A New Design Scheme for Intelligent Upper Limb Rehabilitation Training Robot

Abstract
1. Introduction
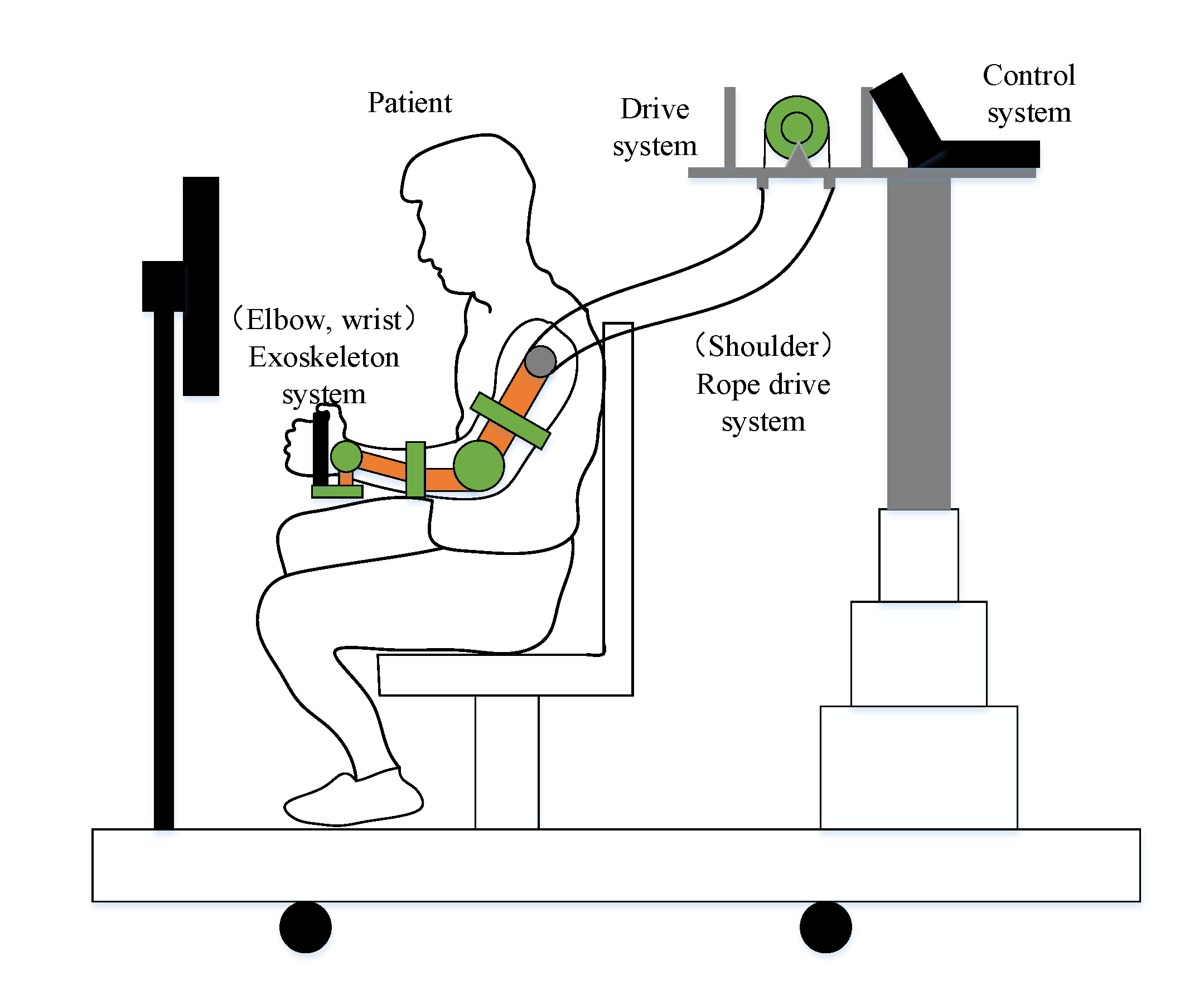
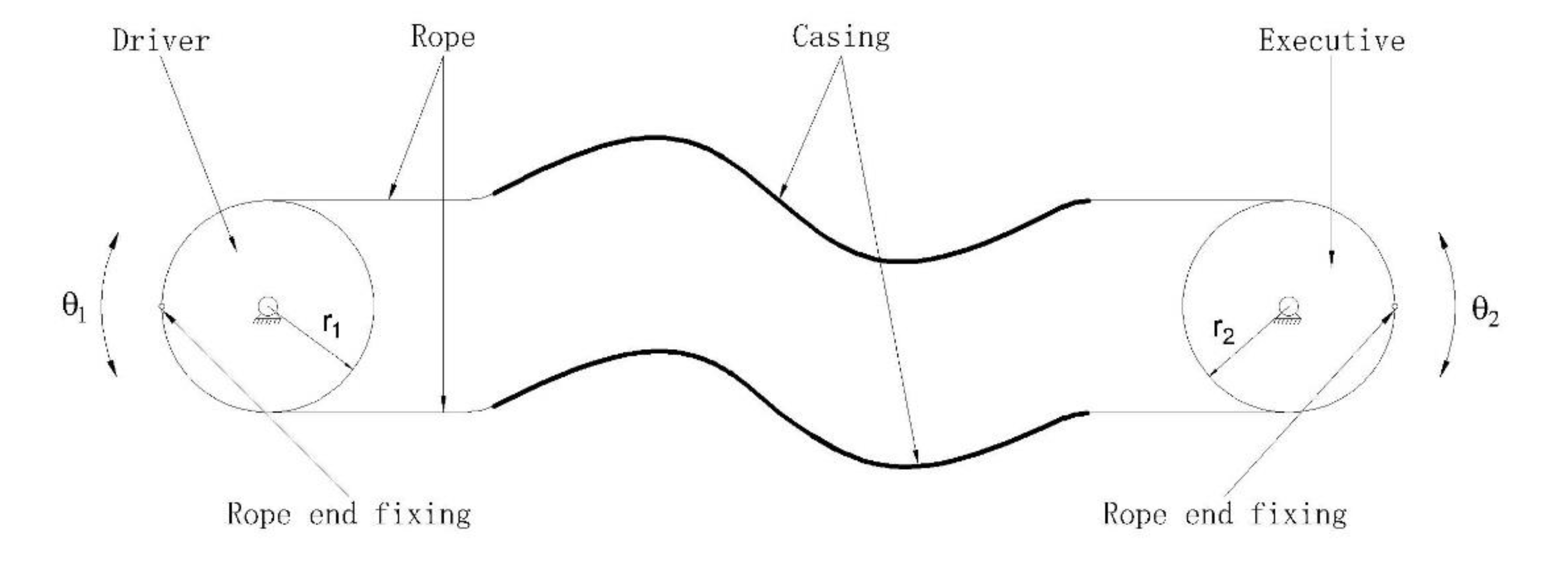
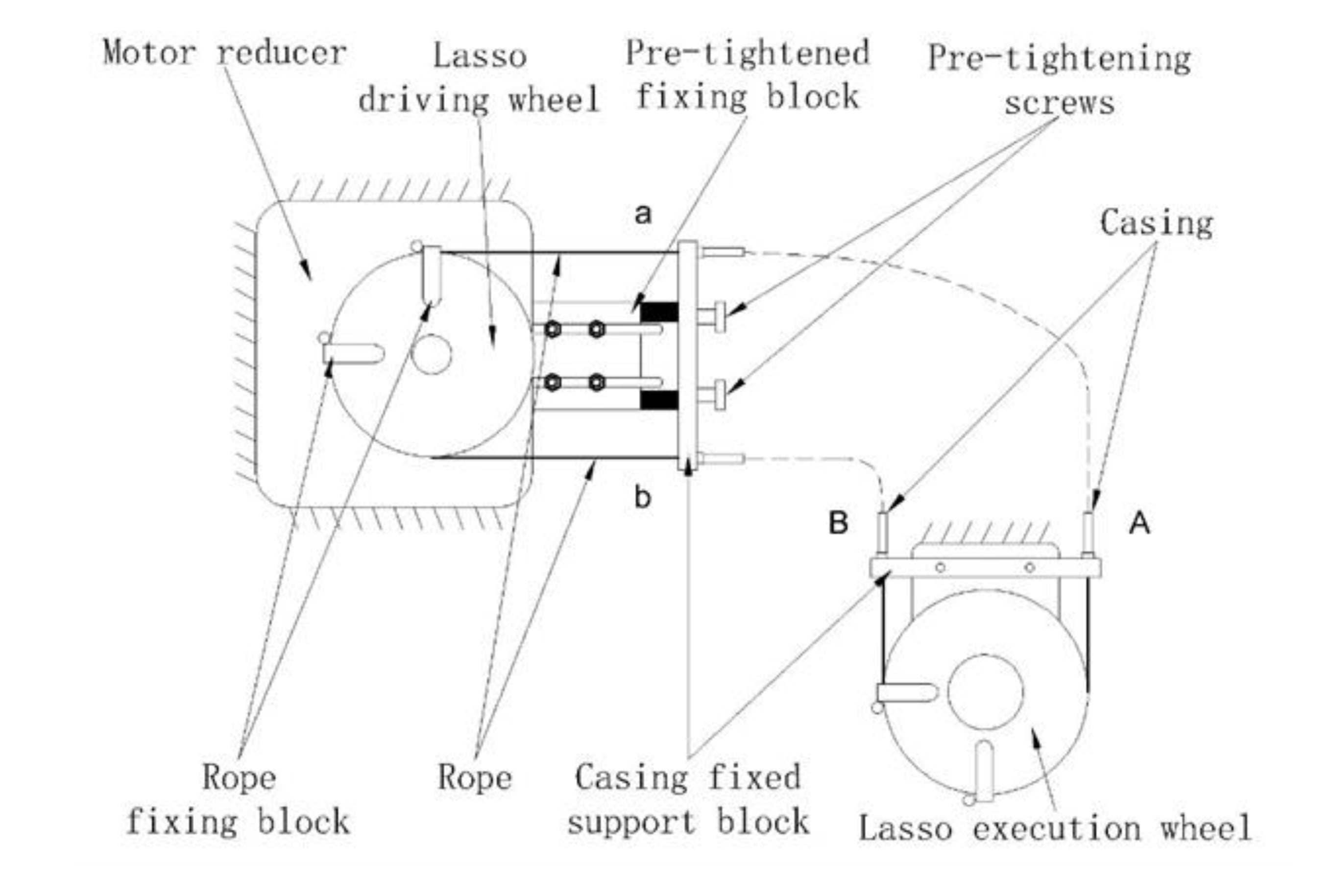
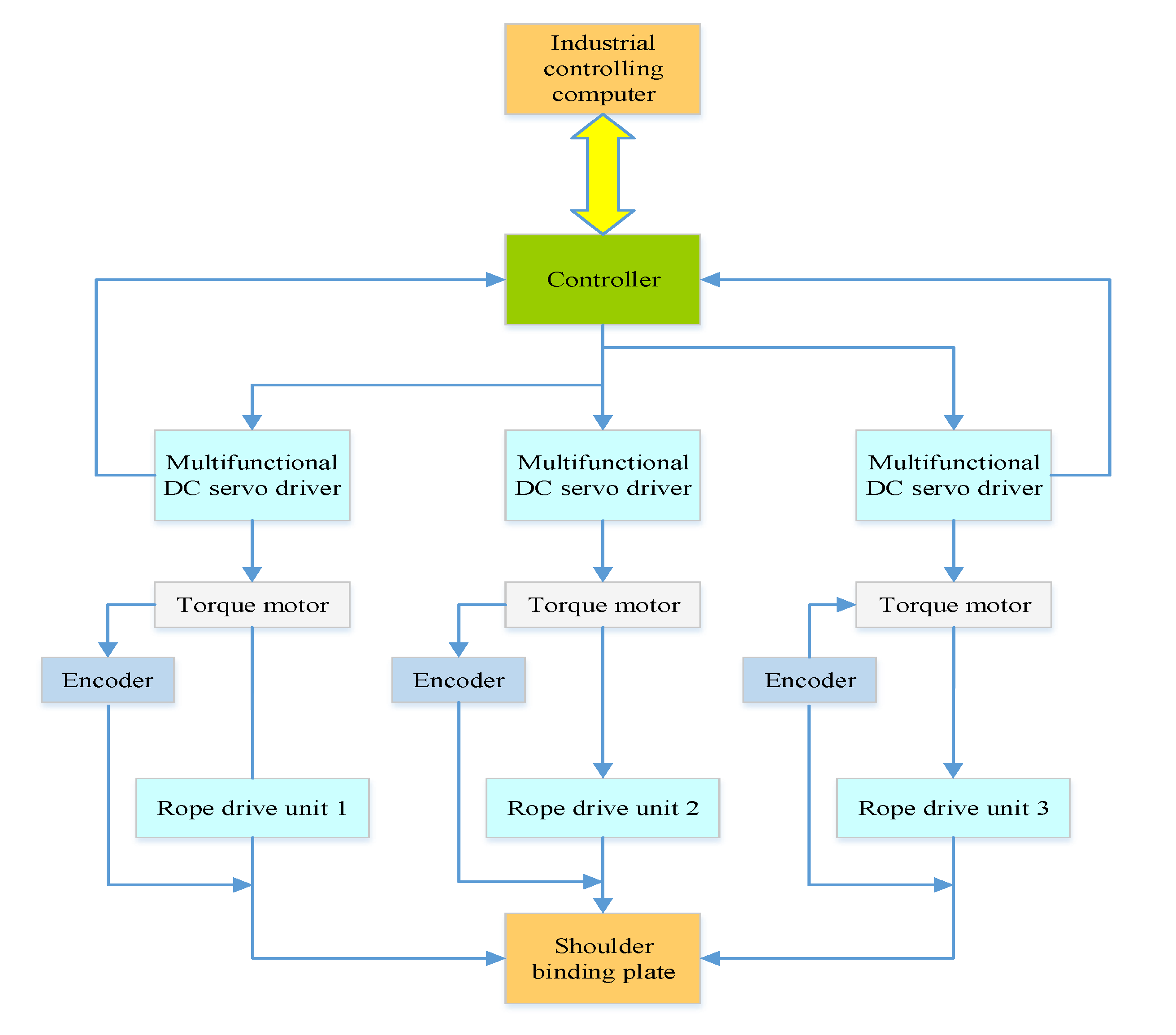
2. Design of the Rehabilitation Robot Structure
3. Design of the Human-Machine Natural Interaction Scheme Based on Perceived Information
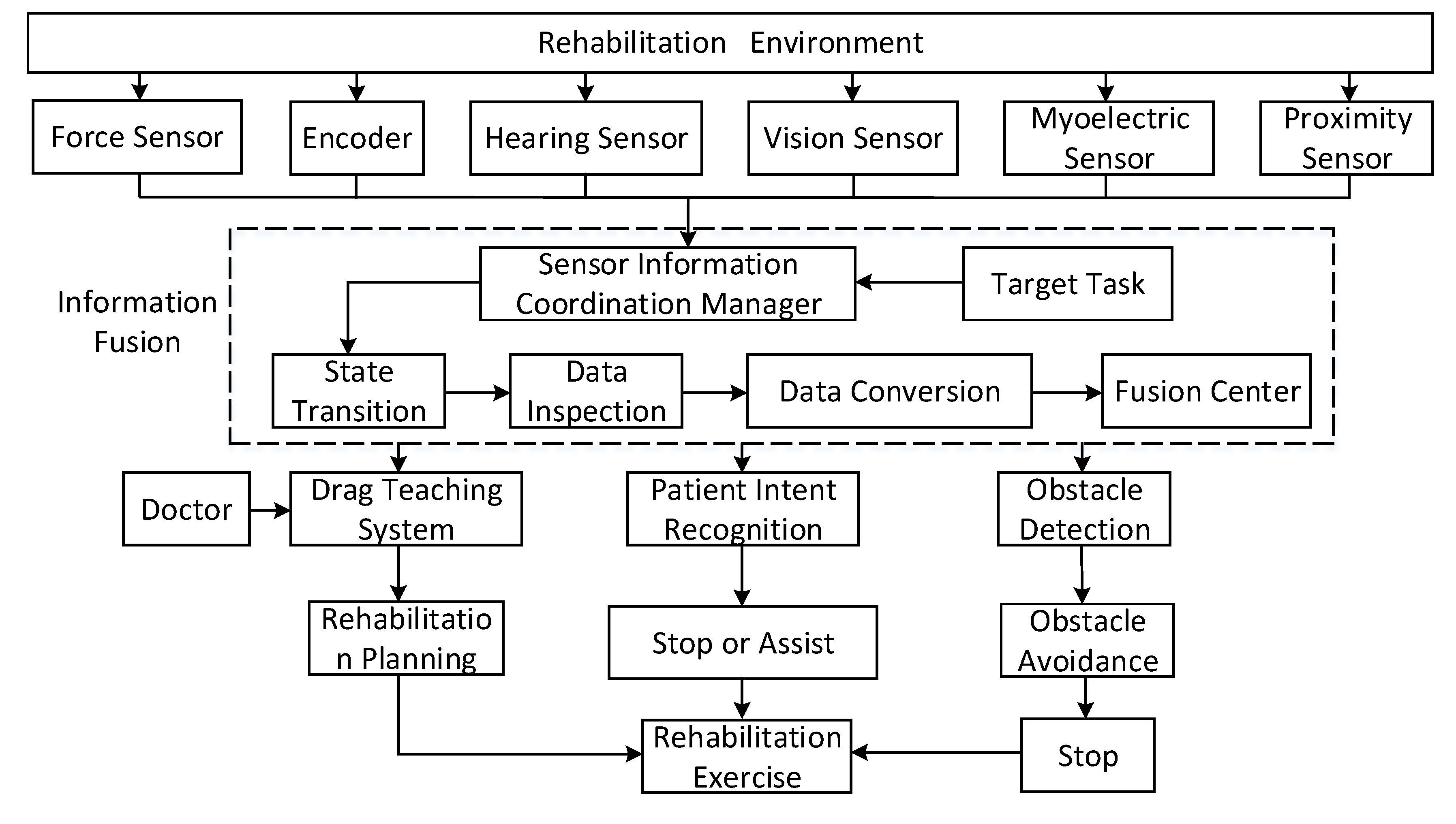
3.1. Method to Process and Coordinate Multiple Pieces of Information
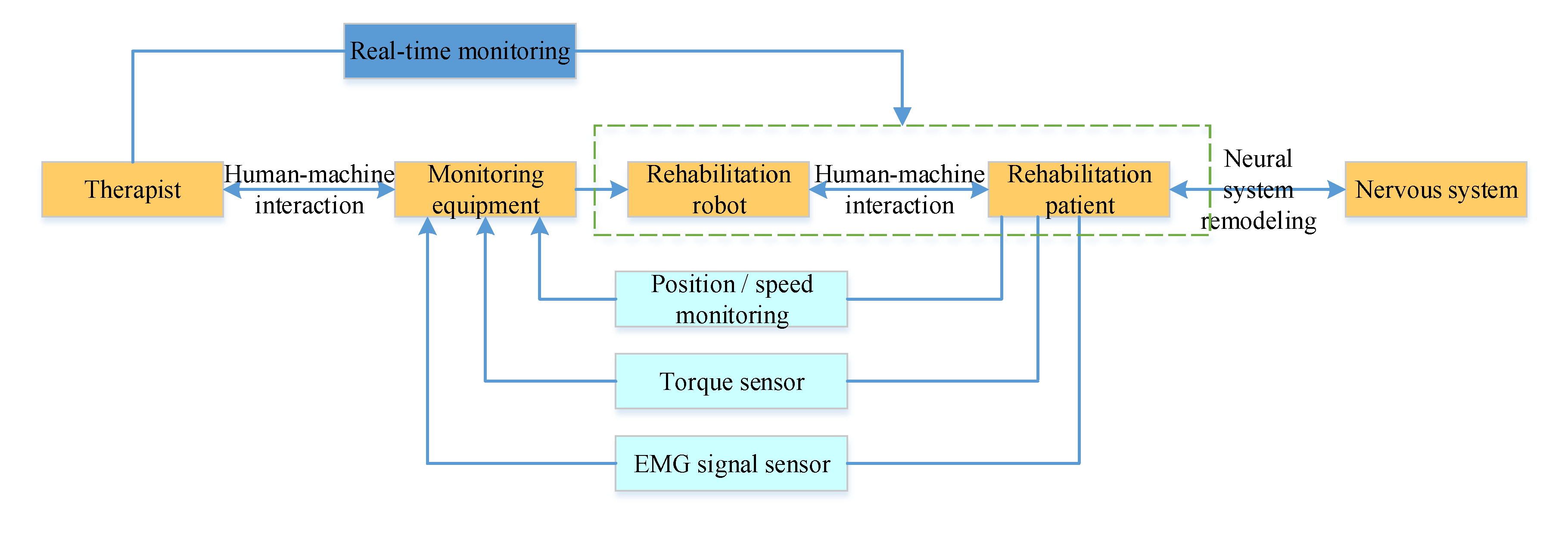
3.2. Human-Machine Natural Interaction Method Based on the Multi-Sensor System
4. Design of the Scheme to Integrate Human, Machine, and Environment Based on a Human’s Natural Response
4.1. Rehabilitation Training Platform with Friendly Cooperation among Human, Machine, and Environmental Elements
4.2. Interactive Training System Based on a Human’s Natural Response and Other Related Data
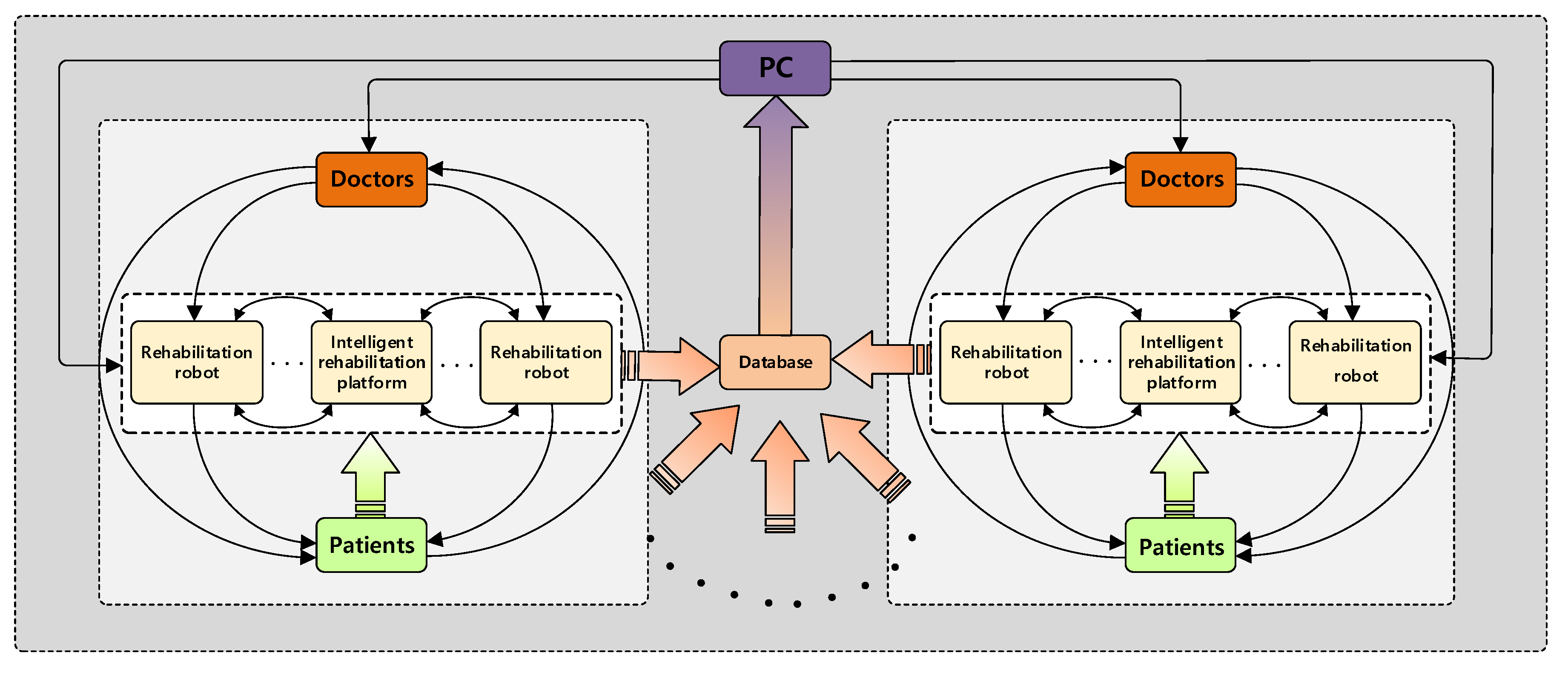
4.3. Multi-Dimensional Intelligent Rehabilitation System
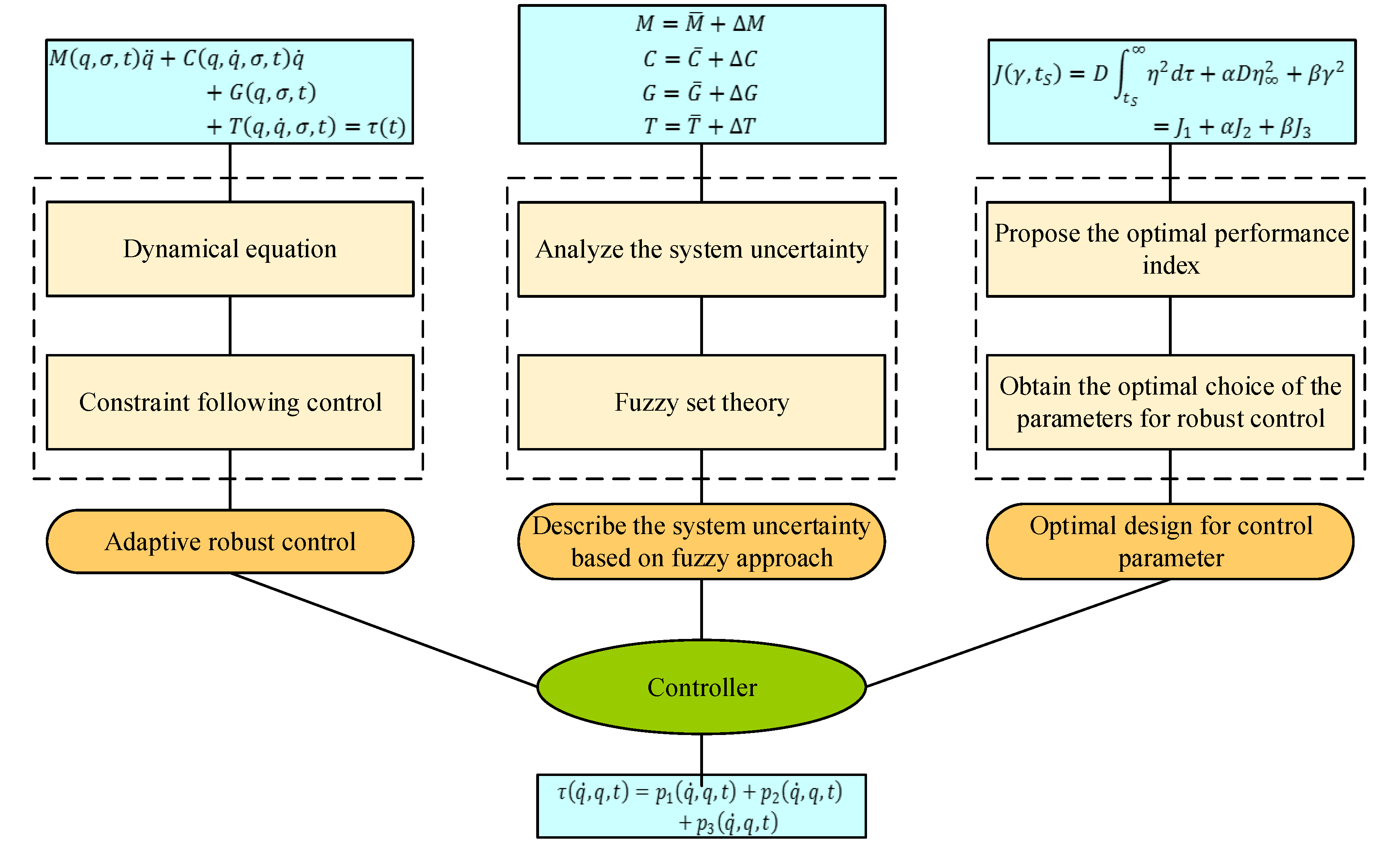
5. Dynamic Modeling and Control Scheme Design
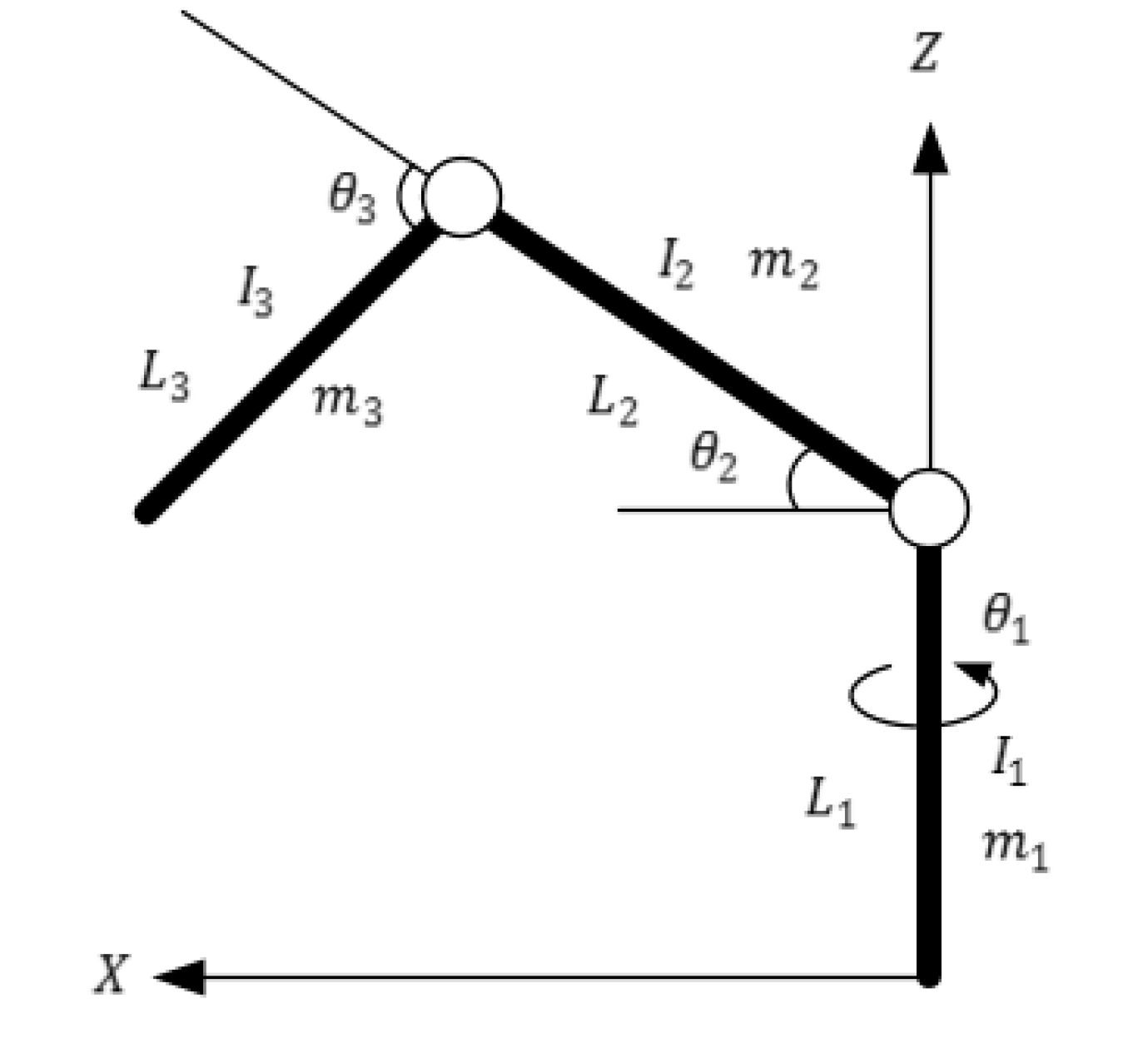
5.1. Dynamic Modeling
5.2. Controller Design
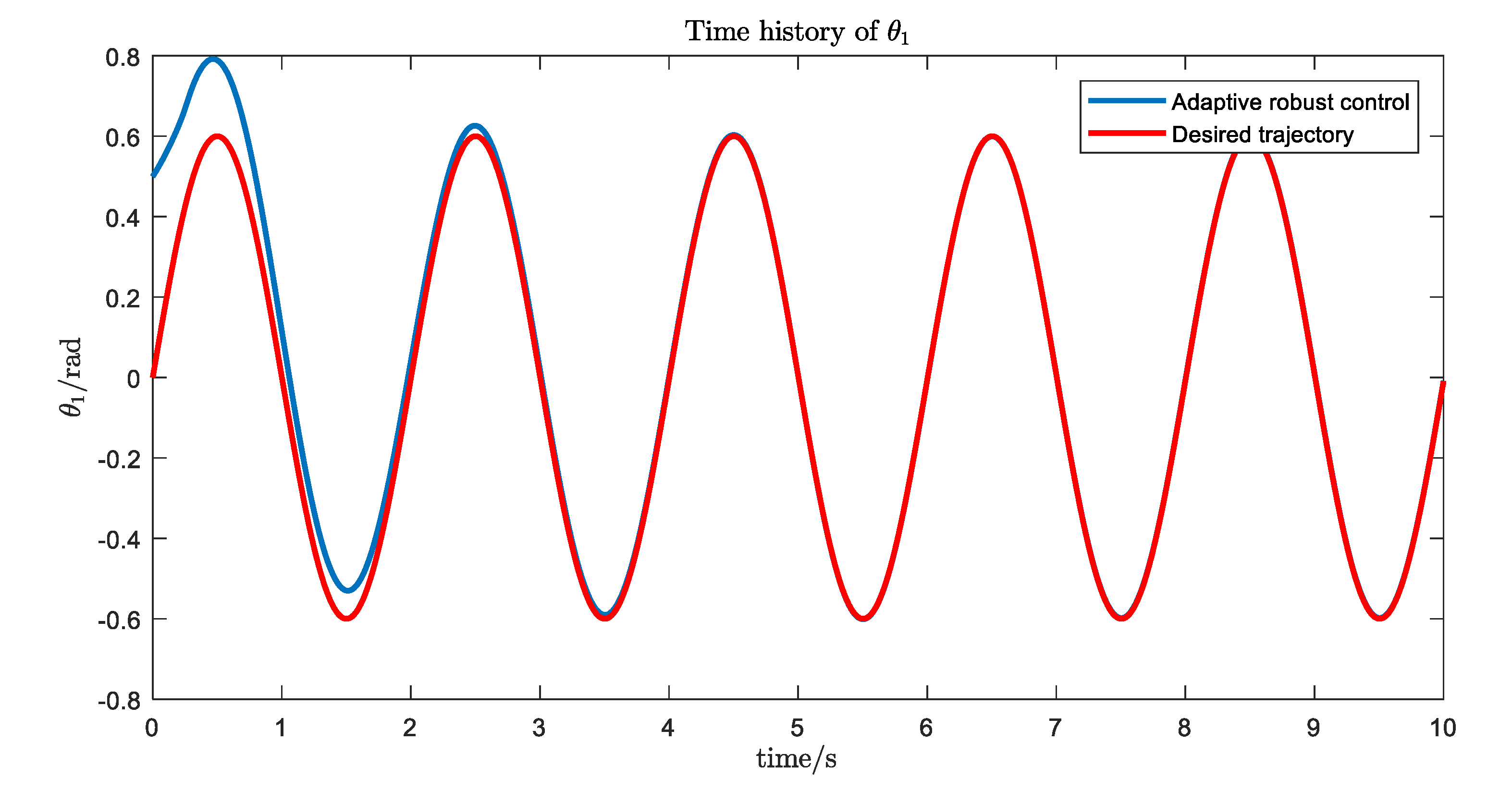
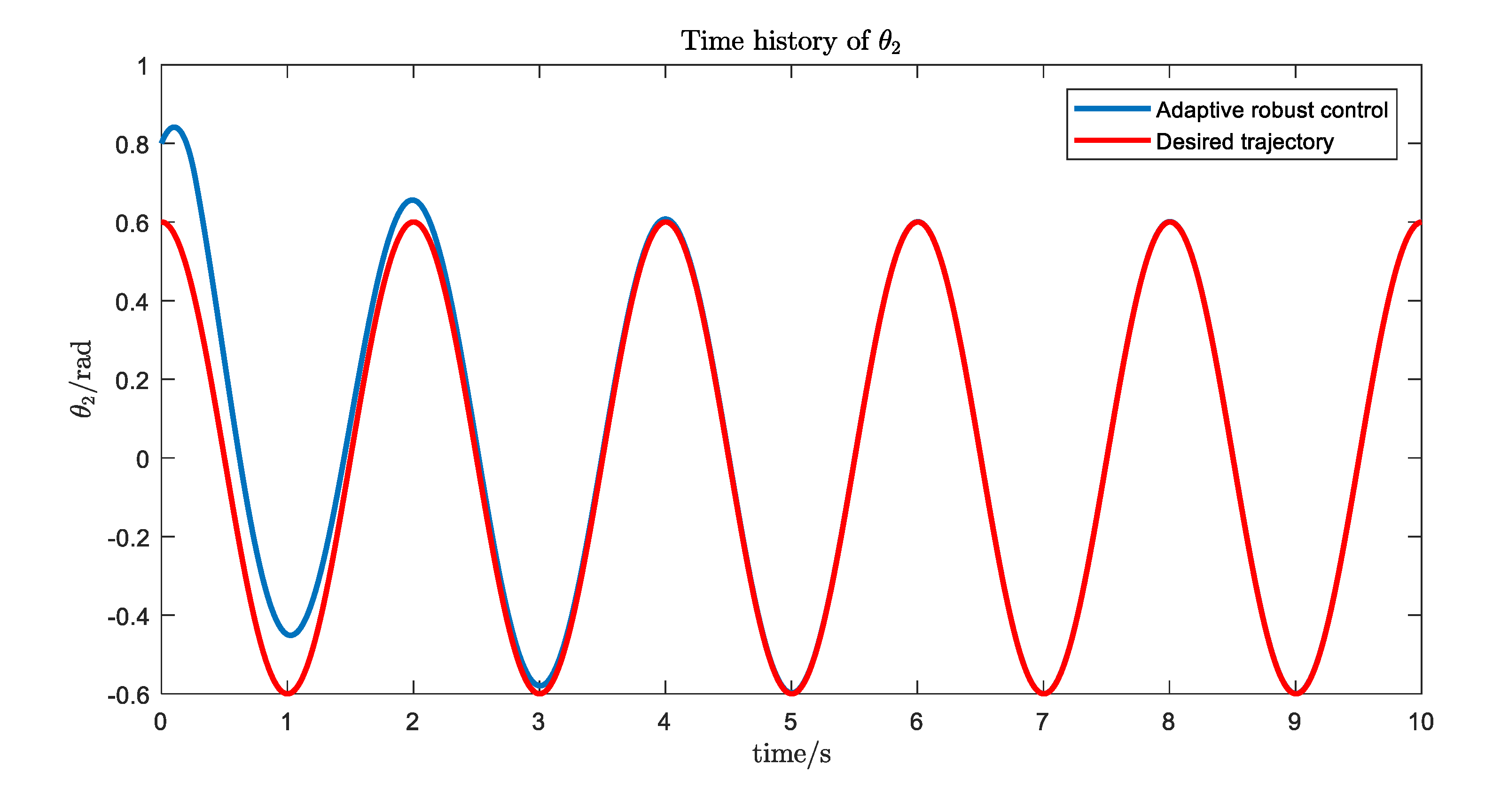
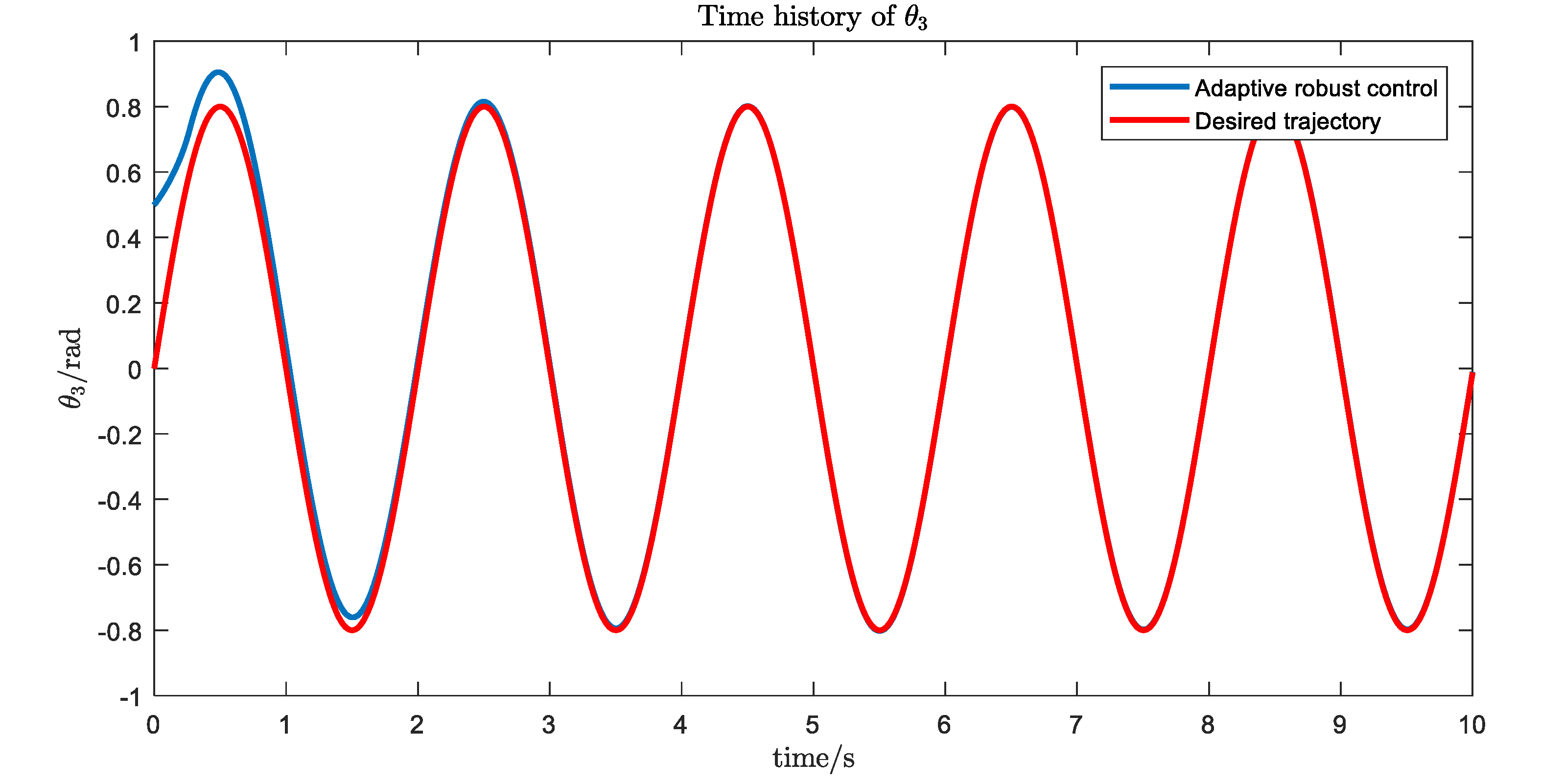
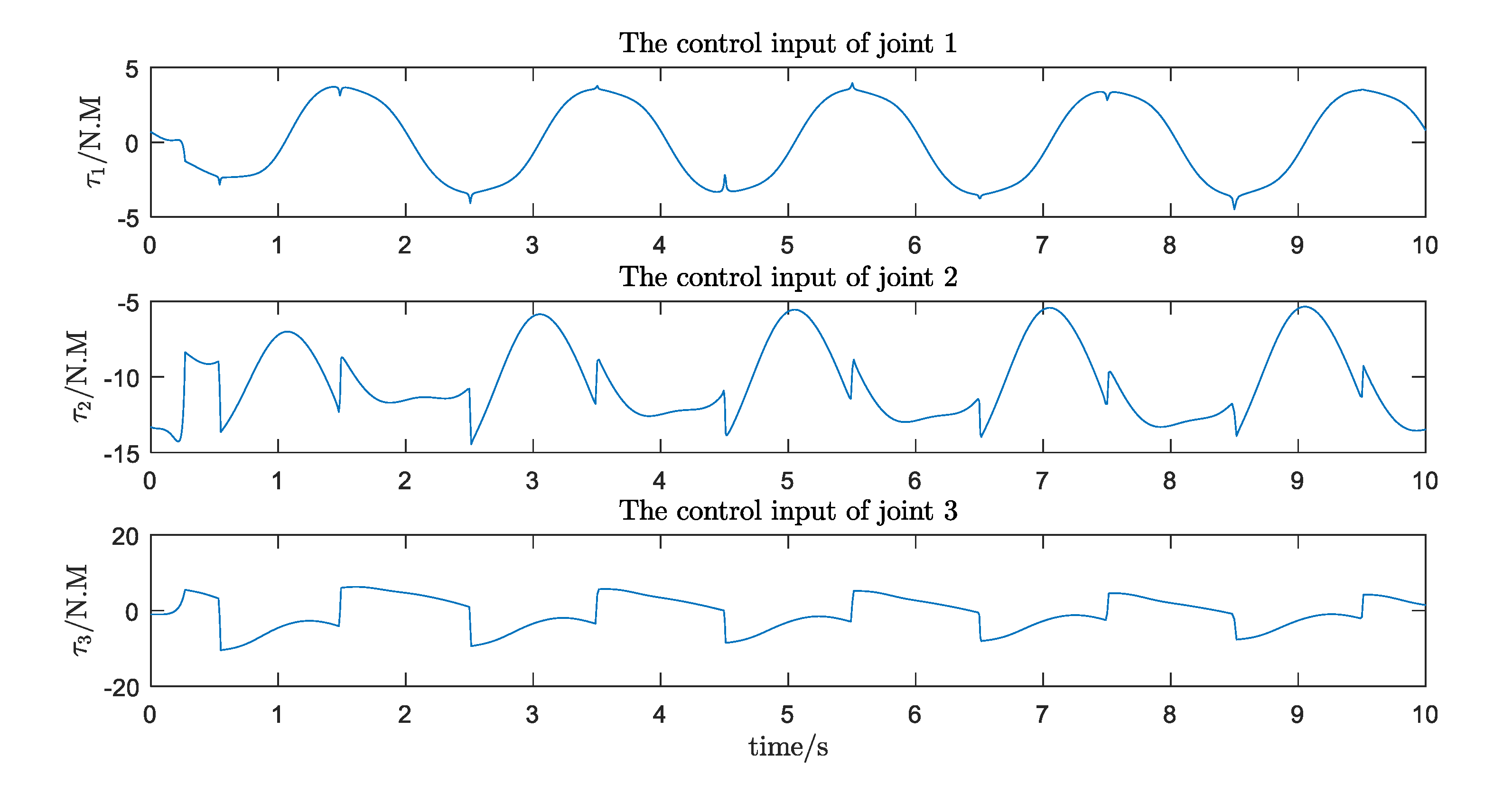
5.3. A Simulation Case
6. Conclusions
- (1)
- A new structure for an upper limb rehabilitation robot is proposed. It combines a flexible rope with an exoskeleton in order to ensure that the moving parts connected with the patient’s upper limbs are light, accurate, and flexible.
- (2)
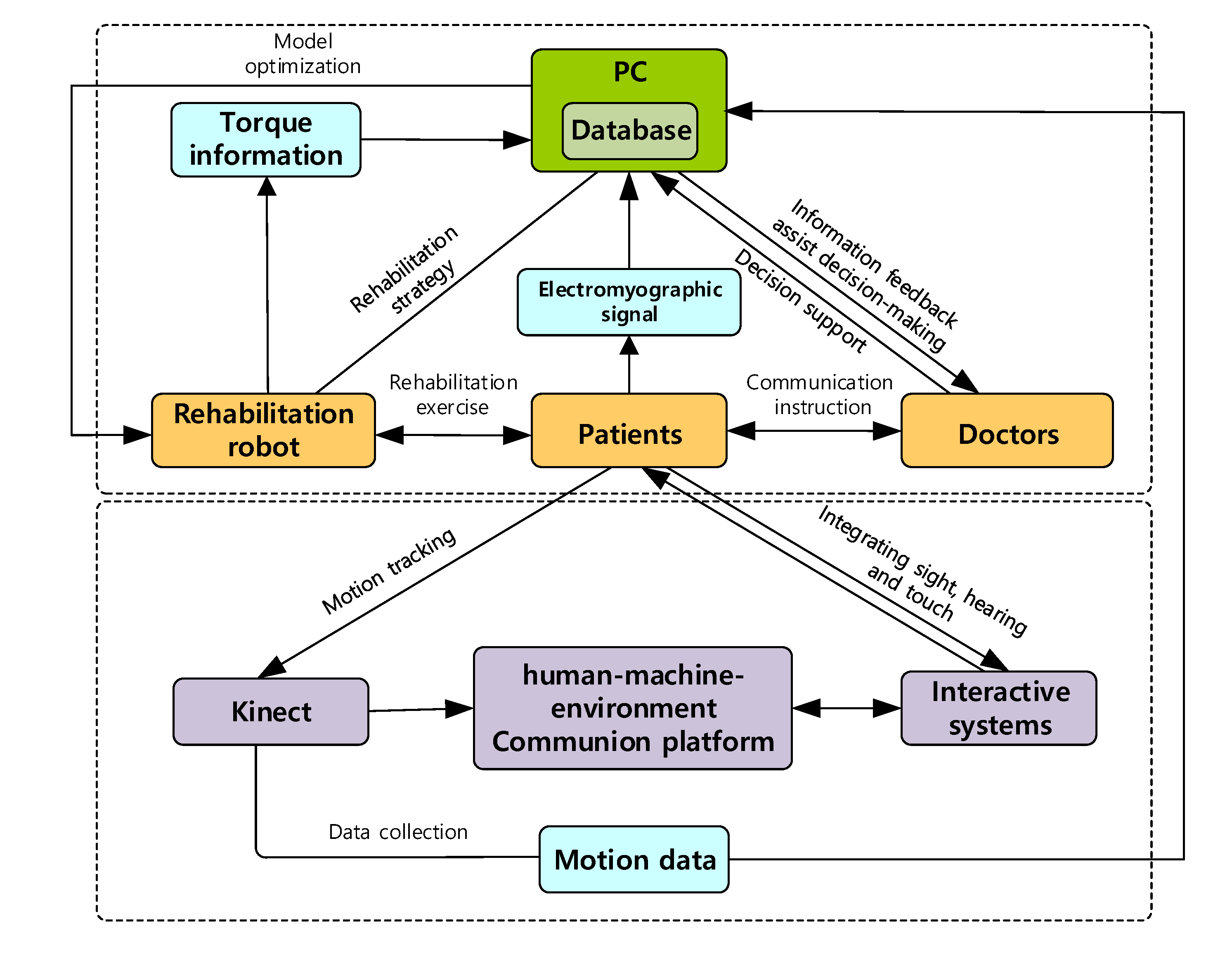
- Applying the theories and technologies of ergonomics, virtual reality, information fusion, big-data analysis, and deep learning, a collaborative, efficient, and intelligent remote rehabilitation system based on a human’s natural response is constructed.
- (3)
- For this multi-degree-of-freedom robot system, the Udwadia-Kalaba approach is applied to establish the dynamic equation of the system. Based on this explicit dynamic equation, optimal adaptive robust control design with fuzzy set theory is presented for the motion control of the system.
- (4)
- The new design will help improve the interest of patients in participating in the training and improve the effects of the rehabilitation, help doctors design a good rehabilitation training program, and help hospitals manage patients in real time and summarize the experiences.
Author Contributions
Funding
Conflicts of Interest
References
- Chuan, L.U. Roadmap of service robot technology in the US. Robot Ind. 2016, 18, 86–97. [Google Scholar]
- Chen, L. IFR released the latest global service robot statistics report. Robot Ind. 2016, 18, 33–36. [Google Scholar]
- The Market Scale of Rehabilitation Robot Reaches 10 Billion under the Stimulation of Aging. Available online: https://www.sohu.com/a/200125545_114835 (accessed on 25 October 2017).
- Reinkensmeyer, D.J. Rehabilitation Robot. Available online: https://www.britannica.com/technology/rehabilitation-robot (accessed on 7 December 2018).
- Napper, S.A.; Seaman, R.L. Applications of robots in rehabilitation. Robot. Auton. Syst. 1989, 5, 227–239. [Google Scholar] [CrossRef]
- Krebs, H.I.; Hogan, N.; Aisen, M.L.; Volpe, B.T. Robot-aided neurorehabilitation. IEEE Trans. Rehabil. Eng. 1998, 6, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Krebs, H.I.; Ferraro, M.; Buerger, S.P.; Newbery, M.J.; Makiyama, A.; Sandmann, M.; Lynch, D.; Volpe, B.T.; Hogan, N. Rehabilitation robotics: Pilot trial of a spatial extension for MIT-Manus. J. Neuroeng. Rehabil. 2004, 1, 1–15. [Google Scholar] [CrossRef]
- Krebs, H.I.; Edwards, D.; Hogan, N. Forging mens et manus: The MIT experience in upper extremity robotic therapy. In Neurorehabilitation Technology; Springer: Cham, Switzerland, 2016; pp. 333–350. [Google Scholar]
- Krebs, H.I.; Palazzolo, J.J.; Dipietro, L.; Ferraro, M.; Krol, J.; Rannekleiv, K.; Volpe, B.T.; Hogan, N. Rehabilitation robotics: Performance-based progressive robot-assisted therapy. Auton. Robot. 2003, 15, 7–20. [Google Scholar] [CrossRef]
- Loureiro, R.; Amirabdollahian, F.; Topping, M.; Driessen, B.; Harwin, W. Upper limb robot mediated stroke therapy-GENTLE/s approach. Auton. Robot. 2003, 15, 35–51. [Google Scholar] [CrossRef]
- Ivanova, E.; Krüger, J.; Steingräber, R.; Schmid, S.; Schmidt, H.; Hesse, S. Design and concept of a haptic robotic telerehabilitation system for upper limb movement training after stroke. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, Singapore, 11–14 August 2015; IEEE: Piscataway, NJ, USA; pp. 666–671. [Google Scholar]
- Reinkensmeyer, D.J.; Kahn, L.E.; Averbuch, M.; McKenna-Cole, A.; Schmit, B.D.; Rymer, W.Z. Understanding and treating arm movement impairment after chronic brain injury: Progress with the ARM guide. J. Rehabil. Res. Dev. 2000, 37, 653–662. [Google Scholar]
- Rosen, J.; Perry, J.C.; Manning, N.; Burns, S.; Hannaford, B. The human arm kinematics and dynamics during daily activities-toward a 7 DOF upper limb powered exoskeleton. In Proceedings of the IEEE 12th International Conference on Advanced Robotics, Seattle, WA, USA, 18–20 July 2005; IEEE: Piscataway, NJ, USA; pp. 532–539. [Google Scholar]
- Nef, T.; Brunschweiler, A.; Riener, R.; Schulz, N. System for Arm Therapy. U.S. Patent 9017271B2, 28 April 2015. [Google Scholar]
- Balasubramanian, S.; Wei, R.; Perez, M.; Shepard, B.; Koeneman, E.; Koeneman, J.; He, J. RUPERT: An exoskeleton robot for assisting rehabilitation of arm functions. In Proceedings of the IEEE Virtual Rehabilitation, Vancouver, BC, Canada, 25–27 August 2008; pp. 163–167. [Google Scholar]
- Li, X.; Liu, Y.; Yu, H. Iterative learning impedance control for rehabilitation robots driven by series elastic actuators. Automatica 2018, 90, 1–7. [Google Scholar] [CrossRef]
- Pan, Y.; Wang, H.; Li, X.; Yu, H. Adaptive command-filtered backstepping control of robot arms with compliant actuators. IEEE Trans. Control Syst. Technol. 2018, 26, 1149–1156. [Google Scholar] [CrossRef]
- Xu, H.; Zhang, M.; Li, Y.; Xu, D.; Fu, J.; Zhang, X.; Li, X.; Xie, S.Q. Development of a pneumatic robotic system for bilateral upper limb interactive training with variable resistance. In Proceedings of the IEEE/ASME International Conference on Advanced Intelligent Mechatronics (AIM), Auckland, New Zealand, 9–12 July 2018; IEEE: Piscataway, NJ, USA; pp. 968–973. [Google Scholar]
- Bulboacă, A.E.; Bolboacă, S.D.; Bulboacă, A.C. Ethical considerations in providing an upper limb exoskeleton device for stroke patients. Med. Hypotheses 2017, 101, 61–64. [Google Scholar] [CrossRef]
- Dovat, L.; Lambercy, O.; Gassert, R.; Maeder, T.; Milner, T.; Leong, T.C.; Burdet, E. HandCARE: A cable-actuated rehabilitation system to train hand function after stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2008, 16, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Agrawal, S.K. Design of a cable-driven arm exoskeleton (CAREX) for neural rehabilitation. IEEE Trans. Robot. 2012, 28, 922–931. [Google Scholar] [CrossRef]
- Chen, Q.; Zi, B.; Sun, Z.; Li, Y.; Xu, Q. Design and development of a new cable-driven parallel robot for waist rehabilitation. IEEE/ASME Trans. Mechatron. 2019, 24, 1497–1507. [Google Scholar] [CrossRef]
- Chen, T.; Casas, R.; Lum, P.S. An elbow exoskeleton for upper limb rehabilitation with series elastic actuator and cable-driven differential. IEEE Trans. Robot. 2019, 35, 1464–1474. [Google Scholar] [CrossRef] [PubMed]
- Hogan, N. Impedance control: An approach to manipulation. In Proceedings of the IEEE American Control Conference, San Diego, CA, USA, 6–8 June 1984. [Google Scholar]
- Richardson, R.; Brown Bhakta, B.; Levesley, M. Impedance control for a pneumatic robot-based around pole-placement, joint space controllers. Control Eng. Pract. 2005, 13, 291–303. [Google Scholar] [CrossRef]
- Rahman, M.H.; Ochoa-Luna, C.; Rahman, M.J.; Saad, M.; Archambault, P. Force-position control of a robotic exoskeleton to provide upper extremity movement assistance. Int. J. Model. Identif. Control 2014, 21, 390–400. [Google Scholar] [CrossRef]
- Brahmi, B.; Saad, M.; Rahman, M.H.; Ochoa-Luna, C. Cartesian trajectory tracking of a 7-DOF exoskeleton robot based on human inverse kinematics. IEEE Trans. Syst. Man Cybern. Syst. 2019, 49, 600–611. [Google Scholar] [CrossRef]
- Li, J.; Xia, Y.; Wang, J.; Dai, K. Research on upper limb rehabilitation robot system based on robust control theory. Inf. Technol. 2018, 7, 5–10. [Google Scholar]
- Xu, G.; Song, A.; Li, H. Adaptive impedance control for upper-limb rehabilitation robot using evolutionary dynamic recurrent fuzzy neural network. J. Intell. Robot. Syst. 2011, 62, 501–525. [Google Scholar] [CrossRef]
- Wu, Q.; Wang, X.; Wu, H.; Chen, B. Fuzzy sliding mode admittance control of the upper limb rehabilitation exoskeleton robot. Robot 2018, 40, 67–75. [Google Scholar]
- Culmer, P.R.; Jackson, A.E.; Makower, S.; Richardson, R.; Cozens, J.A.; Levesley, M.C.; Bhakta, B.B. A control strategy for upper limb robotic rehabilitation with a dual robot system. IEEE/ASME Trans. Mechatron. 2009, 15, 575–585. [Google Scholar] [CrossRef]
- Xu, G.; Song, A.; Pan, L.; Gao, X.; Liang, Z.; Li, J.; Xu, B. Clinical experimental research on adaptive robot-aided therapy control methods for upper-limb rehabilitation. Robotica 2014, 32, 1081–1100. [Google Scholar] [CrossRef]
- Zhang, J.; Cheah, C.C. Passivity and stability of human–robot interaction control for upper-limb rehabilitation robots. IEEE Trans. Robot. 2015, 31, 233–245. [Google Scholar] [CrossRef]
- Riani, A.; Madani, T.; Benallegue, A.; Djouani, K. Adaptive integral terminal sliding mode control for upper-limb rehabilitation exoskeleton. Control Eng. Pract. 2018, 75, 108–117. [Google Scholar] [CrossRef]
- Kiguchi, K.; Iwami, K.; Yasuda, M.; Watanabe, K.; Fukuda, T. An exoskeletal robot for human shoulder joint motion assist. IEEE/ASME Trans. Mechatron. 2003, 8, 125–135. [Google Scholar] [CrossRef]
- Cheng, H.S.; Ju, M.S.; Lin, C.C.K. Improving elbow torque output of stroke patients with assistive torque controlled by EMG signals. J. Biomech. Eng. 2003, 125, 881–886. [Google Scholar] [CrossRef]
- Cozens, J.A. Robotic assistance of an active upper limb exercise in neurologically impaired patients. IEEE Trans. Rehabil. Eng. 1999, 7, 254–256. [Google Scholar] [CrossRef]
- Mavroidis, C.; Nikitczuk, J.; Weinberg, B.; Arango, R.; Danaher, G.; Jensen, K.; Leahey, M.; Pavone, R.; Pelletier, P.; Provo, A.; et al. Smart portable rehabilitation devices. In Proceedings of the International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Long Beach, CA, USA, 24–28 September 2005; Volume 47446, pp. 501–510. [Google Scholar]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 1–29. [Google Scholar] [CrossRef]
- Ruan, B.; Shao, X. Industrial Design Ergonomics; Mechanical Industry Press: Beijing, China, 2005. [Google Scholar]
- Schoone, M.; Van Os, P.; Campagne, A. Robot-mediated Active Rehabilitation (ACRE) A user trial. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; IEEE: Piscataway, NJ, USA; pp. 477–481. [Google Scholar]
- Rosati, G.; Gallina, P.; Masiero, S.; Rossi, A. Design of a new 5 dof wire-based robot for rehabilitation. In Proceedings of the 9th International Conference on Rehabilitation Robotics (ICORR 2005), Chicago, IL, USA, 28 June–1 July 2005; IEEE: Piscataway, NJ, USA; pp. 430–433. [Google Scholar]
- Furusho, J.; Kikuchi, T.; Oda, K.; Ohyama, Y.; Morita, T.; Shichi, N.; Jin, Y.; Inoue, A. A 6-dof rehabilitation support system for upper limbs including wrists “robotherapist” with physical therapy. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; IEEE: Piscataway, NJ, USA; pp. 304–309. [Google Scholar]
- Culmer, P.R.; Jackson, A.E.; Makower, S.G.; Cozens, J.A.; Levesley, M.C.; Mon-Williams, M.; Bhakta, B. A novel robotic system for quantifying arm kinematics and kinetics: Description and evaluation in therapist-assisted passive arm movements post-stroke. J. Neurosci. Methods 2011, 197, 259–269. [Google Scholar] [CrossRef]
- Gao, J. Introduction to Intelligent Information Processing Methods; Mechanical Industry Press: Beijing, China, 2004. [Google Scholar]
- Xie, L.; Wang, Z. Machine Intelligence; Mechanical Industry Press: Beijing, China, 2017. [Google Scholar]
- Liu, P.; Zhang, Y. Deep Learning; Electronic Industry Press: Beijing, China, 2018. [Google Scholar]
- Gu, D.; Liang, C.; Zhao, H. A case-based reasoning system based on weighted heterogeneous value distance metric for breast cancer diagnosis. Artif. Intell. Med. 2017, 77, 31–47. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Liang, C.; Kim, K.S.; Yang, C.; Cheng, W.; Wang, J. Which is more reliable, expert experience or information itself? Weight scheme of complex cases for health management decision making. Int. J. Inf. Technol. Decis. Mak. 2015, 14, 597–620. [Google Scholar] [CrossRef]
- Udwadia, F.E. A new perspective on the tracking control of nonlinear structural and mechanical systems. In Proceedings of the Royal Society of London a: Mathematical, Physical and Engineering Sciences; The Royal Society: London, UK, 2003; Volume 459, pp. 1783–1800. [Google Scholar]
- Huang, K.; Shao, K.; Zhen, S.; Sun, H. A novel approach for modeling and tracking control of a passive-wheel snake robot. Adv. Mech. Eng. 2017, 9, 1–15. [Google Scholar] [CrossRef]
- Zhao, H.; Li, C.; Huang, K.; Sun, H.; Shao, K.; Deng, B. Trajectory tracking control of parallel manipulator based on Udwadia-Kalaba approach. Math. Probl. Eng. 2017, 2017, 1–12. [Google Scholar]
- Sun, H.; Zhao, H.; Zhen, S.; Huang, K.; Zhao, F.; Chen, X.; Chen, Y.H. Application of the Udwadia–Kalaba approach to tracking control of mobile robots. Nonlinear Dyn. 2016, 83, 389–400. [Google Scholar] [CrossRef]
- Sun, H.; Chen, Y.H.; Xiong, Y.; Zhao, H. Configuring tasks as constraints for coordinated mechanical systems: A Udwadia-Kalaba theory based adaptive robust control. J. Frankl. Inst. 2020. [Google Scholar] [CrossRef]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| System Name | DOF (Degree of Freedom) | Supported Movements | Type, Field of Application |
|---|---|---|---|
| ACRE, Schoone [41] | 5 | Shoulder * elbow | Stationary system (end-effector-based), physical therapy |
| MariBot, Rosati [42] | 5 | Shoulder * elbow | Stationary system (end-effector-based, cable-driven robot), physical therapy |
| Robotherapist, Furusho [43] | 6 | Shoulder * elbow * forearm * wrist | Stationary system (end-effector-based), physical therapy |
| iPAM, Culmer [44] | 6 | Shoulder * elbow * forearm | Stationary system (2 robotic arms), physical therapy |
| The proposed rehabilitation robot | 7 | Shoulder * elbow * wrist | Stationary system (end-effector-based), physical therapy and assessment of therapy results |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Liang, C.; Gu, Z.; Zheng, Y.; Wu, Q. A New Design Scheme for Intelligent Upper Limb Rehabilitation Training Robot. Int. J. Environ. Res. Public Health 2020, 17, 2948. https://doi.org/10.3390/ijerph17082948
Zhao Y, Liang C, Gu Z, Zheng Y, Wu Q. A New Design Scheme for Intelligent Upper Limb Rehabilitation Training Robot. International Journal of Environmental Research and Public Health. 2020; 17(8):2948. https://doi.org/10.3390/ijerph17082948
Chicago/Turabian StyleZhao, Yating, Changyong Liang, Zuozuo Gu, Yunjun Zheng, and Qilin Wu. 2020. "A New Design Scheme for Intelligent Upper Limb Rehabilitation Training Robot" International Journal of Environmental Research and Public Health 17, no. 8: 2948. https://doi.org/10.3390/ijerph17082948
APA StyleZhao, Y., Liang, C., Gu, Z., Zheng, Y., & Wu, Q. (2020). A New Design Scheme for Intelligent Upper Limb Rehabilitation Training Robot. International Journal of Environmental Research and Public Health, 17(8), 2948. https://doi.org/10.3390/ijerph17082948