Health Literacy Studies Conducted in Australia: A Scoping Review


 , ,
, ,
Abstract
1. Introduction
Significance of the Study
2. Materials and Methods
2.1. Identification of the Scoping Review Question (Inclusion Criteria) (Stage 1)
2.2. Identification of Relevant Studies (Stage 2)
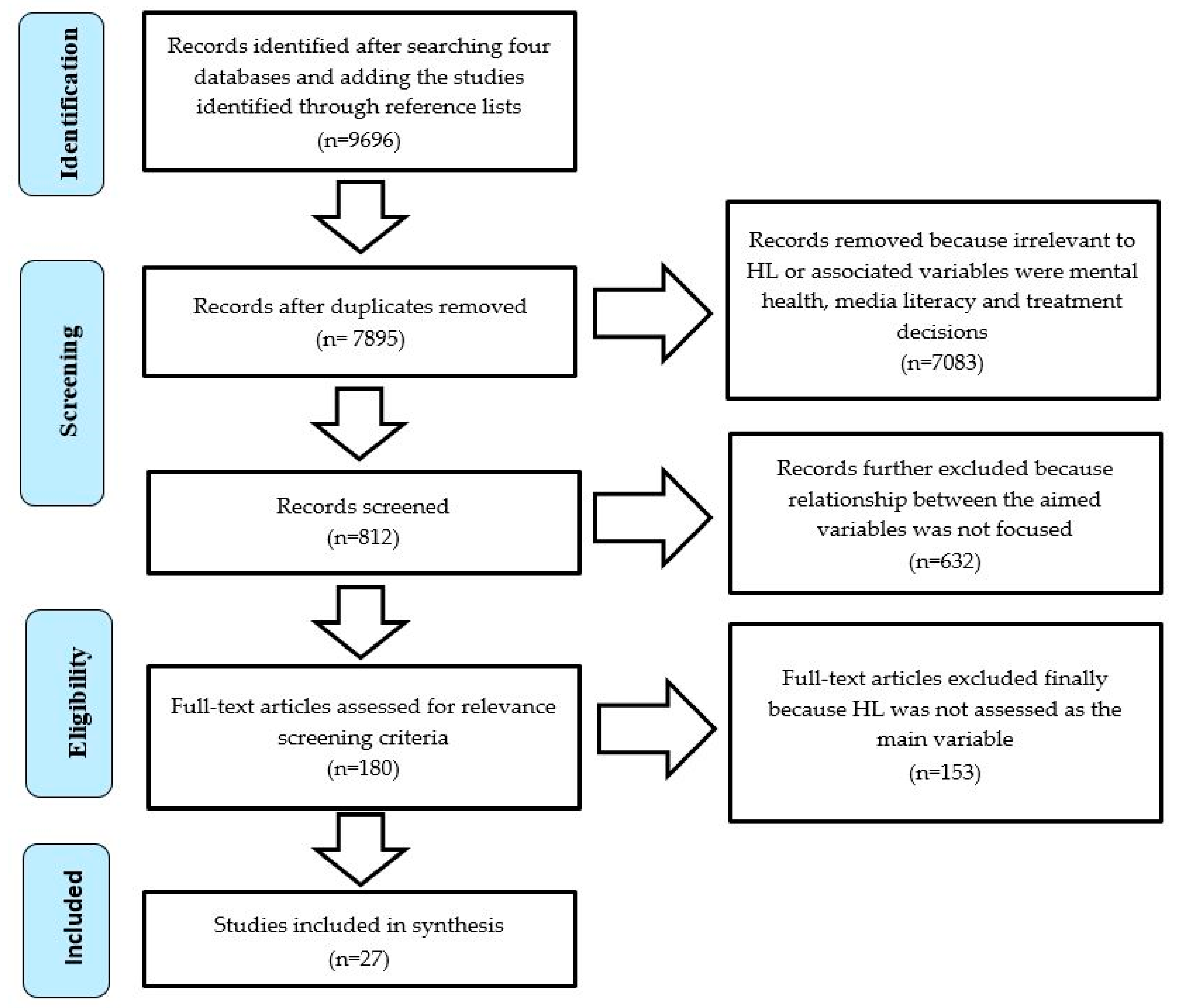
2.3. Study Selection (Stage 3)
2.4. Charting the Data (Stage 4)
2.5. Collating, Summarizing, and Reporting the Results (Stage 5)
3. Results
3.1. Research Designs and Study Populations
3.2. Theme 1—Health Literacy and Health Numeracy
3.3. Theme 2—Health Literacy as Knowledge Gain, Knowledge Deficiency and Knowledge of Current Health System
3.4. Theme 3—Health Literacy Measurement Methods and Its Domains
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- De Wit, L.; Fenenga, C.; Giammarchi, C.; di Furia, L.; Hutter, I.; de Winter, A.; Meijering, L. Community-based initiatives improving critical health literacy: A systematic review and meta-synthesis of qualitative evidence. BMC Public Health 2017, 18, 40. [Google Scholar] [CrossRef] [PubMed]
- Kickbusch, I.; Pelikan, J.M.; Apfel, F.; Tsouros, A.D. Health Literacy. The Solid Facts; World Health Organization, The Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Keleher, H.; Hagger, V. Health literacy in primary health care. Aust. J. Prim. Health 2007, 13, 24–30. [Google Scholar] [CrossRef]
- Simonds, S.K. Health education as social policy. Health Educ. Behav. 1974, 2, 1–10. [Google Scholar] [CrossRef]
- Medicine, I.O. Health Literacy: A Prescription to End Confusion; National Academies Press: Washington, DC, USA, 2004. [Google Scholar] [CrossRef]
- Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs, American Medical Association. Health literacy: Report of the council on scientific affairs. JAMA 1999, 281, 552–557. [Google Scholar] [CrossRef]
- Nutbeam, D. Health promotion glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Peerson, A.; Saunders, M. Health literacy revisited: What do we mean and why does it matter? Health Promot. Int. 2009, 24, 285–296. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef]
- Poureslami, I.; Nimmon, L.; Rootman, I.; Fitzgerald, M.J. Health literacy and chronic disease management: Drawing from expert knowledge to set an agenda. Health Promot. Int. 2017, 32, 743–754. [Google Scholar] [CrossRef]
- Baker, D.W. The meaning and the measure of health literacy. J. Gen. Intern. Med. 2006, 21, 878–883. [Google Scholar] [CrossRef]
- Paasche-Orlow, M.K.; McCaffery, K.; Wolf, M.S. Bridging the International Divide for Health Literacy Research. Patient Educ. Couns. 2009, 75, 293–294. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.J.; Stocks, N.P.; Wilson, D.H.; Hill, C.L.; Gravier, S.; Kickbusch, I.; Beilby, J.J. Health literacy—A new concept for general practice? Aust. Fam. Phys. 2009, 38, 144–147. [Google Scholar]
- Lee, T.W.; Kang, S.J.; Lee, H.J.; Hyun, S.I. Testing health literacy skills in older Korean adults. Patient Educ. Couns. 2009, 75, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Nomura, K.; Sato, M.; Yano, E. Developing a measure of communicative and critical health literacy: A pilot study of Japanese office workers. Health Promot. Int. 2008, 23, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.Y.; Reid, F.; Shaw, A.; Rowlands, G.; Gomez, G.B.; Chesnokov, M.; Ussher, M. Validation of a health literacy screening tool (REALM) in a UK Population with coronary heart disease. J. Public Health 2008, 30, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Twickler, T.B.; Hoogstraaten, E.; Reuwer, A.Q.; Singels, L.; Stronks, K.; Essink-Bot, M.-L. Laaggeltetterdheid en beperkte gezondheidsvaardigheden vragen om een antwoord in de zorg. Ned. Tijdschr. Gennesskunde 2009, 153, A250. [Google Scholar]
- Wang, J.; Schmid, M. Regional Differences in Health Literacy in Switzerland; Institute of Social and Preventive Medicine, University of Zürich: Zürich, Switzerland, 2007. [Google Scholar]
- Kilfoyle, K.A.; Vitko, M.; O’Conor, R.; Bailey, S.C. Health Literacy and Women’s Reproductive Health: A Systematic Review. J. Women’s Health 2016, 25, 1237–1255. [Google Scholar] [CrossRef] [PubMed]
- Kutcher, S.; Wei, Y.; Coniglio, C. Mental Health Literacy: Past, Present, and Future. Can. J. Psychiatry 2016, 61, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Coleman, C.; Kurtz-Rossi, S.; McKinney, J.; Pleasant, A.; Rootman, I.; Shohet, L. The Calgary Charter on Health Literacy: Rational and Core Principles for the Development of Health Literacy Curricula. Available online: http://www.centreforliteracy.qc.ca/sites/default/files/CFL_Calgary_Charter_2011.pdf (accessed on 19 March 2018).
- ACSQHC. Health Literacy National Statement: Taking Action to Improve Safety and Quality; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2014.
- Department of Health and Ageing. Building a 21st Century Primary Health Care System: Australia’s First National Primary Health Care Strategy; Commonwealth of Australia: Canberra, Australia, 2010. [Google Scholar]
- Nutbeam, D.; Wise, M. Australia: Planning for better health. Opportunities for health promotion through the development of national health goals and targets. Promot. Educ. 1993, 1, 19–24. [Google Scholar] [CrossRef]
- WHO. Health Literacy: The Solid Facts; World Health Organization: Copenhagen, Denmark, 2013. [Google Scholar]
- Nutbeam, D.; Wise, M.; Bauman, A.; Harris, E.; Leeder, S. Goals and Targets for Australia’s Health in the Year 2000 and Beyond; Commonwealth of Australia: Canberra, Australia, 1993. [Google Scholar]
- ACSQHC. Health Literacy Stocktake: Consultation Report; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2012.
- Australian Bureau of Statistics. Health Literacy Australia 2006; Australian Bureau of Statistics: Canberra, Australia, 2008.
- Commonwealth of Australia. National Health Reform: Progress and Delivery; Commonwealth of Australia: Canberra, Australia, 2011. [Google Scholar]
- Council of Australian Governments. National Health Reform—Heads of Agreement; Council of Australian Governments: Canberra, Australia, 2011.
- ACSQHC. National Safety and Quality Health Service Standards; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2011.
- Department of Health and Ageing. Fourth National Mental Health Plan: An Agenda for Collaborative Government Action in Mental Health 2009–2014; Commonwealth of Australia: Canberra, Australia, 2009. [Google Scholar]
- Department of Health and Ageing. Living Longer. Living Better; Commonwealth of Australia: Canberra, Australia, 2012. [Google Scholar]
- ABS. Programme for the International Assessment of Adult Competencies, Australia 2011–2012; Australian Bureau of Statistics (ABS): Canberra, Australia, 2013.
- ACSQHC. Consumers, the Health System and Health Literacy: Taking Action to Improve Safety and Quality; Consultation Paper; Australian Commission on Safety and Quality in Health Care (ACSQHC): Sydney, Australia, 2013.
- Kutner, M.; Greenberg, E.; Baer, J. A First Look at the Literacy of America’s Adults in the 21st Century; NCES 2006-470; National Center for Education Statistics: Washington, DC, USA, 2006.
- Murray, T.; Hagey, J.; Willms, D.; Shillington, R.; Desjardins, R. Health Literacy in Canada: A Healthy Understanding; Canadian Council on Learning: Ottawa, ON, Canada, 2008. [Google Scholar]
- US Department of Health and Human Services. America’s Health Literacy: Why We Need Accessible Health Information. 2008; An Issue Brief from the US Department of Health and Human Services Google Scholar; US Department of Health and Human Services: Washington, DC, USA, 2016.
- Barber, M.N.; Staples, M.; Osborne, R.H.; Clerehan, R.; Elder, C.; Buchbinder, R. Up to a quarter of the Australian population may have suboptimal health literacy depending upon the measurement tool: Results from a population-based survey. Health Promot. Int. 2009, 24, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Love, T.; Ehrenberg, N. Addressing Unwarranted Variation: Literature Review on Methods for Influencing Practice; Health Quality & Safety Commission New Zealand: Wellington, New Zealand, 2014; p. 3.
- Villaire, M.; Mayer, G. Low health literacy: The impact on chronic illness management. Prof. Case Manag. 2007, 12, 213–216; quiz 217–218. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.J.; Ownby, R.L.; Acevedo, A.; Waldrop-Valverde, D. A qualitative study examining health literacy and chronic illness self-management in Hispanic and non-Hispanic older adults. J. Multidiscip. Healthc. 2017, 10, 167–177. [Google Scholar] [CrossRef]
- Rootman, I.; Ronson, B. Literacy and health research in Canada: Where have we been and where should we go? Can. J. Public Health 2005, 96 (Suppl. S2), S62–S77. [Google Scholar]
- Bush, R.; Boyle, F.; Ostini, R.; Ozolins, I.; Brabant, M.; Jimenez Soto, E.; Eriksson, L. Advancing Health Literacy through Primary Health Care Systems; Australian Primary Health Care Research Institute: Canberra, Australia, 2010. [Google Scholar]
- DeWalt, D.A.; Berkman, N.D.; Sheridan, S.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- ACSQHC. Patient-Centred Care: Improving Safety and Quality Through Partnerships with Patients and Consumers; Australian Commission on Safety and Quality in Health Care (ACSQHC): Sydney, Australia, 2011.
- ECCV. An Investment Not an Expense: Enhancing Health Literacy in Culturally and Linguistically Diverse Communities; Ethnic Communities’ Council of Victoria (ECCV): Melbourne, Australia, 2012. [Google Scholar]
- Sawkin, M.T.; Deppe, S.J.; Thelen, J.; Stoner, S.C.; Dietz, C.A.; Rasu, R.S. Health Literacy and Medication Adherence Among Patients Treated in a Free Health Clinic: A Pilot Study. Health Serv. Res. Manag. Epidemiol. 2015, 2. [Google Scholar] [CrossRef]
- Freedman, A.M.; Miner, K.R.; Echt, K.V.; Parker, R.; Cooper, H.L. Amplifying diffusion of health information in low-literate populations through adult education health literacy classes. J. Health Commun. 2011, 16 (Suppl. S3), 119–133. [Google Scholar] [CrossRef]
- Freedman, R.B.; Jones, S.K.; Lin, A.; Robin, A.L.; Muir, K.W. Influence of parental health literacy and dosing responsibility on pediatric glaucoma medication adherence. Arch. Ophthalmol. 2012, 130, 306–311. [Google Scholar] [CrossRef]
- Murphy, D.A.; Lam, P.; Naar-King, S.; Robert Harris, D.; Parsons, J.T.; Muenz, L.R. Health literacy and antiretroviral adherence among HIV-infected adolescents. Patient Educ. Couns. 2010, 79, 25–29. [Google Scholar] [CrossRef][Green Version]
- Zhang, N.J.; Terry, A.; McHorney, C.A. Impact of health literacy on medication adherence: A systematic review and meta-analysis. Ann. Pharmacother. 2014, 48, 741–751. [Google Scholar] [CrossRef]
- Koh, H.K.; Berwick, D.M.; Clancy, C.M.; Baur, C.; Brach, C.; Harris, L.M.; Zerhusen, E.G. New federal policy initiatives to boost health literacy can help the nation move beyond the cycle of costly ‘crisis care’. Health Aff. 2012, 31, 434–443. [Google Scholar] [CrossRef]
- Koh, H.K.; Baur, C.; Brach, C.; Harris, L.M.; Rowden, J.N. Toward a systems approach to health literacy research. J. Health Commun. 2013, 18, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, S.C.; Ramachandran, B.; Catz, S. Adherence to Combination Antiretroviral Therapies in HIV Patients of Low Health Literacy. J. Gen. Intern. Med. 1999, 14, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.D.; Wu, J.; Tu, W.; Clark, D.; Weiner, M.; Morrow, D.G.; Brater, D.C. Health literacy predicts medication adherence. Clin. Pharm. 2004, 75, P76. [Google Scholar] [CrossRef]
- AHRQ. Agency for Healthcare Research and Quality. Pharmacy Health Literacy Center. Available online: http://www.ahrq.gov/pharmhealthlit/ (accessed on 19 March 2018).
- Davis, T.C.; Wolf, M.S.; Bass, P.F.; Middlebrooks, M.; Kennen, E.; Baker, D.W.; Bennett, C.L.; Durazo-Arvizu, R.; Bocchini, A.; Savory, S.; et al. Low literacy impairs comprehension of prescription drug warning labels. J. Gen. Intern. Med. 2006, 21, 847–851. [Google Scholar] [CrossRef]
- Davis, T.C.; Wolf, M.S.; Bass, P.F., 3rd; Thompson, J.A.; Tilson, H.H.; Neuberger, M.; Parker, R.M. Literacy and misunderstanding prescription drug labels. Ann. Intern. Med. 2006, 145, 887–894. [Google Scholar] [CrossRef]
- Rudd, R.E. Improving Americans’ health literacy. N. Engl. J. Med. 2010, 363, 2283–2285. [Google Scholar] [CrossRef] [PubMed]
- Agbor Bawa, W.; Rasu, R. PHP4 Health literacy and its impact on national health care utilization. Value Health 2012, 15, A13. [Google Scholar] [CrossRef][Green Version]
- Plsek, P.E.; Greenhalgh, T. The challenge of complexity in health care. BMJ 2001, 323, 625. [Google Scholar] [CrossRef] [PubMed]
- Diug, B.; Evans, S.; Lowthian, J.; Maxwell, E.; Dooley, M.; Street, A.; Wolfe, R.; Cameron, P.; McNeil, J. The unrecognized psychosocial factors contributing to bleeding risk in warfarin therapy. Stroke 2011, 42, 2866–2871. [Google Scholar] [CrossRef]
- Eichler, K.; Wieser, S.; Brügger, U. The costs of limited health literacy: A systematic review. Int. J. Public Health 2009, 54, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.; Drey, N.; Gould, D. What are scoping studies? A review of the nursing literature. Int. J. Nurs. Stud. 2009, 46, 1386–1400. [Google Scholar] [CrossRef] [PubMed]
- Gough, D.; Thomas, J.; Oliver, S. Clarifying differences between review designs and methods. Syst. Rev. 2012, 1, 28. [Google Scholar] [CrossRef]
- Weeks, L.C.; Strudsholm, T. A scoping review of research on complementary and alternative medicine (CAM) and the mass media: Looking back, moving forward. BMC Complement. Altern. Med. 2008, 8, 43. [Google Scholar] [CrossRef]
- Rumrill, P.D.; Fitzgerald, S.M.; Merchant, W.R. Using scoping literature reviews as a means of understanding and interpreting existing literature. Work 2010, 35, 399–404. [Google Scholar]
- Brien, S.E.; Lorenzetti, D.L.; Lewis, S.; Kennedy, J.; Ghali, W.A. Overview of a formal scoping review on health system report cards. Implement. Sci. 2010, 5, 2. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Malloy-Weir, L.J.; Charles, C.; Gafni, A.; Entwistle, V.A. Empirical relationships between health literacy and treatment decision making: A scoping review of the literature. Patient Educ. Couns. 2015, 98, 296–309. [Google Scholar] [CrossRef]
- Porteous, H.E.; Palmer, M.A.; Wilkinson, S.A. Informing maternity service development by surveying new mothers about preferences for nutrition education during their pregnancy in an area of social disadvantage. Women Birth 2014, 27, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.J.; Appleton, S.L.; Hill, C.L.; Ruffin, R.E.; Wilson, D.H. Inadequate health literacy is associated with increased asthma morbidity in a population sample. J. Allergy Clin. Immunol. 2009, 124, 601–603. [Google Scholar] [CrossRef] [PubMed]
- Maguire, P.A.; Reay, R.E.; Looi, J.C.; Cubis, J.; Byrne, G.J.; Raphael, B. Neither the internist nor the Internet: Use of and trust in health information sources by people with schizophrenia. Aust. N. Z. J. Psychiatry 2011, 45, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Oh, E.; Jorm, A.F.; Wright, A. Perceived helpfulness of websites for mental health information. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Eckert, K.A.; Kutek, S.M.; Dunn, K.I.; Air, T.M.; Goldney, R.D. Changes in depression-related mental health literacy in young men from rural and urban South Australia. Aust. J. Rural. Health 2010, 18, 153–158. [Google Scholar] [CrossRef]
- Crawford, G.; Burns, S.K.; Chih, H.J.; Hunt, K.; Tilley, P.M.; Hallett, J.; Coleman, K.; Smith, S. Mental health first aid training for nursing students: A protocol for a pragmatic randomised controlled trial in a large university. BMC Psychiatry 2015, 15, 26. [Google Scholar] [CrossRef] [PubMed]
- Jorm, A.F. Mental health literacy. Public knowledge and beliefs about mental disorders. Br. J. Psychiatry. 2000, 177, 396–401. [Google Scholar]
- Smith, S.; Petrak, L.M.; Dhillon, H.; Taylor, J.; Milross, C. Are radiation oncologists aware of health literacy among people with cancer treated with radiotherapy? Eur. J. Cancer Care 2014, 23, 111–120. [Google Scholar] [CrossRef]
- Nutbeam, D.; Kickbusch, I. Advancing health literacy: A global challenge for the 21st century. Health Promot. Int. 2000, 15, 183–184. [Google Scholar] [CrossRef]
- Rees, C.S.; Austen, T.; Anderson, R.A.; Egan, S.J. Can corrective information reduce negative appraisals of intrusive thoughts in a community sample? Behav. Cogn. Psychother. 2014, 42, 502–507. [Google Scholar] [CrossRef]
- Isaacs, A.N.; Maybery, D.; Gruis, H. Help seeking by Aboriginal men who are mentally unwell: A pilot study. Early Interv. Psychiatry 2013, 7, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, L.; Parker, E.; Richards, L. Using qualitative methodology to inform an Indigenous-owned oral health promotion initiative in Australia. Health Promot. Int. 2008, 23, 52–59. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hosking, S.M.; Buchbinder, R.; Pasco, J.A.; Williams, L.J.; Brennan-Olsen, S.L. The Role of Health Literacy in the Treatment of Osteoporosis. J. Bone Miner. Res. 2016, 31, 1909. [Google Scholar] [CrossRef] [PubMed]
- White, B.; Madden, A.; Hellard, M.; Kerr, T.; Prins, M.; Page, K.; Dore, G.J.; Maher, L. Increased hepatitis C virus vaccine clinical trial literacy following a brief intervention among people who inject drugs. Drug Alcohol Rev. 2013, 32, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.M.; Jordan, J.E.; O’Sullivan, P.B.; Buchbinder, R.; Burnett, A.F.; Osborne, R.H.; Straker, L.M. Individuals with chronic low back pain have greater difficulty in engaging in positive lifestyle behaviours than those without back pain: An assessment of health literacy. BMC Musculoskelet. Disord. 2011, 12, 161. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.K.; Trevena, L.; Simpson, J.M.; Barratt, A.; Nutbeam, D.; McCaffery, K.J. A decision aid to support informed choices about bowel cancer screening among adults with low education: Randomised controlled trial. BMJ 2010, 341, c5370. [Google Scholar] [CrossRef] [PubMed]
- Saunders, M.H.; Peerson, A. Risks associated with low functional health literacy in an Australian population. Comment. Med. J. Aust. 2010, 192, 478–479. [Google Scholar] [PubMed]
- Jennings, W.; Spurling, G.K.; Askew, D.A. Yarning about health checks: Barriers and enablers in an urban Aboriginal medical service. Aust. J. Prim. Health 2014, 20, 151–157. [Google Scholar] [CrossRef]
- Gratwick-Sarll, K.; Bentley, C. Improving eating disorders mental health literacy: A preliminary evaluation of the “Should I Say Something?” workshop. Eat. Disord. 2014, 22, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Caposecco, A.; Hickson, L.; Meyer, C.; Khan, A. Evaluation of a modified user guide for hearing aid management. Ear Hear 2016, 37, 27–37. [Google Scholar] [CrossRef]
- Cashin, A.; Heartfield, M.; Cox, D.; Dunn, S.; Stasa, H. Knowledge and motivation: Two elements of health literacy that remain low with regard to nurse practitioners in Australia. Aust. Health Rev. 2015, 39, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Bukulatjpi, S.; Sharma, S.; Davis, J.; Johnston, V. “Only your blood can tell the story”—A qualitative research study using semi-structured interviews to explore the hepatitis B related knowledge, perceptions and experiences of remote dwelling Indigenous Australians and their health care providers in northern Australia. BMC Public Health 2014, 14, 1233. [Google Scholar] [CrossRef]
- Yuen, E.Y.N.; Dodson, S.; Batterham, R.W.; Knight, T.; Chirgwin, J.; Livingston, P.M. Development of a conceptual model of cancer caregiver health literacy. Eur. J. Cancer Care 2016, 25, 294–306. [Google Scholar] [CrossRef]
- Nasuuna, E.; Santoro, G.; Kremer, P.; de Silva, A.M. Examining the relationship between childhood health conditions and health service utilisation at school entry and subsequent academic performance in a large cohort of Australian children. J. Paediatr. Child Health 2016, 52, 750–758. [Google Scholar] [CrossRef]
- Whittaker, M.; Hodge, N.; Mares, R.E.; Rodney, A. Preparing for the data revolution: Identifying minimum health information competencies among the health workforce. Hum. Resour. Health 2015, 13, 1. [Google Scholar] [CrossRef] [PubMed][Green Version]
- May, S.; Rapee, R.M.; Coello, M.; Momartin, S.; Aroche, J. Mental health literacy among refugee communities: Differences between the Australian lay public and the Iraqi and Sudanese refugee communities. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 757–769. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S.; Clifford, C.; Ross, K.; Sefton, N.; Owen, L.; Blizzard, L.; Turner, R. Sexual health literacy of the student population of the University of Tasmania: Results of the RUSSL Study. Sex Health 2015, 12, 207–216. [Google Scholar] [CrossRef]
- Yiu, A.W.; Bajorek, B.V. Health literacy and knowledge in a cohort of Australian patients taking warfarin. Pharm. Pract. 2018, 16, 1080. [Google Scholar] [CrossRef]
- Stanton, R.; Rebar, A.; Rosenbaum, S. Exercise and mental health literacy in an Australian adult population. Depress. Anxiety 2018. [Google Scholar] [CrossRef]
- Presses de l’Université du Québec. Méthodologie de l’analyse développementale de contenu: Méthode GPS et concept de soi [Methodology of Developmental Content Analysis: GPS Method and Self-Concept]; Presses de l’Université du Québec: Québec, QC, Canada, 1990. [Google Scholar]
- Akoijam, B.S.; Jamir, M.N.; Phesao, E.; Senjam, G.S. Inhalant Use among Schoolchildren in Northeast India: A Preliminary Study. Subst. Abus. 2013, 7, 185–190. [Google Scholar] [CrossRef]
- Mårtensson, L.; Hensing, G. Health literacy—A heterogeneous phenomenon: A literature review. Scand. J. Caring Sci. 2012, 26, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Paasche-Orlow, M.K.; Wolf, M.S. The causal pathways linking health literacy to health outcomes. Am. J. Health Behav. 2007, 31, S19–S26. [Google Scholar] [CrossRef] [PubMed]
- Squiers, L.; Peinado, S.; Berkman, N.; Boudewyns, V.; McCormack, L. The health literacy skills framework. J. Health Commun. 2012, 17, 30–54. [Google Scholar] [CrossRef]
- Jordan, J.E.; Osborne, R.H.; Buchbinder, R. Critical appraisal of health literacy indices revealed variable underlying constructs, narrow content and psychometric weaknesses. J. Clin. Epidemiol. 2011, 64, 366–379. [Google Scholar] [CrossRef] [PubMed]
- Pleasant, A.; McKinney, J.; Rikard, R. Health literacy measurement: A proposed research agenda. J. Health Commun. 2011, 16, 11–21. [Google Scholar] [CrossRef]
- Kanj, M.; Mitic, W. Health Literacy and Health Promotion: Definitions, Concepts and Examples in the Eastern Mediterranean Region; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Baker, D.W.; Gazmararian, J.A.; Williams, M.V.; Scott, T.; Parker, R.M.; Green, D.; Ren, J.; Peel, J. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. Am. J. Public Health 2002, 92, 1278–1283. [Google Scholar] [CrossRef] [PubMed]
- Kickbusch, I.S. Health literacy: Addressing the health and education divide. Health Promot. Int. 2001, 16, 289–297. [Google Scholar] [CrossRef]
- Rudd, R.E.; Horowitz, A.M. Health and literacy: Supporting the oral health research agenda. J. Public Health Dent. 2005, 65, 131–132. [Google Scholar] [CrossRef]
- Smith, S.K.; Dixon, A.; Trevena, L.; Nutbeam, D.; McCaffery, K.J. Exploring patient involvement in healthcare decision making across different education and functional health literacy groups. Soc. Sci. Med. 2009, 69, 1805–1812. [Google Scholar] [CrossRef]
- Buchbinder, R.; Batterham, R.; Ciciriello, S.; Newman, S.; Horgan, B.; Ueffing, E.; Rader, T.; Tugwell, P.S.; Osborne, R.H. Health literacy: What is it and why is it important to measure? J. Rheumatol. 2011, 38, 1791–1797. [Google Scholar] [CrossRef]
- Jordan, J.E.; Buchbinder, R.; Osborne, R.H. Conceptualising health literacy from the patient perspective. Patient Educ. Couns. 2010, 79, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.; Wood, F.; Davies, M.; Edwards, A. The development of health literacy in patients with a long-term health condition: The health literacy pathway model. BMC Public Health 2012, 12, 130. [Google Scholar] [CrossRef] [PubMed]
- Zarcadoolas, C.; Pleasant, A.; Greer, D.S. Advancing Health Literacy: A Framework for Understanding and Action; John Wiley and Sons: San Francisco, CA, USA, 2006. [Google Scholar]


{kind=link}
| Database Type | Database | Temporal Period Covered (Start Date Reflects the Year in Which Each Database was Established. End Date is the Date in Which the Search was Limited to) |
|---|---|---|
| Academic | MEDLINE | 1946–8 August 2018 |
| Academic | Embase | 1980–8 August 2018 |
| Academic | CINAHL | 1982–8 August 2018 |
| Academic | Eric | 1966–8 August 2018 |
| Criterion | Inclusion | Exclusion |
|---|---|---|
| Time period | 1946 to August 2018 | Any study outside these dates |
| Language | English | Non-English |
| Type of article | Original research article or editorials published in a peer reviewed journal. | Any publication that was not original research, systematic reviews/meta-analysis, unpublished research. For example, PhD theses and reports were excluded. |
| Study focus | Articles that directly mentioned the term health literacy. | Nil |
| Geographical area of interest | Only those studies which were carried out in Australia. | Studies other than those which were carried out in Australia. |
| Setting | Any | Nil |
| Sr. No | Authors, Year | Objective | Study Population | Sample Size | Assessment Measure | Study Design and Analyses | Summary of Findings | Study’s Definition of HL, Constructs or Domains/Theoretical Framework |
|---|---|---|---|---|---|---|---|---|
| 1. | (Porteous, Palmer, & Wilkinson, 2014) [76] | To gather knowledge on eating behaviours, and nutrition-related needs during pregnancy and postnatally of women admitted to the postnatal ward. | Women aged at least 18 years who were admitted to the postnatal maternity ward at a hospital | N = 309 women | -------------------- | Study design: Cross-sectional study Analysis: SPSS, Descriptive statistics, Chi-square and independent samples t-tests | Many women reported an interest in nutrition and healthy weight management during pregnancy and in the postnatal period and rated its importance highly, and had poor diet quality, despite identifying healthy eating as a personal priority. 42% of the women self-reported gaining excess weight during pregnancy. One quarter reported knowing their gestational weight gain goals, yet only 1.6% was correct. Half reported interest in receiving nutrition education during pregnancy and post-delivery. Nutrition topics requested included healthy eating for development of baby pre- and post-delivery and maternal weight management. | ---------------- |
| 2. | (Adams, Appleton, Hill, Ruffin, & Wilson, 2009) [77] | To measure the level of functional health literacy in adults with asthma from a representative population sample and explore associations with health status and morbidity. | In a non-replacement sample, 1 adult age 15 years or older, having birthday in near future, was selected for interview in the home by trained health interviewers. | N = 2824 Males = 1358 Females = 1466 | Newest Vital Sign (a screening test developed specifically for use in primary care) | Study design: Data were obtained from the South Australian Health Omnibus Survey during spring 2008. Analysis: SPSS, Bivariate associations with Chi-square tests, Multiple logistic regression models | Inadequate and at-risk functional health literacy is common and is associated with adverse asthma outcomes in a representative sample of adults with asthma. Increased symptoms, functional impairment, and significant health care use were more common in people with less health literacy in analyses adjusted for age, sex, and education | -------------------- |
| 3. | (Maguire et al., 2011) [78] | The aim of this study was to explore health information sources accessed by people with schizophrenia and the level of trust invested in them. | People with schizophrenia, general practice attendees | N = 309 71 = adults with schizophrenia (recruited from both community and inpatient settings) 238 = general practice attendees. | ---------------- | Study design: Cross-sectional survey, questionnaire, Analysis: SPSS version 17, independent t-test, Chi-square test, Mann-Whitney U test and binary logistic regression, Correlation | There are significant differences in the reported utilization and trust of health information sources between people with schizophrenia and attendees at general practice settings. Those with schizophrenia are less likely to trust and obtain information from a doctor, and less likely to access the Internet | ---------------- |
| 4. | (Oh, Jorm, & Wright, 2009) [79] | To compare young people’s preference for a website with self-help books and two face-to-face services—counselling and mental health services. To explore factors associated with believing in the perceived helpfulness of each intervention. | Young Australians aged 12–25 years | N = 3746 | ---------------- | Study design: Telephone survey Analysis: SPSS version 16.0; percentage frequencies, logistic regressions | Most young people are open to the idea of accessing mental health information online, especially for disorders that are often perceived as behavioural problems. These young people also believe in helpseeking in general and are more willing to associate with peers who have mental health problems. | ---------------- |
| 5. | (Eckert, Kutek, Dunn, Air, & Goldney, 2010) [80] | To examine rural and urban differences in depression-related mental health literacy, experience of depression and help-seeking. | South Australian rural and urban young men aged between 15 and 30 years, who participated in two South Australian (SA) cross-sectional population-based Health Omnibus surveys (SAHOS), conducted in the autumns of 1998 and 2008 | 3010 = year 1998 3034 = year 2008 | Questionnaire devised by Jorm et al. which includes a vignette depicting a man (John) with classical features of depression. | Study design: Cross-sectional population-based survey Analysis: SPSS, StataSE, Pearson’s Chi-square tests, Fisher Exact test | Recognition of depression increased significantly in rural and urban young men between 1998 and 2008. More rural young men than urban men identified symptoms of depression in 1998 but that was not evident in 2008. Both groups were more likely to have a close friend experience symptoms of depression and to use antidepressant medications in 2008 compared with 1998. Rural young men experienced a significant increase in recognition of personal depressive symptoms and levels of confidence in psychiatrists and psychologists in 2008 compared with 1998. Both rural and urban young men were significantly less likely to rate dealing with problems on their own as helpful in 2008 as in 1998. | ---------------- |
| 6. | (Crawford et al., 2015) [81] | To determine the efficacy of the Mental Health First Aid (MHFA) training for university nursing students | Undergraduate nursing students at a large university located in Perth, Western Australia | N = 126 63 = intervention group 63 = control group | ---------------- | Study design: Experimental, Randomised Controlled Trial Analysis: SPSS Version 22; independent samples t-test or Pearson’s Chi-square test, Repeated measures analysis of variance, Logistic regression | Given the known burden of mental health disorders among student populations, it is important universities consider effective strategies to address mental health issues. Providing Mental Health First Aid (MHFA) training to students offers the advantage of increasing mental health literacy, among the student population. Further, students trained in MHFA are likely to utilise these skills in the broader community, when they graduate to the workforce. It is anticipated that this trial will demonstrate the scalability of MHFA in the university environment for pre-service nurses and that implementation of MHFA courses, with comprehensive evaluation, could yield positive improvements in the mental health literacy amongst this target group as well as other tertiary student groups | Mental health literacy incorporates several components: “(a) the ability to recognise specific disorders or different types of psychological distress; (b) knowledge and beliefs about risk factors and causes; (c) knowledge and beliefs about self-help interventions; (d) knowledge and beliefs about professional help available; (e) attitudes which facilitate recognition and appropriate help-seeking; and (f) knowledge of how to seek mental health information” (Jorm, 2000) [82]. |
| 7. | (Smith, Petrak, Dhillon, Taylor, & Milross, 2014) [83] | This study aimed to (1) explore radiation oncologists’ understandings and awareness of health literacy among patients with a reasonable command of English; (2) gain insight into oncologists’ views regarding health literacy; and (3) identify techniques oncologists employ to communicate to different literacy populations. | Radiation oncologists | N = 26 radiation oncologists. 19 = male 7 = female | ---------------- | Study design: Qualitative, Semi-structured interviews Analysis: Framework method | Four key themes were identified: (1) identifying a patient’s literacy level; (2) perceived impact of literacy; (3) challenges and strategies to communicating concepts and supporting decision-making; and (4) suggested improvements to the health system. Participants described subjectively assessing a person’s literacy level by monitoring the types of questions asked; analysing the language used; examining non-verbal behaviour, and considering a person’s socio-economic situation. Participants reported the challenges of discussing the subtleties of cancer treatments with lower literacy groups such as the benefits and risks of treatment options and clinical trials, and tended to provide the basic facts to facilitate understanding. | Health literacy represents ‘the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health’ (Nutbeam 2000) [84]. |
| Radiation oncologists acknowledged the importance of health literacy in oncology, and employed a number of techniques to tailor their communication to different literacy populations. | ||||||||
| 8. | (Rees, Austen, Anderson, & Egan, 2014) [85] | This study investigated the impact of providing corrective information about the nature of intrusive thoughts on their subsequent appraisal in a community sample. | Community participants | N = 148 community participants | Obsessive Compulsive Inventory-Revised, Intrusions Inventory | Study design: Experimental design Analysis: Descriptive statistics and mean comparisons, Correlation analysis, Repeated measures ANOVA | The results of this study support the efficacy of provision of brief written information in reducing negative appraisals of intrusive thoughts in a community sample. It suggests a possible role for education about intrusive thoughts as a prevention strategy for obsessive-compulsive disorder. | Mental health literacy is a term used to describe an individual’s understanding of various aspects of mental illness. This can include knowledge about early warning signs for common psychological disorders, or understanding treatment options. |
| 9. | (Isaacs, Maybery, & Gruis, 2013) [86] | To explore the help-seeking behaviour of Aboriginal men who are mentally unwell in a rural Victorian community. | Aboriginal people in Australia including men, carers and those involved in service delivery. | N = 17 Aboriginal people 15 = male | ---------------- | Study design: Qualitative design, semi-structured interviews Analysis: Thematic analysis | The findings suggest that there is a need for programmes that aim to improve mental health literacy and promote help seeking among Aboriginal men who are mentally unwell. Such programmes need to be developed jointly by mental health services as well as Aboriginal stakeholders, and implemented in a culturally sensitive and acceptable way. | ---------------- |
| 10. | (Jamieson, Parker, & Richards, 2008) [87] | To investigate the social, cultural and environmental context of oral health among a group of Indigenous Australians in South Australia’s mid-north region. | Participants were Indigenous and had lived in South Australia’s mid-north region for most of their lives | N = 34 4 = focus group discussions 30 = females 4 = males | ---------------- | Study design: Qualitative design, Focus group discussions Analysis: Nud*st QSR N6 software, Thematic analysis | Five sub-categories were identified; ‘lifestyle changes’, ‘oral health behaviours’, ‘barriers to dental care’, ‘impact of poor oral health’ and ‘oral health literacy’. Participants felt that historical legacy impacted on the oral health of community members, through continued practices of being told what to do, where to live and what oral health services were available to them. Participants perceived they had little power over their oral health or oral health care decisions. | ---------------- |
| 11. | (Hosking, Buchbinder, Pasco, Williams, & Brennan-Olsen, 2016) [88] | To add that health literacy is likely to play a major role in the ability of patients to access, understand, and apply information in order to make informed decisions about osteoporosis treatment. | Osteoporosis patients | Health Literacy Questionnaire (HLQ) (to assess individual’s health literacy needs) | Letter to the editor | The comprehension of health literacy needs of a person by applying most recent tools of health literacy in order to develop understanding regarding obstacles in medication. This strategy would ensure addressing problems of patients in person-centered way, improved adherence to medication and attaining outcomes of patients. | ---------------- | |
| 12. | (White et al., 2013) [89] | To assess the impact of a brief intervention (BI) designed to improve HCV vaccine CTL among people who inject drugs in Sydney, Australia. | People who inject drugs | N = 102 74 = male 28 = female | ---------------- | Study design: Experimental, Community-based prospective observational study Analysis: STATA 12.0; Means, medians, interquartile ranges, paired samples t-test, Multiple logistic regression | A significant increase in hepatitis C virus (HCV) vaccine clinical trial literacy (CTL) was observed, suggesting that new and relatively novel concepts can be learned and recalled in this group. These findings support the feasibility of future trials among this population. | ---------------- |
| 13. | (Briggs et al., 2011) [90] | To measure broad elements of health literacy among individuals with chronic low back pain (CLBP) and without low back pain (LBP) using the Health Literacy Measurement Scale (HeLMS). | adults who reported either CLBP for 3 months or more, or no history of LBP within the last 12 months | N = 80 36 = Community-dwelling adults with chronic low back pain 44 = Community-dwelling adults wit with no history of low back pain | Nordic Musculoskeletal Pain Questionnaire, Nordic Musculoskeletal, Oswestry Disability Index, Avoidance Beliefs Questionnaire, Back Pain Beliefs Questionnaire, Coping Skills Questionnaire, Functional health Literacy (s-TOFHLA). Health Literacy Measurement Scale (HeLMS) (to measure an individual’s ability to seek, understand or utilise health information) | Study design: Community-based cohort study in Perth, Western Australia, from November 2008 to examine familial associations in LBP. Analyses: SPSS Statistics 17.0; independent t-tests Chi-square tests, Mann-Whitney tests | Although no differences were identified in HeLMS scores between the groups for seven of the health literacy domains, adults with CLBP reported greater difficulty in engaging in general positive health behaviours. This aspect of health literacy suggests that self-management support initiatives may benefit individuals with CLBP. | Health literacy—the ability to seek, understand and utilise health information |
| 14. | (Smith et al., 2010) [91] | To determine whether a decision aid designed for adults with low education and literacy can support informed choice and involvement in decisions about screening for bowel cancer. | Adults aged between 55 and 64 with low educational attainment, eligible for bowel cancer screening. | N = 572 adults | ---------------- | Study design: Experimental, Randomized controlled trial Analysis: SPSS, paired sample t-test and Wilcoxon signed rank test, Mann-Whitney test, Chi-square test, Mantel- Haenszel test | Tailored decision support information can be effective in supporting informed choices and greater involvement in decisions about faecal occult blood testing among adults with low levels of education, without increasing anxiety or worry about developing bowel cancer. Using a decision aid to make an informed choice may, however, lead to lower uptake of screening. | ---------------- |
| 15. | (Saunders & Peerson, 2010) [92] | To the editor | To the editor | ---------------- | Letter to the editor | Australian health initiatives aimed at reducing the burden of chronic and preventable disease should consider the role and challenges of health literacy beyond its application to health services use. The growing understanding of the complex behavioural, social, systemic, and ecological forces that influence health and wellbeing should help guide these efforts. | ---------------- | |
| 16. | (Jennings, Spurling, & Askew, 2014) [93] | To identify barriers and enablers to undertaking health checks in an urban Aboriginal Medical Service. | Clinical staff (doctors, nurses and Aboriginal and Torres Strait Islander health workers, AHWs) | N = 25 clinical staff (doctors, nurses and Aboriginal and Torres Strait Islander health workers). 10 = AHWs 8 = nurses 7 = doctors | ---------------- | Study design: Qualitative research design; Semi-structured Interviews Analysis: NVivo 9 software, content analysis | Data analysis revealed that successful completion of HCs was contingent upon several interconnected components, including the client attending the Aboriginal Medical Service (Shamsuddin et al.) and consenting to the Health Check (HC), and staff initiating and completing it. Barriers and potential enablers were indentified at each of these stages, in addition to overarching systems within the clinics. | ---------------- |
| 17. | (Gratwick-Sarll & Bentley, 2014) [94] | To improve eating disorders mental health literacy. | undergraduate Australian National University third year psychology students | N = 177 undergraduate students. 141 = female 35 = male 1 = other | First Aid Experiences Questionnaire, First Aid Knowledge Test, Social Distance Scale, Mental Health Literacy Questionnaire for Bulimic Type Eating Disorders (to assess health literacy related with eating disorders) | Study design: Repeated measures, uncontrolled, preliminary evaluation of a single 3-hour workshop Analysis: Paired samples two-tailed t-tests, repeated measures analyses of variance (ANOVAs), McNemar’s test, Cochran’s Q | Following participation in the workshop, significant increases in eating disorder recognition and knowledge, and significant decreases in stigmatizing attitudes, were reported by participants. Moreover, 85% of participants reported that they provided assistance to someone whom they suspected had a mental health condition, including an eating disorder, during the 3-month follow-up period. | Mental health literacy: the knowledge and beliefs that individuals hold, which lead to improved recognition, management, and prevention of their own or another’s mental disorder (Jorm, Korten, Jacomb, Christensen, Rodgers, & Pollitt, 1997) |
| 18. | (Caposecco, Hickson, Meyer, & Khan, 2016) [95] | This study investigated if a hearing aid user guide modified using best practice principles for health literacy resulted in superior ability to perform hearing aid management tasks, compared with the user guide in the original form. | Participants having ages 55 years or older, living in the community, comfortable speaking and reading English, and have no experience using or managing hearing aids (HAs). | N = 89 adults ages 55 years and over. 47 = Modified guide 42 = The original guide | Demographic Questionnaire, The Measure of Audiologic Rehabilitation Self-Efficacy for Hearing Aids, The Hearing Aid Management test, The Short test of Functional Health Literacy in Adults (Timed reading comprehension test that consists of two prose passages containing actual materials that an adult might encounter in a healthcare setting e.g., instructions for a gastrointestinal procedure), Montreal Cognitive Assessment, Grooved Pegboard Test, Pure-Tone Audiogram | Study design: Experimental, Two-arm study design. Analysis: Stata software, independent samples t test, Chi-square test, Mann–Whitney U test, and the Fisher’s exact test, multivariable linear regression model, multivariable linear regression model | Findings indicate that the need to design hearing aid user guides in line with best practice principles of health literacy as a means of facilitating improved hearing aid management in older adults. | Health literacy refers to “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions” (Ratzan & Parker 2000, p. 3). |
| 19. | (Cashin, Heartfield, Cox, Dunn, & Stasa, 2015) [96] | This paper presents analysis of consumer focus groups that were undertaken as a part of the project to develop the now current Nursing and Midwifery Board of Australia’s Nurse Practitioner Standards for Practice. | Consumer. The age of the consumers varied from people in their early 20s to people who were over 60 years of age. | N = 6 focus groups (32 consumers) | ---------------- | Study design: Qualitative, focus groups Analysis: Interpretive analysis | Consumers’ knowledge of nurses’ roles in the Australian primary healthcare system, and hence system literacy (particularly in terms of navigating the system), was low. Of perhaps greatest importance is the fact that those consumers with low health systems literacy also exhibited a low level of motivation to seek new knowledge. Many consumers relied on the medical profession to direct care. | Health literacy relates not only to individual literacy skills, but also to knowledge of the healthcare context or system Australian Commission on Safety and Quality in Healthcare (ACSQHC 2013). |
| 20. | (Davies, Bukulatjpi, Sharma, Davis, & Johnston, 2014) [97] | To explore the knowledge, perceptions and experiences of remote dwelling Indigenous adults and their health care providers relating to hepatitis B infection with a view to using this as the evidence base to develop a culturally appropriate educational tool. | Health clinic staff, community health educators, liver clinic staff—both urban and remote, —and doctors and nurses, Indigenous and non-Indigenous, Indigenous people living with chronic hepatitis B (CHB) and Indigenous community members. | 12 = patients with hepatitis B 9 = community members 13 = key informants 25 = were Indigenous individuals | ---------------- | Study design: Participatory action research project design, Semi-structured interviews Analysis: Deductive and inductive thematic analysis | Low levels of biomedical knowledge about Hepatitis B, negative perceptions of Hepatitis B, communication (particularly language) and culture were the major themes that emerged from the data. Accurate concepts grounded in Indigenous culture such as “only your blood can tell the story” were present but accompanied by a feeling of disempowerment due to perceived lack of “medical” understanding, and informed partnerships between caregiver and patient. Culturally appropriate discussions in a patient’s first language using visual aids were identified as vital to improving communication. | Paasche-Orlow & Wolf’s model of the pathways linking health literacy and health outcomes (Paasche-Orlow, & Wolf, 2007) |
| 21. | (Yuen et al., 2016) [98] | To develop a conceptual model that describes the elements of cancer caregiver health literacy. | Caregivers, people with cancer and healthcare providers/policymakers. | N = 6 concept mapping workshops were conducted 13 = caregivers 13 = people with cancer 11 = healthcare providers/policymakers | ---------------- | Study design: Mixed methods approach; Concept mapping | Six major themes and 17 subthemes were identified from 279 statements generated by participants during concept mapping workshops. Major themes included: access to information, understanding of information, relationship with healthcare providers, relationship with the care recipient, managing challenges of caregiving and support systems. The study extends conceptualisations of health literacy by identifying factors specific to caregiving within the cancer context. The findings demonstrate that caregiver health literacy is multidimensional, includes a broad range of individual and interpersonal elements, and is influenced by broader healthcare system and community factors. | Health literacy can be understood as a range of ‘personal characteristics and social resources needed for individuals and communities to access, understand, appraise and use information and services to make decisions about health, or that have implications for health. Health literacy includes the capacity to communicate, assert and enact these decisions’ (Yuen et al. 2014) [98]. |
| 22. | (Nasuuna, Santoro, Kremer, & de Silva, 2016) [99] | To examine the relationship between health conditions, specialist health service utilisation and academic performance in Australian children. | Victorian children | N = 24,678 children 12,660 = men 11,982 = women | School Entrant Health Questionnaire (survey tool with parent report on children’s health) | Study design: Prospective quasi-longitudinal study Analysis: Univariable and multivariable linear regression, Linear and logistic regressions | Some health conditions put children at risk of poorer academic performance, and interventions to prevent this such as appropriate support services in schools should be considered. | ---------------- |
| 23. | (Whittaker, Hodge, Mares, & Rodney, 2015) [100] | To identify the minimum health information system (Akoijam, Jamir, Phesao, & Senjam) competencies that could be expected in low- and middle-income countries (LMICs) that do not have advanced technology. | Health workers | N = 38 experts with broad-based HIS knowledge and extensive development experience 21 = male 17 = female | ---------------- | Delphi approach Analysis: Qualtrics® software and content analysis. | Based on the initial competencies identified in the literature review and after two rounds of consultation with experts via a Delphi method, 68 HIS competencies (51 core and 17 ICT-specific) were identified in this consultation. The competencies focused on both the generation and use of data at all levels of the health system, highlighting the importance of embedding a culture of information use. This consultation is one of the first to identify the HIS competencies required among general health workers, as opposed to specialist HIS roles. It is also one of the first attempts to develop a framework on minimum HIS competencies needed in LMICs, highlighting the skills needed at each level of the system, and identifying potential gaps in current training to allow a more systematic approach to HIS capacity-building. | ---------------- |
| 24. | (May, Rapee, Coello, Momartin, & Aroche, 2014) [101] | To investigate differences in mental health knowledge and beliefs between participants from the Iraqi and Sudanese refugee communities, and Australian born individuals, in Sydney, Australia. | Adults (18 years and over); Iraqi nationals, Sudanese nationals, and Australians. | N = 97 32 = Iraqi nationals 32 = Sudanese nationals 33 = Australians. | ---------------- | Study design: Mixed-method, semi-structured interview, Chi-square test, one-way ANOVA Analysis: SPSS, Thematic analysis | Although sampling was non-random, suggesting caution in the interpretation of results, it appears that the mental health literacy of lay Australians may be more aligned with the western medical model of mental disorder than that of Iraqi and Sudanese refugee communities. Mental health literacy support needs of Iraqi and Sudanese refugee communities resettled in western countries such as Australia might include education about specific symptoms and causes of mental disorder and the effectiveness of psychiatric treatments. | Mental health literacy refers to the knowledge and beliefs about mental disorders which aid their recognition, management, and prevention (Jorm, 2000) [82]. |
| 25. | (Simpson et al., 2015) [102] | To evaluate the sexual health literacy among students at the University of Tasmania. | University student populations | N = 1786 | University of Missouri Sexual Health Survey (having three domains i.e. knowledge, sexually transmissible infection and pregnancy), ARCSHS Secondary Students and Sexual Health Survey having two domains (i.e. knowledge and HIV/Hepatitis) | Study design: Cross-sectional study Analysis: STATA/SE 12.0 for Windows (StataCorp, College Station, TX, USA); Linear regression | This study, one of the first among university students in Australia, found a varied SHL by sex, age, sexual education and sexual experience, as well as by birthplace and religious affiliation. These findings have applications in orientation and education programs at Australian universities. | Sexual health literacy (SHL) is the knowledge and familiarity with healthy practices as regards sexual health, and risk reduction strategies to engage in sexual activity safely and minimise negative consequences |
| 26. | (Yiu, & Bajorek, 2018) [103] | To (1) characterise older patients taking warfarin, (2) assess these patients’ level of warfarin knowledge, and (3) describe their strengths and limitations in health literacy, and (4) explore relationships between participants’ characteristics, warfarin knowledge and health literacy. | older patients (aged >65 years) taking warfarin in an Australian general practice setting | N = 34 | Purpose-designed questionnaire to record participants’ medical history, medication history, history of warfarin use, previous education received about warfarin Customised brief Warfarin Knowledge Questionnaire Health Literacy Questionnaire (HLQ | Descriptive, questionnaire-based pilot study, IBM SPSS version 23.0, Microsoft Excel. Descriptive statistics, non-parametric tests, e.g., chi-square test, Mann-Whitney U test, Spearman correlation test | In this study warfarin knowledge gaps and a limitation of health literacy amongst a small sample of older patients were identified. The findings suggest that education and resources may need to be tailored to the needs of older patients taking warfarin and their carers to address these knowledge gaps and limitations in health literacy. Patients who may need greater support include those that need assistance in completing the HLQ, are overseas-born, or are taking 5 or more long-term medications. | World Health Organisation (WHO) definition: the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health [27] |
| 27. | (Stanton, Rebar, & Rosenbaum, 2018) [104] | To examine the community’s mental health literacy, and views regarding exercise delivery for people with depression. | People with depression | N = 1265 | Questionnaire devised by Jorm et al. [82] which includes a vignette depicting a man (John) with classical features of depression | telephone-based 2017 National Social Survey, cross-sectional population survey, descriptive statistics, Chi-square tests for goodness of fit | Australian adults demonstrate a high level of exercise and mental health literacy. The high level of support for accredited exercise physiologists is evidence of the effectiveness of health promotion campaigns from peak exercise professional agencies. | ------------------- |
| Sr. No. | Author, Year | Broader Region (State Wise) | Geographical Location | Time Sequence | ||
|---|---|---|---|---|---|---|
| Data Collected From (Location) | Corresponding Author’s Institutions | Time Frame of Data Collection | Study Published on | |||
| 1. | (Porteous et al., 2014) [76] | Queensland | Socially disadvantaged area approx. 28 km south of Brisbane (Queensland, Australia) | Logan Hospital, Queensland Health, Meadowbrook, Australia. | Between 18th May 2012 and 8th October 2012 | 2014 |
| 2. | (Adams et al., 2009) [77] | South Australia | ------------------- | University of Adelaide | South Australian Health Omnibus Survey during spring 2008 | 2009 |
| 3. | (Maguire et al., 2011) [78] | Australian Capital Territory (ACT) | Australian Capital Territory (ACT) | Australian National University, Canberra Hospital, Woden, Australian Capital Territory, Australia. | July to October 2009 | 2011 |
| 4. | (Oh et al., 2009) [79] | Whole Australia | Covering the whole Australia | University of Melbourne Locked Bag 10 Parkville (Services) 3052, Australia | June to August 2006 | 2009 |
| 5. | (Eckert et al., 2010) [80] | South Australia | South Australia | University of Adelaide, Adelaide, South Australia. | 1998 and 2008 | 2010 |
| 6. | (Crawford et al., 2015) [81] | Western Australia | Perth, Western Australia | Curtin University, Perth, Australia | 2015 | |
| 7. | (Smith et al., 2014) [83] | New South Wales | ------------------- | University of New South Wales, Sydney, Australia | July and December 2011 | 2014 |
| 8. | (Rees et al., 2014) [85] | Western Australia | ------------------- | Curtin University, Perth, Western Australia | ------------------- | 2014 |
| 9. | (Isaacs et al., 2013) [86] | Victoria | Monash University, Australia. | ------------------- | 2013 | |
| 10. | (Jamieson et al., 2008) [87] | Indigenous Australians | rural-dwelling Indigenous Australians; South Australia (those identifying as Aboriginal, Torres Strait Islander or both) Port Augusta and surrounding areas | University of Adelaide, Australia | ------------------- | 2007 |
| 11. | (Hosking et al., 2016) [88] | Victoria | ------------------- | Deakin University, Geelong, Australia | ------------------- | 2016 |
| 12. | (White et al., 2013) [89] | New South Wales | Sydney, Australia. | University of New South Wales, Sydney, Australia. | November 2008 and September 2010 | 2013 |
| 13. | (Briggs et al., 2011) [90] | Western Australia | Perth, Western Australia | Curtin University, Australia | November 2008 | 2011 |
| 14. | (Smith et al., 2010) [91] | New South Wales | New South Wales, Australia | Sydney School of Public Health, University of Sydney, Australia | ------------------- | 2010 |
| 15. | (Saunders & Peerson, 2010) [92] | Victoria | ------------------- | Deakin University, Geelong, Australia | ------------------- | 2010 |
| 16. | (Jennings et al., 2014) [93] | Queensland | Community-controlled Aboriginal and Torres Strait Islander medical services (AMSs) servicing Brisbane, Australia | The University of Queensland, Herston, Australia. | November and December 2010. | 2014 |
| 17. | (Gratwick-Sarll & Bentley, 2014) [94] | ACT | Australian National University | Australian National University, Canberra, Australia | ------------------- | 2014 |
| 18. | (Caposecco et al., 2016) [95] | Queensland | ------------------- | The University of Queensland, Brisbane, Australia. | ------------------- | 2016 |
| 19. | (Cashin et al., 2015) [96] | Western Australia, New South Wales, Queensland, Australian capital city, South Australia, Northern Territory | Southern Cross University and the University of Sydney. The focus groups occurred in: Rockingham, a small city south of Perth in Western Australia; the regional city of Cowra in New South Wales; Southport on the Gold Coast of Queensland; Darwin, the capital city of the Northern Territory; Canberra, the Australian capital city; and Adelaide, the capital city of South Australia. | 2012 | 2015 | |
| 20. | (Davies et al., 2014) [97] | Northern Territory | Northern Australia; health clinic of a remote community in Arnhem Land, 521 km northeast of Darwin (the | Menzies School of Health Research, Rocklands Drive, Tiwi, Darwin, Australia | July 2012 and December 2013. | 2014 |
| 21. | (Yuen et al., 2016) [98] | Victoria | Two chemotherapy clinics from one public health service in Melbourne, Australia | Deakin University, Burwood, Australia | ------------------- | 2016 |
| 22. | (Nasuuna et al., 2016) [99] | Victoria | ------------------- | The University of Melbourne, Parkville, Australia. | Fifty-six percent of 2008 School Entry Health Questionnaire (SEHQ) was linked to the year 3 National Assessment Program—Literacy and Numeracy (NAPLAN) collected in 2011 | 2016 |
| 23. | (Whittaker et al., 2015) [100] | Queensland | Science Direct, Pub Med, CINAHL, Google Scholar, Internet search engine (google.com) | The University of Queensland, Brisbane, Australia | Database searches covered the period 1990–2012. | 2015 |
| 24. | (May et al., 2014) [101] | New South Wales | Sydney, Australia | Macquarie University, Sydney, Australia | --------------------- | 2014 |
| 25. | (Simpson et al., 2015) [102] | Tasmania | University of Tasmania | University of Tasmania, Australia | August/September 2013 | 2015 |
| 26. | (Yiu, & Bajorek, 2018) [103] | New South Wales | The Hills Shire (Greater Western Sydney) | Graduate School of Health, University of Technology of Sydney. Ultimo, NSW (Australia). | September 2015 and January 2016. | 2018 |
| 27. | (Stanton, Rebar & Rosenbaum, 2018) [104] | Queensland | Population Research Laboratory (PRL) at Central Queensland University, Australia. | School of Health, Medical and Applied Sciences, Central Queensland University | July 17 and finished on 23 August 2017 | 2018 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choudhry, F.R.; Ming, L.C.; Munawar, K.; Zaidi, S.T.R.; Patel, R.P.; Khan, T.M.; Elmer, S. Health Literacy Studies Conducted in Australia: A Scoping Review. Int. J. Environ. Res. Public Health 2019, 16, 1112. https://doi.org/10.3390/ijerph16071112
Choudhry FR, Ming LC, Munawar K, Zaidi STR, Patel RP, Khan TM, Elmer S. Health Literacy Studies Conducted in Australia: A Scoping Review. International Journal of Environmental Research and Public Health. 2019; 16(7):1112. https://doi.org/10.3390/ijerph16071112
Chicago/Turabian StyleChoudhry, Fahad Riaz, Long Chiau Ming, Khadeeja Munawar, Syed Tabish R. Zaidi, Rahul P. Patel, Tahir Mehmood Khan, and Shandell Elmer. 2019. "Health Literacy Studies Conducted in Australia: A Scoping Review" International Journal of Environmental Research and Public Health 16, no. 7: 1112. https://doi.org/10.3390/ijerph16071112
APA StyleChoudhry, F. R., Ming, L. C., Munawar, K., Zaidi, S. T. R., Patel, R. P., Khan, T. M., & Elmer, S. (2019). Health Literacy Studies Conducted in Australia: A Scoping Review. International Journal of Environmental Research and Public Health, 16(7), 1112. https://doi.org/10.3390/ijerph16071112