
Prevalence of Temporomandibular Disorder Symptoms Among Dental Students at the Faculty of Dental Medicine in Iași: A Self-Reported Study Based on DC/TMD Criteria

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Instruments and Measured Variables
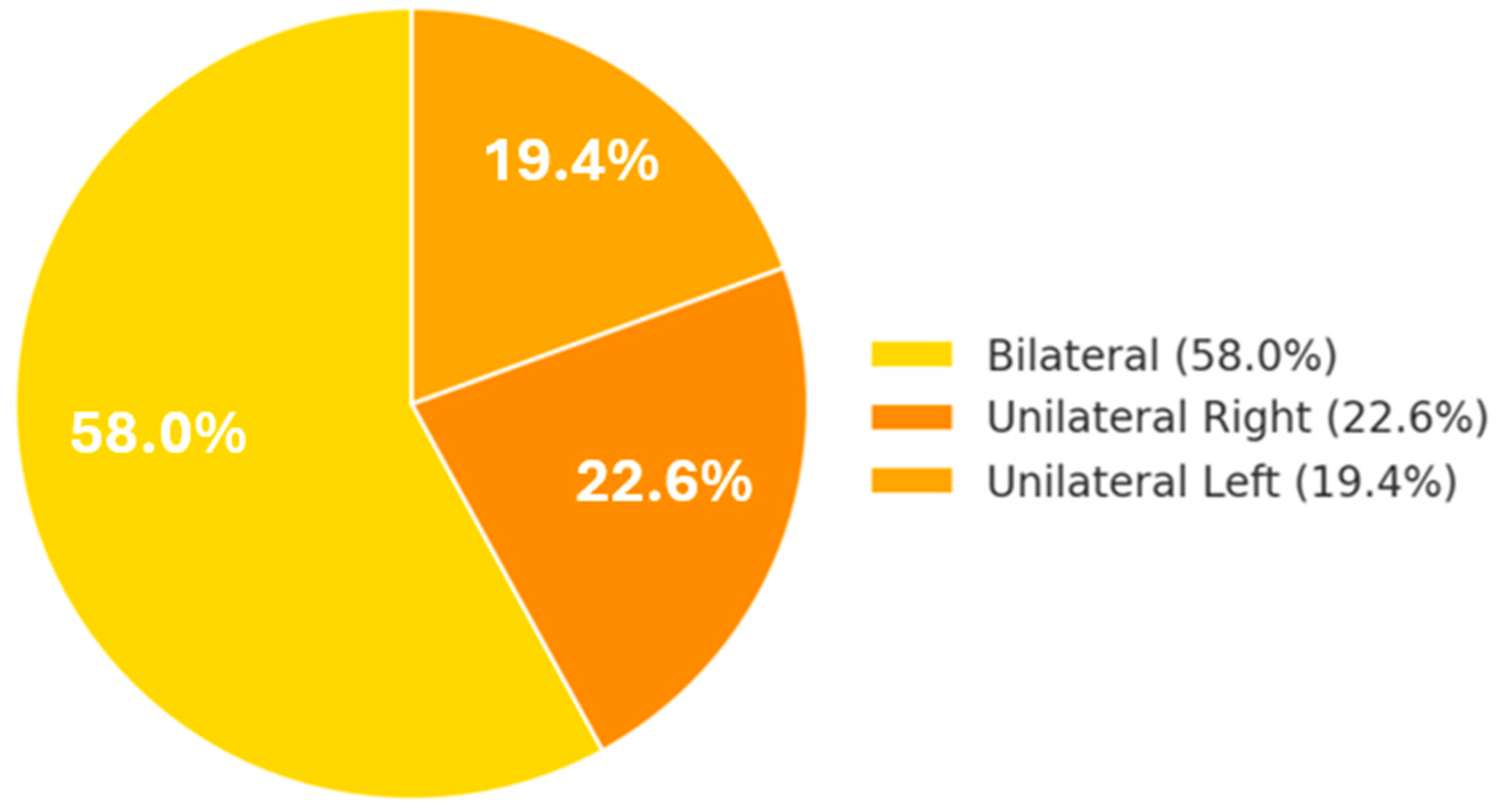
- TMD screening questions (axis I)—the presence of orofacial pain (in the jaw, temple, or ear region) in the last 30 days, pain characteristics (intermittent vs. constant), duration of symptoms (in months), laterality (unilateral/bilateral), the presence of jaw pain/stiffness upon waking, presence of pain triggered or worsened by specific activities (chewing hard foods, yawning/wide mouth opening, teeth clenching or grinding, prolonged speaking, kissing), the presence of joint noises (TMJ clicking or popping), episodes of mandibular joint locking on opening or closing (temporary inability to open the mouth fully, or open-locking—“subluxation”), interference of such locking with eating, headaches in the temporal region associated with mandibular movements. Responses were recorded as yes/no or on nominal scales describing the presence/absence of pain.
- Graded Chronic Pain Scale (GCPS, axis II)—this instrument assessed the intensity and degree of functional impairment due to facial pain. On a scale from 0 to 10, students rated current facial pain intensity (at the time of completion), the most intense pain in the past 30 days, and average pain intensity over the past 30 days. They also reported the number of days (in the past 6 months) with facial pain and the number of days in the past month when pain interfered with normal activities (work, school, and household tasks). Pain interference with daily, social/family, and work activities was rated on a scale from 0 (“not at all”) to 10 (“extremely”). These data allow the classification of subjects by chronic pain grade (0—no pain, I—mild pain, II—moderate pain, III/IV—severe pain with disability).
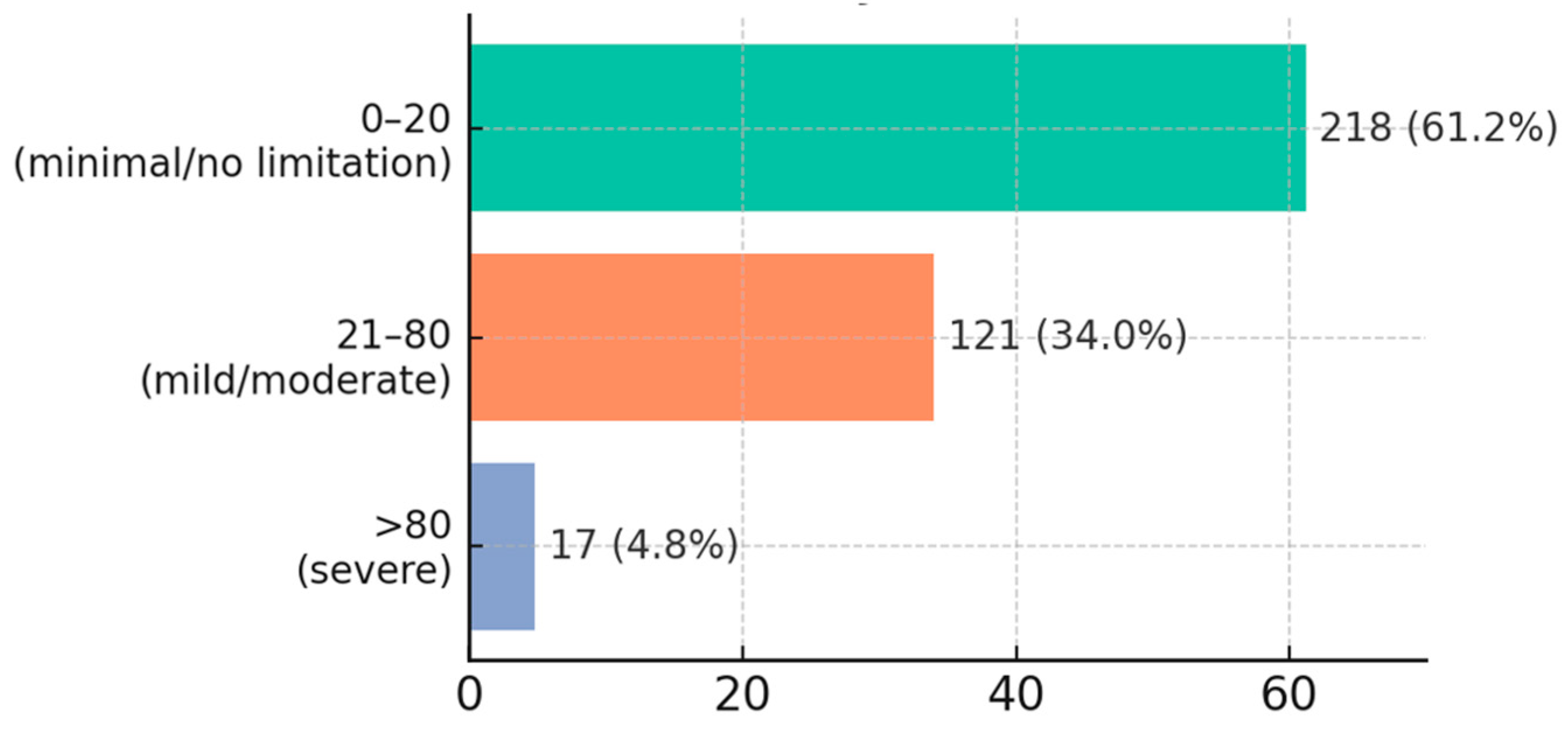
- Jaw Functional Limitation Scale (JFLS-20, axis II)—used to evaluate the impact of TMD on jaw function. The JFLS contains 20 items assessing difficulty level (0 = no difficulty, 10 = impossible) in performing various jaw-related activities. Questions cover masticatory functions (chewing foods of different consistencies, biting into foods), speech and facial expression functions (opening the mouth for speaking, yawning, singing, smiling, facial expressions), and general oral functions (swallowing, kissing). The total JFLS score (0–100) is calculated as the mean of all item scores × 10, with higher values indicating more severe functional limitation.
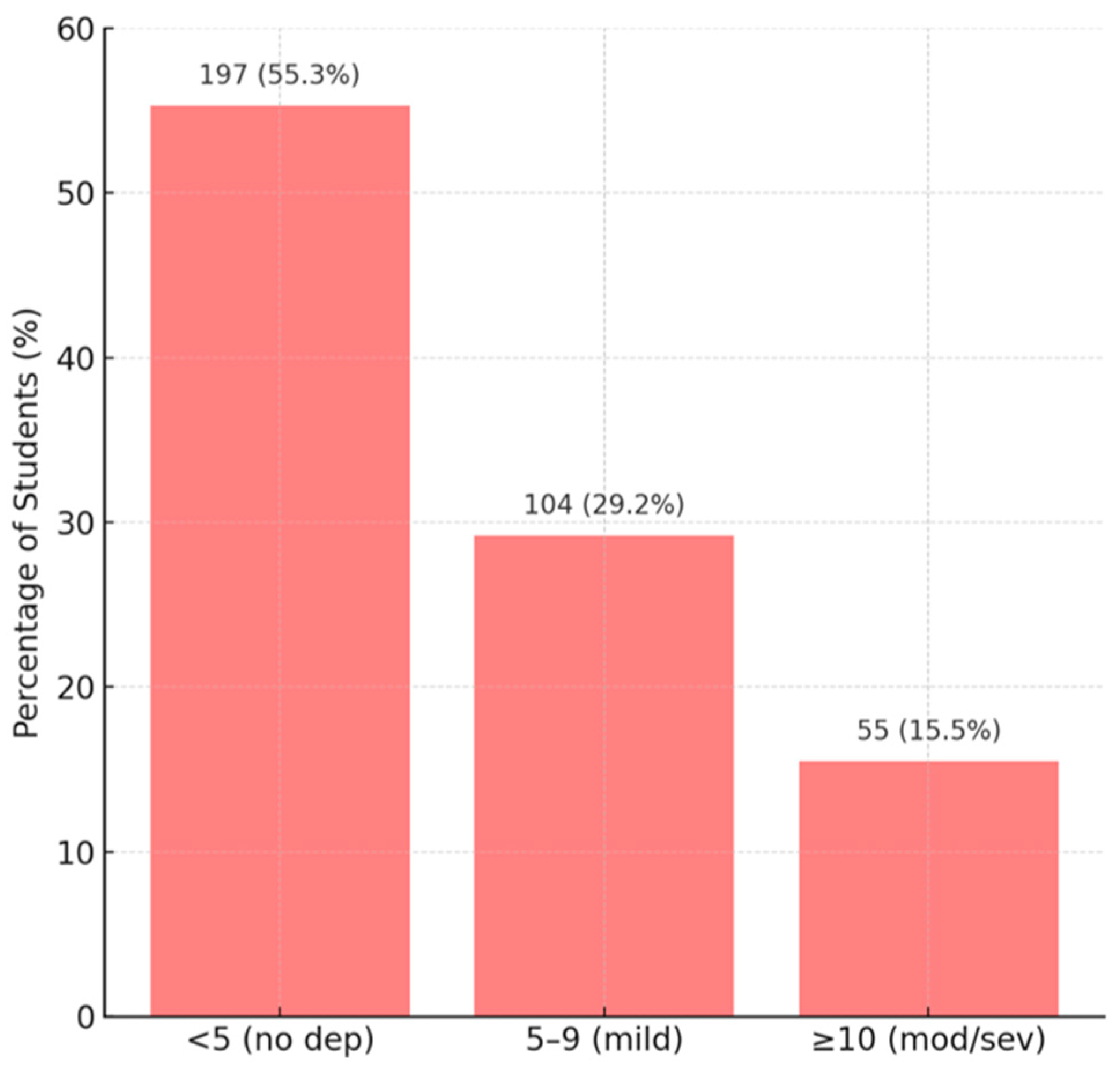
- Patient Health Questionnaire (PHQ-9)—for depressive symptoms. This standardized tool asks respondents to assess the frequency—on a scale from 0 (“not at all”) to 3 (“nearly every day”) —of 9 depression symptoms (low interest, sad mood, sleep disturbances, fatigue, appetite changes, feelings of worthlessness or guilt, concentration problems, psychomotor slowing/agitation, thoughts of death) over the past 2 weeks. The total PHQ-9 score (0–27) reflects depression severity (0–4, minimal; 5–9, mild; 10–14, moderate; ≥15, moderate–severe or severe). An additional question asked how difficult these problems made daily life (response options: “Not difficult at all,” “Somewhat difficult,” “Very difficult,” “Extremely difficult”).
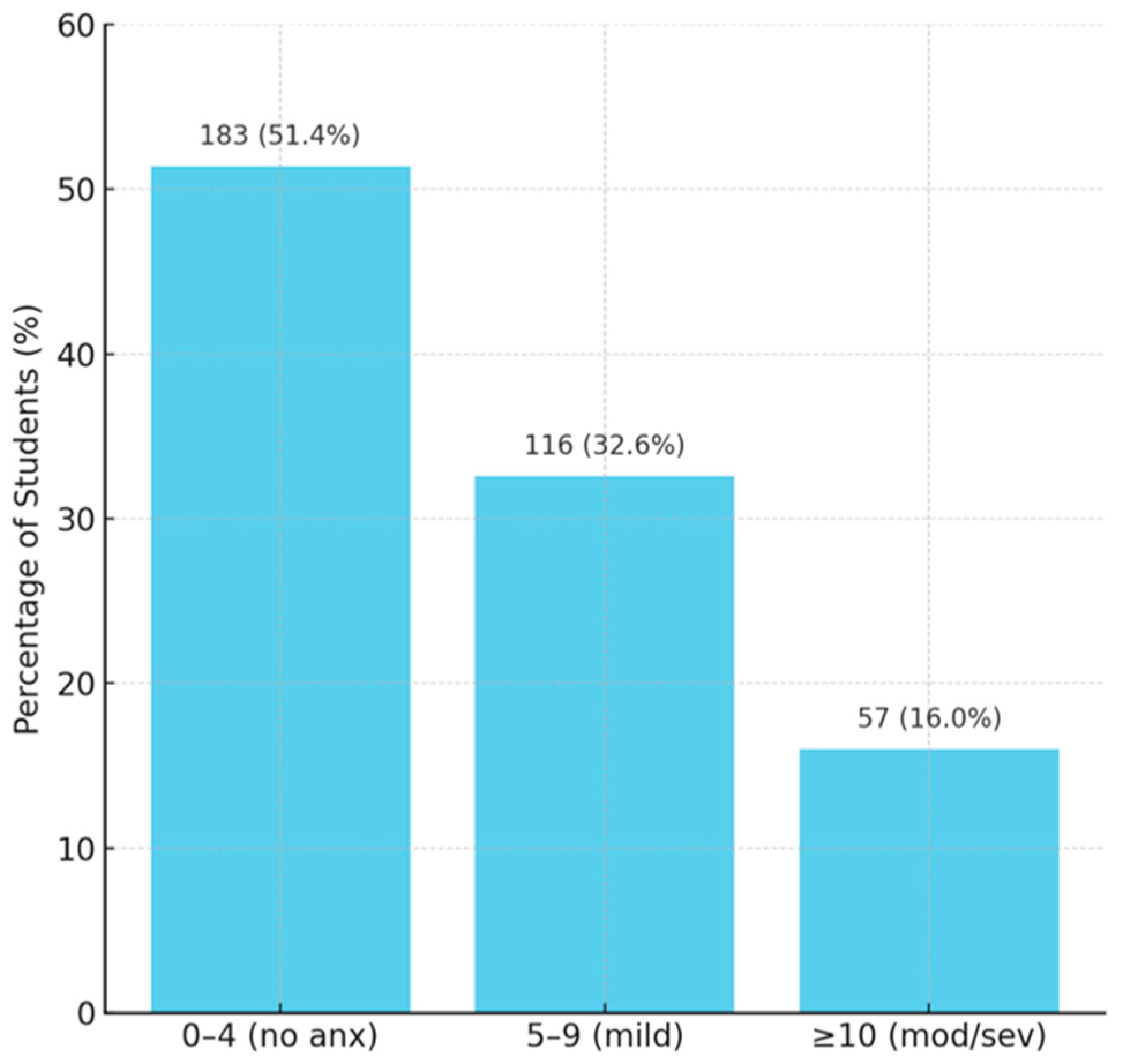
- Generalized Anxiety Disorder Questionnaire (GAD-7)—for anxiety symptoms. Like the PHQ-9, the GAD-7 assesses seven generalized anxiety symptoms (nervousness, inability to control worry, excessive worrying, difficulty relaxing, restlessness, irritability, fear of impending doom) on a 0–3 scale over the past 2 weeks. The total score (0–21) indicates anxiety severity (0–4, minimal; 5–9, mild; 10–14, moderate; ≥15, severe). At the end, participants also indicated how much these problems interfered with daily functioning (“Not difficult at all” to “Extremely difficult”).
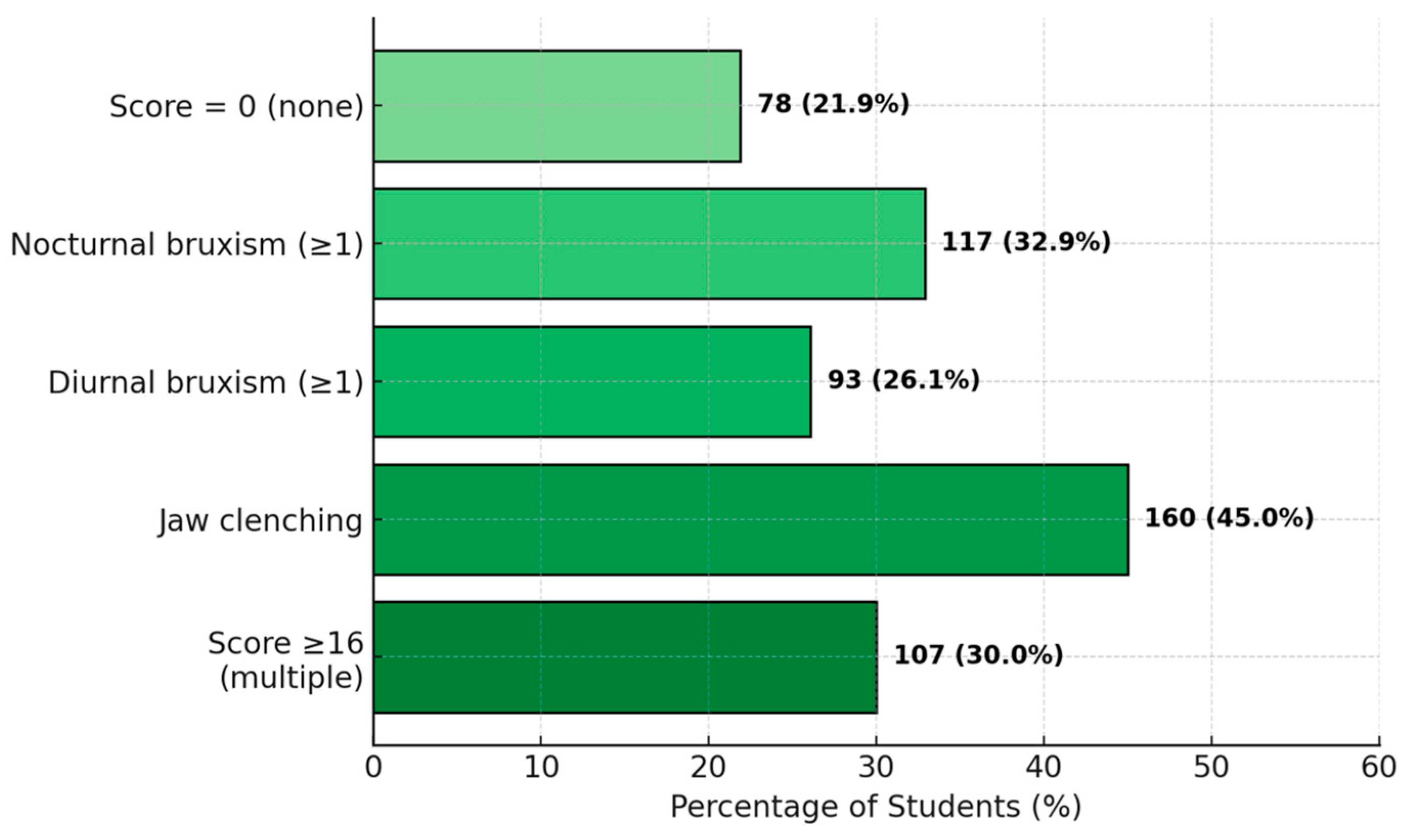
- Oral Behaviors Checklist (OBC)—a list of 18 oral parafunctional behaviors, including two related to sleep (nocturnal bruxism—teeth grinding or clenching during sleep; sleeping in positions that apply pressure to the jaw) and six related to waking hours (teeth grinding/clenching during the day; frequent tooth contact; jaw muscle tension without tooth contact; pushing or shifting the jaw to one side, etc.). Respondents rated the frequency of each habit on a scale from 0 (“never”) to 4 (“always”). A total OBC score was calculated by summing the scores of 8 key behaviors (maximum theoretical score: 32), with higher scores indicating more frequent or multiple parafunctions.
2.3. Statistical Analysis
3. Results
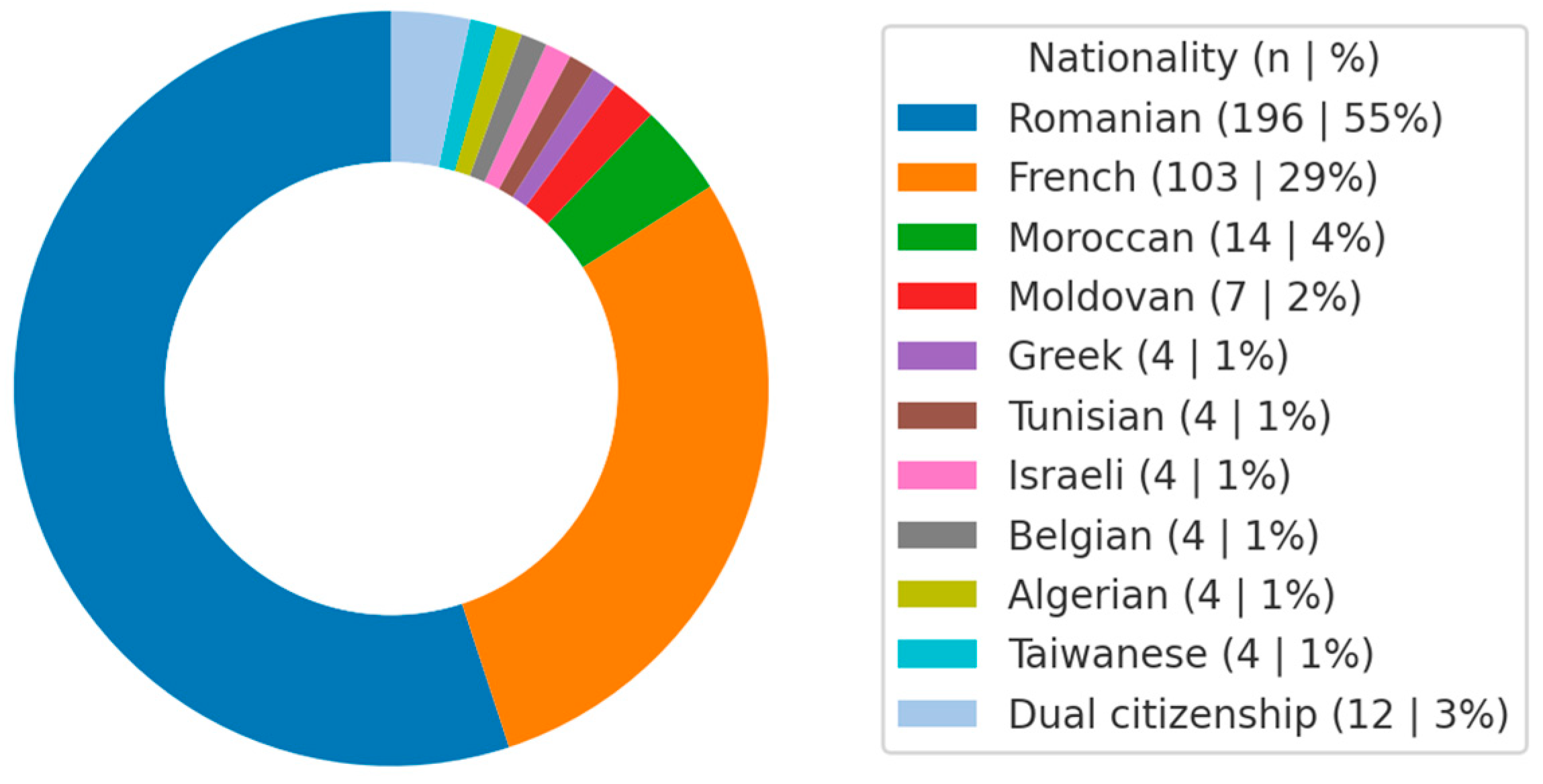
3.1. Sample Characteristics
- Score 0: 189 individuals (53%)
- Score 1: 59 individuals (17%)
- Score 2: 33 (9%)
- Score 3: 27 (8%)
- Score 4: 28 (8%)
- Score 5: 9 (2%)
- Score 6: 10 (3%)
- Score 7: 1 (0%)
3.2. Prevalence of TMD Symptoms
3.3. Detailed Descriptive Analysis of Symptoms
3.3.1. Facial Pain Intensity and Impact
3.3.2. Mandibular Functional Limitation Score (JFLS)
3.3.3. Psychosocial Scores (Axis II)
3.3.4. Associations Between Variables (χ2 Tests)
3.3.5. Differences Between Subgroups (Female vs. Male)
3.3.6. Correlations Between Clinical Variables
4. Discussion
4.1. Clinical and Preventive Implications
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TMD | Temporomandibular disorder |
| TMJ | Temporomandibular joint |
| DC/TMD | Diagnostic Criteria for Temporomandibular Disorders |
| GCPS | Graded Chronic Pain Scale |
| JFLS | Jaw Functional Limitation Scale |
| PHQ | Patient Health Questionnaire |
| GAD | Generalized anxiety disorder |
| OBC | Oral Behaviors Checklist |
| RDC/TMD | Research Diagnostic Criteria for Temporomandibular Disorders |
| CBT | Cognitive behavioral therapy |
| CT | Computed tomography |
| CBCT | Cone beam computed tomography |
| MRI | Magnetic resonance imaging |
| IQR | Interquartile range |
References
- Maixner, W.; Diatchenko, L.; Dubner, R.; Fillingim, R.B.; Greenspan, J.D.; Knott, C.; Ohrbach, R.; Weir, B.; Slade, G.D. Orofacial pain prospective evaluation and risk assessment study—The OPPERA study. J. Pain 2011, 12, T4–T11.e2. [Google Scholar] [CrossRef]
- Ohrbach, R.; Sharma, S. Temporomandibular disorders: Definition and etiology. Semin. Orthod. 2024, 30, 237–242. [Google Scholar] [CrossRef]
- De Leeuw, R.; Klasser, G.D. Orofacial pain: Guidelines for assessment, diagnosis, and management. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 171. [Google Scholar] [CrossRef]
- List, T.; Jensen, R.H. Temporomandibular disorders: Old ideas and new concepts. Cephalalgia 2017, 37, 692–704. [Google Scholar] [CrossRef]
- Wu, J.; Huang, Z.; Chen, Y.; Chen, Y.; Pan, Z.; Gu, Y. Temporomandibular disorders among medical students in China: Prevalence, biological and psychological risk factors. BMC Oral Health 2021, 21, 549. [Google Scholar] [CrossRef] [PubMed]
- Kapos, F.P.; Exposto, F.G.; Oyarzo, J.F.; Durham, J. Temporomandibular disorders: A review of current concepts in aetiology, diagnosis and management. Oral Surg. 2020, 13, 321–334. [Google Scholar] [CrossRef]
- Porporatti, A.L.; Schroder, Â.G.D.; Lebel, A.; Moreau, N.; Guillouet, C.; Stechman-Neto, J.; Boucher, Y. Prevalence of orofacial and head pain: An umbrella review of systematic reviews. J. Oral Facial Pain Headache 2024, 38, 1–14. [Google Scholar] [CrossRef]
- Ilgunas, A.; Fjellman-Wiklund, A.; Häggman-Henrikson, B.; Lobbezoo, F.; Visscher, C.M.; Durham, J.; Lövgren, A. Patients’ experiences of temporomandibular disorders and related treatment. BMC Oral Health 2023, 23, 653. [Google Scholar] [CrossRef]
- Melo, V.; Monteiro, L.; Orge, C.; Sales, M.; Melo, J.; Rodrigues, B.; Melo, A. Prevalence of temporomandibular disorders in the Brazilian population: A systematic review and meta-analysis. Cranio 2025, 43, 629–636. [Google Scholar] [CrossRef]
- Zieliński, G.; Pająk-Zielińska, B.; Ginszt, M. A Meta-Analysis of the Global Prevalence of Temporomandibular Disorders. J. Clin. Med. 2024, 13, 1365. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, D.A.; Camparis, C.M.; Speciali, J.G.; Franco, A.L.; Castanharo, S.M.; Bigal, M.E. Temporomandibular disorders are differentially associated with headache diagnoses: A controlled study. Clin. J. Pain 2011, 27, 611–615. [Google Scholar] [CrossRef]
- Gauer, R.L.; Semidey, M.J. Diagnosis and treatment of temporomandibular disorders. Am. Fam. Physician 2015, 91, 378–386. [Google Scholar]
- National Institute of Dental and Craniofacial Research. Facial Pain. Available online: https://www.nidcr.nih.gov/research/data-statistics/facial-pain (accessed on 15 April 2025).
- Slade, G.D.; Ohrbach, R.; Greenspan, J.D.; Fillingim, R.B.; Bair, E.; Sanders, A.E.; Dubner, R.; Diatchenko, L.; Meloto, C.B.; Smith, S.; et al. Painful Temporomandibular Disorder:Decade of Discovery from OPPERA Studies. J. Dent. Res. 2016, 95, 1084–1092. [Google Scholar] [CrossRef]
- Li, D.T.S.; Leung, Y.Y. Temporomandibular disorders: Current concepts and controversies in diagnosis and management. Diagnostics 2021, 11, 459. [Google Scholar] [CrossRef] [PubMed]
- Benites-Vega, J.C.; Trujillo-Herrera, T. Prevalencia y diagnóstico de disfunción temporomandibular en la práctica médica-Hospital General María Auxiliadora. Acta Médica Peru. 2021, 38, 97–103. [Google Scholar] [CrossRef]
- Srivastava, K.C.; Shrivastava, D.; Khan, Z.A.; Nagarajappa, A.K.; Mousa, M.A.; Hamza, M.O.; Al-Johani, K.; Alam, M.K. Evaluation of temporomandibular disorders among dental students of Saudi Arabia using Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): A cross-sectional study. BMC Oral Health 2021, 21, 211. [Google Scholar] [CrossRef]
- Palmer, J.; Durham, J. Temporomandibular disorders. BJA Educ. 2021, 21, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Wieckiewicz, M.; Grychowska, N.; Nahajowski, M.; Hnitecka, S.; Kempiak, K.; Charemska, K.; Balicz, A.; Chirkowska, A.; Zietek, M.; Winocur, E. Prevalence and overlaps of headaches and pain-related temporomandibular disorders among the polish urban population. J. Oral Facial Pain Headache 2020, 34, 31–39. [Google Scholar] [CrossRef]
- Häggman-Henrikson, B.; Liv, P.; Ilgunas, A.; Visscher, C.M.; Lobbezoo, F.; Durham, J.; Lövgren, A. Increasing gender differences in the prevalence and chronification of orofacial pain in the population. Pain 2020, 161, 1768–1775. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Von Piekartz, H. Clinical reasoning for the examination and physical therapy treatment of temporomandibular disorders (TMD): A narrative literature review. J. Clin. Med. 2020, 9, 3686. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6. [Google Scholar] [CrossRef]
- Durham, J.; Aggarwal, V.; Davies, S.J.; Harrison, S.D.; Jagger, R.G.; Leeson, R.; Lloyd, R.; Thayer, T.; Underhill, H.; Wassell, R.W.; et al. Temporomandibular Disorders (TMDs): An Update and Management Guidance for Primary Care from the UK Specialist Interest Group in Orofacial Pain and TMDs (USOT); Royal College of Surgeons of England: London, UK, 2013; 22p. [Google Scholar]
- Leeuw, R.d.; Klasser, G.D. Orofacial Pain: Guidelines for Assessment, Diagnosis, and Management, 5th ed.; Quintessence Publishing Co., Inc.: Chicago, IL, USA, 2013. [Google Scholar]
- Scrivani, S.J.; Keith, D.A.; Kaban, L.B. Temporomandibular disorders. N. Engl. J. Med. 2008, 359, 2693–2705. [Google Scholar] [CrossRef]
- Yi, Y.; Zhou, X.; Xiong, X.; Wang, J. Neuroimmune interactions in painful TMD: Mechanisms and treatment implications. J. Leukoc. Biol. 2021, 110, 553–563. [Google Scholar] [CrossRef]
- Angeles-García, K.; Ladera-Castañeda, M.; Castro-Ramirez, L.; Paucar-Rodríguez, E.; Castro-Rojas, M.; Cervantes-Ganoza, L.; Cayo-Rojas, C. Presence of TMD-related pain and symptoms associated with anxiety in Peruvian students in their final years of dental education: An analytical cross-sectional study under a multivariable regression model. BMC Oral Health 2025, 25, 277. [Google Scholar] [CrossRef]
- Santos, E.A.d.; Peinado, B.R.R.; Frazão, D.R.; Né, Y.G.d.S.; Fagundes, N.C.F.; Magno, M.B.; Maia, L.C.; Lima, R.R.; Souza-Rodrigues, R.D.d. Association between temporomandibular disorders and anxiety: A systematic review. Front. Psychiatry 2022, 13, 990430. [Google Scholar] [CrossRef] [PubMed]
- Ohrbach, R.; Dworkin, S. The evolution of TMD diagnosis: Past, present, future. J. Dent. Res. 2016, 95, 1093–1101. [Google Scholar] [CrossRef]
- Theroux, J.; Stomski, N.; Cope, V.; Mortimer-Jones, S.; Maurice, L. A cross-sectional study of the association between anxiety and temporomandibular disorder in Australian chiropractic students. J. Chiropr. Educ. 2019, 33, 111–117. [Google Scholar] [CrossRef]
- Alamri, A.; Shahin, S.; Bakhurji, E.A.; Alsulaiman, A.A.; Salloot, Z.; Nazir, M. Association of Test Anxiety with Temporomandibular Disorder in Health Professions Students: A Cross-Sectional Study. Int. J. Dent. 2020, 2020, 8833804. [Google Scholar] [CrossRef] [PubMed]
- Gharavi, S.M.; Qiao, Y.; Faghihimehr, A.; Vossen, J. Imaging of the Temporomandibular Joint. Diagnostics 2022, 12, 1006. [Google Scholar] [CrossRef] [PubMed]
- Petscavage-Thomas, J.M.; Walker, E.A. Unlocking the jaw: Advanced imaging of the temporomandibular joint. AJR Am. J. Roentgenol. 2014, 203, 1047–1058. [Google Scholar] [CrossRef]
- Weitzman, E.R. Poor mental health, depression, and associations with alcohol consumption, harm, and abuse in a national sample of young adults in college. J. Nerv. Ment. Dis. 2004, 192, 269–277. [Google Scholar] [CrossRef]
- Tan, G.X.; Soh, X.C.; Hartanto, A.; Goh, A.Y.; Majeed, N.M. Prevalence of anxiety in college and university students: An umbrella review. J. Affect. Disord. Rep. 2023, 14, 100658. [Google Scholar] [CrossRef]
- Tanculescu, O.; Apostu, A.M.; Doloca, A.; Solomon, S.M.; Diaconu-Popa, D.; Ciongradi, C.I.; Vieriu, R.M.; Aungurencei, O.; Fatu, A.M.; Ioanid, N.; et al. Perception of Remote Learning by Fixed Prosthodontic Students at a Romanian Faculty of Dentistry. Int. J. Environ. Res. Public Health 2023, 20, 3622. [Google Scholar] [CrossRef]
- UMF_Iasi. Available online: https://www.umfiasi.ro/en/academic/facultati/Dental-medicine/Pages/Educational-plans.aspx (accessed on 1 May 2025).
- SurveyMonkey. Available online: https://www.surveymonkey.co.uk/mp/margin-of-error-calculator/ (accessed on 1 May 2025).
- Chuinsiri, N.; Jitprasertwong, P. Prevalence of self-reported pain-related temporomandibular disorders and association with psychological distress in a dental clinic setting. J. Int. Med. Res. 2020, 48, 0300060520951744. [Google Scholar] [CrossRef]
- Alrashdan, M.S.; Nuseir, A.; AL-Omiri, M.K. Prevalence and correlations of temporomandibular disorders in Northern Jordan using diagnostic criteria axis I. J. Investig. Clin. Dent. 2019, 10, e12390. [Google Scholar] [CrossRef]
- Jeremic-Knezevic, M.; Knezevic, A.; Boban, N.; Koprivica, D.D.; Boban, J. Correlation of somatization, depression, and chronic pain with clinical findings of the temporomandibular disorders in asymptomatic women. Cranio® 2021, 39, 17–23. [Google Scholar] [CrossRef]
- Kmeid, E.; Nacouzi, M.; Hallit, S.; Rohayem, Z. Prevalence of temporomandibular joint disorder in the Lebanese population, and its association with depression, anxiety, and stress. Head. Face Med. 2020, 16, 19. [Google Scholar] [CrossRef] [PubMed]
- Fillingim, R.B.; Ohrbach, R.; Greenspan, J.D.; Knott, C.; Diatchenko, L.; Dubner, R.; Bair, E.; Baraian, C.; Mack, N.; Slade, G.D.; et al. Psychological Factors Associated With Development of TMD: The OPPERA Prospective Cohort Study. J. Pain 2013, 14, T75–T90. [Google Scholar] [CrossRef]
- Sorge, R.E.; Totsch, S.K. Sex Differences in Pain. J. Neurosci. Res. 2017, 95, 1271–1281. [Google Scholar] [CrossRef] [PubMed]
- Alahmary, A.W. Association of temporomandibular disorder symptoms with anxiety and depression in Saudi dental students. Open Access Maced. J. Med. Sci. 2019, 7, 4116. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Association | Group 1 | Group 2 | χ2 | df | p-Value |
|---|---|---|---|---|---|
| Orofacial pain vs. TMJ noises | Pain and noises: 79 (22.2%) | Neither: 132 (37.1%) | 9.84 | 1 | ≈0.002 |
| Pain only: 76 (21.3%) | Noises only: 69 (19.4%) | ||||
| Temporal headache vs. orofacial pain | With headache: 131/155 (85%) | Without headache: 44/155 (29%) | 72.3 | 1 | <0.001 |
| Nocturnal bruxism vs. orofacial pain | Bruxers: 58% | Non-bruxers: 38% | 10.8 | 1 | 0.001 |
| Nocturnal bruxism vs. morning jaw stiffness | Bruxers: 41% | Non-bruxers: 13% | 32.7 | 1 | <0.001 |
| TMJ noises vs. oral behaviors | Noises present: mean 15.0 | No noises: mean 10.6 | t-test (approx.) | — | <0.01 |
| Symptom | Female % (n = 235) | Male % (n = 115) | χ2 | df | p-Value |
|---|---|---|---|---|---|
| Orofacial pain | 44.7% (105/235) | 41.7% (48/115) | 0.165 | 1 | 0.684 |
| TMJ noises | 43.0% (101/235) | 39.1% (45/115) | 0.325 | 1 | 0.568 |
| Mandibular locking | 20.4% (48/235) | 19.1% (22/115) | 0.020 | 1 | 0.887 |
| Temporal headache | 43.4% (102/235) | 24.3% (28/115) | 11.208 | 1 | 0.0008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarevici, E.L.; Tanculescu, O.; Apostu, A.M.; Solomon, S.M.; Rotaru-Costin, A.-T.; Doloca, A.; Bodnar, P.; Proca, V.S.; Ciocan-Pendefunda, A.-A.; Tatarciuc, M.; et al. Prevalence of Temporomandibular Disorder Symptoms Among Dental Students at the Faculty of Dental Medicine in Iași: A Self-Reported Study Based on DC/TMD Criteria. Diagnostics 2025, 15, 1908. https://doi.org/10.3390/diagnostics15151908
Tarevici EL, Tanculescu O, Apostu AM, Solomon SM, Rotaru-Costin A-T, Doloca A, Bodnar P, Proca VS, Ciocan-Pendefunda A-A, Tatarciuc M, et al. Prevalence of Temporomandibular Disorder Symptoms Among Dental Students at the Faculty of Dental Medicine in Iași: A Self-Reported Study Based on DC/TMD Criteria. Diagnostics. 2025; 15(15):1908. https://doi.org/10.3390/diagnostics15151908
Chicago/Turabian StyleTarevici, Eugenia Larisa, Oana Tanculescu, Alina Mihaela Apostu, Sorina Mihaela Solomon, Alice-Teodora Rotaru-Costin, Adrian Doloca, Petronela Bodnar, Vlad Stefan Proca, Alice-Arina Ciocan-Pendefunda, Monica Tatarciuc, and et al. 2025. "Prevalence of Temporomandibular Disorder Symptoms Among Dental Students at the Faculty of Dental Medicine in Iași: A Self-Reported Study Based on DC/TMD Criteria" Diagnostics 15, no. 15: 1908. https://doi.org/10.3390/diagnostics15151908
APA StyleTarevici, E. L., Tanculescu, O., Apostu, A. M., Solomon, S. M., Rotaru-Costin, A.-T., Doloca, A., Bodnar, P., Proca, V. S., Ciocan-Pendefunda, A.-A., Tatarciuc, M., Fala, V., & Iordache, M. C. I. (2025). Prevalence of Temporomandibular Disorder Symptoms Among Dental Students at the Faculty of Dental Medicine in Iași: A Self-Reported Study Based on DC/TMD Criteria. Diagnostics, 15(15), 1908. https://doi.org/10.3390/diagnostics15151908