Understanding Factors Influencing Elderly Diabetic Patients’ Continuance Intention to Use Digital Health Wearables: Extending the Technology Acceptance Model (TAM)




Abstract
1. Introduction
2. Literature Reviews
2.1. Digital Health Wearables
2.2. Digital Health Wearables and Diabetes Management
2.3. Technology Acceptance Model (TAM)
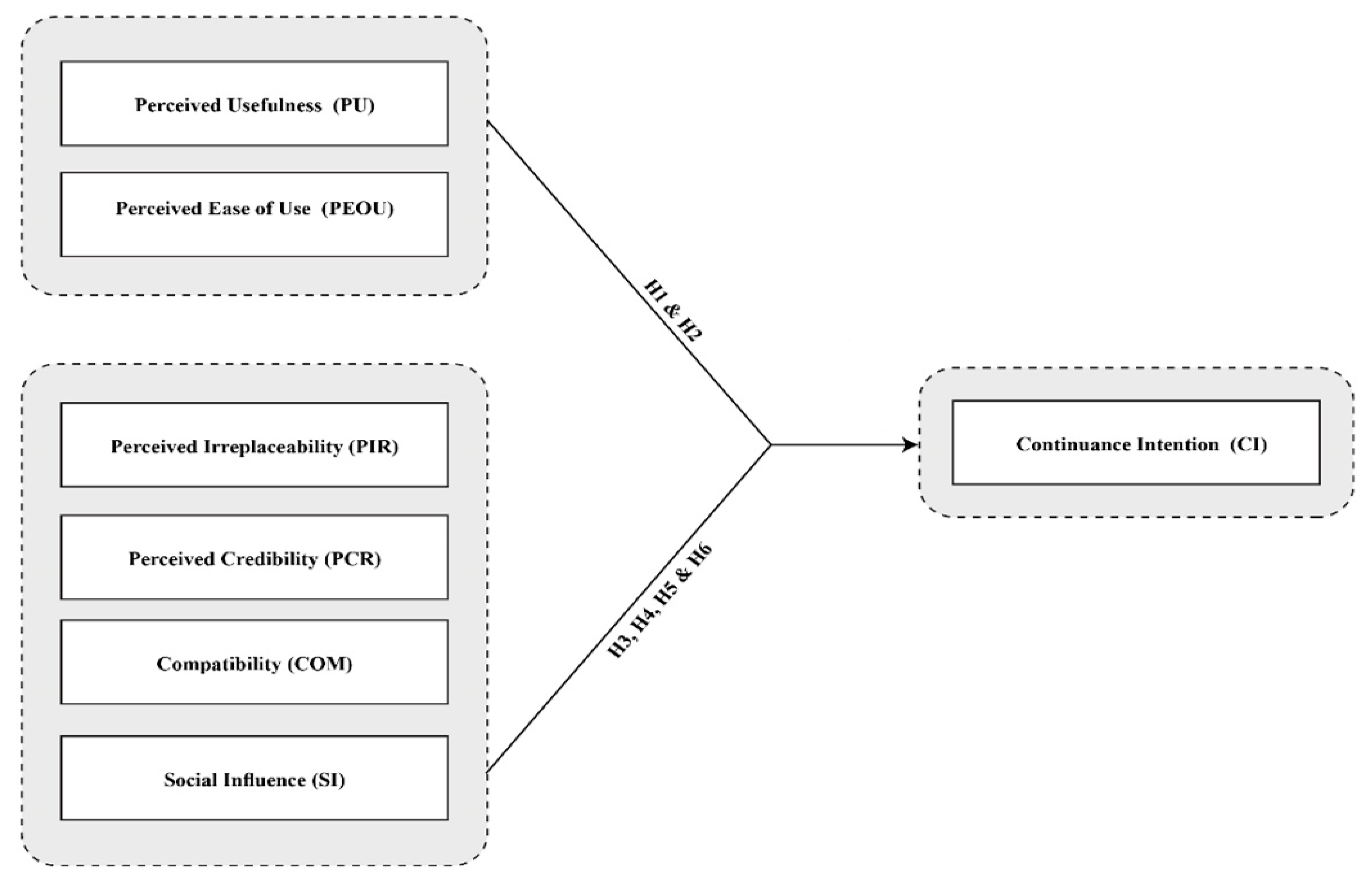
3. Development of Hypotheses
3.1. Perceived Usefulness (PU), Perceived Ease of Use (PEOU) and Continuance Intention (CI)
3.2. Perceived Irreplaceability (PIR)
3.3. Perceived Credibility (PCR)
3.4. Compatibility (COM)
3.5. Social Influence (SI)
4. Questionnaire Design and Data Collection
4.1. Sample
4.2. Measures and Instrument Development
5. Data Analysis and Results
5.1. Measurement Model
5.2. Structural Model Testing
6. Discussion and Conclusions
6.1. Implications for Theory
6.2. Implications for Practice
6.3. Limitations and Directions for Future Research
Author Contributions
Funding
Conflicts of Interest
References
- Talukder, M.S.; Sorwar, G.; Bao, Y.; Ahmed, J.U.; Palash, M.A.S. Predicting antecedents of wearable healthcare technology acceptance by elderly: A combined SEM-Neural Network approach. Technol. Forecast. Soc. Chang. 2020, 150, 119793. [Google Scholar] [CrossRef]
- Quaosar, G.A.A.; Hoque, M.R.; Bao, Y. Investigating factors affecting Elderly’s intention to use m-health services: An empirical study. Telemed. J. E Health 2018, 24, 309–314. [Google Scholar] [CrossRef]
- Khanam, M.A.; Streatfield, P.K.; Kabir, Z.N.; Qiu, C.; Cornelius, C.; Wahlin, Å. Prevalence and patterns of multimorbidity among elderly people in rural Bangladesh: A cross-sectional study. J. Health Popul Nutr. 2011, 29, 406. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, A.A. Nutritional challenges in the elderly with diabetes. Int. J. Diabetes Mellit. 2009, 1, 26–31. [Google Scholar] [CrossRef]
- Afroz, A.; Ali, L.; Karim, M.N.; Alramadan, M.J.; Alam, K.; Magliano, D.J.; Billah, B. Glycaemic Control for People with Type 2 Diabetes Mellitus in Bangladesh—An urgent need for optimization of management plan. Sci. Rep. 2019, 9, 10248. [Google Scholar] [CrossRef]
- Atlas, D.; International Diabetes Federation. IDF Diabetes Atlas; International Diabetes Federation: Brussels, Belgium, 2015. [Google Scholar]
- Kekade, S.; Hseieh, C.-H.; Islam, M.M.; Atique, S.; Mohammed Khalfan, A.; Li, Y.-C.; Abdul, S.S. The usefulness and actual use of wearable devices among the elderly population. Comput. Methods Programs Biomed. 2018, 153, 137–159. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Lee, K. Factors that influence an individual’s intention to adopt a wearable healthcare device: The case of a wearable fitness tracker. Technol. Forecast. Soc. Chang. 2018, 129, 154–163. [Google Scholar] [CrossRef]
- Ataide, E.J.G.; Sinha, R.K.; Maiya, G.A. Understanding the Need for a Non-invasive Wearable Real-time Database Device for Diabetic Patients. J. Health Manag. 2018, 20, 190–196. [Google Scholar] [CrossRef]
- Lyons, E.J.; Lewis, Z.H.; Mayrsohn, B.G.; Rowland, J.L. Behavior Change Techniques Implemented in Electronic Lifestyle Activity Monitors: A Systematic Content Analysis. J. Med. Internet Res. 2014, 16, 192. [Google Scholar] [CrossRef]
- Gupta, A.; Dhiman, N.; Yousaf, A.; Arora, N. Social comparison and continuance intention of smart fitness wearables: An extended expectation confirmation theory perspective. Behav. Inf. Technol. 2020. [Google Scholar] [CrossRef]
- Gao, Y.; Li, H.; Luo, Y. An empirical study of wearable technology acceptance in healthcare. Ind. Manag. Data Syst. 2015, 115, 1704–1723. [Google Scholar] [CrossRef]
- Li, H.; Wu, J.; Gao, Y.; Shi, Y. Examining individuals’ adoption of healthcare wearable devices: An empirical study from privacy calculus perspective. Int. J. Med. Inf. 2016, 88, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Farnell, G.; Barkley, J. The effect of a wearable physical activity monitor (Fitbit One) on physical activity behaviour in women: A pilot study. J. Hum. Sport Exerc. 2017, 1230–1237. [Google Scholar] [CrossRef]
- Montgomery, K.; Chester, J.; Kopp, K. Health Wearables: Ensuring Fairness, Preventing Discrimination, and Promoting Equity in an Emerging Internet-of-Things Environment. J. Inf. Policy 2018, 8, 34–77. [Google Scholar] [CrossRef]
- Hakonen, M.; Piitulainen, H.; Visala, A. Current state of digital signal processing in myoelectric interfaces and related applications. Biomed. Signal Process. Control 2015, 18, 334–359. [Google Scholar] [CrossRef]
- Rault, T.; Bouabdallah, A.; Challal, Y.; Marin, F. A survey of energy-efficient context recognition systems using wearable sensors for healthcare applications. Pervasive Mob. Comput. 2017, 37, 23–44. [Google Scholar] [CrossRef]
- Seneviratne, S.; Hu, Y.; Nguyen, T.; Lan, G.; Khalifa, S.; Thilakarathna, K.; Hassan, M.; Seneviratne, A. A Survey of Wearable Devices and Challenges. IEEE Commun. Surv. Tutor. 2017, 19, 2573–2620. [Google Scholar] [CrossRef]
- Islam, S.M.S.; Niessen, L.W.; Seissler, J.; Ferrari, U.; Biswas, T.; Islam, A.; Lechner, A. Diabetes knowledge and glycemic control among patients with type 2 diabetes in Bangladesh. SpringerPlus 2015, 4, 284. [Google Scholar] [CrossRef]
- Rollo, M.E.; Aguiar, E.J.; Williams, R.L.; Wynne, K.; Kriss, M.; Callister, R.; Collins, C.E.J.D. Metabolic syndrome. eHealth technologies to support nutrition and physical activity behaviors in diabetes self-management. Diabetes Metab. Syndr. Obes. Targets Ther. 2016, 9, 381. [Google Scholar] [CrossRef]
- Hartz, J.; Yingling, L.; Powell-Wiley, T.M. Use of Mobile Health Technology in the Prevention and Management of Diabetes Mellitus. Curr. Cardiol. Rep. 2016, 18, 130. [Google Scholar] [CrossRef]
- Polonsky, W.H.; Fisher, L.; Schikman, C.H.; Hinnen, D.A.; Parkin, C.G.; Jelsovsky, Z.; Petersen, B.; Schweitzer, M.; Wagner, R.S. Structured Self-Monitoring of Blood Glucose Significantly Reduces A1C Levels in Poorly Controlled, Noninsulin-Treated Type 2 Diabetes. Results Struct. Test. Program Study 2011, 34, 262–267. [Google Scholar] [CrossRef]
- Deiss, D.; Bolinder, J.; Riveline, J.-P.; Battelino, T.; Bosi, E.; Tubiana-Rufi, N.; Kerr, D.; Phillip, M. Improved Glycemic Control in Poorly Controlled Patients with Type 1 Diabetes Using Real-Time Continuous Glucose Monitoring. Diabetes Care 2006, 29, 2730–2732. [Google Scholar] [CrossRef] [PubMed]
- Heintzman, N.D. A Digital Ecosystem of Diabetes Data and Technology: Services, Systems, and Tools Enabled by Wearables. Sens. Appl. J. Diabetes Sci. Technol. 2016, 10, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Natarajan, T.; Balasubramanian, S.A.; Kasilingam, D.L. The moderating role of device type and age of users on the intention to use mobile shopping applications. Technol. Soc. 2018, 53, 79–90. [Google Scholar] [CrossRef]
- Okumus, B.; Bilgihan, A. Proposing a model to test smartphone users’ intention to use smart applications when ordering food in restaurants. J. Hosp. Tour. Technol. 2014, 5, 31–49. [Google Scholar] [CrossRef]
- Moores, T.T. Towards an integrated model of IT acceptance in healthcare. Decis. Support Syst. 2012, 53, 507–516. [Google Scholar] [CrossRef]
- Beglaryan, M.; Petrosyan, V.; Bunker, E. Development of a tripolar model of technology acceptance: Hospital-based physicians’ perspective on EHR. Int. J. Med. Inf. 2017, 102, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Kohli, R.; Tan, S.S.-L. Electronic health records: How can IS researchers contribute to transforming healthcare? MIS Q. 2016, 40, 553–573. [Google Scholar] [CrossRef]
- Zhang, M.; Luo, M.; Nie, R.; Zhang, Y. Technical attributes, health attribute, consumer attributes and their roles in adoption intention of healthcare wearable technology. Int. J. Med. Inf. 2017, 108, 97–109. [Google Scholar] [CrossRef]
- Bhattacherjee, A. Understanding Information Systems Continuance: An Expectation-Confirmation Model. MIS Q. 2001, 25, 351–370. [Google Scholar] [CrossRef]
- Cho, J. The impact of post-adoption beliefs on the continued use of health apps. Int. J. Med. Inf. 2016, 87, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Schifferstein, H.N.; Zwartkruis-Pelgrim, E.P. Consumer-product attachment: Measurement and design implications. Int. J. Des. 2008, 2, 1–13. [Google Scholar]
- Luarn, P.; Lin, H.-H. Toward an understanding of the behavioral intention to use mobile banking. Comput. Hum. Behav. 2005, 21, 873–891. [Google Scholar] [CrossRef]
- Wang, Y.S.; Wang, Y.M.; Lin, H.H.; Tang, T.-I. Determinants of user acceptance of Internet banking: An empirical study. Int. J. Serv. Ind. Manag. 2003, 14, 501–519. [Google Scholar] [CrossRef]
- Yang, H.; Yu, J.; Zo, H.; Choi, M. User acceptance of wearable devices: An extended perspective of perceived value. Telemat. Inform. 2016, 33, 256–269. [Google Scholar] [CrossRef]
- Cheng, Y.-M. Towards an understanding of the factors affecting m-learning acceptance: Roles of technological characteristics and compatibility. Asia Pac. Manag. Rev. 2015, 20, 109–119. [Google Scholar] [CrossRef]
- Wei, T.T.; Marthandan, G.; Chong, A.Y.L.; Ooi, K.B.; Arumugam, S.J.I.M. What drives Malaysian m-commerce adoption? An empirical analysis. Ind. Manag. Data Syst. 2009, 109, 370–388. [Google Scholar]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User Acceptance of Information Technology: Toward a Unified View. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Chen, K.; Chan, A.H.S. Gerontechnology acceptance by elderly Hong Kong Chinese: A senior technology acceptance model (STAM). Ergo 2014, 57, 635–652. [Google Scholar] [CrossRef]
- Or, C.K.L.; Karsh, B.-T. A Systematic Review of Patient Acceptance of Consumer Health Information Technology. J. Am. Med. Inf. Assoc. 2009, 16, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Thong, J.Y.L.; Hong, S.-J.; Tam, K.Y. The effects of post-adoption beliefs on the expectation-confirmation model for information technology continuance. Int. J. Hum. Comput. Stud. 2006, 64, 799–810. [Google Scholar] [CrossRef]
- Venkatesh, V.; Thong, J.Y.L.; Chan, F.K.Y.; Hu, P.J.-H.; Brown, S.A. Extending the two-stage information systems continuance model: Incorporating UTAUT predictors and the role of context. Inf. Syst. 2011, 21, 527–555. [Google Scholar] [CrossRef]
- Brinkman, W.P.; Haakma, R.; Bouwhuis, D.G. The theoretical foundation and validity of a component-based usability questionnaire. Behav. Inform. Technol. 2009, 28, 121–137. [Google Scholar] [CrossRef]
- Hung, S.-Y.; Chang, C.-M.; Kuo, S.-R. User acceptance of mobile e-government services: An empirical study. Gov. Inf. Q. 2013, 30, 33–44. [Google Scholar] [CrossRef]
- Wang, C. Antecedents and consequences of perceived value in Mobile Government continuance use: An empirical research in China. Comput. Hum. Behav. 2014, 34, 140–147. [Google Scholar] [CrossRef]
- Bhattacherjee, A.; Barfar, A. Information technology continuance research: Current state and future directions. Asia Pac. J. Inf. Syst. 2011, 21, 1–18. [Google Scholar]
- Venkatesh, V.; Goyal, S. Expectation Disconfirmation and Technology Adoption: Polynomial Modeling and Response Surface Analysis. MIS Q. 2010, 34, 281–303. [Google Scholar] [CrossRef]
- Flavián, C.; Gurrea, R. Perceived substitutability between digital and physical channels: The case of newspapers. Online Inf. Rev. 2007, 31, 793–813. [Google Scholar] [CrossRef]
- Bradford, M.; Florin, J. Examining the role of innovation diffusion factors on the implementation success of enterprise resource planning systems. Int. J. Account. Inf. Syst. 2003, 4, 205–225. [Google Scholar] [CrossRef]
- Li, J.; Ma, Q.; Chan, A.H.S.; Man, S.S. Health monitoring through wearable technologies for older adults: Smart wearables acceptance model. Appl. Ergon. 2019, 75, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Chong, A.Y.-L.; Chan, F.T.S.; Ooi, K.-B. Predicting consumer decisions to adopt mobile commerce: Cross country empirical examination between China and Malaysia. Decis. Support Syst. 2012, 53, 34–43. [Google Scholar] [CrossRef]
- Venkatesh, V.; Thong, J.Y.L.; Xu, X. Consumer Acceptance and Use of Information Technology: Extending the Unified Theory of Acceptance and Use of Technology. MIS Q. 2012, 36, 157–178. [Google Scholar] [CrossRef]
- Götz, O.; Liehr-Gobbers, K.; Krafft, M. Evaluation of Structural Equation Models Using the Partial Least Squares (PLS) Approach. In Handbook of Partial Least Squares: Concepts, Methods and Applications; Esposito Vinzi, V., Chin, W.W., Henseler, J., Wang, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; pp. 691–711. ISBN 978-3-540-32827-8. [Google Scholar]
- Premkumar, G.; Ramamurthy, K. The Role of Interorganizational and Organizational Factors on the Decision Mode for Adoption of Interorganizational Systems. Decis. Sci. 1995, 26, 303–336. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 1998. [Google Scholar]
- Nunnally, J.C. Psychometric Theory, 3rd ed.; Tata McGraw-Hill Education: New Delhi, India, 1994. [Google Scholar]
- Fornell, C.; Larcker, D.F. Structural Equation Models with Unobservable Variables and Measurement Error: Algebra and Statistics. J. Mark. Res. 1981, 18, 382–388. [Google Scholar] [CrossRef]
- Chang, C.-C.; Chi-Fang, Y.; Ju-Shih, T. Perceived convenience in an extended technology acceptance model: Mobile technology and English learning for college students. Australas. J. Educ. Technol. 2012, 28. [Google Scholar] [CrossRef]
- Ohk, K.; Park, S.-B.; Hong, J.-W. The influence of perceived usefulness, perceived ease of use, interactivity, and ease of navigation on satisfaction in mobile application. Adv. Sci. Technol. Lett. 2015, 84, 88–92. [Google Scholar]
- Roy, S. App adoption and switching behavior: Applying the extended tam in smartphone app usage. J. Inf. Technol. Manag. 2017, 14, 239–261. [Google Scholar] [CrossRef]
- Hsu, C.-L.; Lin, J.C.-C. What drives purchase intention for paid mobile apps?–An expectation confirmation model with perceived value. Electron. Commer. Res Appl 2015, 14, 46–57. [Google Scholar] [CrossRef]
- Tam, C.; Santos, D.; Oliveira, T. Exploring the influential factors of continuance intention to use mobile Apps: Extending the expectation confirmation model. Inf. Syst. Front. 2020, 22, 243–257. [Google Scholar] [CrossRef]
- Tang, J.; Zhang, B.; Akram, U. User willingness to purchase applications on mobile intelligent devices: Evidence from app store. Asia Pac. J. Mark. Logist. 2019. [Google Scholar] [CrossRef]
- Humbani, M.; Wiese, M. An integrated framework for the adoption and continuance intention to use mobile payment apps. Int. J. Bank Mark. 2019, 37, 646–664. [Google Scholar] [CrossRef]
- Khasawneh, M.H.A.; Irshaidat, R. Retailing. Empirical validation of the decomposed theory of planned behaviour model within the mobile banking adoption context. Int. J. Electron. Mark. Retail. 2017, 8, 58–76. [Google Scholar] [CrossRef]
- Liébana-Cabanillas, F.; Ramos de Luna, I.; Montoro-Ríos, F.J. User behaviour in QR mobile payment system: The QR Payment Acceptance Model. Technol. Anal. Strateg. Manag. 2015, 27, 1031–1049. [Google Scholar] [CrossRef]
- Mallat, N. Exploring consumer adoption of mobile payments–A qualitative study. J. Strateg. Inf. Syst. 2007, 16, 413–432. [Google Scholar] [CrossRef]
- Muñoz-Leiva, F.; Climent-Climent, S.; Liébana-Cabanillas, F. Determinants of intention to use the mobile banking apps: An extension of the classic TAM model. Span. J. Mark. ESIC 2017, 21, 25–38. [Google Scholar] [CrossRef]
- Okumus, B.; Ali, F.; Bilgihan, A.; Ozturk, A.B. Psychological factors influencing customers’ acceptance of smartphone diet apps when ordering food at restaurants. Int. J. Hosp. Manag. 2018, 72, 67–77. [Google Scholar] [CrossRef]
- Baumgartner, H.; Homburg, C. Applications of structural equation modeling in marketing and consumer research: A review. Int. J. Mark. Res. 1996, 13, 139–161. [Google Scholar] [CrossRef]
- Doll, W.J.; Xia, W.; Torkzadeh, G. A Confirmatory Factor Analysis of the End-User Computing Satisfaction Instrument. MIS Q. 1994, 18, 453–461. [Google Scholar] [CrossRef]
- Hair, J.; Black, W.; Babin, B.; Anderson, R. Multivariate Data Analysis: A Global Perspective, 7th ed.; Pearson Prentice Hall: London, UK, 2010. [Google Scholar]
- Bartholomew, D.J.; Knott, M.; Moustaki, I. Latent Variable Models and Factor Analysis: A Unified Approach, 3rd ed.; Wiley: Chichester, UK, 2011; ISBN 978-0-470-97192-5. [Google Scholar]
- Gefen, D.; Straub, D.; Boudreau, M. Structural Equation Modeling and Regression: Guidelines for Research Practice. Commun. Assoc. Inf. Syst. 2000, 7, 1–70. [Google Scholar] [CrossRef]
- Singh, R.; Sandhu, H.S.; Metri, B.A.; Kaur, R.J.I. Organizational performance and retail challenges: A structural equation approach. iBusiness 2011, 3, 159. [Google Scholar] [CrossRef][Green Version]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models; Long, J.S., Bollen, K.A., Eds.; Sage: Beverly Hills, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Yoon, C.; Kim, S. Convenience and TAM in a ubiquitous computing environment: The case of wireless LAN. Electron. Commer. Res. Appl. 2007, 6, 102–112. [Google Scholar] [CrossRef]
- Kim Ki, J.; Shin, D.-H. An acceptance model for smart watches: Implications for the adoption of future wearable technology. Internet Res. 2015, 25, 527–541. [Google Scholar] [CrossRef]
- Jeong, S.C.; Kim, S.-H.; Park, J.Y.; Choi, B. Domain-specific innovativeness and new product adoption: A case of wearable devices. Telemat. Inform. 2017, 34, 399–412. [Google Scholar] [CrossRef]


{kind=link}
| Absolute Numbers | % | |
|---|---|---|
| Gender | ||
| Female | 89 | 39.9% |
| Male | 134 | 60.1% |
| Age | ||
| 60–64 years | 93 | 41.7% |
| 65–69 years | 67 | 30.0% |
| 70–74 years | 41 | 18.4% |
| 75+ years | 22 | 9.9% |
| Marital status | ||
| Married | 124 | 55.6% |
| Never married | 69 | 30.9% |
| Separated/Divorced | 23 | 10.3% |
| Widowed | 7 | 3.1% |
| Employment status | ||
| Work Full Time | 158 | 70.9% |
| Work Part Time | 19 | 8.5% |
| Away from Work | 4 | 1.8% |
| Unemployed | 7 | 3.1% |
| Not in the Labour force | 35 | 15.7% |
| Highest level of education | ||
| High School | 12 | 5.4% |
| Diploma | 25 | 11.2% |
| Undergraduate degree | 119 | 53.4% |
| Postgraduate degree | 67 | 30.0% |
| Constructs | Items | Loadings | Mean | SD |
|---|---|---|---|---|
| PU | PU1 | 0.679 | 4.72 | 1.71 |
| AVE = 0.501 | PU2 | 0.780 | ||
| CR = 0.800 | PU3 | 0.668 | ||
| C-Alpha = 0.799 | PU4 | 0.700 | ||
| PEOU | PEOU1 | 0.780 | 5.33 | 1.76 |
| AVE = 0.560 | PEOU2 | 0.721 | ||
| CR = 0.840 | PEOU3 | 0.710 | ||
| C-Alpha = 0.835 | PEOU4 | 0.779 | ||
| PIR AVE = 0.674 CR = 0.861 C-Alpha = 0.861 | PIR1 PIR2 PIR3 | 0.795 0.836 0.831 | 4.01 | 1.46 |
| PCR | PCR1 | 0.787 | 5.40 | 1.83 |
| AVE = 0.573 | PCR2 | 0.784 | ||
| CR = 0.843 | PCR3 | 0.712 | ||
| C-Alpha = 0.842 | PCR4 | 0.742 | ||
| COM AVE = 0.530 CR = 0.770 C-Alpha = 0.757 | COM1 COM2 COM3 | 0.563 0.748 0.842 | 3.99 | 1.34 |
| SI | SI1 | 0.578 | 6.33 | 2.11 |
| AVE = 0.520 | SI2 | 0.808 | ||
| CR = 0.841 | SI3 | 0.873 | ||
| C-Alpha = 0.848 | SI4 | 0.620 | ||
| SI5 | 0.681 | |||
| CI | CI1 | 0.834 | 4.04 | 1.74 |
| AVE = 0.734 | CI2 | 0.874 | ||
| CR = 0.917 | CI3 | 0.888 | ||
| C-Alpha = 0.922 | CI4 | 0.829 |
| CI | PU | PEOU | PIR | PCR | COM | SI | |
|---|---|---|---|---|---|---|---|
| CI | 0.857 a | - | |||||
| PU | 0.291 *** | 0.708 a | - | ||||
| PEOU | 0.297 *** | 0.349 *** | 0.748 a | - | |||
| PIR | 0.287 *** | 0.099 ns | 0.256 ** | 0.821 a | - | ||
| PCR | 0.249 ** | 0.108 ns | 0.100 ns | 0.192 * | 0.757 a | - | |
| COM | 0.311 *** | 0.193 * | 0.078 ns | 0.288 *** | 0.107 ns | 0.728 a | - |
| SI | 0.279 *** | 0.194 * | 0.241 ** | 0.163 * | 0.111 ns | 0.127 ns | 0.721 a |
| Hypothesis | Path | Β | T Statistics | Comments |
|---|---|---|---|---|
| H1 | PU → CI | 0.183 | 2.258 | Supported * |
| H2 | PEOU → CI | 0.165 | 2.305 | Supported * |
| H3 | PIR → CI | 0.138 | 2.120 | Supported * |
| H4 | PCR → CI | 0.165 | 2.429 | Supported * |
| H5 | COM → CI | 0.285 | 2.815 | Supported ** |
| H6 | SI → CI | 0.226 | 2.429 | Supported * |
| Fit Indices | Recommended Value | Research Model |
|---|---|---|
| χ2/df | ≤3.00 | 1.716 |
| GFI | ≥0.90 | 0.840 |
| AGFI | ≥0.80 | 0.810 |
| CFI | ≥0.90 | 0.918 |
| TLI | ≥0.90 | 0.910 |
| NFI | ≥0.90 | 0.825 |
| RMSEA | ≤0.08 | 0.057 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad, A.; Rasul, T.; Yousaf, A.; Zaman, U. Understanding Factors Influencing Elderly Diabetic Patients’ Continuance Intention to Use Digital Health Wearables: Extending the Technology Acceptance Model (TAM). J. Open Innov. Technol. Mark. Complex. 2020, 6, 81. https://doi.org/10.3390/joitmc6030081
Ahmad A, Rasul T, Yousaf A, Zaman U. Understanding Factors Influencing Elderly Diabetic Patients’ Continuance Intention to Use Digital Health Wearables: Extending the Technology Acceptance Model (TAM). Journal of Open Innovation: Technology, Market, and Complexity. 2020; 6(3):81. https://doi.org/10.3390/joitmc6030081
Chicago/Turabian StyleAhmad, Ashfaq, Tareq Rasul, Anish Yousaf, and Umer Zaman. 2020. "Understanding Factors Influencing Elderly Diabetic Patients’ Continuance Intention to Use Digital Health Wearables: Extending the Technology Acceptance Model (TAM)" Journal of Open Innovation: Technology, Market, and Complexity 6, no. 3: 81. https://doi.org/10.3390/joitmc6030081
APA StyleAhmad, A., Rasul, T., Yousaf, A., & Zaman, U. (2020). Understanding Factors Influencing Elderly Diabetic Patients’ Continuance Intention to Use Digital Health Wearables: Extending the Technology Acceptance Model (TAM). Journal of Open Innovation: Technology, Market, and Complexity, 6(3), 81. https://doi.org/10.3390/joitmc6030081