

The Prospective Effects of Coping Strategies on Mental Health and Resilience at Five Months after HSCT

 ,
,
Abstract
1. Background
2. Methods
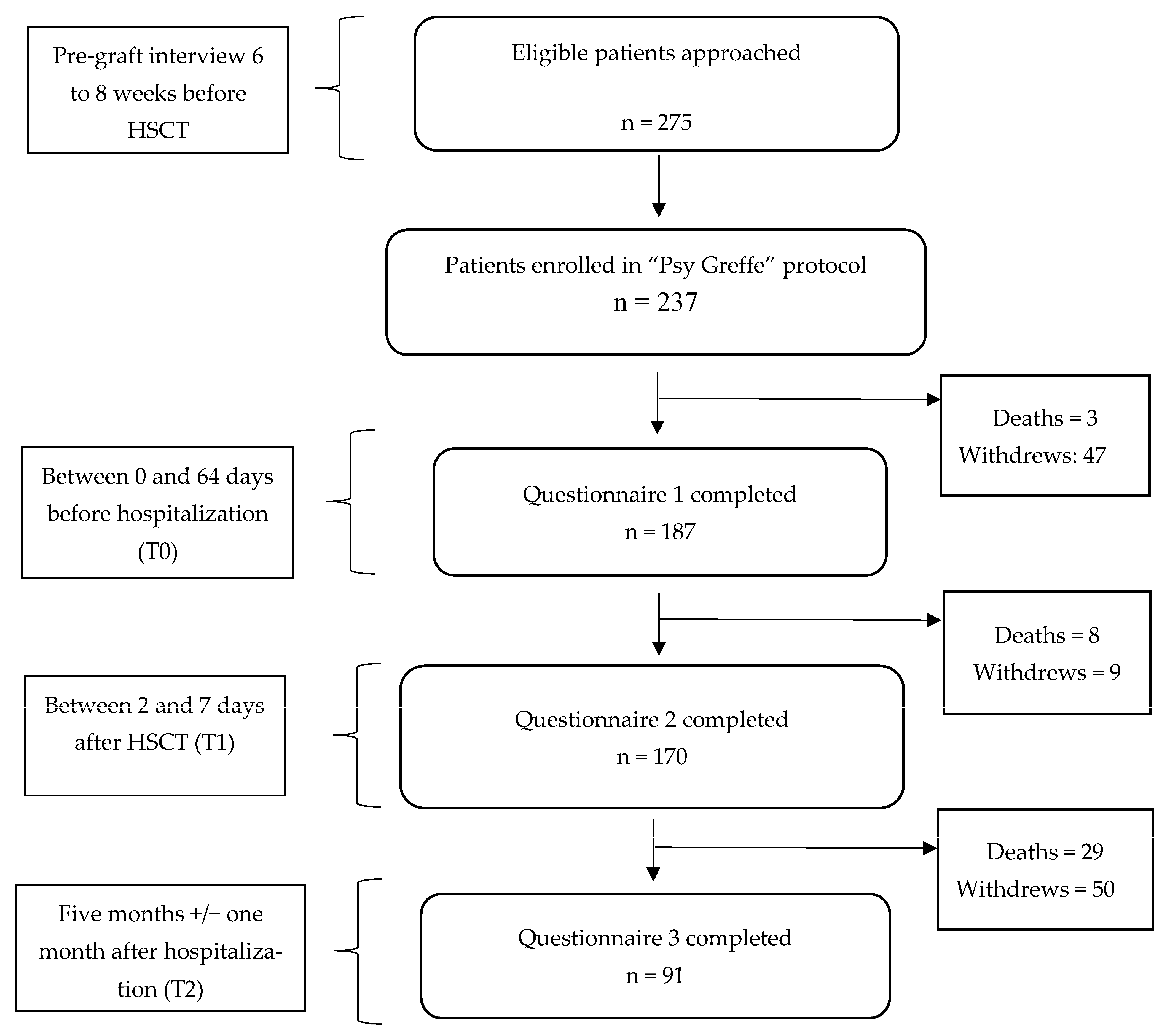
2.1. Participants
2.2. Procedures
2.3. Measures
3. Results
3.1. Descriptive Statistics
3.2. Relationships between Perceived Stress, Perceived Social Support, Perceived Control, and Adjustment Coping Strategies at t1
3.3. The Prospective Effects of Coping Strategies on Quality of Life, Mental Health, PTSD, and Resilience at Five Months after Transplantation
3.4. Relationships between Coping Strategies and Medical Outcomes
4. Discussion
4.1. Study Limitations
4.2. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- El-Jawahri, A.R.; Bs, H.B.V.; Traeger, L.N.; Ba, J.N.F.; Keenan, T.; Gallagher, E.R.; Greer, J.A.; Pirl, W.F.; Jackson, V.A.; Spitzer, T.R.; et al. Quality of life and mood predict posttraumatic stress disorder after hematopoietic stem cell transplantation. Cancer 2016, 122, 806–812. [Google Scholar] [CrossRef]
- Kisch, A.; Lenhoff, S.; Zdravkovic, S.; Bolmsjö, I. Factors associated with changes in quality of life in patients undergoing allogeneic haematopoietic stem cell transplantation. Eur. J. Cancer Care 2012, 21, 735–746. [Google Scholar] [CrossRef]
- Sun, C.-L.; Kersey, J.H.; Francisco, L.; Armenian, S.H.; Baker, K.S.; Weisdorf, D.J.; Forman, S.J.; Bhatia, S. Burden of morbidity in 10+ year survivors of hematopoietic cell transplantation: Report from the bone marrow transplantation survivor study. Biol. Blood Marrow Transpl. 2013, 19, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Pillay, B.; Lee, S.J.; Katona, L.; De Bono, S.; Burney, S.; Avery, S. A prospective study of the relationship between sense of coherence, depression, anxiety, and quality of life of haematopoietic stem cell transplant patients over time. Psycho-Oncology 2014, 24, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Artherholt, S.B.; Hong, F.; Berry, D.L.; Fann, J.R. Risk factors for depression in patients undergoing hematopoietic cell transplantation. Biol. Blood Marrow Transpl. 2014, 20, 946–950. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hefner, J.; Kapp, M.; Drebinger, K.; Dannenmann, A.; Einsele, H.; Grigoleit, G.-U.; Faller, H.; Csef, H.; Mielke, S. High prevalence of distress in patients after allogeneic hematopoietic SCT: Fear of progression is associated with a younger age. Bone Marrow Transpl. 2014, 49, 581–584. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S.; Scherwath, A.; Schirmer, L.; SchulzKindermann, F.; Neumann, K.; Kruse, M.; Dinkel, A.; Kunze, S.; Balck, F.; Kroger, N.; et al. Fear of recurrence and its impact on quality of life in patients with hematological cancers in the course of allogeneic hematopoietic SCT. Bone Marrow Transpl. 2014, 49, 1217–1222. [Google Scholar] [CrossRef] [PubMed]
- Biagioli, V.; Piredda, M.; Mauroni, M.R.; Alvaro, R.; De Marinis, M.G. The lived experience of patients in protective isolation during their hospital stay for allogeneic haematopoietic stem cell transplantation. Eur. J. Oncol. Nurs. 2016, 24, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Biagioli, V.; Piredda, M.; Alvaro, R.; de Marinis, M. The experiences of protective isolation in patients undergoing bone marrow or haematopoietic stem cell transplantation: Systematic review and metasynthesis. Eur. J. Cancer Care 2016, 26, e12461. [Google Scholar] [CrossRef]
- Biagioli, V.; Piredda, M.; Annibali, O.; Tirindelli, M.C.; Pignatelli, A.; Marchesi, F.; Mauroni, M.R.; Soave, S.; Del Giudice, E.; Ponticelli, E.; et al. Factors influencing the perception of protective isolation in patients undergoing haematopoietic stem cell transplantation: A multicentre prospective study. Eur. J. Cancer Care 2019, 28, e13148. [Google Scholar] [CrossRef]
- Prieto, J.M.; Atala, J.; Blanch, J.; Carreras, E.; Rovira, M.; Cirera, E.; Espinal, A.; Gasto, C. Role of depression as a predictor of mortality among cancer patients after stem-cell transplantation. J. Clin. Oncol. 2005, 23, 6063–6071. [Google Scholar] [CrossRef] [PubMed]
- Baliousis, M.; Rennoldson, M.; Dawson, D.; Mills, J.; das Nair, R. Perceptions of hematopoietic stem cell transplantation and coping predict emotional distress during the acute phase after transplantation. Oncol. Nurs. Forum 2017, 44, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Tecchio, C.; Bonetto, C.; Bertani, M.; Cristofalo, D.; Lasalvia, A.; Nichele, I.; Bonani, A.; Andreini, A.; Benedetti, F.; Ruggeri, M.; et al. Predictors of anxiety and depression in hematopoietic stem cell transplant patients during protective isolation. Psycho-Oncology 2013, 22, 1790–1797. [Google Scholar] [CrossRef]
- Lazarus, R.F.; Folkman, S.C.S. Stress, Appraisal and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Efficace, F.; Breccia, M.; Cottone, F.; Okumura, I.; Doro, M.; Riccardi, F.; Rosti, G.; Baccarani, M. Psychological well-being and social support in chronic myeloid leukemia patients receiving lifelong targeted therapies. Support. Care Cancer 2016, 24, 4887–4894. [Google Scholar] [CrossRef]
- Paterson, C.; Jones, M.; Rattray, J.; Lauder, W. Exploring the relationship between coping, social support and health-related quality of life for prostate cancer survivors: A review of the literature. Eur. J. Oncol. Nurs. 2013, 17, 750–759. [Google Scholar] [CrossRef]
- Bárez, M.; Blasco, T.; Fernández-Castro, J.; Viladrich, C. Perceived control and psychological distress in women with breast cancer: A longitudinal study. J. Behav. Med. 2008, 32, 187–196. [Google Scholar] [CrossRef]
- Groarke, A.; Curtis, R.; Kerin, M. Global stress predicts both positive and negative emotional adjustment at diagnosis and post-surgery in women with breast cancer. Psycho-Oncology 2013, 22, 177–185. [Google Scholar] [CrossRef]
- Li, Y.; Yang, Y.; Zhang, R.; Yao, K.; Liu, Z. The mediating role of mental adjustment in the relationship between perceived stress and depressive symptoms in hematological cancer patients: A cross-sectional study. PLoS ONE 2015, 10, e0142913. [Google Scholar] [CrossRef] [PubMed]
- Hulbert-Williams, N.; Storey, L.; Wilson, K. Psychological interventions for patients with cancer: Psychological flexibility and the potential utility of Acceptance and Commitment Therapy. Eur. J. Cancer Care 2015, 24, 15–27. [Google Scholar] [CrossRef]
- Moritz, S.; Jahns, A.K.; Schröder, J.; Berger, T.; Lincoln, T.M.; Klein, J.P.; Göritz, A.S. More adaptive versus less maladaptive coping: What is more predictive of symptom severity? Development of a new scale to investigate coping profiles across different psychopathological syndromes. J. Affect. Disord. 2015, 191, 300–307. [Google Scholar] [CrossRef]
- Thompson, R.J.; Mata, J.; Jaeggi, S.M.; Buschkuehl, M.; Jonides, J.; Gotlib, I.H. Maladaptive coping, adaptive coping, and depressive symptoms: Variations across age and depressive state. Behav. Res. Ther. 2010, 48, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Hodges, K.; Winstanley, S. Effects of optimism, social support, fighting spirit, cancer worry and internal health locus of control on positive affect in cancer survivors: A path analysis. Stress Health 2012, 28, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Manne, S.; Myers-Virtue, S.; Kashy, D.; Ozga, M.; Kissane, D.; Heckman, C.; Rubin, S.C.; Rosenblum, N. Resilience, positive coping, and quality of life among women newly diagnosed with gynecological cancers. Cancer Nurs. 2015, 38, 375. [Google Scholar] [CrossRef]
- Brunault, P.; Champagne, A.-L.; Huguet, G.; Suzanne, I.; Senon, J.-L.; Body, G.; Rusch, E.; Magnin, G.; Voyer, M.; Réveillère, C.; et al. Major depressive disorder, personality disorders, and coping strategies are independent risk factors for lower quality of life in non-metastatic breast cancer patients. Psycho-Oncology 2016, 25, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Allart, P.; Soubeyran, P.; Cousson-Gélie, F. Are psychosocial factors associated with quality of life in patients with haematological cancer? A critical review of the literature. Psycho-Oncology 2012, 22, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, C.; Pocock, M.; Titley, K.; Lloyd, K. Predicting psychological distress in patients with leukaemia and lymphoma. J. Psychosom. Res. 2003, 54, 289–292. [Google Scholar] [CrossRef] [PubMed]
- O’connor, M.; Guilfoyle, A.; Breen, L.; Mukhardt, F.; Fisher, C. Relationships between quality of life, spiritual well-being, and psychological adjustment styles for people living with leukaemia: An exploratory study. Ment. Health Relig. Cult. 2007, 10, 631–647. [Google Scholar] [CrossRef]
- Barata, A.; Gonzalez, B.D.; Sutton, S.K.; Small, B.J.; Jacobsen, P.B.; Field, T.; Fernandez, H.; Jim, H.S. Coping strategies modify risk of depression associated with hematopoietic cell transplant symptomatology. J. Health Psychol. 2016, 23, 1028–1037. [Google Scholar] [CrossRef]
- Fife, B.L.; Huster, G.A.; Cornetta, K.G.; Kennedy, V.N.; Akard, L.P.; Broun, E.R. Longitudinal study of adaptation to the stress of bone marrow transplantation. J. Clin. Oncol. 2000, 18, 1539–1549. [Google Scholar] [CrossRef]
- Rodrigue, J.R.; Boggs, S.R.; Weiner, R.S.; Behen, J.M. Mood, coping style, and personality functioning among adult bone marrow transplant candidates. Psychosomatics 1993, 34, 159–165. [Google Scholar] [CrossRef]
- Wells, K.J.; Booth-Jones, M.; Jacobsen, P.B. Do coping and social support predict depression and anxiety in patients undergoing hematopoietic stem cell transplantation? J. Psychosoc. Oncol. 2009, 27, 297–315. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, P.B.; Sadler, I.J.; Booth-Jones, M.; Soety, E.; Weitzner, M.A.; Fields, K.K. Predictors of posttraumatic stress disorder symptomatology following bone marrow transplantation for cancer. J. Consult. Clin. Psychol. 2002, 70, 235. [Google Scholar] [CrossRef]
- Cayrou, S.; Dickès, P.; Gauvain-Piquard, A.; Rogé, B. The mental adjustment to cancer (MAC) scale: French replication and assessment of positive and negative adjustment dimensions. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2002, 12, 8–23. [Google Scholar] [CrossRef] [PubMed]
- Watson, M.; Greer, S.; Young, J.; Inayat, Q.; Burgess, C.; Robertson, B. Development of a questionnaire measure of adjustment to cancer: The MAC scale. Psychol. Med. 1988, 18, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Caron, J. L’Échelle de provisions sociales: Une validation québécoise. Santé Ment. Au Québec 1996, 21, 158–180. [Google Scholar] [CrossRef]
- Cutrona, C.E.; Russell, D.W. The provisions of social relationships and adaptation to stress. Adv. Pers. Relatsh. 1987, 1, 37–67. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Bellinghausen, L.; Collange, J.; Botella, M.; Emery, J.L.; Albert, É. Validation factorielle de l’échelle française de stress perçu en milieu professionnel. Santé Publique 2009, 21, 365–373. [Google Scholar] [CrossRef]
- Jutras, S. L’IPAH, version canadienne-française de l’Échelle de Levenson mesurant le lieu de contrôle tridimensionnel. Can. J. Behav. Sci./Rev. Can. Des Sci. Du Comport. 1987, 19, 74. [Google Scholar] [CrossRef]
- Levenson, H. Multidimensional locus of control in psychiatric patients. J. Consult. Clin. Psychol. 1973, 41, 397–404. [Google Scholar] [CrossRef]
- Gandek, B.; Ware, J.E.; Aaronson, N.K.; Apolone, G.; Bjorner, J.B.; Brazier, J.E.; Bullinger, M.; Kaasa, S.; Leplege, A.; Prieto, L.; et al. Cross-validation of item selection and scoring for the sf-12 health survey in nine countries: Results from the iqola project. International quality of life assessment. J. Clin. Epidemiol. 1998, 51, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Dambrun, M.; Ricard, M.; Després, G.; Drelon, E.; Gibelin, E.; Gibelin, M.; Loubeyre, M.; Py, D.; Delpy, A.; Garibbo, C.; et al. Measuring happiness: From fluctuating happiness to authentic–durable happiness. Front. Psychol. 2012, 3, 16. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Huska, J.A.; Keane, T.M. The PTSD Checklist (PCL): Reliability, Validity, and Diagnostic Utility; Annual Convention of the International Society for Traumatic Stress Studies: San Antonio, TX, USA, 1993; Volume 462. [Google Scholar]
- Yao, S.-N.; Cottraux, J.; Note, I.; De Mey-Guillard, C.; Mollard, E.; Ventureyra, V. Evaluation of Post-traumatic Stress Disorder: Validation of a measure, the PCLS. L’Encephale 2003, 29 Pt 1, 232–238. [Google Scholar]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Guihard, G.; Morice-Ramat, A.; Deumier, L.; Goronflot, L.; Alliot-Licht, B.; Bouton-Kelly, L. Évaluer la résilience des étudiants en santé en France: Adaptation et mesure de l’invariance de l’échelle CD-RISC 10. Mes. Eval. En Educ. 2018, 41, 67–96. [Google Scholar] [CrossRef]
- Krueger, J.I.; Heck, P.R. Putting the P-Value in its Place. Am. Stat. 2019, 73, 122–128. [Google Scholar] [CrossRef]
- Zhou, E.S.; Penedo, F.J.; Bustillo, N.E.; Benedict, C.; Rasheed, M.; Lechner, S.; Soloway, M.; Kava, B.R.; Schneiderman, N.; Antoni, M.H. Longitudinal effects of social support and adaptive coping on the emotional well-being of survivors of localized prostate cancer. J. Support. Oncol. 2010, 8, 196–201. [Google Scholar] [CrossRef]
- Kvillemo, P.; Bränström, R. Coping with breast cancer: A meta-analysis. PLoS ONE 2014, 9, e112733. [Google Scholar] [CrossRef]
- Fang, C.Y.; Daly, M.B.; Miller, S.M.; Zerr, T.; Malick, J.; Engstrom, P. Coping with ovarian cancer risk: The moderating effects of perceived control on coping and adjustment. Br. J. Health Psychol. 2006, 11, 561–580. [Google Scholar] [CrossRef]
- Braamse, A.M.J.; Gerrits, M.M.J.G.; van Meijel, B.; Visser, O.; van Oppen, P.; Boenink, A.D.; Cuijpers, P.; Huijgens, P.C.; Beekman, A.T.F.; Dekker, J. Predictors of health-related quality of life in patients treated with auto- and allo-SCT for hematological malignancies. Bone Marrow Transpl. 2012, 47, 757–769. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, A.; Sauerland, C.; Silling, G.; Berdel, W.E.; Stelljes, M. Resilience in patients after allogeneic stem cell transplantation. Support. Care Cancer 2014, 22, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Amonoo, H.L.; Brown, L.A.; Scheu, C.F.; Millstein, R.A.; Pirl, W.F.; Vitagliano, H.L.; Antin, J.H.; Huffman, J.C. Positive psychological experiences in allogeneic hematopoietic stem cell transplantation. Psycho-Oncology 2019, 28, 1633–1639. [Google Scholar] [CrossRef] [PubMed]
- Nipp, R.D.; El-Jawahri, A.; Fishbein, J.N.; Eusebio, J.; Stagl, J.M.; Gallagher, E.R.; Park, E.R.; Jackson, V.A.; Pirl, W.F.; Greer, J.A.; et al. The relationship between coping strategies, quality of life, and mood in patients with incurable cancer. Cancer 2016, 122, 2110–2116. [Google Scholar] [CrossRef] [PubMed]
- Hack, T.F.; Degner, L.F. Coping responses following breast cancer diagnosis predict psychological adjustment three years later. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2003, 13, 235–247. [Google Scholar] [CrossRef]
- Cousson-Gélie, F. How do patients cope with cancer? The latest advances in cancer coping strategies and the cognitive models that underlie them. Rev. Neuropsychol. 2019, 11, 289–293. [Google Scholar]
- Folkman, S. The case for positive emotions in the stress process. Anxiety Stress. Coping 2008, 21, 3–14. [Google Scholar] [CrossRef]
- Kangas, M.; Henry, J.L.; Bryant, R.A. Correlates of acute stress disorder in cancer patients. J. Trauma. Stress Off. Publ. Int. Soc. Trauma. Stress Stud. 2007, 20, 325–334. [Google Scholar] [CrossRef]
- Kim, S.-D.; Kim, H.-S. Effects of a relaxation breathing exercise on anxiety, depression, and leukocyte in hemopoietic stem cell transplantation patients. Cancer Nurs. 2005, 28, 79–83. [Google Scholar] [CrossRef]
- Hoyt, M.A.; Stanton, A.L.; Irwin, M.R.; Thomas, K.S. Cancer-related masculine threat, emotional approach coping, and physical functioning following treatment for prostate cancer. Health Psychol. 2013, 32, 66–74. [Google Scholar] [CrossRef]
- Karekla, M.; Panayiotou, G. Coping and experiential avoidance: Unique or overlapping constructs? J. Behav. Ther. Exp. Psychiatry 2011, 42, 163–170. [Google Scholar] [CrossRef]
- Casellas-Grau, A.; Font, A.; Vives, J. Positive psychology interventions in breast cancer. A systematic review. Psycho-Oncology 2014, 23, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Feros, D.L.; Lane, L.; Ciarrochi, J.; Blackledge, J.T. Acceptance and Commitment Therapy (ACT) for improving the lives of cancer patients: A preliminary study. Psycho-Oncology 2013, 22, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Grossman, P.; Zwahlen, D.; Halter, J.P.; Passweg, J.R.; Steiner, C.; Kiss, A. A mindfulness-based program for improving quality of life among hematopoietic stem cell transplantation survivors: Feasibility and preliminary findings. Support. Care Cancer 2015, 23, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, C.; Casellas-Grau, A.; Vives, J.; Font, A.; Borràs, J.-M. Positive psychotherapy for distressed cancer survivors: Posttraumatic growth facilitation reduces posttraumatic stress. Int. J. Clin. Health Psychol. 2016, 17, 28–37. [Google Scholar] [CrossRef]
- Amonoo, H.L.; Massey, C.N.; Freedman, M.E.; El-Jawahri, A.; Vitagliano, H.L.; Pirl, W.F.; Huffman, J.C. Psychological considerations in hematopoietic stem cell transplantation. Psychosomatics 2019, 60, 331–342. [Google Scholar] [CrossRef]


{kind=link}
| % (Excluding Missing Values) | Mean (SD) | n | |
|---|---|---|---|
| Controlled socio demographic variables Age | 52.03 (13.28) | 217 | |
| Sex (women) | 42.7 | 221 | |
| Marital Status (married) | 46.4 | 181 | |
| Educational Level (post-graduate) | 46.3 | 175 | |
| Socioprofessional Category (employed) | 69.6 | 151 | |
| Follow-up (in months) Controlled medical variables | 6.58 (4.04) | ||
| Disease Status Acute Leukemia Myelodysplastic Syndrome Myeloproliferative Neoplasia Non Hodgkin Lymphoma | 36 17.4 10.1 11.8 | 178 | |
| Alcohol consumption (yes) Smoking (yes) Physical Activity (yes) Body Mass Index Sleeping hours Number of transplantations Latency between disease diagnostic and transplantation (in years) Myeloablative conditioning Chronic GvHD Donor type Identical sibling Mismatched unrelated Mismatched relative Matched unrelated Unrelated Matched other relative | 30.8 15.8 45.3 25.8 16.5 25.7 8.9 12.8 38 14 0.6 | 24.92 (4.61) 7.42 (1.15) 1.07 (0.3) 2.61 (4.41) | 172 177 172 176 161 178 178 178 164 179 |
| Dependant Medical Variables | |||
| Latency engrafment (in days) | 20.24 (6.95) | 161 | |
| Acute GvHD Relapse Number of infections Death | 51.5 14.8 16.4 | 2.14 (1.8) | 171 162 170 177 |
| SPS-R | PSS | IPC Internality | IPC Externality | FS | H/H | A | A/P | D | |
|---|---|---|---|---|---|---|---|---|---|
| Social Provisions Scale-Revised (SPS-R) | - | −0.22 ** | 0.14 | −0.19 * | −0.30 *** | −0.41 *** | −0.19 * | −0.28 *** | −0.23 ** |
| Perceived Stress Scale (PSS) | - | 0.01 | 0.34 *** | −0.46 *** | 0.57 *** | 0.04 | 0.60 *** | 0.08 | |
| IPC internality | - | 0.23 ** | 0.24 ** | 0.01 | 0.08 | 0.08 | −0.02 | ||
| IPC externality | - | −0.15 | 0.43 *** | 0.29 *** | 0.47 *** | 0.27 *** | |||
| Fighting Spirit (FS) | - | −0.47 *** | 0.10 | −0.29 *** | 0.04 | ||||
| Hopelessness/ Helplessness (H/H) | - | 0.14 | 0.61 *** | 0.21 * | |||||
| Avoidance (A) | - | 0.32 *** | 0.46 *** | ||||||
| Anxious Preoccupations (A/P) | - | 0.29 *** |
| Fighting Spirit | Hopelessness/Helplessness | Avoidance | Anxious Preoccupations | Denial | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Z-O | Adjusted β | Z-O | Adjusted β | Z-O | Adjusted β | Z-O | Adjusted β | Z-O | Adjusted β | |
| Health Outcomes: | ||||||||||
| Mental QoL a | 0.20 | - | −0.35 ** | 0.01 | −0.15 | - | −0.52 *** | −0.42 ** | −0.14 | - |
| Anxiety b | −0.27 * | −0.01 | 0.46 *** | −0.04 | −0.02 | - | 0.62 *** | 0.34 * | 0.16 | - |
| Depression c | −0.30 * | 0.10 | 0.34 ** | 0.10 | −0.06 | - | 0.35 ** | 0.07 | 0.11 | - |
| Happiness d | 0.53 *** | 0.19 + | −0.45 *** | 0.04 | 0.05 | - | −0.47 *** | −0.17 | 0.07 | - |
| PTSD a | −0.06 | - | 0.30 * | −0.25 + | 0.08 | - | 0.59 *** | 0.72 *** | 0.20 | - |
| Resilience a | 0.40 *** | 0.33 * | −0.36 ** | −0.16 | −0.08 | - | −0.34 ** | −0.05 | −0.22 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corman, M.; Dambrun, M.; Rubio, M.-T.; Cabrespine, A.; Brindel, I.; Bay, J.-O.; Peffault de La Tour, R. The Prospective Effects of Coping Strategies on Mental Health and Resilience at Five Months after HSCT. Healthcare 2023, 11, 1975. https://doi.org/10.3390/healthcare11131975
Corman M, Dambrun M, Rubio M-T, Cabrespine A, Brindel I, Bay J-O, Peffault de La Tour R. The Prospective Effects of Coping Strategies on Mental Health and Resilience at Five Months after HSCT. Healthcare. 2023; 11(13):1975. https://doi.org/10.3390/healthcare11131975
Chicago/Turabian StyleCorman, Maya, Michael Dambrun, Marie-Thérèse Rubio, Aurélie Cabrespine, Isabelle Brindel, Jacques-Olivier Bay, and Régis Peffault de La Tour. 2023. "The Prospective Effects of Coping Strategies on Mental Health and Resilience at Five Months after HSCT" Healthcare 11, no. 13: 1975. https://doi.org/10.3390/healthcare11131975
APA StyleCorman, M., Dambrun, M., Rubio, M.-T., Cabrespine, A., Brindel, I., Bay, J.-O., & Peffault de La Tour, R. (2023). The Prospective Effects of Coping Strategies on Mental Health and Resilience at Five Months after HSCT. Healthcare, 11(13), 1975. https://doi.org/10.3390/healthcare11131975