Co-producing Progression Criteria for Feasibility Studies: A Partnership between Patient Contributors, Clinicians and Researchers

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
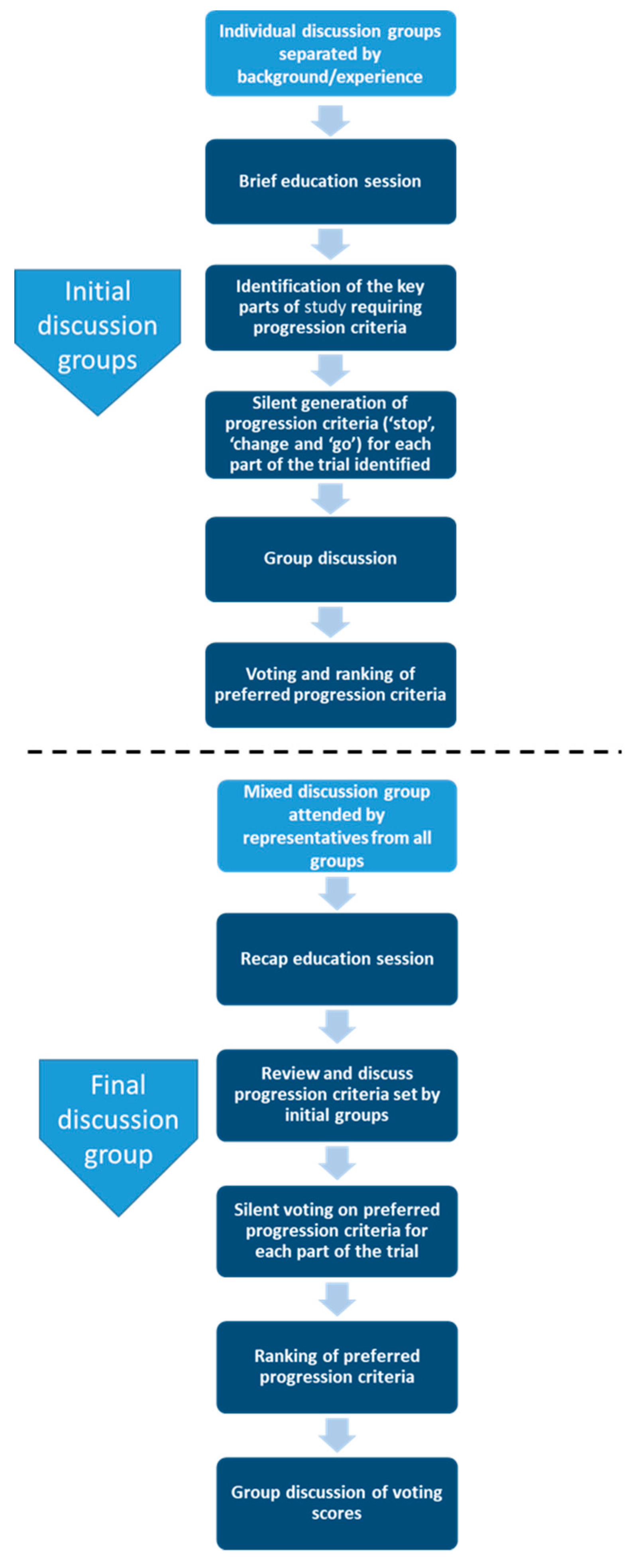
2.1. Design
2.2. Group Members and Settings
2.3. Stage One. Initial Discussion Groups
2.4. Stage Two. Final Discussion Group
2.5. Impact Evaluation
2.6. Ethics Approval
3. Results
3.1. Initial Groups
3.2. Characteristics of Final Groups
3.3. Ranking of Progression Criteria
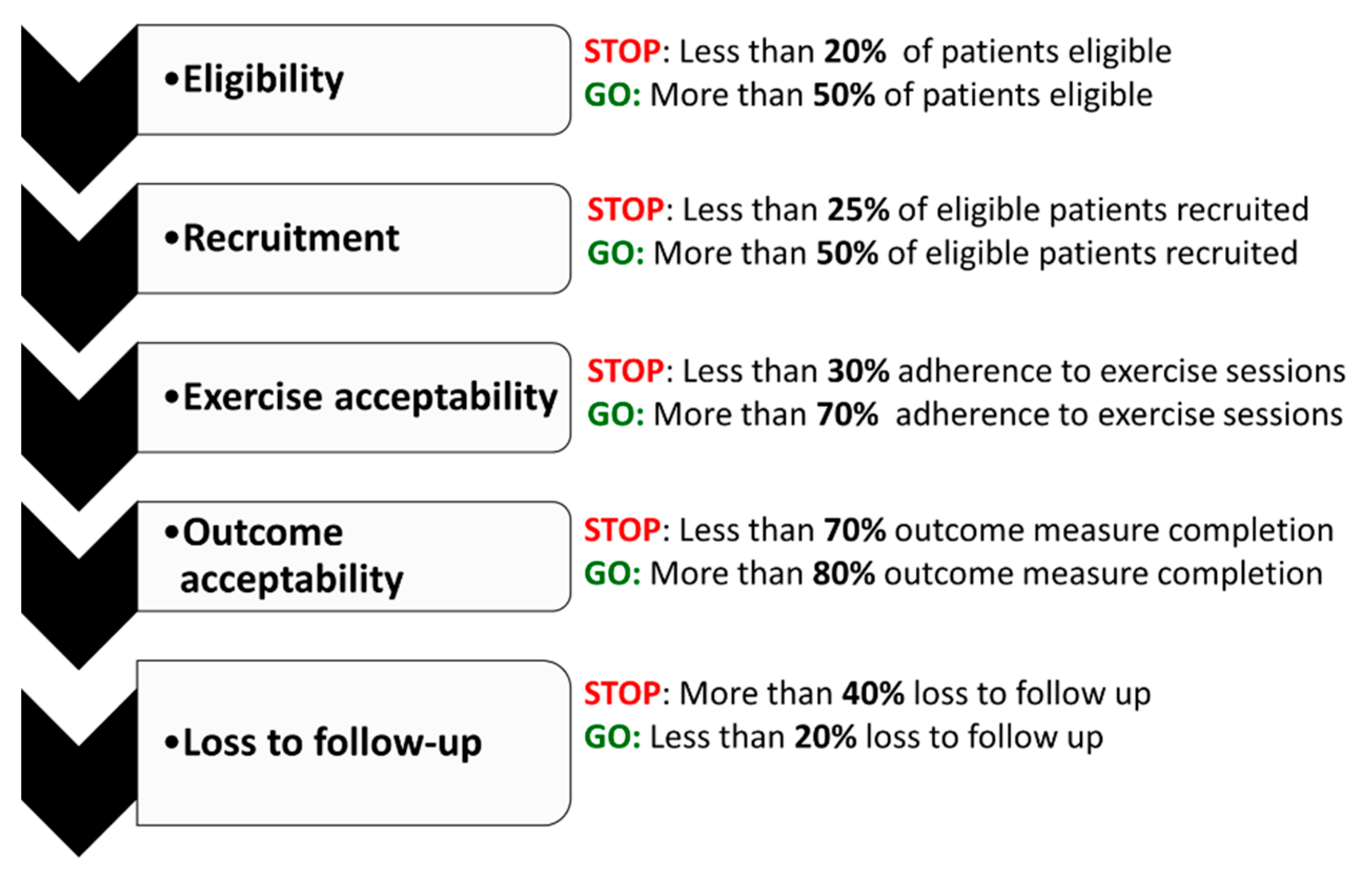
3.4. Final Progression Criteria
3.5. Change Criteria
3.6. Resource Implications
3.7. Impact and Feedback
4. Discussion
4.1. Involving Patients, Clinicians and Researchers Equally in the Co-Production of Progression Criteria
4.2. The Challenges of Co-Producing Progression Criteria
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bugge, C.; Williams, B.; Hagen, S.; Logan, J.; Glazener, C.; Pringle, S.; Sinclair, L. A process for decision-making after pilot and feasibility trials (ADePT): Development following a feasibility study of a complex intervention for pelvic organ prolapse. Trials 2013, 14, 353. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; MacIntyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new medical research council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. Pilot Feasibility Study 2016, 2, 64. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, G.A.; Dodd, S.; Williamson, P.R. Design and analysis of pilot studies: Recommendations for good practice. J. Eval. Clin. Pract. 2004, 10, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: The what, why and how. BMC Med. Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef]
- National Institute of Health Research. Feasibility and Pilot Studies. 2017. Available online: https://www.nihr.ac.uk/funding-and-support/documents/funding-for-research-studies/research-programmes/PGfAR/CCF-PGfAR-Feasibility-and-Pilot-studies.pdf (accessed on 8 February 2019).
- Hallingberg, B.; Turley, R.; Segrott, J.; Wight, D.; Craig, P.; Craig, L.; Murphy, S.; Robling, M.; Simpson, A.; Moore, G. Feasibility studies to decide whether and how to proceed with full-scale evaluations of public health interventions: A systematic review of guidance. Pilot Feasibility Study 2018, 4, 104. [Google Scholar] [CrossRef]
- Shanyinde, M.; Pickering, R.M.; Weatherall, M. Questions asked and answered in pilot and feasibility randomized controlled trials. BMC Med. Res. Methodol. 2011, 11, 117. [Google Scholar] [CrossRef]
- Avery, K.N.L.; Williamson, P.R.; Gamble, C.; Francischetto, E.O.; Metcalfe, C.; Davidson, P.; Williams, H.; Blazeby, J.M.; Blencowe, N.; Bugge, C.; et al. Informing efficient randomised controlled trials: Exploration of challenges in developing progression criteria for internal pilot studies. BMJ Open 2017, 7, e013537. [Google Scholar] [CrossRef]
- Craig, P.; Di Ruggiero, E.; Frolich, K.L.; Mykhalovskiy, E.; White, M.; On Behalf of the Canadian Institutes of Health Research (CIHR)–National Institute for Health Research (NIHR) Context Guidance Authors Group. Taking Account of Context in Population Health Intervention Research: Guidance for Producers, Users and Funders of Research; NIHR Journals Library: Southampton, UK, 2018 April. Available online: https://www.ncbi.nlm.nih.gov/books/NBK498645/ (accessed on 8 February 2019). [CrossRef]
- INVOLVE. Guidance on Co-Producing a Research Project. 2018. Available online: https://www.invo.org.uk/posttypepublication/guidance-on-co-producing-a-research-project/ (accessed on 7 February 2019).
- Price, A.; Albarqouni, L.; Kirkpatrick, J.; Clarke, M.; Liew, S.M.; Roberts, N.; Burls, A. Patient and public involvement in the design of clinical trials: An overview of systematic reviews. J. Eval. Clin. Pract. 2018, 24, 240–253. [Google Scholar] [CrossRef]
- Yardley, L.; Ainsworth, B.; Arden-Close, E.; Muller, I. The person-based approach to enhancing the acceptability and feasibility of interventions. Pilot Feasibility Study 2015, 1, 37. [Google Scholar] [CrossRef]
- Barratt, H.; Campbell, M.; Moore, L.; Zwarenstein, M.; Bower, P. Randomised controlled trials of complex interventions and large-scale transformation of services. Health Serv. Deliv. Res. 2016, 4, 16. [Google Scholar]
- O’Cathain, A.; Hoddinott, P.; Lewin, S.; Thomas, K.; Young, B.; Adamson, J.; Jansen, Y.; Mills, N.; Moore, G.; Donovan, J. Maximising the impact of qualitative research in feasibility studies for randomised controlled trials: Guidance for researchers. Pilot Feasibility Study 2015, 1, 32. [Google Scholar] [CrossRef] [PubMed]
- MRC Clinical Trials Series. MRC Guidelines for Management of Global Health Trials Involving Clinical or Public Health Interventions. 2017. Available online: https://mrc.ukri.org/documents/pdf/guidelines-for-management-of-global-health-trials/ (accessed on 7 February 2019).
- National Institute of Health Research. Research Governance Guidelines. 2012. Available online: https://www.nihr.ac.uk/funding-and-support/documents/funding-for-research-studies/how-to-apply/NETSCC_Project_Oversight_Groups_Guidance.pdf (accessed on 7 February 2019).
- Harman, N.L.; Conroy, E.J.; Lewis, S.C.; Murray, G.; Norrie, J.; Sydes, M.; Lane, J.A.; Altman, D.G.; Baigent, C.; Bliss, J.M.; et al. Exploring the role and function of trial steering committees: Results of an expert panel meeting. Trials 2015, 16, 597. [Google Scholar] [CrossRef]
- Buck, D.; Gamble, C.; Dudley, L.; Preston, J.; Hanley, B.; Williamson, P.R.; Young, B. From plans to actions in patient and public involvement: Qualitative study of documented plans and the accounts of researchers and patients sampled from a cohort of clinical trials. BMJ Open 2014, 4, e006400. [Google Scholar] [CrossRef] [PubMed]
- Dudley, L.; Gamble, C.; Preston, J.; Buck, D.; Hanley, B.; Williamson, P.; Young, B. What difference does patient and public involvement make and what are its pathways to impact? Qualitative study of patients and researchers from a cohort of randomised clinical trials. PLoS ONE 2015, 10, e0128817. [Google Scholar] [CrossRef]
- Department of Health and Human Services, Centres for Disease Control and Prevention. Gaining Consensus among Stakeholders through the Nominal Group Technique. 2006. Available online: https://www.cdc.gov/healthyyouth/evaluation/pdf/brief7.pdf (accessed on 7 February 2019).
- Potter, M.; Gordon, S.; Hamer, P. The nominal group technique: A useful consensus methodology in physiotherapy research. N. Z. J. Physiother. 2004, 32, 126–130. [Google Scholar]
- McMillan, S.S.; Kelly, F.; Sav, A.; Kendall, E.; King, M.A.; Whitty, J.A.; Wheeler, A.J. Using the nominal group technique: How to analyse across multiple groups. Health Serv. Outcomes Res. 2014, 14, 92–108. [Google Scholar] [CrossRef]
- Ospina, M.B.; Michas, M.; Deuchar, L.; Leigh, R.; Bhutani, M.; Rowe, B.H.; Marciniuk, D.; Goodridge, D.; Dechman, G.; Bourbeau, J.; et al. Development of a patient-centred, evidence-based and consensus-based discharge care bundle for patients with acute exacerbation of chronic obstructive pulmonary disease. BMJ Open Respir. Res. 2018, 5, e000265. [Google Scholar] [CrossRef]
- Haugland, H.; Rehn, M.; Klepstad, P.; Krüger, A. Developing quality indicators for physician-staffed emergency medical services: A consensus process. Scand. J. Trauma Resusc. Emerg. Med. 2017, 25, 14. [Google Scholar] [CrossRef]
- Rayment, J.; Lanlehin, R.; McCourt, C.; Husain, S.M. Involving seldom-heard groups in a PPI process to inform the design of a proposed trial on the use of probiotics to prevent preterm birth: A case study. Res. Involv. Engagem. 2017, 3, 11. [Google Scholar] [CrossRef]
- INVOLVE. Policy on Payment of Fees and Expenses for Members of the Public Actively Involved with INVOLVE. 2016. Available online: https://www.invo.org.uk/posttypepublication/involve-policy-on-payments-and-expenses-for-members-of-the-public-including-involve-group-members-february-2016/olicy on payment of fees (accessed on 8 February 2019).
- INVOLVE. Deliberative Public Engagement: Nine Principles. 2008. Available online: https://www.involve.org.uk/sites/default/files/field/attachemnt/Deliberative-public-engagement-nine-principles_1.pdf (accessed on 10 February 2019).
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Pandya-Wood, R.; Barron, D.S.; Elliott, J. A framework for public involvement at the design stage of NHS health and social care research: Time to develop ethically conscious standards. Res. Involv. Engagem. 2017, 3, 6. [Google Scholar] [CrossRef] [PubMed]
- INVOLVE. Jargon Buster. 2019. Available online: https://www.invo.org.uk/resource-centre/jargon-buster/ (accessed on 8 February 2019).
- Age UK and British Geriatrics Society. Frailty: Language and Perceptions. A Report Prepared by BritainThinks on Behalf of Age UK and the British Geriatrics Society. 2015. Available online: https://www.ageuk.org.uk/documents/en-gb/for-professionals/policy/health-and-wellbeing/report_bgs_frailty_language_and_perceptions.pdf?dtrk=true (accessed on 10 February 2019).
- James Lind Alliance. The James Lind Alliance guidebook. Version 8. 2018. Available online: www.jla.nihr.ac.uk/jla-guidebook/downloads/Version-8-JLA-Guidebook-for-download-from-website.pdf (accessed on 10 February 2019).
- Gray, T.A.; Dumville, J.C.; Christie, J.; Cullum, N.A. Rapid research and implementation priority setting for wound care uncertainties. PLoS ONE 2017, 12, e0188958. [Google Scholar] [CrossRef] [PubMed]
- Crocker, J.C.; Boylan, A.; Bostock, J.; Locock, L. Is it worth it? patient and public views on the impact of their involvement in health research and its assessment: A UK-based qualitative interview study. Health Expect. 2017, 20, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Health Research Authority. Is My Project Research? Available online: http://www.hra-decisiontools.org.uk/research/ (accessed on 16 February 2019).
- INVOLVE. Patient and Public Involvement in Research and Research Ethics Committee Review. 2016. Available online: https://www.invo.org.uk/posttypepublication/public-involvement-in-research-and-research-ethics-committee-review/ (accessed on 2 September 2019).
- Heaven, A.; Brown, L.; Foster, M.; Clegg, A. Keeping it credible in cohort multiple randomised controlled trials: The community ageing research 75 (CARE 75) study model of patient and public involvement and engagement. Res. Involv. Engagem. 2016, 2, 30. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Guralnik, J.M.; Studenski, S.; Fried, L.P.; Cutler, G.B.; Walston, J.D. Designing randomized, controlled trials aimed at preventing or delaying functional decline and disability in frail, older persons: A consensus report. J. Am. Geriatr. Soc. 2004, 52, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Dyson, E. Recruitment of frail older people to research: Lessons learnt through experience. J. Adv. Nurs. 2001, 36, 643–651. [Google Scholar] [CrossRef]
- Clarke, D.; Jones, F.; Harris, R.; Robert, G. What outcomes are associated with developing and implementing co-produced interventions in acute healthcare settings? A rapid evidence synthesis. BMJ Open 2017, 7, e014650. [Google Scholar] [PubMed]
- Komaie, G.; Goodman, M.; McCall, A.; McGill, G.; Patterson, C.; Hayes, C.; Thompson, V.S. Training community members in public health research: Development and implementation of a community participatory research pilot project. Health Equity 2018, 2, 282–287. [Google Scholar] [CrossRef]
- Baines, R.L.; Regan de Bere, S. Optimizing patient and public involvement (PPI): Identifying its “essential” and “desirable” principles using a systematic review and modified delphi methodology. Health Expect. 2018, 21, 327–335. [Google Scholar] [CrossRef]
- Isler, M.R.; Brown, A.L.; Eley, N.; Mathews, A.; Batten, K.; Rogers, R.; Powell, N.; White, C.; Underwood, R.; MacQueen, K.M. Curriculum development to increase minority research literacy for HIV prevention research: A CBPR approach. Prog. Community Health Partnersh. Res. Educ. Action 2014, 8, 511. [Google Scholar] [CrossRef] [PubMed]
- Gamble, C.; Dudley, L.; Allam, A.; Bell, P.; Buck, D.; Goodare, H.; Hanley, B.; Preston, J.; Walker, A.; Williamson, P.R.; et al. An Evidence Base to Optimise Methods for Involving Patient and Public Contributors in Clinical Trials: A Mixed-Methods Study; NIHR Journals Library: Southampton, UK, September 2015; (Health Services and Delivery Research, No. 3.39). Available online: https://www.ncbi.nlm.nih.gov/books/NBK316049/ doi:10.3310/hsdr03390 (accessed on 8 February 2019).
- Coats, J.V.; Stafford, J.D.; Sanders Thompson, V.; Johnson Javois, B.; Goodman, M.S. Increasing research literacy: The community research fellows training program. J. Empir. Res. Hum. Res. Ethics 2015, 10, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Goodman, M.S.; Dias, J.J.; Stafford, J.D. Increasing research literacy in minority communities: CARES fellows training program. J. Empir. Res. Hum. Res. Ethics 2010, 5, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.; Yerby, L.; Tucker, M.; Foster, P.P.; Hamilton, K.C.; Fifolt, M.M.; Hites, L.; Shreves, M.K.; Page, S.B.; Bissell, K.L. Bringing community and academic scholars together to facilitate and conduct authentic community based participatory research: Project UNITED. Int. J. Environ. Res. Public Health 2016, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- Ashcroft, J.; Wykes, T.; Taylor, J.; Crowther, A.; Szmukler, G. Impact on the individual: What do patients and carers gain, lose and expect from being involved in research? J. Ment. Health 2016, 25, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.A.; Haring, R.; Rodriguez, E.M.; González, E.; Kaur, J.S.; Kirschner, M.; Tom, L.; O’Brian, C.A.; Katz, M.L. Improving research literacy in diverse minority populations with a novel communication tool. J. Cancer Educ. 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Moran, E.; Duran, N.; Jenders, R.A. Using animation as an information tool to advance health research literacy among minority participants. In Proceedings of the AMIA Annual Symposium, Washington, DC, USA, 16–20 November 2013; p. 475. [Google Scholar]
- James, D.; Warren-Forward, H. Research methods for formal consensus development. Nurse Res. 2015, 22, 35. [Google Scholar] [CrossRef]
- Humphrey-Murto, S.; Varpio, L.; Gonsalves, C.; Wood, T.J. Using consensus group methods such as delphi and nominal group in medical education research. Med. Teach. 2017, 39, 14–19. [Google Scholar] [CrossRef]
- Bagley, H.J.; Short, H.; Harman, N.L.; Hickey, H.R.; Gamble, C.L.; Woolfall, K.; Young, B.; Williamson, P.R. A patient and public involvement (PPI) toolkit for meaningful and flexible involvement in clinical trials—A work in progress. Res. Involv. Engagem. 2016, 2, 15. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Topic | Content |
|---|---|
| Overview of RCT design | What is an RCT? What are complex interventions? Challenges to RCTS of complex interventions |
| Introduction to feasibility studies | What is a feasibility study? |
| Introduction to progression criteria | What are progression criteria? What are they for? How are progression criteria structured? (introduction to ‘stop/go/change’ thresholds) Examples of progression criteria from other studies and analogies from everyday life |
| Overview of the FLEX-HD study | Aims of the study Design of the study and secondary outcomes Overview of the exercise intervention |
| Aspect of the Trial Requiring Progression Criteria | Plain English Explanation Provided in the Discussion Session |
|---|---|
| Eligibility | The number of patients who can take part in the study, whether they later agree to or not. |
| Recruitment | The number of patients who agree to take part in the study |
| Intervention acceptability | Whether participants can stick to the exercise programme |
| Outcome acceptability | Whether participants can complete the assessments at the start and the end of the study. These assessments can tell us whether intervention might be beneficial. |
| Loss to follow-up | The numbers of participants who drop out or were ‘lost’ (lost to follow-up) |
| Group (n) | Members (n) | Age (years) | Gender | Ethnicity | Research Experience (yes) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Female | Male | White British | Asian British | Black British | Not Stated | ||||
| Researcher (2) | 13 | 44 (26–48) | 7 (54%) | 6 (46%) | 10 (77%) | 3 (23%) | 0 (0%) | 0 (0%) | 13 (100%) |
| Clinician (3) | 24 | 38 (33–49) | 20 (80%) | 5 (20%) | 23 (92%) | 1 (4%) | 1 (4%) | 0 (0%) | 7 (28%) |
| Patient (3) | 15 | 63 (50–82) | 10 (67%) | 5 (33%) | 12 (80%) | 2 (13%) | 0 (0%) | 1 (7%) | 12 (80%) |
| Aspect of Trial | Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Progression Criteria | Patient Groups | Researcher Groups | Clinician Groups | |||||||
| Older People’s Group | Renal Patient Group 1 | Renal Patient Group 2 | Age and Aging Research group | Renal Exercise and Rehabilitation Research Group | Renal and Falls Therapist Group | Older People’s Therapist Group | Renal Doctors and Nurses’ Group | |||
| n = 8 | n = 4 | n = 2 | n = 8 | n = 5 | n = 7 | n = 6 | n = 12 | |||
| Eligibility % | Stop | <50% | <30% | <50% | <15% | <20% | <45% | <15% | <5% | |
| Go | >75% | >45% | >25% | >40% | >65% | >30% | >20% | |||
| Recruitment % | Stop | <25% | <35% | <30% | <30% | <20% | <25% | <40% | ||
| Go | >80% | >60% | >20% | >30% | >50% | >55% | >50% | >50% | ||
| Intervention acceptability (Adherence %) | Stop | <60% | <50% | <25% | <65% | <65% | <50% | <50% | ||
| Go | >75% | >60% | >40% | >75% | >80% | >70% | >75% | >70% | ||
| Outcome acceptability (Completion %) | Stop | <55% | <60% | <70–80% | <80% | <60% | <80% | |||
| Go | >66% | >80% | >40% | >80–90% | >60% | >90% | ||||
| Loss to follow up (% withdrawn or lost) | Stop | >55% | >60% | >80% | >80% | >40% | >50% | >40% | >30% | |
| Go | <25% | <50% | <25% | <40% | <25% | <20% | <25% | <20% | ||
| Aspect of Trial | Results Agreed For Voting | Voting Scores | Ranking | Final Criteria If Tied Ranking | |
|---|---|---|---|---|---|
| Eligibility | Stop | <20% | 22 | 1 | |
| <30% | 18 | 2 | |||
| Go | >40% | 15 | = 2 | ||
| >45% | 15 | = 2 | |||
| >50% | 16 | 1 | |||
| Recruitment | Stop | <20% | 16 | 2 | |
| <25% | 17 | = 1 | <25 | ||
| <30% | 17 | = 1 | |||
| Go | >50% | 24 | 1 | ||
| Intervention acceptability (adherence %) | Stop | <25% | 6 | 3 | |
| <30% | 21 | 1 | |||
| <50% | 16 | 2 | |||
| Go | >70% | 18 | 1 | ||
| >75% | 15 | 2 | |||
| >80% | 12 | 3 | |||
| Outcome acceptability (measure completion %) | Stop | <60% | 19 | = 1 | <70 |
| <80% | 19 | = 1 | |||
| Go | >80% | 20 | 1 | ||
| >90% | 15 | 2 | |||
| Loss to follow up | Stop | >30% | 17 | = 1 | >40 |
| >50% | 17 | = 1 | |||
| Go | <20% | 18 | = 1 | <20 | |
| <25% | 18 | = 1 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Young, H.M.L.; Goodliffe, S.; Madhani, M.; Phelps, K.; Regen, E.; Locke, A.; Burton, J.O.; Singh, S.J.; Smith, A.C.; Conroy, S. Co-producing Progression Criteria for Feasibility Studies: A Partnership between Patient Contributors, Clinicians and Researchers. Int. J. Environ. Res. Public Health 2019, 16, 3756. https://doi.org/10.3390/ijerph16193756
Young HML, Goodliffe S, Madhani M, Phelps K, Regen E, Locke A, Burton JO, Singh SJ, Smith AC, Conroy S. Co-producing Progression Criteria for Feasibility Studies: A Partnership between Patient Contributors, Clinicians and Researchers. International Journal of Environmental Research and Public Health. 2019; 16(19):3756. https://doi.org/10.3390/ijerph16193756
Chicago/Turabian StyleYoung, Hannah M. L., Samantha Goodliffe, Meeta Madhani, Kay Phelps, Emma Regen, Anthony Locke, James O. Burton, Sally J. Singh, Alice C. Smith, and Simon Conroy. 2019. "Co-producing Progression Criteria for Feasibility Studies: A Partnership between Patient Contributors, Clinicians and Researchers" International Journal of Environmental Research and Public Health 16, no. 19: 3756. https://doi.org/10.3390/ijerph16193756
APA StyleYoung, H. M. L., Goodliffe, S., Madhani, M., Phelps, K., Regen, E., Locke, A., Burton, J. O., Singh, S. J., Smith, A. C., & Conroy, S. (2019). Co-producing Progression Criteria for Feasibility Studies: A Partnership between Patient Contributors, Clinicians and Researchers. International Journal of Environmental Research and Public Health, 16(19), 3756. https://doi.org/10.3390/ijerph16193756