Socioeconomic Disparities in Cancer Treatment, Service Utilization and Catastrophic Health Expenditure in China: A Cross-Sectional Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Indicators
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Study Population
3.2. Cancer Treatment, Health Service Utilization, and Catastrophic Health Expenditure
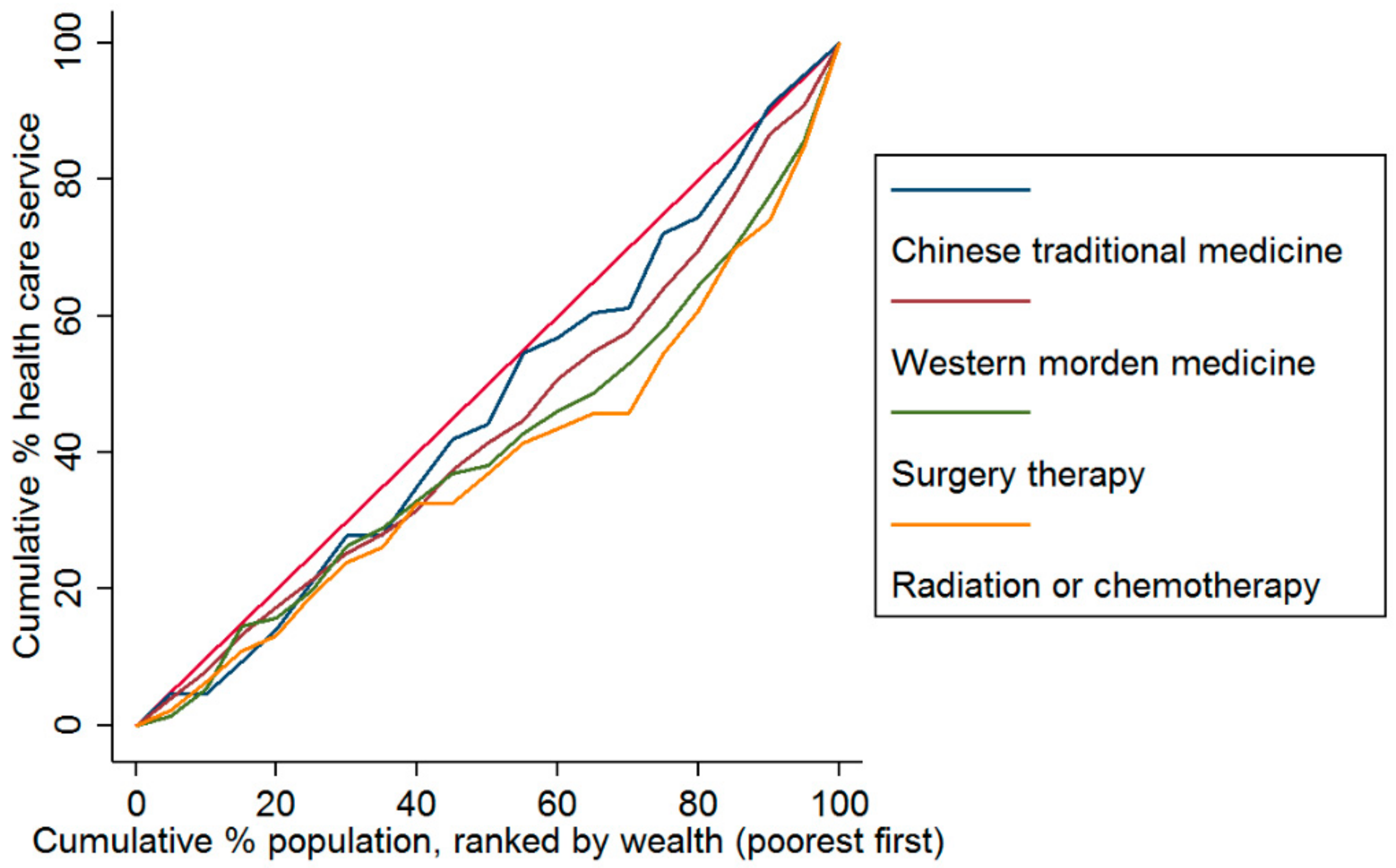
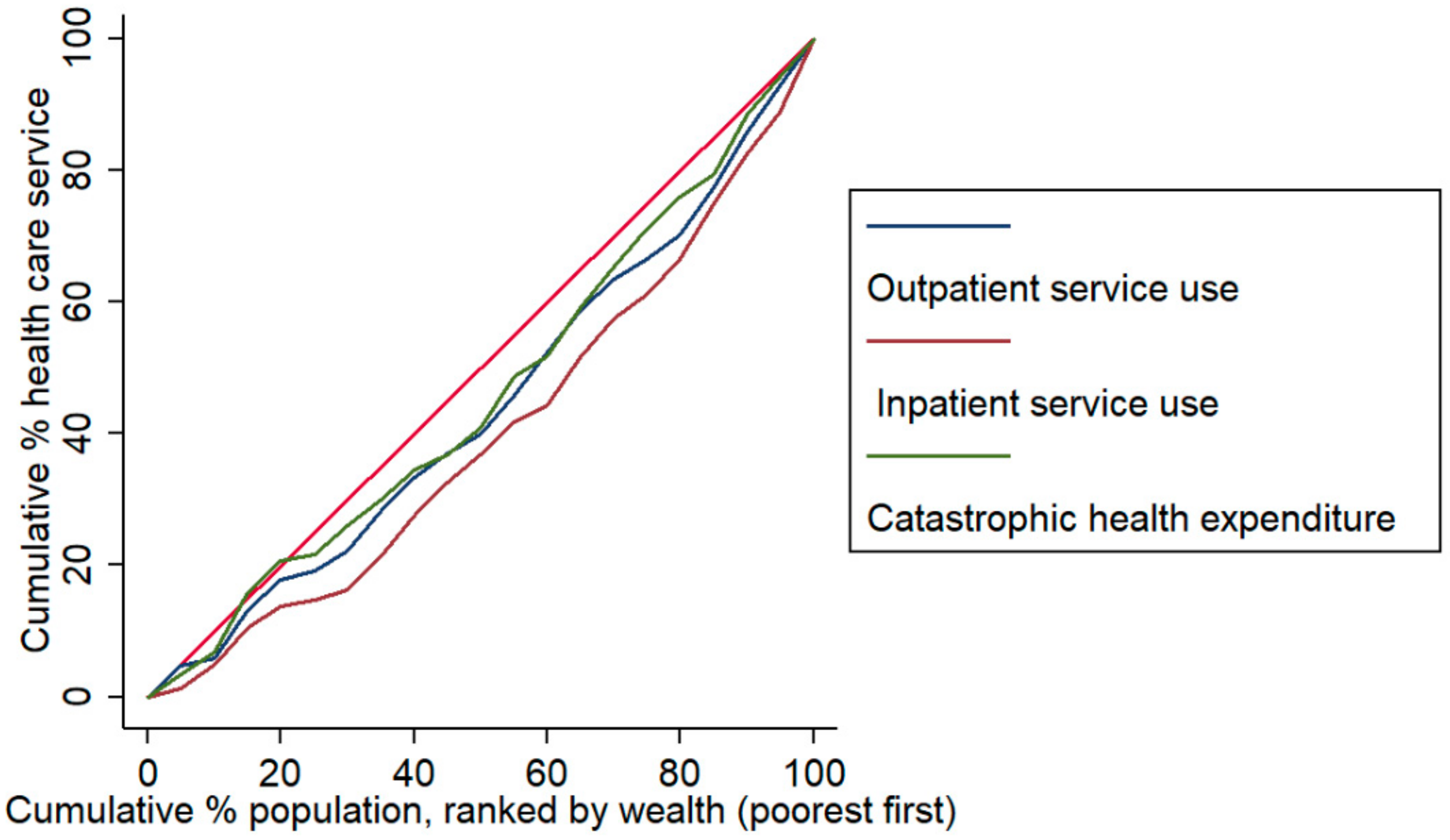
3.3. Economic-Related Disparities in Healthcare for Cancer
3.4. Impacts of the Cancer Treatment on Health Service Use and CHE
4. Discussion
4.1. Impact of Cancer Treatment on Health Service Use
4.2. Association between Cancer Treatment and CHE
4.3. Regional and Economic Disparities in Healthcare and CHE
4.4. Policy Implications
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.; Torre, L.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Eggleston, K.; Hanson, K.; Wu, M. Enhancing financial protection under China’s social health insurance to achieve universal health coverage. BMJ 2019, 365, l2378. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Gao, S.; Rizzo, J. The expansion of public health insurance and the demand for private health insurance in rural China. China Econ. Rev. 2011, 22, 28–41. [Google Scholar] [CrossRef]
- Mao, W.; Tang, S.; Zhu, Y.; Xie, Z.; Chen, W. Financial burden of healthcare for cancer patients with social medical insurance: A multi-centered study in urban China. Int. J. Equity Health 2017, 16, 180. [Google Scholar] [CrossRef] [PubMed]
- Meng, Q.; Xu, L.; Zhang, Y.; Qian, J.; Cai, M.; Xin, Y.; Gao, J.; Xu, K.; Boerma, J.T.; Barber, S.L. Trends in access to health services and financial protection in China between 2003 and 2011: A cross-sectional study. Lancet 2012, 379, 805–814. [Google Scholar] [CrossRef]
- Meng, Q.; Fang, H.; Liu, X.; Yuan, B.; Xu, J. Consolidating the social health insurance schemes in China: Towards an equitable and efficient health system. Lancet 2015, 386, 1484–1492. [Google Scholar] [CrossRef]
- Chatfield, M. Primary Health Care: The Chinese Experience. Health Care Manag. Rev. 1984, 9, 82. [Google Scholar] [CrossRef]
- Kumachev, A.; Trudeau, M.E.; Chan, K.K.W. Associations among socioeconomic status, patterns of care, and outcomes in breast cancer patients in a universal health care system: Ontario’s experience. Cancer 2016, 122, 893–898. [Google Scholar] [CrossRef]
- Aileen, T.; Rachael, G.H.; Linda, S. “It’s at a Time in Your Life When You Are Most Vulnerable”: A Qualitative Exploration of the Financial Impact of a Cancer Diagnosis and Implications for Financial Protection in Health. PLoS ONE 2013, 8, e77549. [Google Scholar] [CrossRef]
- Derouen, M.C.; Parsons, H.M.; Kent, E.E.; Pollock, B.H.; Keegan, T.H.M. Sociodemographic disparities in survival for adolescents and young adults with cancer differ by health insurance status. Cancer Causes Control 2017, 28, 841–851. [Google Scholar] [CrossRef]
- Penson, D.F.; Stoddard, M.L.; Pasta, D.J.; Lubeck, D.P.; Flanders, S.C.; Litwin, M.S. The association between socioeconomic status, health insurance coverage, and quality of life in men with prostate cancer. J. Clin. Epidemiol. 2001, 54, 350–358. [Google Scholar] [CrossRef]
- Fei, X.; Wu, J.; Kong, Z.; Christakos, G. Urban-Rural Disparity of Breast Cancer and Socioeconomic Risk Factors in China. PLoS ONE 2015, 10, e0117572. [Google Scholar] [CrossRef]
- Zhang, Y.; Bu, Y.; Gao, H. Rural–urban disparities of breast cancer patients in China. Med. Oncol. 2012, 30, 387. [Google Scholar] [CrossRef]
- Wen, D.; Wen, X.; Yang, Y.; Chen, Y.; Wei, L.; He, Y.; Shan, B. Urban rural disparity in female breast cancer incidence rate in China and the increasing trend in parallel with socioeconomic development and urbanization in a rural setting. Thorac. Cancer 2017, 9, 262–272. [Google Scholar] [CrossRef]
- Wen, X.; Wen, D.; Yang, Y.; Chen, Y.; Wang, G.; Shan, B. Urban-Rural Disparity in Helicobacter Pylori Infection-Related Upper Gastrointestinal Cancer in China and the Decreasing Trend in Parallel with Socioeconomic Development and Urbanization in an Endemic Area. Ann. Glob. Health 2017, 83, 444–462. [Google Scholar] [CrossRef]
- Wen, D.; Zou, W.; Wen, X.; Yang, Y.; Chen, Y.; He, Y.; Wang, G.; Shan, B. Urban–rural disparity in colorectal cancer incidence and increasing trend in relation to socioeconomic development and urbanization in China. J. Int. Med. Res. 2018, 46, 4181–4196. [Google Scholar] [CrossRef]
- Xia, C.; Ding, C.; Zheng, R.; Zhang, S.; Zeng, H.; Wang, J.; Liao, Y.; Zhang, N.; Yang, Z.; Chen, W. Trends in geographical disparities for cervical cancer mortality in China from 1973 to 2013: A subnational spatio-temporal study. Chin. J. Cancer Res. 2017, 29, 487–495. [Google Scholar] [CrossRef]
- Jiang, X.; Cai, S.; Hu, Y.; Ye, D.; Li, Q.; Chen, K.; Jin, M. Sex disparities in cancer incidence in Jiashan County, China, 1995–2014. Cancer Epidemiol. 2017, 50, 46–52. [Google Scholar] [CrossRef]
- Yang, L.; Zhang, X.; Yang, X.; Yang, J.; Wang, Z.; Chen, H.; Yan, H.-H.; Xu, C.-R.; Guan, J.-L.; He, Y.-Y.; et al. Lung Cancer Treatment Disparities in China: A Question in Need of an Answer. Oncologist 2014, 19, 1084–1090. [Google Scholar] [CrossRef]
- Zhao, Y.; Oldenburg, B.; Mahal, A.; Haregu, T.; Katar, A.; Zhang, L. Trends and inequalities in the health care and hypertension outcomes in China, 2011 to 2015. Int. J. Environ. Res. Public Health 2019, 16, 4578. [Google Scholar] [CrossRef]
- Liu, X.; Sun, X.; Zhao, Y.; Meng, Q. Financial protection of rural health insurance for patients with hypertension and diabetes: Repeated cross-sectional surveys in rural China. BMC Health Serv. Res. 2016, 16, 481. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Oldenburg, B.; Zhao, S.; Haregu, T.; Zhang, L. Temporal trends and geographic disparity in hypertension care in China. J. Epidemiol. 2019, 30, JE20190029. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Oldenburg, B.; Mahal, A.; Lin, Y.; Tang, S.; Liu, X. Trends and socioeconomic disparities in catastrophic health expenditure and health impoverishment in China: 2010 to 2016. Trop. Med. Int. Health 2019, 24, 236–247. [Google Scholar] [CrossRef]
- Yin, P.; Zhang, M.; Li, Y.; Jiang, Y.; Zhao, W. Prevalence of COPD and its association with socioeconomic status in China: Findings from China Chronic Disease Risk Factor Surveillance 2007. BMC Public Health 2011, 11, 586. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, L.; Zhao, S.; Zhang, L. Impact of multimorbidity on health service use and catastrophic health expenditure in China: An analysis of data from a nationwide longitudinal survey. Lancet 2019, 394 (Suppl. 1), S69. [Google Scholar] [CrossRef]
- Yao, N.; Wang, J.; Cai, Y.; Yuan, J.; Wang, H.; Gong, J.; Anderson, R.; Sun, X. Patterns of cancer screening, incidence and treatment disparities in China: Protocol for a population-based study. BMJ Open 2016, 6, e012028. [Google Scholar] [CrossRef]
- Zhao, Y.; Hu, Y.; Smith, J.; Strauss, J.; Yang, G. Cohort Profile: The China Health and Retirement Longitudinal Study (CHARLS). Int. J. Epidemiol. 2012, 43, 61–68. [Google Scholar] [CrossRef]
- Raban, M.; Dandona, R.; Dandona, L. Variations in catastrophic health expenditure estimates from household surveys in India. Bull. World Health Organ. 2013, 91, 726–735. [Google Scholar] [CrossRef]
- Brinda, E.; Kowal, P.; Attermann, J.; Enemark, U. Health service use, out-of-pocket payments and catastrophic health expenditure among older people in India: The WHO Study on global AGEing and adult health (SAGE). J. Epidemiol. Community Health 2015, 69, 489–494. [Google Scholar] [CrossRef]
- Ranson, M.K. Reduction of catastrophic health care expenditures by a community-based health insurance scheme in Gujarat, India: Current experiences and challenges. Bull. World Health Organ. 2002, 80, 613–621. [Google Scholar]
- O’Donnell, O.; Van Doorslaer, E.; Wagstaff, A.; Lindelow, M. Analyzing Health Equity Using Household Survey Data: A Guide to Techniques and Their Implementation; World Bank Publications: Washington, DC, USA, 2008; pp. 83–93. [Google Scholar]
- Chumbler, N.; Kobb, R.; Harris, L.; Richardson, L.; Darkins, A.; Sberna, M.; Neha, D.; Patricia, R.; Molla, D.; Gary, L.K. Healthcare Utilization Among Veterans Undergoing Chemotherapy. J. Ambul. Care Manag. 2007, 30, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Deal, A.; Kris, M.; Scher, H.; Hudis, C.; Sabbatini, P.; Rogak, L.; Bennett, A.V.; Dueck, A.C.; Atkinson, T.M.; et al. Symptom Monitoring With Patient-Reported Outcomes During Routine Cancer Treatment: A Randomized Controlled Trial. J. Clin. Oncol. 2016, 34, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Shi, J.; Guo, L.; Zhu, X.; Wang, L.; Liao, X.; Liu, G.X.; Bai, Y.N.; Mao, A.Y.; Ren, J.S.; et al. Expenditure and financial burden for common cancers in China: A hospital-based multicentre cross-sectional study. Lancet 2016, 388, S10. [Google Scholar] [CrossRef]
- Choi, J.; Cho, K.; Choi, Y.; Han, K.; Kwon, J.; Park, E. Changes in Economic Status of Households Associated with Catastrophic Health Expenditures for Cancer in South Korea. Asian Pac. J. Cancer Prev. 2014, 15, 2713–2717. [Google Scholar] [CrossRef]
- Penson, D. Re: Financial Hardship Associated with Cancer in the United States: Findings from a Population-Based Sample of Adult Cancer Survivors. J. Urol. 2016, 196, 1234. [Google Scholar] [CrossRef]
- Mariotto, A.; Robin Yabroff, K.; Shao, Y.; Feuer, E.; Brown, M. Projections of the Cost of Cancer Care in the United States: 2010–2020. JNCI J. Natl. Cancer Inst. 2011, 103, 117–128. [Google Scholar] [CrossRef]
- Brown, M.; Riley, G.; Schussler, N.; Etzioni, R. Estimating Health Care Costs Related to Cancer Treatment from SEER-Medicare Data. Med. Care 2002, 40, IV104–IV117. [Google Scholar] [CrossRef]
- Stommel, M.; Given, C.; Given, B. The cost of cancer home care to families. Cancer 1993, 71, 1867–1874. [Google Scholar] [CrossRef]
- Rim, S.; Guy, G.; Yabroff, K.; McGraw, K.; Ekwueme, D. The impact of chronic conditions on the economic burden of cancer survivorship: A systematic review. Expert Rev. Pharm. Outcomes Res. 2016, 16, 579–589. [Google Scholar] [CrossRef]
- Yabroff, K.; Kim, Y. Time costs associated with informal caregiving for cancer survivors. Cancer 2009, 115, 4362–4373. [Google Scholar] [CrossRef]
- Dowling, E.; Chawla, N.; Forsythe, L.; de Moor, J.; McNeel, T.; Rozjabek, H.M.; Ekwueme, D.U.; Yabroff, K.R. Lost productivity and burden of illness in cancer survivors with and without other chronic conditions. Cancer 2013, 119, 3393–3401. [Google Scholar] [CrossRef] [PubMed]
- Hollenbeck, B. Commentary on Cancer survivors and unemployment: A meta-analysis and meta-regression. Urol. Oncol. Semin. Orig. Investig. 2009, 27, 577. [Google Scholar] [CrossRef]
- Yardim, M.; Cilingiroglu, N.; Yardim, N. Catastrophic health expenditure and impoverishment in Turkey. Health Policy 2010, 94, 26–33. [Google Scholar] [CrossRef]
- Li, Y.; Wu, Q.; Xu, L.; Legge, D.; Hao, Y.; Gao, L.; Ning, N.; Wan, G. Factors affecting catastrophic health expenditure and impoverishment from medical expenses in China: Policy implications of universal health insurance. Bull. World Health Organ. 2012, 90, 664–671. [Google Scholar] [CrossRef]
- Xinhua, China to Add More Cancer Drugs on MEDICAL Insurance List. Available online: https://www.chinadailyhk.com/articles/247/66/101/1539231359976.html?newsId=50485 (accessed on 11 October 2019).
- Statistical Bulletin on National Economic and Social Development in 2015. Available online: http://www.stats.gov.cn/tjsj/zxfb/201602/t20160229_1323991.html (accessed on 15 September 2019).
- Wu, R.X.; Cai, Y.; Lan, L.; Fan, Z.W.; Xue, M. Trend analysis on the allocation of primary health care resources between urban and rural areas in China from 2008 to 2015. Chin. Health Resour. 2017, 3, 20–23. [Google Scholar]
- Zheng, R.; Sun, K.; Zhang, S.; Zeng, H.; Zou, X.; Chen, R.; Gu, X.Y.; Wei, W.W.; He, J. Report of Cancer Epidemiology in China, 2015. Chin. J. Oncol. 2019, 41, 19–28. [Google Scholar] [CrossRef]
- Chen, W.; Zheng, R.; Baade, P.; Zhang, S.; Zeng, H.; Bray, F.; Jemal, A.; Yu, X.Q.; He, J. Cancer statistics in China, 2015. CA Cancer J. Clin. 2016, 66, 115–132. [Google Scholar] [CrossRef]
- Yu, H. Universal health insurance coverage for 1.3 billion people: What accounts for China’s success? Health Policy 2015, 119, 1145–1152. [Google Scholar] [CrossRef]
- Niu, J.; Qi, Y. Regional Disparity in China’s Medical Insurance System and Its Implication on Health Service Use. Sociol. Rev. China 2016, 4, 43. [Google Scholar]
- Li, Y.; Ying, C.; Sufang, G.; Brant, P.; Bin, L.; Hipgrave, D. Evaluation, in three provinces, of the introduction and impact of China’s National Essential Medicines Scheme. Bull. World Health Organ. 2013, 91, 184–194. [Google Scholar] [CrossRef]
- Liu, G.; Vortherms, S.; Hong, X. China’s Health Reform Update. Annu. Rev. Public Health 2017, 38, 431–448. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Pang, M.; Beard, J. Health system strengthening and hypertension awareness, treatment and control: Data from the China Health and Retirement Longitudinal Study. Bull. World Health Organ. 2013, 92, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Levin, C.; Sellors, J.; Shi, J.; Ma, L.; Qiao, Y.; Ortendahl, J.; O’Shea, M.K.H.; Goldie, S.J. Cost-effectiveness analysis of cervical cancer prevention based on a rapid human papillomavirus screening test in a high-risk region of China. Int. J. Cancer 2010, 127, 1404–1411. [Google Scholar] [CrossRef] [PubMed]
- Raina, P.; Torrance-Rynard, V.; Wong, M.; Woodward, C. Agreement between self-reported and routinely collected healthcare utilization data among seniors. Health Serv. Res. 2002, 37, 751–774. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Number | Unweighted Proportion, % | Weighted Proportion, % |
|---|---|---|---|
| Total | 381 | 100.00 | 100.00 |
| Age (years) | |||
| 45–60 | 185 | 48.56 | 50.94 |
| ≥60 | 196 | 51.44 | 49.06 |
| Gender | |||
| Male | 120 | 31.50 | 37.06 |
| Female | 261 | 68.50 | 62.94 |
| Marital status | |||
| Married/partnered | 336 | 88.19 | 86.65 |
| Never married/divorced | 45 | 11.81 | 13.35 |
| Level of education | |||
| Primary school/below | 269 | 70.60 | 69.27 |
| Middle school/above | 112 | 29.40 | 30.73 |
| Residence location | |||
| Urban area | 170 | 44.62 | 56.90 |
| Rural area | 211 | 55.38 | 43.10 |
| Region | |||
| East | 158 | 41.47 | 52.11 |
| Central | 145 | 38.06 | 31.28 |
| West | 78 | 20.47 | 16.61 |
| Health insurance | |||
| None | 41 | 10.76 | 9.37 |
| NCMS | 218 | 57.22 | 43.98 |
| URBMI/others | 59 | 15.49 | 25.15 |
| UEBMI | 63 | 16.54 | 21.50 |
| Complication | |||
| None | 134 | 35.17 | 31.00 |
| 1–2 | 135 | 35.43 | 45.06 |
| 3 and above | 112 | 29.40 | 23.94 |
| PCE, Mean (CNY) | |||
| All | 259 | 21,450.27 | 21,594.80 |
| Rural | 150 | 18,161.54 | 17,866.11 |
| Urban | 109 | 25,976.04 | 25,452.49 |
| Variables | Total | Urban | Rural | p Value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| All patients | 381 | 100.00 | 170 | 100.00 | 211 | 100.00 | |
| Overall treatments | 189 | 49.61 | 95 | 55.88 | 94 | 44.55 | 0.028 |
| Chinese traditional medicine (TCM) | 70 | 18.37 | 39 | 22.94 | 31 | 14.69 | 0.039 |
| Western modern medicine (WMM) | 117 | 30.71 | 58 | 34.12 | 59 | 27.96 | 0.195 |
| Medication treatment (TCM or WMM) | 137 | 35.96 | 71 | 41.76 | 66 | 31.28 | 0.034 |
| Surgery therapy | 101 | 26.51 | 51 | 30.00 | 50 | 23.7 | 0.166 |
| Radiation/chemotherapy | 67 | 17.59 | 32 | 18.82 | 35 | 16.59 | 0.569 |
| Multiple treatments | 0 | ||||||
| TCM & WMM | 50 | 13.12 | 26 | 15.29 | 24 | 11.37 | 0.26 |
| Medication & Surgery therapy | 61 | 16.01 | 31 | 18.24 | 30 | 14.22 | 0.288 |
| Medication & Radiation/chemotherapy | 45 | 11.81 | 23 | 13.53 | 22 | 10.43 | 0.351 |
| Surgery & Radiation/chemotherapy | 39 | 10.24 | 22 | 12.94 | 17 | 8.06 | 0.118 |
| Health service use | 0 | 1 | |||||
| Outpatient visit | 115 | 30.18 | 46 | 27.06 | 69 | 32.7 | 0.233 |
| Inpatient visit | 113 | 29.66 | 55 | 32.35 | 58 | 27.49 | 0.301 |
| Outpatient & Inpatient visit | 44 | 11.55 | 18 | 10.59 | 26 | 12.32 | 0.599 |
| Catastrophic health expenditure | 102 | 26.77 | 34 | 20.00 | 68 | 32.23 | 0.007 |
| PCE, Quartile | Chinese Traditional Medicine | Western Modern Medicine | Surgery Therapy | Radiation/Chemotherapy | Outpatient Service Use | Inpatient Service Use | Catastrophic Health Expenditure |
|---|---|---|---|---|---|---|---|
| All | |||||||
| 1st (Lowest) | 13.85 | 24.62 | 23.08 | 13.85 | 24.62 | 18.46 | 29.23 |
| 2nd | 15.38 | 23.08 | 21.54 | 12.31 | 27.69 | 27.69 | 26.15 |
| 3rd | 18.46 | 26.15 | 23.08 | 12.31 | 33.85 | 29.23 | 40.00 |
| 4th (Highest) | 18.75 | 42.19 | 50.00 | 32.81 | 43.75 | 48.44 | 39.06 |
| Ratio (highest/lowest) | 1.35 | 1.71 | 2.17 | 2.37 | 1.78 | 2.62 | 1.34 |
| p value | 0.849 | 0.061 | 0.001 | 0.004 | 0.099 | 0.002 | 0.239 |
| Urban | |||||||
| 1st (Lowest) | 21.43 | 28.57 | 25.00 | 17.86 | 21.43 | 14.29 | 25.00 |
| 2nd | 18.52 | 29.63 | 18.52 | 3.70 | 33.33 | 22.22 | 14.81 |
| 3rd | 22.22 | 33.33 | 29.63 | 18.52 | 18.52 | 33.33 | 25.93 |
| 4th (Highest) | 25.93 | 40.74 | 59.26 | 37.04 | 44.44 | 59.26 | 37.04 |
| Ratio (highest/lowest) | 1.21 | 1.43 | 2.37 | 2.07 | 2.07 | 4.15 | 1.48 |
| p value | 0.932 | 0.772 | 0.008 | 0.021 | 0.136 | 0.002 | 0.321 |
| Rural | |||||||
| 1st (Lowest) | 7.89 | 18.42 | 21.05 | 7.89 | 28.95 | 23.68 | 36.84 |
| 2nd | 16.22 | 24.32 | 27.03 | 18.92 | 29.73 | 21.62 | 24.32 |
| 3rd | 10.53 | 18.42 | 18.42 | 10.53 | 36.84 | 36.84 | 52.63 |
| 4th (Highest) | 16.22 | 43.24 | 40.54 | 29.73 | 43.24 | 37.84 | 43.24 |
| Ratio (highest/lowest) | 2.06 | 2.35 | 1.93 | 3.77 | 1.49 | 1.60 | 1.17 |
| p value | 0.619 | 0.045 | 0.134 | 0.050 | 0.526 | 0.274 | 0.084 |
| Treatment Type | Outpatient Visit | Inpatient Visit | Catastrophic Health Expenditure | ||||||
|---|---|---|---|---|---|---|---|---|---|
| AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | ||||
| All | |||||||||
| Chinese traditional medicine | 2.156 * | 1.193 | 3.896 | 1.091 | 0.589 | 2.019 | 1.873 | 0.987 | 3.554 |
| Western modern medicine | 2.171 ** | 1.292 | 3.649 | 1.124 | 0.658 | 1.919 | 1.358 | 0.779 | 2.367 |
| Surgery therapy | 2.224 ** | 1.299 | 3.809 | 2.244 ** | 1.313 | 3.834 | 3.697 *** | 2.052 | 6.662 |
| Radiation/chemotherapy | 1.373 | 0.731 | 2.579 | 2.504 ** | 1.369 | 4.579 | 2.361 ** | 1.232 | 4.526 |
| Treatment overall | 2.492 *** | 1.506 | 4.125 | 1.817 * | 1.098 | 3.007 | 2.744 *** | 1.578 | 4.772 |
| Urban | |||||||||
| Chinese traditional medicine | 1.973 | 0.828 | 4.697 | 1.161 | 0.481 | 2.805 | 2.763 * | 1.045 | 7.307 |
| Western modern medicine | 2.606 * | 1.135 | 5.981 | 1.500 | 0.673 | 3.343 | 2.389 | 0.977 | 5.839 |
| Surgery therapy | 2.077 | 0.905 | 4.765 | 3.487 ** | 1.509 | 8.058 | 9.723 *** | 3.393 | 27.866 |
| Radiation/chemotherapy | 2.255 | 0.852 | 5.963 | 2.290 | 0.889 | 5.901 | 3.080 * | 1.066 | 8.898 |
| Treatment overall | 2.168 | 0.968 | 4.855 | 2.441 * | 1.108 | 5.379 | 7.277 ** | 2.325 | 22.774 |
| Rural | |||||||||
| Chinese traditional medicine | 2.315 | 0.968 | 5.539 | 0.906 | 0.345 | 2.382 | 1.303 | 0.492 | 3.447 |
| Western modern medicine | 1.991 | 0.975 | 4.067 | 0.950 | 0.436 | 2.070 | 1.088 | 0.500 | 2.366 |
| Surgery therapy | 3.169 ** | 1.440 | 6.974 | 1.802 | 0.820 | 3.961 | 2.726 * | 1.212 | 6.131 |
| Radiation/chemotherapy | 1.101 | 0.457 | 2.655 | 3.603 ** | 1.496 | 8.682 | 3.402 * | 1.270 | 9.115 |
| Treatment overall | 3.017 ** | 1.536 | 5.929 | 1.654 | 0.822 | 3.329 | 2.133 * | 1.057 | 4.306 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Zhang, L.; Fu, Y.; Wang, M.; Zhang, L. Socioeconomic Disparities in Cancer Treatment, Service Utilization and Catastrophic Health Expenditure in China: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2020, 17, 1327. https://doi.org/10.3390/ijerph17041327
Zhao Y, Zhang L, Fu Y, Wang M, Zhang L. Socioeconomic Disparities in Cancer Treatment, Service Utilization and Catastrophic Health Expenditure in China: A Cross-Sectional Analysis. International Journal of Environmental Research and Public Health. 2020; 17(4):1327. https://doi.org/10.3390/ijerph17041327
Chicago/Turabian StyleZhao, Yang, Lin Zhang, Yu Fu, Minyu Wang, and Luwen Zhang. 2020. "Socioeconomic Disparities in Cancer Treatment, Service Utilization and Catastrophic Health Expenditure in China: A Cross-Sectional Analysis" International Journal of Environmental Research and Public Health 17, no. 4: 1327. https://doi.org/10.3390/ijerph17041327
APA StyleZhao, Y., Zhang, L., Fu, Y., Wang, M., & Zhang, L. (2020). Socioeconomic Disparities in Cancer Treatment, Service Utilization and Catastrophic Health Expenditure in China: A Cross-Sectional Analysis. International Journal of Environmental Research and Public Health, 17(4), 1327. https://doi.org/10.3390/ijerph17041327