

Effects of Psychotherapy on the Problem Behaviors of Humidifier Disinfectant Survivors: The Role of Individual Characteristics and Adaptive Functioning


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Treatment
2.3. Measures
2.3.1. Problem Behavior Scale
2.3.2. Adaptive Functioning Scale
2.4. Data Analysis
3. Results
3.1. Mean Differences in Problem Behavior Scores
3.2. Treatment Effects and Interaction with the Demographic and Life Functioning Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Park, H.S.; Kwon, S.Y. A study on the life experiences of family of social disaster victim: Focusing on spouse of victim of humidifier disinfectants. Korean Assoc. Christ. Counsel. Psychol. 2020, 31, 175–221. [Google Scholar] [CrossRef]
- Kim, J. Life after “Humidifier Disinfectant”: Parents’ Becoming Victims in a Risk Society. Master’s Thesis, Seoul National University, Seoul, Republic of Korea, 2018. Available online: https://hdl.handle.net/10371/142138 (accessed on 1 February 2023).
- Choi, J.E.; Hong, S.B.; Do, K.H.; Kim, H.J.; Chung, S.; Lee, E.; Choi, J.; Hong, S.J. Humidifier disinfectant lung injury, how do we approach the issues? Environ. Health Toxicol. 2016, 31, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Seo, J.H.; Kim, H.Y.; Yu, J.; Jhang, W.K.; Park, S.J.; Kwon, J.W.; Kim, B.J.; Do, K.H.; Cho, Y.A.; et al. Toxic inhalational injury-associated interstitial lung disease in children. J. Korean Med. Sci. 2013, 28, 915–923. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, M.S.; Hong, S.B.; Huh, J.W.; Do, K.H.; Jang, S.J.; Lim, C.M.; Chae, E.J.; Lee, H.; Jung, M.; et al. A cluster of lung injury cases associated with home humidifier use: An epidemiological investigation. Thorax 2014, 69, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Park, D.U.; Lee, S.; Lim, H.K.; Kim, S.Y.; Kim, J.; Park, J.; Zoh, K.E. Comprehensive review on humidifier disinfectant (HD) products, focusing on the number of products and their disinfectant type. J. Environ. Health Sci. 2020, 46, 481–494. [Google Scholar] [CrossRef]
- Choi, Y.; Lee, I. A comparative study of the humidifier disinfectant disaster and Minamata disease. J. Environ. Health Sci. 2019, 45, 326–339. [Google Scholar] [CrossRef]
- Yoon, J.; Cho, H.J.; Lee, E.; Choi, Y.J.; Kim, Y.H.; Lee, J.L.; Lee, Y.J.; Hong, S.J. Rate of humidifier and humidifier disinfectant usage in Korean children: A nationwide epidemiologic study. Environ. Res. 2017, 155, 60–63. [Google Scholar] [CrossRef]
- Yoon, J.; Kang, M.; Jung, J.; Ju, M.J.; Jeong, S.H.; Yang, W.; Choi, Y.H. Humidifier disinfectant consumption and humidifier disinfectant-associated lung injury in South Korea: A nationwide population-based study. Int. J. Environ. Res. Public Health 2021, 18, 6136. [Google Scholar] [CrossRef]
- Park, J.H.; Ko, M.H. A Study on the Damage Relief in Humidifier Sterilizer Case—Focused on Expanding the Role of Epidemiological Causality for Presumption of Causal Relationship. Law J. 2020, 48, 265–306. [Google Scholar] [CrossRef]
- Ryu, S.H.; Park, D.U.; Lee, E.; Park, S.; Lee, S.Y.; Jung, S. Humidifier disinfectant and use characteristics associated with lung injury in Korea. Indoor Air 2019, 29, 735–747. [Google Scholar] [CrossRef]
- Jeon, B.H.; Park, Y.J. Frequency of humidifier and humidifier disinfectant usage Gyeonggi provine. Environ. Health Toxicol. 2012, 27, e2012002. [Google Scholar] [CrossRef]
- Chang, M.H.; Park, H.; Ha, M.; Kim, Y.; Hong, Y.C.; Ha, E.H. Characteristics of humidifier use in Korean pregnant women: The Mothers and Children’s Environmental Health (MOCEH) study. Environ. Health Toxicol. 2012, 27, 123–137. [Google Scholar] [CrossRef]
- Choi, Y.; Ryu, H.; Yoon, J.; Lee, S.; Kwak, J.; Han, B.; Chu, Y.H.; Kim, P.G.; Yang, W. Demographic Characteristics and Exposure Assessment for Applicants Who Have Been Injured by Humidifier Disinfectant: Focusing on 4-1 and 4-2 Applicants. J. Korean Soc. Environ. Health 2018, 44, 301–314. [Google Scholar] [CrossRef]
- Yoo, S.; Sim, M.; Choi, J.; Jeon, K.; Shin, J.; Chung, S.; Hong, S.B.; Lee, S.Y.; Hong, S.J. Psychological responses among humidifier disinfectant disaster victims and their families. J. Korean Med. Sci. 2019, 34, e29. [Google Scholar] [CrossRef] [PubMed]
- Leem, J.H.; Joh, J.S.; Hong, Y.S.; Kim, J.; Park, S.; Lim, S.; Kim, Y. Characteristics of a new respiratory syndrome associated with the use of a humidifier disinfectant: Humidifier disinfectant-related respiratory syndrome (HDRS). Int. J. Occup. Med. Environ. Health 2020, 33, 829–839. [Google Scholar] [CrossRef]
- Ko, H.-Y.; Ryu, S.-H.; Lee, M.-J.; Lee, H.-J.; Kwon, S.-Y.; Kim, S.-M.; Lee, S.-M. Exploring Socio-Demographic Factors Affecting Psychological Symptoms in Humidifier Disinfectant Survivors. Int. J. Environ. Res. Public Health 2021, 18, 11811. [Google Scholar] [CrossRef] [PubMed]
- Matliwala, K. The effect of psychological counseling on mental health. J. Psychol. Clin. Psychiatry 2017, 7, 4–36. [Google Scholar] [CrossRef][Green Version]
- Shea, M.T.; Stout, R.L.; Reddy, M.K.; Sevin, E.; Presseau, C.; Lambert, J.; Cameron, A. Treatment of anger problems in previously deployed post-911 veterans: A randomized controlled trial. Depress. Anxiety 2022, 39, 274–285. [Google Scholar] [CrossRef]
- Howard, K.I.; Kopta, S.M.; Krause, M.S.; Orlinsky, D.E. The dose–effect relationship in psychotherapy. Am. Psychol. 1986, 41, 159–164. [Google Scholar] [CrossRef]
- Cuijpers, P.; Karyotaki, E.; Reijnders, M.; Ebert, D.D. Was Eysenck right after all? A reassessment of the effects of psychotherapy for adult depression. Epidemiol. Psychiatr. Sci. 2019, 28, 21–30. [Google Scholar] [CrossRef]
- Wang, M.-C.; Nyutu, P.; Tran, K.; Spears, A. Finding resilience: The mediation effect of sense of community on the psychological well-being of military spouses. J. Ment. Health Couns. 2015, 37, 164–174. [Google Scholar] [CrossRef]
- Humphreys, K.; Mankowski, E.S.; Moos, R.H.; Finney, J.W. Do enhanced friendship networks and active coping mediate the effect of self-help groups on substance abuse? Ann. Behav. Med. 1999, 21, 54–60. [Google Scholar] [CrossRef]
- Miller, S.D.; Duncan, B.L. The Outcome and Session Rating Scales: Administration and Scoring Manuals; Institute for the Study of Therapeutic Change: Chicago, IL, USA, 2004. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Adult Forms & Profiles; ASEBA: Burlington, VT, USA, 2003. [Google Scholar]
- Kim, M.Y.; Kim, Y.A.; Lee, J.; Kim, H.J.; Oh, K.J. A Validity Study on the Korean Version of the Adult Self Report. Korean J. Clin. Psychol. 2014, 33, 615–632. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA School-Age Forms & Profiles; ASEBA: Burlington, VT, USA, 2001. [Google Scholar]
- Mann, H.B.; Whitney, D.R. On a test of whether one of two random variables is stochastically larger than the other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Norman, B. A generalized Kruskal-Wallis test for comparing K samples subject to unequal patterns of censorship. Biometrika 1970, 57, 579–594. [Google Scholar] [CrossRef]
- Wilcoxon, F. Individual comparisons by ranking methods. Biometrics 1945, 1, 80–83. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Science, 2nd ed.; Routledge: New York, NY, USA, 1988; pp. 25–27. [Google Scholar]
- McGraw, A.P.; Mellers, B.A.; Tetlock, P.E. Expectations and emotions of Olympic athletes. J. Exp. Soc. Psychol. 2005, 41, 438–446. [Google Scholar] [CrossRef]
- Ford, M.T.; Cerasoli, C.P.; Higgins, J.A.; Decesare, A.L. Relationships between psychological, physical, and behavioural health and work performance: A review and meta-analysis. Work Stress 2011, 25, 185–204. [Google Scholar] [CrossRef]
- Brooks, S.K.; Dunn, R.; Amlôt, R.; Rubin, G.J.; Greenberg, N. Social and occupational factors associated with psychological wellbeing among occupational groups affected by disaster: A systematic review. J. Ment. Health 2017, 26, 373–384. [Google Scholar] [CrossRef]
- Lee, M.J.; Lee, H.J.; Ko, H.; Ryu, S.H.; Lee, S.M. Multi-layer relationships between psychological symptoms and life adaptation among humidifier disinfectant survivors. Front. Psychiatry 2022, 13, 890122. [Google Scholar] [CrossRef]
- Wiseman, T.; Foster, K.; Curtis, K. Mental health following traumatic physical injury: An integrative literature review. Injury 2013, 44, 1383–1390. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, S.W.; Kim, J.M. The Impact of Community Disaster Trauma: A Focus on Emerging Research of PTSD and Other Mental Health Outcomes. Chonnam Med. J. 2020, 56, 99–107. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.L.; Lau, W.; Fredrickson, J.; Gibson, K.; Bryant, R.A.; Bisson, J.; Burke, S.; Busuttil, W.; Coghlan, A.; Creamer, M.; et al. An open label pilot study of a brief psychosocial intervention for disaster and trauma survivors. Front. Psychiatry 2020, 11, 483. [Google Scholar] [CrossRef] [PubMed]
- Levers, L.L. An introduction to counseling survivors of trauma: Beginning to understand the historical and psychosocial implications of trauma, stress, crisis, and disaster. In Trauma Counseling; Springer Publishing Company: New York, NY, USA, 2022. [Google Scholar] [CrossRef]
- Norris, F.H.; Friedman, M.J.; Watson, P.J. 60,000 disaster victims speak: Part II. Summary and implications of the Disaster Mental Health Research. Psychiatry Interpers. Biol. Process. 2002, 65, 240–260. [Google Scholar] [CrossRef]
- Kaniasty, K. Predicting social psychological well-being following trauma: The role of postdisaster social support. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 22–33. [Google Scholar] [CrossRef]
- Watson, P.J.; Brymer, M.J.; Bonanno, G.A. Postdisaster psychological intervention since 9/11. Am. Psychol. 2011, 66, 482–494. [Google Scholar] [CrossRef]
- Stellman, J.M.; Smith, R.P.; Katz, C.L.; Sharma, V.; Charney, D.S.; Herbert, R.; Moline, J.; Luft, B.J.; Markowitz, S.; Udasin, I.; et al. Enduring mental health morbidity and social function impairment in world trade center rescue, recovery, and cleanup workers: The psychological dimension of an environmental health disaster. Environ. Health Perspect. 2008, 116, 1248–1253. [Google Scholar] [CrossRef]
- Lê, F.; Tracy, M.; Norris, F.H.; Galea, S. Displacement, County Social Cohesion, and Depression After a Large-Scale Traumatic Event. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1729–1741. [Google Scholar] [CrossRef]
- Huang, Y.; Wong, H. Impacts of Sense of Community and Satisfaction with Governmental Recovery on Psychological Status of the Wenchuan Earthquake Survivors. Soc. Indic. Res. 2014, 117, 421–436. [Google Scholar] [CrossRef]
- Manesi, Z.; Van Lange, P.A.; Van Doesum, N.J.; Pollet, T.V. What Are the Most Powerful Predictors of Charitable Giving to Victims of Typhoon Haiyan: Prosocial Traits, Socio-Demographic Variables, or Eye Cues? Personal. Individ. Differ. 2019, 146, 217–225. [Google Scholar] [CrossRef]
- Guilaran, J.; de Terte, I.; Kaniasty, K.; Stephens, C. Psychological Outcomes in Disaster Responders: A Systematic Review and Meta-Analysis on the Effect of Social Support. Int. J. Disaster Risk Sci. 2018, 9, 344–358. [Google Scholar] [CrossRef]
- Strine, T.W.; Kroenke, K.; Dhingra, S.; Balluz, L.S.; Gonzalez, O.; Berry, J.T.; Mokdad, A.H. The associations between depression, health-related quality of life, social support, life satisfaction, and disability in community-dwelling US adults. J. Nerv. Ment. Dis. 2009, 197, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Young, K.W. Social support and life satisfaction. Int. J. Psychosoc. Rehabil. 2005, 10, 155–164. [Google Scholar]
- Helliwell, J.F.; Layard, R.; Sachs, J.D.; Neve, J.E.D. World Happiness Report 2021; Sustainable Development Solutions Network: New York, NY, USA, 2021. [Google Scholar]


{kind=link}
| Variable | n | Pre-Test | Post-Test | Cohen’d | |||
|---|---|---|---|---|---|---|---|
| M(SD) | Md(IQR) | M(SD) | Md(IQR) | ||||
| Compensation Presence | With Compensation | 26 | 63.77(17.138) | 59.50(52.75–80.75) | 57.88(12.854) | 55.00(49.50–65.25) | 0.39 |
| Without Compensation | 43 | 61.81(13.512) | 60.00(52.75–80.75) | 58.53(15.906) | 54.00(45.00–66.00) | 0.22 | |
| Compensation Subject | Self | 44 | 64.36(14.989) | 61.50(55.00–71.25) | 60.86(15.200) | 58.50(49.25–67.75) | 0.23 |
| Family member | 25 | 59.36(14.454) | 57.00(49.50–66.50) | 53.76(12.950) | 52.00(43.50–62.50) | 0.41 | |
| Gender | Male | 31 | 59.65(16.390) | 58.00(48.00–68.00) | 54.97(12.828) | 52.00(44.00–65.00) | 0.32 |
| Female | 38 | 64.92(13.294) | 60.50(56.75–69.75) | 61.00(15.774) | 55.50(50.75–70.50) | 0.27 | |
| Age | Under 19 | 12 | 54.92(9.885) | 57.00(48.50–63.50) | 48.17(8.100) | 45.00(42.00–53.75) | 0.75 |
| 20 to 39 | 15 | 62.47(15.793) | 58.00(49.00–79.00) | 57.07(13.956) | 52.00(47.00–65.00) | 0.36 | |
| 40 to 59 | 42 | 64.76(15.303) | 62.50(54.75–72.75) | 61.62(15.300) | 61.50(50.75–68.50) | 0.21 | |
| SES | High | 38 | 67.50(15.866) | 63.50(57.00–86.25) | 61.05(16.319) | 59.00(50.00–68.75) | 0.40 |
| Middle | 24 | 56.46(11.077) | 56.00(49.00–62.75) | 55.83(12.345) | 54.50(45.00–62.00) | 0.053 | |
| Low | 7 | 56.57(12.012) | 55.00(48.00–63.00) | 51.71(10.547) | 47.00(43.00–65.00) | 0.43 | |
| Life functioning | High | 28 | 54.50(12.816) | 53.50(47.25–61.75) | 53.64(14.952) | 50.50(42.24–61.75) | 0.062 |
| Low | 41 | 68.05(13.769) | 63.00 (57.00–82.50) | 61.46(13.884) | 59.00(51.50–68.00) | 0.48 | |
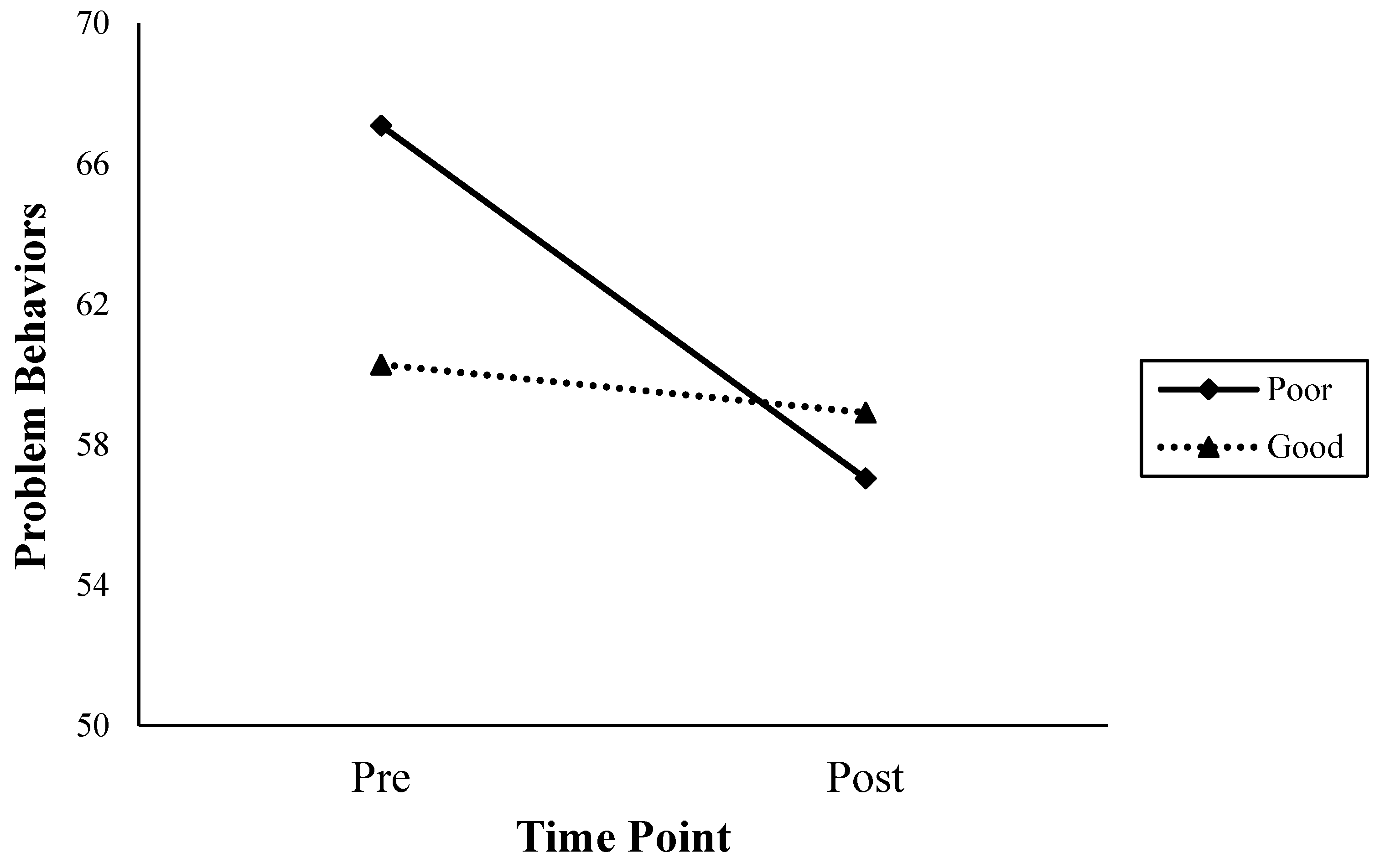
| Friendship | Good | 35 | 60.28(15.156) | 57.00(48.00–63.00) | 58.91(16.220) | 55.00(43.00–65.00) | 0.087 |
| Poor | 34 | 67.09(13.527) | 63.00(57.00–80.75) | 57.04(11.424) | 55.50(50.75–67.25) | 0.80 | |
| Family Relationship | Good | 14 | 61.07(14.143) | 53.00(47.00–62.25) | 58.98(14.455) | 50.00(43.50–63.75) | 0.15 |
| Poor | 14 | 71.36(15.174) | 59.00 (57.00–89.25) | 62.21(14.110) | 64.50(54.75–71.75) | 0.62 | |
| Job Adjustment | High | 20 | 55.60(10.713) | 57.00(49.50–60.75) | 53.50(10.511) | 54.00(44.75–63.75) | 0.20 |
| Low | 8 | 77.88(18.019) | 89.00(59.25–91.50) | 71.75(16.334) | 68.00(57.50–89.00) | 0.36 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.J.; Chung, Y.; Hong, S.; Lee, H.-J.; Park, G.; Lee, S.M. Effects of Psychotherapy on the Problem Behaviors of Humidifier Disinfectant Survivors: The Role of Individual Characteristics and Adaptive Functioning. Healthcare 2023, 11, 2179. https://doi.org/10.3390/healthcare11152179
Lee MJ, Chung Y, Hong S, Lee H-J, Park G, Lee SM. Effects of Psychotherapy on the Problem Behaviors of Humidifier Disinfectant Survivors: The Role of Individual Characteristics and Adaptive Functioning. Healthcare. 2023; 11(15):2179. https://doi.org/10.3390/healthcare11152179
Chicago/Turabian StyleLee, Min Joo, Yubin Chung, Soeun Hong, Hun-Ju Lee, Gippeum Park, and Sang Min Lee. 2023. "Effects of Psychotherapy on the Problem Behaviors of Humidifier Disinfectant Survivors: The Role of Individual Characteristics and Adaptive Functioning" Healthcare 11, no. 15: 2179. https://doi.org/10.3390/healthcare11152179
APA StyleLee, M. J., Chung, Y., Hong, S., Lee, H.-J., Park, G., & Lee, S. M. (2023). Effects of Psychotherapy on the Problem Behaviors of Humidifier Disinfectant Survivors: The Role of Individual Characteristics and Adaptive Functioning. Healthcare, 11(15), 2179. https://doi.org/10.3390/healthcare11152179