
Associations between Health Literacy and Sociodemographic Factors: A Cross-Sectional Study in Malaysia Utilising the HLS-M-Q18

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Approval
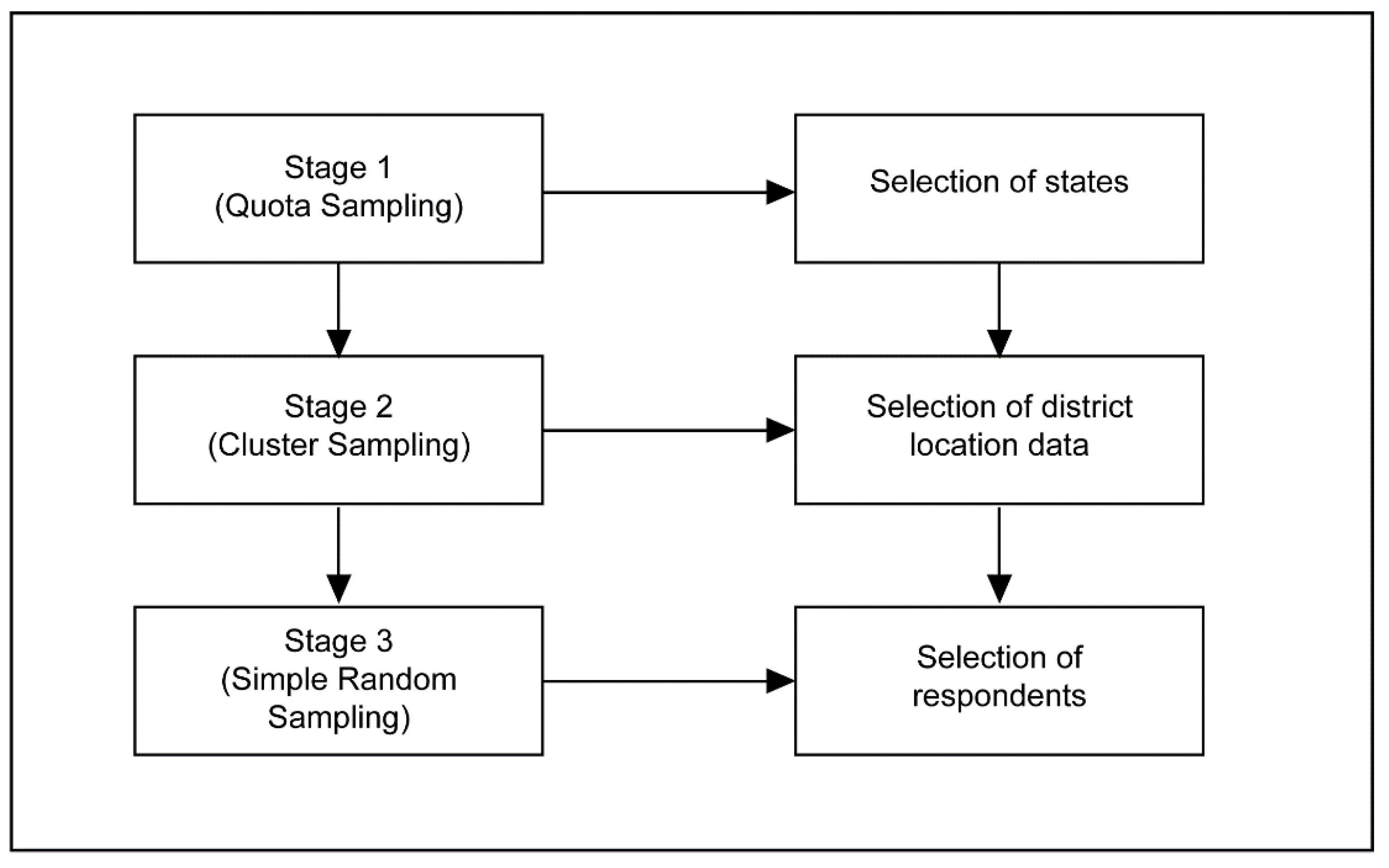
2.3. Recruitment Procedure
2.4. Study Instrument
2.5. Statistical Analysis
3. Results
Demographic Characteristics
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, L.; Qian, X.; Chen, Z.; He, T. Health literacy and its effect on chronic disease prevention: Evidence from China’s data. BMC Public Health 2020, 20, 690. [Google Scholar] [CrossRef] [PubMed]
- Gonza´lez-Chica, D.A.; Mnisi, Z.; Avery, J.; Duszynski, K.; Doust, J.; Tideman, P.; Murphy, A.; Burgees, J.; Beilby, J.; Stocks, N. Effect of health literacy on quality of life amongst patients with ischaemic heart disease in Australian general practice. PLoS ONE 2016, 11, e0151079. [Google Scholar]
- Santos, P.; Sá, L.; Couto, L.; Hespanhol, A. Health literacy as a key for effective preventive medicine. Cogent. Soc. Sci. 2017, 3, 1407522. [Google Scholar] [CrossRef]
- Jandorf, S.; Nielsen, M.K.; Sørensen, K.; Sørensen, T.L. Low health literacy levels in patients with chronic retinal disease. BMC Ophthalmol. 2019, 19, 174. [Google Scholar] [CrossRef] [PubMed]
- Anwar, W.A.; Mostafa, N.S.; Hakim, S.A.; Sos, D.G.; Abozaid, D.A.; Osborne, R.H. Health literacy strengths and limitations among rural fishing communities in Egypt using the Health Literacy Questionnaire (HLQ). PLoS ONE 2020, 15, e0235550. [Google Scholar] [CrossRef]
- McCaffery, K.J.; Dodd, R.H.; Cvejic, E.; Ayre, J.; Batcup, C.; Isautier, J.M.J.; Copp, T.; Bonner, C.; Pickles, K.; Nickel, B.; et al. Health literacy and disparities in COVID-19–related knowledge, attitudes, beliefs and behaviours in Australia. Public Health Res. Pract. 2020, 30, e30342012. [Google Scholar] [CrossRef] [PubMed]
- Haun, J.N.; Patel, N.R.; French, D.D.; Campbell, R.R.; Bradham, D.D.; Lapcevic, W.A. Association between health literacy and medical care costs in an integrated healthcare system: A regional population based study. BMC Health Serv. Res. 2015, 15, 249. [Google Scholar] [CrossRef]
- Lopes-Marques, S.R.; Aguiar-Lemos, S.M. Health literacy assessment instruments: Literature review. Audiol. Commun. Res. 2017, 22, e1757. [Google Scholar]
- Guo, S.; Armstrong, R.; Waters, E.; Sathish, T.; Alif, S.M.; Browne, G.R.; Yu, X. Quality of health literacy instruments used in children and adolescents: A systematic review. BMJ Open 2018, 8, e020080. [Google Scholar] [CrossRef]
- Abdullah, A.; Liew, S.M.; Salim, H.S.; Ng, C.J.; Chinna, K. Health literacy research in Malaysia: A scoping review. Sains Malays. 2020, 49, 5. [Google Scholar] [CrossRef]
- Mohamad, E.M.W.; Kaudan, M.K.; Hamzah, M.R.; Azlan, A.A.; Ayub, S.H.; Tham, J.S.; Ahmad, A.L. Establishing the HLS-M-Q18 short version of the European health literacy survey questionnaire for the Malaysian context. BMC Public Health 2020, 20, 580. [Google Scholar] [CrossRef]
- Shahrir, S.N.; Shamsuddin, K.; Mohamad Nor, N.S.; Man, C.S.; Omar, M.A.; Ahmad, M.H.; Ambak, R. Limited health literacy and its associated factors among overweight and obese housewives living in Klang Valley low cost flats: Findings from the my body is fit and fabulous at home (Mybff@Home) study. Malays. J. Public Health Med. 2018, 18, 19–27. [Google Scholar]
- Cheah, Y.K.; Su, T.T. The determinants of consumer health information on chronic non-communicable disease: An exploratory study in Penang, Malaysia. J. Univ. Malaya Med. Cent. 2012, 15, 1–7. [Google Scholar]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Pub. Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Duong, T.V.; Aringazina, A.; Baisunova, G.; Nurjannah, P.T.V.; Pham, K.M.; Truong, T.Q.; Nguyen, K.T.; Oo, W.M.; Mohamad, E.; Su, T.T.; et al. Measuring health literacy in Asia: Validation of the HLS-EU-Q47 survey tool in six Asian countries. J. Epidemiol. 2017, 27, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Dodson, S.; Good, S.; Osborne, R.H. Health Literacy Toolkit for Low- and Middle-Income Countries: A Series of Information Sheets to Empower Communities and Strengthen Health Systems; World Health Organization, Regional Office for South-East Asia: New Delhi, India, 2015. [Google Scholar]
- Trezona, A.; Dodson, S.; Osborne, R.H. Development of the Organizational Health Literacy Responsiveness (Org-HLR) Framework in Collaboration with Health and Social Services Professionals. BMC Health Serv. Res. 2017, 17, 513. [Google Scholar] [CrossRef] [PubMed]
- Froze, S.; Arif, M.T.; Saimon, R. Does health literacy predict preventive lifestyle on metabolic syndrome? A population-based study in Sarawak Malaysia. Open J. Prev. Med. 2018, 8, 169. [Google Scholar] [CrossRef][Green Version]
- Charmaraman, L.; Woo, M.; Quach, A.; Erkut, S. How have researchers studied multiracial populations? A content and methodological review of 20 years of research. Cult. Divers. Ethn. Minor. Psychol. 2014, 20, 336–352. [Google Scholar] [CrossRef]
- Berens, E.M.; Vogt, D.; Ganahl, K.; Weishaar, H.; Pelikan, J.; Schaeffer, D. Health literacy and health service use in Germany. Health Lit. Res. Pract. 2018, 2, 115–122. [Google Scholar] [CrossRef]
- Ministry of Rural Development. The Rural Master Plan; Kementerian Kemajuan Luar Bandar dan Wilayah: Putrajaya, Malaysia, 2010.
- Koran, J. Preliminary proactive sample size determination for confirmatory factor analysis models. Meas. Eval. Couns. Dev. 2017, 49, 296–308. [Google Scholar] [CrossRef]
- Conroy, R. Sample size: A rough guide. Ethics (Med. Res.) Comm. 2015. Available online: http://www.beaumontethics.ie/docs/application/samplesizecalculation.pdf (accessed on 14 January 2021).
- Israel, G.D. Determining Sample Size; Report No.: Fact Sheet PEOD-6; University of Florida: Gainesville, FL, USA, 1992. [Google Scholar]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross Cult. Psychol. 1970, 3, 185–216. [Google Scholar] [CrossRef]
- Uysal, N.; Ceylan, E.; Koç, A. Health literacy level and influencing factors in university students. Health Soc. Care Community 2019, 28, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.G.; Curtis, L.M.; Wardle, J.; von Wagner, C.; Wolf, M.S. Skill set or mind set? Associations between health literacy, patient activation and health. PLoS ONE 2013, 8, e74373. [Google Scholar] [CrossRef] [PubMed]
- Storey, A.; Hanna, L.; Missen, K.; Hakman, N.; Osborne, R.H.; Beauchamp, A. The association between health literacy and self-rated health amongst Australian university students. J. Health Commun. 2020, 25, 333–343. [Google Scholar] [CrossRef]
- Svendsen, M.T.; Bak, C.K.; Sørensen, K.; Pelikan, J.; Riddersholm, S.J.; Skals, R.K.; Mortensen, R.N.; Maidal, H.T.; Boggild, H.; Nielsen, G.; et al. Associations of health literacy with socioeconomic position, health risk behavior, and health status: A large national population-based survey among Danish adults. BMC Public Health 2020, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bo, A.; Friis, K.; Osborne, R.H.; Maindal, H.T. National indicators of health literacy: Ability to understand health information and to engage actively with healthcare providers—A population-based survey among Danish adults. BMC Public Health 2014, 14, 1095. [Google Scholar] [CrossRef] [PubMed]
- Rohrich, R.J.; Dayan, E. Improving communication with millennial patients. Plast. Reconstr. Surg. 2019, 144, 533–535. [Google Scholar] [CrossRef] [PubMed]
- McKee, M.; van Schalkwyk, M.C.I.; Stuckler, D. The second information revolution: Digitalization brings opportunities and concerns for public health. Eur. J. Environ. Public Health. 2019, 29, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Azlan, A.A. Measures of eHealth literacy: Options for the Malaysian population. J. Komun. Malays. J. Commun. 2019, 35, 211–228. [Google Scholar] [CrossRef]
- Yilma, T.M.; Inthiran, A.; Reidpath, D.D.; Orimaye, S.O. Context-based interactive health information searching. Inf. Res. 2019, 24, 1–22. [Google Scholar]
- Norrafizah, J.; Nor Asiah, M.; Suraiya, S.M.; Zawaha, H.I.; Normawati, A. Assessment of health literacy among people in a rural area in Malaysia using newest vital signs assessment. J. Educ. Soc. Behav. Sci. 2016, 16, 1–7. [Google Scholar] [CrossRef]
- Rani, H.; Su, Y.H.; Ding, S.A.; Yahya, N.A.; Jaafar, A. Comparison of visual oral health literacy level pre and post oral health education among adolescents. J. Int. Dent. Med Res. 2019, 12, 640–644. [Google Scholar]
- Muhd Noor, N.; Rani, H.; Zakaria, A.S.I.; Yahya, N.A.; Sockalingam, S.N. Sociodemography, oral health status and behaviours related to oral health literacy. Pesqui Bras. Odontopediatria Clin. Integr. 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Ibrahim, N.; Amit, N.; Shahar, S.; Wee, L.H.; Ismail, R.; Khairuddin, R.; Ching, S.S.; Mohd Safien, A. Do depression literacy, mental illness beliefs & stigma influence mental health help-seeking attitude? A cross-sectional study of secondary school and university students from B40 households in Malaysia. BMC Public Health 2019, 1–8, 544. [Google Scholar]


{kind=link}
| State | Locality | Ethnicity | N | Area |
|---|---|---|---|---|
| Peninsular—Selangor (6.298 mil = 58.2%) n= 466 | Urban (93.3%) n = 435 | Malay | 299 | Shah Alam |
| Chinese | 103 | |||
| Indian | 33 | |||
| Rural (6.7%) n = 31 | Malay | 21 | Hulu Langat | |
| Chinese | 7 | |||
| Indian | 3 | |||
| Peninsular—Kuala Lumpur (1.782 mil = 16.5%) n = 132 | Urban (100%) n = 132 | Malay | 82 | Segambut and Lembah Pantai |
| Chinese | 38 | |||
| Indian | 12 | |||
| Borneo—Sarawak (2.741 mil = 25.3%) n= 202 | Urban (57.8%) n = 117 | Bumiputera | 91 | Kuching |
| Chinese | 26 | |||
| Indian | 0 | |||
| Rural (42.2%) n = 85 | Bumiputera | 66 | Sarikei (Maradong) and Samarahan (Simujan) | |
| Chinese | 19 | |||
| Indian | 0 |
| N (%) | Health Literacy Level N (%) | ||||
|---|---|---|---|---|---|
| Inadequate | Problematic | Sufficient | Excellent | ||
| Respondents | 866 (100) | 154 (17.8) | 348 (40.2) | 284 (32.8) | 79 (9.1) |
| Age (mean) | 866 (33.6) | 33.1 | 33.8 | 33.5 | 33.8 |
| Gen Z (1995–2012) | 211 (24.4) | 33 (15.6) | 75 (35.5) | 78 (37.0) | 25 (11.8) |
| Gen Y (1977–1994) | 377 (43.6) | 73 (19.4) | 162 (43.0) | 114 (30.2) | 28 (7.4) |
| Gen X (1966–1976) | 184 (21.3) | 34 (18.5) | 77 (41.8) | 58 (31.5) | 15 (8.2) |
| Baby Boomers (1950–1965) | 93 (9.8) | 13 (14.0) | 34 (36.6) | 35 (37.6) | 11 (11.8) |
| Gender | |||||
| Male | 303 (35) | 65 (21.5) | 109 (36.0) | 105 (34.7) | 24 (7.9) |
| Female | 563 (65) | 89 (15.8) | 239 (42.5) | 180 (32.0) | 55 (9.8) |
| Race | |||||
| Malay | 470 (54.3) | 68 (14.5) | 188 (40.0) | 170 (36.2) | 44 (9.4) |
| Chinese | 213 (24.6) | 46 (21.6) | 89 (41.8) | 59 (27.7) | 19 (8.9) |
| Indian | 65 (7.5) | 15 (23.1) | 21 (32.3) | 23 (35.4) | 6 (9.2) |
| Bumiputera | 115 (13.3) | 25 (21.7) | 48 (41.7) | 32 (27.8) | 10 (8.7) |
| Marital status | |||||
| Not married | 429 (49.7) | 74 (17.2) | 163 (38.0) | 149 (34.7) | 43 (10.0) |
| Married | 394 (45.6) | 74 (18.8) | 162 (41.1) | 125 (31.7) | 33 (8.4) |
| Separated/Divorced | 21 (2.4) | 4 (19.0) | 12 (57.1) | 4 (19.0) | 1 (4.8) |
| Widowed | 20 (2.3) | 2 (10.0) | 10 (50.0) | 6 (30.0) | 2 (10.0) |
| Income | |||||
| Below RM3000 (including no income) | 510 (59.4) | 88 (17.3) | 220 (43.1) | 162 (31.8) | 40 (7.8) |
| RM3001–RM9000 | 293 (34.1) | 58 (19.8) | 105 (35.8) | 99 (33.8) | 31 (10.6) |
| ≥RM9001 | 55 (6.4) | 7 (12.7) | 20 (36.4) | 20 (36.4) | 8 (14.5) |
| Exercise (days a week) | |||||
| 0–2 days | 347(40.1) | 85 (24.5) | 130 (37.5) | 111 (32.0) | 21 (6.1) |
| More than 2 days a week | 519 (59.9) | 69 (13.3) | 218 (42.0) | 174 (33.5) | 58 (11.2) |
| Health Problems | |||||
| 1 and more than 1 disease | 219 (25.3) | 42 (19.2) | 84 (38.4) | 76 (34.7) | 17 (7.8) |
| No disease | 646 (74.7) | 17.3 (17.3) | 40.9 (40.9) | 32.2 (32.2) | 9.6 (9.6) |
| Health status | |||||
| Bad | 248 (28.7) | 70 (28.2) | 105 (42.3) | 61 (24.6) | 12 (4.8) |
| Good | 617 (71.3) | 84 (13.6) | 242 (39.2) | 224 (36.3) | 67(10.9) |
| Adequate Health Literacy (Yes = 1) | ||||
|---|---|---|---|---|
| p Value | Exp (B) | 95% C.I for Exp (B) | ||
| Lower | Upper | |||
| a Gender—Male | 0.843 | 0.969 | 0.709 | 1.324 |
| b Age | ||||
| Gen Z | 0.478 | 0.793 | 0.417 | 1.505 |
| Gen Y | 0.031 | 0.549 | 0.319 | 0.946 |
| Gen X | 0.179 | 0.682 | 0.390 | 1.191 |
| c Race | ||||
| Chinese | 0.115 | 0.751 | 0.526 | 1.073 |
| Indian | 0.886 | 0.960 | 0.553 | 1.667 |
| Bumiputera | 0.177 | 0.735 | 0.470 | 1.149 |
| Others | 0.724 | 0.638 | 0.053 | 7.720 |
| d Health Status | ||||
| Bad | 0.000 | 0.431 | 0.301 | 0.618 |
| e Health Problem | ||||
| One or more than one | 0.050 | 1.447 | 1.000 | 2.096 |
| f Marital status | ||||
| Not married | 1.000 | |||
| Married | 0.269 | 0.814 | 0.565 | 1.173 |
| Separated/divorced | 0.076 | 0.381 | 0.131 | 1.105 |
| Widowed | 0.383 | 0.631 | 0.224 | 1.775 |
| g Income | ||||
| Below RM3000 (including no income) | ||||
| RM3001–9000 | 0.122 | 1.281 | 0.936 | 1.754 |
| ≥RM9001 | 0.126 | 1.580 | 0.879 | 2.841 |
| h Exercise (days a week) | ||||
| More than 2 days a week | 0.252 | 1.186 | 0.885 | 1.590 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azlan, A.A.; Hamzah, M.R.; Tham, J.S.; Ayub, S.H.; Ahmad, A.L.; Mohamad, E. Associations between Health Literacy and Sociodemographic Factors: A Cross-Sectional Study in Malaysia Utilising the HLS-M-Q18. Int. J. Environ. Res. Public Health 2021, 18, 4860. https://doi.org/10.3390/ijerph18094860
Azlan AA, Hamzah MR, Tham JS, Ayub SH, Ahmad AL, Mohamad E. Associations between Health Literacy and Sociodemographic Factors: A Cross-Sectional Study in Malaysia Utilising the HLS-M-Q18. International Journal of Environmental Research and Public Health. 2021; 18(9):4860. https://doi.org/10.3390/ijerph18094860
Chicago/Turabian StyleAzlan, Arina Anis, Mohammad Rezal Hamzah, Jen Sern Tham, Suffian Hadi Ayub, Abdul Latiff Ahmad, and Emma Mohamad. 2021. "Associations between Health Literacy and Sociodemographic Factors: A Cross-Sectional Study in Malaysia Utilising the HLS-M-Q18" International Journal of Environmental Research and Public Health 18, no. 9: 4860. https://doi.org/10.3390/ijerph18094860
APA StyleAzlan, A. A., Hamzah, M. R., Tham, J. S., Ayub, S. H., Ahmad, A. L., & Mohamad, E. (2021). Associations between Health Literacy and Sociodemographic Factors: A Cross-Sectional Study in Malaysia Utilising the HLS-M-Q18. International Journal of Environmental Research and Public Health, 18(9), 4860. https://doi.org/10.3390/ijerph18094860