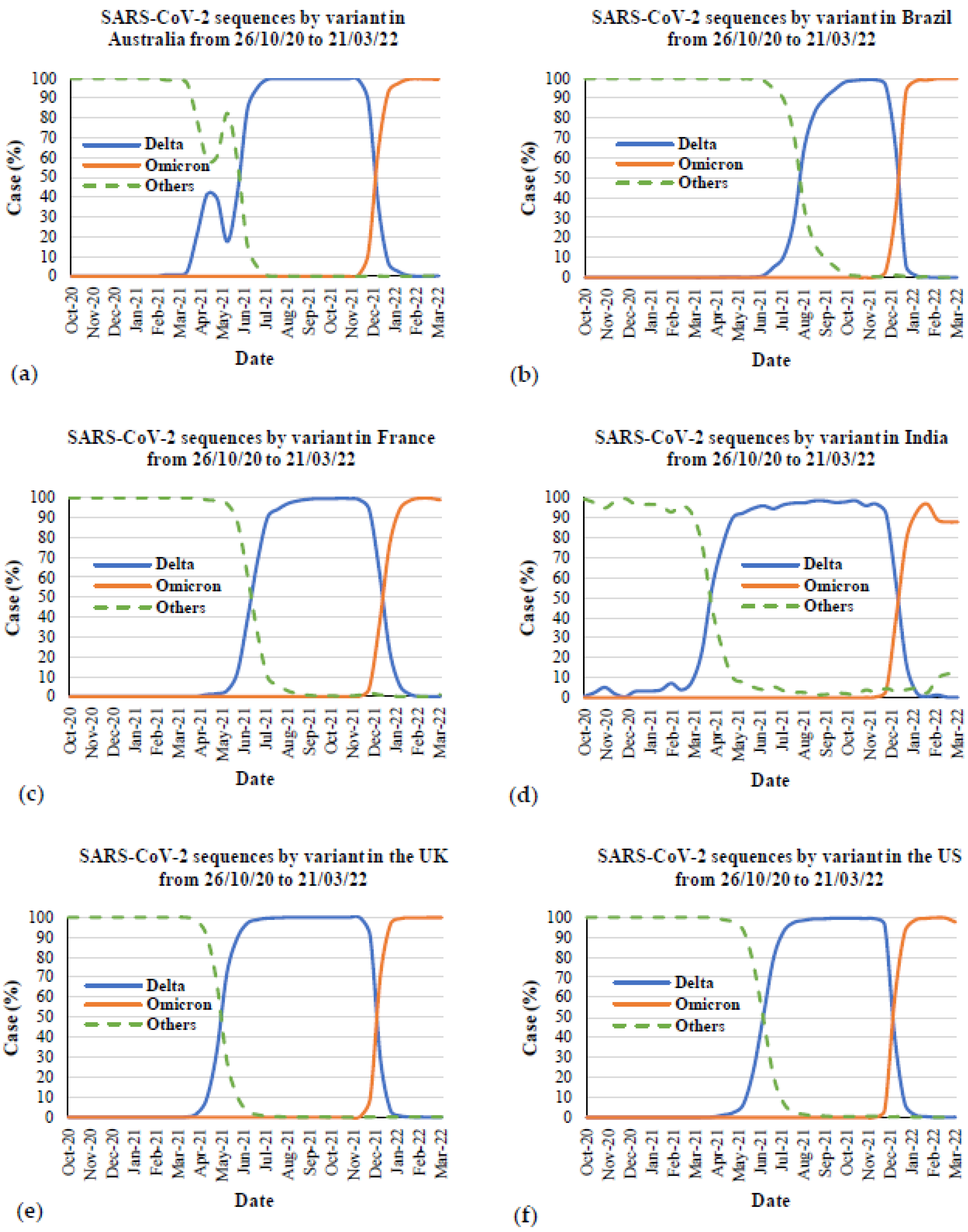
Figure 10 presents the comparison between the Delta and Omicron variants in the most affected countries and Australia. Figure 11 presents the SARS-CoV-2 sequences by the Delta, Omicron and other variants in Australia and the five most affected countries from the first emergence in October to March 2022. The data for all countries were also taken from Our World in Data [67]. The first emergence case from the Delta variant was in October 2020 in India and November 2021 for the Omicron variant in South Africa. From this Figure, it is evident that the Delta and Omicron variants are the main causes of COVID-19 since the first emergence of these two variants. From the COVID-19 cases due to the Delta variant, it took over three months in all countries to reach 100% of cases caused by this variant since first emergence. After that, this variant remained stable at 100% of COVID-19 cases from all countries and rapidly decreased since November 2021. In contrast, COVID-19 cases due to the Omicron variant rapidly increased between December 2021 and January 2022. Focusing on the peak of the Delta outbreak with 80% to 100% cases in total, the peak outbreak in Australia (Figure 11a) was between June and December 2021, whereas in Brazil (Figure 11b), it was between September and December 2021. The peak outbreaks in France (Figure 11c), India (Figure 11d), and the US (Figure 11f) were between July and December 2021. For the peak outbreak in the UK (Figure 11e), it was from May to December 2021. From the meta-data, it can be seen that the beginning time of the peak outbreak is different in Australia, Brazil, and the UK, whereas the beginning of the peak outbreak in other countries is the same month of July 2021. This could be because of the different first emergences in each country. However, the end of the peak outbreak from Delta was found to be during the same month in December 2021, which was the same time as the rapid increase of cases by the Omicron variant. Focusing on the cases by the Omicron variant after reaching 100% cases in total, the trend of 100% cases was likely stable in all countries except for India. There were around 88% cases caused by the Omicron variant from February to March 2022, while fewer cases were caused by other variants (Figure 11d).
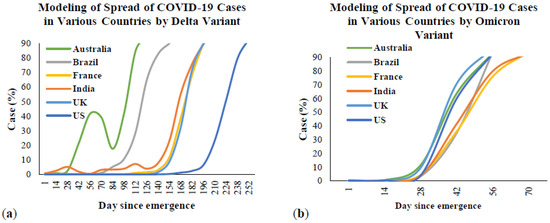
Figure 10.
Comparison between Delta and Omicron outbreaks in the most affected countries and Australia: (a) cases by Delta variant; (b) cases by Omicron variant.
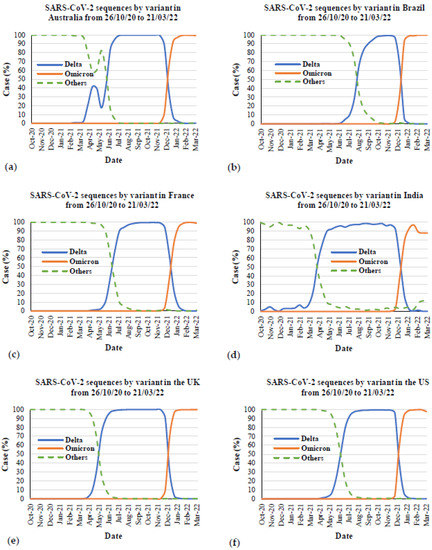
Figure 11.
SARS-CoV-2 sequences by variant in Australia and the most affected countries from 26 October 2020 to 21 March 2022: (a) Australia, (b) Brazil, (c) France, (d) India, (e) the UK, and (f) the US.
2.5. Severity and Mortality
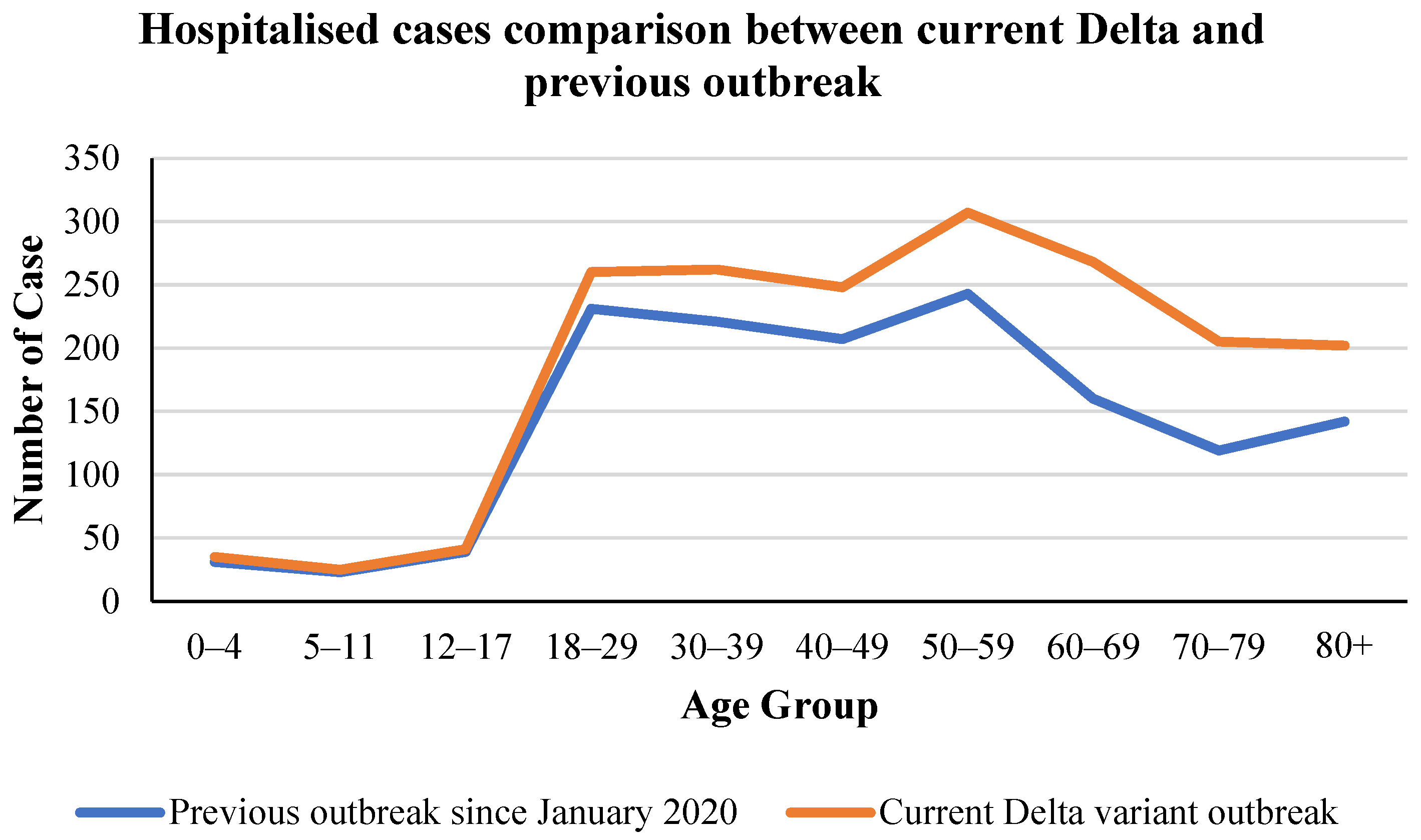
It is demonstrated in the previous section that the Delta variant was the most transmissible and has recently become the most concerning strain of COVID-19 in many countries around the world [77,78,79,80,81]. However, another question needed to be clarified: how severe and fatal is the Delta variant among infected patients. Several studies have suggested that the Delta variant can cause more severe health impacts on infected people in relation to severity and fatality. First, a study in the US stated that the Delta variant is deadlier than other variants [65]. Higher viral loads mean that different people can be infected in the same space, all in close contact, making it harder to control. Faster means the virus has a shorter disease incubation period, a shorter transmission time, and a faster transmission rate. The incubation period decreased from 5.9 days to 3.2 days on average. The interval between infection and infecting another person was even shorter, about two days on average. In addition, the study also showed that approximately 80% of COVID-19 Delta deaths occurred in patients over 65 years old [82]. For COVID-19 patients of any age, having underlying health conditions and underlying diseases also increased the risk of serious illness or death [70]. Apart from this, a British survey asserted that the death rate seemed to increase exponentially with age; men, obesity, socio-economic poverty, and many comorbidities are also associated with higher risks [83]. Furthermore, Sheikh et al. [42] conducted a cohort study in Scotland to compare the hospitalization rate between Alpha- and Delta-infected people. They claim that the Delta variant was 85% greater than the Alpha variant in hospitalization rate [42]. This is supported by Figure 12, showing the comparison between hospitalized cases of the previous outbreak since January 2020 and the current Delta variant outbreak within different age groups in Australia. In Figure 12, there is no difference between the age groups of 0–4, 5–11 and 12–17 hospitalized cases. However, for the groups from 18 to 80+ ages, the number of hospitalized cases in the Delta variant outbreak is higher than in the previous outbreak, at approximately 20%.
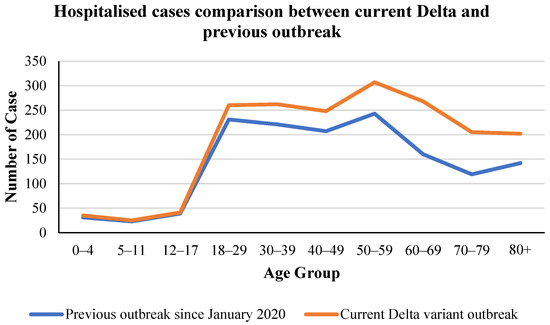
Figure 12.
Hospitalized cases comparison by age group between the current Delta and previous outbreaks in Australia [66].
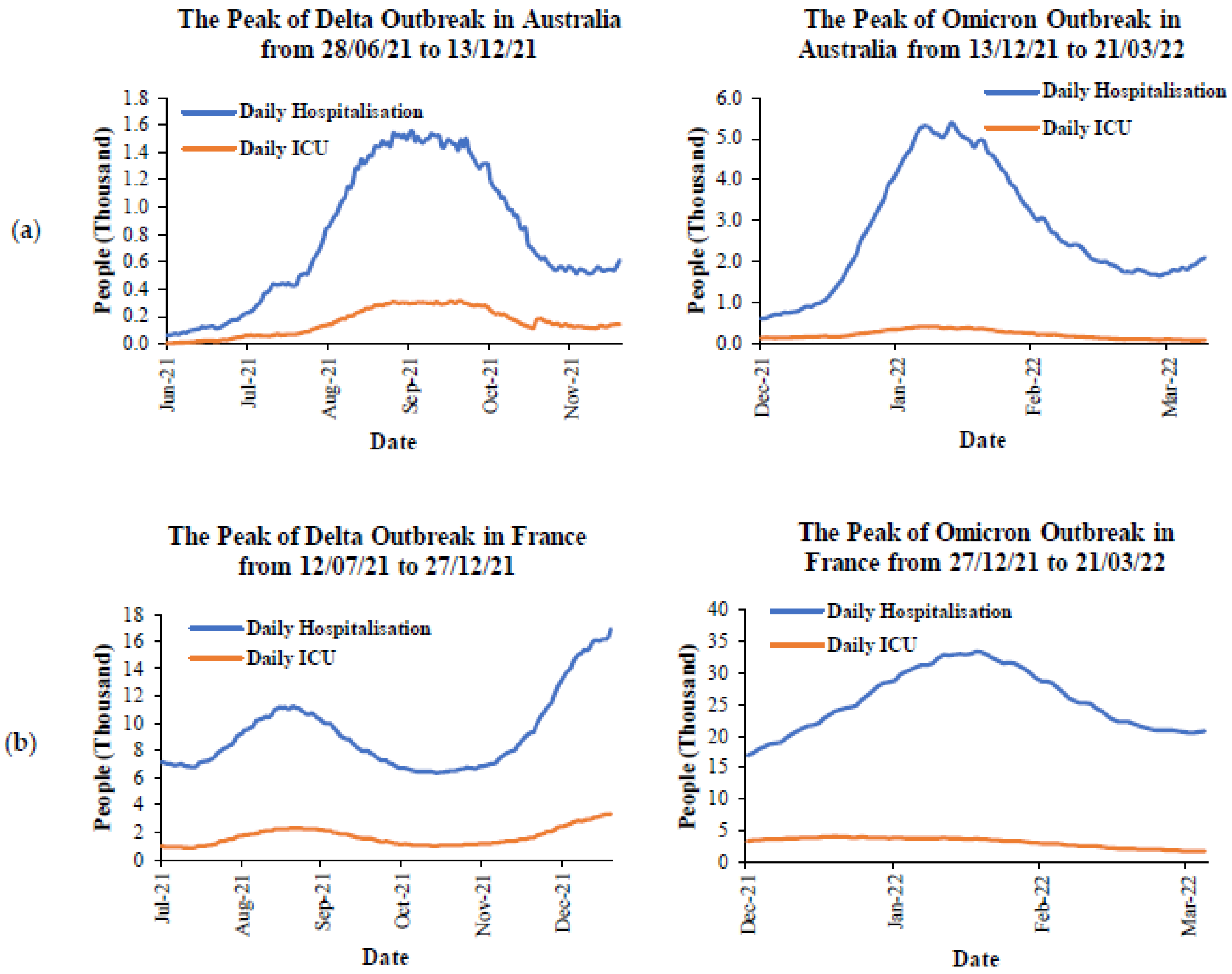
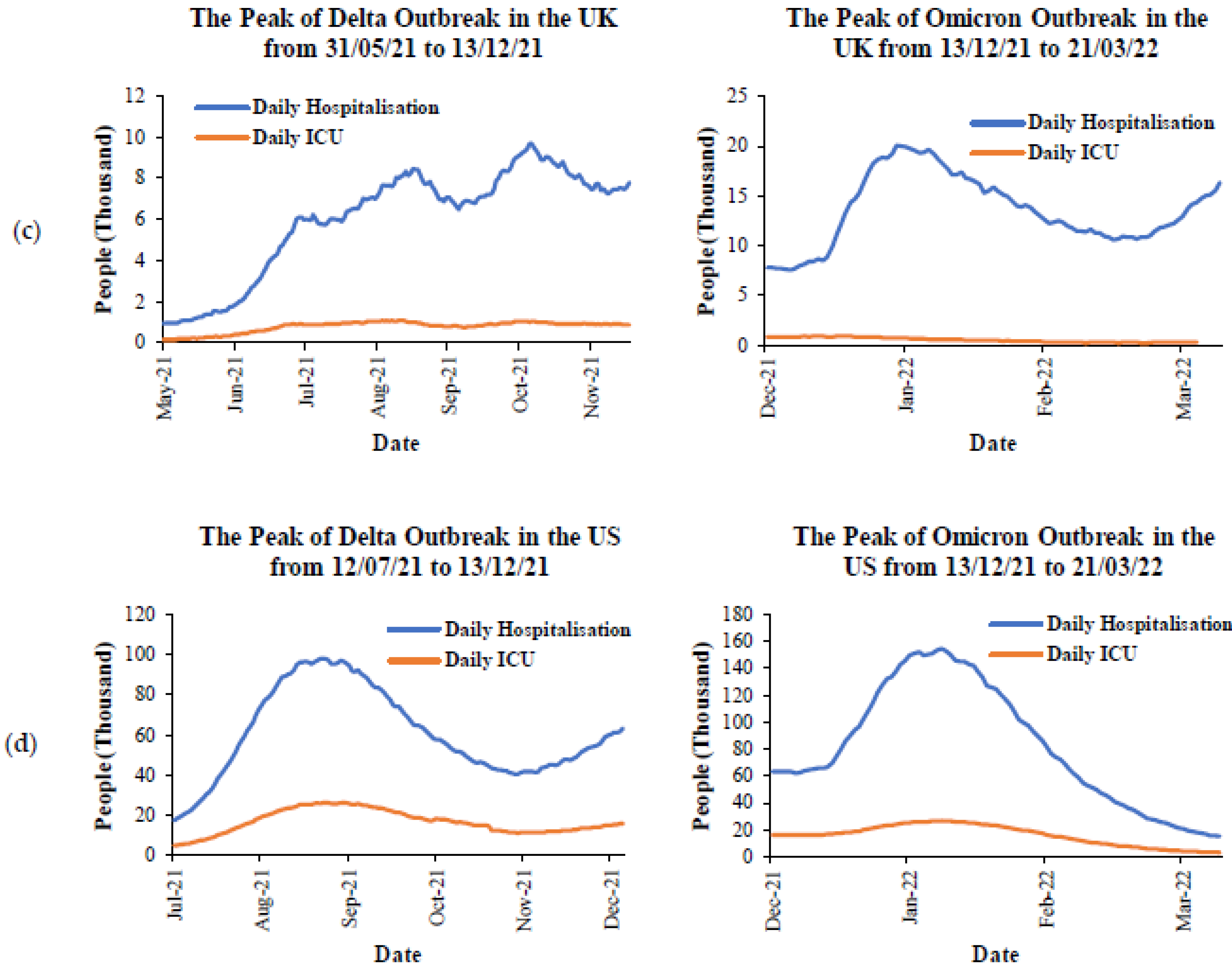
To understand the impact of the Delta and Omicron variants on severity, the peak of the Delta and Omicron outbreaks in each country from Figure 11 are selected by focusing on the range between 80% to 100% cases in total for each variant. Figure 13 presents the daily cases of hospitalization and ICU during the peak of the Delta and Omicron outbreaks in Australia and the five most affected countries. The data for daily hospitalization and ICU cases were taken from the government websites in each country [66,83,84,85]. During the peak outbreak of the Delta variant in Australia (Figure 13a), there were less than 200 people minimum and around 1400 people maximum for daily hospitalization. For ICU cases, there were around 200 people maximum for daily ICU rates. However, when compared to the peak outbreak of the Omicron variant, there were around 5000 people maximum and less than 100 people minimum of daily hospitalizations. It can be seen that the maximum daily hospitalization during the peak of the Omicron outbreak was significantly higher than during the Delta outbreak at three instances. For the daily ICU cases, the maximum number of cases due to the Omicron outbreak was less than 500 cases, but it was still higher than the maximum number of cases due to the Delta outbreak around one time. In terms of France (Figure 13b), the maximum and minimum daily hospitalization rates during the peak outbreak due to the Omicron variant were found to be around one time higher than the cases by the Delta variant. For the daily ICU cases, the maximum number of cases during the Omicron outbreak was found to be higher than the cases during the peak Delta outbreak, with around 600 people, which is less than one time. Similarly, the daily hospitalization cases during the peak outbreak from the Omicron variant in the UK (Figure 13c) and the US (Figure 13d) were observed to be around one-time higher than the cases during the peak outbreak from the Delta variant. These were observed for both minimum and maximum daily cases. However, the maximum daily ICU cases during the peak outbreak from these variants were similar. Furthermore, the trend of daily ICU cases was found to be reduced in all countries. In contrast, the trend line of daily hospitalization cases was found to have fluctuated for all countries except for the US, which was reduced. To summarize, the Omicron variant significantly affected the daily cases of hospitalization, and it was around one to three times the daily cases from the Delta variant. However, the Omicron variant had less effect on the daily ICU cases. This was probably due to the total number of vaccinated people in each country. The discussion of this factor is provided in the Prevention section.
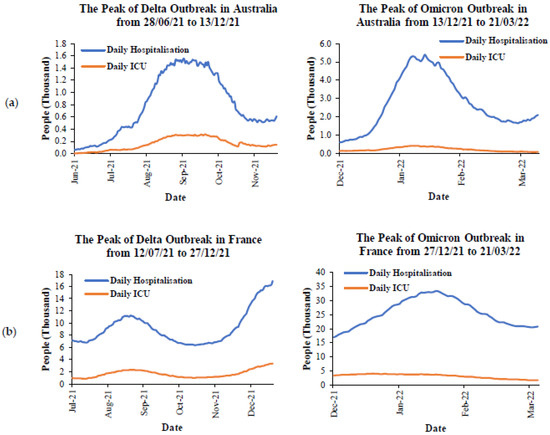
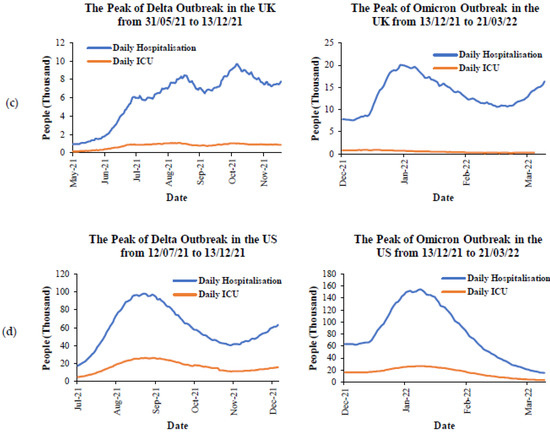
Figure 13.
The comparison of severity during the peaks of Delta and Omicron outbreaks in: (a) Australia, (b) France, (c) the UK, and (d) the US.
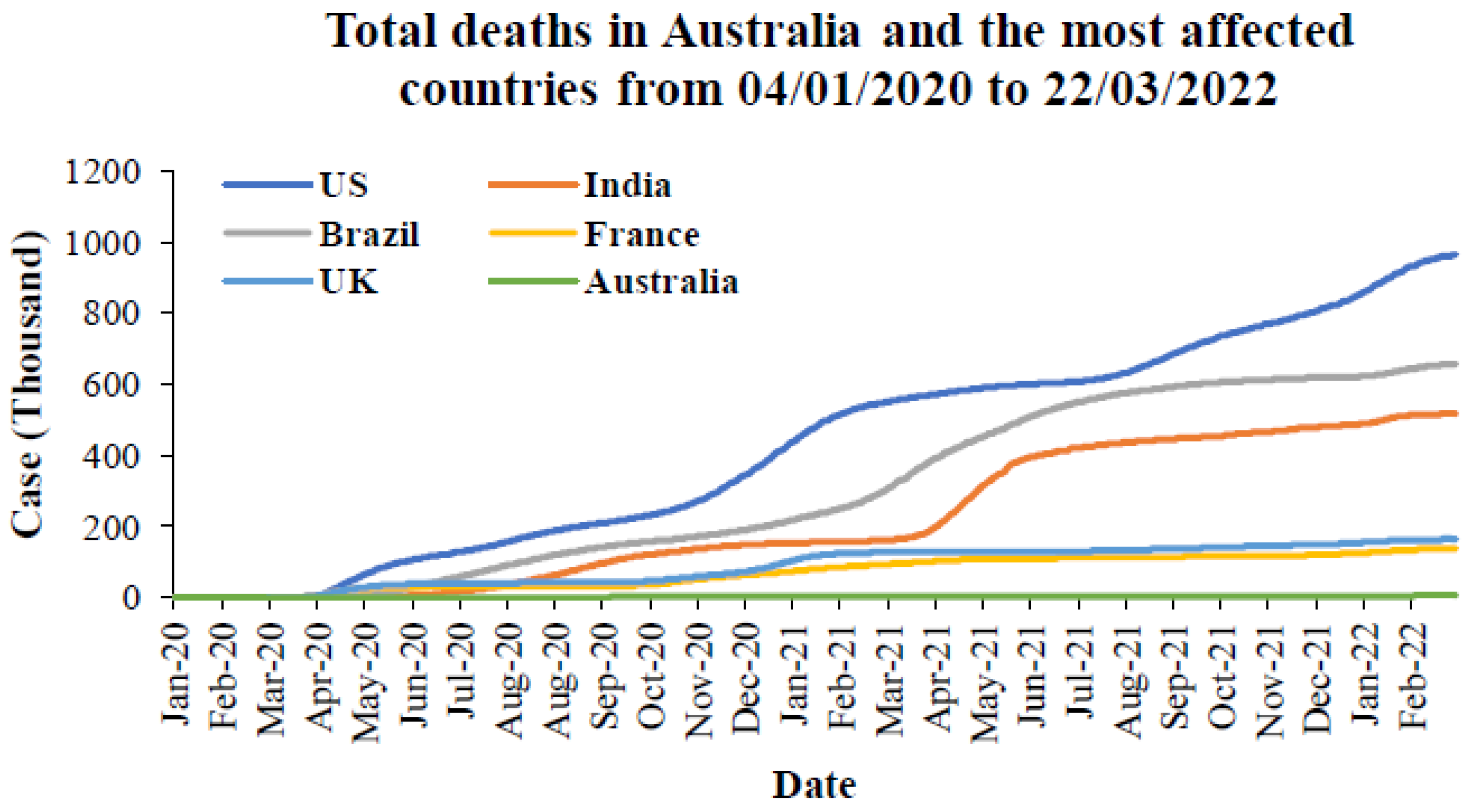
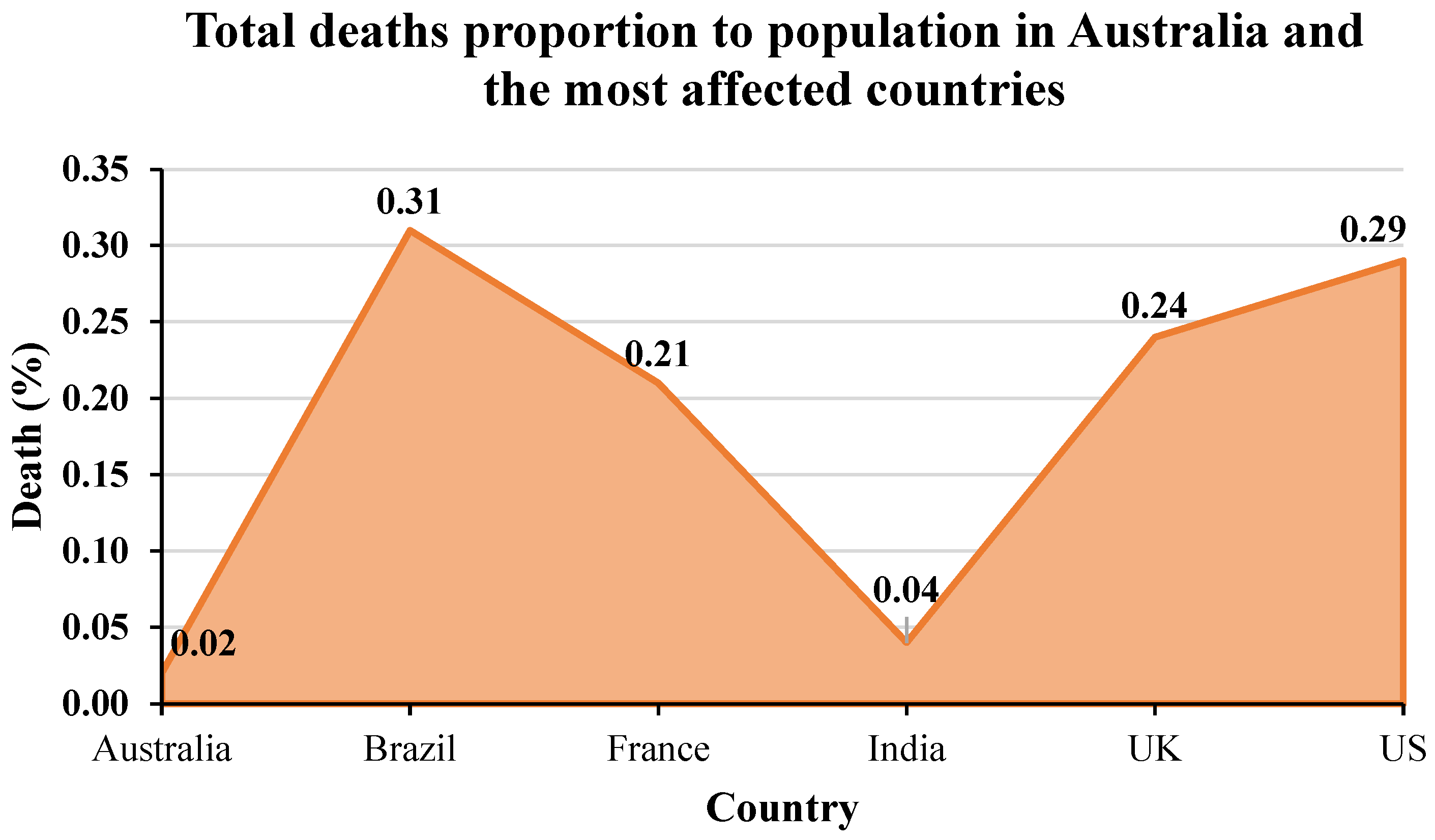
To understand the mortality caused by the COVID-19 pandemic, the total deaths in Australia and the most affected countries from the first emergence to March 2022 are provided in Figure 14. The meta-data from this figure were taken from the WHO [64]. From this figure, it can be seen that the US has the highest number of deaths followed by Brazil, India, the UK, and France. When comparing the total cases in Figure 3, India has higher cumulative cases than Brazil, followed by France. Australia has fewer deaths compared to the five most affected countries. However, when considering the proportion of the population in Figure 15, Brazil has the highest number of deaths, followed by the US, UK, and France. India and Australia have similar deaths in terms of the proportion of populations.
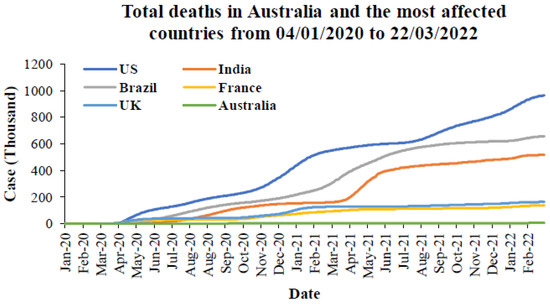
Figure 14.
Total deaths in Australia and the most affected countries from 4 January 2020 to 22 March 2022 [64].
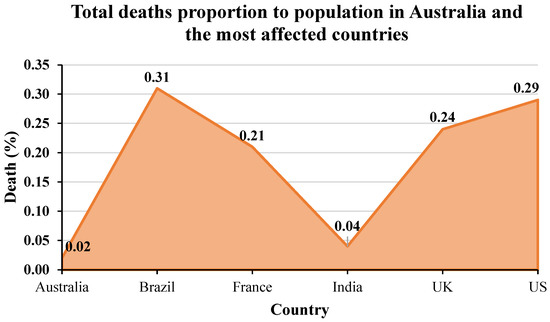
Figure 15.
Total deaths proportion to population in Australia and the most affected countries from the first emergence to March 2022.
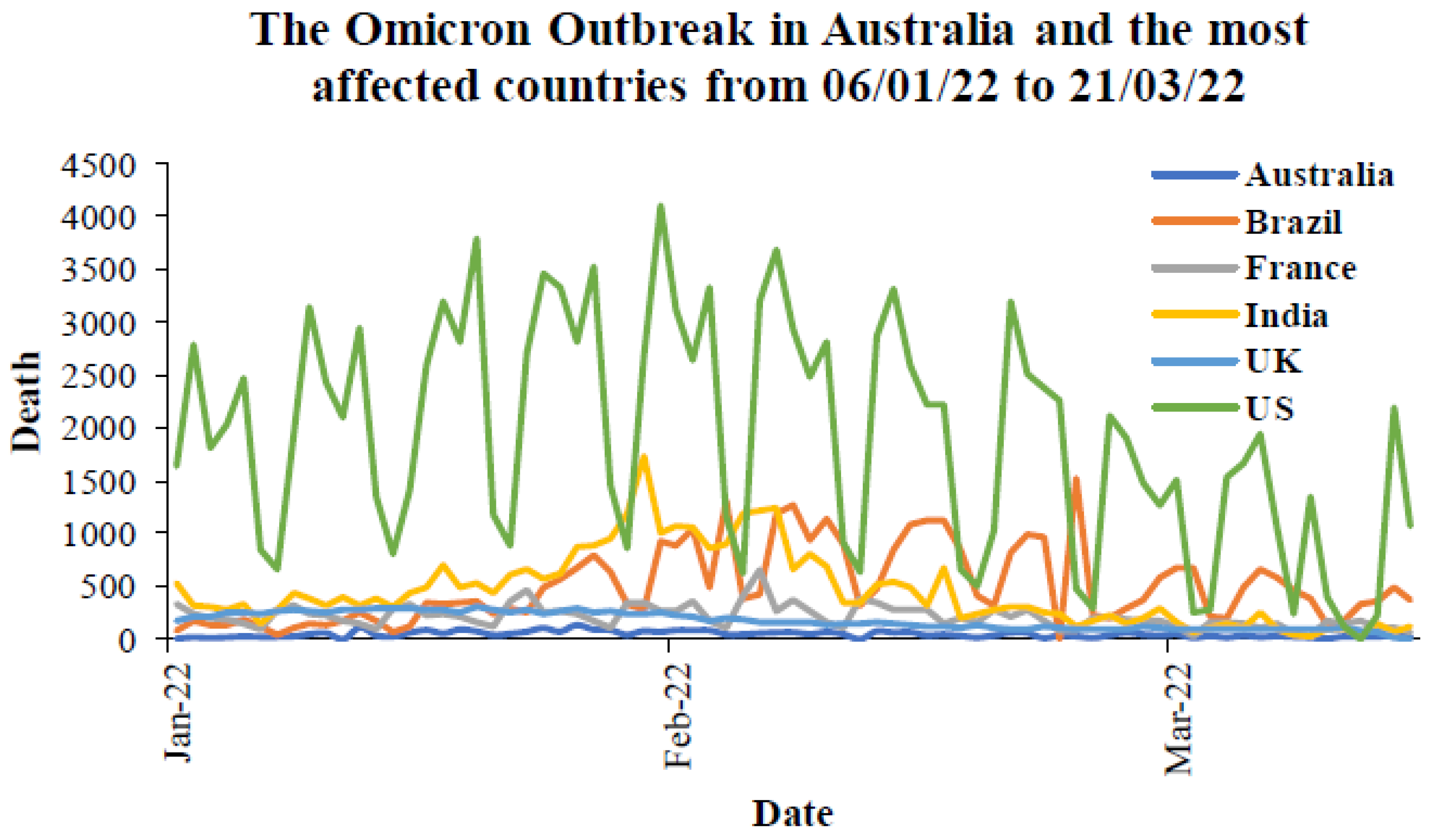
For more analysis, the daily deaths due to COVID-19 during the peak of the Delta outbreak in each country are provided in Figure 16. The peak period is taken from 80% to 100% of cases in total from Figure 11. Figure 17 presents the daily deaths during the Omicron outbreak from January to March 2022. For Australia (Figure 16a), the maximum number of daily deaths during the peak of the Delta outbreak was less than 40 cases, while there were over 100 deaths during the Omicron outbreak in Australia (Figure 17). For other countries, the maximum number of daily deaths during the peak of the Delta outbreak in Brazil (Figure 16b), France (Figure 16c), India (Figure 16d), the UK (Figure 16e), and the US (Figure 16f) were 935, 238, 6148, 192, and 3871 cases, respectively. During the Omicron outbreak in each country (Figure 17), the maximum number of daily deaths in Brazil, France, India, the UK, and the US were 482, 623, 2680, 280, and 4107 cases, respectively. It can be seen that Brazil and India had lower daily deaths during the Omicron outbreak, whereas other countries had higher daily deaths. However, the different mortalities might be because of the vaccination rate, other preventions for each country, and other parameters. The next section provides information on the prevention and the discussion of vaccination effectiveness.
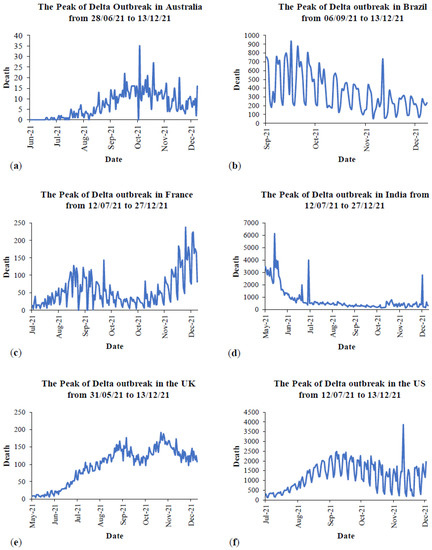
Figure 16.
Mortality during the peak of Delta outbreaks in: (a) Australia, (b) Brazil, (c) France, (d) India, (e) the UK, and (f) the US [64].
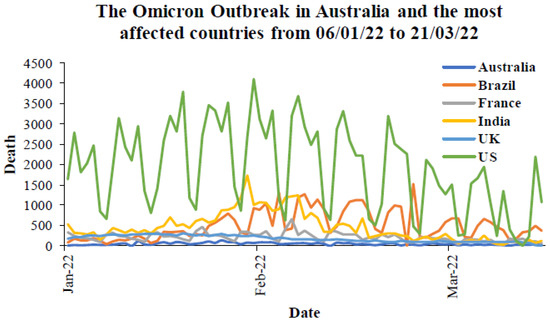
Figure 17.
Mortality during the Omicron outbreaks in Australia and the most affected countries from 6 January to 21 March 2022 [64].
3. Preventions
Currently, the SARS-CoV-2 epidemics are not over, and the Delta and Omicron variants have been circulating around the world with catastrophic consequences to societies and economies. In this consideration, it is extremely vital to continuously implement and practice safety prevention measures. For instance, there are several measures listed and discussed in Table 3, including vaccination effectiveness [86,87,88,89,90].
Table 3.
Delta variant preventive measures.
Vaccination Programs
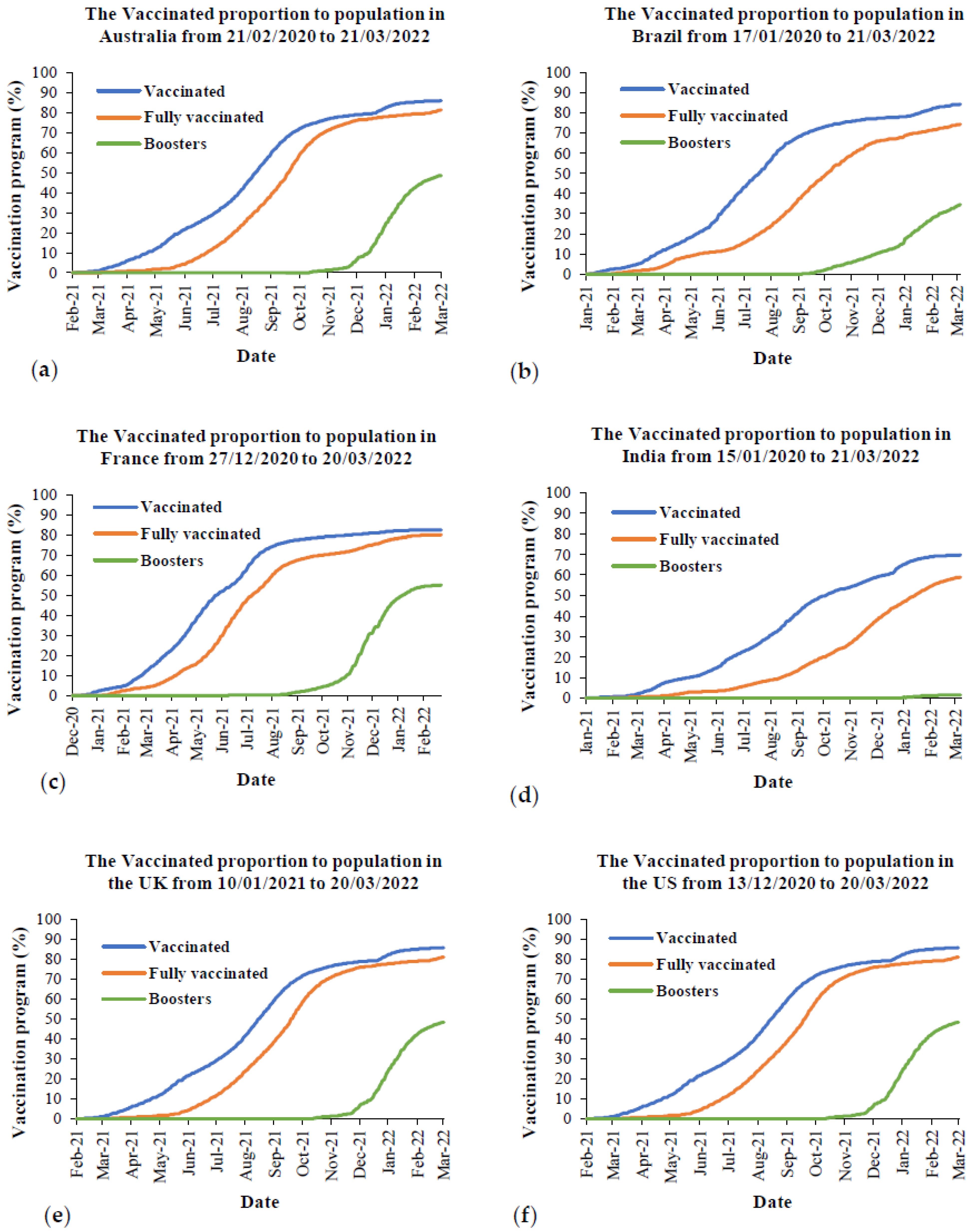
One of the most effective ways to prevent people from SARS-CoV-2 is to become vaccinated. Figure 18 provides the vaccination programs from the first vaccination day to the current day for Australia and the five most affected countries. The meta-data from this figure were taken from Our World in Data [67]. From this figure, it is obvious that over 80% of the population of all countries is vaccinated, except for India, which is around 70% of the population. Regarding the fully vaccinated population, it is around 80% for the populations of Australia, France, the UK and the US, while it is around 74% and 59% for the populations of Brazil and India, respectively. For the boosters, it is around 50% for the populations of Australia, France, the UK and the US, and it is around 34% and 1% for the populations of Brazil and India, respectively.
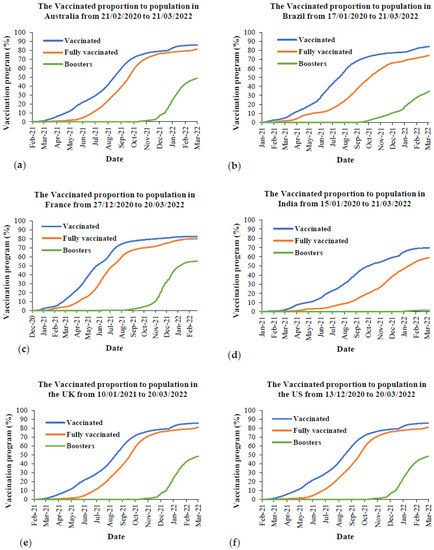
Figure 18.
The vaccination programs in Australia and the most affected countries from the beginning to March 2022: (a) Australia, (b) Brazil, (c) France, (d) India, (e) the UK, and (f) the US.
To have insight into Delta variant transmissibility, it is necessary to analyse Massachusetts’s cluster, where there have been 469 cases since July 2021 during multiple summer events with huge public crowds. Notably, Massachusetts has a 69% fully vaccinated rate among its residents; however, in 469 cases, 346 cases occurred in fully vaccinated people, standing at 74% of total cases [92]. Thus, the Delta variant causes a great number of breakthrough infections, indicating its lofty contagion. When it comes to the severity and mortality profile of the latest Omicron variant, according to UK Health Security Agency [93], the risk of hospital admission from the Omicron variant is around one-third of the Delta variant. Moreover, they also suggest that the considerable reduction in hospitalization is attributed to three doses of the vaccine. However, it is highlighted that the dramatic number of infected cases is highly dedicated to a large number of hospital admissions, which steadily increases in the number of deaths. Thus, the Omicron variant is an actual threat to unvaccinated people.
The Delta variant, with a higher probability of hospitalization and ICU, leads an undoubted threat to unvaccinated people in the way that it spreads in low-vaccination areas. It can be explained by the fact that Australia had a low vaccination rate when the Delta variant hit the country, which was 24% including 5.8% and 18% for fully vaccinated and partially vaccinated people, respectively. When comparing the severity based on the peak of the Delta outbreak from Figure 13 to the vaccination programs, it was around 67% to 77% of the fully vaccinated population for all countries, except for India where it was around 41% of the fully vaccinated population. Thus, one of the possible factors causing a higher severity in both hospitalization and ICU due to the Delta variant is having a lower fully vaccinated rate. During the Omicron outbreak in each country, there was around 80% of the fully vaccinated population from all countries, except for India at around 50% fully vaccinated. Although there was a higher vaccination rate during the Omicron outbreak in all countries, the overall daily hospitalization during this period was still higher than the overall daily cases during the peak outbreak of the Delta variant. For the daily ICU cases, the overall daily ICU cases during the peak outbreak of the Delta variant was higher than the overall daily ICU cases during the Omicron outbreak for all countries (Figure 13). This was probably because of the higher vaccination rate. In terms of the mortality caused by the Delta and Omicron variants, there are limited indications that the Delta variant causes more deaths than other variants when it comes to mortality. However, it is accurate that the Delta variant has been currently posed to a high proportion of COVID-19 deaths among unvaccinated people [77,78]. When comparing the mortality from Figure 16 to the vaccination rate in Figure 18, the overall daily deaths during the Omicron outbreak, having a higher fully vaccinated rate, are still higher than the overall daily deaths during the peak of the Delta outbreak. This was observed in Australia, France, the UK, and the US. This might be because of the reduction of vaccine effectiveness due to the Omicron variant, prevention strategies, as well as the density of populations in each country.
4. Conclusions
In conclusion, the evidence to date demonstrates that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been continuously evolving into new forms of variants. Unfortunately, these mutated variants with new infectious characteristics present a wide range of challenges in many countries. Although the Delta variant drastically increased in the number of infection waves in many countries in 2021, the Omicron variant has spread into over 63 countries since its initial discovery in November 2021 in South Africa. Conversely, by examining several recent infection waves in different countries with diverse backgrounds, there are some major characteristics of the Delta and Omicron variants listed below:
- The Delta variant is highly infectious, estimated to be more than double that of the previous variants.
- Fully vaccinated people can significantly become infected by the Delta variant versus other variants, known as breakthrough infections.
- The Omicron variant is currently the most divergent variant, with a high number of 26 unique mutations in the spike protein.
- There are limited data on the severity and mortality profile of the Omicron variant. However, based on the available meta-data from the validated resources, the Omicron variant significantly affected the increase in daily hospitalization compared to the daily cases during the peak of the Delta outbreak. However, the Omicron variant had less effect on the daily ICU case. A higher fully vaccinated rate is one of the main factors for the reduction of daily ICU cases recently.
However, the mortality rate during the Omicron outbreak is still higher than at the peak of the Delta outbreak. Even with a higher fully vaccinated rate, the mortality rate during this period is still higher than the previous Delta outbreak. This factor is still under investigation. The Delta variant can result in a great number of deaths, and there is still a shortage of confirmed information to indicate that the Delta variant causes a death toll in younger ages. Further reviews will consider more parameters that affect the mortality rate, especially at younger ages.
Author Contributions
Conceptualization, M.S.I. and Y.G.; Methodology, B.V.D., P.L., T.F. and M.S.I.; investigation, B.V.D., P.L. and T.F., formal analysis, B.V.D., P.L., T.F. and S.I.H.; data curation, B.V.D., P.L., T.F. and S.I.H.; writing—original draft preparation, B.V.D., P.L., T.F., Y.G., M.S.I. and S.I.H.; writing—review and editing, B.V.D., P.L., T.F., Y.G., M.S.I., S.C.S. and S.I.H.; supervision, Y.G. and M.S.I. All authors have read and agreed to the published version of the manuscript.
Funding
The authors thank the Australian Research Council for their support, grants DP180103009 and IC190100020.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data will be available upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hasnain, M.; Pasha, M.F.; Ghani, I. Combined measures to control the COVID-19 pandemic in Wuhan, Hubei, China: A narrative review. J. Biosaf. Biosecur. 2020, 2, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Gui, X.; Gao, S.; Ke, H.; Xiong, Y. Clinical progression and changes of chest CT findings among asymptomatic and pre-symptomatic patients with SARS-CoV-2 infection in Wuhan, China. Expert Rev. Respir. Med. 2021, 15, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Duan, S.; Zhou, M.; Zhang, W.; Shen, J.; Qi, R.; Qin, X.; Yu, H.; Zhou, C.; Hu, Q.; Yu, X.-J. Seroprevalence and asymptomatic carrier status of SARS-CoV-2 in Wuhan City and other places of China. PLoS Negl. Trop. Dis. 2021, 15, e0008975. [Google Scholar] [CrossRef] [PubMed]
- Dash, D.P.; Sethi, N.; Dash, A.K. Infectious disease, human capital, and the BRICS economy in the time of COVID-19. MethodsX 2021, 8, 101202. [Google Scholar] [CrossRef]
- Khurshid, A.; Khan, K. How COVID-19 shock will drive the economy and climate? A data-driven approach to model and forecast. Environ. Sci. Pollut. Res. 2021, 28, 2948–2958. [Google Scholar] [CrossRef]
- Lim, W.M.; To, W.-M. The economic impact of a global pandemic on the tourism economy: The case of COVID-19 and Macao’s destination- and gambling-dependent economy. Curr. Issues Tour. 2021, 25, 1258–1269. [Google Scholar] [CrossRef]
- Pham, T.D.; Dwyer, L.; Su, J.-J.; Ngo, T. COVID-19 impacts of inbound tourism on Australian economy. Ann. Tour. Res. 2021, 88, 103179. [Google Scholar] [CrossRef]
- Sandmann, F.G.; Davies, N.G.; Vassall, A.; Edmunds, W.J.; Jit, P.M. The potential health and economic value of SARS-CoV-2 vaccination alongside physical distancing in the UK: A transmission model-based future scenario analysis and economic evaluation. Lancet Infect. Dis. 2021, 21, 962–974. [Google Scholar] [CrossRef]
- Gu, Q.; Qi, S.; Yue, Y.; Shen, J.; Zhang, B.; Sun, W.; Qian, W.; Islam, M.S.; Saha, S.; Wu, J. Structural and functional alterations of the tracheobronchial tree after left upper pulmonary lobectomy for lung cancer. Biomed. Eng. Online 2019, 18, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S.; Saha, S.C.; Sauret, E.; Gu, Y.; Ristovski, Z. Numerical investigation of aerosol particle transport and deposition in realistic lung airway. In Proceedings of the International Conference on Computational Methods, Auckland, New Zealand, 14–17 July 2015. [Google Scholar]
- Islam, M.S.; Saha, S.C.; Sauret, E.; Ong, H.; Young, P.; Gu, Y. Euler–Lagrange approach to investigate respiratory anatomical shape effects on aerosol particle transport and deposition. Toxicol. Res. Appl. 2019, 3, 2397847319894675. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.; Larpruenrudee, P.; Hossain, S.; Rahimi-Gorji, M.; Gu, Y.; Saha, S.; Paul, G. Polydisperse Aerosol Transport and Deposition in Upper Airways of Age-Specific Lung. Int. J. Environ. Res. Public Health 2021, 18, 6239. [Google Scholar] [CrossRef] [PubMed]
- Hendryx, M.; Islam, M.S.; Dong, G.-H.; Paul, G. Air Pollution Emissions 2008–2018 from Australian Coal Mining: Implications for Public and Occupational Health. Int. J. Environ. Res. Public Health 2020, 17, 1570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, M.S.; Gu, Y.; Farkas, A.; Paul, G.; Saha, S.C. Helium–Oxygen Mixture Model for Particle Transport in CT-Based Upper Airways. Int. J. Environ. Res. Public Health 2020, 17, 3574. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Raghav, V.; Padhmashali, V.; Paul, G.; Islam, M.S.; Saha, S.C. Airflow and Particle Transport Prediction through Stenosis Airways. Int. J. Environ. Res. Public Health 2020, 17, 1119. [Google Scholar] [CrossRef] [Green Version]
- Larpruenrudee, P.; Islam, M.S.; Paul, G.; Paul, A.R.; Gu, Y.T.; Saha, S.C. Model for Pharmaceutical Aerosol Transport through Stenosis Airway. In Handbook of Lung Targeted Drug Delivery Systems; Pathak, Y., Islam, N., Eds.; Taylor & Francis Group: Boca Raton, FL, USA, 2021; p. 38. Available online: https://www.taylorfrancis.com/chapters/edit/10.1201/9781003046547-8/model-pharmaceutical-aerosol-transport-stenosis-airway-puchanee-larpruenrudee-mohammad-islam-gunther-paul-akshoy-paul-gu-suvash-saha (accessed on 23 March 2022).
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature 2020, 582, 557–560. [Google Scholar] [CrossRef]
- Islam, M.S.; Larpruenrudee, P.; Saha, S.C.; Pourmehran, O.; Paul, A.R.; Gemci, T.; Collins, R.; Paul, G.; Gu, Y. How severe acute respiratory syndrome coronavirus-2 aerosol propagates through the age-specific upper airways. Phys. Fluids 2021, 33, 081911. [Google Scholar] [CrossRef]
- Islam, M.S.; Larpruenrudee, P.; Paul, A.R.; Paul, G.; Gemci, T.; Gu, Y.; Saha, S.C. SARS CoV-2 aerosol: How far it can travel to the lower airways? Phys. Fluids 2021, 33, 061903. [Google Scholar] [CrossRef]
- Ghosh, A.; Islam, M.S.; Saha, S.C. Targeted Drug Delivery of Magnetic Nano-Particle in the Specific Lung Region. Computation 2020, 8, 10. [Google Scholar] [CrossRef] [Green Version]
- Frampton, M.W. Systemic and Cardiovascular Effects of Airway Injury and Inflammation: Ultrafine Particle Exposure in Humans. Environ. Health Perspect. 2001, 109, 529. [Google Scholar] [CrossRef]
- Hsiao, I.-L.; Huang, Y.-J. Effects of serum on cytotoxicity of nano- and micro-sized ZnO particles. J. Nanopart. Res. 2013, 15, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Oberdörster, G. Pulmonary effects of inhaled ultrafine particles. Int. Arch. Occup. Environ. Health 2000, 74, 1–8. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 29 March 2022).
- Van Oosterhout, C.; Hall, N.; Ly, H.; Tyler, K.M. COVID-19 evolution during the pandemic—Implications of new SARS-CoV-2 variants on disease control and public health policies. Virulence 2021, 12, 507–508. [Google Scholar] [CrossRef] [PubMed]
- Sixt, T.; Moretto, F.; Devilliers, H.; Abdallahoui, M.; Eberl, I.; Rogier, T.; Duong, M.; Salmon-Rousseau, A.; Mahy, S.; Buisson, M.; et al. The Usefullness of NEWS2 at Day 7 of Hospitalisation in Predicting COVID-19 Evolution and As an Early Endpoint in Therapeutic Trials. J. Infect. 2021, 82, 282–327. [Google Scholar] [CrossRef]
- Ben Hassen, H.; Elaoud, A.; Ben Salah, N.; Masmoudi, A. A SIR-Poisson Model for COVID-19: Evolution and Transmission Inference in the Maghreb Central Regions. Arab. J. Sci. Eng. 2021, 46, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Veronese, S.; Sbarbati, A. Chemosensory Systems in COVID-19: Evolution of Scientific Research. ACS Chem. Neurosci. 2021, 12, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Communicable Diseases Genomics Network. Available online: https://www.cdgn.org.au/variants-of-concern (accessed on 23 August 2021).
- European Centre for Disease Prevention and Control. SARS-CoV-2 Variants of Concern as of 26 August 2021. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 26 August 2021).
- Centers for Disease Control and Prevention. SARS-CoV-2 Variant Classifications and Definitions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-info.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fcases-updates%2Fvariant-surveillance%2Fvariant-info.html (accessed on 24 August 2021).
- World Health Organization. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 23 March 2022).
- Kadri, S.S.; Simpson, S.Q. Potential Implications of SARS-CoV-2 Delta Variant Surges for Rural Areas and Hospitals. JAMA 2021, 326, 1003–1004. [Google Scholar] [CrossRef]
- Del Rio, C.; Malani, P.N.; Omer, S.B. Confronting the Delta Variant of SARS-CoV-2, Summer 2021. JAMA 2021, 326, 1001–1002. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, M.; Bhattacharyya, R.; Purkayastha, S.; Zimmermann, L.; Ray, D.; Hazra, A.; Kleinsasser, M.; Mellan, T.; Whittaker, C.; Flaxman, S.; et al. Resurgence of SARS-CoV-2 in India: Potential role of the B.1.617.2 (Delta) variant and delayed interventions. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.06.23.21259405v1 (accessed on 23 March 2022).
- Yang, W.; Shaman, J. COVID-19 Pandemic Dynamics in India and Impact of the SARS-CoV-2 Delta (B.1.617.2) Variant. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.06.21.21259268v1 (accessed on 23 March 2022).
- Novelli, G.; Colona, V.L.; Pandolfi, P.P. A focus on the spread of the delta variant of SARS-CoV-2 in India. Indian J. Med. Res. 2021, 153, 537. [Google Scholar] [CrossRef]
- Kupferschmidt, K.; Wadman, M. Delta variant triggers new phase in the pandemic. Science 2021, 372, 1375–1376. [Google Scholar] [CrossRef]
- Alexandar, S.; Ravisankar, M.; Kumar, R.S.; Jakkan, K. A Comprehensive Review on COVID-19 Delta Variant. International Journal of Parmacology and Clinical Research (IJPCR). Available online: https://www.researchgate.net/profile/Ravisankar-Mathesan/publication/353179027_A_Comprehensive_Review_on_Covid-19_Delta_variant/links/60ec151630e8e50c01fbf87c/A-Comprehensive-Review-on-Covid-19-Delta-variant.pdf (accessed on 23 March 2022).
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital Admission and Emergency Care Attendance Risk for SARS-CoV-2 Delta (B.1.617.2) Compared with Alpha (B.1.1.7) Variants of Concern: A Cohort Study. Lancet Infect. Dis. 2021, 22, 35–42. [Google Scholar] [CrossRef]
- Liu, Y.; Rocklöv, J. The reproductive number of the Delta variant of SARS-CoV-2 is far higher compared to the ancestral SARS-CoV-2 virus. J. Travel Med. 2021, 28, taab124. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Fisman, D.N.; Tuite, A.R. Progressive Increase in Virulence of Novel SARS-CoV-2 Variants in Ontario, Canada. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.07.05.21260050v2 (accessed on 23 March 2022).
- Riemersma, K.A.; Grogan, B.E.; Kirta-Yarbo, A.; Halfmann, P.J.; Segaloff, H.E.; Kocharian, A.; Florek, K.R.; Westergaard, R.; Bateman, A.; Jeppson, G.E.; et al. Vaccinated and Unvaccinated Individuals Have Similar Viral Loads in Communities with a High Prevalence of the SARS-CoV-2 Delta Variant. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.07.31.21261387v1 (accessed on 23 March 2022).
- Nasreen, S.; Chung, H.; He, S.; Brown, K.A.; Gubbay, J.B.; Buchan, S.A.; Fell, D.B.; Austin, P.C.; Schwartz, K.L.; Sundaram, M.E.; et al. Effectiveness of COVID-19 Vaccines against Variants of Concern in Ontario, Canada. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.06.28.21259420v2 (accessed on 23 March 2022).
- Chang, S.L.; Cliff, O.M.; Zachreson, C.; Prokopenko, M. Nowcasting Transmission and Suppression of the Delta Variant of SARS-CoV-2 in Australia. Available online: https://assets.researchsquare.com/files/rs-757351/v1_covered.pdf?c=1631875806 (accessed on 23 March 2022).
- Blakely, T.; Thompson, J.; Carvalho, N.; Bablani, L.; Wilson, N.; Stevenson, M. The Probability of the 6-Week Lockdown in Victoria (Commencing 9 July 2020) Achieving Elimination of Community Transmission of SARS-CoV-2. Med. J. Aust. 2020, 213, 349–351.e341. [Google Scholar] [CrossRef] [PubMed]
- Zachreson, C.; Mitchell, L.; Lydeamore, M.J.; Rebuli, N.; Tomko, M.; Geard, N. Risk mapping for COVID-19 Outbreaks in Australia using mobility data. J. R. Soc. Interface 2021, 18, 20200657. [Google Scholar] [CrossRef]
- Nguyen, K. Sweeping New Lockdown Restrictions Announced as NSW Records 111 New COVID Cases. ABC News. 2021. Available online: https://www.abc.net.au/news/2021-07-17/nsw-records-111-covid-19-cases/100300492 (accessed on 17 July 2021).
- World Health Organization. Classification of Omicron (B.1.1529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 26 November 2021).
- Rao, S.; Singh, M. The Newly Detected B.1.1.529 (Omicron) Variant of SARS-CoV-2 with Multiple Mutations. DHR Proc. 2021, 1, 7–10. [Google Scholar] [CrossRef]
- Venkatakrishnan, A.; Anand, P.; Lenehan, P.; Suratekar, R.; Raghunathan, B.; Niesen, M.J.; Soundararajan, V. Omicron Variant of SARS-CoV-2 Harbors a Unique Insertion Mutation of Putative Viral or Human Genomic Origin. Available online: https://osf.io/f7txy/ (accessed on 23 March 2022).
- Karim SS, A.; Karim, Q.A. Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). COVID-19 Situation Updates. Available online: https://www.ecdc.europa.eu/en/covid-19/situation-updates (accessed on 23 March 2022).
- Meo, S.A.; Meo, A.S.; Al-Jassir, F.F.; Klonoff, D.C. Omicron SARS-CoV-2 new variant: Global prevalence and biological and clinical characteristics. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 8012–8018. [Google Scholar] [PubMed]
- Mohapatra, R.K.; Sarangi, A.K.; Kandi, V.; Azam, M.; Tiwari, R.; Dhama, K. Omicron (B.1.1.529 variant of SARS-CoV-2); an emerging threat: Current global scenario. J. Med. Virol. 2021, 94, 1780–1783. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Understanding Variants. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/understanding-variants.html (accessed on 23 March 2022).
- Alizong, S.; Haim-Boukobza, S.; Foulongne, V.; Verdurme, L.; Trombert-Paolantoni, S.; Lecorche, E.; Roquebert, B.; Sofonea, M.T. Rapid Spread of the SARS-CoV-2 Delta Variant in Some French Regions, June 2021. Eurosurveillance 2021, 26, 2100573. [Google Scholar]
- Stern, A.; Fleishon, S.; Kustin, T.; Dotan, E.; Mandelboim, M.; Erster, O.; Israel Consortium of SARS-CoV-2 Sequencing; Mendelson, E.; Mor, O.; Zuckerman, N.S. The Unique Evolutionary Dynamics of the SARS-CoV-2 Delta Variant. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.08.05.21261642v2.full.pdf+html (accessed on 23 March 2022).
- Patane, J.; Viala, V.; Lima, L.; Martins, A.; Barros, C.; Marqueze, E.; Bernardino, J.; Moretti, D.; Slavov, S.; Bezerra, R.; et al. SARS-CoV-2 Delta Variant of Concern in Brazil—Multiple Introdutions, Communitary Transmission, and Early Signs of Local Evolution. medRxiv 2021. Available online: https://www.medrxiv.org/content/10.1101/2021.09.15.21262846v1 (accessed on 23 March 2022).
- Kannan, S.R.; Spratt, A.N.; Cohen, A.R.; Naqvi, S.H.; Chand, H.S.; Quinn, T.P.; Lorson, C.L.; Byrareddy, S.N.; Singh, K. Evolutionary analysis of the Delta and Delta Plus variants of the SARS-CoV-2 viruses. J. Autoimmun. 2021, 124, 102715. [Google Scholar] [CrossRef]
- Mishra, S.; Mindermann, S.; Sharma, M.; Whittaker, C.; A Mellan, T.; Wilton, T.; Klapsa, D.; Mate, R.; Fritzsche, M.; Zambon, M.; et al. Changing composition of SARS-CoV-2 lineages and rise of Delta variant in England. EClinicalMedicine 2021, 39, 101064. [Google Scholar] [CrossRef]
- Mohammadi, M.; Shayestehpour, M.; Mirzaei, H. The impact of spike mutated variants of SARS-CoV2 [Alpha, Beta, Gamma, Delta, and Lambda] on the efficacy of subunit recombinant vaccines. Braz. J. Infect. Dis. 2021, 25, 101606. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 23 March 2022).
- Ashly Hagen, M.S. How Dangerous Is the Delta Variant (B.1.617.2). Available online: https://asm.org/Articles/2021/July/How-Dangerous-is-the-Delta-Variant-B-1-617-2 (accessed on 30 July 2021).
- NSW Health, COVID-19 (Coronavirus). Available online: https://www.health.nsw.gov.au/Infectious/covid-19/Pages/stats-nsw.aspx (accessed on 23 March 2022).
- Our World in Data, SARS-CoV-2 Sequences by Variant, 21 March 2022. Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=latest&facet=none&pickerSort=asc&pickerMetric=location&Interval=7-day+rolling+average&Relative+to+Population=true&Color+by+test+positivity=false&country=USA~GBR~IND~AUS~BRA~FRA&Metric=Variants (accessed on 23 March 2022).
- Tommaso, C.B.; Mohsen, M.; George, W.R.; Nooshin, R. Outdoor Transmission of SARS-CoV-2 and Other Respiratory Viruses: A Systematic Review. J. Infect. Dis. 2021, 223, 550–561. [Google Scholar] [CrossRef]
- Athalia, C.; John, T.; Lauri, A.; Sauber-Schatz, E.K.; Yoder, J.S.; Honein, M.A. Guidance for Implementing COVID-9 Prevention Strategies in the Context of Varying Community Transmission Levels and Vaccination Coverage. Available online: https://www.cdc.gov/mmwr/volumes/70/wr/mm7030e2.htm (accessed on 27 July 2021).
- Jonathan, R.; Kendall, D.; Russell, E.; Christensen, J.H.; Halvorsen, T.G.; Hogan, C.G., Jr.; O’horo, J.C.; Breeher, L.E.; Callstrom, M.R.; Wehde, M.B. Combined Effects of Masking and Distance on Aerosol Exposure Potential. Mayo Clin. Proc. 2021, 96, 1792–1800. [Google Scholar] [CrossRef]
- Morawska, L.; Johnson, G.R.; Ristovski, Z.D.; Hargreaves, M.; Mengersen, K.; Corbett, S.; Chao, C.Y.H.; Li, Y.; Katoshevski, D. Size distribution and sites of origin of droplets expelled from the human respiratory tract during expiratory activities. J. Aerosol. Sci. 2009, 40, 256–269. [Google Scholar] [CrossRef] [Green Version]
- Lea, H.; Polly, D.; Ian, C.; Ross, A.; Jordan, A.; Lee, J.; Lynn, J.; Ball, A.; Narwal, S.; Russell, S.; et al. High SARS-CoV-2 Attack Rate Following Exposure at a Choir Practice—Skagit County, Washington, March 2020. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/mmwr/volumes/69/wr/mm6919e6.htm (accessed on 15 May 2020).
- Jamous, F.; Meyer, N.; Buus, D.; Ateeli, H.; Taggart, K.; Hanson, T.; Alzoubaidi, M.; Nazir, J.; Devasahayam, J. Critical Illness Due to Covid-19: A Description of the Surge in a Single Center in Sioux Falls. SD Med. 2020, 73, 312–317. [Google Scholar]
- De Man, P.; Paltansing, S.; Ong, D.S.Y.; Vaessen, N.; van Nielen, G.; Koeleman, J.G.M. Outbreak of Coronavirus Disease 2019 (COVID-19) in a Nursing Home Associated with Aerosol Transmission as a Result of Inadequate Ventilation. Clin. Infect. Dis. 2020, 73, 170–171. [Google Scholar] [CrossRef] [PubMed]
- Bilinski, A.; Mostashari, F.; Salomon, J.A. Modeling Contact Tracing Strategies for COVID-19 in the Context of Relaxed Physical Distancing Measures. JAMA Netw. Open 2020, 3, e2019217. [Google Scholar] [CrossRef]
- Public Health England. SARS-CoV-2 Variants of Concern and Variants under Investigation in England. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1018547/Technical_Briefing_23_21_09_16.pdf (accessed on 23 March 2022).
- Khedar, R.S.; Mittal, K.; Ambaliya, H.C.; Mathur, A.; Gupta, J.B.; Sharma, K.K.; Singh, Y.; Sharma, G.; Gupta, A.; Bhargava, V. Greater Covid-19 Severity and Mortality in Hospitalized Patients in Second (Delta Variant) Wave Compared to the First: Single Centre Prospective Study in India. medRxiv 2021. [Google Scholar] [CrossRef]
- Chia, P.Y.; Xiang Ong, S.W.; Chiew, C.J.; Ang, L.W.; Chavatte, J.-M.; Mak, T.-M.; Cui, L.; Kalimuddin, S.; Chia, W.N.; Tan, C.W.; et al. Virological and serological kinetics of SARS-CoV-2 Delta variant vaccine-breakthrough infections: A multi-center cohort study. medRxiv 2021, 28, 612.e1–612.e7. [Google Scholar] [CrossRef]
- Riemersma, K.K.; Grogan, B.E.; Kita-Yarbro, A.; Halfmann, P.J.; Segaloff, H.E.; Kocharian, A.; Florek, K.R.; Westergaard, R.; Bateman, A.; Jeppson, G.E.; et al. Shedding of Infectious SARS-CoV-2 Despite Vaccination. medRxiv 2021. [Google Scholar] [CrossRef]
- Chakraborty, C.; Bhattacharya, M.; Sharma, A.R. Present variants of concern and variants of interest of severe acute respiratory syndrome coronavirus 2: Their significant mutations in S-glycoprotein, infectivity, re-infectivity, immune escape and vaccines activity. Rev. Med. Virol. 2021, 32, e2270. [Google Scholar] [CrossRef]
- Lechien, J.R.; Saussez, S. Importance of epidemiological factors in the evaluation of transmissibility and clinical severity of SARS-CoV-2 variants. Lancet Infect. Dis. 2021, 22, 2–3. [Google Scholar] [CrossRef]
- Honein, M.A.; Christie, A.; Rose, D.A.; Brooks, J.T.; Meaney-Delman, D.; Cohn, A.; Sauber-Schatz, E.K.; Walker, A.; McDonald, L.C.; Liburd, L.C.; et al. Summary of Guidance for Public Health Strategies to Address High Levels of Community Transmission of SARS-CoV-2 and Related Deaths, December 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1860–1867. [Google Scholar] [CrossRef] [PubMed]
- Heath Data. Gov, COVID-19 Report Patient Impact and Hospital Capacity by State Timeseries. Available online: https://healthdata.gov/Hospital/COVID-19-Reported-Patient-Impact-and-Hospital-Capa/g62h-syeh (accessed on 23 March 2022).
- GOV.UK Coronavirus (COVID-19) in the UK, Healthcare in United Kingdom. Available online: https://coronavirus.data.gov.uk/details/healthcare (accessed on 23 March 2022).
- Données Hospitalières Relatives à l’épidémie de COVID-19 SIVIC. Available online: https://www.data.gouv.fr/fr/datasets/donnees-hospitalieres-relatives-a-lepidemie-de-covid-19/ (accessed on 23 March 2022).
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; COVID-19 Systematic Urgent Review Group Effort (SURGE) Study Authors. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Harris, R.J.; Hall, J.A.; Zaidi, A.; Andrews, N.J.; Dunbar, J.K.; Dabrera, G. Effect of Vaccination on Household Transmission of SARS-CoV-2 in England. N. Engl. J. Med. 2021, 385, 759–760. [Google Scholar] [CrossRef] [PubMed]
- Bose, P. Researchers Examnie the Effectiveness of the Pfizer-BioNTech COVID-19 Vaccine in Reducing Household Transmission. News Medical Life Sciences. Available online: https://www.news-medical.net/news/20210720/Researchers-examine-the-effectiveness-of-the-Pfizer-BioNTech-COVID-19-vaccine-in-reducing-household-transmission.aspx (accessed on 20 July 2021).
- Vitiello, A.; Ferrara, F.; Troiano, V.; La Porta, R. COVID-19 vaccines and decreased transmission of SARS-CoV-2. Inflammopharmacology 2021, 29, 1357–1360. [Google Scholar] [CrossRef]
- Howard, J.; Huang, A.; Li, Z.; Tufekci, Z.; Zdimal, V.; van der Westhuizen, H.-M.; von Delft, A.; Price, A.; Fridman, L.; Tang, L.-H.; et al. An evidence review of face masks against COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2014564118. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Catherine, M.; Johanna, V.; Hillary, J.; Burns, M.; Gharpure, R.; Sami, S.; Sabo, R.T.; Hall, N.; Foreman, A.; Schubert, P.L.; et al. Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings—Barnstable County, Massachusetts. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm (accessed on 6 August 2021).
- UK Health Security Agency. Technical Briefing: Update on Hospitalisation and Vaccine Effectiveness for Omicron VOC-21NOV-01 (B.1.1529). SARS-CoV-2 Variants of Concern and Variants Under Investigation in England. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1044481/Technical-Briefing-31-Dec-2021-Omicron_severity_update.pdf (accessed on 31 December 2021).








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).