Morehouse Choice Accountable Care Organization and Education System (MCACO-ES): Integrated Model Delivering Equitable Quality Care

 ,
,  , ,
, ,
Abstract
:1. Introduction
- Builds on the history, mission and value proposition for unparalleled community health improvement of M-ACO and its partners.
- Incorporates its distinguished training capacity to expand knowledge and understanding about value-based care to clinical care and health administration teams.
- Optimizes existing and new collaborative community relationships.
- Makes use of comprehensive, aggregated data and vast experience with underserved populations.
- Addresses health disparities and social determinants of health.
2. Materials and Methods
2.1. M-ACO Participant Organizations
2.2. Program Goals and Objectives
- Re-design Patient Care to attain “Triple Aim” goals [11]
- Research and engagement of providers and patients in predominantly underserved communities
- Education and Training utilizing scalable, digital training models
- Community Health bridging biopsychosocial determinants to health outcomes
- Payment Reform with Aligned Incentives across independent health care organizations
2.3. Demographics of M-ACO Service Area
2.4. Hypothesis
2.5. Approach
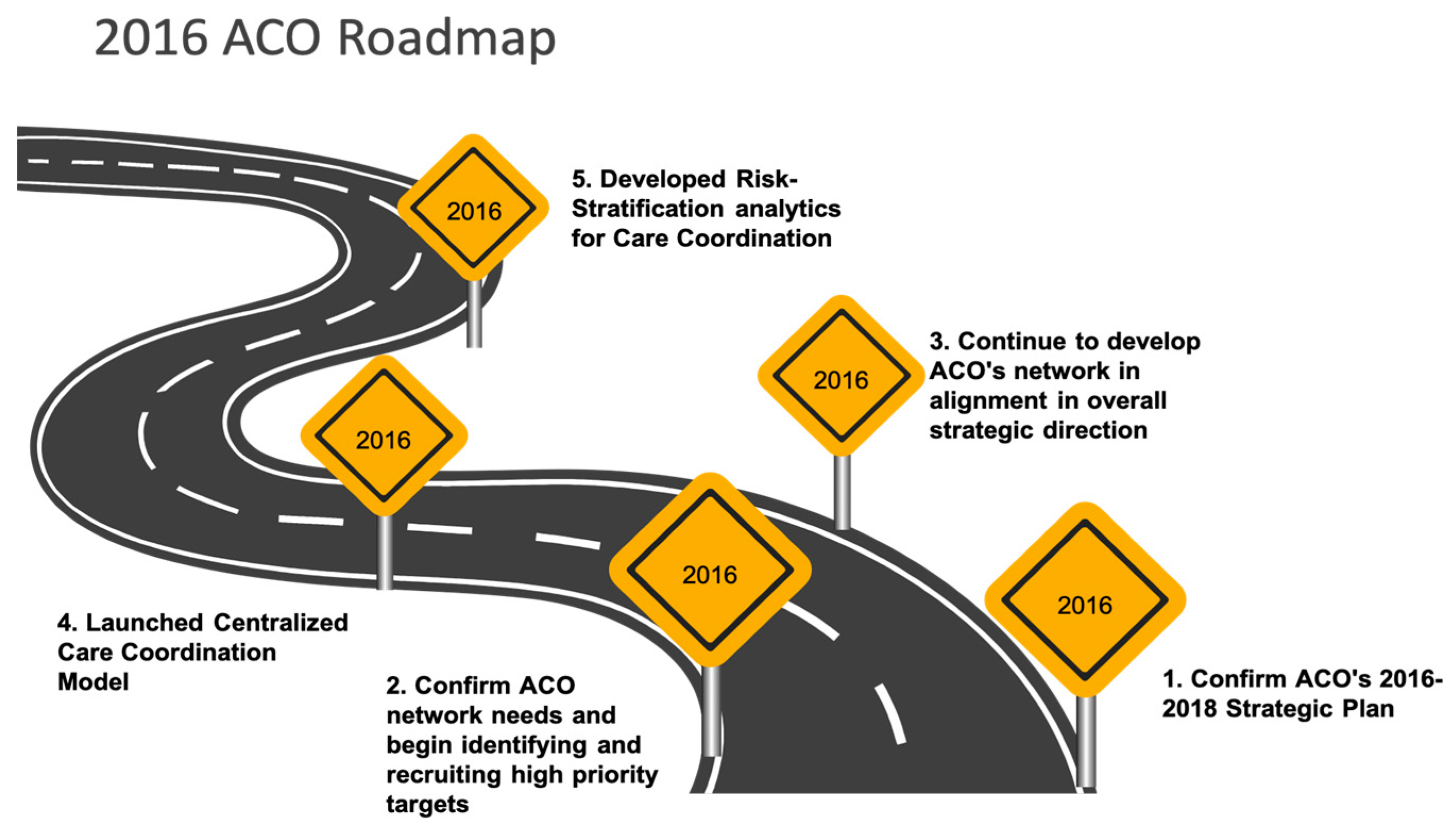
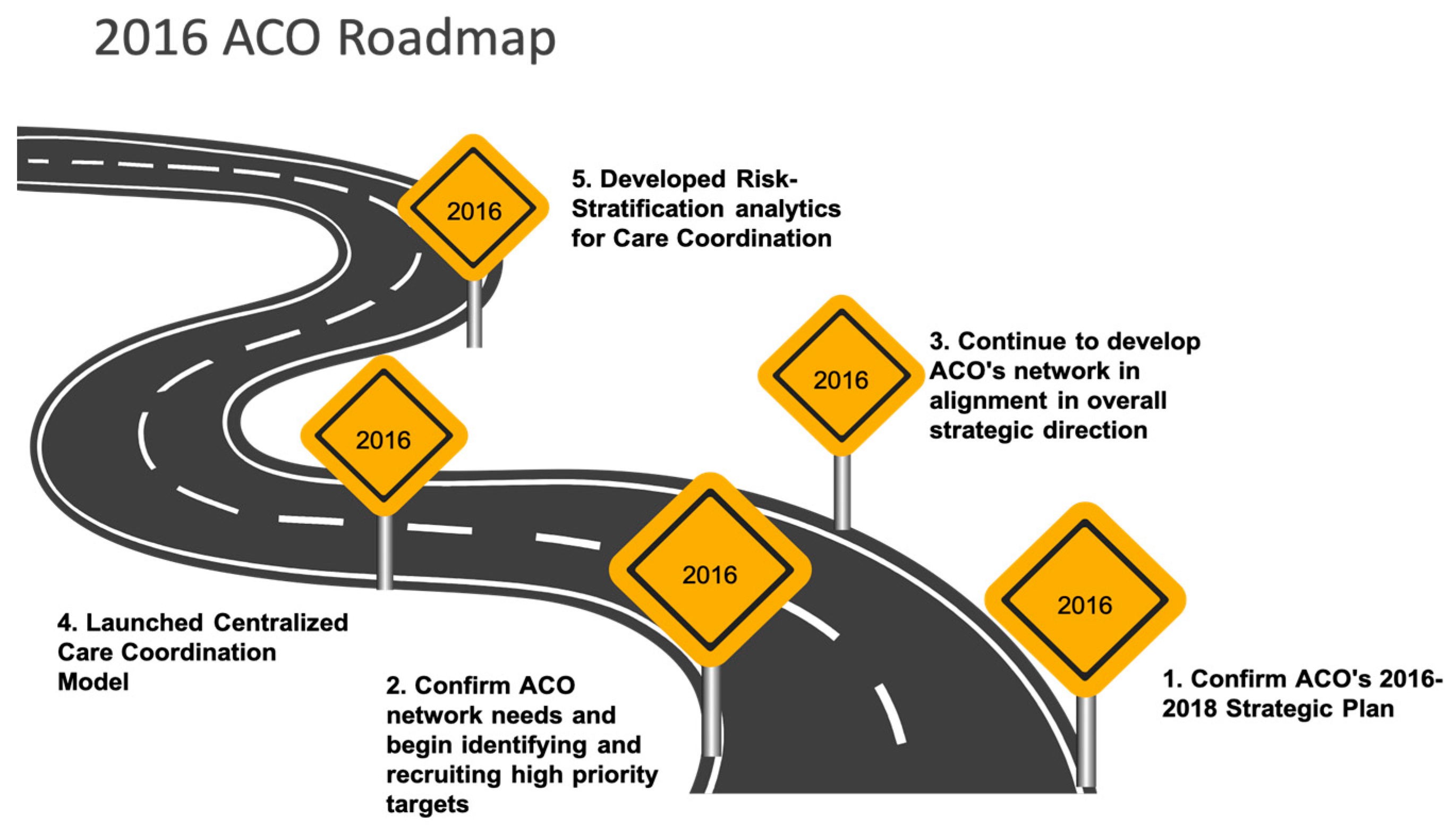
2.6. Implementing M-ACO Strategic Plan
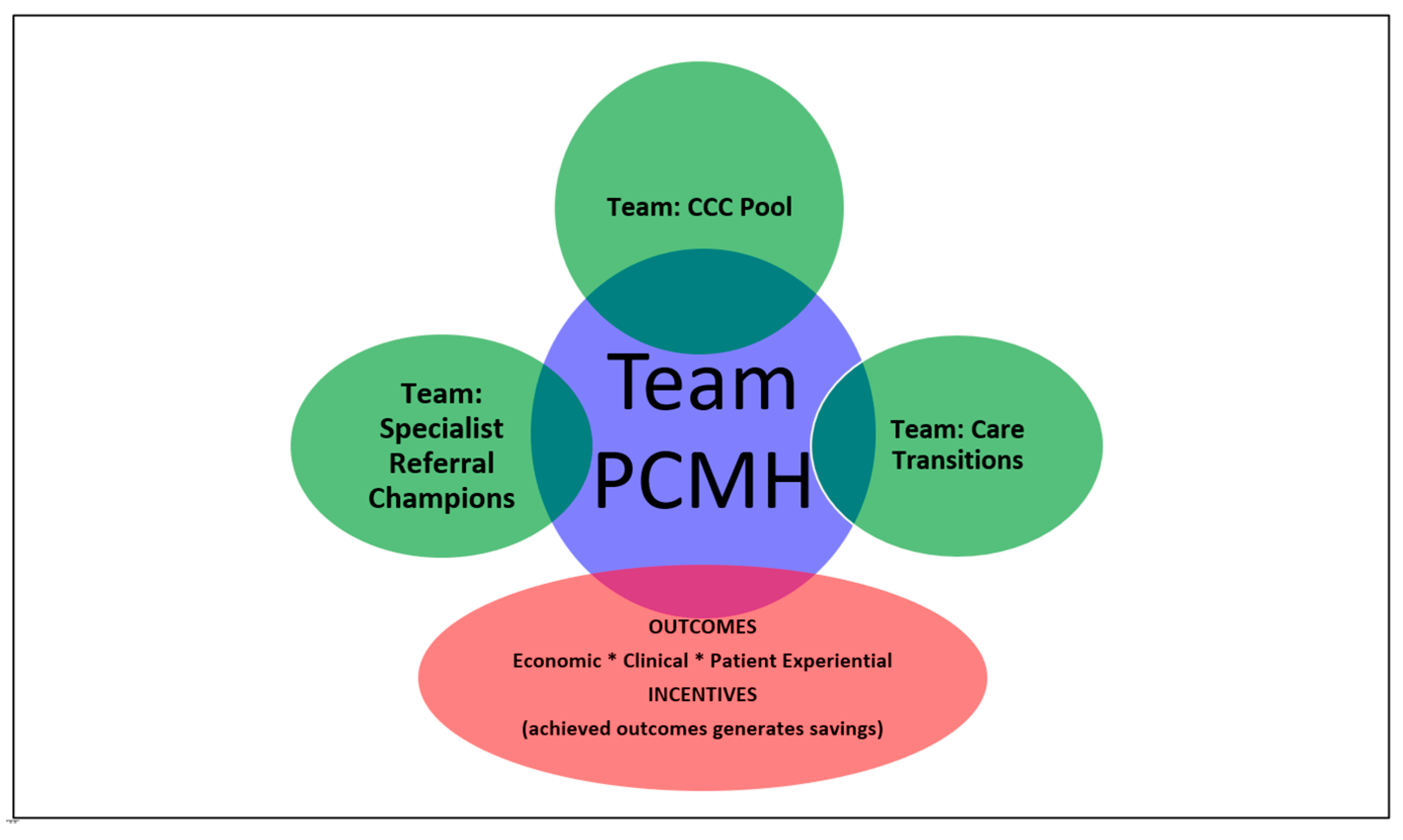
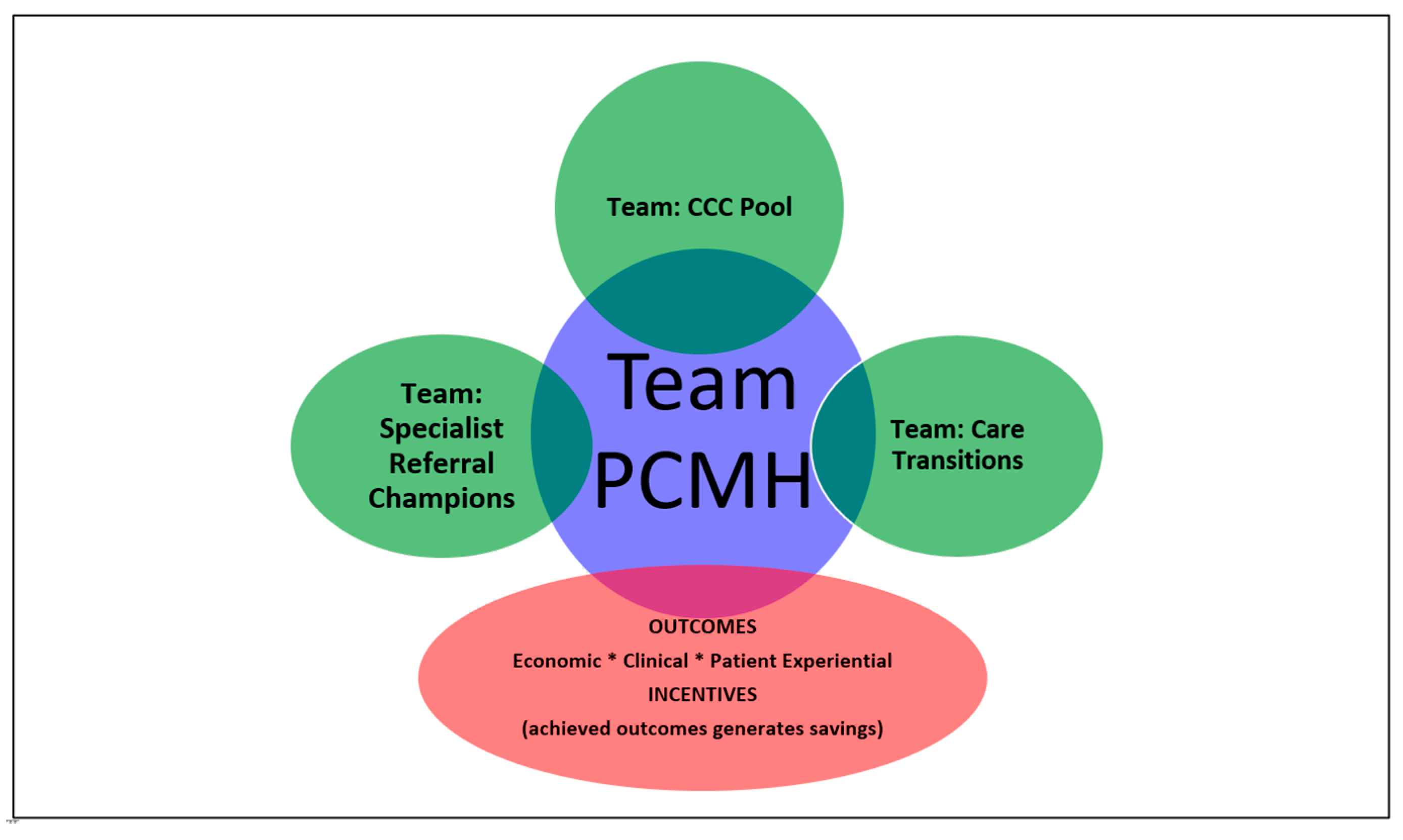
2.7. Centralized (Integrated) Care Coordination
2.8. Web Accessible Communications Platform
2.9. Enterprise Data Warehouse with Interoperability
2.10. Data Analysis
3. Results
3.1. Medicare Beneficiary’s Health Conditions in M-ACO Compared with All Medicare Shared Savings Program (MSSP) ACOs
3.2. MSSP Shared Savings Outcomes for M-ACO
- Proportion invested in infrastructure: 24%,
- Proportion invested in redesigned care processes/resources: 15%,
- Proportion of distribution to ACO participants: 61%.
3.3. M-ACO Compared with All MSSP ACO Quality Measures as Publicly Reported by CMS
3.4. M-ACO Access Primary Care Services and Specialist Physicians Compared with All MSSP ACO as Publicly Reported by CMS
4. Limitations
4.1. HCC Coding Opportunity
4.2. Performance and Impact based on 1) Populations of Interest and 2) Processes and Outcomes of Care
4.3. Future Directions to address Limitations in Data Integration, Performance and Impact
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sisko, A.M.; Keehan, S.P.; Poisal, J.A.; Cuckler, G.A.; Smith, S.D.; Madison, A.J.; Rennie, K.E.; Hardesty, J.C. National Health Expenditure Projections, 2018–2027: Economic and Demographic Trends Drive Spending And Enrollment Growth. Health Aff. 2019, 38, 491–501. [Google Scholar] [CrossRef] [PubMed]
- McGinnis, J.M.; Williams-Russo, P.; Knickman, J.R. The case for more active policy attention to health promotion. Health Aff. (Millwood) 2002, 21, 78–93. [Google Scholar] [CrossRef] [PubMed]
- Adler, N.E.; Stead, W.W. Patients in context—EHR capture of social and behavioral determinants of health. N. Engl. J. Med. 2015, 372, 698–701. [Google Scholar] [CrossRef] [PubMed]
- Moy, E.; Chang, E.; Barrett, M. Potentially preventable hospitalizations—United States, 2001–2009. MMWR Surveill. Summ. 2013, 62 (Suppl. 3), 139–143. [Google Scholar]
- Sandberg, S.F.; Erikson, C.; Owen, R.; Vickery, K.D.; Shimotsu, S.T.; Linzer, M.; Garrett, N.A.; Johnsrud, K.A.; Soderlund, D.M.; DeCubellis, J.; et al. Hennepin Health: A Safety-net Accountable Care Organization for the expanded Medicaid population. Health Aff. (Millwood) 2014, 33, 1975–1984. [Google Scholar] [CrossRef] [PubMed]
- Eggleston, E.M.; Finkelstein, J.A. Finding the role of health care in population health. JAMA 2014, 311, 797–798. [Google Scholar] [CrossRef] [PubMed]
- Alley, D.E.; Asomugha, C.N.; Conway, P.H.; Sanghavi, D.M. Accountable Health Communities—Addressing Social Needs through Medicare and Medicaid. N. Engl. J. Med. 2016, 374, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Center for Medicare and Medicaid Services. Program Data: Shared Savings Program. Available online: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/program-data.html (accessed on 22 August 2018).
- Center for Medicare and Medicaid Services. About the Program. Available online: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/about.html (accessed on 14 August 2018).
- Muhlestein, D.; Saunders, R.; Richards, R.; McClellan, M. Recent Progress in The Value Journey: Growth of ACOs and Value-Based Payment Models in 2018. Health Aff. Blog 2018, 14. [Google Scholar] [CrossRef]
- Stiefel, M.; Nolan, K. A Guide to Measuring the Triple Aim: Population Health, Experience of Care, and Per Capita Cost; IHI Innovation Series white paper; Institute for Healthcare Improvement: Cambridge, MA, USA, 2012; Available online: www.IHI.org (accessed on 20 June 2019).
- People, H. Conclusion and future directions: CDC Health Disparities & Inequalities Report—United States, 2013. CDC Health Disparities Inequal. Rep. U.S. 2013, 62 (Suppl. 3), 1–187. [Google Scholar]
- Health Resources and Services Administration. Available online: https://data.hrsa.gov/ExportedMaps/HPSAs/HGDWMapGallery_BHPR_HPSAs_PC.pdf (accessed on 20 June 2019).
- Higgins, T.C.; Crosson, J.; Peikes, D.; McNellis, R.; Genevro, J.; Meyers, D. Using Health Information Technology to Support Quality Improvement in Primary Care; AHRQ Publication No. 15-0031-EF; Agency for Healthcare Research and Quality: Rockville, MD, USA, March 2015.
- Lipson, D.; Rich, E.; Libersky, J.; Parchman, M. Ensuring That Patient-Centered Medical Homes Effectively Serve Patients with Complex Health Needs; (Prepared by Mathematica Policy Research under Contract No. HHSA290200900019I TO 2.) AHRQ Publication No. 11-0109; Agency for Healthcare Research and Quality: Rockville, MD, USA, October 2011.
- Croghan, T.W.; Brown, J.D. Integrating Mental Health Treatment into the Patient Centered Medical Home; (Prepared by Mathematica Policy Research under Contract No. HHSA290200900019I TO2.) AHRQ Publication No. 10-0084-EF; Agency for Healthcare Research and Quality: Rockville, MD, USA, June 2010.
- Rich, E.; Lipson, D.; Libersky, J.; Parchman, M. Coordinating Care for Adults with Complex Care Needs in the Patient-Centered Medical Home: Challenges and Solutions; White Paper (Prepared by Mathematica Policy Research under Contract No. HHSA290200900019I/HHSA29032005T). AHRQ Publication No. 12-0010-EF; Agency for Healthcare Research and Quality: Rockville, MD, USA, January 2012.
- Ofili, E.O.; Pemu, P.E.; Quarshie, A.; Alema Mensah, E.; Rollins, L.; Ojutalayo, F.; McCaslin, A.; Saint Clair, B. Democratizing discovery health with n = me. Trans. Am. Clin. Climatol. Assoc. 2018, 129, 215–234. [Google Scholar] [PubMed]
- Ofili, E.; Pemu, P.I.; Quarshie, A.; Johnson, P.; Linn, L.J.; Kaur, D.; Ali, J. System and Method for Chronic Illness Care. U.S. Patent 8,234,131 B2, 31 July 2012. [Google Scholar]
- Pemu, P.E.; Quarshie, A.Q.; Josiah-Willock, R.; Ojutalayo, F.O.; Alema-Mensah, E.; Ofili, E.O. Socio-demographic psychosocial and clinical characteristics of participants in e-HealthyStrides©: An interactive ehealth program to improve diabetes self-management skills. J. Health. Care Poor Underserved 2011, 22 (Suppl. 4), 146–164. [Google Scholar] [CrossRef] [PubMed]
- Pemu, P.; Willock, R.J.; Alema-Mensah, E.; Rollins, L.; Brown, M.; Saint Clair, B.; Olorundare, E.; McCaslin, A.; Akintobi, T.H.; Quarshie, A.; et al. Achieving Health Equity with e-Healthystrides©: Patient Perspectives of a Consumer Health Information Technology Application. Ethn. Dis. 2019, 29 (Suppl. 2), 393–404. [Google Scholar] [CrossRef] [PubMed]
- Holden, K.B.; Ofili, E.; Jones, C.P.; Satcher, D. Advancing health equity and reducing disparities with collaborative policy research. Ethn. Dis. 2019, 29 (Suppl. 2), 317–450. [Google Scholar]
- Holden, K.B.; Hopkins, J.; Belton, A.; Butty, K.; Tabor, D.C.; Satcher, D. Leveraging Science to Advance Health Equity: A Regional Health Policy Research Center’s Approach. Ethn. Dis. 2019, 29 (Suppl. 2), 323–328. [Google Scholar] [CrossRef] [PubMed]
- Douglas, M.D.; Robina Willock, R.J.; Respress, E.; Rollins, L.; Tabor, D.; Heiman, H.J.; Hopkins, J.; Dawes, D.E.; Holden, K.B. Applying a Health Equity Lens to Evaluate and inform policy. Ethn. Dis. 2019, 29 (Suppl. 2), 329–342. [Google Scholar] [CrossRef] [PubMed]
- Dawes, D.E. The Future of Health Equity in America: Addressing the Multiple, Intersecting Determinants of Health. Ethn. Dis. 2019, 29 (Suppl. 2), 343–344. [Google Scholar] [CrossRef] [PubMed]
- Fisher, E.S.; Shortell, S.M.; Kreindler, S.A.; Van Citters, A.D.; Larson, B.K. A Framework for Evaluating the Formation, Implementation, and Performance of Accountable Care Organizations. Health Aff. 2012, 31, 2368–2378. [Google Scholar] [CrossRef] [PubMed]
- McWilliams, J.M.; Hatfield, L.A.; Chernew, M.E.; Landon, B.E.; Shwartz, A.L. Early Performance of Accountable Care Organizations in Medicare. N. Engl. J. Med. 2016, 374, 2357–2366. [Google Scholar] [CrossRef] [PubMed]
- Mandl, K.D.; Mandel, J.C.; Murphy, S.N.; Elmer Victor Bernstam, E.V.; Ramoni, R.L.; Kreda, D.A.; McCoy, J.M.; Ben Adida, B.; Kohane, I.S. The SMART Platform: Early experience enabling substitutable applications for electronic health records. J. Am. Med. Inform. Assoc. 2012, 19, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Mandel, J.C.; Kreda, D.A.; Mandl, K.D.; Kohane, I.S.; Ramoni, R.B. SMART on FHIR: A standards-based, interoperable apps platform for electronic health records. J. Am. Med. Inform. Assoc. 2016, 23, 899–908. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Organization | Practice Type and Locations |
|---|---|
| Morehouse School of Medicine and Morehouse Healthcare | Primary care and select multispecialty: Two Urban locations |
| Southside Medical Center | FQHC: Eleven Urban and Rural locations including school-based health centers, Adult and Pediatric Primary care, specialty care, dental optometry, behavioral health and mobile medical and dental unit. |
| Family Health Centers of Georgia | FQHC: Seven Urban locations including school-based health centers, Adult and Pediatric Primary care, specialty care, dental optometry, behavioral health and mobile medical and dental unit. |
| Four Corners Primary Care | FQHC: Three Urban locations |
| CareConnect Health | FQHC: Forty-one Rural locations, including school-based clinics, Dental, OB/GYB, Urgent Care Centers. |
| Medical Associates Plus | FQHC: Eight Suburban and Rural locations including Adult and Pediatric Primary care, specialty care, dental optometry, behavioral health and pulmonary health |
| Community Health Care Systems | FQHC: Thirteen Rural locations including Adult and Pediatric Primary care, podiatry, behavioral health and mobile medical unit |
| East Georgia Healthcare Center | FQHC: Ten Rural locations including Adult and Pediatric Primary care, specialty care, dental and behavioral health |
| MedLink Georgia | FQHC: Eighteen Rural locations including Adult and Pediatric Primary care, specialty care, dental optometry, behavioral health |
| Albany Area Primary Health Care | FQHC: Twenty-six Rural locations including school-based health centers, Adult and Pediatric Primary care, specialty care, dental optometry, behavioral health and mobile medical and dental unit. |
| North Georgia Healthcare Center | Independent Rural practice including Adult and Pediatric Primary care, specialty care, dental optometry, behavioral health and physical therapy |
| Atlanta Family Physicians | Independent Urban practice |
| The Clinic For All | Independent Urban Practice |
| Medicare Beneficiary | MCACO-ES * | All MSSP ACOs |
|---|---|---|
| ESRD | 2.96% | 0.69% |
| ESRD Dual Eligible | 1.34% | 0.24% |
| ESRD Non-Dual Eligible | 1.62% | 0.45% |
| Disabled | 33.36% | 11.72% |
| Disabled Dual Eligible | 17.61% | 5.56% |
| Disabled Non-Dual Eligible | 15.75% | 6.14% |
| Aged | 63.68% | 87.41% |
| Aged Dual Eligible | 15.99% | 6.19% |
| Aged Non-Dual Eligible | 47.69% | 80.86% |
| CMS-HCC Condition | MCACO-ES | All MSSP ACOs |
|---|---|---|
| Diabetes w/Chronic complications | 2134 | 1670 |
| Chronic Obstructive Pulmonary Disease | 1481 | 1318 |
| Congestive Heart Failure | 1202 | 1196 |
| Morbid Obesity | 1180 | 544 |
| Diabetes without Complication | 1162 | 1172 |
| Vascular Disease | 1120 | 1402 |
| Major Depressive, Bipolar & Paranoid Disorder | 930 | 737 |
| Specified Heart Arrhythmias | 898 | 1525 |
| Rheumatoid Arthritis and Inflammatory Connective Tissue Disease | 644 | 716 |
| Seizure Disorders and Convulsions | 500 | 295 |
| Select ACO Quality Measures | M-ACO (%) | All MSSP ACOs (%) |
|---|---|---|
| Getting Timely Care, Appointments, and Information | 72.20 | 80.60 |
| How Well Your Providers Communicate | 90.71 | 93.13 |
| Access to Specialists | 78.43 | 83.32 |
| Shared Decision Making | 70.36 | 75.85 |
| Influenza immunization | 62.37 | 72.52 |
| Diabetes A1c poor control | 23.94 | 16.74 |
| Hypertension control (High BP control) | 60.18 | 71.47 |
| Primary Care Services | M-ACO | All MSSP ACOs | National Assignable FFS |
|---|---|---|---|
| With a Primary Care Physician | 8760 | 9711 | 10,120 |
| With a Specialist Physician | 1004 | 3811 | 3713 |
| With a Nurse Practitioner/Physician Assistant/Clinical Nurse | 3383 | 4348 | 4491 |
| With a FQHC/RHC | 762 | 1110 | 1427 |
| Medicare Category | M-ACO HCC Risk Score | CMS-HCC Risk Score (National Mean) | M-ACO Demographic Risk Score | CMS Demographic Risk Score (National Mean) |
|---|---|---|---|---|
| ESRD | 0.893 | 1.115 | 1.005 | 1.021 |
| Disabled | 0.865 | 1.282 | 0.987 | 1.057 |
| Aged/Dual | 0.750 | 1.805 | 0.946 | 1.562 |
| Aged/Non-Dual | 0.904 | 1.055 | 1.002 | 0.911 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, M.; Ofili, E.O.; Okirie, D.; Pemu, P.; Franklin, C.; Suk, Y.; Quarshie, A.; Mubasher, M.; Sow, C.; Montgomery Rice, V.; et al. Morehouse Choice Accountable Care Organization and Education System (MCACO-ES): Integrated Model Delivering Equitable Quality Care. Int. J. Environ. Res. Public Health 2019, 16, 3084. https://doi.org/10.3390/ijerph16173084
Brown M, Ofili EO, Okirie D, Pemu P, Franklin C, Suk Y, Quarshie A, Mubasher M, Sow C, Montgomery Rice V, et al. Morehouse Choice Accountable Care Organization and Education System (MCACO-ES): Integrated Model Delivering Equitable Quality Care. International Journal of Environmental Research and Public Health. 2019; 16(17):3084. https://doi.org/10.3390/ijerph16173084
Chicago/Turabian StyleBrown, Michelle, Elizabeth O. Ofili, Debbie Okirie, Priscilla Pemu, Cheryl Franklin, Yoon Suk, Alexander Quarshie, Mohamed Mubasher, Charles Sow, Valerie Montgomery Rice, and et al. 2019. "Morehouse Choice Accountable Care Organization and Education System (MCACO-ES): Integrated Model Delivering Equitable Quality Care" International Journal of Environmental Research and Public Health 16, no. 17: 3084. https://doi.org/10.3390/ijerph16173084
APA StyleBrown, M., Ofili, E. O., Okirie, D., Pemu, P., Franklin, C., Suk, Y., Quarshie, A., Mubasher, M., Sow, C., Montgomery Rice, V., Williams, D., Brooks, M., Alema-Mensah, E., Mack, D., & Dawes, D. (2019). Morehouse Choice Accountable Care Organization and Education System (MCACO-ES): Integrated Model Delivering Equitable Quality Care. International Journal of Environmental Research and Public Health, 16(17), 3084. https://doi.org/10.3390/ijerph16173084