
Causes and Risk Factors of Pediatric Spontaneous Intracranial Hemorrhage—A Systematic Review

 ,
,  ,
,  and
and
Abstract
1. Introduction
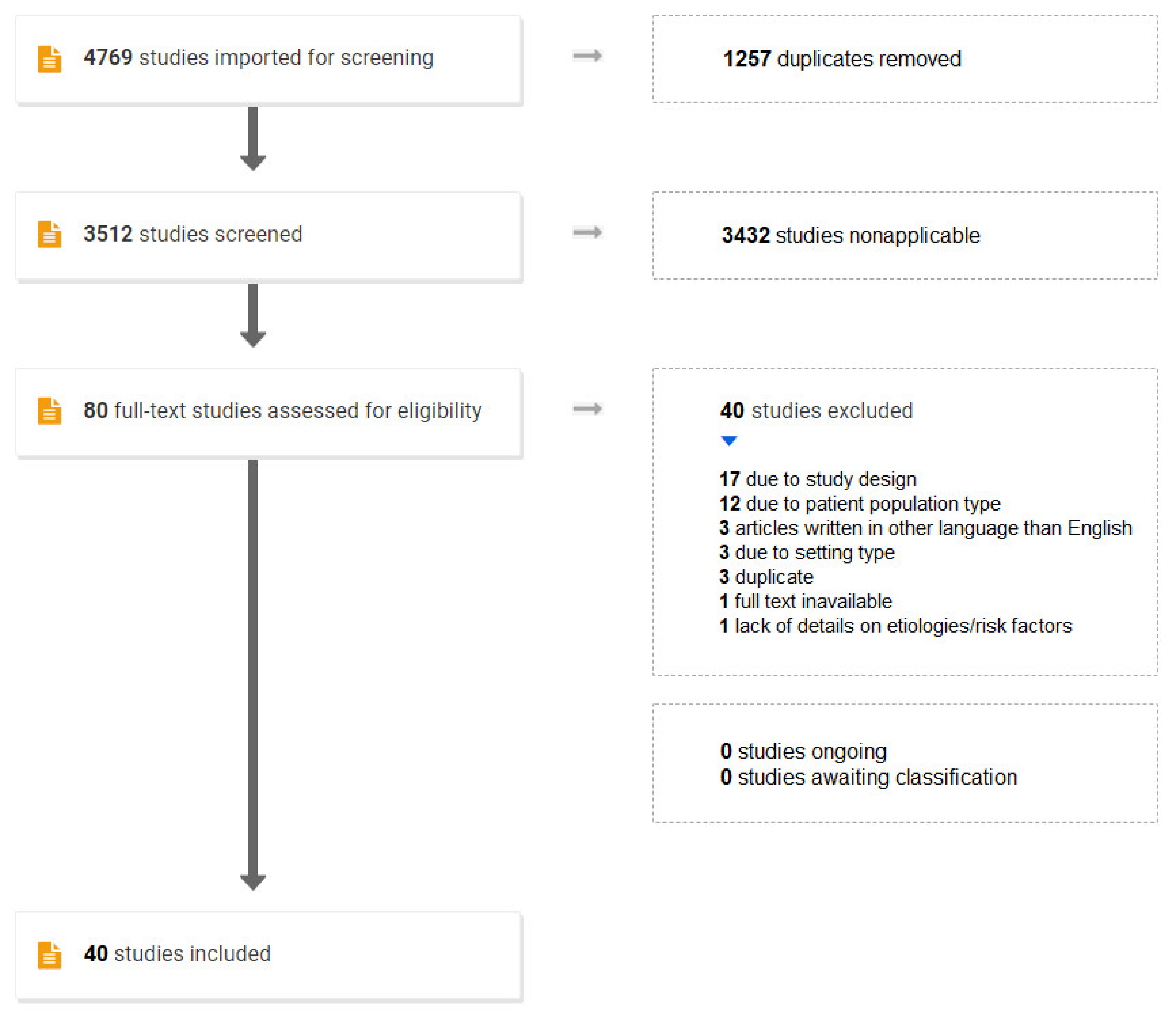
2. Materials and Methods
3. Results

{kind=link}
| Publication | Study Type * | Time Period | Number of Patients/Causes ** | Age | Hemato-Logical Cause | Vas-Cular Cause | Intra-cranial Infection | Brain Tumor | Cardiac Cause | Systemic Cause *** | Unknown Cause | Comments—Hemorrhage Type Analyzed |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lanthier et al., 2000 [21] | Single/retrosp. | 1991–1997 | 21 | 1 m–18 y | 9.52% | 66.67% | N/A | 9.52% | N/A | N/A | 14.28% | ICH with or without SDH, EDH or SAH. |
| Al-Jarallah et al., 2000 [3] | Single/retrosp. | 1990–1998 | 68/79 | 3 m–18 y | 26.58% | 40.51% | 1.26% | 11.39% | N/A | 2.53% | 17.72% | ICH with or without SDH or SAH. |
| Sandberg et al., 2001 [22] | Single/retrosp. | 1960–2000 | 3 | 43 d–3 m | 66.67% | 33.33% | N/A | N/A | N/A | N/A | N/A | ICH with SDH and IVH, ICH with SDH, ICH. |
| Suh et al., 2001 [23] | Single/retrosp. | 1985–? | 16 | 2 m–2 y | N/A | 100.0% | N/A | N/A | N/A | N/A | N/A | ICH, SAH, SDH, IVH. |
| Blom et al., 2003 [4] | Single/retrosp. | 1978–1998 | 56 | 1 m–16 y | 17.86% | 53.57% | 5.36% | 1.78% | N/A | 1.78% | 19.64% | ICH, IVH, SAH. |
| Meyer-Heim et al., 2003 [24] | Single/retrosp. | 1990–2000 | 34 | 2 m–17 y | 11.76% | 73.53% | N/A | 2.94% | N/A | N/A | 11.76% | ICH, SAH, IVH, ITH, SDH. |
| Zahuranec et al., 2005 [25] | One county/retrosp. | 2002–2003 | 5 | 2 m–17 y | N/A | 40.00% | N/A | N/A | 20.00% | 20.00% | 20.00% | ICH. |
| Aydinli et al., 2006 [26] | Single/retrosp. | 1995–2003 | 22 | 40 d–8 y | 77.27% | N/A | N/A | N/A | N/A | N/A | 22.73% | Not specified, probably ICH. |
| Liu et al., 2006 [27] | Single/retrosp. | 1997–2003 | 50 | 1 m–16 y | N/A | 62.00% | N/A | 10.00% | N/A | 16.00% | 12.00% | ICH with or without IVH or SAH. |
| de Ribaupierre et al., 2008 [20] | Dual/retrosp. | 1995–2005 | 22 | 2 m–18 y | N/A | 81.82% | N/A | N/A | N/A | N/A | 18.18% | ICH, SAH. |
| Kumar et al., 2009 [28] | Single/retrosp. | 1998–2007 | 50 | 2 m–17 y | 4.00% | 88.00% | N/A | 4.00% | N/A | N/A | 4.00% | ICH, SAH, IVH, intracerebellar hemorrhage. |
| Wang et al., 2009 [12] | Single/retrosp. | 1996–2006 | 94/181 | 1 m–16 y | 82.32% | 7.73% | 2.21% | N/A | N/A | 0.55% | 7.18% | SAH, ICH, other intracerebral hemorrhages. |
| Del Balzo et al., 2009 [29] | Triple/retrosp. | 2001–2006 | 4/5 | 2 y–14 y | N/A | 80.00% | N/A | N/A | N/A | 20.00% | N/A | Hemorrhagic stroke, no further details provided. |
| Tham et al., 2009 [30] | Single/retrosp. | 1999–2006 | 11 | 3 m–18 y | 27.27% | 36.36% | N/A | N/A | 9.09% | N/A | 27.27% | SAH, SDH, ICH, IVH. |
| Laugesaar et al., 2010 [31] | Regional + national registry/retrosp. + prosp. | 1995–2006 (retrosp.), 2004–2006 (prosp.) | 16 | 30 d–18 y | N/A | 62.5% | 6.25% | N/A | N/A | 12.5% | 18.75% | ICH, SAH. |
| Beslow et al., 2010 [32] | Single/prosp. | 2006–2008 | 22 | 4 y–17 y | N/A | 90.91% | N/A | N/A | N/A | N/A | 9.09% | ICH, wthout or with IVH or other hemorrhage types. |
| Paonessa et al., 2010 [33] | Single/retrosp. | 10 years (unspecified) | 17 | 5 y–16 y | N/A | 82.35% | N/A | N/A | N/A | N/A | 17.65% | ICH, SAH. |
| Christerson et al., 2010 [34] | Regional registry/retrosp. | 2000–2006 | 21/22 | 9 y–16 y | 13.64% | 77.27% | N/A | N/A | N/A | 4.54% | 4.54% | ICH, SAH. |
| Statler et al., 2010 [35] | Multistate registry/retrosp. | 2000–2003 | 4424/4425 **** | 1 m–18 y | 8.38% | 6.85% | 2.24% | 6.15% | 1.74% | 0.18% | 74.46% | Hemorrhagic stroke, no further details provided. |
| Yock-Corrales et al., 2011 [36] | Single/retrosp. | 2003–2008 | 31 | 1 m–16 y | N/A | 61.29% | N/A | N/A | N/A | N/A | 38.71% | ICH and “unspecified intracranial hemorrhage” (ICD-10 codes). |
| Zidan et al., 2012 [37] | Single/retrosp. | 2008–2009 | 17 | 1 m–18 y | 52.94% | 35.29% | N/A | 11.76% | N/A | N/A | N/A | ICH. |
| Lo et al., 2013 [38] | Single/retrosp. | 2000–2009 | 59 | 0.1 y–18 y | 3.39% | 52.54% | 1.69% | 18.64% | 8.47% | 8.47% | 6.79% | SAH with ICH or IVH, ICH, IVH with other hemorrhage types. |
| Kalita et al., 2013 [39] | Single/retrosp. | 2001–2011 | 10 | 1 m–18 y | N/A | 40.00% | N/A | N/A | N/A | 20.00% | 40.00% | ICH only. |
| Beslow et al., 2013 [40] | Triple/prosp. | 2007–2012 | 53/54 | 28 d–18 y | 20.37% | 62.96% | N/A | N/A | N/A | N/A | 16.67% | ICH, IVH, ICH with IVH. |
| Xie et al., 2014 [11] | Single/retrosp. | 2003–2011 | 109/201 | 1 m–18 y | 67.16% | 8.95% | 5.97% | 0.99% | 0.50% | N/A | 16.42% | SAH, ICH, SDH, other non-traumatic hemorrhage. |
| Deng et al., 2015 [41] | Single/retrosp. | 2002–2011 | 249 | 1 m–18 y | N/A | 45.78% | N/A | N/A | N/A | 37.35% | 16.87% | ICH, SAH. |
| Adil et al., 2015 [42] | Multistate registry/retrosp. | 2003, 2006, 2009 | 1172 | 1 y–18 y | 15.95% | 17.58% | N/A | N/A | 1.88% | 24.57% | 40.02% | ICH and ICH with SAH. |
| Liu et al., 2015 [43] | Single/prosp. | 2012–2014 | 70 | 1 y–18 y | 1.43% | 74.28% | N/A | 2.86% | N/A | 1.43% | 20.00% | ICH with or without IVH or SAH. |
| Gelfand et al., 2015 [44] | State registry/retrosp. | 1997–2007 | 42 | 2 y–17 y | N/A | 66.67% | N/A | N/A | N/A | N/A | 33.33% | Hemorrhagic stroke, no further details provided. |
| Abbas et al., 2016 [45] | Single/retrosp. | 2007–2014 | 50 | 1 m–16 y | 56.00% | 14.00% | 4.00% | N/A | N/A | N/A | 26.00% | ICH, SAH, SDH, IVH. |
| Chiang et al., 2018 [46] | National registry/retrosp. | 2010–2011 | 299 | 1 m–18 y | 9.70% | 30.77% | 9.36% | 11.37% | 8.70% | 17.39% | 12.71% | Hemorrhagic stroke, no further details provided. |
| Yock-Corrales et al., 2018 [13] | Single/retrosp. | 7 y, unspecified. | 34 | 1 m–18 y | 14.70% | 35.29% | N/A | N/A | N/A | N/A | 50.00% | 5 patients with SAH, no details on the remaining. |
| Uzunhan et al., 2019 [47] | Single/retrosp. | 2007–2013 | 12 | 1.5 y–13 y | 16.67% | 41.67% | N/A | 8.33% | N/A | N/A | 33.33% | ICH or SAH. |
| Söbü et al., 2019 [48] | Single/retrosp. | 2000–2011 | 15 | 1 m–18 y | 73.33% | 6.67% | 6.67% | N/A | N/A | 6.67% | 6.67% | ICH, SAH. |
| de Montferrand et al., 2019 [49] | Single/retrosp. | 1992–2015 | 105 | 1 m–15 y | 1.90% | 88.57% | N/A | N/A | N/A | N/A | 9.52% | Hemorrhagic stroke, no further details provided. |
| Gerstl et al., 2019 [1] | Single/retrosp. | 2010–2016 | 33 | 1 m–17 y | 6.06% | 39.39% | 3.03% | 42.42% | N/A | 6.06% | 3.03% | ICH, IVH, SAH. |
| Boulouis et al., 2021 [8] | Single/retrosp. + prosp. ***** | 2000–2019 | 243 | 28 d–18 y | 5.76% | 77.37% | N/A | 2.88% | 6.99% | 0.82% | 6.17% | ICH with or without IVH. |
| Huang et al., 2021 [50] | Dual/retrosp. | 2008–2020 | 200 | 29 d–18 y | 33.50% | 37.00% | 1.50% | 3.50% | N/A | 2.50% | 22.00% | ICH with or without IVH or SAH. |
| Deng et al., 2021 [51] | Multi/retrosp. | 2018–2018 | 140/152 | 1 m–18 y | N/A | 78.95% | N/A | 2.63% | 1.97% | 3.29% | 13.16% | ICH and SAH. |
| Pangprasertkul et al., 2022 [52] | Single/retrosp. | 2009–2018 | 32/39 | 1 m–18 y | 61.54% | 28.21% | 2.56% | N/A | 2.56% | 2.56% | 2.56% | Radiological evidence of intracranial hemorrhage. |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gerstl, L.; Badura, K.; Heinen, F.; Weinberger, R.; Peraud, A.; Dorn, F.; Bonfert, M.V.; Berweck, S.; O’Callaghan, F.J. Childhood hemorrhagic stroke: A 7-year single-centre experience. Arch. Dis. Child. 2019, 104, 1198–1202. [Google Scholar] [CrossRef] [PubMed]
- Lo, W.D.; Lee, J.; Rusin, J.; Perkins, E.; Roach, E.S. Intracranial hemorrhage in children: An evolving spectrum. Arch. Neurol. 2008, 65, 1629–1633. [Google Scholar] [CrossRef] [PubMed]
- Al-Jarallah, A.; Al-Rifai, M.T.; Riela, A.R.; Roach, E.S. Nontraumatic brain hemorrhage in children: Etiology and presentation. J. Child Neurol. 2000, 15, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Blom, I.; De Schryver, E.L.L.M.; Jaap Kappelle, L.; Rinkel, G.J.E.; Jennekens-Schinkel, A.; Boudewyn Peters, A.C. Prognosis of haemorrhagic stroke in childhood: A long-term follow-up study. Dev. Med. Child Neurol. 2003, 45, 233–239. [Google Scholar] [CrossRef]
- Kolb, B.; Gibb, R. Brain Plasticity and Behaviour in the Developing Brain. J. Can. Acad. Child Adolesc. Psychiatry 2011, 20, 265–276. [Google Scholar]
- Osborn, A.G. Osborn’s Brain, 2nd ed.; Elsevier Inc.: Salt Lake City, UT, USA, 2017; pp. 111–114. [Google Scholar]
- Gumer, L.B.; Del Vecchio, M.; Aronoff, S. Strokes in Children: A Systematic Review. Pediatr. Emerg. Care 2014, 30, 660–664. [Google Scholar] [CrossRef]
- Boulouis, G.; Stricker, S.; Benichi, S.; Hak, J.-F.; Gariel, F.; Alias, Q.; de Saint Denis, T.; Kossorotoff, M.; Bajolle, F.; Garzelli, L.; et al. Etiology of intracerebral hemorrhage in children: Cohort study, systematic review, ant meta-analysis. J. Neurosurg. Pediatr. 2021, 27, 357–363. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Covidence—Better Systematic Review Management. Available online: https://www.covidence.org (accessed on 1 April 2022).
- Xie, L.-L.; Jiang, L. Arterial ischemic stroke and hemorrhagic stroke in Chinese children: A retrospective analysis. Brain Dev. 2014, 36, 153–158. [Google Scholar] [CrossRef]
- Wang, J.-J.; Shi, K.-L.; Li, J.-W.; Jiang, L.-Q.; Caspi, O.; Fang, F.; Xiao, J.; Jing, H.; Zou, L.-P. Risk factors for arterial ischemic and hemorrhagic stroke in childhood. Pediatr. Neurol. 2009, 40, 277–281. [Google Scholar] [CrossRef]
- Yock-Corrales, A.; Varela-Bulgarelli, F.; Barboza, C.; Gutierrez-Mata, A.; Mackay, M.T.; Babl, F. Presentation of Acute Childhood Stroke in a Tertiary Pediatric Emergency Department. Pediatr. Emerg. Care 2018, 34, 552–557. [Google Scholar] [CrossRef]
- Heit, J.J.; Iv, M.; Wintermark, M. Imaging of Intracranial Hemorrhage. J. Stroke 2017, 19, 11–27. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Baker, C.; Grant, A.M.; George, M.G.; Grosse, S.D.; Adamkiewicz, T.V. Contribution of Sickle Cell Disease to the Pediatric Stroke Burden Among Hospital Discharges of African-Americans-United States, 1997–2012. Pediatr. Blood. Cancer 2015, 62, 2076–2081. [Google Scholar] [CrossRef]
- Tuppin, P.; Samson, S.; Woimant, F.; Chabrier, S. Management and 2-year follow-up of children aged 29 days to 17 years hospitalized for a first stroke in France (2009–2010). Arch. Pediatr. 2014, 21, 1305–1315. [Google Scholar] [CrossRef]
- Murphy, L.K.; Compas, B.E.; Gindville, M.C.; Reeslund, K.L.; Jordan, L.C. Cognitive functioning over 2 years after intracerebral hemorrhage in school-aged children. Dev. Med. Child. Neurol. 2017, 59, 1146–1151. [Google Scholar] [CrossRef]
- Boulouis, G.; Stricker, S.; Benichi, S.; Hak, J.-F.; Gariel, F.; Kossorotoff, M.; Garcelon, N.; Harroche, A.; Alias, Q.; Garzelli, L.; et al. Mortality and functional outcome after pediatric intracerebral hemorrhage: Cohort study and meta-analysis. J. Neurosurg. Pediatr. 2021, 9, 1–7. [Google Scholar] [CrossRef]
- De Ribaupierre, S.; Rilliet, B.; Cotting, J.; Regli, L. A 10-year experience in paediatric cerebral hemorrhage: Which children with headache need more than a clinical examination? Swiss Med. Wkly. 2008, 138, 59–69. [Google Scholar]
- Lanthier, S.; Carmant, L.; David, M.; Larbrisseau, A.; de Veber, G. Stroke in children: The coexistence of multiple risk factors predicts poor outcome. Neurology 2000, 54, 371–378. [Google Scholar] [CrossRef]
- Sandberg, D.I.; Lamberti-Pasculli, M.; Drake, J.M.; Humphreys, R.P.; Rutka, J.T. Spontaneous intraparenchymal hemorrhage in full-term neonates. Neurosurgery 2001, 48, 1042–1048. [Google Scholar] [CrossRef]
- Suh, D.C.; Alvarez, H.; Bhattacharya, J.J.; Rodesch, G.; Lasjaunias, P.L. Intracranial Haemorrhage Within the First two Years of Life. Acta Neurochir. 2001, 143, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Heim, A.D.; Boltshauser, E. Spontaneous intracranial haemorrhage in children: Aetiology, presentation and outcome. Brain Dev. 2003, 25, 416–421. [Google Scholar] [CrossRef]
- Zahuraniec, D.B.; Brown, D.L.; Lisabeth, L.D.; Morgenstern, L.B. Is It Time for a Large, Collaborative Study of Pediatric Stroke? Stroke 2005, 36, 1825–1829. [Google Scholar] [CrossRef] [PubMed]
- Aydinli, N.; Tatli, B.; Çalişkan, M.; Ozmen, M.; Citak, A.; Unuvar, A.; Baykal, T.; Omeroglu, R.E.; Aydin, K.; Sencer, S.; et al. Stroke in Childhood: Experience in Istanbul, Turkey. J. Trop. Pediatr. 2006, 52, 158–162. [Google Scholar] [CrossRef]
- Liu, A.C.Y.; Segaren, N.; Cox, T.S.C.; Hayward, R.D.; Chong, W.K.; Ganesan, V.; Saunders, D.E. Is there a role for magnetic resonance imaging in the evaluation of non-traumatic intraparenchymal haemorrhage in children? Pediatr. Radiol. 2006, 36, 940–946. [Google Scholar] [CrossRef]
- Kumar, R.; Shukla, D.; Mahapatra, A.K. Spontaneous intracranial hemorrhage in children. Pediatr. Neurosurg. 2009, 45, 37–45. [Google Scholar] [CrossRef]
- Del Balzo, F.; Spalice, A.; Ruggieri, M.; Greco, F.; Properzi, E.; Iannetti, P. Stroke in children: Inherited and acquired factors and age-related variations in the presentation of 48 paediatric patients. Acta Paediatr. 2009, 98, 1130–1136. [Google Scholar] [CrossRef]
- Tham, E.H.; Tay, S.K.H.; Low, P.S. Factors Predictive of Outcome in Childhood Stroke in an Asian Population. Ann. Acad. Med. Singap. 2009, 38, 876–881. [Google Scholar]
- Laugesaar, R.; Kolk, A.; Uustalu, U.; Ilves, P.; Tomberg, T.; Talvik, I.; Köbas, K.; Sander, V.; Talvik, T. Epidemiology of childhood stroke in Estonia. Pediatr. Neurol. 2010, 42, 93–100. [Google Scholar] [CrossRef]
- Beslow, L.A.; Licht, D.J.; Smith, S.E.; Storm, P.B.; Heuer, G.G.; Zimmerman, R.A.; Feiler, A.M.; Kasner, S.E.; Ichord, R.N.; Jordan, L.C. Predictors of outcome in childhood intracerebral hemorrhage: A prospective consecutive cohort study. Stroke 2010, 41, 313. [Google Scholar] [CrossRef]
- Paonessa, A.; Limbucci, N.; Tozzi, E.; Splendiani, A.; Gallucci, M. Radiological strategy in acute stroke in children. Eur. J. Radiol. 2010, 74, 77–85. [Google Scholar] [CrossRef]
- Christerson, S.; Strömberg, B. Childhood stroke in Sweden I: Incidence, symptoms, risk factors and short-term outcome. Acta Paediatr. 2010, 99, 1641–1649. [Google Scholar] [CrossRef]
- Statler, K.D.; Dong, L.; Nielsen, D.M.; Bratton, S.L. Pediatric stroke: Clinical characteristics, acute care utilization patterns, and mortality. Childs Nerv. Syst. 2011, 27, 565–573. [Google Scholar] [CrossRef]
- Yock-Corrales, A.; Mackay, M.T.; Mosley, I.; Maixner, W.; Babl, F.E. Acute Childhood Arterial Ischemic and Hemorrhagic Stroke in the Emergency Department. Ann. Emerg. Med. 2011, 58, 156–163. [Google Scholar] [CrossRef]
- Zidan, I.; Ghanem, A. Intracerebral hemorrhage in children. Alex. J. Med. 2012, 48, 139–145. [Google Scholar] [CrossRef]
- Lo, W.D.; Hajek, C.; Pappa, C.; Wang, W.; Zumberge, N. Outcomes in Children with Hemorrhagic Stroke. JAMA Neurol. 2013, 70, 66–71. [Google Scholar] [CrossRef]
- Kalita, J.; Goyal, G.; Misra, U.K. Experience of pediatric stroke from a tertiary medical center in North India. J. Neurol. Sci. 2013, 325, 67–73. [Google Scholar] [CrossRef]
- Beslow, L.A.; Abend, N.S.; Gindville, M.C.; Bastian, R.A.; Licht, D.J.; Smith, S.E.; Hillis, A.E.; Ichord, R.N.; Jordan, L.C. Pediatric Intracerebral Hemorrhage: Acute Symptomatic Seizures and Epilepsy. JAMA Neurol. 2013, 70, 448–454. [Google Scholar] [CrossRef]
- Deng, Y.; Wang, Y.; Yang, W.; Yu, Y.; Xu, J.; Wang, Y.; Gao, B. Risk Factors and Imaging Characteristics of Childhood Stroke in China. J. Child. Neurol. 2015, 30, 339–343. [Google Scholar] [CrossRef]
- Adil, M.M.; Qurashi, A.I.; Beslow, L.A.; Malik, A.A.; Jordan, L.C. Factors Associated with Increased In-Hospital Mortality Among Children with Intracerebral Hemorrhage. J. Child. Neurol. 2015, 30, 1024–1028. [Google Scholar] [CrossRef]
- Liu, J.; Wang, D.; Lei, C.; Xiong, Y.; Yuan, R.; Hao, Z.; Tao, W.; Liu, M. Etiology, clinical characteristics and prognosis of spontaneous intracerebral hemorrhage in children: A prospective cohort study in China. J. Neurol. Sci. 2015, 358, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, A.A.; Fullerton, H.J.; Jacobson, A.; Sidney, S.; Goadsby, P.J.; Kurth, T.; Pressman, A. Is Migraine a Risk Factor for Pediatric Stroke? Cephalalgia 2015, 35, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Abbas, Q.; Ain Merchant, Q.U.; Nasir, B.; Haque, A.U.; Salam, B.; Javed, G. Spectrum of Intracerebral Hemorrhage in Children: A Report from PICU of a Resource Limited Country. Crit. Care Res. Pract. 2016, 2016, 9124245. [Google Scholar] [CrossRef] [PubMed]
- Chiang, K.-L.; Cheng, C.-Y. Epidemiology, risk factors and characteristics of pediatric stroke: A nationwide population-based study. QJM 2018, 111, 445–454. [Google Scholar] [CrossRef]
- Uzunhan, T.A.; Aydinli, N.; Çalişkan, M.; Tatli, B.; Özmen, M. Short-term neurological outcomes in ischemic and hemorrhagic pediatric stroke. Pediatr. Int. 2019, 61, 166–174. [Google Scholar] [CrossRef]
- Söbü, E.; Özdemir, N.; Uysal, S.; Buyru, N.; Celkan, T. Pediatric Stroke: A Single-Center Experience. J. Pediatr. Hematol. Oncol. 2019, 41, 519–524. [Google Scholar] [CrossRef]
- de Montferrand, C.; Vassel-Hitier, J.; Yvon-Chaou, E.; Câmara-Costa, H.; Dellatolas, G.; Chevignard, M. Language and cognitive outcomes after childhood stroke: Theoretical implications for hemispheric specialization. Cortex 2019, 120, 509–523. [Google Scholar] [CrossRef]
- Huang, X.; Cheng, Z.; Xu, Y.; Xia, L.; Zhan, Z.; Xu, T.; Cao, Y.; Han, Z. Associations of Clinical Characteristics and Etiology with Death in Hospitalized Chinese Children After Spontaneous Intracerebral Hemorrhage: A Single-Center, Retrospective Cohort Study. Front. Pediatr. 2021, 8, 576077. [Google Scholar] [CrossRef]
- Deng, Y.; Liu, G.; Zhang, G.; Xu, J.; Yao, C.; Wang, L.; Zhao, C.; Wang, Y. Childhood strokes in China describing clinical characteristics, risk factors and performance indicators: A case-series study. Stroke Vasc. Neurol. 2021, 7, 140–148. [Google Scholar] [CrossRef]
- Pangprasertkul, S.; Borisoot, W.; Buawangpong, N.; Sirikul, W.; Wiwattanadittakul, N.; Katanyuwong, K.; Sanguansermsri, C. Comparison of Arterial Ischemic and Hemorrhagic Pediatric Stroke in Etiology, Risk Factors, Clinical Manifestations, and Prognosis. Pediatr. Emerg. Care 2022. online ahead of print. [Google Scholar] [CrossRef]
- International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Available online: https://www.cdc.gov/nchs/icd/icd9cm.htm (accessed on 1 April 2022).
- Boulouis, G.; Blauwblomme, T.; Hak, J.F.; Benichi, S.; Kirton, A.; Meyer, P.; Chevignard, M.; Tournier-Lasserve, E.; Mackay, M.T.; Chabrier, S.; et al. Nontraumatic Pediatric Intracerebral Hemorrhage. Stroke 2019, 50, 3654–3661. [Google Scholar] [CrossRef]
- Carvi y Nievas, M.N.; Archavlis, E. Atypical causes of nontraumatic intracranial subarachnoid hemorrhage. Clin. Neurol. Neurosurg. 2009, 111, 354–358. [Google Scholar] [CrossRef]
- Coombs, J.B.; Coombs, B.L.; Chin, E.J. Acute spontaneous subdural hematoma in a middle-aged adult: Case report and review of the literature. J. Emerg. Med. 2014, 47, e63–e68. [Google Scholar] [CrossRef]
- Ng, W.H.; Yeo, T.T.; Seow, W.T. Non-traumatic spontaneous acute epidural haematoma—Report of two cases and review of the literature. J. Clin. Neurosci. 2004, 11, 791–793. [Google Scholar] [CrossRef]
- Passero, S.; Ulivelli, M.; Reale, F. Primary intraventricular haemorrhage in adults. Acta Neurol. Scand. 2002, 105, 115–119. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciochon, U.M.; Bindslev, J.B.B.; Hoei-Hansen, C.E.; Truelsen, T.C.; Larsen, V.A.; Nielsen, M.B.; Hansen, A.E. Causes and Risk Factors of Pediatric Spontaneous Intracranial Hemorrhage—A Systematic Review. Diagnostics 2022, 12, 1459. https://doi.org/10.3390/diagnostics12061459
Ciochon UM, Bindslev JBB, Hoei-Hansen CE, Truelsen TC, Larsen VA, Nielsen MB, Hansen AE. Causes and Risk Factors of Pediatric Spontaneous Intracranial Hemorrhage—A Systematic Review. Diagnostics. 2022; 12(6):1459. https://doi.org/10.3390/diagnostics12061459
Chicago/Turabian StyleCiochon, Urszula Maria, Julie Bolette Brix Bindslev, Christina Engel Hoei-Hansen, Thomas Clement Truelsen, Vibeke Andrée Larsen, Michael Bachmann Nielsen, and Adam Espe Hansen. 2022. "Causes and Risk Factors of Pediatric Spontaneous Intracranial Hemorrhage—A Systematic Review" Diagnostics 12, no. 6: 1459. https://doi.org/10.3390/diagnostics12061459
APA StyleCiochon, U. M., Bindslev, J. B. B., Hoei-Hansen, C. E., Truelsen, T. C., Larsen, V. A., Nielsen, M. B., & Hansen, A. E. (2022). Causes and Risk Factors of Pediatric Spontaneous Intracranial Hemorrhage—A Systematic Review. Diagnostics, 12(6), 1459. https://doi.org/10.3390/diagnostics12061459