
Do Dietary Supplements Affect Inflammation, Oxidative Stress, and Antioxidant Status in Adults with Hypothyroidism or Hashimoto’s Disease?—A Systematic Review of Controlled Trials

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
3. Results
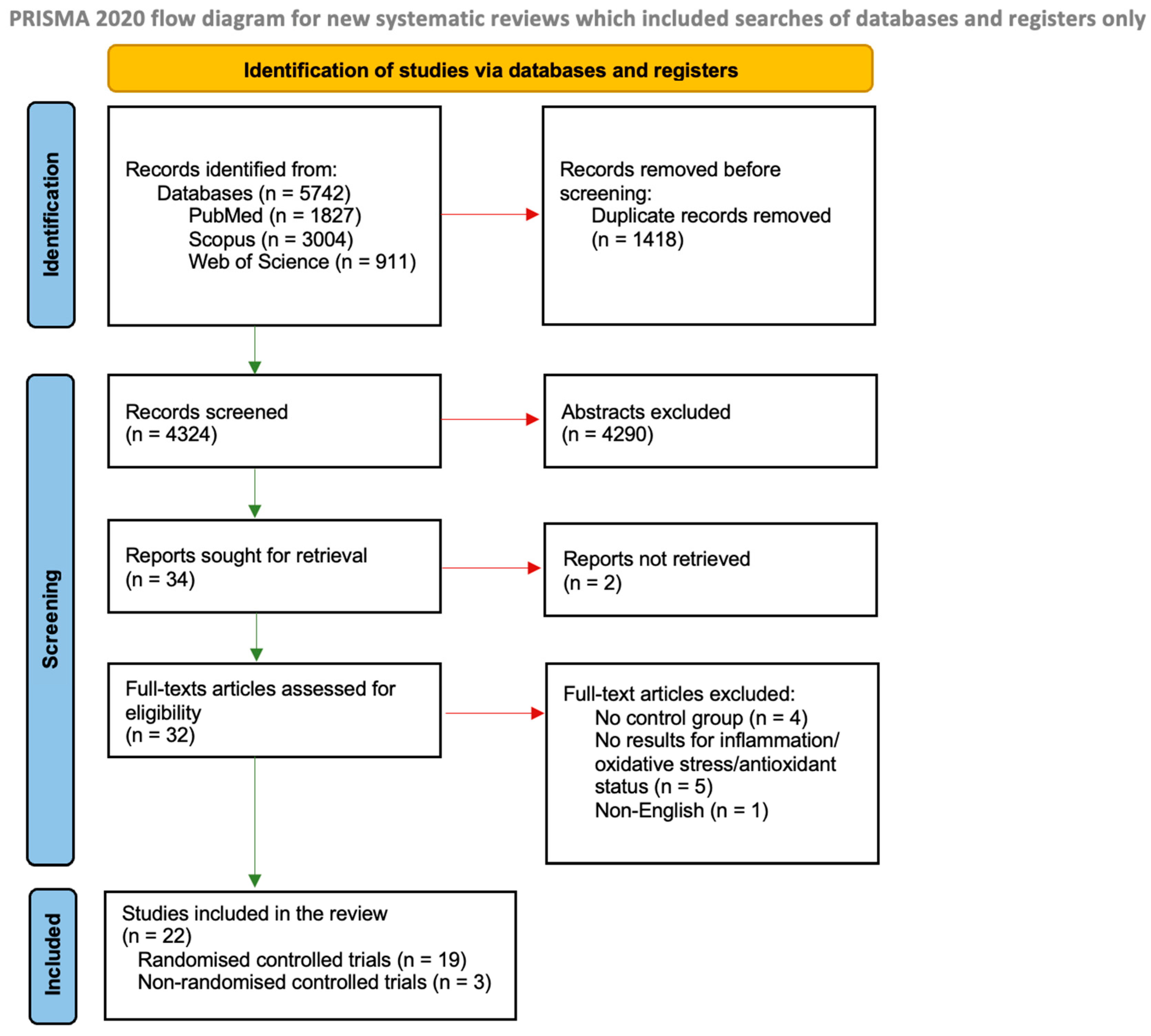
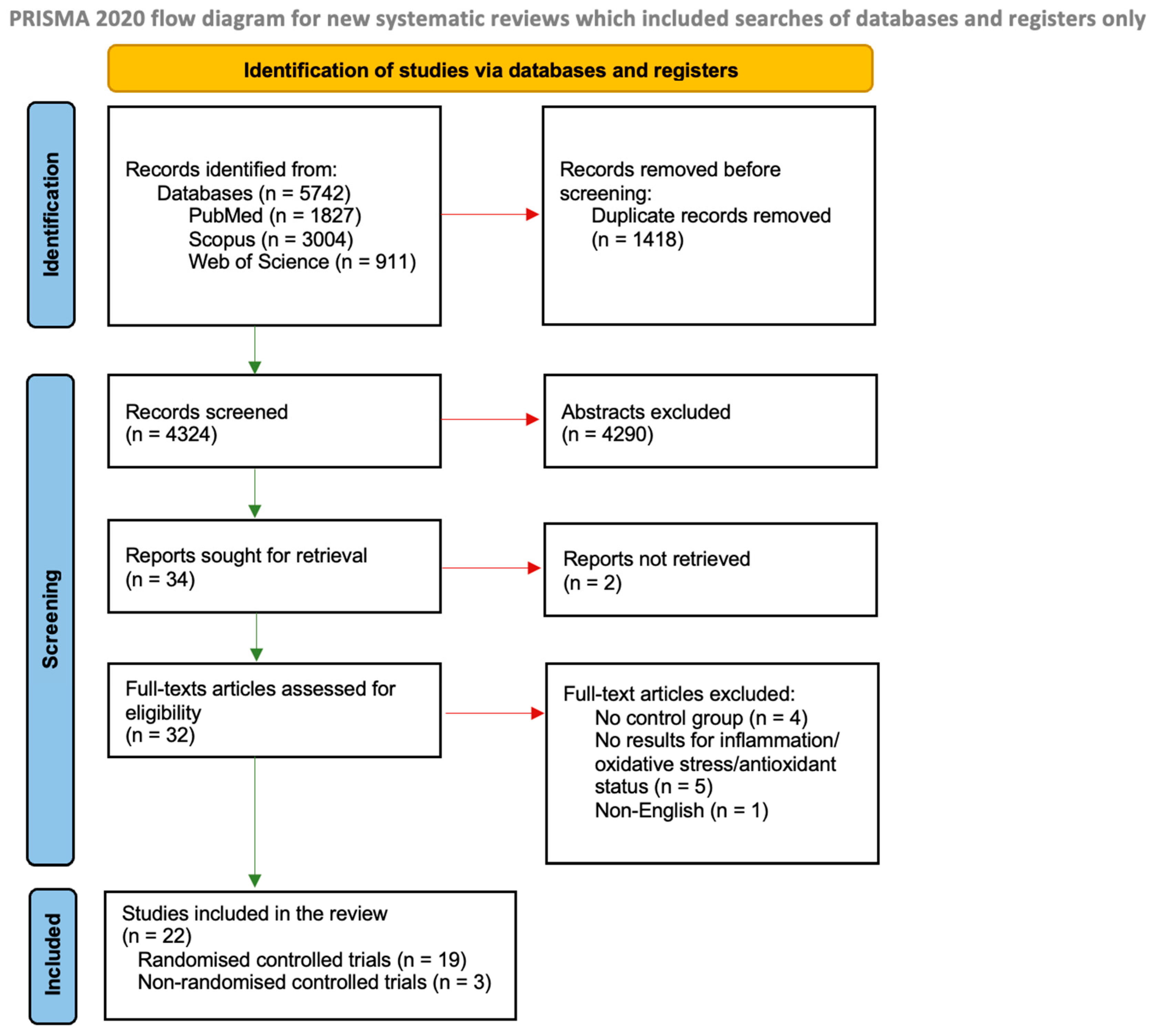
3.1. Trial Selection
3.2. Characteristics of Included Studies
3.3. Study Quality
3.4. Results of Vitamin D Supplementation
3.4.1. Vitamin D Status
3.4.2. Inflammation Parameters
3.4.3. Oxidative Stress and Antioxidant Status Parameters
3.4.4. Thyroid Parameters
3.5. Results of Selenium Supplementation
3.5.1. Selenium Status
3.5.2. Inflammation Parameters
3.5.3. Oxidative Stress Parameters
3.5.4. Antioxidant Status Parameters
3.5.5. Thyroid Parameters
3.6. Results of the Studies with Other DS
3.6.1. Inflammation, Oxidative Stress, and Antioxidant Status Parameters
3.6.2. Thyroid Parameters
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). International Classification of Diseases, Eleventh Revision (ICD-11); World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Chaker, L.; Bianco, A.C.; Jonklaas, J.; Peeters, R.P. Hypothyroidism. Lancet 2017, 390, 1550–1562. [Google Scholar] [CrossRef] [PubMed]
- Chiovato, L.; Magri, F.; Carlé, A. Hypothyroidism in Context: Where We’ve Been and Where We’re Going. Adv. Ther. 2019, 36, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Mendes, D.; Alves, C.; Silverio, N.; Batel Marques, F. Prevalence of Undiagnosed Hypothyroidism in Europe: A Systematic Review and Meta-Analysis. Eur. Thyroid J. 2019, 8, 130–143. [Google Scholar] [CrossRef]
- Muñoz-Ortiz, J.; Sierra-Cote, M.C.; Zapata-Bravo, E.; Valenzuela-Vallejo, L.; Marin-Noriega, M.A.; Uribe-Reina, P.; Terreros-Dorado, J.P.; Gómez-Suarez, M.; Arteaga-Rivera, K.; de-la-Torre, A. Prevalence of Hyperthyroidism, Hypothyroidism, and Euthyroidism in Thyroid Eye Disease: A Systematic Review of the Literature. Syst. Rev. 2020, 9, 201. [Google Scholar] [CrossRef]
- Hu, X.; Chen, Y.; Shen, Y.; Tian, R.; Sheng, Y.; Que, H. Global Prevalence and Epidemiological Trends of Hashimoto’s Thyroiditis in Adults: A Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 1020709. [Google Scholar] [CrossRef]
- Burek, C.L.; Talor, M.V. Environmental Triggers of Autoimmune Thyroiditis. J. Autoimmun. 2009, 33, 183–189. [Google Scholar] [CrossRef]
- Aseervatham, G.S.B.; Sivasudha, T.; Jeyadevi, R.; Arul Ananth, D. Environmental Factors and Unhealthy Lifestyle Influence Oxidative Stress in Humans—An Overview. Environ. Sci. Pollut. Res. 2013, 20, 4356–4369. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.M. Clinical Relevance of Environmental Factors in the Pathogenesis of Autoimmune Thyroid Disease. Endocrinol. Metab. 2016, 31, 213. [Google Scholar] [CrossRef]
- Botelho, I.M.B.; Moura Neto, A.; Silva, C.A.; Tambascia, M.A.; Alegre, S.M.; Zantut-Wittmann, D.E. Vitamin D in Hashimoto’s Thyroiditis and Its Relationship with Thyroid Function and Inflammatory Status. Endocr. J. 2018, 65, 1029–1037. [Google Scholar] [CrossRef]
- Tellechea, M.L. Meta-Analytic Evidence for Increased Low-Grade Systemic Inflammation and Oxidative Stress in Hypothyroid Patients. Can Levothyroxine Replacement Therapy Mitigate the Burden? Endocrine 2021, 72, 62–71. [Google Scholar] [CrossRef]
- Ruggeri, R.M.; Cristani, M.; Vicchio, T.M.; Alibrandi, A.; Giovinazzo, S.; Saija, A.; Campennì, A.; Trimarchi, F.; Gangemi, S. Increased Serum Interleukin-37 (IL-37) Levels Correlate with Oxidative Stress Parameters in Hashimoto’s Thyroiditis. J. Endocrinol. Investig. 2019, 42, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Zake, T.; Skuja, S.; Kalere, I.; Konrade, I.; Groma, V. Upregulated Tissue Expression of T Helper (Th) 17 Pathogenic Interleukin (IL)-23 and IL-1β in Hashimoto’s Thyroiditis but Not in Graves’ Disease. Endocr. J. 2019, 66, 423–430. [Google Scholar] [CrossRef]
- Uppu, S.; Gupta, M. Association between C-Reactive Protein and Interleukin-6 Levels in Subclinical Hypothyroid Patients. J. Datta Meghe Inst. Med. Sci. Univ. 2018, 13, 195. [Google Scholar] [CrossRef]
- Gerenova, J. Serum Levels of Interleukin—23 and Interleukin—17 in Hashimoto’s Thyroiditis. Acta Endocrinol. Buchar. 2019, 15, 74–79. [Google Scholar] [CrossRef]
- Zheng, T.; Xu, C.; Mao, C.; Mou, X.; Wu, F.; Wang, X.; Bu, L.; Zhou, Y.; Luo, X.; Lu, Q.; et al. Increased Interleukin-23 in Hashimoto’s Thyroiditis Disease Induces Autophagy Suppression and Reactive Oxygen Species Accumulation. Front. Immunol. 2018, 9, 96. [Google Scholar] [CrossRef] [PubMed]
- Falkowski, B.; Szczepanek-Parulska, E.; Krygier, A.; Wrotkowska, E.; Ruchala, M. Evaluation of Interleukin-29 in Autoimmune and Inflammatory Thyroid Diseases. Clin. Endocrinol. 2021, 94, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.-S.; Wang, C.-S.; Yeh, C.-T.; Lin, K.-H. Roles of Thyroid Hormone-Associated MicroRNAs Affecting Oxidative Stress in Human Hepatocellular Carcinoma. Int. J. Mol. Sci. 2019, 20, 5220. [Google Scholar] [CrossRef]
- Mikulska, A.A.; Karaźniewicz-Łada, M.; Filipowicz, D.; Ruchała, M.; Główka, F.K. Metabolic Characteristics of Hashimoto’s Thyroiditis Patients and the Role of Microelements and Diet in the Disease Management-An Overview. Int. J. Mol. Sci. 2022, 23, 6580. [Google Scholar] [CrossRef]
- Aktas, G.; Sit, M.; Dikbas, O.; Tekce, B.K.; Savli, H.; Tekce, H.; Alcelik, A. Could Red Cell Distribution Width Be a Marker in Hashimoto’s Thyroiditis? Exp. Clin. Endocrinol. Diabetes 2014, 122, 572–574. [Google Scholar] [CrossRef]
- Woźniak, D.; Drzymała, S.; Przysławski, J.; Drzymała-Czyż, S. Dietary Supplements in Hypothyroidism. Acta Sci. Pol. Technol. Aliment. 2021, 20, 375–381. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP Randomised Controlled Trial Checklist. 2020. Available online: https://Casp-Uk.Net/Casp-Tools-Checklists/ (accessed on 4 April 2023).
- Pollock, A.; Campbell, P.; Cheyne, J.; Cowie, J.; Davis, B.; McCallum, J.; McGill, K.; Elders, A.; Hagen, S.; McClurg, D.; et al. Interventions to Support the Resilience and Mental Health of Frontline Health and Social Care Professionals during and after a Disease Outbreak, Epidemic or Pandemic: A Mixed Methods Systematic Review. Cochrane Database Syst. Rev. 2020, 2020, 15. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Karanikas, G.; Schuetz, M.; Kontur, S.; Duan, H.; Kommata, S.; Schoen, R.; Antoni, A.; Kletter, K.; Dudczak, R.; Willheim, M. No Immunological Benefit of Selenium in Consecutive Patients with Autoimmune Thyroiditis. Thyroid 2008, 18, 7–12. [Google Scholar] [CrossRef]
- Xiang, G.D.; Pu, J.H.; Sun, H.L.; Zhao, L.S. Alpha-Lipoic Acid Improves Endothelial Dysfunction in Patients with Subclinical Hypothyroidism. Exp. Clin. Endocrinol. Diabetes 2010, 118, 625–629. [Google Scholar]
- Farhangi, M.A.; Tajmiri, S. The Effects of Powdered Black Cumin Seeds on Markers of Oxidative Stress, Intracellular Adhesion Molecule (ICAM)-1 and Vascular Cell Adhesion Molecule (VCAM)-1 in Patients with Hashimoto’s Thyroiditis. Clin. Nutr. ESPEN 2020, 37, 207–212. [Google Scholar] [CrossRef]
- Hu, Y.; Feng, W.; Chen, H.; Shi, H.; Jiang, L.; Zheng, X.; Liu, X.; Zhang, W.; Ge, Y.; Liu, Y.; et al. Effect of Selenium on Thyroid Autoimmunity and Regulatory T Cells in Patients with Hashimoto’s Thyroiditis: A Prospective Randomized-Controlled Trial. Clin. Transl. Sci. 2021, 14, 1390–1402. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, E.; Golgiri, F.; Janani, L.; Moradi, N.; Fallah, S.; Abiri, B.; Vafa, M. Randomized Study of the Effects of Zinc, Vitamin A, and Magnesium Co-Supplementation on Thyroid Function, Oxidative Stress, and Hs-CRP in Patients with Hypothyroidism. Biol. Trace Elem. Res. 2021, 199, 4074–4083. [Google Scholar] [CrossRef]
- Robat-Jazi, B.; Mobini, S.; Chahardoli, R.; Mansouri, F.; Nodehi, M.; Esfahanian, F.; Yaraghi, A.A.S. The Impact of Vitamin D Supplementation on the IFN Gamma-IP10 Axis in Women with Hashimoto’s Thyroiditis Treated with Levothyroxine: A Double-Blind Randomized Placebo-Controlled Trial. Iran. J. Allergy Asthma Immunol. 2022, 21, 407–417. [Google Scholar] [PubMed]
- Sun, C.; Zhu, M.; Li, L.; Fan, H.; Lv, F.; Zhu, D. Clinical Observation of Levothyroxine Sodium Combined with Selenium in the Treatment of Patients with Chronic Lymphocytic Thyroiditis and Hypothyroidism and the Effects on Thyroid Function, Mood, and Inflammatory Factors. Evid.-Based Complement. Altern. Med. ECAM 2021, 2021, 5471281. [Google Scholar] [CrossRef] [PubMed]
- Talebi, S.; Karimifar, M.; Heidari, Z.; Mohammadi, H.; Askari, G. The Effects of Synbiotic Supplementation on Thyroid Function and Inflammation in Hypothyroid Patients: A Randomized, Double-Blind, Placebo-Controlled Trial. Complement. Ther. Med. 2020, 48, 102234. [Google Scholar] [CrossRef]
- Tian, X.; Li, N.; Su, R.; Dai, C.; Zhang, R. Selenium Supplementation May Decrease Thyroid Peroxidase Antibody Titer via Reducing Oxidative Stress in Euthyroid Patients with Autoimmune Thyroiditis. Int. J. Endocrinol. 2020, 2020, 9210572. [Google Scholar] [CrossRef]
- Wang, W.; Mao, J.; Zhao, J.; Lu, J.; Yan, L.; Du, J.; Lu, Z.; Wang, H.; Xu, M.; Bai, X.; et al. Decreased Thyroid Peroxidase Antibody Titer in Response to Selenium Supplementation in Autoimmune Thyroiditis and the Influence of a Selenoprotein P Gene Polymorphism: A Prospective, Multicenter Study in China. Thyroid 2018, 28, 1674–1681. [Google Scholar] [CrossRef]
- Yu, L.; Zhou, L.; Xu, E.; Bi, Y.; Hu, X.; Pei, X.; Jin, G. Levothyroxine Monotherapy versus Levothyroxine and Selenium Combination Therapy in Chronic Lymphocytic Thyroiditis. J. Endocrinol. Investig. 2017, 40, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Wang, Y.; Ma, W.; Hu, Z.; Zhao, P. Genistein Improves Thyroid Function in Hashimoto’s Thyroiditis Patients through Regulating Th1 Cytokines. Immunobiology 2017, 222, 183–187. [Google Scholar] [CrossRef]
- Anaraki, P.V.; Aminorroaya, A.; Amini, M.; Feizi, A.; Iraj, B.; Tabatabaei, A. Effects of Vitamin D Deficiency Treatment on Metabolic Markers in Hashimoto Thyroiditis Patients. J. Res. Med. Sci. 2016, 21, 1–6. [Google Scholar] [CrossRef]
- Nodehi, M.; Ajami, A.; Izad, M.; Asgarian Omran, H.; Chahardoli, R.; Amouzegar, A.; Yekaninejad, S.; Hemmatabadi, M.; Azizi, F.; Esfahanian, F.; et al. Effects of Vitamin D Supplements on Frequency of CD4+ T-Cell Subsets in Women with Hashimoto’s Thyroiditis: A Double-Blind Placebo-Controlled Study. Eur. J. Clin. Nutr. 2019, 73, 1236–1243. [Google Scholar] [CrossRef]
- Chakrabarti, S.K.; Ghosh, S.; Banerjee, S.; Mukherjee, S.; Chowdhury, S. Oxidative Stress in Hypothyroid Patients and the Role of Antioxidant Supplementation. Indian J. Endocrinol. Metab. 2016, 20, 674–678. [Google Scholar] [CrossRef]
- Esposito, D.; Rotondi, M.; Accardo, G.; Vallone, G.; Conzo, G.; Docimo, G.; Selvaggi, F.; Cappelli, C.; Chiovato, L.; Giugliano, D.; et al. Influence of Short-Term Selenium Supplementation on the Natural Course of Hashimoto’s Thyroiditis: Clinical Results of a Blinded Placebo-Controlled Randomized Prospective Trial. J. Endocrinol. Investig. 2017, 40, 83–89. [Google Scholar] [CrossRef]
- Nordio, M.; Basciani, S. Efficacy of a Food Supplement in Patients with Hashimoto Thyroiditis. J. Biol. Regul. Homeost. Agents 2015, 29, 93–102. [Google Scholar] [PubMed]
- Tomella, C.; Catanzaro, R.; Illuzzi, N.; Cabeca, A.; Zerbinati, N.; Celep, G.; Milazzo, M.; Sapienza, C.; Italia, A.; Lorenzetti, A.; et al. The Hidden Phenomenon of Oxidative Stress During Treatment of Subclinical-Mild Hypothyroidism: A Protective Nutraceutical Intervention. Rejuvenation Res. 2014, 17, 180–183. [Google Scholar] [CrossRef]
- Pilli, T.; Cantara, S.; Cenci, V.; Cardinale, S.; Sestini, F.; Fioravanti, C.; Pacini, F. IFN Gamma-Inducible Chemokines Are Down-Modulated By Selenomethionine (Semet) Supplementation in Women with Euthyroid Chronic Autoimmune Thyroiditis (AIT): Comparison Between 2 Doses of Semet (80 Mu g or 160 Mu g) Versus Placebo. Endocr. Rev. 2014, 35, 226–233. [Google Scholar]
- Krysiak, R.; Okopien, B. The Effect of Levothyroxine and Selenomethionine on Lymphocyte and Monocyte Cytokine Release in Women with Hashimoto’s Thyroiditis. J. Clin. Endocrinol. Metab. 2011, 96, 2206–2215. [Google Scholar] [CrossRef] [PubMed]
- Preda, C.; Vasiliu, I.; Mihalache, L.; Armasu, I.; Serban, I.L.; Serban, D.N.; Stoica, B.; Ciobanu, D.G.; Bredetean, O.; Strungaru, S.A.; et al. Selenium-Essential Antioxidant Element. Rev. Chim. 2017, 68, 1617–1621. [Google Scholar] [CrossRef]
- De Farias, C.R.; Cardoso, B.R.; De Oliveira, G.M.B.; De Mello Guazzelli, I.C.; Catarino, R.M.; Chammas, M.C.; Cozzolino, S.M.F.; Knobel, M. A Randomized-Controlled, Double-Blind Study of the Impact of Selenium Supplementation on Thyroid Autoimmunity and Inflammation with Focus on the GPx1 Genotypes. J. Endocrinol. Investig. 2015, 38, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Aktaş, H.Ş. Vitamin B12 and Vitamin D Levels in Patients with Autoimmune Hypothyroidism and Their Correlation with Anti-Thyroid Peroxidase Antibodies. Med. Princ. Pract. 2020, 29, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Rayman, M.P.; Lv, H.; Schomburg, L.; Cui, B.; Gao, C.; Chen, P.; Zhuang, G.; Zhang, Z.; Peng, X.; et al. Low Population Selenium Status Is Associated With Increased Prevalence of Thyroid Disease. J. Clin. Endocrinol. Metab. 2015, 100, 4037–4047. [Google Scholar] [CrossRef] [PubMed]
- Gautam, N.; Regmi, D.; Shahi, A.; Bohara, S.; Subedi, S.; Jayan, A. Status of Serum Zinc Level in Hypothyroid Patients with Normal Serum Albumin Level: A Case Control Study. J. Univers. Coll. Med. Sci. 2019, 7, 34–38. [Google Scholar] [CrossRef]
- Jiang, H.; Chen, X.; Qian, X.; Shao, S. Effects of Vitamin D Treatment on Thyroid Function and Autoimmunity Markers in Patients with Hashimoto’s Thyroiditis—A Meta-analysis of Randomized Controlled Trials. J. Clin. Pharm. Ther. 2022, 47, 767–775. [Google Scholar] [CrossRef]
- Kim, D. The Role of Vitamin D in Thyroid Diseases. Int. J. Mol. Sci. 2017, 18, 1949. [Google Scholar] [CrossRef]
- Shin, D.Y.; Kim, K.J.; Kim, D.; Hwang, S.; Lee, E.J. Low Serum Vitamin D Is Associated with Anti-Thyroid Peroxidase Antibody in Autoimmune Thyroiditis. Yonsei Med. J. 2014, 55, 476. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Zhang, W.; Ma, C.; Zhao, Y.; Xiong, R.; Wang, H.; Chen, W.; Zheng, S.G. Immunomodulatory Function of Vitamin D and Its Role in Autoimmune Thyroid Disease. Front. Immunol. 2021, 12, 574967. [Google Scholar] [CrossRef]
- Bizzaro, G.; Shoenfeld, Y. Vitamin D and Thyroid Autoimmune Diseases: The Known and the Obscure. Immunol. Res. 2015, 61, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Drutel, A.; Archambeaud, F.; Caron, P. Selenium and the Thyroid Gland: More Good News for Clinicians. Clin. Endocrinol. 2013, 78, 155–164. [Google Scholar] [CrossRef]
- Nettore, I.C.; De Nisco, E.; Desiderio, S.; Passaro, C.; Maione, L.; Negri, M.; Albano, L.; Pivonello, R.; Pivonello, C.; Portella, G.; et al. Selenium Supplementation Modulates Apoptotic Processes in Thyroid Follicular Cells: Apoptotic Processes in Thyroid Follicular Cells. BioFactors 2017, 43, 415–423. [Google Scholar] [CrossRef]
- Winther, K.H.; Wichman, J.E.M.; Bonnema, S.J.; Hegedüs, L. Insufficient Documentation for Clinical Efficacy of Selenium Supplementation in Chronic Autoimmune Thyroiditis, Based on a Systematic Review and Meta-Analysis. Endocrine 2017, 55, 376–385. [Google Scholar] [CrossRef]
- Hariharan, S.; Dharmaraj, S. Selenium and Selenoproteins: It’s Role in Regulation of Inflammation. Inflammopharmacology 2020, 28, 667–695. [Google Scholar] [CrossRef]
- Duntas, L.H.; Benvenga, S. Selenium: An Element for Life. Endocrine 2015, 48, 756–775. [Google Scholar] [CrossRef] [PubMed]
- Schrauzer, G.N. Selenium Yeast: Composition, Quality, Analysis, and Safety. Pure Appl. Chem. 2006, 78, 105–109. [Google Scholar] [CrossRef]
- Wichman, J.; Winther, K.H.; Bonnema, S.J.; Hegedüs, L. Selenium Supplementation Significantly Reduces Thyroid Autoantibody Levels in Patients with Chronic Autoimmune Thyroiditis: A Systematic Review and Meta-Analysis. Thyroid 2016, 26, 1681–1692. [Google Scholar] [CrossRef]
- Winther, K.H.; Papini, E.; Attanasio, R.; Negro, R.; Hegedüs, L. A 2018 European Thyroid Association Survey on the Use of Selenium Supplementation in Hashimoto’s Thyroiditis. Eur. Thyroid J. 2020, 9, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, A.; Soltani, S.; Ghorabi, S.; Keshtkar, A.; Daneshzad, E.; Nasri, F.; Mazloomi, S.M. Effect of Probiotic and Synbiotic Supplementation on Inflammatory Markers in Health and Disease Status: A Systematic Review and Meta-Analysis of Clinical Trials. Clin. Nutr. 2020, 39, 789–819. [Google Scholar] [CrossRef] [PubMed]
- Płudowski, P.; Kos-Kudła, B.; Walczak, M.; Fal, A.; Zozulińska-Ziółkiewicz, D.; Sieroszewski, P.; Peregud-Pogorzelski, J.; Lauterbach, R.; Targowski, T.; Lewiński, A.; et al. Guidelines for Preventing and Treating Vitamin D Deficiency: A 2023 Update in Poland. Nutrients 2023, 15, 695. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Authors, Publication Year | Intervention/Control Group Size (Country) | Inclusion Criteria | Exclusion Criteria | Age Intervention /Control Group (Years; Mean ± SD) | Inflammatory Parameters | Oxidative Stress Parameters | Antioxidant/Nutritional Status Parameters | Thyroid Parameters |
|---|---|---|---|---|---|---|---|---|
| Vitamin D | ||||||||
| Anaraki et al., 2017 [38] Randomised, double-blind, placebo-controlled clinical trial | 30/26 (Iran) | Female/Male, AIT with/without HT Intervention (vitamin D): adults; hypothyroidism or euthyroidism with positive TPO-Ab; stable on LT4 at least for 6 months/or a mild hypothyroidism on enrolment TSH < 15 mU/L Control (placebo): the same criteria as in the intervention group | Renal or liver disease; cancer; pregnancy; severe weight loss; immunosuppressive medication, insulin, sulfonamides; any supplements. | 43.55 ± 1.56 /44.12 ± 1.56 | CRP | — | 25(OH)D | TSH |
| Nodehi et al., 2019 [39] Randomised, double-blind, placebo-controlled trial | 17/17 (Iran) | Female, AIT Intervention (vitamin D): Hashimoto’s thyroiditis, age 20–45 years; constant doses of LT4. Control (placebo): the same criteria as in the intervention group | History of other specific diseases; receiving vitamin supplements in the last 3 months. | 36.4 ± 5.2 /35.9 ± 7.8 | IL-10, IFN-γ, IL-17, IL-4 | — | 25(OH)D | TSH, TPO-Ab, Tg-Ab |
| Robat-Jazi et al., 2022 [31] Randomised, double-blind, placebo-controlled trial | 18/20 (Iran) | Female, AIT Intervention (vitamin D): Hashimoto’s thyroiditis, age 18–48 years; BMI 18.5–30; treatment with LT4 for 6 months Control (placebo): the same criteria as in the intervention group | Severe hepatic, biliary, pancreatic, and fatty liver disease; diseases affecting the balance of CD4+ T cells (asthma, active viral diseases); autoimmune diseases; malnutrition; obesity; treatment with vitamin D supplementation within 3 months prior; pregnancy, lactation; alcoholism; history of stroke or MI. | 36.4 ± 5.2 /35.9 ± 7.8 | IFN-γ, TNF-α | — | 25(OH)D | TSH, TPO-Ab, Tg-Ab |
| Selenium | ||||||||
| Chakrabarti et al., 2016 [40] Placebo-controlled trial | 30/30 (India) | Female/Male, HT Intervention (selenium): adults; overt hypothyroidism, based on the low fT4 level with elevated TSH level; treatment-naïve Control (placebo): the same criteria as in the intervention group | Patients with hypothyroidism but on treatment with LT4; taking lipid-lowering drugs and antioxidant supplements; smokers and alcoholics; pregnancy; patients with hypertension, diabetes mellitus, hepatic or renal impairment, CAD, or heart failure. | 34.63 ± 10.94 /39.57 ± 13.62 | — | MDA | — | TSH, fT4 |
| de Farias et al., 2015 [47] Prospective, randomised, double-blind, placebo-controlled trial | 23/30 (Brazil) | Female/Male, AIT Intervention (selenium): Hashimoto’s thyroiditis is established by an increased level of TPO-Ab (>100 UI/mL), a normal or increased Tg-Ab level (>100 UI/mL), thyroid hypoechogenicity on high-resolution ultrasound, a normal or elevated TSH level, and normal fT4 Control (placebo): the same criteria as in the intervention group | Use of immunosuppressive or anti-inflammatory drugs, supplements containing micronutrients, antidepressants, anticonvulsants, or antiarrhytmic drugs; health conditions that may interfere with gastrointestinal absorption or with the metabolism of selenium; and diabetes. | 48 (20–58) /44 (21–56) * | — | — | GPx1, Se | TSH, TPO-Ab, Tg-Ab |
| Esposito et al., 2017 [41] Prospective, randomised, blinded, placebo-controlled trial | 38/38 (Italy) | Female, AIT Intervention (selenium): newly diagnosed subjects with elevated plasma TPO-Ab and Tg-Ab above 350 IU/ml; thyroid parenchyma heterogeneity with reduced echogenicity; normal TSH, fT3, and fT4 serum levels; without LT4 treatment Control (placebo): the same criteria as in the intervention group | Male; living outside the Campania district area; hyperthyroidism with antithyroid drugs; hypothyroidism with LT4 treatment; other medication that can influence thyroid and immunity status; pregnancy. | 40.0 ± 12.1 /46.0 ± 14.1 | CXCL-10 | — | — | TSH, fT3, fT4, TPO-Ab, Tg-Ab |
| Hu et al., 2021 [29] Randomised, controlled study | 43/47 (China) | Female/Male, AIT Intervention (selenium): age 18–65 years; positive serum TPO-Ab (>34 IU/mL) or/and Tg-Ab (>115 IU/mL); diffuse thyroid disease and heterogeneous echogenicity on ultrasonography; euthyroid or subclinical hypothyroid; newly diagnosed HT patients not receiving LT4 replacement, immunomodulator, vitamins, and other trace elements Control (none): the same criteria as in the intervention group | Previous treatments with immune suppressors or modulators; combined with other autoimmune diseases; pregnancy or lactation in women, or planning pregnancy within 6 months; unability to take medication on time; participation in another clinical trial, informed consent withdrawn | 39.4 ± 12.0 /37.8 ± 11.2 | — | — | GPx3, Se, SePP | TSH, fT3, fT4, TPO-Ab, Tg-Ab |
| Karanikas et al., 2008 [26] Randomised, placebo-controlled trial | 18/18 (Austria) | Female, AIT Intervention (selenium): verified Hashimoto’s thyroiditis; LT4 substitution; positivity for TPO-AB, negativity for anti-thyrotropin (TSH) receptor antibodies; thyroid ultrasound imaging suggestive for a chronic thyroiditis (typical hypoechogenicity); no clinical history of hyperthyroidism; no treatment with drugs known to induce thyroid dysfunction (cytokines, lithium, amiodarone); no pregnancy in the last 12 months prior to enrolment Control (placebo): the same criteria as in the intervention group | Not meeting inclusion criteria | Mean for all: 47 | IL-2, IL-4, IL-10, IL-13, IFN-γ, TNF-α | — | Se | TSH, fT4, TPO-Ab |
| Krysiak and Okopień, 2011 [45] Randomised, double-blind, placebo-controlled trial | Two intervention groups: SE: 42; LT4 + Se: 42 Control with LT4:41 Placebo:40 (Poland) | Female, AIT Intervention (selenium): age 18–60 years; newly diagnosed and previously untreated Hashimoto’s thyroiditis; positive TPO-Ab level (>100 U/mL); reduced echogenicity of the thyroid parenchyma on ultrasonography; TSH level < 4.0 mU/L; normal level of free T4 and free T3 Control (placebo, LT4): the same criteria as in the intervention group | Any acute/chronic inflammatory processes; other autoimmune disorders; positive serum antibodies against the TSH receptor; current treatment with thyroid hormones; treatment with drugs that may affect inflammatory processes in the vascular wall; treatment with drugs known to affect thyroid hormones or to interact with LT4 and selenomethionine; BMI > 40 kg/m2; Turner or Down syndrome; severe cardiovascular disease, diabetes, impaired glucose tolerance or impaired fasting glucose; impaired renal or hepatic function; pregnancy or lactation; poor patient compliance | 40 ± 4 /37 ± 3 /39 ± 4 /38 ± 3 | IL-1β, IL-2, IL-6, IFN-γ, TNF-α, hsCRP MCP-1/CCL-2 | — | — | TSH, fT3, fT4, TPO-Ab, Tg-Ab |
| Pilli et al., 2015 [44] Randomised, placebo-controlled trial | Se (80 μg/day): 20 Se (160 μg/day): 20 / 20 (Germany) | Female, AIT Intervention (selenium): Hashimoto’s thyroiditis (present of elevated TPO-Ab or/and Tg-Ab serum levels (≥100 U/ml), characteristic thyroid ultrasound pattern (scattered or widespread hypoechogenicity), normal thyroid function; no previous treatment with LT4 replacement therapy Control (placebo): the same criteria as in the intervention group | Not meeting inclusion criteria | 48.8 ± 14 46.9 ± 7.6 /43.0 ± 11.2 | IFN-γ, TNF-α, CXCL-9, CXCL-10, CXCL-11 | — | GPx3, Se, SePP | TSH, fT3, fT4, TPO-Ab, Tg-Ab, Thyroid volume, Thyroid echogenicity |
| Preda et al., 2017 [46] Randomised, placebo-controlled trial | 50/50 (Romania) | Female, AIT Intervention (selenium): adults; euthyroid Hashimoto’s thyroiditis, detectable TPO-Ab levels (>35 UI/mL), normal TSH level (0.4–4 uIU/mL) Control (placebo): the same criteria as in the intervention group | Not meeting inclusion criteria | 46.2 ± 12.5 /50.5 ± 13.5 | — | — | GPx1, Se | TSH, TPO-Ab |
| Sun et al., 2021 [32] Randomised-controlled trial | 69/69 (China)) | Female/Male, AIT with HT Intervention (selenium): age 20–64 years, no serious cardiovascular, cerebrovascular, hepatic, renal, and hematopoietic system disease; psychiatric disorders; not receiving LT4; immunomodulatory preparations and selenium preparations in the 1 month prior to enrolment; no comorbid autoimmune disease Control (none): the same criteria as in the intervention group | Obvious gastrointestinal disorders that cause problems with the use of oral medication; pregnancy or lactation; planning to become pregnant within 6 months; allergies or hypersensitivity to the medication used in the study; other combined thyroid disorders | 42.6 ± 5.3 /41.6 ± 6.1 | IL-2, IL-10, TNF-α | — | — | TSH, TT3, TT4, TPO-Ab, Tg-Ab |
| Tian et al., 2020 [34] Randomised, placebo-controlled trial | 16/16 (China) | Female/Male, AIT Intervention (selenium): euthyroid, newly diagnosed with Hashimoto’s thyroiditis, age ≥ 18 years old Control (placebo): the same criteria as in the intervention group | Nonthyroidal disorders, including cancer, hypertension, diabetes mellitus, coronary artery disease, chronic kidney disease, liver diseases, heart failure, cerebrovascular disease, rheumatism, and smokers; use of other antioxidant agents or vitamin supplements within the past 6 months; pregnancy | 42.3 ± 5.4 /41.6 ± 6.8 | — | MDA | TAC, SOD, Se | TSH, TPO-Ab, Tg-Ab |
| Wang et al., 2018 [35] Randomised, double-blind, placebo-controlled trial | 181 (including 153 subclinical and 28 clinical AIT) 183 placebo (including 160 subclinical and 23 clinical AIT) (China) | Female, AIT Intervention (selenium): age 15–70 years; elevated serum TPO-Ab (>300 IU/mL); thyroid hormone levels within the reference range—TSH may be above the upper normal level (subclinical hypothyroidism); without any medication that can affect either Se bioavailability or peripheral conversion of T4 to T3 or medications that could influence thyroid autoimmunity; nonsmokers Control (placebo): the same criteria as in the intervention group | Not meeting inclusion criteria | 40.3 ± 12.2 /43.1 ± 11.6 | — | MDA | GPx3, Se | TSH, fT4, TPO-Ab |
| Yu et al., 2017 [36] Open-label, randomised controlled trial | 34/36 (China) | Female/Male, AIT Intervention (selenium): Hashimoto’s thyroiditis Control (none): the same criteria as in the intervention group | Residence in an iodine deficiency area with goitre; treatment with immune suppressors or modulators, selenium or other antioxidants, within one month; other autoimmune diseases; severe liver, kidney, GI tract, blood system, brain, circulation system, or blood-vessel system illness; pregnancy or lactation or planning pregnancy within 6 months; mental or nervous system disease not allowing to cooperate or take medication on time, and abuse of drugs or other substances; malignant tumour; allergy to the test drug; surgery or other stressful conditions; participation in another clinical trial. | 34.12 ± 12.7 /39.50 ± 15.1 | IL-2, IL-10 | — | Se | TPO-Ab, Tg-Ab |
| Other supplements | ||||||||
| Rabbani et al., 2021 [30] Randomised, double-blind, placebo-controlled trial | 44/44 (Iran) | Female/Male, HT Intervention (zinc, magnesium, vitamin A): hypothyroidism; age 20–65 years; BMI ≤ 35 kg/m2; no serious medical illness (e.g., diabetes); no uncontrolled hypertension or gastrointestinal diseases. Control (placebo): the same criteria as in the intervention group | Pregnancy or lactation; smoking; drinking alcohol; consumption of anti-inflammatory medication; use of dietary supplements containing Zn, Mg, and vitamin A during the past 3 months; unwillingness to continue the study; and taking less than 80% of supplements in any follow-up visit | 42.47 ± 10.7 /48.33 ± 11.0 | hsCRP | MDA | TAC | TSH, fT3, fT4, TT4 |
| Nordio and Basciani, 2015 [42] Non-randomised placebo-controlled trial | Wob:15 LT4 + Wob:15 /15 (Italy) | Female/male, AIT Intervention (Wobenzym): age 18–80 years; Hashimoto’s thyroiditis, with or without hypothyroidism; no serious illnesses. Control (placebo): the same criteria as in the intervention group | Use of cortisone, NSAIDs, antiinflammatory agents, and anticoagulants; smokers; alcohol or drug use; pregnancy or lactation | All participants: 44.3 ± 6.8 | CRP | — | — | TSH, fT3, TPO-Ab, HTg-Ab, HTG |
| Farhangi and Tajmiri, 2020 [28] Double-blinded, placebo-controlled randomised trial | 20/20 (Iran) | Female/Male, AIT Intervention (Nigella sativa): age 20–50 years, diagnosed with Hashimoto’s thyroiditis. Control (placebo): the same criteria as in the intervention group | Taking any nutritional supplements for at least 3 months prior to the study; any history of autoimmune disease, cardiovascular events, or other thyroid abnormalities; dietary regimens during and 3 months before recruitment into the trial | 35.70 ± 8.2 /33.95 ± 8.7 | — | MDA | TAC, SOD, GPx | TSH, T3, T4, TPO-Ab, |
| Zhang et al., 2017 [37] Randomised, double-blind placebo-controlled clinical trial | 102/116 (China) | Female, AIT Intervention (genistein): Hashimoto’s thyroiditis patients; age 20–60 years; normal fT3, fT4 levels, with or without LT4 therapy; normal or elevated but <20 mU/L TSH level; elevated serum TPO-Ab (>100 U/mL) Control (placebo): the same criteria as in the intervention group | Treatment with immunoregulators; acute infections or other chronic inflammatory diseases; thyroid nodules; thyroid hypoplasia; prior treatment with radioiodine; pregnancy; serious illness (such as cancer, kidney, or liver failure) | 42.9 ± 10.2 /41.4 ± 9.3 | IL-2, IL-4, IL-6, IL-10, IFN-γ, TNF-α | — | — | — |
| Tomella et al., 2014 [43] Placebo-controlled trial | 30/39 (Italy) | Female, HT Intervention (fermented papaya-based nutraceutical): patients treated for subclinical or mild hypothyroidism; age 18–55 years; not on a birth control pill; not taking a soy supplement. Control (placebo): the same criteria as in the intervention group | Main chronic diseases, relevant medications, major dyslipidemia disorders, heavy physical activity, and psychiatric disorders | N/A | — | MDA | L-HPX, SOD, GPx | — |
| Talebi et al., 2020 [33] Randomised, double-blind, placebo-controlled | 30/30 (Iran) | Female/Male, HT Intervention (synbiotic): age 18–65 years, primary hypothyroid patients with more than one year of levothyroxine therapy, at least one year of thyroid-stimulating hormone (TSH) levels in the normal range with a stable dose of levothyroxine; no thyroidectomy for thyroid cancer treatment; not having acute or chronic infectious diseases; not taking drugs that effect the metabolism or absorption of levothyroxine; not using antibiotics for at least 3 months before intervention; no history of smoking, alcohol, or drug abuse; no pregnancy or lactation Control (placebo): the same criteria as in the intervention group | Not meeting inclusion criteria | 42.37 ± 2.2 /43.96 ± 1.8 | CRP | — | — | TSH, fT3, TPO-Ab |
| Xiang et al., 2010 [27] Randomised controlled trial | 20/18 (China) | Female, AIT Intervention (alpha-lipoic acid): age 46–68 years; newly diagnosed Hashimoto’s thyroiditis (elevated TSH levels (> 5.5 mU/L, normal fT3 and fT4 values), positive for TPO-Ab and Tg-AB. Control (none): the same criteria as in the intervention group | Obesity, smoking, thyroid operation, artery disease, other diseases, taking drugs like oestrogen supplements, thyroxine, diuretics, antihypertensive, hypolipidemic, etc. | 57 ± 9 /56 ± 8 | CRP | — | — | TSH, fT3, fT4, TPO-Ab, Tg-Ab |
| Authors | Vitamin D (Cholecalciferol) Dose (IU/Week) (Duration of Intervention) | Parameter (Unit) | Intervention Group Baseline vs. after Supplementation (Mean ± SD) | p-Value | Control Group Baseline vs. after Placebo (Mean ± SD) | p-Value | p-Value after Supplementation vs. Control |
|---|---|---|---|---|---|---|---|
| Anaraki et al. [38] | 50,000 (3 months) | 25(OH)D (ng/mL) | 12.8 ± 0.7 vs. 45.5 ± 1.8 | 0.001 | 13.3 ± 0.9 vs. 14.9 ± 1.1 | 0.090 | 0.001 |
| CRP (mg/dL) | 1.1 ± 0.1 vs. 1.1 ± 0.1 | 0.890 | 1.2 ± 0.1 vs. 1.2 ± 0.1 | 0.970 | 0.790 | ||
| TSH (mU/L) | 3.3 ± 0.5 vs. 3.9 ± 0.8 | 0.405 | 3.4 ± 0.4 vs. 2.7 ± 0.4 | 0.092 | 0.160 | ||
| Nodehi et al. [39] | 50,000 (3 months) | 25(OH)D (ng/mL) | 26.0 ± 14.6 vs. 42.3 ± 16.0 * | 0.002 | 29.8 ± 12.3 vs. 36.2 ± 15.2 * | NS | 0.230 |
| IL-4 (MFI) | 22.2 ± 3.7 vs. 20.2 ± 0.9 * | N/A | 37.5 ± 9.6 vs. 19.8 ± 0.8 * | N/A | 0.601 | ||
| IL-10 (MFI) | 144 ± 14.7 vs. 183 ± 18.0 * | N/A | 151 ± 17.1 vs. 153 ± 15.1 * | N/A | 0.198 | ||
| IL-17 (MFI) | 336 ± 38.4 vs. 388 ± 34.8 * | N/A | 396 ± 42.5 vs. 347 ± 30.3 * | N/A | 0.206 | ||
| IFN-γ (MFI) | 637 ± 54.9 vs. 558 ± 64.9 * | N/A | 681 ± 55.6 vs. 624 ± 69.2 * | N/A | 0.481 | ||
| TSH (μIU/mL) | 3.7 ± 3.3 * vs. N/A | N/A | 4.3 ± 7.1 * vs. N/A | N/A | N/A | ||
| TPO-Ab (IU/mL) | 258 ± 133 * vs. N/A | N/A | 312 ± 123 * vs. N/A | N/A | N/A | ||
| Tg-Ab (IU/mL) | 551 ± 1094 * vs. N/A | N/A | 396 ± 813 * vs. N/A | N/A | N/A | ||
| Robat-Jazi et al. [47] | 50,000 (3 months) | 25(OH)D (ng/mL) | 25.3 ± 11.3 vs. 50.7 ± 15.3 | N/A | 19.9 ± 9.0 vs. 22.2 ± 9.7 | N/A | <0.01 |
| IFN-γ (pg/mL) | 13.9 ± 7.9 vs. 8.4 ± 4.8 | 0.001 | 14.1 ± 8.2 vs. 8.8 ± 5.6 | <0.001 | 0.868 | ||
| TNF-α (pg/mL) | 29.7 ± 18.4 vs. 15.3 ± 10.8 | 0.010 | 26.7 ± 24.8 vs. 12.3 ± 11.8 | 0.008 | 0.987 | ||
| TSH (μIU/mL) | 3.7 ± 3.3 vs. N/A | N/A | 4.3 ± 7.1 vs. N/A | N/A | N/A | ||
| TPO-Ab (IU/mL) | 258 ± 133 vs. N/A | N/A | 312 ± 123 vs. N/A | N/A | N/A | ||
| Tg-Ab (IU/mL) | 551 ± 1094 vs. N/A | N/A | 396 ± 813 vs. N/A | N/A | N/A |
| Authors | Selenium Dose and Form, μg/Day (Duration of Intervention) | Parameter (Unit) | Intervention Group Baseline vs. after Supplementation (Mean ± SD) | p-Value | Control Group Baseline vs. after Placebo/No Treatment (Mean ± SD) | p-Value | p-Value after Supplementationvs. Control |
|---|---|---|---|---|---|---|---|
| Chakrabarti et al. [40] | 200, selenium acid (6 months) | MDA (mg/dL) | 3.8 ± 2.0 vs. 1.8 ± 0.4 | <0.001 | 4.3 ± 2.1 vs. 2.2 ± 0.5 | <0.001 | 0.052 |
| TSH (μIU/mL) | 25.8 ± 9.5 vs. 1.7 ± 0.7 | <0.001 | 33.2 ± 23.5 vs. 1.7 ± 0.8 | <0.001 | N/A | ||
| fT4 (ng/dL) | 0.6 ± 0.1 vs. 1.6 ± 0.2 | <0.001 | 0.6 ± 0.1 vs. 1.7 ± 0.2 | <0.001 | N/A | ||
| de Farias et al. [47] | 200, selenomethionine (3 months) | Se (μg/L) | N/A vs. 63.4 ± 12.8 | <0.001 | N/A vs. 36.8 ± 9.6 | NS | <0.001 |
| GPx1 (U/gHB) | 58.4 ± 23.2 vs. 80.2 ± 12.1 | <0.001 | 61.0 ± 21.7 vs. 61.8 ± 17.0 | NS | <0.001 | ||
| TSH (μIU/mL) | 1.7 ± 0.5 vs. 3.0 ± 1.5 | <0.001 | 1.7 ± 0.4 vs. 2.2 ± 1.5 | NS | N/A | ||
| TPO-Ab (U/mL) | 1009 ± 1015 vs. 958 ± 913 Δ: −5% | 0.668 | 1206 ± 969 vs. 1405 ± 1070 Δ: 16% | N/A | N/A Δ:0.084 | ||
| Tg-Ab (U/mL) | 510 ± 989 vs. 528 ± 997 | N/A | 521 ± 884 vs. 622 ± 1041 | N/A | N/A | ||
| Esposito et al. [41] | 166, selenomethionine (6 months) | CXCL10 (pg/mL) | N/A vs. N/A | NS | N/A vs. N/A | N/A | N/A |
| TSH (μUI/mL) | 2.7 ± 0.8 vs. N/A | NS | 2.0 ± 0.4 vs. N/A | NS | NS | ||
| fT3 (pmol/L) | N/A vs. ↑ | <0.040 | N/A vs. ↓ | <0.02 | N/A | ||
| fT4 (pmol/L) | No change | NS | N/A vs. N/A | NS | N/A | ||
| TPO-Ab (UI/mL) | 2070 ± 575 vs. N/A | NS | 3049 ± 757 | NS | N/A | ||
| Tg-Ab (N/A) | N/A vs. N/A | NS | N/A vs. N/A | NS | N/A | ||
| Hu et al. [29] | 200, selenium yeast tablet (6 months) | Se (μg/L) (median) | 73.6 vs. 187 | <0.01 | 65.0 vs. 72.0 | NS | <0.001 |
| SePP (ng/mL) (median) | 16.0 vs. 17.2 | <0.05 | 12.9 vs. 10.7 | <0.01 | 0.007 | ||
| GPx3 (ng/mL) (median) | 18.8 vs. 45.2 | <0.01 | 18.5 vs. 24.2 | <0.05 | 0.028 | ||
| TSH (mIU/L) (median) | 3.2 vs. 2.4 Δ: −0.16 | NS | 2.8 vs. 3.2 Δ: 0.48 | <0.01 | 0.021 Δ: 0.001 | ||
| fT3 (pmol/L) | 4.4 ± 0.7 vs. 4.7 ± 0.7 | NS | 4.6 ± 0.7 vs. 4.6 ± 0.7 | NS | 0.691 | ||
| fT4 (pmol/L) | 15.4 ± 2.6 vs. 16.4 ± 2.6 | NS | 15.7 ± 2.4 vs. 15.8 ± 1.9 | NS | 0.191 | ||
| TPO-Ab (IU/mL) (median) | 237 vs. 178 Δ: −28.4 | <0.01 | 177 vs. 211 Δ: 0 | NS | 0.942 Δ: 0.01 | ||
| Tg-Ab (IU/mL) (median) | 435 vs. 388 | NS | 371 vs. 365 | NS | 0.891 | ||
| Karanikas et al. [26] | 200, sodium selenite (3 months) | Se (μg/L) | 75 ± 11 vs. 125 ± 71 | <0.05 | 76 ± 12 vs. 78 ± 12 | NS | <0.05 |
| IL-2 (percentages) | CD4+ 67.3 ± 9.3 vs. 61.4 ± 10.7 CD8+ 30.6 ± 10.7 vs. 29.4 ± 14.9 | NS NS | CD4+ 58.7 ± 13.6 vs. 64.6 ± 12.4 CD8+ 29.4 ± 14.3 vs. 29.4 ± 8.1 | NS NS | NS NS | ||
| IL-4 (percentages) | CD4+ 7.0 ± 3.2 vs. 7.1 ± 7.0 CD8+ 7.7 ± 9.3 vs. 5.0 ± 4.3 | NS NS | CD4+ 6.6 ± 3.6 vs. 5.2 ± 2.6 CD8+ 6.9 ± 7.6 vs. 4.8 ± 5.1 | NS NS | NS NS | ||
| IL-10 (percentages) | CD4+ 6.9 ± 9.9 vs. 5.9 ± 7.9 CD8+ 1.2 ± 1.9 vs. 1.3 ± 2.6 | NS NS | CD4+ 15.4 ± 26 vs. 5.8 ± 6.6 CD8+ 7.2 ± 27 vs. 2.2 ± 4.4 | NS NS | NS NS | ||
| IL-13 (percentages) | CD4+ 4.1 ± 1.7 vs. 5.1 ± 6.2 CD8+ 3.9 ± 3.4 vs. 3.3 ± 3.1 | NS NS | CD4+ 4.6 ± 2.6 vs. 3.6 ± 1.8 CD8+ 5.7 ± 6.8 vs. 4.6 ± 6.6 | NS NS | NS NS | ||
| IFN-γ (percentages) | CD4+ 17.6 ± 8.6 vs. 17.9 ± 6.0 CD8+ 42.1 ± 20.6 vs. 38.7 ± 15.0 | NS NS | CD4+ 18.7 ± 5.3 vs. 17.5 ± 8.7 CD8+ 42.0 ± 15.4 vs. 38.8 ± 17.9 | NS NS | NS NS | ||
| TNF-α (percentages) | CD4+ 67.4 ± 24.4 vs. 63.8 ± 24.0 CD8+ 48.6 ± 26.3 vs. 45.5 ± 25.7 | NS NS | CD4+ 76.9 ± 11.7 vs. 68.3 ± 11.5 CD8+ 57.2 ± 16.7 vs. 48.2 ± 20.0 | NS NS | NS NS | ||
| TSH (μIU/mL) | 2.1 ± 1.4 vs. 1.8 ± 0.8 | NS | 2.2 ± 1.7 vs. 2.0 ± 0.8 | NS | NS | ||
| fT4 (ng/dL) | 1.5 ± 0.3 vs. 1.5 ± 0.4 | NS | 1.5 ± 0.4 vs. 1.5 ± 0.3 | NS | NS | ||
| TPO-Ab (IU/mL) | 524 ± 452 vs. 505 ± 464 | NS | 521 ± 349 vs. 527 ± 354 | NS | NS | ||
| Krysiak and Okopień [45] | 200, selenomethionine (6 months) S: selenium LS: LT4 + Se L: LT4 P: placebo | hsCRP (mg/L) | S: 8.8 ± 1.5 vs. 4.4 ± 0.7LS: 8.5 ± 1.4 vs. 2.2 ± 0.4 | <0.001 <0.001 | L: 8.6 ± 1.2 vs. 4.3 ± 0.8 P: 8.0 ± 1.7 vs. 8.2 ± 1.8 | <0.001 NS | S vs. p < 0.001 LS vs. P/L < 0.001 LS vs. S < 0.001 S vs. L NS L vs. P NS |
| IL-1β (pg/mL) | S: 231 ± 34.2 vs. 188 ± 29.3 LS: 235 ± 29.0 vs. 103 ± 12.1 | NS <0.001 | L: 229 ± 23.2 vs. 140 ± 16.1 P: 220 ± 21.3 vs. 235 ± 30.1 | <0.001 NS | L vs. S < 0.01 LS vs. P/L/S < 0.001 S vs. P NS L vs. P NS | ||
| IL-2 (ng/mL) | S: 10.9 ± 1.5 vs. 6.8 ± 0.8 LS: 11.6 ± 1.9 vs. 4.9 ± 0.8 | <0.001 <0.001 | L: 11.4 ± 1.7 vs. 9.2 ± 1.6 P: 11.2 ± 1.3 vs. 10.8 ± 1.6 | NS NS | S vs. p < 0.001 S vs. L < 0.05 LS vs. P/L < 0.001 LS vs. S < 0.01 L vs. P NS | ||
| IL-6 (ng/mL) | S: 23.0 ± 2.8 vs. 19.0 ± 2.8 LS: 23.6 ± 2.5 vs. 11.9 ± 1.0 | NS <0.001 | L: 22.5 ± 2.3 vs. 14.4 ± 1.4 P: 22.9 ± 2.5 vs. 23.4 ± 2.9 | <0.001 NS | L vs. S < 0.01 LS vs. P/S < 0.001 LS vs. L < 0.05 S vs. P NS L vs. P NS | ||
| IFN-γ (ng/mL) | S: 133 ± 17.4 vs. 75.2 ± 9.5 LS: 129 ± 14.8 vs. 52.4 ± 7.4 | <0.001 <0.001 | L: 122 ± 14.6 vs. 103 ± 13.4 P: 126 ± 16.3 vs. 125 ± 20.4 | NS NS | S vs. P/L < 0.001 LS vs. P/L/S < 0.001L vs. P NS | ||
| TNF-α (pg/mL) | Monocyte: S: 2698 ± 312 vs. 2193 ± 198 LS: 2595 ± 348 vs. 1121 ± 135Lymphocyte: S: 792 ± 87 vs. 490 ± 51LS: 776 ± 79 vs. 349 ± 53 | <0.001 <0.001 <0.001 <0.001 | Monocyte: L: 2672 ± 321 vs. 1565 ± 186 P: 2560 ± 310 vs. 2598 ± 281 Lymphocyte: L: 803 ± 92 vs. 650 ± 65 P: 782 ± 82 vs. 762 ± 85 | <0.001 NS NS NS | Monocyte: L vs. S < 0.001 LS vs. P/L/S < 0.001 S vs. L NS S vs. P NS Lymphocyte: S vs. p < 0.001 S vs. L < 0.01 LS vs. P/L/S < 0.001L vs. P NS | ||
| MCP-1 (ng/mL) | S: 38.2 ± 4.2 vs. 30.6 ± 3.7 LS: 37.9 ± 4.4 vs. 18.6 ± 2.2 | NS <0.001 | L: 38.0 ± 4.6 vs. 23.2 ± 2.1 P: 37.2 ± 4.1 vs. 37.5 ± 3.9 | <0.001 NS | L vs. S < 0.001 LS vs. P/S < 0.001 LS vs. L < 0.05 S vs. P NS L vs. P NS | ||
| Krysiak and Okopień [45] | 200, selenomethionine (6 months) S: selenium LS: LT4 + Se L: LT4 P: placebo | TSH (mIU/L) | S: 2.18 ± 0.6 vs. 1.95 ± 0.6 LS: 2.27 ± 0.5 vs. 1.01 ± 0.3 | NS <0.01 | L: 2.24 ± 0.6 vs. 1.15 ± 0.4 P: 2.32 ± 0.6 vs. 2.21 ± 0.6 | <0.001 NS | L vs. S < 0.05 LS vs. P/S < 0.001 LS vs. L NS S vs. P NS L vs. P NS |
| fT3 (pmol/L) | S: 3.52 ± 0.28 vs. 3.75 ± 0.39 LS: 3.42 ± 0.34 vs. 4.46 ± 0.45 | NS <0.001 | L: 3.48 ± 0.35 vs. 4.39 ± 0.28 P: 3.46 ± 0.29 vs. 3.56 ± 0.35 | <0.01 NS | LS vs. p < 0.01 S vs. LS/P/L NS LS vs. P NS L vs. P NS | ||
| fT4 (pmol/L) | S: 14.3 ± 1.5 vs. 14.5 ± 1.3 LS: 13.9 ± 1.2 vs. 17.5 ± 1.5 | NS <0.01 | L: 14.1 ± 1.3 vs. 17.6 ± 1.7 P: 13.8 ± 1.2 vs. 14.3 ± 1.7 | <0.01 NS | L vs. S < 0.05 LS vs. P/S < 0.05 | ||
| TPO-Ab (U/mL) | S: 1761 ± 375 vs. 1005 ± 331 LS: 1810 ± 452 vs. 463 ± 104 | <0.01 <0.001 | L: 1780 ± 328 vs. 1023 ± 294 P: 1723 ± 410 vs. 1884 ± 346 | <0.01 NS | S vs. p < 0.001 LS vs. P/L/S < 0.001 S vs. L NS L vs. P NS | ||
| Tg-Ab (U/mL) | S: 1565 ± 324 vs. 1312 ± 387 LS: 1695 ± 403 vs. 1291 ± 453 | NS NS | L: 1650 ± 361 vs. 1320 ± 392 P: 1602 ± 308 vs. 1701 ± 355 | NS NS | NS | ||
| Pilli et al. [44] | 80 (I group) or 160 (II group), selenomethionine (12 months, 6th month, and 12th month assessment) | Se (μg/L) (median) | I: 84 vs. 112 (6th month, no further increase) II: 80 vs. 150 (6th month, no further increase) | <0.001 <0.001 | 82.1 vs. N/A | 0.001 | N/A |
| SePP (mg/L) | no change | NS | N/A | N/A | N/A | ||
| IFN-γ (pg/mL) (median) | baseline vs. 6th vs. 12th month: I: 9.7 vs. 7.3 vs. ↑ to baseline II: 8.9 vs. 7.8 vs. ↑ to baseline | 6th month I: 0.017 II: 0.055 12th month I: NS II: NS | N/A | NS | N/A | ||
| TNF-α (pg/mL) | baseline vs. 6th vs. 12th month: I: 12.4 vs. 9.9 vs. ↑ to baseline II: 12.1 vs. 10.1 vs. ↑ to baseline | 6th month I: 0.016 II: 0.006 12th month I: NS II: NS | N/A | NS | N/A | ||
| CXCL-9 (pg/mL) (median) | I: 70 vs. 40.9 (12th month) II: 66.4 vs. 49.0 (6th month, no further decrease) | I: 0.007 II: 0.001 | N/A | 0.012 | <0.05 | ||
| CXCL-10 (pg/mL) median | I: 123 vs. 93.8 (12th month) II: 142 vs. 99.6 (12th month) | I: 0.017 II: 0.002 | N/A | 0.004 | <0.05 | ||
| CXCL-11 (pg/mL) (median) | baseline vs. 6th vs. 12th month: I: 84.4 vs. 73.7 vs. ↑ to baseline II: 99.2 vs. 71.9 vs. ↑ to baseline | 6th month I: 0.017 II: 0.001 12th month I: NS II: NS | N/A | NS | NS | ||
| Pilli et al. [44] | 80 (I group) or 160 (II group), selenomethionine (12 months, 6th month, and 12th month assessment) | GPx3 (U/L) | no change | NS | N/A | N/A | N/A |
| TSH (μU/mL) | baseline vs. 6th vs. 12th month: I: 2.4 ± 0.9 vs. N/A II: 2.6 ± 0.9 vs. N/A | N/A | 2.2 ± 1.0 | N/A | N/A | ||
| fT3 (pg/mL) | baseline vs. 6th vs. 12th month: I: 3.1 ± 0.3 vs. N/A II: 3.1 ± 0.4 vs. N/A | N/A | 3.2 ± 0.3 | N/A | N/A | ||
| fT4 (pg/mL) | baseline vs. 6th vs. 12th month: I: 8.2 ± 1.1 vs. N/A II: 8.1 ± 1.1 vs. N/A | N/A | 8.3 ± 1.2 | N/A | N/A | ||
| TPO-Ab (U/mL) (median) | I: 410—stable II: 186—stable | NS | 409 vs. 595 (6th month) vs. 518 (9th month) vs. stable | 0.002 (9th month) | NS | ||
| Tg-Ab (U/mL) (median) | I: no change II: 212 vs. 54.1 | I: NS II: 0.007 | 144 vs. 87.8 | 0.0006 | NS | ||
| Thyroid volume (mL) (median) | baseline vs. 6th vs. 12th month: I: 10.5 vs. 9.7 vs. 9.6 II: 9.1 vs. 8.7 vs. 9.2 | N/A | 11.8 vs. 12.5 vs. 11.8 | N/A | NS | ||
| Thyroid echogenicity(gsp) | baseline vs. 6th vs. 12th month: I: 90.0 ± 20.4 vs. N/A II: 92.4 ± 14.9 vs. N/A | N/A | 90.9 ± 13.1 vs. N/A | N/A | N/A | ||
| Preda et al. [46] | 100, selenomethionine(3 months) | Se (μg/L) | 258 ± 241 vs. 560 ± 363 | 0.001 | 237 ± 212 vs. 316 ± 160 | 0.014 | 0.001 |
| GPx1 (mU/dL) | 0.64 ± 0.37 vs. 0.64 ± 0.38 | 0.979 | N/A | N/A | N/A | ||
| TSH (μUI/mL) | 2.1 ± 1.0 vs. 2.5 ± 1.3 | 0.001 | 1.9 ± 1.1 vs. 2.4 ± 1.3 | 0.008 | 0.677 | ||
| TPO-Ab (UI/mL) | 363 ± 348 vs. 307.9 ± 306.1 | 0.002 | 285 ± 235 vs. 290 ± 288 | 0.850 | 0.781 | ||
| Sun et al. [32] | 100, selenium yeast tablets (3 months) | IL-2 (N/A) | N/A vs. ↓ | <0.05 | N/A vs. ↓ | NS | <0.05 |
| IL-10 (N/A) | N/A vs. ↑ | <0.05 | N/A vs. ↑ | NS | <0.05 | ||
| TNF-α (N/A) | N/A vs. ↓ | <0.05 | N/A vs. ↓ | NS | <0.05 | ||
| TSH (N/A) | N/A vs. ↓ | <0.05 | N/A vs. ↓ | <0.05 | NS | ||
| TT3 (N/A) | N/A vs. ↑ | <0.05 | N/A vs. ↑ | <0.05 | NS | ||
| TT4 (N/A) | N/A vs. ↑ | <0.05 | N/A vs. ↑ | <0.05 | NS | ||
| TPO-Ab (N/A) | N/A vs. ↓ | <0.05 | N/A vs. ↓ | <0.05 | <0.05 | ||
| Tg-Ab (N/A) | N/A vs. ↓ | <0.05 | N/A vs. ↓ | <0.05 | <0.05 | ||
| Tian et al. [34] | 200, selenium yeast tablet (3 months) | Se (µg/L) | 110 ± 16.3 vs. N/A | N/A | 123 ± 19.1 vs. N/A | N/A | N/A |
| MDA (nmol/mL) | 6.8 ± 1.3 vs. 4.9 ± 0.7 | <0.001 | 7.0 ± 1.6 vs. 7.2 ± 1.2 | 0.700 | N/A | ||
| TAC (mmol/L) | 10.0 ± 1.9 vs. 12.9 ± 3.1 | 0.003 | 10.5 ± 2.5 vs. 9.2 ± 2.7 | 0.171 | N/A | ||
| SOD (U/mL) | 72.3 ± 10.3 vs. 84.3 ± 13.2 | 0.007 | 69.1 ± 9.1 vs. 68.3 ± 11.4 | 0.832 | N/A | ||
| TSH (μUI/mL) median | 1.7 vs. 1.4 | 0.734 | 1.94 vs. 2.12 | 0.935 | N/A | ||
| TPO-Ab (IU/mL) (median) | 603 vs. 497 | <0.001 | 581 vs. 569 | 0.110 | N/A | ||
| Tg-Ab (IU/mL) (median) | 482 vs. 454 | 0.081 | 501 vs. 486 | 0.363 | N/A | ||
| Wang et al. [35] | 200 selenium yeast tablet (6 months) G1-S: subclinical AIT group with Se G1-P: subclinical AIT group with placeboG2-S: clinical AIT group with Se G2-P: clinical AIT group with placebo | Se (μg/L) | G1-S: 101 ± 19.3 vs. 181 ± 42.6 G2-S: 91.6 ± 19.9 vs. 188 ± 26.5 | <0.01 <0.01 | G1-P: 111 ± 27.9 vs. 106 ± 26.2 G2-P: 94.7 ± 21.1 vs. 87.1 ± 15.9 | NS NS | G1-S vs. G1-p < 0.001 G2-S vs. G2-P < 0.001 |
| MDA (nmol/mL) | N/A vs. ↓ | <0.001 | N/A vs. ↑ | 0.026 | NS | ||
| GPx3 (U/mL) | N/A vs. ↑ | <0.001 | N/A vs. ↓ | <0.001 | NS | ||
| TSH (mIU/L) (median) | G1-S: 3.3 vs. 3.2 G2-S: 2.1 vs. 2.5 | NS NS | G1-P: 3.8 vs. 3.8 G2-P: 3.9 vs. 3.4 | NS NS | G1-S vs. G1-P 0.318 G2-S vs. G2-P 0.219 | ||
| fT4 (pmol/L) | G1-S: 15.2 ± 3.1 vs. 14.1 ± 4.5 G2-S: 16.5 ± 2.4 vs. 15.3 ± 2.8 | NS NS | G1-P: 14.7 ± 3.7 vs. 14.3 ± 4.3 G2-P: 15.3 ± 2.5 vs. 15.9 ± 3.9 | NS NS | G1-S vs. G1-P 0.632G2-S vs. G2-P 0.922 | ||
| TPO-Ab (IU/mL) (median) | G1-S: 1020 vs. 873 Δ: −10.7% G2-S: 1310 vs. 960 Δ: −16.7% | <0.05 <0.05 | G1-P: 977 vs. 930 Δ:−1.8% G2-P: 1037 vs. 1090 Δ: 1.2% | NS NS | G1-S vs. G1-P 0.643 Δ:0.105 G2-S vs. G2-P 0.845 Δ: 0.53 | ||
| Yu et al. [36] | 200 twice daily, selenium yeast tablet (3 months) | Se (μg/L) (median) | 23.3 vs. 90.1 Δ:59.8 | <0.05 | 24.0 vs. 39.6 Δ:8.2 | NS | <0.001 Δ: <0.001 |
| Il-2 (pg/mL) (median) | 216 vs. 159 Δ: −68.4 | <0.05 | 212 vs. 227 Δ: −2.63 | NS | <0.001 Δ: <0.001 | ||
| IL-10 (pg/mL) (median) | 15.9 vs. 23.1 Δ: 7.7 | <0.05 | 16.3 vs. 24.7 Δ: 7.3 | <0.05 | 0.754 Δ: 0.80 | ||
| TPO-Ab (%) | 33.6 ± 6.9 vs. 23.6 ± 9.3Δ: −10.0 | <0.05 | 34.5 ± 8.6 vs. 32.0 ± 10.4 Δ: −2.5 | NS | 0.002 Δ: 0.002 | ||
| Tg-Ab (%) | 50.4 ± 10.7 vs. 35.8 ± 15.2Δ: −14.6 | <0.05 | 51.4 ± 11.5 vs. 45.5 ± 14.2 Δ: −6.0 | NS | 0.015 Δ: 0.011 |
| Authors | Supplement, Form, Dose (Duration of Intervention) | Parameter (Unit) | Intervention Group Baseline vs. after Supplementation (Mean ± SD) | p-Value | Control Group Baseline vs. after Placebo (Mean ± SD) | p-Value | p-Value after Supplementationvs. Control |
|---|---|---|---|---|---|---|---|
| Rabbani et al. [30] | 30 mg zinc gluconate/day 250 mg magnesium oxide/day 25,000 IU vitamin A twice a week (10 weeks) | hsCRP (mg/dL) (median) | 3.2 vs. 3.0 Δ: −0.13 | 0.007 | 2.9 vs. 3.2 Δ: 0.18 | 0.004 | 0.154 Δ: <0.001 |
| MDA (mg/dL) (median) | 16.7 vs. 12.3 Δ: −1.60 | 0.408 | 11.0 vs. 12.6 Δ: 0.03 | 0.182 | 0.666 Δ: 0.119 | ||
| TAC (mg/dL) (median) | 2.2 vs. 2.2 Δ: 0.03 | 0.378 | 2.4 vs. 2.1 Δ: −0.14 | 0.004 | 0.364 Δ: 0.007 | ||
| TSH (mIU/L) (median) | 1.6 vs. 1.2 Δ: −0.08 | 0.966 | 1.1 vs. 1.4 Δ: −0.02 | 0.319 | 0.601 Δ: 0.308 | ||
| fT3 (pg/mL) (median) | 3.0 vs. 3.1 Δ: 0.07 | 0.293 | 3.3 vs. 3.2 Δ: 0.10 | 0.984 | 0.179 Δ: 0.473 | ||
| fT4 (ng/dL) (median) | 1.2 vs. 1.4 Δ: 0.12 | 0.002 | 1.3 vs. 1.2 Δ: 0.00 | 0.618 | 0.034 Δ: 0.007 | ||
| TT4 (μg/dL) (median) | 6.6 vs. 6.7 Δ: 0.20 | 0.165 | 6.5 vs. 6.8 Δ: 0.00 | 0.856 | 0.531 Δ: 0.434 | ||
| Nordio and Basciani [42] | Wobenzym vital (4 tablets twice a day for 1 week, 2 tablets twice a day for the rest of the 6 month period) (6 months) W: Wobenzym W + LT4: Wobenzym + LT4 (without placebo; LT4 in the control group) | CRP (mg/L) | W: 6.3 ± 1.9 vs. 2.9 ± 1.3 W + LT4: 6.7 ± 1.4 vs. 2.2 ± 1.2 | <0.05 <0.05 | 5.8 ± 2.8 vs. 3.1 ± 1.8 | NS | N/A |
| TSH (mcIU/mL) | W: 3.3 ± 1.4 vs. 2.6 ± 1.2 W + LT4: 3.8 ± 1.0 vs. 0.7 ± 03 | NS <0.05 | 3.6 ± 1.1 vs. 1.2 ± 0.4 | NS | N/A | ||
| fT3 (N/A) | N/A vs. ↓ | NS | N/A vs. ↓ | NS | N/A | ||
| TPO-Ab (IU/mL) | W: 1017 ± 674 vs. 619 ± 473 W + LT4: 937 ± 518 vs. 475 ± 327 | NS NS | 971 ± 574 vs. 818 ± 379 | NS | N/A | ||
| HTg-Ab (IU/mL) | W: 896 ± 312 vs. 435 ± 323 W + LT4: 814 ± 242 vs. 387 ± 168 | NS <0.05 | 787 ± 298 vs. 662 ± 304 | NS | N/A | ||
| HTg (ng/mL) | W: 37.6 ± 16.1 vs. 16.4 ± 9.3 W + LT4: 38.8 ± 13.9 vs. 14.5 ± 10.7 | <0.05 <0.05 | 41.1 ± 11.7 vs. 36.6 ± 12.3 | NS | N/A | ||
| Farhangi and Tajmiri [28] | 2 g/day Nigella sativa powder (8 weeks) | MDA (nmol/mL) | 1.7 ± 0.7 vs. 1.4 ± 0.4 | 0.034 | 1.7 ± 0.7 vs. 1.6 ± 0.6 | 0.53 | 0.53 |
| TAC (nmol/l) | 1.3 ± 0.3 vs. 1.4 ± 0.3 | 0.04 | 1.1 ± 0.4 vs. 1.2 ± 0.3 | 0.182 | 0.41 | ||
| SOD (IU/L) | 1286 ± 351 vs. 1390 ± 282 | 0.05 | 1251 ± 980 vs. 1211 ± 357 | 0.98 | 0.67 | ||
| GPx (IU/L) | 45.1 ± 17.9 vs. 47.0 ± 10.6 | 0.56 | 39.2 ± 18.1 vs. 40.6 ± 3.8 | 0.67 | 0.61 | ||
| TSH (mIU/L) | 6.4 ± 3.9 vs. 4.1 ± 2.4 | 0.03 | 8.1 ± 7.3 vs. 8.3 ± 7.2 | 0.40 | 0.02 | ||
| T3 (mmol/L) | 0.9 ± 0.3 vs. 1.1 ± 0.3 | 0.008 | 1.2 ± 0.4 vs. 1.2 ± 0.4 | 0.15 | 0.39 | ||
| T4 (mmol/L) | 8.1 ± 2.6 vs. 8.9 ± 1.4 | 0.21 | 8.0 ± 3.1 vs. 7.7 ± 2.2 | 0.32 | 0.04 | ||
| TPO-Ab (IU/mL) | 295 ± 210 vs. 148 ± 158 | 0.019 | 278 ± 171 vs. 274 ± 167 | 0.28 | 0.01 | ||
| Zhang et al. [3] | 600 mg/day genistein (purified soy extract) (1 month) | IL-2 (pg/mL) | 11.8 ± 2.2 vs. 7.5 ± 1.9 | <0.01 | N/A | NS | N/A |
| IL-4 (pg/mL) | N/A | NS | N/A | NS | N/A | ||
| IL-6 (pg/mL) | N/A | NS | N/A | NS | N/A | ||
| IL-10 (pg/mL) | N/A | NS | N/A | NS | N/A | ||
| IFN-γ (ng/mL) | 12.0 vs. 16.4 | <0.05 | N/A | NS | N/A | ||
| TNF-α (pg/mL) | no change | NS | N/A | NS | N/A | ||
| Zhang et al. [3] | 600 mg/day genistein (purified soy extract) (1 month) | TSH (mU/L) | 12.8 ± 3.1 vs. 8.8 ± 2.3 | <0.01 | N/A | N/A | N/A |
| T3 (ng/mL) | 112 ± 26.5 vs. 131 ± 25.3 | NS | N/A | N/A | N/A | ||
| T4 (μg/dL) | 9.5 ± 2.5 vs. 12.7 ± 2.7 | <0.05 | N/A | N/A | N/A | ||
| fT4 (μg/dL) | 0.9 ± 0.2 vs. 1.3 ± 0.3 | <0.01 | N/A | N/A | N/A | ||
| TPO-Ab (U/mL) | 1108 ± 239 vs. 789 ± 173 | <0.01 | N/A | N/A | N/A | ||
| Tg-Ab (U/mL) | 764 ± 152 vs. 436 ± 146 | <0.01 | N/A | N/A | N/A | ||
| Tomella et al. [42] | Fermented papaya-based nutraceutical, 3 g twice a day (6 months) | MDA (μmol/L) | N/A vs. 0.3 ± 0.3 | NS | N/A vs. 0.7 ± 0.2 | <0.01 | <0.05 |
| L-HPX (nmol/L) | N/A vs. 3.1 ± 0.8 | NS | N/A vs. 6.2 ± 0.6 | <0.01 | <0.05 | ||
| SOD (U/L) | N/A vs. 30.8 ± 2.6 | NS | N/A vs. 23.6 ± 2.2 | NS | <0.05 | ||
| GPx (U/L) | N/A vs. 649 ± 94.3 | NS | N/A vs. 689 ± 102 | <0.01 | <0.05 | ||
| Talebi et al. [32] | Familact (synbiotic) 500 mg/day: (8 weeks) | CRP (mg/dL) | 1.4 ± 0.5 vs. 2.5 ± 0.9 Δ: 0.58 | 0.006 | 2.5 ± 1.0 vs. 1.6 ± 0.3 Δ: 0.34 | 0.250 | 0.699 |
| TSH (μUI/mL) | 2.0 ± 0.3 vs. 1.4 ± 0.2 Δ: −0.28 | 0.007 | 1.5 ± 0.2 vs. 1.3 ± 0.2 Δ: −0.08 | 0.358 | 0.374 | ||
| fT3 (pg/mL) | 2.4 ± 0.1 vs. 2.8 ± 0.1 Δ: 0.38 | 0.001 | 2.3 ± 0.1 vs. 2.7 ± 0.04 Δ: 0.35 | 0.001 | 0.259 | ||
| TPO-Ab (IU/mL) | 220 ± 38.9 vs. 233 ± 40.5 Δ: 13.6 | 0.161 | 118 ± 36.4 vs. 121 ± 36.2 Δ: 2.78 | 0.157 | 0.317 | ||
| Xiang et al. [26] | Alpha lipoic acid 300 mg/day (3 weeks) | CRP (mg/L) | 2.9 ± 0.4 vs. 2.5 ± 0.5 | NS | 2.7 ± 0.4 vs. 2.8 ± 0.4 | NS | N/A |
| TSH (mU/L) | 9.3 ± 2.8 vs. 10.2 ± 2.8 | NS | 10.5 ± 2.5 vs. 11.1 ± 2.5 | NS | N/A | ||
| fT3 (pmol/L) | 5.1 ± 0.6 vs. 5.2 ± 0.7 | NS | 5.0 ± 0.7 vs. 5.2 ± 0.6 | NS | N/A | ||
| fT4 (pmol/L) | 14.0 ± 2.1 vs. 14.8 ± 2.0 | NS | 15.0 ± 2.2 vs. 14.9 ± 2.6 | NS | N/A | ||
| TPO-Ab (U/mL) | 542 ± 287 vs. 582 ± 295 | NS | 506 ± 268 vs. 496 ± 298 | NS | N/A | ||
| Tg-Ab (U/mL) | 465 ± 306 vs. 487 ± 289 | NS | 492 ± 311 vs. 473 ± 295 | NS | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kubiak, K.; Szmidt, M.K.; Kaluza, J.; Zylka, A.; Sicinska, E. Do Dietary Supplements Affect Inflammation, Oxidative Stress, and Antioxidant Status in Adults with Hypothyroidism or Hashimoto’s Disease?—A Systematic Review of Controlled Trials. Antioxidants 2023, 12, 1798. https://doi.org/10.3390/antiox12101798
Kubiak K, Szmidt MK, Kaluza J, Zylka A, Sicinska E. Do Dietary Supplements Affect Inflammation, Oxidative Stress, and Antioxidant Status in Adults with Hypothyroidism or Hashimoto’s Disease?—A Systematic Review of Controlled Trials. Antioxidants. 2023; 12(10):1798. https://doi.org/10.3390/antiox12101798
Chicago/Turabian StyleKubiak, Katarzyna, Maria Karolina Szmidt, Joanna Kaluza, Agnieszka Zylka, and Ewa Sicinska. 2023. "Do Dietary Supplements Affect Inflammation, Oxidative Stress, and Antioxidant Status in Adults with Hypothyroidism or Hashimoto’s Disease?—A Systematic Review of Controlled Trials" Antioxidants 12, no. 10: 1798. https://doi.org/10.3390/antiox12101798
APA StyleKubiak, K., Szmidt, M. K., Kaluza, J., Zylka, A., & Sicinska, E. (2023). Do Dietary Supplements Affect Inflammation, Oxidative Stress, and Antioxidant Status in Adults with Hypothyroidism or Hashimoto’s Disease?—A Systematic Review of Controlled Trials. Antioxidants, 12(10), 1798. https://doi.org/10.3390/antiox12101798