Media Exposure and Anxiety during COVID-19: The Mediation Effect of Media Vicarious Traumatization

Abstract
1. Introduction
1.1. Crisis Event, Anxiety, and Media Dependence
1.2. Media Exposure and Vicarious Traumatization
1.3. Factors Moderating the Impact of Vicarious Traumatization
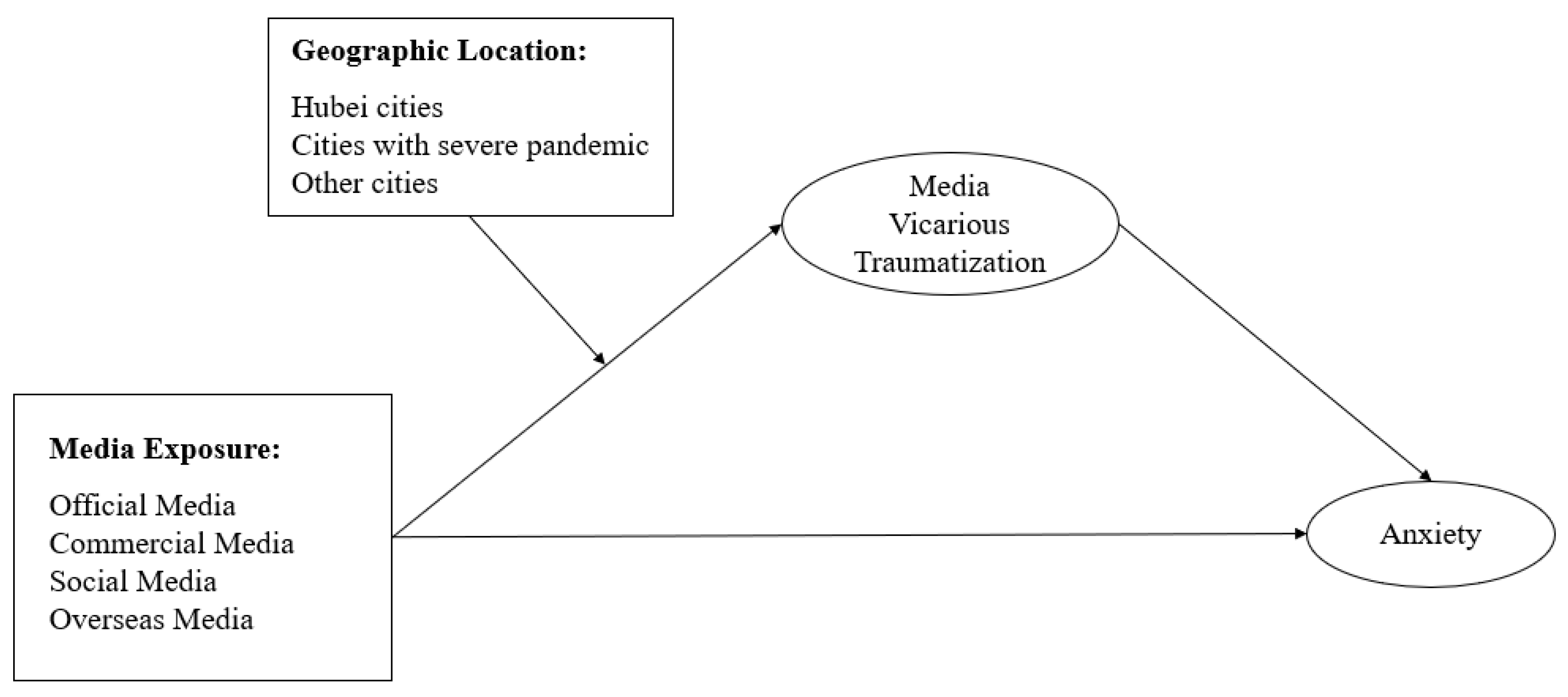
1.4. The Current Study
2. Materials and Methods
2.1. Data Collection
2.2. Participants
2.3. Measurements
2.3.1. Media Exposure in Terms of Time Length and Media Sources
2.3.2. Media Vicarious Traumatization
2.3.3. Anxiety Status
2.4. Statistical Analysis
3. Results
3.1. Media Exposure and Anxiety Status during COVID-19
3.1.1. Media Exposure
3.1.2. Anxiety Status
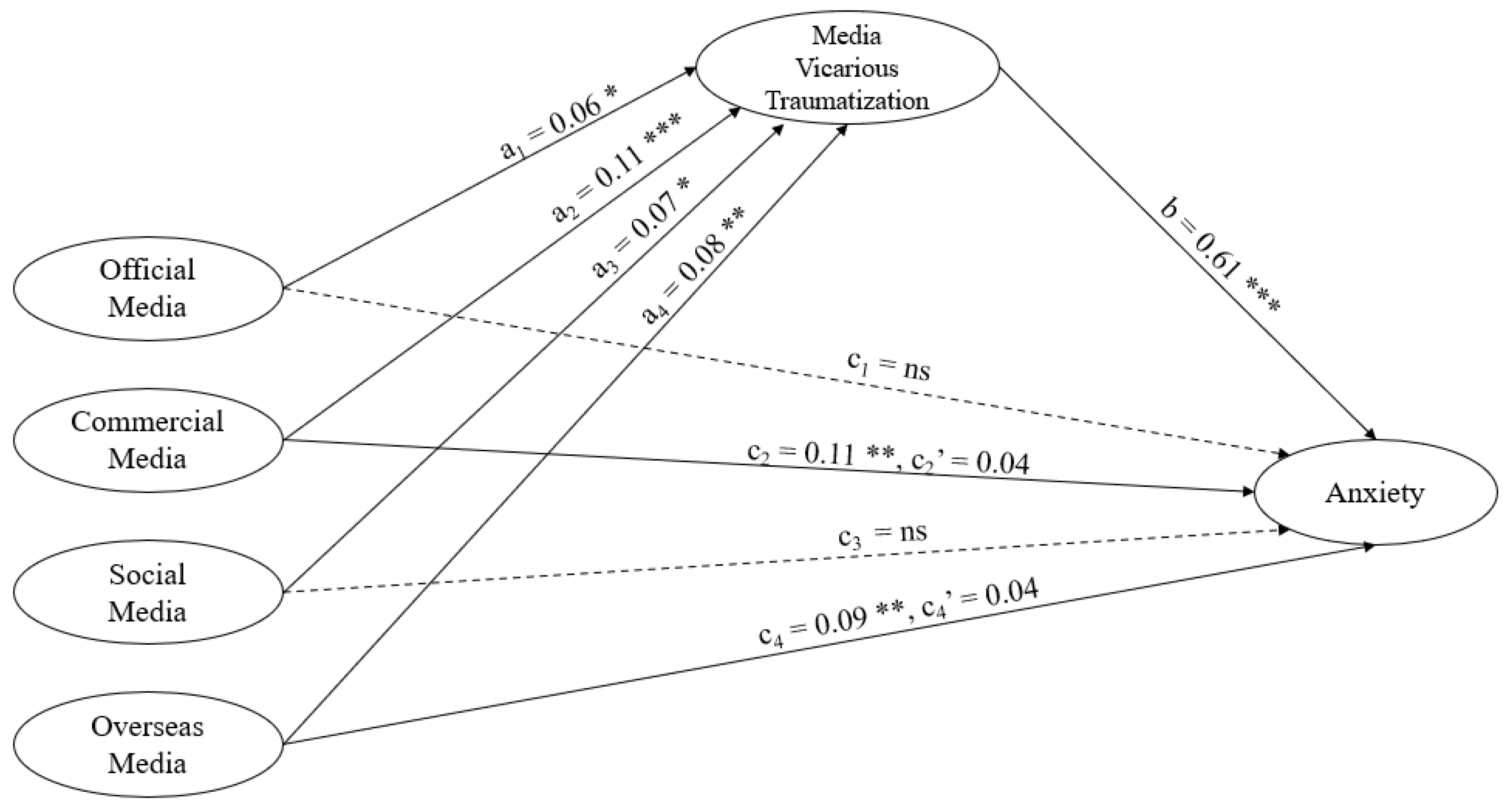
3.2. Mediation Effect of Media Vicarious Traumatization
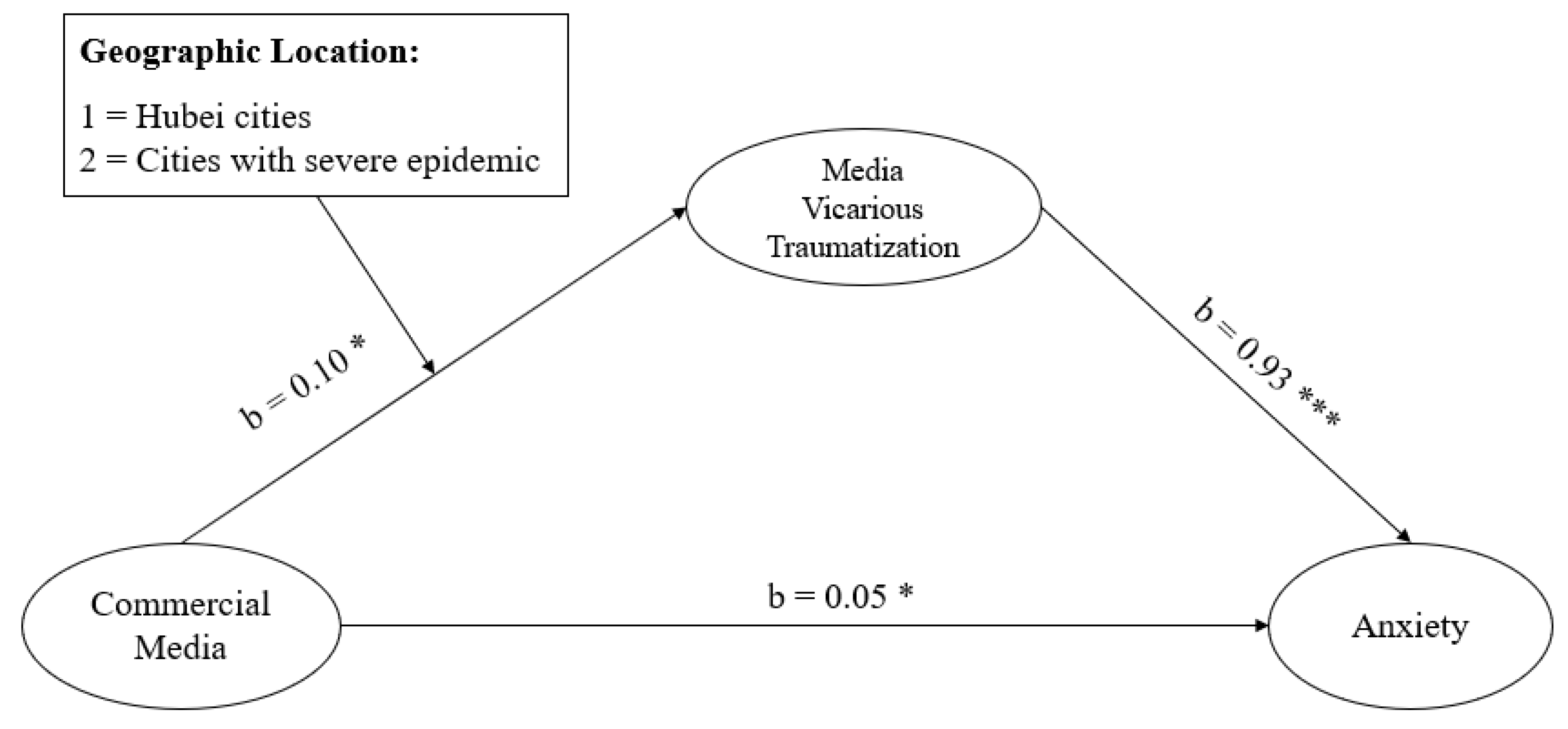
3.3. Moderation Effect of Geographic Location
4. Discussion
4.1. Media Vicarious Traumatization
4.2. Comparisons Between Commercial Media and Other Media Sources
4.3. Implications
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questionnaires | Indicators |
|---|---|
| Demographics | |
| Sex | 1 = male 2 = female |
| Age | 1 = below 18 2 = 18–25 3 = 26–30 4 = 31–35 5 = 36–40 6 = 41–50 7 = above 50 |
| Education | 1 = primary school 2 = middle school 3 = high school 4 = college/university 5 = postgraduate |
| Social Economic Status | 1 = lower class 2 = lower to middle class 3 = middle class 4 = middle to upper class 5 = upper class |
| Health Condition | 1 = very poor 2 = relatively poor 3 = average 4 = relatively good 5 = very good |
| Location | 1 = Hubei (Wuhan) 2 = Hubei (excluding Wuhan) 3 = cities with severe pandemic (including Beijing, Shanghai, Chongqing, Guangzhou, Shenzhen, and Wenzhou) 4 = other cities |
| Accommodation | 1 = staying with family 2 = staying with friends/colleagues/classmates/roommates 3 = staying alone |
| Media Exposure | |
| 1. Time spent on coronavirus information each day | 1 = hardly ever 2 = less than an hour 3 = 1–3 h 4 = 3–5 h 5 = more than 5 h |
| 2. Time spent on information irrelevant to coronavirus each day | 1 = hardly ever 2 = less than an hour 3 = 1–3 h 4 = 3–5 h 5 = more than 5 h |
| 3. Use of different media sources—official media (e.g., CCTV, People’s Daily, Hubei Daily) | 1 = never 5 = often |
| 4. Use of different media sources—commercial media (e.g., The Paper, Sanlian Life Week, Caixin) | 1 = never 5 = often |
| 5. Use of different media sources—social media (e.g., WeChat, Weibo, TikTok) | 1 = never 5 = often |
| 6. Use of different media sources—overseas media | 1 = never 5 = often |
| Media Vicarious Traumatization | |
| 1. I was exposed to distressing news and experiences via media. | 1 = strongly disagree 5 = strongly agree |
| 2. I find myself distressed by reading the stories and situations on media. | 1 = strongly disagree 5 = strongly agree |
| 3. It is hard to stay positive and optimistic given some of the information I get from the media. | 1 = strongly disagree 5 = strongly agree |
| 4. I find myself thinking about distressing news on media. | 1 = strongly disagree 5 = strongly agree |
| 5. Sometimes I feel helpless because I cannot give help to people in need. | 1 = strongly disagree 5 = strongly agree |
| 6. Sometimes I feel overwhelmed by reading the media reports. | 1 = strongly disagree 5 = strongly agree |
| 7. I find it difficult to deal with the media content. | 1 = strongly disagree 5 = strongly agree |
| Anxiety Status | |
| 1. I feel nervous and anxious due to the coronavirus pandemic. | 1 = strongly disagree 5 = strongly agree |
| 2. I have sleeping problems during the coronavirus pandemic. | 1 = strongly disagree 5 = strongly agree |
| 3. I feel panicky and cannot sit still easily during the coronavirus pandemic. | 1 = strongly disagree 5 = strongly agree |
References
- Chan, J.F.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef]
- The Government of Wuhan. Available online: http://www.wuhan.gov.cn/zwgk/tzgg/202003/t20200316_972434.shtml (accessed on 18 June 2020).
- China Center for Disease Control Prevention. Available online: http://2019ncov.chinacdc.cn/2019-nCoV/ (accessed on 18 June 2020).
- Public Health Emergency of International Concern declared by WHO. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 18 June 2020).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 18 June 2020).
- Seeger, M.; Sellnow, T.L.; Ulmer, R.R. Communication and Organizational Crisis; Praeger: Westport, CT, USA, 2003. [Google Scholar]
- Wang, J.; Gao, W. Xin Guan Fei Yan Yi Qing Xia De She Hui Xin Tai Diao Cha Bao Gao [Social psychology survey under novel coronavirus pneumonia: An analysis based on the survey data of 24–25 January 2020]. Governance 2020, Z1, 55–64. [Google Scholar]
- PEW Research Center. Available online: https://www.pewsocialtrends.org/2020/03/30/most-americans-say-coronavirus-ou (accessed on 29 April 2020).
- Sarault, J. Understanding Media Consumption during the Coronavirus Pandemic. Available online: https://www.comscore.com/Insights/Presentations-and-Whitepapers/2020/Understanding-Media-Consumption-During-the-Coronavirus-Pandemic (accessed on 29 April 2020).
- Ball-Rokeach, S.J.; DeFleur, M.L. A dependency model of mass-media effects. Commun. Res. 1976, 3, 3–21. [Google Scholar] [CrossRef]
- Lowrey, W. Media dependency during a large-scale social disruption: The case of September 11. Mass Commun. Soc.S 2004, 7, 339–357. [Google Scholar] [CrossRef]
- Mukkamala, A.; Beck, R. The role of social media for collective behaviour development in response to natural disasters. In Proceedings of the ECIS 2018, Portsmouth, UK, 23–28 June 2018. [Google Scholar]
- Martínez-Rojas, M.; Pardo-Ferreira, M.D.C.; Rubio-Romero, J.C. Twitter as a tool for the management and analysis of emergency situations: A systematic literature review. Int. J. Inf. Manag. 2018, 43, 196–208. [Google Scholar] [CrossRef]
- Burnap, P.; Williams, M.L.; Sloan, L.; Rana, O.; Housley, W.; Edwards, A.; Knight, V.; Procter, R.; Voss, A. Tweeting the terror: Modelling the social media reaction to the woolwich terrorist attack. Soc. Netw. Anal. Min. 2014, 4, 206. [Google Scholar] [CrossRef]
- Berger, C.R. Communicating under uncertainty. In Interpersonal Processes: New Directions for Communication Research; Roloff, M.E., Miller, G.R., Eds.; Sage: Newberry Park, CA, USA, 1987; Volume 14, pp. 39–62. [Google Scholar]
- Brashers, D.E.; Neidig, J.L.; Haas, S.M.; Dobbs, L.K.; Cardillo, L.W.; Russell, J.A. Communication in the management of uncertainty: The case of persons living with HIV or AIDS. Commun. Monogr. 2000, 67, 63–84. [Google Scholar] [CrossRef]
- Chen, C.Y.; Hong, R.Y. Intolerance of uncertainty moderates the relation between negative life events and anxiety. Pers. Individ. Differ. 2010, 49, 49–53. [Google Scholar] [CrossRef]
- Ladouceur, R.; Gosselin, P.; Dugas, M.J. Experimental manipulation of intolerance of uncertainty: A study of the theoretical model of worry. Behav. Res. Ther. 2000, 38, 933–941. [Google Scholar] [CrossRef]
- Taha, S.A.; Matheson, K.; Anisman, H. H1N1 was not all that scary: Uncertainty and stressor appraisals predict anxiety related to a coming viral threat. Stress Health 2013, 30, 149–157. [Google Scholar] [CrossRef]
- Heath, R.L.; Gay, C.D. Risk communication: Involvement, uncertainty, and control’s effect on information scanning and monitoring by expert stakeholders in SARA Title III. Manag. Commun. Q. 1997, 10, 342–372. [Google Scholar] [CrossRef]
- Figley, C.R. Compassion fatigue as secondary traumatic stress disorder: An overview. In Compassion Fatigue: Coping with Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized; Figley, C.R., Ed.; Brunner/Mazel: New York, NY, USA, 1995; pp. 1–20. [Google Scholar]
- McCann, L.; Pearlman, L.A. Vicarious traumatization: A framework for understanding the psychological effects of working with victims. J. Trauma. Stress 1990, 3, 131–149. [Google Scholar] [CrossRef]
- Pearlman, L.A.; Saakvitne, K.W. Trauma and the Therapist: Countertransference and Vicarious Traumatization in Psychotherapy with Incest Survivors; W. W. Norton: London, UK, 1995. [Google Scholar]
- Saakvitne, K.W.; Pearlman, L.A. Transforming the Pain: A Workbook on Vicarious Traumatization; W. W. Norton: London, UK, 1996. [Google Scholar]
- Sabin-Farrell, R.; Turpin, G. Vicarious traumatization: Implications for the mental health of health workers? Clin. Psychol. Rev. 2003, 23, 449–480. [Google Scholar] [CrossRef]
- Stamm, B.H. Work-related secondary traumatic stress. Ptsd Res. Q. 1997, 8, 2. [Google Scholar]
- Ahern, J.; Galea, S.; Resnick, H.; Vlahov, D. Television images and probable posttraumatic stress disorder after September 11. J. Nerv. Ment. Dis. 2004, 192, 217–226. [Google Scholar] [CrossRef]
- Bourne, C.; Mackay, C.E.; Holmes, E.A. The neural basis of flashback formation: The impact of viewing trauma. Psychol. Med. 2013, 43, 1521–1532. [Google Scholar] [CrossRef]
- Thompson, R.R.; Jones, N.M.; Holman, E.A.; Silver, R.C. Media exposure to mass violence events can fuel a cycle of distress. Sci. Adv. 2019, 5, eaav3502. [Google Scholar] [CrossRef]
- Bernstein, K.T.; Ahern, J.; Tracy, M.; Boscarino, J.A.; Vlahov, D.; Galea, S. Television watching and the risk of incident probable posttraumatic stress disorder: A prospective evaluation. J. Nerv. Ment. Dis. 2007, 195, 41–47. [Google Scholar] [CrossRef]
- Holman, E.A.; Silver, R.C. Health status and health care utilization following collective trauma: A 3-year national study of the 9/11 terrorist attacks in the United States. Soc. Sci. Med. 2011, 73, 483–490. [Google Scholar] [CrossRef]
- Silver, R.C.; Holman, E.A.; Andersen, J.P.; Poulin, M.J.; Mcintosh, D.N.; Gil-Rivas, V. Mental- and physical-health effects of acute exposure to media images of the September 11, 2001, attacks and the Iraq War. Psychol. Sci. 2013, 24, 1623–1634. [Google Scholar] [CrossRef]
- Hadjistavropoulos, H.D.; Craig, K.D.; Hadjistavropoulos, T. Cognitive and behavioral responses to illness information: The role of health anxiety. Behav. Res. Ther. 1998, 36, 149–164. [Google Scholar] [CrossRef]
- Thompson, R.R.; Garfin, D.R.; Holman, E.A.; Silver, R.C. Distress, worry, and functioning following a global health crisis: A national study of Americans’ responses to Ebola. Clin. Psychol. Sci. 2017, 5, 513–521. [Google Scholar] [CrossRef]
- Lachlan, K.A.; Spence, P.R.; Seeger, M. Terrorist attacks and uncertainty reduction: Media use after September 11. Behav. Sci. Terror. Political Aggress. 2009, 1, 101–110. [Google Scholar] [CrossRef]
- Garfin, D.R.; Holman, E.A.; Silver, R.C. Cumulative exposure to prior collective trauma and acute stress responses to the Boston marathon bombings. Psychol. Sci. 2015, 26, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Kassam-Adams, N. The risks of treating sexual trauma: Stress and secondary trauma in psychotherapists. In Secondary Traumatic Stress: Self Care Issues for Clinicians, Researchers, and Educators; Stamm, B.H., Ed.; Sidran: Lutherville, MD, USA, 1995; pp. 37–47. [Google Scholar]
- Schauben, L.J.; Frazier, P.A. Vicarious trauma: The effects on female counselors of working with sexual violence victims. Psychol. Women Q. 1995, 19, 49–64. [Google Scholar] [CrossRef]
- Follette, V.M.; Polusny, M.M.; Mi1beck, K. Mental health and law enforcement professionals: Trauma history, psychological symptoms, and impact of providing services to child sexual abuse survivors. Prof. Psychol. Res. Pract. 1994, 25, 275–282. [Google Scholar] [CrossRef]
- Ghahramanlou, M.; Brodbeck, C. Predictors of secondary trauma in sexual assault trauma counselors. Int. J. Emerg. Ment. Health 2000, 2, 229–240. [Google Scholar]
- Pearlman, L.A.; Mac Ian, P.S. Vicarious traumatization: An empirical study of the effects of trauma work on trauma therapists. Professional Psychology. Res. Pract. 1995, 26, 558–565. [Google Scholar]
- Spence, P.R.; Westerman, D.; Skalski, P.D.; Seeger, M.; Ulmer, R.R.; Venette, S.; Sellnow, T.L. Proxemic effects on information seeking after the September 11 attacks. Commun. Res. Rep. 2005, 22, 39–46. [Google Scholar] [CrossRef]
- Vrklevski, L.P.; Franklin, J. Vicarious trauma: The impact on solicitors of exposure to traumatic material. Traumatology 2008, 14, 106–118. [Google Scholar] [CrossRef]
- Zung, W.W. A rating instrument for anxiety disorders. Psychosomatics 1971, 12, 371–379. [Google Scholar] [CrossRef]
- Ball-Rokeach, S.J. From pervasive ambiguity to a definition of the situation. Sociometry 1973, 38, 378–389. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Bratslavsky, E.; Finkenauer, C.; Vohs, K.D. Bad is stronger than good. Rev. Gen. Psychol. 2001, 5, 323–370. [Google Scholar] [CrossRef]
- Haslam, S.A.; Jetten, J.; O’Brian, A.; Jacobs, E. Social identity, social influence and reactions to potentially stressful tasks: Support for the self-categorization model of stress. Stress Health 2004, 20, 3–9. [Google Scholar] [CrossRef]
- Ball-Rokeach, S.J. The origins of individual media-system dependency. Commun. Res. 1985, 12, 485–510. [Google Scholar] [CrossRef]





| Demographics | Percentage |
|---|---|
| Sex | |
| Male | 45.9% |
| Female | 54.1% |
| Age | |
| Below 18 | 4.1% |
| 18–25 | 30.6% |
| 26–30 | 22.6% |
| 31–35 | 23.5% |
| 36–40 | 9% |
| 41–50 | 7.6% |
| Above 50 | 2.5% |
| Education | |
| High school or below | 12.7% |
| College/university | 79.8% |
| Postgraduate | 7.5% |
| Social Economic Status | |
| Lower to middle class | 36.0% |
| Middle class | 53.7% |
| Middle to upper class | 10.3% |
| Health Condition (Mean = 3.92, SD = 0.72) | |
| Very poor | 0.1% |
| Relatively poor | 2.0% |
| Average | 24.0% |
| Relatively good | 53.7% |
| Very good | 20.3% |
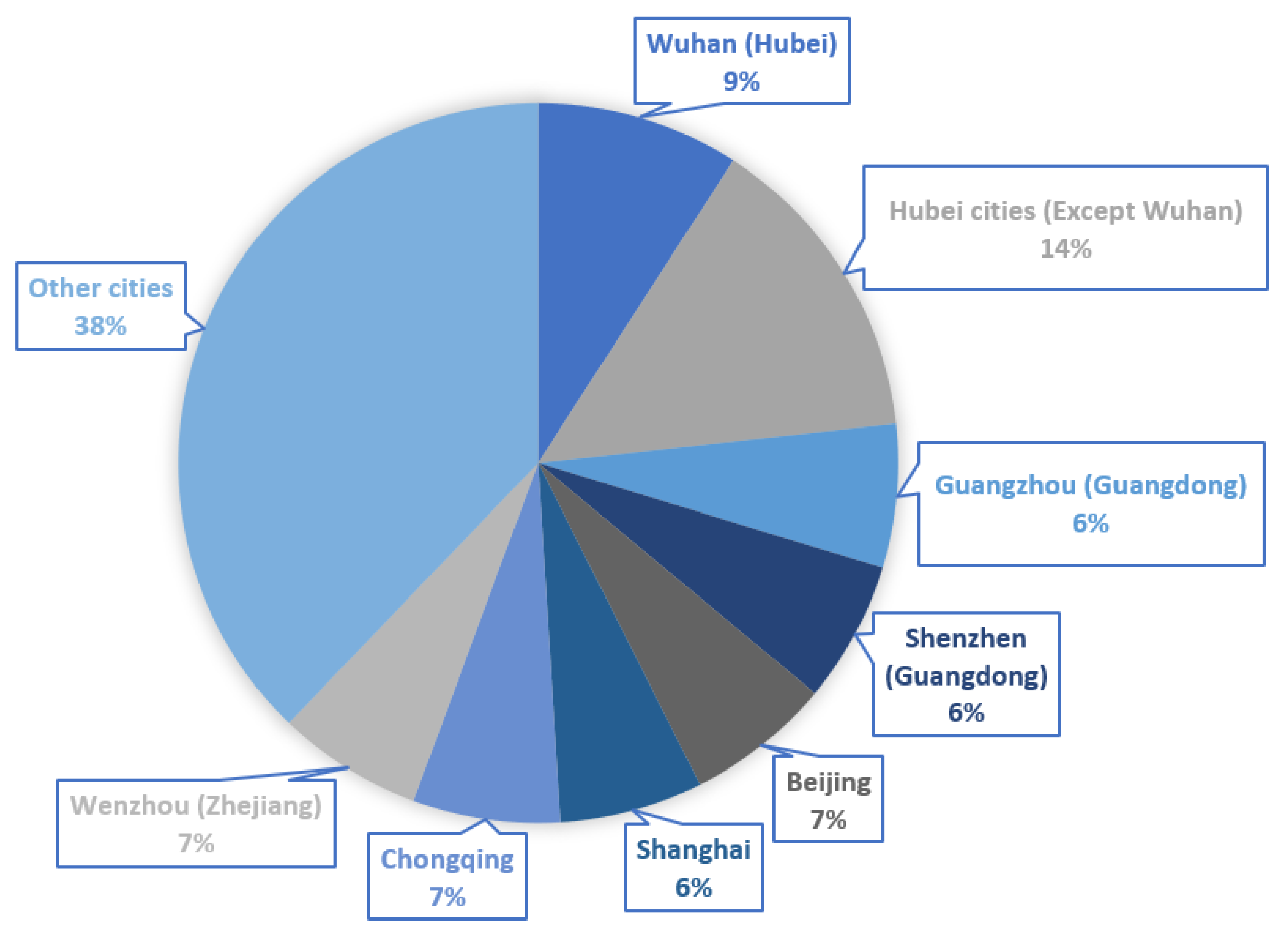
| Location of Residence During the Pandemic | |
| Hubei (Wuhan) | 4.7% |
| Hubei (excluding Wuhan) | 17.8% |
| Cities with severe pandemic (including Beijing, Shanghai, Chongqing, Guangzhou in Guangdong province, Shenzhen in Guangdong province, and Wenzhou in Zhejiang province) | 36.2% |
| Other cities (not significantly impacted by the coronavirus) | 41.3% |
| Accommodation | |
| Staying with family | 95.1% |
| Staying with friends | 2.6% |
| Staying alone | 2.3% |
| Variables | Outcome: Anxiety | Outcome: Media Vicarious Traumatization | Outcome: Anxiety |
|---|---|---|---|
| Time Spent on COVID-19 Information | 0.19 | 0.16 | 0.09 *** |
| Official Media Use | −0.01 | 0.06 * | −0.05 * |
| Commercial Media Use | 0.11 ** | 0.11 *** | 0.04 |
| Social Media Use | 0.02 | 0.07 * | −0.02 |
| Overseas Media Use | 0.09 ** | 0.08 ** | 0.04 |
| Media Vicarious Traumatization | 0.61 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.; Liu, Y. Media Exposure and Anxiety during COVID-19: The Mediation Effect of Media Vicarious Traumatization. Int. J. Environ. Res. Public Health 2020, 17, 4720. https://doi.org/10.3390/ijerph17134720
Liu C, Liu Y. Media Exposure and Anxiety during COVID-19: The Mediation Effect of Media Vicarious Traumatization. International Journal of Environmental Research and Public Health. 2020; 17(13):4720. https://doi.org/10.3390/ijerph17134720
Chicago/Turabian StyleLiu, Cong, and Yi Liu. 2020. "Media Exposure and Anxiety during COVID-19: The Mediation Effect of Media Vicarious Traumatization" International Journal of Environmental Research and Public Health 17, no. 13: 4720. https://doi.org/10.3390/ijerph17134720
APA StyleLiu, C., & Liu, Y. (2020). Media Exposure and Anxiety during COVID-19: The Mediation Effect of Media Vicarious Traumatization. International Journal of Environmental Research and Public Health, 17(13), 4720. https://doi.org/10.3390/ijerph17134720