Effects of the Amount and Frequency of Fluid Intake on Cognitive Performance and Mood among Young Adults in Baoding, Hebei, China: A Randomized Controlled Trial




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants Recruitment
2.2. Sample Size Calculation
2.3. Ethical Review
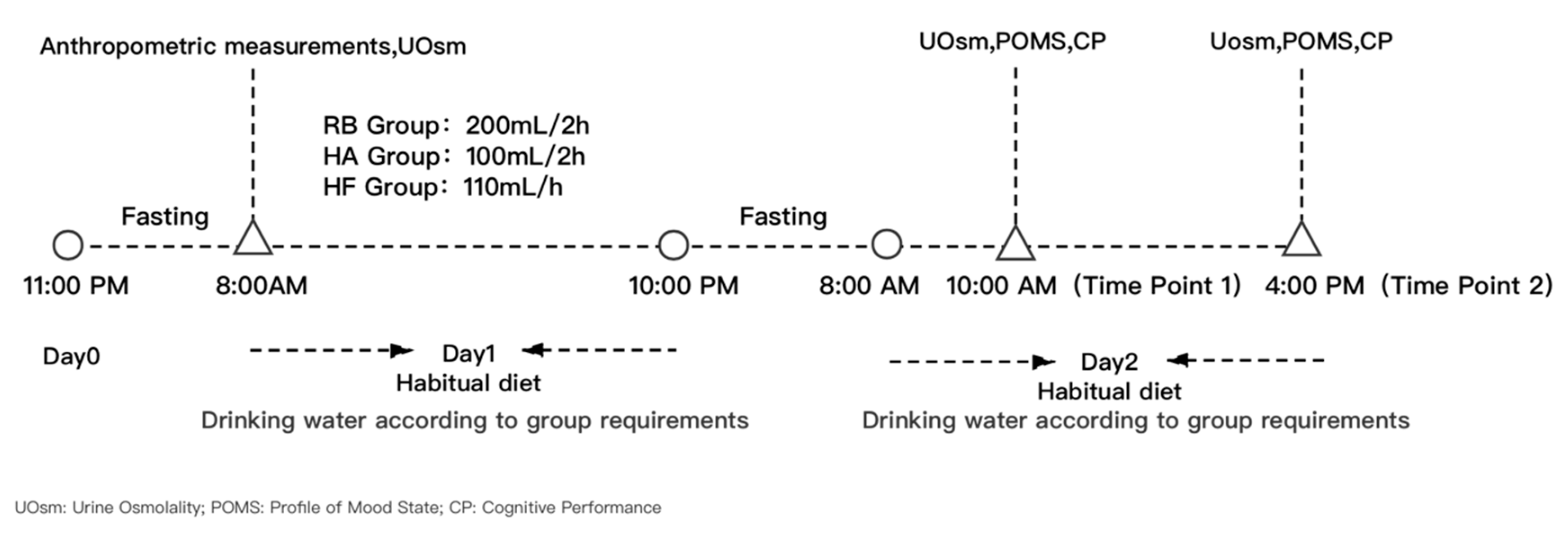
2.4. Study Procedure
2.5. Anthropometric Measurements
2.6. Assessment of Hydration Status
2.7. Assessment of Cognitive Performance
2.8. Assessment of Mood
2.9. Temperature and Humidity of the Environment
2.10. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
3.2. Temperature and Humidity
3.3. Effects of Different Amounts and Frequencies of Fluid Intake on Hydration Status
3.4. Effects of Different Amounts and Frequencies of Fluid Intake on Cognitive Performance and Mood
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| RB group | Recommended behavior group |
| HA group | Half amount group |
| HF group | High frequency group |
| Uosm | Urine osmolality |
| CP | Cognitive performance |
| BMI | Body mass index |
| TMD | Total mood disturbance |
| POMS | Profile of Mood State |
Appendix A

{kind=link}
| Indoors | Outdoors | |||
|---|---|---|---|---|
| Temperature (°C) | Humidity (%RH) | Temperature (°C) | Humidity (%RH) | |
| Day 1—10 a.m. | 25.1 | 73.0 | 23.2 | 70.0 |
| Day 1—2 p.m. | 25.4 | 72.0 | 26.2 | 73.0 |
| Day 1—8 p.m. | 24.9 | 70.0 | 24.9 | 72.0 |
| Day 2—10 a.m. | 24.4 | 70.0 | 25.7 | 72.0 |
| Day 2—2 p.m. | 25.6 | 71.0 | 25.8 | 79.0 |
| Day 2—8 p.m. | 25.2 | 70.0 | 25.6 | 73.0 |
| F | 2.295 | 2.571 | 4.550 | 4.129 |
| p | 0.204 | 0.184 | 0.100 | 0.112 |
References
- Chinese Nutrition Society. Chinese Dietary Reference Intakes 2013; Science Press: Beijing, China, 2014; p. 442. [Google Scholar]
- Jéquier, E.; Constant, F. Water as an essential nutrient: The physiological basis of hydration. Eur. J. Clin. Nutr. 2010, 64, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Białecka-Dębek, A.; Pietruszka, B. The association between hydration status and cognitive function among free-living elderly volunteers. Aging Clin. Exp. Res. 2019, 31, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Clark, W.F.; Sontrop, J.M.; Huang, S.-H.; Moist, L.; Bouby, N.; Bankir, L. Hydration and Chronic Kidney Disease Progression: A Critical Review of the Evidence. Am. J. Nephrol. 2016, 43, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Nuccio, R.P.; Barnes, K.A.; Carter, J.M.; Baker, L.B. Fluid Balance in Team Sport Athletes and the Effect of Hypohydration on Cognitive, Technical, and Physical Performance. Sports Med. 2017, 47, 1951–1982. [Google Scholar] [CrossRef]
- Masento, N.A.; Golightly, M.; Field, D.T.; Butler, L.T.; van Reekum, C.M. Effects of hydration status on cognitive performance and mood. Br. J. Nutr. 2014, 111, 1841–1852. [Google Scholar] [CrossRef]
- Mix, J.; Elon, L.; Vi Thien Mac, V.; Flocks, J.; Economos, E.; Tovar-Aguilar, A.J.; Stover Hertzberg, V.; McCauley, L.A. Hydration Status, Kidney Function, and Kidney Injury in Florida Agricultural Workers. J. Occup. Environ. Med. 2018, 60, e253–e260. [Google Scholar] [CrossRef]
- Siegel, A.J. Fatal water intoxication and cardiac arrest in runners during marathons: Prevention and treatment based on validated clinical paradigms. Am. J. Med. 2015, 128, 1070–1075. [Google Scholar] [CrossRef]
- Sawka, M.N.; Latzka, W.A.; Matott, R.P.; Montain, S.J. Hydration effects on temperature regulation. Int. J. Sports Med. 1998, 19 (Suppl. 2), S108–S110. [Google Scholar] [CrossRef]
- European Food Safety Authority. Scientific opinion on dietary reference values for water. EFSA J. 2010, 8, 1459. [Google Scholar]
- Armstrong, L.E.; Johnson, E.C. Water Intake, Water Balance, and the Elusive Daily Water Requirement. Nutrients 2018, 10, 1928. [Google Scholar] [CrossRef]
- Zhang, J.F.; Zhang, N.; He, H.R.; Cai, H.; Yan, X.Y.; Guo, X.H.; Li, Y.B.; Zhang, M.; Ma, G.S. The total fluids intake, volume of urine and hydration status among young adults from Hebei Province in spring. Zhonghua Yu Fang Yi Xue Za Zhi [Chin. J. Prev. Med.] 2019, 53, 355–359. [Google Scholar] [CrossRef]
- Zhang, N.; Morin, C.; Guelinckx, I.; Moreno, L.A.; Kavouras, S.A.; Gandy, J.; Martinez, H.; Salas-Salvadó, J.; Ma, G. Fluid intake in urban China: Results of the 2016 Liq.In (7) national cross-sectional surveys. Eur. J. Nutr. 2018, 57, 77–88. [Google Scholar] [CrossRef]
- Perrier, E.T.; Buendia-Jimenez, I.; Vecchio, M.; Armstrong, L.E.; Tack, I.; Klein, A. Twenty-four-hour urine osmolality as a physiological index of adequate water intake. Dis. Markers 2015, 2015, 231063. [Google Scholar] [CrossRef] [PubMed]
- Benton, D.; Jenkins, K.T.; Watkins, H.T.; Young, H.A. Minor degree of hypohydration adversely influences cognition: A mediator analysis. Am. J. Clin. Nutr. 2016, 104, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Young, H.A.; Cousins, A.; Johnston, S.; Fletcher, J.M.; Benton, D. Autonomic adaptations mediate the effect of hydration on brain functioning and mood: Evidence from two randomized controlled trials. Sci. Rep. 2019, 9, 16412. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J.; Shirreffs, S.M.; Leiper, J.B. Errors in the estimation of hydration status from changes in body mass. J. Sports Sci. 2007, 25, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.S.; Zuo, J.L. [Adequate water intakes]. Zhonghua Yu Fang Yi Xue Za Zhi 2011, 45, 675–676. [Google Scholar] [CrossRef] [PubMed]
- Merhej, R. Dehydration and cognition: An understated relation. Int. J. Health Gov. 2019, 24, 19–30. [Google Scholar] [CrossRef]
- Stachenfeld, N.S.; Leone, C.A.; Mitchell, E.S.; Freese, E.; Harkness, L. Water intake reverses dehydration associated impaired executive function in healthy young women. Physiol. Behav. 2018, 185, 103–111. [Google Scholar] [CrossRef]
- Chard, A.N.; Trinies, V.; Edmonds, C.J.; Sogore, A.; Freeman, M.C. The impact of water consumption on hydration and cognition among schoolchildren: Methods and results from a crossover trial in rural Mali. PLoS ONE 2019, 14, e0210568. [Google Scholar] [CrossRef]
- Broad, E.M.; Burke, L.M.; Cox, G.R.; Heeley, P.; Riley, M. Body weight changes and voluntary fluid intakes during training and competition sessions in team sports. Int. J. Sport Nutr. 1996, 6, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Dugas, J.P.; Noakes, T.D. Hyponatraemic encephalopathy despite a modest rate of fluid intake during a 109 km cycle race. Br. J. Sports Med. 2005, 39, e38. [Google Scholar] [CrossRef] [PubMed]
- Dugas, J.P.; Oosthuizen, U.; Tucker, R.; Noakes, T.D. Rates of fluid ingestion alter pacing but not thermoregulatory responses during prolonged exercise in hot and humid conditions with appropriate convective cooling. Eur. J. Appl. Physiol. 2009, 105, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, E.M.R.; Schmahl, R.M.; Senden, J.M.G.; Brouns, F. Effect of high and low rates of fluid intake on post-exercise rehydration. Int. J. Sport Nutr. Exerc. Metab. 2002, 12, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Pross, N.; Demazières, A.; Girard, N.; Barnouin, R.; Metzger, D.; Klein, A.; Perrier, E.; Guelinckx, I. Effects of changes in water intake on mood of high and low drinkers. PLoS ONE 2014, 9, e94754. [Google Scholar] [CrossRef]
- Zhang, N.; Du, S.M.; Zhang, J.F.; Ma, G.S. Effects of Dehydration and Rehydration on Cognitive Performance and Mood among Male College Students in Cangzhou, China: A Self-Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 1891. [Google Scholar] [CrossRef]
- Yang, Y.X.; Wang, X.L.; Leong, P.M.; Zhang, H.M.; Yang, X.G.; Kong, L.Z.; Zhai, F.Y.; Cheng, Y.Y.; Guo, J.S.; Su, Y.X. New Chinese dietary guidelines: Healthy eating patterns and food-based dietary recommendations. Asia Pac. J. Clin. Nutr. 2018, 27, 908–913. [Google Scholar] [CrossRef]
- Bar-David, Y.; Urkin, J.; Landau, D.; Bar-David, Z.; Pilpel, D. Voluntary dehydration among elementary school children residing in a hot arid environment. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2009, 22, 455–460. [Google Scholar] [CrossRef]
- Jaeger, J. Digit Symbol Substitution Test: The Case for Sensitivity over Specificity in Neuropsychological Testing. J. Clin. Psychopharmacol. 2018, 38, 513–519. [Google Scholar] [CrossRef]
- Wu, Y.H.; de Rotrou, J.; Vidal, J.S.; Jeandel, C.; Rigaud, A.S.; Kesse-Guyot, E.; Hanon, O. The K-T cancellation test in the older adults: Normative data and construct validity. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2013, 20, 429–442. [Google Scholar] [CrossRef]
- Wu, Y.H.; de Rotrou, J.; Sikkes, S.A.; Rigaud, A.S.; Plichart, M. Clinical utility of the K-T cancellation test in a memory clinic population. J. Clin. Exp. Neuropsychol. 2016, 38, 1094–1102. [Google Scholar] [CrossRef] [PubMed]
- Conway, A.R.; Kane, M.J.; Bunting, M.F.; Hambrick, D.Z.; Wilhelm, O.; Engle, R.W. Working memory span tasks: A methodological review and user’s guide. Psychon. Bull. Rev. 2005, 12, 769–786. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-j.; Yun, X.-p. Reliability and validity of Chinese version of Rivermead Behavioural Memory Test-third edition among Chinese population. Chin. J. Rehabil. Theory Pract. 2016, 22, 511–513. [Google Scholar] [CrossRef]
- Shepard, R.N.; Feng, C. A chronometric study of mental paper folding. Cogn. Psychol. 1972, 3, 228–243. [Google Scholar] [CrossRef]
- Grove, J.R.; Prapavessis, H. Preliminary evidence for the reliability and validity of an abbreviated Profile of Mood States. Int. J. Sport Psychol. 1992, 23, 93–109. [Google Scholar] [CrossRef]
- Pross, N. Effects of Dehydration on Brain Functioning: A Life-Span Perspective. Ann. Nutr. Metab. 2017, 70 (Suppl. 1), 30–36. [Google Scholar] [CrossRef]
- Liska, D.; Mah, E.; Brisbois, T.; Barrios, P.L.; Baker, L.B.; Spriet, L.L. Narrative Review of Hydration and Selected Health Outcomes in the General Population. Nutrients 2019, 11, 70. [Google Scholar] [CrossRef]
- Bell, L.; Lamport, D.J.; Field, D.T.; Butler, L.T.; Williams, C.M. Practice effects in nutrition intervention studies with repeated cognitive testing. Nutr. Healthy Aging 2018, 4, 309–322. [Google Scholar] [CrossRef]
- Cerulla, N.; Arcusa, A.; Navarro, J.B.; de la Osa, N.; Garolera, M.; Enero, C.; Chico, G.; Fernandez-Morales, L. Cognitive impairment following chemotherapy for breast cancer: The impact of practice effect on results. J. Clin. Exp. Neuropsychol. 2019, 41, 290–299. [Google Scholar] [CrossRef]

| Age (years) | Height (cm) | Weight (kg) | Body Mass Index (BMI) (kg/m2) | |
|---|---|---|---|---|
| Recommended behavior (RB) group (n = 29, 15 males) | 19.7 ± 1.3 | 166.8 ± 7.5 | 62.4 ± 12.4 | 21.6 ± 5.6 |
| Half amount (HA) group (n = 32, 16 males) | 19.7 ± 1.4 | 165.0 ± 9.0 | 60.9 ± 10.2 | 22.4 ± 3.4 |
| High frequency (HF) group (n = 31, 15 males) | 19.9 ± 1.1 | 163.1 ± 6.7 | 60.1 ± 9.9 | 22.5 ± 3.0 |
| Total (n = 92) | 19.8 ± 1.2 | 164.9 ± 7.9 | 61.0 ± 10.8 | 22.2 ± 4.1 |
| p | 0.724 | 0.190 | 0.715 | 0.654 |
| UOsm | p | Hydration Status (n (%)) | p | ||||
|---|---|---|---|---|---|---|---|
| Optimal Hydration | Euhydration | Dehydration | |||||
| Baseline | RB group | 604 ± 222 | 0.800 | 9 (31.0) | 14 (48.3) | 6 (20.7) | 0.564 |
| HA group | 625 ± 238 | 14 (43.8) | 9 (28.1) | 9 (28.1) | |||
| HF group | 643 ± 216 | 10 (32.3) | 12 (38.7) | 9 (29.0) | |||
| Time Point 1 | RB group | 646 ± 210 a | <0.001 | 5 (17.2) a | 18 (62.1) a | 6 (20.7) a | 0.003 |
| HA group | 934 ± 219 b | 1 (3.1) b | 9 (28.1) b | 22 (68.8) b | |||
| HF group | 682 ± 215 c | 5 (16.1) a,b | 15 (48.4) a,b | 11 (35.5) a,b | |||
| Time Point 2 | RB group | 583 ± 291 a | <0.001 | 13 (44.8) | 7 (24.1) | 9 (31.0) | 0.058 |
| HA group | 792 ± 281 b | 7 (21.9) | 10 (31.2) | 15 (46.9) | |||
| HF group | 509 ± 244 c | 17 (54.8) | 10 (32.3) | 4 (12.9) | |||
| Time Point 1 | Time Point 2 | |||||
|---|---|---|---|---|---|---|
| RB Group | HA Group | HF Group | RB Group | HA Group | HF Group | |
| Digit symbol substitution test | 66.2 ± 8.9 | 69.9 ± 9.8 | 70.2 ± 11.6 | 75.5 ± 11.3 | 76.6 ± 9.7 | 76.4 ± 9.2 |
| Number cancellation test | 12.1 ± 2.7 | 12.1 ± 3.0 | 11.9 ± 2.8 | 13.7 ± 2.5 | 13.3 ± 2.2 | 13.7 ± 2.4 |
| Working memory span test | 9.8 ± 2.0 | 9.4 ± 1.9 | 9.6 ± 2.2 | 10.2 ± 2.0 | 10.0 ± 1.7 | 10.1 ± 1.9 |
| Portrait memory test | 7.5 ± 5.1 #† | 13.2 ± 9.1 #* | 20.7 ± 9.1 *† | 22.6 ± 8.4 | 20.8 ± 7.4 | 21.8 ± 7.5 |
| Paper-folding test | 30.5 ± 6.8 | 29.2 ± 5.5 | 29.2 ± 4.8 | 34.3 ± 5.1 | 33.4 ± 4.7 | 35.0 ± 3.3 |
| Time Point 1 | Time Point 2 | |||||
|---|---|---|---|---|---|---|
| RB Group | HA Group | HF Group | RB Group | HA Group | HF Group | |
| Tension | 2.8 ± 2.3 | 3.2 ± 3.2 | 3.5 ± 3.7 | 2.2 ± 2.2 | 2.8 ± 3.6 | 3.5 ± 3.7 |
| Anger | 2.0 ± 2.7 | 2.9 ± 4.4 | 3.1 ± 4.4 | 1.5 ± 1.9 | 1.8 ± 3.1 | 3.1 ± 4.4 |
| Fatigue | 2.6 ± 2.8 | 4.0 ± 4.3 | 3.9 ± 3.7 | 2.7 ± 2.7 | 3.0 ± 3.4 | 3.9 ± 3.7 |
| Depression | 1.7 ± 1.8 | 2.0 ± 2.7 | 3.2 ± 4.2 | 1.1 ± 1.4 | 1.8 ± 2.8 | 3.2 ± 4.2 |
| Confusion | 2.9 ± 2.8 | 3.2 ± 2.7 | 3.7 ± 3.2 | 2.5 ± 2.5 | 3.3 ± 3.2 | 3.7 ± 3.2 |
| Vigor | 12.4 ± 4.2 #† | 9.2 ± 4.9 # | 9.0 ± 4.3 † | 11.8 ± 4.2 #† | 9.1 ± 4.7 # | 9.0 ± 4.3 † |
| Esteem | 7.4 ± 3.6 | 6.1 ± 3.7 | 6.4 ± 3.5 | 7.5 ± 3.6 | 5.8 ± 3.4 | 6.4 ± 3.5 |
| TMD | 92.1 ± 13.0 | 100.0 ± 17.0 | 101.9 ± 18.8 | 90.8 ± 12.9 | 97.8 ± 16.2 | 101.9 ± 18.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, H.; Zhang, J.; Zhang, N.; Du, S.; Liu, S.; Ma, G. Effects of the Amount and Frequency of Fluid Intake on Cognitive Performance and Mood among Young Adults in Baoding, Hebei, China: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 8813. https://doi.org/10.3390/ijerph17238813
He H, Zhang J, Zhang N, Du S, Liu S, Ma G. Effects of the Amount and Frequency of Fluid Intake on Cognitive Performance and Mood among Young Adults in Baoding, Hebei, China: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(23):8813. https://doi.org/10.3390/ijerph17238813
Chicago/Turabian StyleHe, Hairong, Jianfen Zhang, Na Zhang, Songming Du, Shufang Liu, and Guansheng Ma. 2020. "Effects of the Amount and Frequency of Fluid Intake on Cognitive Performance and Mood among Young Adults in Baoding, Hebei, China: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 23: 8813. https://doi.org/10.3390/ijerph17238813
APA StyleHe, H., Zhang, J., Zhang, N., Du, S., Liu, S., & Ma, G. (2020). Effects of the Amount and Frequency of Fluid Intake on Cognitive Performance and Mood among Young Adults in Baoding, Hebei, China: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 17(23), 8813. https://doi.org/10.3390/ijerph17238813