Development of an Individualized Prediction Calculator for the Benefit of Postoperative Radiotherapy in Patients with Surgically Resected De Novo Stage IV Breast Cancer

 , ,
, ,
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
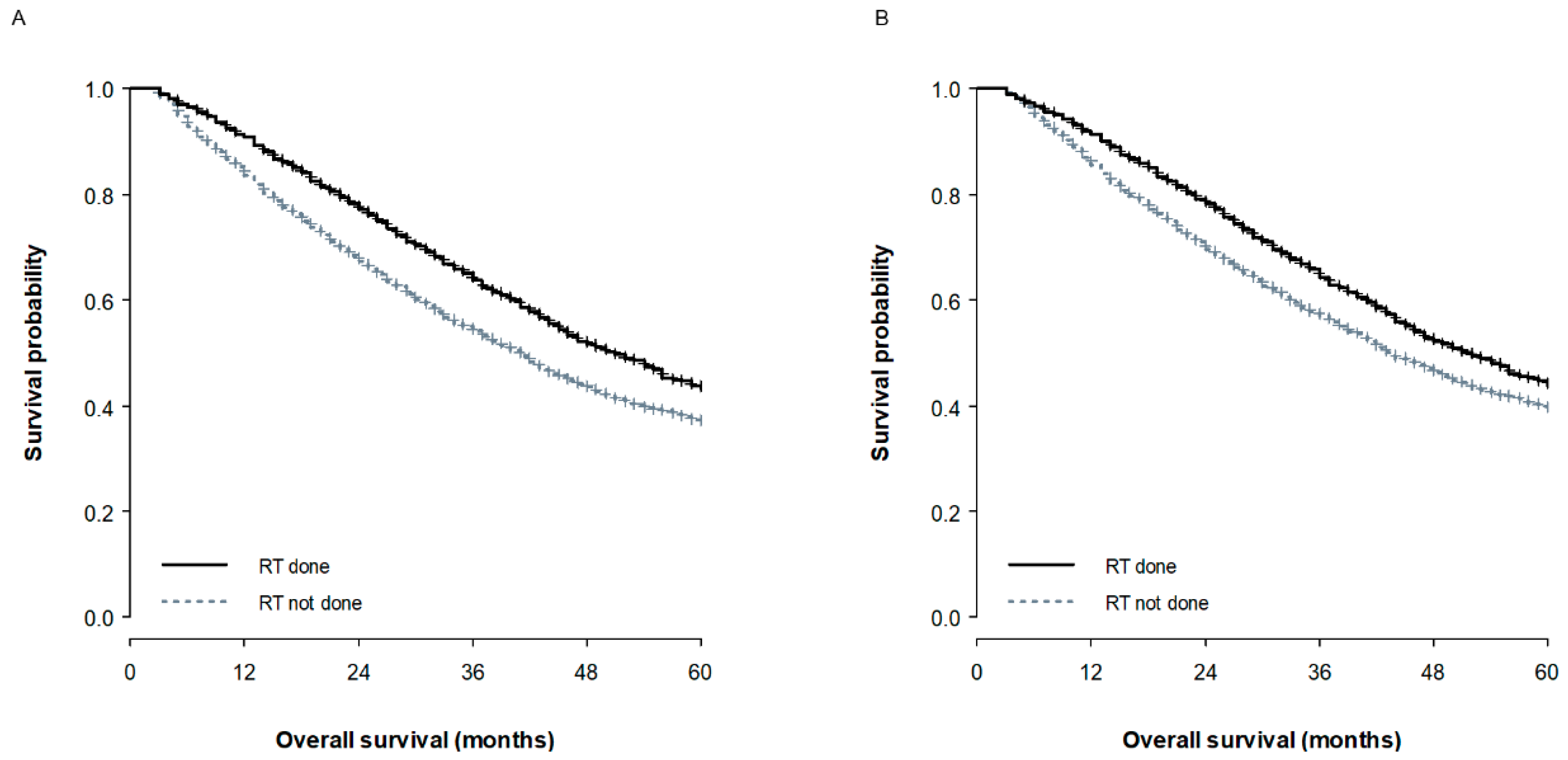
2.2. Survival Analysis for the Entire Cohort
2.3. Propensity Score Matched Survival Analysis
2.4. Development of a Nomogram and a Web-Based Survival Calculator
3. Discussion
4. Materials and Methods
4.1. Patient Cohort
4.2. Clinicopathological Variables
4.3. Statistical Analysis and the Development of a Nomogram and Web-Based Calculator
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Heller, D.R.; Chiu, A.S.; Farrell, K.; Killelea, B.K.; Lannin, D.R. Why Has Breast Cancer Screening Failed to Decrease the Incidence of de Novo Stage IV Disease? Cancers 2019, 11, 500. [Google Scholar] [CrossRef]
- Pagani, O.; Senkus, E.; Wood, W.; Colleoni, M.; Cufer, T.; Kyriakides, S.; Costa, A.; Winer, E.P.; Cardoso, F. ESO-MBC Task Force International guidelines for management of metastatic breast cancer: Can metastatic breast cancer be cured? J. Natl. Cancer Inst. 2010, 102, 456–463. [Google Scholar] [CrossRef]
- Chia, S.K.; Speers, C.H.; D’yachkova, Y.; Kang, A.; Malfair-Taylor, S.; Barnett, J.; Coldman, A.; Gelmon, K.A.; O’reilly, S.E.; Olivotto, I.A. The impact of new chemotherapeutic and hormone agents on survival in a population-based cohort of women with metastatic breast cancer. Cancer 2007, 110, 973–979. [Google Scholar] [CrossRef]
- Liao, Y.; Fan, X.; Wang, X. Effects of different metastasis patterns, surgery and other factors on the prognosis of patients with stage IV non-small cell lung cancer: A Surveillance, Epidemiology, and End Results (SEER) linked database analysis. Oncol. Lett. 2019, 18, 581–592. [Google Scholar] [CrossRef]
- Leone, B.A.; Vallejo, C.T.; Romero, A.O.; Machiavelli, M.R.; Pérez, J.E.; Leone, J.; Leone, J.P. Prognostic impact of metastatic pattern in stage IV breast cancer at initial diagnosis. Breast Cancer Res. Treat. 2017, 161, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Bertaut, A.; Mounier, M.; Desmoulins, I.; Guiu, S.; Beltjens, F.; Darut-Jouve, A.; Ponnelle, T.; Arnould, L.; Arveux, P. Stage IV breast cancer: A population-based study about prognostic factors according to HER2 and HR status. Eur. J. Cancer Care (Engl.) 2015, 24, 920–928. [Google Scholar] [CrossRef]
- Bale, R.; Putzer, D.; Schullian, P. Local Treatment of Breast Cancer Liver Metastasis. Cancers 2019, 11, 1341. [Google Scholar] [CrossRef]
- Nguyen, D.H.A.; Truong, P.T.; Alexander, C.; Walter, C.V.; Hayashi, E.; Christie, J.; Lesperance, M. Can locoregional treatment of the primary tumor improve outcomes for women with stage IV breast cancer at diagnosis? Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 39–45. [Google Scholar] [CrossRef]
- Lang, J.E.; Tereffe, W.; Mitchell, M.P.; Rao, R.; Feng, L.; Meric-Bernstam, F.; Bedrosian, I.; Kuerer, H.M.; Hunt, K.K.; Hortobagyi, G.N.; et al. Primary tumor extirpation in breast cancer patients who present with stage IV disease is associated with improved survival. Ann. Surg. Oncol. 2013, 20, 1893–1899. [Google Scholar] [CrossRef]
- Rapiti, E.; Verkooijen, H.M.; Vlastos, G.; Fioretta, G.; Neyroud-Caspar, I.; Sappino, A.P.; Chappuis, P.O.; Bouchardy, C. Complete excision of primary breast tumor improves survival of patients with metastatic breast cancer at diagnosis. J. Clin. Oncol. 2006, 24, 2743–2749. [Google Scholar] [CrossRef] [PubMed]
- Gnerlich, J.; Jeffe, D.B.; Deshpande, A.D.; Beers, C.; Zander, C.; Margenthaler, J.A. Surgical removal of the primary tumor increases overall survival in patients with metastatic breast cancer: Analysis of the 1988-2003 SEER data. Ann. Surg. Oncol. 2007, 14, 2187–2194. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.M.; Kim, J.Y.; Park, H.S.; Park, S.; Kim, G.M.; Sohn, J.; Kim, S.I. Effect of primary tumor resection on overall survival in patients with stage IV breast cancer. Breast J. 2019, 25, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Mudgway, R.; Chavez de Paz Villanueva, C.; Lin, A.C.; Senthil, M.; Garberoglio, C.A.; Lum, S.S. The Impact of Primary Tumor Surgery on Survival in HER2 Positive Stage IV Breast Cancer Patients in the Current Era of Targeted Therapy. Ann. Surg. Oncol. 2020, 27, 2711–2720. [Google Scholar] [CrossRef]
- Harris, E.; Barry, M.; Kell, M.R. Meta-analysis to determine if surgical resection of the primary tumour in the setting of stage IV breast cancer impacts on survival. Ann. Surg. Oncol. 2013, 20, 2828–2834. [Google Scholar] [CrossRef]
- Soran, A.; Ozmen, V.; Ozbas, S.; Karanlik, H.; Muslumanoglu, M.; Igci, A.; Canturk, Z.; Utkan, Z.; Ozaslan, C.; Evrensel, T.; et al. Randomized Trial Comparing Resection of Primary Tumor with No Surgery in Stage IV Breast Cancer at Presentation: Protocol MF07-01. Ann. Surg. Oncol. 2018, 25, 3141–3149. [Google Scholar] [CrossRef]
- Badwe, R.; Hawaldar, R.; Nair, N.; Kaushik, R.; Parmar, V.; Siddique, S.; Budrukkar, A.; Mittra, I.; Gupta, S. Locoregional treatment versus no treatment of the primary tumour in metastatic breast cancer: An open-label randomised controlled trial. Lancet Oncol. 2015, 16, 1380–1388. [Google Scholar] [CrossRef]
- Fitzal, F.; Bjelic-Radisic, V.; Knauer, M.; Steger, G.; Hubalek, M.; Balic, M.; Singer, C.; Bartsch, R.; Schrenk, P.; Soelkner, L.; et al. Impact of Breast Surgery in Primary Metastasized Breast Cancer: Outcomes of the Prospective Randomized Phase III ABCSG-28 POSYTIVE Trial. Ann. Surg. 2019, 269, 1163–1169. [Google Scholar] [CrossRef]
- Early Surgery or Standard Palliative Therapy in Treating Patients with Stage IV Breast Cancer—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT01242800 (accessed on 17 July 2019).
- Mauro, G.P.; de Andrade Carvalho, H.; Stuart, S.R.; Mano, M.S.; Marta, G.N. Effects of locoregional radiotherapy in patients with metastatic breast cancer. Breast 2016, 28, 73–78. [Google Scholar] [CrossRef]
- Lane, W.O.; Thomas, S.M.; Blitzblau, R.C.; Plichta, J.K.; Rosenberger, L.H.; Fayanju, O.M.; Hyslop, T.; Hwang, E.S.; Greenup, R.A. Surgical Resection of the Primary Tumor in Women With De Novo Stage IV Breast Cancer: Contemporary Practice Patterns and Survival Analysis. Ann. Surg. 2019, 269, 537–544. [Google Scholar] [CrossRef]
- Choi, S.H.; Kim, J.W.; Choi, J.; Sohn, J.; Kim, S.I.; Park, S.; Park, H.S.; Jeong, J.; Suh, C.-O.; Keum, K.C.; et al. Locoregional Treatment of the Primary Tumor in Patients With De Novo Stage IV Breast Cancer: A Radiation Oncologist’s Perspective. Clin. Breast Cancer 2018, 18, e167–e178. [Google Scholar] [CrossRef] [PubMed]
- Bourgier, C.; Khodari, W.; Vataire, A.-L.; Pessoa, E.L.; Dunant, A.; Delaloge, S.; Uzan, C.; Balleyguier, C.; Mathieu, M.-C.; Marsiglia, H.; et al. Breast radiotherapy as part of loco-regional treatments in stage IV breast cancer patients with oligometastatic disease. Radiother. Oncol. 2010, 96, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Hazard, H.W.; Gorla, S.R.; Scholtens, D.; Kiel, K.; Gradishar, W.J.; Khan, S.A. Surgical resection of the primary tumor, chest wall control, and survival in women with metastatic breast cancer. Cancer 2008, 113, 2011–2019. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhao, J.; Zhu, L.; Su, F.; Chen, K. Development and validation of a nomogram predicting the overall survival of stage IV breast cancer patients. Cancer Med. 2017, 6, 2586–2594. [Google Scholar] [CrossRef] [PubMed]
- Corradini, S.; Ballhausen, H.; Weingandt, H.; Freislederer, P.; Schönecker, S.; Niyazi, M.; Simonetto, C.; Eidemüller, M.; Ganswindt, U.; Belka, C. Left-sided breast cancer and risks of secondary lung cancer and ischemic heart disease: Effects of modern radiotherapy techniques. Strahlenther. Onkol. 2018, 194, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Chang, J.S.; Choi, S.H.; Kim, Y.B.; Keum, K.C.; Suh, C.-O.; Yang, G.; Cho, Y.; Kim, J.W.; Lee, I.J. Radiotherapy for initial clinically positive internal mammary nodes in breast cancer. Radiat. Oncol. J. 2019, 37, 91–100. [Google Scholar] [CrossRef]
- Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Incidence—SEER 18 Regs Custom Data (with additional treatment fields), Nov 2018 Sub (1975-2016 varying)—Linked To County Attributes—Total U.S., 1969–2017 Counties. National Cancer Institute, DCCPS, Surveillance Research Program 2018. Available online: https://seer.cancer.gov/data/citation.html (accessed on 5 May 2020).
- Li, C.I.; Uribe, D.J.; Daling, J.R. Clinical characteristics of different histologic types of breast cancer. Br. J. Cancer 2005, 93, 1046–1052. [Google Scholar] [CrossRef]
- George, B.; Seals, S.; Aban, I. Survival analysis and regression models. J. Nucl. Cardiol. 2014, 21, 686–694. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number of Patients (%) | |
|---|---|---|
| Age at diagnosis | Median (IQR), years | 59 (49–68) |
| ≤50 years | 1227 (27.4) | |
| 51–70 years | 2307 (51.6) | |
| >70 years | 939 (21.0) | |
| Sex | Male | 62 (1.4) |
| Female | 4411 (98.6) | |
| Race * | White | 3380 (75.7) |
| Black | 732 (16.4) | |
| American Indian/Alaska Native | 325 (7.3) | |
| Asian or Pacific Islander | 27 (0.6) | |
| Year of diagnosis | 2010 | 1001 (22.4) |
| 2011 | 944 (21.1) | |
| 2012 | 925 (20.7) | |
| 2013 | 833 (18.6) | |
| 2014 | 770 (17.2) | |
| Laterality * | Right | 2183 (48.9) |
| Left | 2285 (51.1) | |
| T Stage * | 1 | 653 (15.1) |
| 2 | 1638 (37.8) | |
| 3 | 813 (18.8) | |
| 4 | 1227 (28.3) | |
| N stage * | 0 | 292 (6.9) |
| 1 | 1532 (36.5) | |
| 2 | 2343 (55.7) | |
| 3 | 36 (0.9) | |
| Histologic grade * | Well differentiated | 292 (6.9) |
| Moderately differentiated | 1532 (36.5) | |
| Poorly differentiated | 2343 (55.7) | |
| Undifferentiated | 36 (0.9) | |
| Hormone receptor * | Negative | 1066 (25.4) |
| Positive | 3123 (74.6) | |
| HER2 receptor * | Negative | 3076 (73.4) |
| Positive | 1113 (26.6) | |
| Bone metastasis * | Absent | 1914 (43.6) |
| Present | 2479 (56.4) | |
| Brain metastasis * | Absent | 4203 (96.8) |
| Present | 137 (3.2) | |
| Liver metastasis * | Absent | 3525 (80.7) |
| Present | 842 (19.3) | |
| Lung metastasis * | Absent | 3347 (76.8) |
| Present | 1012 (23.2) | |
| Breast operation | Mastectomy | 1256 (28.3) |
| Lumpectomy | 3181 (71.7) | |
| Chemotherapy | Not done/unknown | 1447 (32.3) |
| Done | 3026 (67.7) | |
| Radiotherapy | Not done/unknown | 2683 (60.0) |
| Done | 1790 (40.0) |
| Unmatched Cohort | Propensity Score Matched Cohort | ||||||
|---|---|---|---|---|---|---|---|
| Characteristics | Non-RT Group (n = 2683) | RT Group (n = 1790) | p | Non-RT Group (n = 1653) | RT Group (n = 1653) | p | |
| Age at diagnosis | Median (IQR), years | 61 (51–71) | 57 (48–65) | <0.001 | 57 (48–66) | 58 (48–65) | 0.716 |
| Race | White/others | 2223 (82.9) | 1517 (84.7) | 0.094 | 1395 (84.4) | 1401 (84.8) | 0.773 |
| Black | 460 (17.1) | 273 (15.3) | 258 (15.6) | 252 (15.2) | |||
| T stage | 1 | 444 (16.5) | 240 (13.4) | 0.002 | 242 (14.6) | 223 (13.5) | 0.299 |
| 2 | 1015 (37.8) | 675 (37.7) | 612 (37.0) | 629 (38.1) | |||
| 3 | 512 (19.1) | 321 (17.9) | 324 (19.6) | 293 (17.7) | |||
| 4 | 712 (26.5) | 554 (30.9) | 475 (28.7) | 508 (30.7) | |||
| N stage | 0–2 | 2133 (79.5) | 1331 (74.4) | < 0.001 | 1240 (75.0) | 1239 (75.0) | 0.968 |
| 3 | 550 (20.5) | 459 (25.6) | 413 (25.0) | 414 (25.0) | |||
| Grade | 1–2 | 1176 (43.8) | 762 (42.6) | 0.404 | 718 (43.4) | 703 (42.5) | 0.598 |
| 3–4 | 1507 (56.2) | 1028 (57.4) | 935 (56.6) | 950 (57.5) | |||
| Hormone receptor | Negative | 693 (25.8) | 439 (24.5) | 0.326 | 411 (24.9) | 405 (24.5) | 0.809 |
| Positive | 1990 (74.2) | 1351 (75.5) | 1242 (75.1) | 1248 (75.5) | |||
| HER2 receptor | Negative | 1981 (73.8) | 1330 (74.3) | 0.727 | 1230 (74.4) | 1223 (74.0) | 0.781 |
| Positive | 702 (26.2) | 460 (25.7) | 423 (25.6) | 430 (26.0) | |||
| Breast operation | Mastectomy | 721 (26.9) | 549 (30.7) | 0.006 | 493 (29.8) | 487 (29.5) | 0.819 |
| Lumpectomy | 1962 (73.1) | 1241 (69.3) | 1160 (70.2) | 1166 (70.5) | |||
| Chemotherapy | Not done/unknown | 1043 (38.9) | 404 (22.6) | <0.001 | 412 (24.9) | 395 (23.9) | 0.491 |
| Done | 1640 (61.1) | 1386 (77.4) | 1241 (75.1) | 1258 (76.1) | |||
| Bone metastasis | Absent | 1230 (45.8) | 726 (40.6) | <0.001 | 660 (39.9) | 672 (40.7) | 0.670 |
| Present | 1453 (54.2) | 1064 (59.4) | 993 (60.1) | 981 (59.3) | |||
| Brain metastasis | Absent | 2644 (98.5) | 1681 (93.9) | <0.001 | 1614 (97.6) | 1602 (96.9) | 0.200 |
| Present | 39 (1.5) | 109 (6.1) | 39 (2.4) | 51 (3.1) | |||
| Liver metastasis | Absent | 2090 (77.9) | 1522 (85.0) | <0.001 | 1381 (83.5) | 1397 (84.5) | 0.447 |
| Present | 593 (22.1) | 268 (15.0) | 272 (16.5) | 256 (15.5) | |||
| Lung metastasis | Absent | 1955 (72.9) | 1483 (82.8) | <0.001 | 1370 (82.9) | 1365 (82.6) | 0.818 |
| Present | 728 (27.1) | 307 (17.2) | 283 (17.1) | 288 (17.4) | |||
| No of metastatic site | 0 | 483 (18.0) | 399 (22.3) | <0.001 | 357 (21.6) | 376 (22.7) | 0.759 |
| 1 | 1679 (62.6) | 1101 (61.5) | 1047 (63.3) | 1025 (62.0) | |||
| 2 | 432 (16.1) | 229 (12.8) | 210 (12.7) | 417 (12.6) | |||
| 3–4 | 89 (3.3) | 61 (3.4) | 39 (2.4) | 84 (2.5) | |||
| Characteristics | 3-Year OS (%) | Univariate Analysis a | Multivariate Analysis b | TR c (95% CI) | |
|---|---|---|---|---|---|
| Age at diagnosis | <0.001 | <0.001 | 0.99 (0.98–0.99) | ||
| Race | White/others | 63.0 | <0.001 | <0.001 | 1 |
| Black | 47.6 | 0.72 (0.65–0.80) | |||
| T stage | 1 | 70.3 | <0.001 | 1 | |
| 2 | 63.9 | 0.020 | 0.87 (0.77–0.98) | ||
| 3 | 59.9 | 0.001 | 0.80 (0.70–0.91) | ||
| 4 | 52.3 | <0.001 | 0.71 (0.62–0.80) | ||
| N stage | 0–2 | 62.3 | <0.001 | <0.001 | 1 |
| 3 | 55.7 | 0.85 (0.78–0.92) | |||
| Grade | 1–2 | 70.7 | <0.001 | <0.001 | 1 |
| 3–4 | 53.1 | 0.74 (1.68–0.80) | |||
| HR | Negative | 42.5 | <0.001 | <0.001 | 1 |
| Positive | 66.6 | 1.93 (1.71–2.18) | |||
| HER2 receptor | Negative | 56.4 | <0.001 | <0.001 | 1 |
| Positive | 72.9 | 1.66 (1.52–1.82) | |||
| Chemotherapy | Not done/unknown | 57.3 | <0.001 | <0.001 | 1 |
| Done | 61.7 | 1.33 (1.21–1.47) | |||
| RT | Not done/unknown | 57.1 | <0.001 | <0.001 | 1 |
| Done | 64.1 | 1.47 (1.28–1.70) | |||
| Brain metastasis | Absent | 61.5 | <0.001 | 0.679 | 1 |
| Present | 27.5 | 0.93 (0.67–1.30) | |||
| Liver metastasis | Absent | 62.9 | <0.001 | <0.001 | 1 |
| Present | 48.7 | 0.76 (0.67–0.87) | |||
| Lung metastasis | Absent | 62.4 | <0.001 | 0.331 | 1 |
| Present | 51.9 | 1.06 (0.94–1.20) | |||
| No of metastatic site * | 0 | 65.5 | <0.001 | 1 | |
| 1 | 62.5 | 0.006 | 0.87 (0.79–0.96) | ||
| 2 | 49.1 | <0.001 | 0.68 (0.57–0.81) | ||
| 3–4 | 29.9 | <0.001 | 0.55 (0.40–0.75) | ||
| RT * Brain metastasis | RT done * Brain metastasis (−) | <0.001 | 1 | ||
| RT done * Brain metastasis (+) | 0.41 (0.27–0.63) | ||||
| RT * HR | RT done * HR (−) | 0.018 | 1 | ||
| RT done * HR (+) | 0.82 (0.70–0.97) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, B.H.; Kim, S.; Kim, Y.I.; Chang, J.H.; Hwang, K.-T.; Kim, S.; Cho, M.-J.; Kwon, J. Development of an Individualized Prediction Calculator for the Benefit of Postoperative Radiotherapy in Patients with Surgically Resected De Novo Stage IV Breast Cancer. Cancers 2020, 12, 2103. https://doi.org/10.3390/cancers12082103
Kim BH, Kim S, Kim YI, Chang JH, Hwang K-T, Kim S, Cho M-J, Kwon J. Development of an Individualized Prediction Calculator for the Benefit of Postoperative Radiotherapy in Patients with Surgically Resected De Novo Stage IV Breast Cancer. Cancers. 2020; 12(8):2103. https://doi.org/10.3390/cancers12082103
Chicago/Turabian StyleKim, Byoung Hyuck, Suzy Kim, Young Il Kim, Ji Hyun Chang, Ki-Tae Hwang, Sup Kim, Moon-June Cho, and Jeanny Kwon. 2020. "Development of an Individualized Prediction Calculator for the Benefit of Postoperative Radiotherapy in Patients with Surgically Resected De Novo Stage IV Breast Cancer" Cancers 12, no. 8: 2103. https://doi.org/10.3390/cancers12082103
APA StyleKim, B. H., Kim, S., Kim, Y. I., Chang, J. H., Hwang, K.-T., Kim, S., Cho, M.-J., & Kwon, J. (2020). Development of an Individualized Prediction Calculator for the Benefit of Postoperative Radiotherapy in Patients with Surgically Resected De Novo Stage IV Breast Cancer. Cancers, 12(8), 2103. https://doi.org/10.3390/cancers12082103