
A Cluster Randomized Controlled Trial Feasibility Study of a WhatsApp-Delivered Intervention to Promote Healthy Eating Habits in Male Firefighters


Abstract
:1. Introduction
2. Materials and Methods
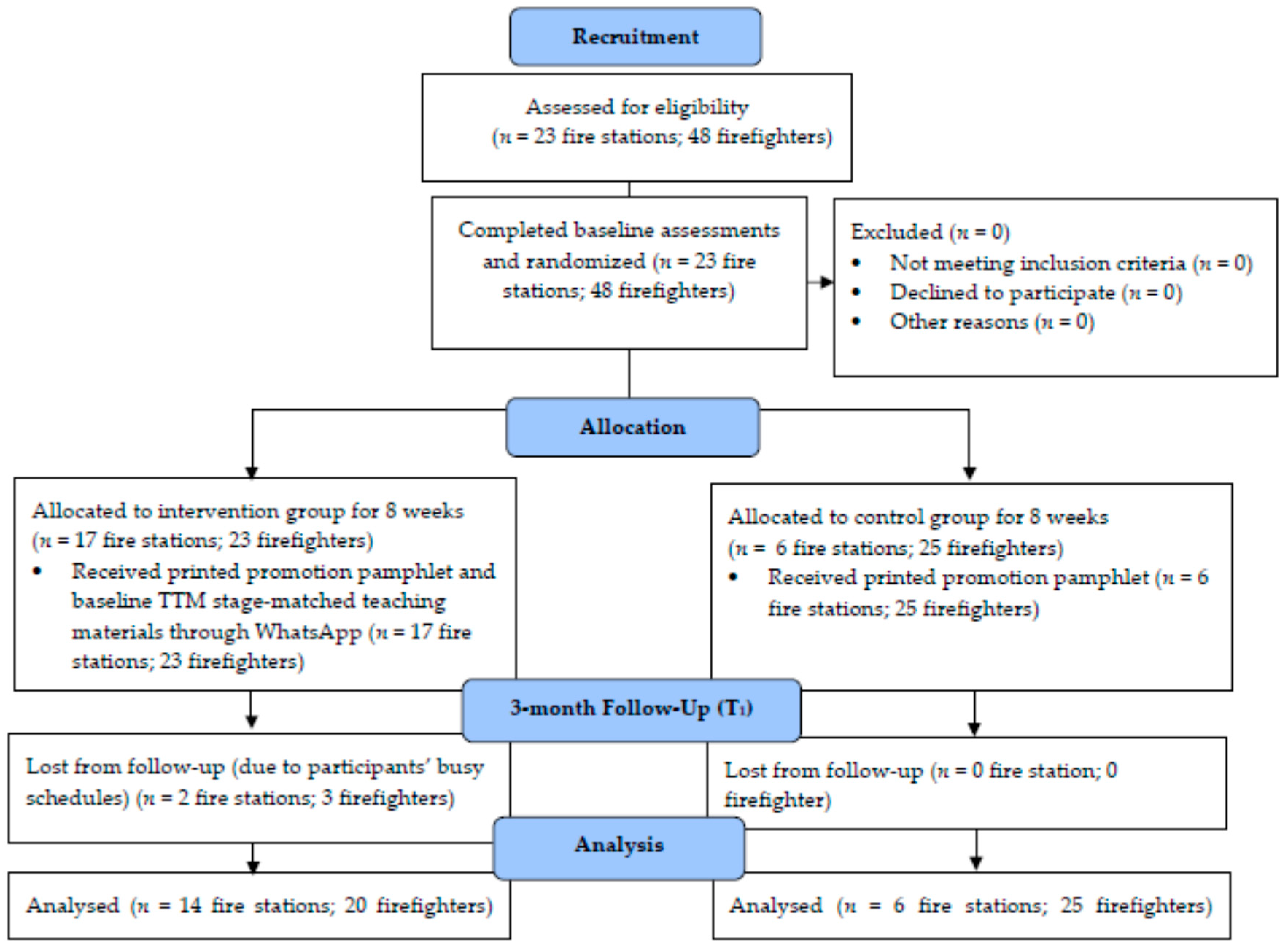
2.1. Study Design
2.2. Sample Size
2.3. Participants
2.4. Procedures
2.5. Interventions
2.5.1. Intervention and Control Groups
2.5.2. Fidelity of Teaching Materials and Pamphlet
2.5.3. Validity and Reliability for Questionnaire
2.6. Measures
2.6.1. F&V Consumption
2.6.2. Practicality and Implementation
2.7. Statistical Analysis
3. Results
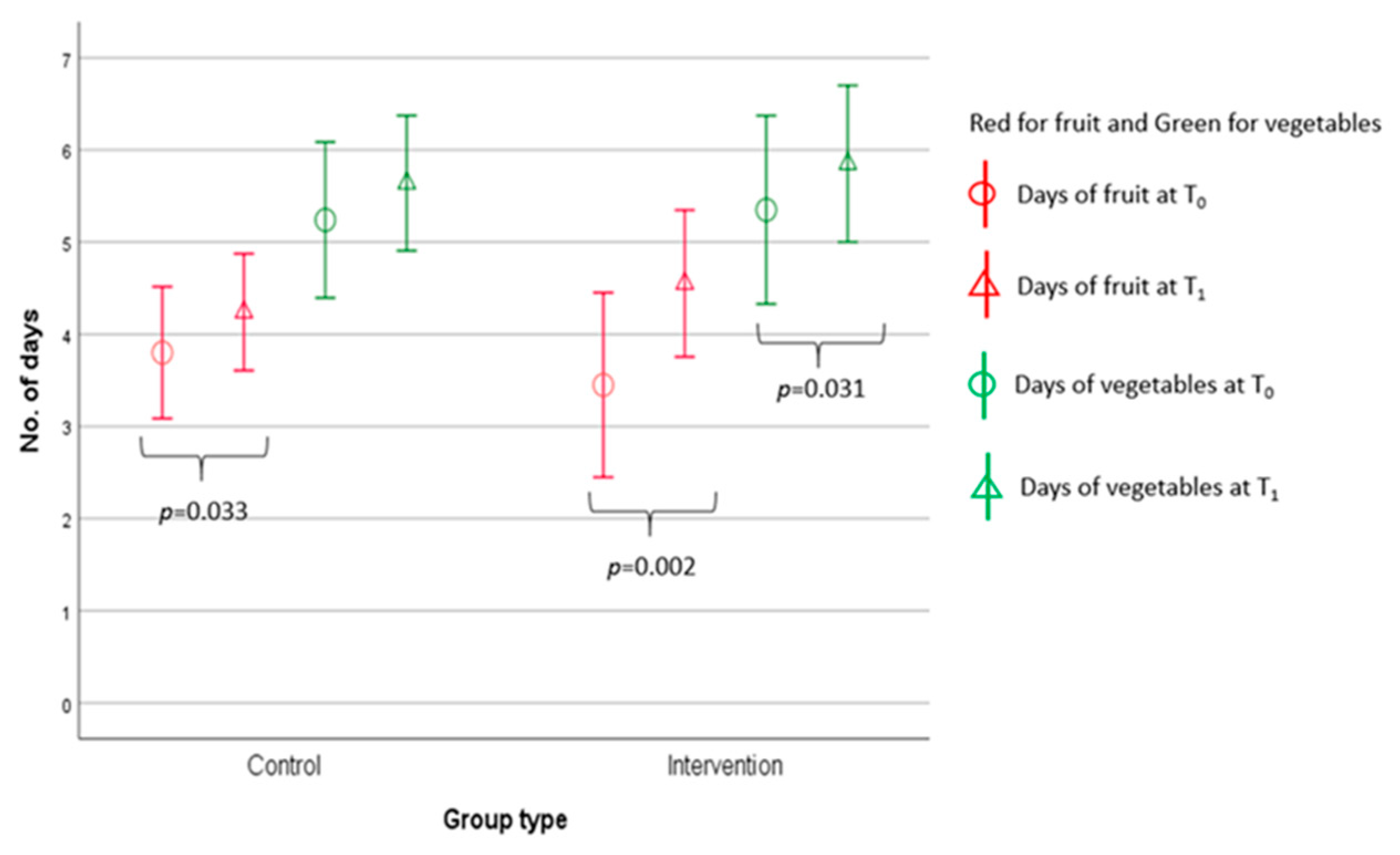
3.1. Eating Habits
3.1.1. Number of Days of F&V Intake within a Week
3.1.2. Number of Servings of F&V Intake Per Day
3.2. Recruitment
3.3. Retention
3.4. Practicality
3.5. Implementation
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mo, X.; Gai, R.T.; Sawada, K.; Takahashi, Y.; Cox, S.E.; Nakayama, T.; Mori, R. Coronary heart disease and stroke disease burden attributable to fruit and vegetable intake in Japan: Projected DALYS to 2060. (Disability Adjusted Life Years) (Report). BMC Public Health 2019, 19. [Google Scholar] [CrossRef] [Green Version]
- Volpe, L.S. Fruit and Vegetable Intake and Prevention of Chronic Disease. ACSMʼs Health Fit. J. 2019, 23, 30–31. [Google Scholar] [CrossRef]
- Angelino, D.; Godos, J.; Ghelfi, F.; Tieri, M.; Titta, L.; Lafranconi, A.; Marventano, S.; Alonzo, E.; Gambera, A.; Sciacca, S. Fruit and vegetable consumption and health outcomes: An umbrella review of observational studies. Int. J. Food Sci. Nutr. 2019, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Munir, F.; Clemes, S.; Houdmont, J.; Randall, R. Overweight and obesity in UK firefighters. Occup. Med. 2012, 62, 362–365. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.L. Firefighter fitness: Improving performance and preventing injuries and fatalities. Curr. Sports Med. Rep. 2011, 10, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, D.; Au, C.T.; Lee, F.Y.; So, R.C.; Wong, J.P.; Mak, G.Y.; Chien, E.P.; McManus, A.M. Association between Leisure Time Physical Activity, Cardiopulmonary Fitness, Cardiovascular Risk Factors, and Cardiovascular Workload at Work in Firefighters. Saf. Health Work 2015, 6, 192–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavie, C.J.; Thomas, R.J.; Squires, R.W.; Allison, T.G.; Milani, R.V. Exercise training and cardiac rehabilitation in primary and secondary prevention of coronary heart disease. (SYMPOSIUM ON CARDIOVASCULAR DISEASES) (Report). Mayo Clin. Proc. 2009, 84, 373. [Google Scholar] [CrossRef] [Green Version]
- Muegge, C.M.; Zollinger, T.W.; Song, Y.; Wessel, J.; Monahan, P.O.; Moffatt, S.M. Barriers to Weight Management Among Overweight and Obese Firefighters. J. Occup. Environ. Med. 2020, 62, 37. [Google Scholar] [CrossRef]
- Ranby, K.W.; MacKinnon, D.P.; Fairchild, A.J.; Elliot, D.L.; Kuehl, K.S.; Goldberg, L. The PHLAME (Promoting Healthy Lifestyles: Alternative Models’ Effects) firefighter study: Testing mediating mechanisms. J. Occup. Health Psychol. 2011, 16, 501–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kales, S.N.; Soteriades, E.S.; Christophi, C.A.; Christiani, D.C. Emergency duties and deaths from heart disease among firefighters in the United States. NEJM 2007, 356, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Fahy, R.F.; LeBlanc, P.R.; Molis, J.L. Firefighter fatalities in the United States—2014. NFPA J. 2015, 109, 72–81. [Google Scholar]
- Scheer, F.A.; Morris, C.J.; Shea, S.A. The internal circadian clock increases hunger and appetite in the evening independent of food intake and other behaviors. Obesity 2013, 21, 421–423. [Google Scholar] [CrossRef]
- Sargent, C.; Zhou, X.; Matthews, R.W.; Darwent, D.; Roach, G.D. Daily rhythms of hunger and satiety in healthy men during one week of sleep restriction and circadian misalignment. Int. J. Environ. Res. Public Health 2016, 13, 170. [Google Scholar] [CrossRef] [Green Version]
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D. Dietary quality among men and women in 187 countries in 1990 and 2010: A systematic assessment. Lancet Glob. Health 2015, 3, e132–e142. [Google Scholar] [CrossRef] [Green Version]
- MacKinnon, D.P.; Elliot, D.L.; Thoemmes, F.; Kuehl, K.S.; Moe, E.L.; Goldberg, L.; Burrell, G.L.; Ranby, K.W. Long-term effects of a worksite health promotion program for firefighters. Am. J. Health Behav. 2010, 34, 695–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, B.; Dobson, M.; Schnall, P.; Garcia-Rivas, J. 24-hour work shifts, sedentary work, and obesity in male firefighters. Am. J. Ind. Med. 2016, 59, 486–500. [Google Scholar] [CrossRef]
- Cheung, K. Report on the Study of Hypertension and Eating Habits among Firefighters; The Hong Kong Polytechnic University: Hong Kong, China, 2012. [Google Scholar]
- Dehghan, M.; Akhtar-Danesh, N.; Merchant, A. Factors associated with fruit and vegetable consumption among adults. J. Hum. Nutr. Diet. 2011, 24, 128–134. [Google Scholar] [CrossRef]
- Slavin, J.; Green, H. Dietary fibre and satiety. Nutr. Bull. 2007, 32, 32–42. [Google Scholar] [CrossRef]
- Jih, J.; Le, G.; Woo, K.; Tsoh, J.Y.; Stewart, S.; Gildengorin, G.; Burke, A.; Ching, W.; Chan, E.; Lei-Chun, F.; et al. Educational Interventions to Promote Healthy Nutrition and Physical Activity Among Older Chinese Americans: A Cluster-Randomized Trial. Am. J. Public Health 2016, 106, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Unified Fire Authority. Firefighter Work Schedule. Available online: https://unifiedfire.org/work-schedule/ (accessed on 11 May 2021).
- Hampshire Fire and Resue Service. Hours and Pay. Available online: https://www.hantsfire.gov.uk/work-with-us/about-our-careers/firefighter/hours-and-pay/ (accessed on 11 May 2021).
- Standing Committee on Disciplined Services Salaries and Conditions of Service. Report on the Grade Structure Review of the Disciplined Services. Available online: https://www.jsscs.gov.hk/reports/en/scds_gs_08/gs_2008.pdf (accessed on 11 May 2021).
- Park, S.; Kwon, J.; Noh, K.; Lee, C.G.; Song, W.; Park, J.-j.; Lee, H.-j.; Seo, D.-i.; Kang, H.J.; Ahn, Y.S. Relationship between shift type and voluntary exercise training in South Korean firefighters. Int. J. Environ. Res. Public Health 2020, 17, 728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Menezes, M.C.; Mingoti, S.A.; Cardoso, C.S.; de Deus Mendonça, R.; Lopes, A.C.S. Intervention based on Transtheoretical Model promotes anthropometric and nutritional improvements—A randomized controlled trial. Eat. Behav. 2015, 17, 37–44. [Google Scholar] [CrossRef]
- Number of Monthly Active WhatsApp Users Worldwide from April 2013 to December 2017. Available online: https://www.statista.com/statistics/260819/number-of-monthly-active-whatsapp-users/ (accessed on 16 March 2021).
- Othman, M.; Menon, V. Developing a nationwide spine care referral programme on the WhatsApp messenger platform: The Oman experiment. Int. J. Med. Inform. 2019, 126, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Rajini, S.; Kannan, K.; Alli, P. Study on Prevalence of Whatsapp Addiction among Medical Students in a Private Medical College, Pondicherry. Indian J. Public Health Res. Dev. 2018, 9, 113–116. [Google Scholar] [CrossRef]
- Carfora, V.; Caso, D.; Conner, M. Randomized controlled trial of a messaging intervention to increase fruit and vegetable intake in adolescents: Affective versus instrumental messages. Br. J. Health Psychol. 2016, 21, 937–955. [Google Scholar] [CrossRef]
- Inauen, J.; Bolger, N.; E Shrout, P.; Stadler, G.; Amrein, M.; Rackow, P.; Scholz, U. Using Smartphone-Based Support Groups to Promote Healthy Eating in Daily Life: A Randomized Trial. Appl. Psychol. Health Well-Being 2017, 9, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leme, A.C.B.; Lubans, D.R.; Guerra, P.H.; Dewar, D.; Toassa, E.C.; Philippi, S.T. Preventing obesity among Brazilian adolescent girls: Six-month outcomes of the Healthy Habits, Healthy Girls–Brazil school-based randomized controlled trial. Prev. Med. 2016, 86, 77–83. [Google Scholar] [CrossRef]
- Painter, J.E.; Borba, C.P.; Hynes, M.; Mays, D.; Glanz, K. The use of theory in health behavior research from 2000 to 2005: A systematic review. Ann. Behav. Med. 2008, 35, 358. [Google Scholar] [CrossRef] [PubMed]
- Moe, E.L.; Elliot, D.L.; Goldberg, L.; Kuehl, K.S.; Stevens, V.J.; Breger, R.K.R.; DeFrancesco, C.L.; Ernst, D.; Duncan, T.; Dulacki, K.; et al. Promoting Healthy Lifestyles: Alternative Models’ Effects (PHLAME). Health Educ. Res. 2002, 17, 586–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliot, D.L.; Goldberg, L.; Duncan, T.E.; Kuehl, K.S.; Moe, E.L.; Breger, R.K.; DeFrancesco, C.L.; Ernst, D.B.; Stevens, V.J. The PHLAME firefighters’ study: Feasibility and findings. Am. J. Health Behav. 2004, 28, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; DiClemente, C.C. Stages and Processes of Self-Change of Smoking: Toward an Integrative Model of Change. J. Consult. Clin. Psychol. 1983, 51, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Spencer, L.; Wharton, C.; Moyle, S.; Adams, T. The transtheoretical model as applied to dietary behaviour and outcomes. Nutr. Res. Rev. 2007, 20, 46–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuah, N.; Amiel, C.; Qureshi, S.; Car, J.; Kaur, B.; Majeed, A. Transtheoretical model for dietary and physical exercise modification in weight loss management for overweight and obese adults. Cochrane Database Syst. Rev. 2011, 10. [Google Scholar] [CrossRef]
- de Menezes, M.C.; Bedeschi, L.B.; dos Santos, L.C.; Lopes, A.C.S. Interventions directed at eating habits and physical activity using the Transtheoretical Model: A systematic review. Nutr. Hosp. 2016, 33, 1194–1204. [Google Scholar]
- Polit, D.F.; Beck, C. Nursing Research: Principles and Methods, 7th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2004. [Google Scholar]
- Hertzog, M.A. Considerations in determining sample size for pilot studies. Res. Nurs. Health 2008, 31, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Martins, R.K.; McNeil, D.W. Review of motivational interviewing in promoting health behaviors. Clin. Psychol. Rev. 2009, 29, 283–293. [Google Scholar] [CrossRef]
- Diaz, D.P. Comparison of Student Characteristics, and Evaluation of Student Success, in an Online Health Education Course. Ph.D. Thesis, Nova Southeastern University, Fort Lauderdale, FL, USA, 2000. [Google Scholar]
- Di Noia, J.; Prochaska, J.O. Mediating variables in a transtheoretical model dietary intervention program. Health Educ. Behav. 2010, 37, 753–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gnau, J. A Feasibility Study on the Implementation of a Web-Based Intuitive Eating Program in a University Setting. Master’s Thesis, Missouri State University, Springfield, MI, USA, 2020. [Google Scholar]
- Center for Health Promotion Research. PHLAME Team Leader Manual (Kin Cheung, School of Nursing, The Hong Kong Polytechnic University, Translation in Chinese in 2017); Oregon Health & Science University: Portland, OR, USA, 2005. [Google Scholar]
- Centre for Food Safety. Nutrient Values of Fruit and Vegetables–Risk Assessment Studies—Report No. 28; Centre for Food Safety: Hong Kong, China, 2007. [Google Scholar]
- Department of Health (Hong Kong SAR Government). Eat Smart Anytime and Anywhere. Available online: https://www.change4health.gov.hk/en/healthy_diet/facts/eat_smart/index.html (accessed on 11 May 2021).
- Lee, J.E.; Lee, D.E.; Kim, K.; Shim, J.E.; Sung, E.; Kang, J.H.; Hwang, J.Y. Development of tailored nutrition information messages based on the transtheoretical model for smartphone application of an obesity prevention and management program for elementary-school students. Nutr. Res. Pract. 2017, 11, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Department of Health. Behavioral Risk Factor Survey (April 2016); Surveillance and Epidemiology Branch, Centre for Health Protection, Department of Health: Hong Kong, China, 2016. [Google Scholar]
- Dobson, M.; Choi, B.; Schnall Peter, L.; Wigger, E.; Garcia-Rivas, J.; Israel, L.; Baker Dean, B. Exploring Occupational and Health Behavioral Causes of Firefighter Obesity: A Qualitative Study. Am. J. Ind. Med. 2013, 56, 776–790. [Google Scholar] [CrossRef]
- Ohkuma, T.; Hirakawa, Y.; Nakamura, U.; Kiyohara, Y.; Kitazono, T.; Ninomiya, T. Association between eating rate and obesity: A systematic review and meta-analysis. Int. J. Obes. 2015, 39, 1589–1596. [Google Scholar] [CrossRef]
- Thompson, T.P.; Greaves, C.J.; Ayres, R.; Aveyard, P.; Warren, F.C.; Byng, R.; Taylor, R.S.; Campbell, J.L.; Ussher, M.; Michie, S. Factors associated with study attrition in a pilot randomised controlled trial to explore the role of exercise-assisted reduction to stop (EARS) smoking in disadvantaged groups. Trials 2016, 17, 524. [Google Scholar] [CrossRef] [Green Version]
- Kornelia, N.B.; Linda, C.M.; Marc, N.P. Risk-taking and decision-making in youth: Relationships to addiction vulnerability. J. Behav. Addict. 2013, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Van Beijsterveldt, C.; Van Boxtel, M.; Bosma, H.; Houx, P.; Buntinx, F.; Jolles, J. Predictors of attrition in a longitudinal cognitive aging study: The Maastricht Aging Study (MAAS). J. Clin. Epidemiol. 2002, 55, 216–223. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.; Steele, M.; Stuart, B.; Joseph, J.; Miller, S.; Morrison, L.; Little, P.; Yardley, L. Using an analysis of behavior change to inform effective digital intervention design: How did the PRIMIT website change hand hygiene behavior across 8993 users? Ann. Behav. Med. 2017, 51, 423–431. [Google Scholar] [CrossRef] [Green Version]
- Van der Mispel, C.; Poppe, L.; Crombez, G.; Verloigne, M.; De Bourdeaudhuij, I. A Self-Regulation-Based eHealth Intervention to Promote a Healthy Lifestyle: Investigating User and Website Characteristics Related to Attrition. J. Med. Int. Res. 2017, 19, e241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiman, T.; Olenik-Shemesh, D. Perceived body appearance and eating habits: The voice of young and adult students attending higher education. Int. J. Environ. Res. Public Health 2019, 16, 451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weeks, M. Effectiveness of Wellness Programming to Improve Health and Fitness Metrics in Rural Firefighters. Ph.D. Thesis, Georgia Southern University, Statesboro, Georgia, 2020. [Google Scholar]
- Soliman, G.A.; Kim, J.; Lee, J.-M.; High, R.; Hortman, S.; Kim, Y.; Wehbi, N.K.; Canedy, J. Wellness programme at the workplace promotes dietary change and improves health indicators in a longitudinal retrospective study. Public Health Nutr. 2019, 22, 354–362. [Google Scholar] [CrossRef]
- Nitzke, S.; Kritsch, K.; Boeckner, L.; Greene, G.; Hoerr, S.; Horacek, T.; Kattelmann, K.; Lohse, B.; Oakland, M.J.; Phillips, B. A stage-tailored multi-modal intervention increases fruit and vegetable intakes of low-income young adults. Am. J. Health Promot. 2007, 22, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Mastellos, N.; Gunn, L.H.; Felix, L.M.; Car, J.; Majeed, A. Transtheoretical model stages of change for dietary and physical exercise modification in weight loss management for overweight and obese adults. CLIB 2014. [Google Scholar] [CrossRef] [Green Version]
- De Vet, E.; De Nooijer, J.; De Vries, N.K.; Brug, J. Comparing stage of change and behavioral intention to understand fruit intake. Health Educ. Res. 2007, 22, 599–608. [Google Scholar] [CrossRef] [Green Version]
- Amrein, M.A.; Rackow, P.; Inauen, J.; Radtke, T.; Scholz, U. The role of Compensatory Health Beliefs in eating behavior change: A mixed method study. Appetite 2017, 116, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Gholami, M.; Wiedemann, A.; Knoll, N.; Schwarzer, R. Mothers improve their daughters’ vegetable intake: A randomized controlled trial. Psychol. Health Med. 2015, 20, 1–7. [Google Scholar] [CrossRef]
- Kerr, D.A.; Harray, A.J.; Pollard, C.M.; Dhaliwal, S.S.; Delp, E.J.; Howat, P.A.; Pickering, M.R.; Ahmad, Z.; Meng, X.; Pratt, I.S. The connecting health and technology study: A 6-month randomized controlled trial to improve nutrition behaviours using a mobile food record and text messaging support in young adults. Inte. J. Behav. Nutr. Phys. Act. 2016, 13, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahril, M.R.; Wan Dali, W.P.E.; Lua, P.L. A 10-week multimodal nutrition education intervention improves dietary intake among university students: Cluster randomised controlled trial. J. Nutr. Metab. 2013, 2013, 11. [Google Scholar] [CrossRef] [PubMed]
- Chu, J.T.; Wang, M.P.; Shen, C.; Lam, T.H.; Viswanath, K.; Chan, S.S.C. How, when and why people seek health information online: Qualitative study in Hong Kong. Interact. J. Med. Res. 2017, 6, e7000. [Google Scholar] [CrossRef] [Green Version]
- Pollard, J.; Kirk, S.L.; Cade, J.E. Factors affecting food choice in relation to fruit and vegetable intake: A review. Nutr. Res. Rev. 2002, 15, 373–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Characteristics | Total (N = 45) | Intervention (n = 20) | Control (n = 25) |
|---|---|---|---|
| Age (Years) | 35.0 ± 9.6 | 32.9 ± 9.5 | 36.6 ± 9.6 |
| Years of work experience (Years) | 11.3 ± 9.9 | 9.4 ± 9.6 | 12.8 ± 10.1 |
| Marital status (%) | |||
| Single | 47 | 55 | 40 |
| Married | 51 | 40 | 60 |
| Divorced | 2 | 5 | 0 |
| Current major duty (%) | |||
| Front-line | 93 | 95 | 92 |
| Management work | 4 | 0 | 8 |
| Others | 2 | 5 | 0 |
| Current position (%) | |||
| Fireman | 62 | 70 | 56 |
| Senior fireman | 16 | 5 | 24 |
| Principal fireman | 11 | 10 | 12 |
| Probationary station officer | 9 | 15 | 4 |
| Senior station officer | 2 | 0 | 4 |
| Time | Serving | Total (N = 45) n (%) | Intervention (n = 20) n (%) | Control (n = 25) n (%) | p |
|---|---|---|---|---|---|
| T0 | <2 servings of fruits and <3 servings of vegetables 1 | 37 (82) | 17 (85) | 37 (82) | 0.304 |
| ≥2 servings of fruits or ≥3 servings of vegetables | 8 (18) | 3 (15) | 8 (18) | ||
| T1 | <2 servings of fruits and <3 servings of vegetables | 28 (62) | 12 (60) | 28 (62) | 0.789 |
| ≥2 servings of fruits or ≥3 servings of vegetables | 17 (38) | 8 (40) | 17 (38) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, W.W.M.; Wong, A.S.W.; Cheung, K. A Cluster Randomized Controlled Trial Feasibility Study of a WhatsApp-Delivered Intervention to Promote Healthy Eating Habits in Male Firefighters. Int. J. Environ. Res. Public Health 2021, 18, 6633. https://doi.org/10.3390/ijerph18126633
Ng WWM, Wong ASW, Cheung K. A Cluster Randomized Controlled Trial Feasibility Study of a WhatsApp-Delivered Intervention to Promote Healthy Eating Habits in Male Firefighters. International Journal of Environmental Research and Public Health. 2021; 18(12):6633. https://doi.org/10.3390/ijerph18126633
Chicago/Turabian StyleNg, Winnie Wing Man, Anthony Siu Wo Wong, and Kin Cheung. 2021. "A Cluster Randomized Controlled Trial Feasibility Study of a WhatsApp-Delivered Intervention to Promote Healthy Eating Habits in Male Firefighters" International Journal of Environmental Research and Public Health 18, no. 12: 6633. https://doi.org/10.3390/ijerph18126633
APA StyleNg, W. W. M., Wong, A. S. W., & Cheung, K. (2021). A Cluster Randomized Controlled Trial Feasibility Study of a WhatsApp-Delivered Intervention to Promote Healthy Eating Habits in Male Firefighters. International Journal of Environmental Research and Public Health, 18(12), 6633. https://doi.org/10.3390/ijerph18126633