
The Value of Total Body Photography for the Early Detection of Melanoma: A Systematic Review

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Types of Outcome Measures
2.3. Search Methods for Identification of Studies
2.4. Selection of Studies
2.5. Data Extraction and Management
2.6. Assessment of Methodological Quality
3. Results
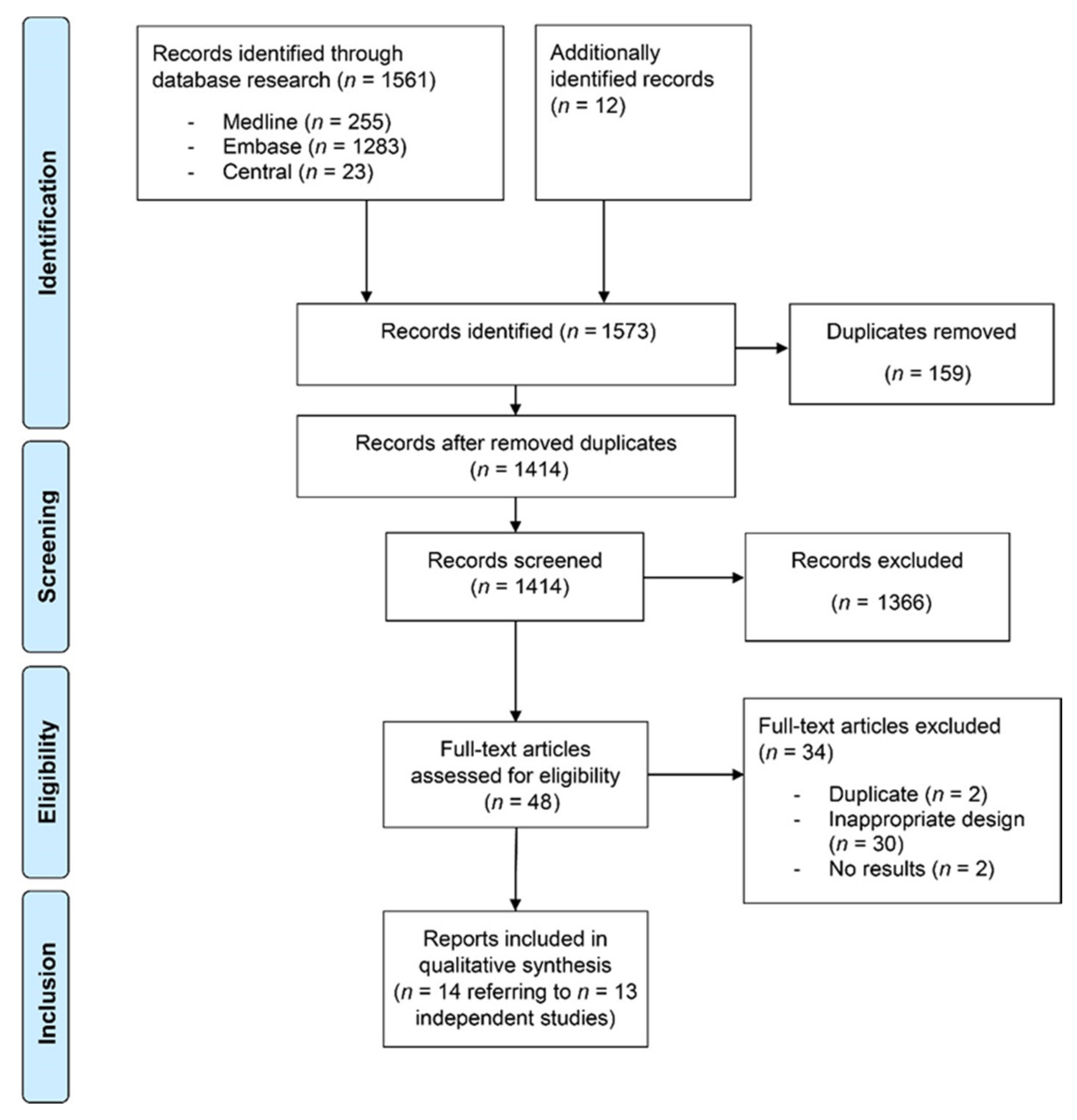
3.1. Study Identification
3.2. Study Characteristics
3.3. Outcomes
3.3.1. Prospective Studies
3.3.2. Retrospective Studies and Chart Reviews
3.4. Breslow Index of Invasive Melanoma
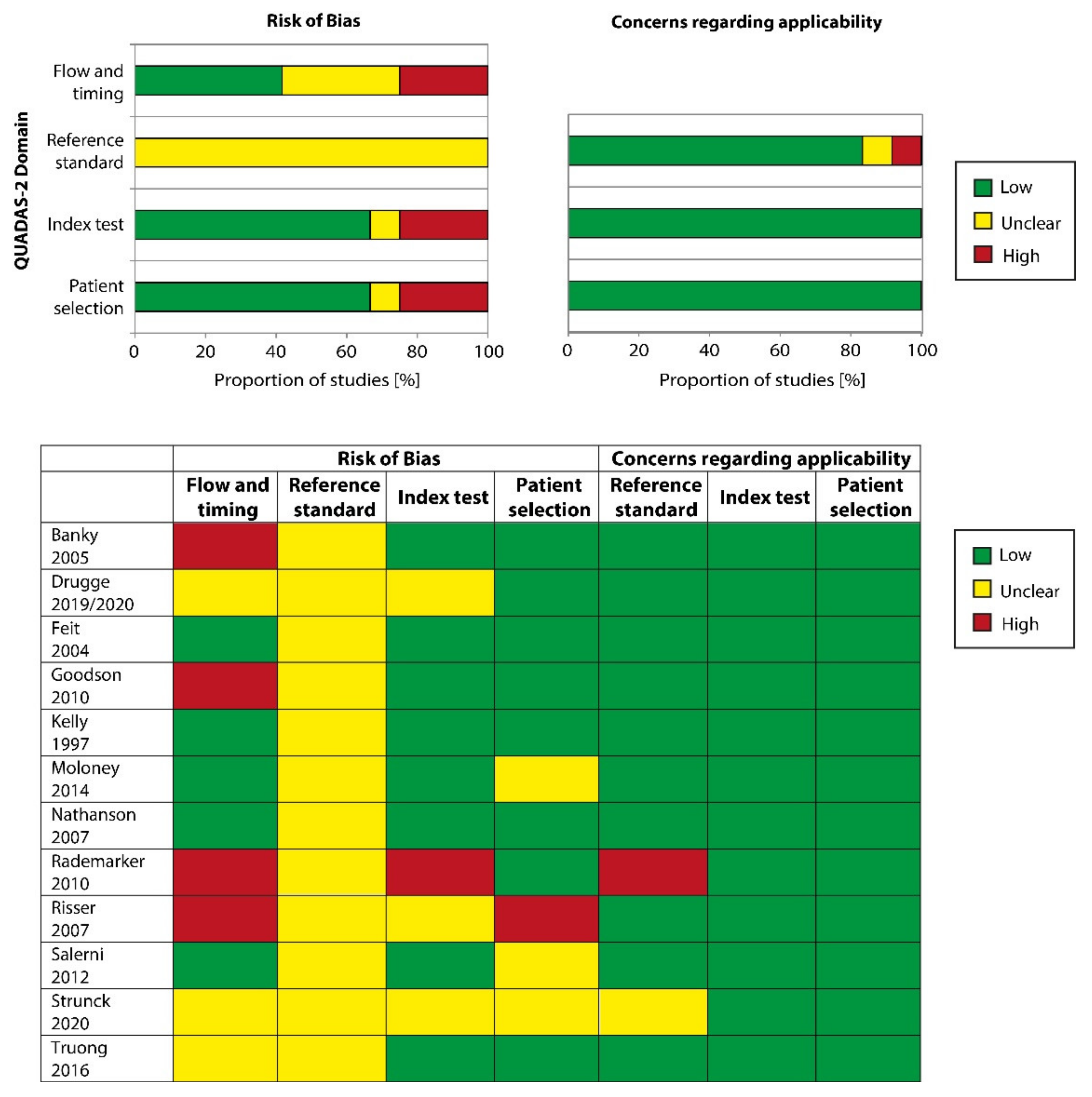
3.5. Methodological Quality of Included Studies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garbe, C.; Keim, U.; Eigentler, T.K.; Amaral, T.; Katalinic, A.; Holleczek, B.; Martus, P.; Leiter, U. Time trends in incidence and mortality of cutaneous melanoma in Germany. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1272–1280. [Google Scholar] [CrossRef]
- Glazer, A.M.; Winkelmann, R.R.; Farberg, A.S.; Rigel, D.S. Analysis of Trends in US Melanoma Incidence and Mortality. JAMA Dermatol. 2017, 153, 225–226. [Google Scholar] [CrossRef]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer; World Health Organisation (WHO). GLOBOCAN 2018: Estimated Cancer Incidence, Mortality, and Prevalence Worldwide in 2018. Available online: http://globocan.iarc.fr (accessed on 15 October 2019).
- Ugurel, S.; Rohmel, J.; Ascierto, P.A.; Flaherty, K.T.; Grob, J.J.; Hauschild, A.; Larkin, J.; Long, G.V.; Lorigan, P.; McArthur, G.A.; et al. Survival of patients with advanced metastatic melanoma: The impact of novel therapies—Update 2017. Eur. J. Cancer 2017, 83, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.A.; Wolchok, J.D.; Sznol, M. Immunotherapy of Melanoma: Facts and Hopes. Clin. Cancer Res. 2019, 25, 5191–5201. [Google Scholar] [CrossRef]
- Green, A.C.; Baade, P.; Coory, M.; Aitken, J.F.; Smithers, M. Population-based 20-year survival among people diagnosed with thin melanomas in Queensland, Australia. J. Clin. Oncol. 2012, 30, 1462–1467. [Google Scholar] [CrossRef] [PubMed]
- Lo, S.N.; Scolyer, R.A.; Thompson, J.F. Long-Term Survival of Patients with Thin (T1) Cutaneous Melanomas: A Breslow Thickness Cut Point of 0.8 mm Separates Higher-Risk and Lower-Risk Tumors. Ann. Surg. Oncol. 2018, 25, 894–902. [Google Scholar] [CrossRef]
- McKinnon, J.G.; Yu, X.Q.; McCarthy, W.H.; Thompson, J.F. Prognosis for patients with thin cutaneous melanoma: Long-term survival data from New South Wales Central Cancer Registry and the Sydney Melanoma Unit. Cancer 2003, 98, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Stadler, R.; Reusch, M.; Schafer, I.; Kornek, T.; Luger, T. Skin cancer screening in Germany—Perception by the public. J. Dtsch Dermatol. Ges. 2012, 10, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Usher-Smith, J.A.; Kassianos, A.P.; Emery, J.D.; Abel, G.A.; Teoh, Z.; Hall, S.; Neal, R.D.; Murchie, P.; Walter, F.M. Identifying people at higher risk of melanoma across the U.K.: A primary-care-based electronic survey. Br. J. Dermatol. 2017, 176, 939–948. [Google Scholar] [CrossRef]
- Williams, L.H.; Shors, A.R.; Barlow, W.E.; Solomon, C.; White, E. Identifying Persons at Highest Risk of Melanoma Using Self-Assessed Risk Factors. J. Clin. Exp. Dermatol. Res. 2011, 2, 1000129. [Google Scholar] [PubMed]
- Rayner, J.E.; Laino, A.M.; Nufer, K.L.; Adams, L.; Raphael, A.P.; Menzies, S.W.; Soyer, H.P. Clinical Perspective of 3D Total Body Photography for Early Detection and Screening of Melanoma. Front. Med. (Lausanne) 2018, 5, 152. [Google Scholar] [CrossRef]
- Halpern, A.C. Total body skin imaging as an aid to melanoma detection. Semin. Cutan. Med. Surg. 2003, 22, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Halpern, A.C. The use of whole body photography in a pigmented lesion clinic. Dermatol. Surg. 2000, 26, 1175–1180. [Google Scholar]
- Young, A.T.; Vora, N.B.; Cortez, J.; Tam, A.; Yeniay, Y.; Afifi, L.; Yan, D.; Nosrati, A.; Wong, A.; Johal, A.; et al. The role of technology in melanoma screening and diagnosis. Pigment. Cell Melanoma Res. 2020, 18. [Google Scholar] [CrossRef] [PubMed]
- Adler, N.R.; Kelly, J.W.; Guitera, P.; Menzies, S.W.; Chamberlain, A.J.; Fishburn, P.; Button-Sloan, A.E.; Heal, C.; Soyer, H.P.; Thompson, J.F. Methods of melanoma detection and of skin monitoring for individuals at high risk of melanoma: New Australian clinical practice guidelines. Med. J. Aust. 2019, 210, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Open Med. 2009, 3, e123–e130. [Google Scholar] [PubMed]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Salameh, J.P.; Bossuyt, P.M.; McGrath, T.A.; Thombs, B.D.; Hyde, C.J.; Macaskill, P.; Deeks, J.J.; Leeflang, M.; Korevaar, D.A.; Whiting, P.; et al. Preferred reporting items for systematic review and meta-analysis of diagnostic test accuracy studies (PRISMA-DTA): Explanation, elaboration, and checklist. BMJ 2020, 370, m2632. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.0; (Updated July 2019); Cochrane: London, UK, 2019; Available online: www.training.cochrane.org/handbook (accessed on 11 November 2020).
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; Group, Q. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Drugge, E.D.; Okundaye, O.I.; Sarac, R.M.; Drugge, R.J. Melanoma screening using patient self-assessed risk and total body photography. Dermatol. Online J. 2019, 25, 15. [Google Scholar]
- Risser, J.; Pressley, Z.; Veledar, E.; Washington, C.; Chen, S.C. The impact of total body photography on biopsy rate in patients from a pigmented lesion clinic. J. Am. Acad. Dermatol. 2007, 57, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Truong, A.; Strazzulla, L.; March, J.; Boucher, K.M.; Nelson, K.C.; Kim, C.C.; Grossman, D. Reduction in nevus biopsies in patients monitored by total body photography. J. Am. Acad. Dermatol. 2016, 75, 135–143.e135. [Google Scholar] [CrossRef] [PubMed]
- Goodson, A.G.; Florell, S.R.; Hyde, M.; Bowen, G.M.; Grossman, D. Comparative analysis of total body and dermatoscopic photographic monitoring of nevi in similar patient populations at risk for cutaneous melanoma. Dermatol. Surg. 2010, 36, 1087–1098. [Google Scholar] [CrossRef]
- Strunck, J.L.; Smart, T.C.; Boucher, K.M.; Secrest, A.M.; Grossman, D. Improved melanoma outcomes and survival in patients monitored by total body photography: A natural experiment. J. Dermatol. 2020, 47, 342–347. [Google Scholar] [CrossRef]
- Feit, N.E.; Dusza, S.W.; Marghoob, A.A. Melanomas detected with the aid of total cutaneous photography. Br. J. Dermatol. 2004, 150, 706–714. [Google Scholar] [CrossRef]
- Drugge, E.D.; Sarac, R.M.; Elston, D.M.; Drugge, R.J. Correlation of total body photography frequency and invasive melanoma depth. J. Am. Acad. Dermatol. 2020, 82, 768–769. [Google Scholar] [CrossRef]
- Kelly, J.W.; Yeatman, J.M.; Regalia, G.; Mason, G.; Henham, A.P. A high incidence of melanoma found in patients with multiple dysplastic naevi by photographic surveillance. Med. J. Aust. 1997, 167, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Moloney, F.; Guitera, P.; Coates, E.; Haass, N.; Ho, K.; Khoury, R.; Mann, G.; Menzies, S. Sequential digital dermoscopic imaging and total body photography aid detection of primary melanoma in individuals at high risk: A prospective 5-year follow-up study. Br. J. Dermatol. 2012, 167, 4. [Google Scholar]
- Banky, J.P.; Kelly, J.W.; English, D.R.; Yeatman, J.M.; Dowling, J.P. Incidence of new and changed nevi and melanomas detected using baseline images and dermoscopy in patients at high risk for melanoma. Arch. Dermatol. 2005, 141, 998–1006. [Google Scholar] [CrossRef]
- Salerni, G.; Carrera, C.; Lovatto, L.; Marti-Laborda, R.M.; Isern, G.; Palou, J.; Alos, L.; Puig, S.; Malvehy, J. Characterization of 1152 lesions excised over 10 years using total-body photography and digital dermatoscopy in the surveillance of patients at high risk for melanoma. J. Am. Acad. Dermatol. 2012, 67, 836–845. [Google Scholar] [CrossRef]
- Salerni, G.; Carrera, C.; Lovatto, L.; Puig-Butille, J.A.; Badenas, C.; Plana, E.; Puig, S.; Malvehy, J. Benefits of total body photography and digital dermatoscopy (“two-step method of digital follow-up”) in the early diagnosis of melanoma in patients at high risk for melanoma. J. Am. Acad. Dermatol. 2012, 67, e17–e27. [Google Scholar] [CrossRef]
- Rademaker, M.; Oakley, A. Digital monitoring by whole body photography and sequential digital dermoscopy detects thinner melanomas. J. Prim. Health Care 2010, 2, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Nathansohn, N.; Orenstein, A.; Trau, H.; Liran, A.; Schachter, J. Pigmented lesions clinic for early detection of melanoma: Preliminary results. Isr. Med. Assoc. J. 2007, 9, 708–712. [Google Scholar] [PubMed]
- Primiero, C.A.; McInerney-Leo, A.M.; Betz-Stablein, B.; Whiteman, D.C.; Gordon, L.; Caffery, L.; Aitken, J.F.; Eakin, E.; Osborne, S.; Gray, L.; et al. Evaluation of the efficacy of 3D total-body photography with sequential digital dermoscopy in a high-risk melanoma cohort: Protocol for a randomised controlled trial. BMJ Open 2019, 9, e032969. [Google Scholar] [CrossRef] [PubMed]
- Gilmore, S. Melanoma screening: Informing public health policy with quantitative modelling. PLoS ONE 2017, 12, e0182349. [Google Scholar] [CrossRef]
- Kaiser, I.; Pfahlberg, A.B.; Uter, W.; Heppt, M.V.; Veierod, M.B.; Gefeller, O. Risk Prediction Models for Melanoma: A Systematic Review on the Heterogeneity in Model Development and Validation. Int. J. Environ. Res. Public Health 2020, 17, 7919. [Google Scholar] [CrossRef]
- Vuong, K.; McGeechan, K.; Armstrong, B.K.; Cust, A.E. Risk prediction models for incident primary cutaneous melanoma: A systematic review. JAMA Dermatol. 2014, 150, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Usher-Smith, J.A.; Emery, J.; Kassianos, A.P.; Walter, F.M. Risk prediction models for melanoma: A systematic review. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1450–1463. [Google Scholar] [CrossRef] [PubMed]
- Janda, M.; Soyer, H.P. Using Advances in Skin Imaging Technology and Genomics for the Early Detection and Prevention of Melanoma. Dermatology 2019, 235, 1–3. [Google Scholar] [CrossRef]
- Brinker, T.J.; Hekler, A.; Enk, A.H.; Klode, J.; Hauschild, A.; Berking, C.; Schilling, B.; Haferkamp, S.; Schadendorf, D.; Frohling, S.; et al. A convolutional neural network trained with dermoscopic images performed on par with 145 dermatologists in a clinical melanoma image classification task. Eur. J. Cancer 2019, 111, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Tschandl, P.; Rinner, C.; Apalla, Z.; Argenziano, G.; Codella, N.; Halpern, A.; Janda, M.; Lallas, A.; Longo, C.; Malvehy, J.; et al. Human-computer collaboration for skin cancer recognition. Nat. Med. 2020, 26, 1229–1234. [Google Scholar] [CrossRef] [PubMed]
- Hekler, A.; Kather, J.N.; Krieghoff-Henning, E.; Utikal, J.S.; Meier, F.; Gellrich, F.F.; Upmeier Zu Belzen, J.; French, L.; Schlager, J.G.; Ghoreschi, K.; et al. Effects of Label Noise on Deep Learning-Based Skin Cancer Classification. Front. Med. (Lausanne) 2020, 7, 177. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Daily and Versions(R) 1946 to 04 August 2020 n = 255 |
|---|
|
| Embase 1974 to 2020 Week 31, n = 1283 |
|
| Cochrane library, n = 23 trials |
|
| Study | Design | Population | Risk Factors for Inclusion | Imaging Technique | Baseline vs. Serial TBP |
|---|---|---|---|---|---|
| Prospective Trials | |||||
| Banky 2005 | prospective single cohort | >16 years median age 38 years (range 16–74) n = 309 (female n = 168, male n = 141) Australia | >4 dysplastic nevi >100 nevi positive family history of melanoma positive personal history of melanoma | 14 baseline photographs 35 mm single-lens reflex camera dermoscopy allowed, no SDDI | baseline TBP |
| Goodson 2010 | prospective single cohort | n = 1076 USA | ≥3 atypical nevi >50 nevi personal history of melanoma positive family history of melanoma extensive lentiginosis | approx. 27 regional photographs on standard poses; additional photographs were taken to monitor atypical lesions in other regions FinePix S2 Pro digital camera dermoscopy allowed, no SDDI | baseline TBP |
| Kelly 1997 | prospective single cohort | >18 years mean age 37 years (range 18–67) n = 278 (female n = 162, male n = 116) Australia | dysplastic melanocytic nevi | systematic set of 14 baseline photographs with definition of standard views epiluminescence microscopy | baseline TBP |
| Moloney 2014 | prospective single cohort | >18 years median age 53 years (range 21–85) n = 311 Australia | 4 groups: (i) personal history of at least one invasive melanoma and dysplastic nevus syndrome (ii) personal history of at least one invasive melanoma and a family history of at least three first-degree or second-degree relatives with a confirmed history of malignant melanoma (iii) personal history of at least two primary invasive melanomas with at least one occurring in the 10 years prior to recruitment for patients with only two melanomas (iv) confirmed CDKN2A (OMIM 600160) or CDK4 (OMIM123829) gene mutation | 12–24 digital high-resolution photographs according to a standardized protocol SDDI allowed | serial TBP |
| Nathansohn 2007 | prospective single cohort | 0–82 years median age 34 years n = 895 (female n = 401, male n = 494) Israel | >20 nevi or multiple freckles multiple dysplastic nevi positive family history of melanoma children with congenital nevi | 12 MP digital single-lens reflex camera and 7 MP digital camera with polarized light dermoscope standard set of 20 photos and photos of marked lesions | serial TBP |
| Salerni 2012 | prospective single cohort | mean age 37 years n = 618 (female n = 337, male n = 281) Europe | moderate to severe atypical mole syndrome (>100 nevi and/or >10 atypical and/or dysplastic nevi) personal and/or family history of melanoma carriers of melanoma gene mutations other cancer risk conditions (congenital nevus, immunosuppression, genodermatosis) | standardized digital system for images (standardized method for total body mapping) total-body mapping with digital images SDDI allowed | serial TBP |
| Retrospective studies | |||||
| Drugge 2019 | retrospective two cohorts (TBP 1 vs. non-TBP) | >18 years median age 54 years (IQR 29) n = 4692 (2473 with TBP) USA | no special risk factors as inclusion criteria | simultaneous image capture of 25 cameras dermoscopy allowed | serial TBP |
| Drugge 2020 | retrospective single cohort | n = 218 (subgroup of Drugge 2019) USA | personal or family history of melanoma ≥4 dysplastic nevi ≥100 nevi | simultaneous image capture of 25 cameras dermoscopy allowed | serial TBP |
| Feit 2004 | retrospective single cohort | n = 576 USA | no special risk factors as inclusion criteria | standardized series of poses dermoscopy allowed, no SDDI | baseline TBP |
| Rademaker 2010 | retrospective two cohorts | n = 100 patients (female n = 53, male n = 47) with melanoma (n = 52 invasive, n = 48 in situ) mean age 51 years New Zealand | patients diagnosed with melanoma or melanoma-in-situ | panoramic views, macroscopic views and dermoscopic views Nikon D50 Digital SLR camera for panoramic images Hewlett Packard Photosmart 912 or Canon Photoshot G6 1/1.8 inch 7 megapixel CCD digital camera for macro/micro images SDDI | serial TBP |
| Risser 2007 | retrospective two cohorts (TBP vs. non-TBP) | median age 33.6 years n = 128 (female n = 71; male n = 57) USA | multiple atypical nevi | no dermoscopy | n.r. |
| Strunck 2020 | retrospective two cohorts | >18 years median age 40 years (range 18–84) n = 1955 (female n = 1179, male n = 776) US | no special risk factors as inclusion criteria | dermoscopy, but no SDDI | n.r. |
| Truong 2016 | retrospective single cohort | >18 years median age 39.0 years n = 926 (female n = 541, male n = 385) USA | no special risk factors as inclusion criteria | n.r. | n.r. |
| Study | Biopsies | Melanoma Cases | Benign-to-Malignant Ratio | Mean/Median Breslow Index | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Numbers | Due to TBP | Due to Change of Existing /Tracked Lesion | Due to Newly Emerged Lesion | Number | Due to TBP | Due to Change of Existing /Tracked Lesion | Due to Newly Emerged Lesion | |||
| Prospective Trials | ||||||||||
| Banky 2005 | n.r. | n.r. | n.r. | n.r. | 18 (19 per 1000 patient-year) | n.r. | n.r. | n.r. | 3:1 | 0.39 mm |
| Goodson 2010 | 548 in 1076 patients (0.51 biopsies per patient) 273 at initial visit 275 at follow-up | 168 | 148 of 275 | 20 of 275 | 16 at initial visit (invasive 8) 12 at follow-up (invasive 5) | n.r. | 5 | 2 | n.r. | At initial visit: median 0.39 average 0.83 mm range 0.25–>3mm At follow-up: median 0.36 mm average 0.38 mm range 0.19–0.65 mm |
| Kelly 1997 | 210 | n.r. | n.r. | n.r. | 20 melanomas in 16 patients (in situ 8; invasive 12) | 11 | n.r. | n.r. | n.r. | Median 0.40 mm |
| Moloney 2014 | n.r. | n.r. | n.r. | n.r. | 75 primary melanoma (82 absolute) 14 at baseline 61 at post-baseline | 23 | n.r. | n.r. | 4.4:1 | Median Breslow: in situ (range in situ to 0.60 mm) |
| Nathansohn 2007 | 236 | n.r. | n.r. | n.r. | 7 | n.r. | n.r. | n.r. | n.r. | n.r. |
| Salerni 2012 | 1152 in 407 patients (mean 1.86 lesions per patient) | n.r. | n.r. | n.r. | 98 in 78 patients (8.5% of excised lesions); (in situ 53) | n.r. | 60 | 38 | Monitored lesions: 11.9:1 New lesions: 8.8:1 | Median 0.5 mm |
| Retrospective Studies | ||||||||||
| Drugge 2019 | 268 biopsies in 218 patients | n.r. | n.r. | n.r. | 65 in 218 patients (in situ 39; invasive 26) In situ/ invasive ratio 1.56:1 | n.r. | n.r. | n.r. | 3.1:1 | n.r. |
| Drugge 2020 | 225 biopsies in 218 patients | n.r. | 149 of 225 | 76 of 225 | 67 of 225 biopsies (in situ 44; invasive 23) | n.r. | n.r. | n.r. | n.r. | Median 0.30 mm (range 0.12–0.65 mm) |
| Feit 2004 | 77 melanocytic lesions (93 in total) | n.r. | 47 | 27 | 27 in 12 patients (in situ 21; invasive 6) | n.r. | 20 | 5 | n.r. | Absolut values of tumors: 0.2 mm/0.25 mm/0.25 mm/0.35 mm /0.9 mm/1.1 mm |
| Study | Biopsies | Melanoma Cases | Benign-to-Malignant Ratio | Mean/Median Breslow Index | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Numbers | Due to TBP | Due to Change of Existing /Tracked Lesion | Due to Newly Emerged Lesion | Number | Due to TBP | Due to Change of Existing /Tracked Lesion | Due to Newly Emerged Lesion | |||
| Retrospective Studies | ||||||||||
| Rademaker 2010 | n.r. | n.r. | n.r. | n.r. | n.r. | n.r. | n.r. | n.r. | n.r. | Breslow index with TBP (vs. register data): <0.75 mm: 69% (vs. 52%) 0.76–1.49: 21% (vs. 22%) 1.5-3.0: 8% (vs. 15%) >3.0 mm: 2% (vs. 11%) First visit average 0.87 mm (range 0.3–3.35) Follow-up average 0.67 (range 0.22–1.60 mm |
| Risser 2007 | Mean: 0.81 TBSE: 0.82 (51 in 29 patients) TBP: 0.8 (53 in 28 patients) | n.r. | n.r. | n.r. | TBSE: 3 in 19 patients TBP: 0 in 16 patients | n.r. | n.r. | n.r. | n.r. | Absolute: 0.3, 0.44 and 1.1 mm |
| Strunck 2020 | n.r. | n.r. | n.r. | n.r. | 121 (in situ 51, invasive 70) | 54 changing; 11 new | 65 | 12 | Median depth - 0.33 mm in follow-up group (range 0.11–1.5) - 0.83 mm in control group without follow-up (range 0.11–3.3) Median depth, if TBP was used: - 0.31 mm (range 0.11–1.5) Median depth without use of TBP: - 0.48 mm (0.10–3.3) | |
| Truong 2016 | Pre-TBP 3489 biopsies in 589 patients (mean 5.92) Post-TBP 921 biopsies in 589 patients (mean 1.56) | n.r. | n.r. | n.r. | Pre-TBP: 278 biopsies with 32 melanomas (in situ 14; invasive 18) Post-TBP: 1419 biopsies with 93 melanomas (in situ 46; invasive 47) | n.r. | n.r. | n.r. | Pre-TBP 7.7 Post-TBP 14.3 | Range: - Pre-TBP: 0.2–3.0 mm - Post-TBP: 0.11–2.1 mm |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hornung, A.; Steeb, T.; Wessely, A.; Brinker, T.J.; Breakell, T.; Erdmann, M.; Berking, C.; Heppt, M.V. The Value of Total Body Photography for the Early Detection of Melanoma: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1726. https://doi.org/10.3390/ijerph18041726
Hornung A, Steeb T, Wessely A, Brinker TJ, Breakell T, Erdmann M, Berking C, Heppt MV. The Value of Total Body Photography for the Early Detection of Melanoma: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(4):1726. https://doi.org/10.3390/ijerph18041726
Chicago/Turabian StyleHornung, Annkathrin, Theresa Steeb, Anja Wessely, Titus J. Brinker, Thomas Breakell, Michael Erdmann, Carola Berking, and Markus V. Heppt. 2021. "The Value of Total Body Photography for the Early Detection of Melanoma: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 4: 1726. https://doi.org/10.3390/ijerph18041726
APA StyleHornung, A., Steeb, T., Wessely, A., Brinker, T. J., Breakell, T., Erdmann, M., Berking, C., & Heppt, M. V. (2021). The Value of Total Body Photography for the Early Detection of Melanoma: A Systematic Review. International Journal of Environmental Research and Public Health, 18(4), 1726. https://doi.org/10.3390/ijerph18041726