Poor Mobilizers in Lymphoma but Not Myeloma Patients Had Significantly Poorer Progression-Free Survival after Autologous Stem Cell Transplantation: Results of a Large Retrospective, Single-Center Observational Study

 , , , ,
, , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Study Endpoints
2.3. Statistical Methods
3. Results
3.1. Efficacy of G-CSF +/− Plerixafor for Stem Cell Mobilization, Engraftment Kinetics, and Transfusion Requirements after ASCT
3.2. Autologous Stem Cell Transplantation and Engraftment Kinetics
3.3. Survival Outcomes and Secondary Malignancies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rollig, C.; Bornhauser, M. Multiple Myeloma. Lancet 2015, 385, 2197–2208. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S. Multiple Myeloma: Every Year a New Standard? Hematol. Oncol. 2019, 37 (Suppl. S1), 62–65. [Google Scholar] [CrossRef] [PubMed]
- Dhakal, B.; Szabo, A.; Chabra, S.; Hamadani, M.; D’Souza, A.; Usmani, S.; Sieracki, R.; Gyawali, B.; Jackson, J.; Asimakopoulos, F.; et al. Autologous Transplantation for Newly Diagnosed Multiple Myeloma in the Era of Novel Agent Induction: A Systematic Review and Meta-Analysis. JAMA Oncol. 2018, 4, 343–350. [Google Scholar] [CrossRef]
- Attal, M.; Lauwers-Cances, V.; Hulin, C.; Leleu, X.; Caillot, D.; Escoffre, M.; Arnulf, B.; Macro, M.; Belhadj, K.; Garderet, L.; et al. Lenalidomide, Bortezomib, and Dexamethasone with Transplantation for Myeloma. N. Engl. J. Med. 2017, 376, 1311–1320. [Google Scholar] [CrossRef] [PubMed]
- Gay, F.; Engelhardt, M.; Terpos, E.; Wäsch, R.; Giaccone, L.; Auner, H.; Caers, J.; Gramatzki, M.; van de Donk, N.; Oliva, S.; et al. From Transplant to Novel Cellular Therapies in Multiple Myeloma: European Myeloma Network Guidelines and Future Perspectives. Haematologica 2018, 103, 197–211. [Google Scholar] [CrossRef]
- Philip, T.; Guliemlmi, C.; Hagenbeek, A.; Somers, R.; Van der Lelie, H.; Bron, D.; Sonneveld, P.; Gisselbrecht, C.; Cahn, J.; Harousseau, J.; et al. Autologous Bone Marrow Transplantation as Compared with Salvage Chemotherapy in Relapses of Chemotherapy-Sensitive Non-Hodgkin’s Lymphoma. N. Engl. J. Med. 1995, 333, 1540–1545. [Google Scholar] [CrossRef]
- Gisselbrecht, C.; Glass, B.; Mounier, N.; Singh Gill, D.; Linch, D.; Trneny, M.; Bosly, A.; Ketterer, N.; Shpilberg, O.; Hagberg, H.; et al. Salvage Regimens With Autologous Transplantation for Relapsed Large B-Cell Lymphoma in the Rituximab Era. J. Clin. Oncol. 2010, 28, 4184–4190. [Google Scholar] [CrossRef]
- Crump, M.; Kuruvilla, J.; Couban, S.; MacDonald, D.; Kukreti, V.; Kouroukis, C.; Rubinger, M.; Buckstein, R.; Imrie, K.; Federico, M.; et al. Randomized Comparison of Gemcitabine, Dexamethasone, and Cisplatin Versus Dexamethasone, Cytarabine, and Cisplatin Chemotherapy Before Autologous Stem-Cell Transplantation for Relapsed and Refractory Aggressive Lymphomas: NCIC-CTG LY.12. J. Clin. Oncol. 2014, 32, 3490–3496. [Google Scholar] [CrossRef]
- Philip, T.; Chauvin, F.; Armitage, J.; Bron, D.; Hagenbeek, A.; Biron, P.; Spitzer, G.; Velasquez, W.; Weisenburger, D.; Fernandez-Ranada, J.; et al. Parma International Protocol: Pilot Study of DHAP Followed by Involved-Field Radiotherapy and BEAC with Autologous Bone Marrow Transplantation. Blood 1991, 77, 1587–1592. [Google Scholar] [CrossRef]
- Dreyling, M.; Lenz, G.; Hoster, E.; Van Hoof, A.; Gisselbrecht, C.; Schmits, R.; Metzner, B.; Truemper, L.; Reiser, M.; Steinhauser, H.; et al. Early Consolidation by Myeloablative Radiochemotherapy Followed by Autologous Stem Cell Transplantation in First Remission Significantly Prolongs Progression-Free Survival in Mantle-Cell Lymphoma: Results of a Prospective Randomized Trial of the European MCL Network. Blood 2005, 105, 2677–2684. [Google Scholar] [CrossRef]
- Montoto, S.; Corradini, P.; Dreyling, M.; Ghielmini, M.; Kimby, E.; López-Guillermo, A.; Mackinnon, S.; Marcus, R.; Salles, G.; Schouten, H.; et al. Indications for Hematopoietic Stem Cell Transplantation in Patients with Follicular Lymphoma: A Consensus Project of the EBMT-Lymphoma Working Party. Haematologica 2013, 98, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.; Burns, L.; Besien, K.; LeRademacher, J.; He, W.; Fenske, T.; Suzuki, R.; Hsu, J.; Schouten, H.; Hale, G.; et al. Hematopoietic Cell Transplantation for Systemic Mature T-Cell Non-Hodgkin Lymphoma. J. Clin. Oncol. 2013, 31, 3100–3109. [Google Scholar] [CrossRef] [PubMed]
- Hübel, K.; Fresen, M.; Apperley, J.; Basak, G.; Douglas, K.; Gabriel, I.; Geraldes, C.; Jaksic, O.; Koristek, Z.; Kröger, N.; et al. European Data on Stem Cell Mobilization with Plerixafor in Non-Hodgkin’s Lymphoma, Hodgkin’s Lymphoma and Multiple Myeloma Patients. A Subgroup Analysis of the European Consortium of Stem Cell Mobilization. Bone Marrow Transpl. 2012, 47, 1046–1050. [Google Scholar] [CrossRef]
- Worel, N.; Rosskopf, K.; Neumeister, P.; Kasparu, H.; Nachbaur, D.; Russ, G.; Namberger, K.; Witt, V.; Schloegl, E.; Zojer, N.; et al. Plerixafor and Granulocyte-Colony-Stimulating Factor (G-CSF) in Patients with Lymphoma and Multiple Myeloma Previously Failing Mobilization with G-CSF with or without Chemotherapy for Autologous Hematopoietic Stem Cell Mobilization: The Austrian Experience on a Named Patient Program. Transfusion 2011, 51, 968–975. [Google Scholar] [CrossRef] [PubMed]
- Gerlach, L.; Skerlj, R.; Schwartz, T.; Bridger, G. Molecular Interactions of Cyclam and Bicyclam Non-Peptide Antagonists with the CXCR4 Chemokine Receptor. J. Biol. Chem. 2001, 276, 14153–14160. [Google Scholar] [CrossRef] [PubMed]
- Matthys, P.; Hatse, S.; Vermeire, K.; Wuyts, A.; Bridger, G.; Henson, G.; De Clercq, E.; Billiau, A.; Schols, D. AMD3100, a Potent and Specific Antagonist of the Stromal Cell-Derived Factor-1 Chemokine Receptor CXCR4, Inhibits Autoimmune Joint Inflammation in IFN-Gamma Receptor-Deficient Mice. J. Immunol. 2001, 167, 4686–4692. [Google Scholar] [CrossRef]
- DiPersio, J.; Stadtmauer, E.; Nademanee, A.; Micaleff, I.; Stiff, P.; Kaufman, J.; Maziarz, R.; Hosing, C. Plerixafor and G-CSF versus Placebo and G-CSF to Mobilize Hematopoietic Stem Cells for Autologous Stem Cell Transplantation in Patients with Multiple Myeloma. Blood 2009, 113, 5720–5726. [Google Scholar] [CrossRef]
- DiPersio, J.; Micaleff, I.; Stiff, P.; Bolwell, B.; Maziarz, R.; Jacobsen, E.; Nademanee, A.; McCarty, J.; Bridger, G.; Calandra, G. Phase III Prospective Randomized Double-Blind Placebo-Controlled Trial of Plerixafor Plus Granulocyte Colony-Stimulating Factor Compared With Placebo Plus Granulocyte Colony-Stimulating Factor for Autologous Stem-Cell Mobilization and Transplantation for Patients with Non-Hodgkin’s Lymphoma. J. Clin. Oncol. 2009, 27, 4767–4773. [Google Scholar] [CrossRef]
- Steiner, N.; Göbel, G.; Michaeler, D.; Platz, A.; Prokop, W.; Wolf, A.; Wolf, D.; Duftner, C.; Gunsilius, E. Rheumatologic Diseases Impact the Risk of Progression of MGUS to Overt Multiple Myeloma. Blood Adv. 2021, 5, 1746–1754. [Google Scholar] [CrossRef]
- Al Hamed, R.; Bazarbachi, A.; Malard, F.; Harousseau, J.; Mohty, M. Current Status of Autologous Stem Cell Transplantation for Multiple Myeloma. Blood Cancer J. 2019, 9, 44. [Google Scholar] [CrossRef]
- Josting, A.; Reiser, M.; Rueffer, U.; Salzberger, B.; Diehl, V.; Engert, A. Treatment of Primary Progressive Hodgkin’s and Aggressive Non-Hodgkin’s Lymphoma: Is There a Chance for Cure? J. Clin. Oncol. 2000, 18, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Rancea, M.; Monsef, I.; von Tresckow, B.; Engert, A.; Skoetz, N. High-Dose Chemotherapy Followed by Autologous Stem Cell Transplantation for Patients with Relapsed/Refractory Hodgkin Lymphoma. Cochrane Database Syst. Rev. 2013, 6, CD009411. [Google Scholar] [CrossRef] [PubMed]
- Wullenkord, R.; Berning, P.; Niemann, A.; Wethmar, K.; Bergmann, S.; Lutz, M.; Schliemann, C.; Mesters, R.; Keßler, T.; Schmitz, N.; et al. The Role of Autologous Stem Cell Transplantation (ASCT) in Aggressive B-Cell Lymphomas: Real-World Data from a Retrospective Single-Center Analysis. Ann. Hematol. 2021, 100, 2733–2744. [Google Scholar] [CrossRef] [PubMed]
- Worel, N.; Fritsch, G.; Agis, H.; Böhm, A.; Engelich, G.; Leitner, G.; Geissler, K.; Gleixner, K.; Kalhs, P.; Buxhofer-Ausch, V.; et al. Plerixafor as Preemptive Strategy Results in High Success Rates in Autologous Stem Cell Mobilization Failure. J. Clin. Apher. 2017, 32, 224–234. [Google Scholar] [CrossRef]
- Prakash, V.; Malik, P.; Sahoo, R.; Pramanik, R.; Choudhary, P.; Varshney, A.; Kumar, L. Multiple Myeloma: Risk Adapted Use of Plerixafor for Stem Cell Mobilization Prior to Autologous Stem Cell Transplantation Is Effective and Cost Efficien. Clin. Lymphoma Myeloma Leuk. 2022, 22, 44–51. [Google Scholar] [CrossRef]
- Yuan, S.; Palmer, J.; Tsai, N.; Dagis, A.; Nademanee, A.; Wang, S. Engraftment and Outcomes Following Autologous Stem Cell Transplantation in Hodgkin Lymphoma Patients Mobilized with Plerixafor. Hematol. Oncol. 2017, 35, 281–287. [Google Scholar] [CrossRef]
- Mombled, M.; Rodriguez, L.; Avalon, M.; Duchez, P.; Vlaski-Lafarge, M.; Debeissat, C.; Pérard, B.; Sawai, K.; Pasquet, J.; Bijou, F.; et al. Characteristics of Cells with Engraftment Capacity within CD34+ Cell Population upon G-CSF and Plerixafor Mobilization. Leukemia 2020, 34, 3370–3381. [Google Scholar] [CrossRef]
- Sureda, A.; Chabannon, C.; Masszi, T.; Pohlreich, D.; Scheid, C.; Thieblemont, C.; Wahlin, B.; Sakellari, I.; Russel, N.; Janikova, A.; et al. Analysis of Data Collected in the European Society for Blood and Marrow Transplantation (EBMT) Registry on a Cohort of Lymphoma Patients Receiving Plerixafor. Bone Marrow Transpl. 2020, 55, 613–622. [Google Scholar] [CrossRef]
- Varmavuo, V.; Rimpiläinen, J.; Kuitunen, H.; Nihtinen, A.; Vasala, K.; Mikkola, M.; Kutila, A.; Lehtonen, P.; Kuittinen, T.; Mäntymaa, P.; et al. Engraftment and Outcome after Autologous Stem Cell Transplantation in Plerixafor-Mobilized Non-Hodgkin’s Lymphoma Patients. Transfusion 2014, 54, 1243–1250. [Google Scholar] [CrossRef]
- Hübel, K.; Ostermann, H.; Glaß, B.; Noppeney, R.; Kron, A.; Milkovich, G.; Mohty, M. Plerixafor in Non-Hodgkin’s Lymphoma Patients: A German Analysis of Time, Effort and Costs. Bone Marrow Transpl. 2019, 54, 123–129. [Google Scholar] [CrossRef]
- Mohty, M.; Azar, N.; Chabannon, C.; Le Gouill, S.; Karlin, L.; Farina, L.; Milkovich, G.; Ostermann, H.; Glaß, B.; Noppeney, R.; et al. Plerixafor in Poor Mobilizers with Non-Hodgkin’s Lymphoma: A Multi-Center Time-Motion Analysis. Bone Marrow Transpl. 2018, 53, 246–254. [Google Scholar] [CrossRef]
- Gordan, L.; Sugrue, M.; Lynch, J.; Wiliams, K.; Khan, S.; Wingard, J.; Moreb, J. Poor Mobilization of Peripheral Blood Stem Cells Is a Risk Factor for Worse Outcome in Lymphoma Patients Undergoing Autologous Stem Cell Transplantation. Leuk. Lymphoma 2003, 44, 815–820. [Google Scholar] [CrossRef]
- Tricot, G.; Jagannath, S.; Vesole, D.; Nelson, J.; Tindle, S.; Miller, L.; Cheson, B.; Crowley, J.; Barlogie, B. Peripheral Blood Stem Cell Transplants for Multiple Myeloma: Identification of Favorable Variables for Rapid Engraftment in 225 Patients. Blood 1995, 85, 588–596. [Google Scholar] [CrossRef]
- Moreb, J.; Byrne, M.; Shugarman, I.; Zou, F.; Yiong, S.; May, W.; Norking, M.; Hiemenz, J.; Brown, R.; Cogle, C.; et al. Poor Peripheral Blood Stem Cell Mobilization Affects Long-Term Outcomes in Multiple Myeloma Patients Undergoing Autologous Stem Cell Transplantation. J. Clin. Apher. 2018, 33, 29–37. [Google Scholar] [CrossRef]
- Chua, C.; Lim, H.; Chai, K.; Ong, J.; Sim, S.; Wood, C.; Dickinson, M.; Campbell, P.; Hempton, J.; King, H.; et al. Peripheral Blood Stem Cell Mobilisation with G-CSF Alone versus G-CSF and Cyclophosphamide after Bortezomib, Cyclophosphamide and Dexamethasone Induction in Multiple Myeloma. Bone Marrow Transpl. 2018, 53, 1116–1123. [Google Scholar] [CrossRef]
- Bakeer, M.; Zubair, A.; Roy, V. Low Baseline Platelet Count Predicts Poor Response to Plerixafor in Patients with Multiple Myeloma Undergoing Autologous Stem Cell Mobilization. Cytotherapy 2020, 22, 16–20. [Google Scholar] [CrossRef]
- Douglas, K.; Gilleece, M.; Hayden, P.; Hunter, H.; Johnson, P.; Kallmeyer, C.; Malladi, R.; Paneesha, S.; Pawson, R.; Quinn, M.; et al. UK Consensus Statement on the Use of Plerixafor to Facilitate Autologous Peripheral Blood Stem Cell Collection to Support High-Dose Chemoradiotherapy for Patients with Malignancy. J. Clin. Apher. 2018, 33, 46–59. [Google Scholar] [CrossRef]
- Zannetti, B.; Saraceni, F.; Cellini, C.; Fabbri, E.; Monaco, F.; Guarini, A.; Laszlo, D.; Martino, M.; Olivieri, A.; Imola, M.; et al. Low-Dose Cyclophosphamide versus Intermediate-High-Dose Cyclophosphamide versus Granulocyte Colony-Stimulating Factor Alone for Stem Cell Mobilization in Multiple Myeloma in the Era of Novel Agents: A Multicenter Retrospective Study. Transpl. Cell. Ther. 2021, 27, 244.e1–244.e8. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Xiang, H.; Yan, Y.; Deng, Z.; Li, H.; Li, X.; Liu, J. Correction to: Comparison of the Efficiency, Safety, and Survival Outcomes in Two Stem Cell Mobilization Regimens with Cyclophosphamide plus G-CSF or G-CSF Alone in Multiple Myeloma: A Meta-Analysis. Ann. Hematol. 2021, 100, 575. [Google Scholar] [CrossRef] [PubMed]
- Crocchiolo, R.; Chabannon, C.; El-Cheikh, J.; Esterni, B.; Lemarié, C.; Fürst, S.; Castagna, L.; Bouabdallah, R.; Ladaique, P.; Coso, D.; et al. Poor Autologous Mobilization Status Does Not Impact on Hematological Recovery but Affects Outcome after Allogeneic Stem Cell Transplant for Lymphoma and Myeloma. Leuk. Lymphoma 2013, 54, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Pavone, V.; Gaudio, F.; Console, G.; Vitolo, U.; Iacopino, P.; Guarini, A.; Liso, V.; Perrone, T.; Liso, A. Poor Mobilization Is an Independent Prognostic Factor in Patients with Malignant Lymphomas Treated by Peripheral Blood Stem Cell Transplantation. Bone Marrow Transpl. 2006, 37, 719–724. [Google Scholar] [CrossRef]
- Wuchter, P.; Ran, D.; Bruckner, T.; Schmitt, T.; Witzens-Harig, M.; Neben, K.; Goldschmidt, H.; Ho, A. Poor Mobilization of Hematopoietic Stem Cells-Definitions, Incidence, Risk Factors, and Impact on Outcome of Autologous Transplantation. Bone Marrow Transpl. 2010, 16, 490–499. [Google Scholar] [CrossRef]
- Akhtar, S.; Weshi, A.; Rahal, M.; Khafaga, Y.; Tbakhi, A.; Humaidan, H.; Maghfoor, I. Factors Affecting Autologous Peripheral Blood Stem Cell Collection in Patients with Relapsed or Refractory Diffuse Large Cell Lymphoma and Hodgkin Lymphoma: A Single Institution Result of 168 Patient. Leuk. Lymphoma 2008, 49, 769–778. [Google Scholar] [CrossRef]
- Kuittinen, T.; Nousiainen, T.; Halonen, P.; Mahlamäki, E.; Jantunen, E. Prediction of Mobilisation Failure in Patients with Non-Hodgkin’s Lymphoma. Bone Marrow Transpl. 2004, 33, 907–912. [Google Scholar] [CrossRef]
- Mendrone, A.; Arrais, C.; Saboya, R.; Chamone, D.A.; Dulley, F. Factors Affecting Hematopoietic Progenitor Cell Mobilization: An Analysis of 307 Patients. Transfus. Apher. Sci. 2008, 39, 187–192. [Google Scholar] [CrossRef]
- Pusic, I.; Jiang, S.; Landua, S.; Uy, G.; Rettig, M.; Cashen, A.; Westervelt, P.; Vij, R.; Abboud, C.; Stockerl-Goldstein, K.; et al. Impact of Mobilization and Remobilization Strategies on Achieving Sufficient Stem Cell Yields for Autologous Transplantation. Biol. Blood Marrow Transpl. 2008, 14, 1045–1056. [Google Scholar] [CrossRef]
- Bensinger, W.; Appelbaum, F.; Rowley, S.; Storb, R.; Sanders, J.; Lilleby, K.; Gooley, T.; Demirer, T.; Schiffman, K.; Weaver, C. Factors that Influence Collection and Engraftment of Autologous Peripheral-Blood Stem Cells. J. Clin. Oncol. 1995, 13, 2547–2555. [Google Scholar] [CrossRef]
- Moskowitz, C.; Glassman, J.; Wuest, D.; Maslak, P.; Reich, L.; Gucciardo, A.; Coady-Lyons, N.; Zelenetz, A.; Nimer, S. Factors Affecting Mobilization of Peripheral Blood Progenitor Cells in Patients with Lymphoma. Clin. Cacer Res. 1998, 4, 311–316. [Google Scholar]
- Michallet, M.; Thiébaut, A.; Dreger, P.; Remes, K.; Milpied, N.; Santini, G.; Hamon, M.; Björkstrad, B.; Kimby, E.; Belhabri, A.; et al. Peripheral Blood Stem Cell (PBSC) Mobilization and Transplantation after Fludarabine Therapy in Chronic Lymphocytic Leukaemia (CLL): A Report of the European Blood and Marrow Transplantation (EBMT) CLL Subcommittee on Behalf of the EBMT Chronic Leukaemias Working Party (CLWP). Br. J. Haematol. 2000, 108, 595–601. [Google Scholar] [CrossRef]
- Deol, A.; Abrams, J.; Masood, A.; Al-Kadhimi, Z.; Abidi, M.; Ayash, L.; Lum, L.; Ratanatharathorn, V.; Uberti, J. Long-Term Follow up of Patients Proceeding to Transplant Using Plerixafor Mobilized Stem Cells and Incidence of Secondary Myelodysplastic Syndrome/AML. Bone Marrow Transpl. 2013, 48, 1112–1116. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Multiple Myeloma Patients | Plerixafor Group | G-CSF Group | p Value |
|---|---|---|---|
| Number of patients—N (%) | 108 (51) | 103 (49) | |
| Age at diagnosis (years)—median [IQR] | 59 [52–64] | 55 [47–62] | 0.01 |
| Gender | 0.6 | ||
| Male—N (%) | 63 (58) | 64 (62) | |
| Female—N (%) | 45 (42) | 39 (38) | |
| Bone marrow infiltration at diagnosis | 0.4 | ||
| Yes—N (%) | 91 (85) | 90 (88) | |
| No—N (%) | 4 (4) | 3 (3) | |
| n.a. | 13 (12) | 10 (10) | |
| Disease stage at diagnosis (ISS) | 0.9 | ||
| ISS I—N (%) | 48 (44) | 46 (45) | |
| ISS II—N (%) | 34 (32) | 28 (27) | |
| ISS III—N (%) | 22 (20) | 24 (23) | |
| n.a.—N (%) | 4 (4) | 5 (5) | |
| Chemomobilization—N (%) | 0 (0) | 0 (0) | |
| Prior lines of therapy | 0.04 | ||
| 1—N (%) | 108 (100) | 97 (94) | |
| 2—N (%) | 0 (0) | 3 (3) | |
| ≥3—N (%) | 0 (0) | 3 (3) | |
| Prior radiotherapy | 0.2 | ||
| Yes—N (%) | 39 (36) | 28 (27) | |
| No—N (%) | 69 (64) | 75 (73) | |
| Disease status at ASCT | <0.001 | ||
| CR, nCR, sCR—N (%) | 42 (39) | 16 (16) | |
| VGPR—N (%) | 27 (25) | 36 (35) | |
| PR—N (%) | 28 (26) | 26 (25) | |
| SD—N (%) | 2 (2) | 1 (1) | |
| PD—N (%) | 8 (7) | 5 (5) | |
| n.a.—N (%) | 1 (1) | 19 (18) |
| Lymphoma Patients | Plerixafor Group | G-CSF Group | p Value |
|---|---|---|---|
| Number of Patients —N (%) | 82 (55) | 67 (45) | |
| DLBCL | 29 (35) | 17 (25) | |
| MCL | 10 (12) | 15 (22) | |
| FL | 8 (10) | 5 (8) | |
| HL | 9 (11) | 4 (6) | |
| Burkitt’s lymphoma | 5 (6) | 6 (9) | |
| AITL | 5 (6) | 3 (5) | |
| TLBL | 7 (9) | 0 (0) | |
| PTCL | 4 (5) | 2 (3) | |
| Primary CNS lymphoma | 1 (1) | 4 (6) | |
| Other B/T-NHL | 4 (5) | 11 (16) | |
| Age at diagnosis (years)—median [IQR] | 52 [44–58] | 49 [41–57] | 0.4 |
| Gender | 0.8 | ||
| Male—N (%) | 57 (70) | 45 (67) | |
| Female—N (%) | 25 (30) | 22 (33) | |
| Bone marrow infiltration at diagnosis | 0.4 | ||
| Yes—N (%) | 12 (15) | 16 (24) | |
| No—N (%) | 48 (58) | 35 (52) | |
| n.a. | 22 (27) | 16 (24) | |
| Disease stage at diagnosis (Ann Arbor) | 0.4 | ||
| I–II N (%) | 18 (22) | 7 (11) | |
| III–IV N (%) | 60 (74) | 42 (62) | |
| n.a.—N (%) | 4 (5) | 18 (27) | |
| Chemomobilization—N (%) | 82 (100) | 67 (100) | |
| Prior lines of therapy | 0.8 | ||
| 1—N (%) | 22 (27) | 16 (24) | |
| 2—N (%) | 43 (52) | 39 (58) | |
| ≥3—N (%) | 17 (21) | 12 (18) | |
| Prior radiotherapy | 0.8 | ||
| Yes—N (%) | 11 (13) | 10 (15) | |
| No—N (%) | 71 (87) | 57 (85) | |
| Disease status at ASCT | 0.08 | ||
| CR—N (%) | 40 (49) | 29 (43) | |
| PR—N (%) | 25 (30.5) | 21 (31) | |
| SD—N (%) | 8 (10) | 1 (1.5) | |
| Mixed response—N (%) | 0 (0) | 1 (1.5) | |
| PD—N (%) | 2 (2) | 5 (8) |
| Multiple Myeloma Patients | Plerixafor Group | G-CSF Group | p Value |
|---|---|---|---|
| Number of stem cell mobilized patients—N (%) | 108 (51) | 103 (49) | |
| Total number of CD34+ cells collected (×106/kg)—median [IQR] | 6.5 [4.9–8.8] | 5.7 [4.8–7.7] | 0.2 |
| Total number of apheresis procedures | 0.9 | ||
| 1—N (%) | 83 (77) | 78 (76) | |
| 2—N (%) | 19 (17.5) | 20 (19) | |
| 3—N (%) | 6 (5.5) | 5 (5) | |
| Success defined as: | |||
| ≥4 × 106/kg CD34+ cells—N (%) | 93 (86) | 98 (95) | 0.03 |
| Success in a single apheresis procedure—N (%) | 81 (75) | 76 (74) | 0.8 |
| Number of patients receiving a first ASCT | 100 (93) | 103 (100) | 0.02 |
| Transplanted CD34+ cell number (×106/kg)—median [IQR] | 3.5 [2.7–4.9] | 3.8 [2.6–5.3] | 0.9 |
| Time to neutrophil engraftment—median [range] | 12 [8–15] | 12 [9–20] | 0.9 |
| Time to platelet engraftment—median [range] | 12 [8–25] | 11 [8–34] | 0.1 |
| Number of red cell transfusions—median [range] | 1.5 [0–12] | 0 [0–10] | 0.6 |
| Number of platelet transfusions—median [range] | 2 [0–14] | 2 [0–12] | 0.1 |
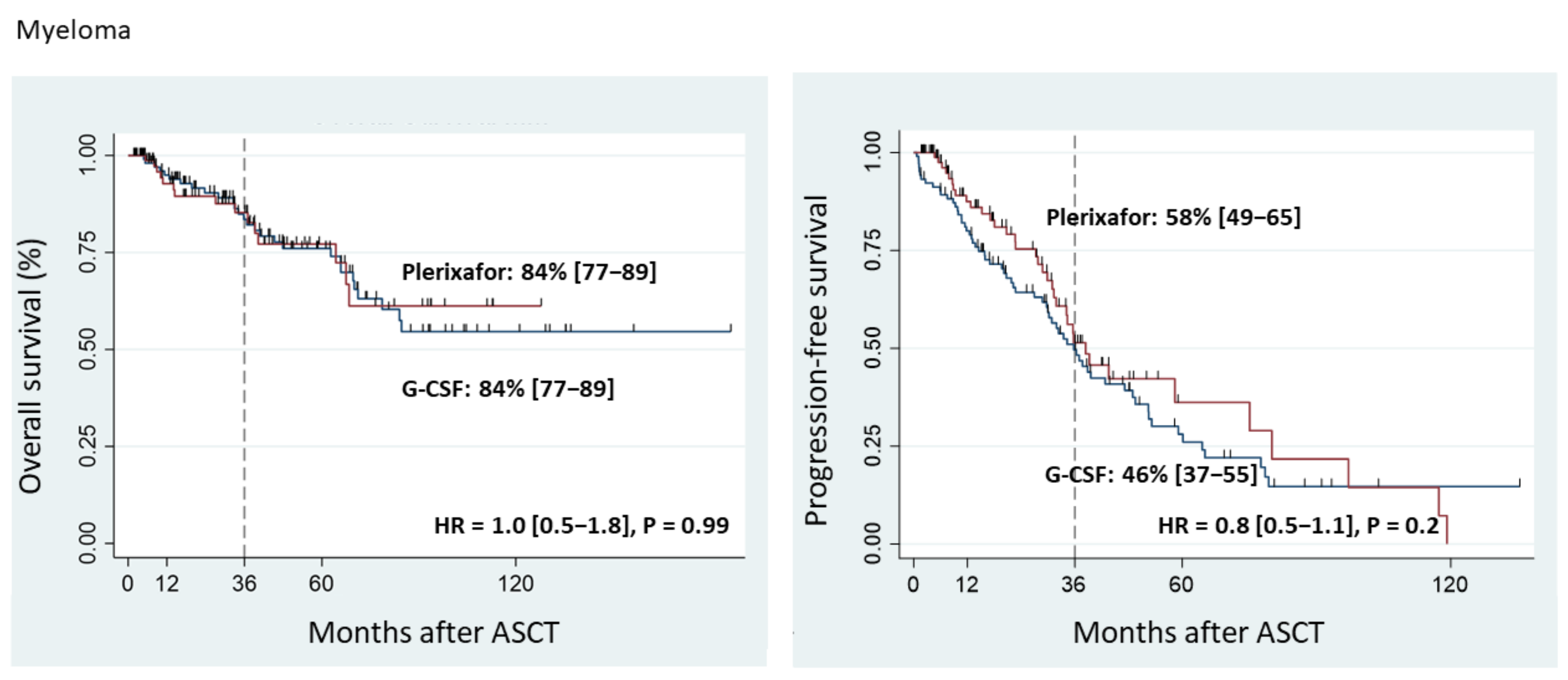
| 3-year progression-free survival—months % (95% CI) | 58 (49–65) | 46 (37–55) | 0.2 |
| 3-year overall survival—months % (95% CI) | 84 (77–89) | 84 (77–89) | 0.9 |
| Secondary malignancies—N (%) | 4 (4) | 4(4) | 0.9 |
| Lymphoma Patients | Plerixafor Group | G-CSF Group | p Value |
|---|---|---|---|
| Number of stem cell mobilized patients—N (%) | 79 (54) | 67 (46) | |
| Total number of CD34+ cells collected (×106/kg)—median [IQR] | 3.3 [2.2–6.1] | 5.6 [3.4–11.0] | <0.001 |
| Total number of apheresis procedures | 0.02 | ||
| 1—N (%) | 52 (66) | 58 (87) | |
| 2—N (%) | 24 (30) | 7 (10) | |
| 3—N (%) | 2 (3) | 2 (3) | |
| 4—N (%) | 1 (1) | 0 (0) | |
| Success defined as: | |||
| ≥2 × 106/kg CD34+ cells—N (%) | 69 (87) | 67 (100) | 0.003 |
| Success in a single apheresis procedure—N (%) | 52 (67) | 60 (91) | <0.001 |
| Number of patients receiving a first ASCT—N (%) | 57 (79) | 67 (100) | <0.001 |
| Transplanted CD34+ cell number (×106/kg)—median [IQR] | 4.0 [2.4–6.2] | 5.2 [3.2–9.3] | 0.03 |
| Time to neutrophil engraftment—median [range] | 11 [8–14] | 10 [8–16] | 0.0004 |
| Time to platelet engraftment—median [range] | 13 [5–59] | 12 [5–17] | 0.04 |
| Number of red cell transfusions—median [range] | 4 [0–24] | 2 [0–10] | 0.43 |
| Number of platelet transfusions—median [range] | 5 [1–54] | 3 [1–20] | 0.01 |
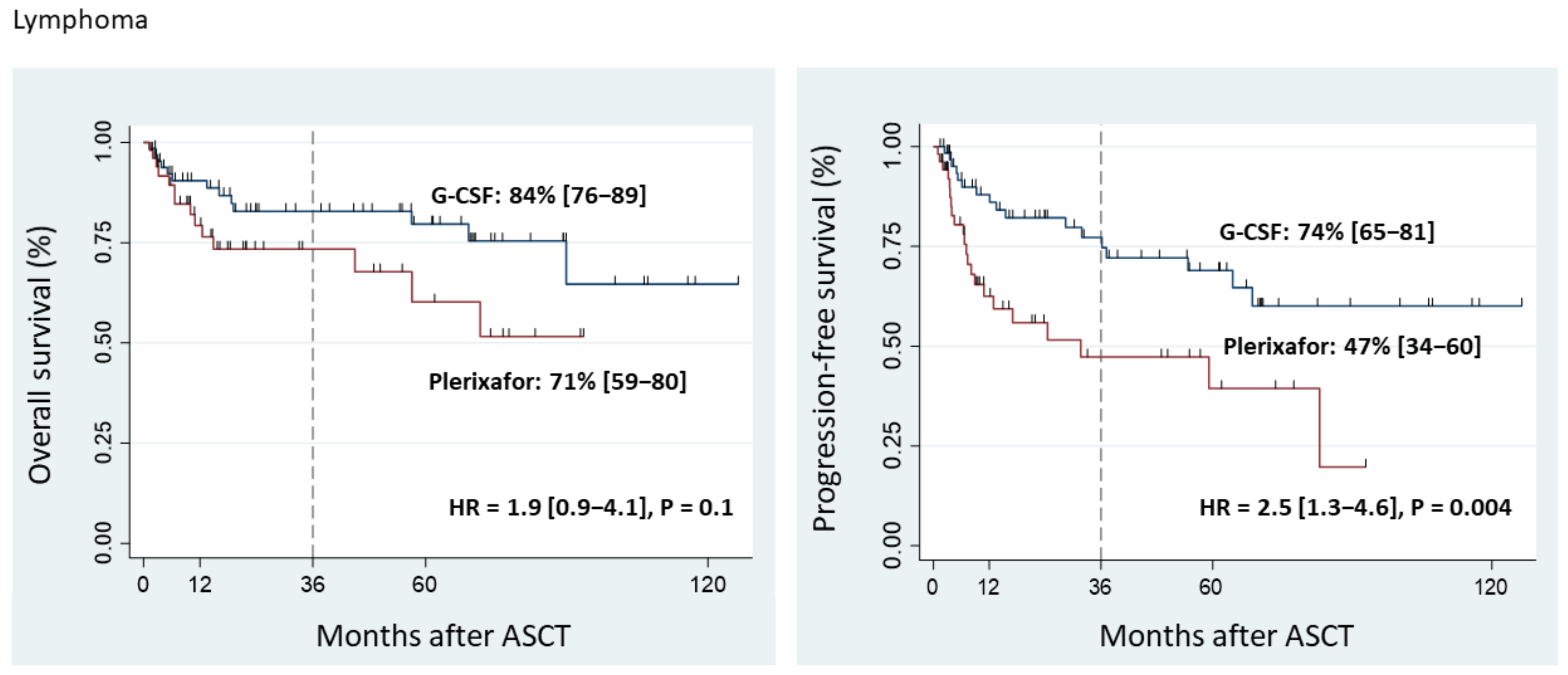
| 3-year progression-free survival—months % (95% CI) | 47 (34–60) | 74 (65–81) | 0.003 |
| 3-year overall survival—months % (95% CI) | 71 (59–80) | 84 (76–89) | 0.1 |
| Secondary malignancies | 5 (6) | 1 (1.5) | 0.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steiner, N.; Göbel, G.; Mauser, L.; Mühlnikel, L.; Fischinger, M.; Künz, T.; Willenbacher, W.; Hetzenauer, G.; Rudzki, J.; Nussbaumer, W.; et al. Poor Mobilizers in Lymphoma but Not Myeloma Patients Had Significantly Poorer Progression-Free Survival after Autologous Stem Cell Transplantation: Results of a Large Retrospective, Single-Center Observational Study. Cancers 2023, 15, 608. https://doi.org/10.3390/cancers15030608
Steiner N, Göbel G, Mauser L, Mühlnikel L, Fischinger M, Künz T, Willenbacher W, Hetzenauer G, Rudzki J, Nussbaumer W, et al. Poor Mobilizers in Lymphoma but Not Myeloma Patients Had Significantly Poorer Progression-Free Survival after Autologous Stem Cell Transplantation: Results of a Large Retrospective, Single-Center Observational Study. Cancers. 2023; 15(3):608. https://doi.org/10.3390/cancers15030608
Chicago/Turabian StyleSteiner, Normann, Georg Göbel, Leonie Mauser, Lena Mühlnikel, Marie Fischinger, Tina Künz, Wolfgang Willenbacher, Gabriele Hetzenauer, Jakob Rudzki, Walter Nussbaumer, and et al. 2023. "Poor Mobilizers in Lymphoma but Not Myeloma Patients Had Significantly Poorer Progression-Free Survival after Autologous Stem Cell Transplantation: Results of a Large Retrospective, Single-Center Observational Study" Cancers 15, no. 3: 608. https://doi.org/10.3390/cancers15030608
APA StyleSteiner, N., Göbel, G., Mauser, L., Mühlnikel, L., Fischinger, M., Künz, T., Willenbacher, W., Hetzenauer, G., Rudzki, J., Nussbaumer, W., Mayer, W., Gunsilius, E., Kircher, B., Wolf, D., & Nachbaur, D. (2023). Poor Mobilizers in Lymphoma but Not Myeloma Patients Had Significantly Poorer Progression-Free Survival after Autologous Stem Cell Transplantation: Results of a Large Retrospective, Single-Center Observational Study. Cancers, 15(3), 608. https://doi.org/10.3390/cancers15030608